advance angioplasty 2004 london, jan 15-16 2004 latest clinical evidence with dexamet germano di...
TRANSCRIPT
ADVANCE ANGIOPLASTY 2004LONDON, Jan 15-16 2004
LATEST CLINICAL EVIDENCEWITH DEXAMET
GERMANO DI SCIASCIO, MD, FACC, FESC
Professor and Chairman of Cardiology,Campus Bio-Medico University of Rome
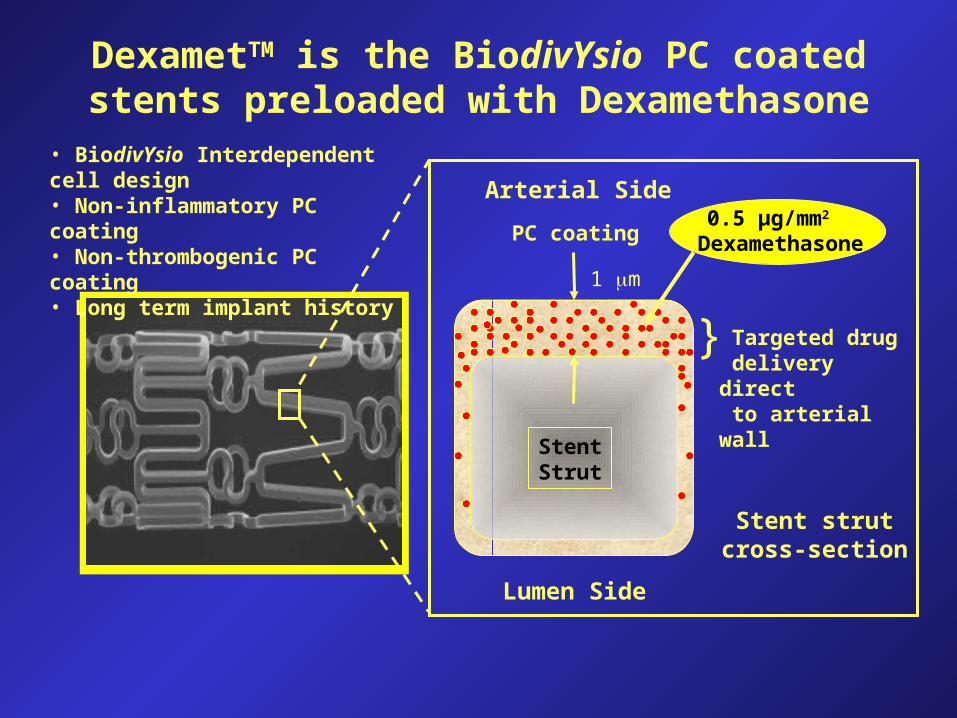
DexametTM is the BiodivYsio PC coated stents preloaded with Dexamethasone
• BiodivYsio Interdependent cell design• Non-inflammatory PC coating • Non-thrombogenic PC coating• Long term implant history
1 m
StentStrut
} Targeted drug delivery direct to arterial wall
0.5 µg/mm2 DexamethasonePC coating
Arterial Side
Lumen Side
Stent strutcross-section

• is a potent anti-inflammatory agent that treats the first step of the neointima formation/restenosis process
• has also anti-proliferative action by affecting the inflammation process
• is non-cytotoxic and does not destroy healthy cells and does not reduce or slow down the re-endothelisation
DexamethasoneO
HO
F
HOO
OH
1 S.H.Park and A.M.Lincoff, Semin. Interv. Cardiol., 1998, 3, 191-195

• is delivered (when it’s most needed) early to target the inflammatory cells
• has strong clinical experience in humans
demonstrated clinical benefits preferably in unstable in STRIDE and SAFE
Dexamethasone (II)O
HO
F
HOO
OH
1 S.H.Park and A.M.Lincoff, Semin. Interv. Cardiol., 1998, 3, 191-195

- A pilot Phase II trial, multi-centre, prospective, non-randomised study. Dexamethasone dose 0.5 ug/mm2
- 71 patients in 8 centres in Belgium
- PI: Ivan De Scheerder
- Endpoints:
- 30-day and 6-month MACE
- In-stent restenosis 6 months
- Clinical and QCA :Late loss, loss index, MLD
Dexamet’s first clinical trial :STRIDEStudy of anti-restenosis with BiodivYsio Dexamethasone-Eluting stent

STRIDESTudy of Anti-Restenosis with BIodivYsio Dexamethasone-Eluting Stent
71 patients with 6-month angiographic follow-up
Stent: BiodivYsio stent (dexamethasone 45 μg) %
in-s
tent
sten
osis
Unstable angina Stable angina
p=0.017
MACE at 30 days = 1% (TLR =1%)MACE at 6 months = 3% (TLR=3%)MACE at 12 months: 3% (TLR=3%)
0
10
20
30
40
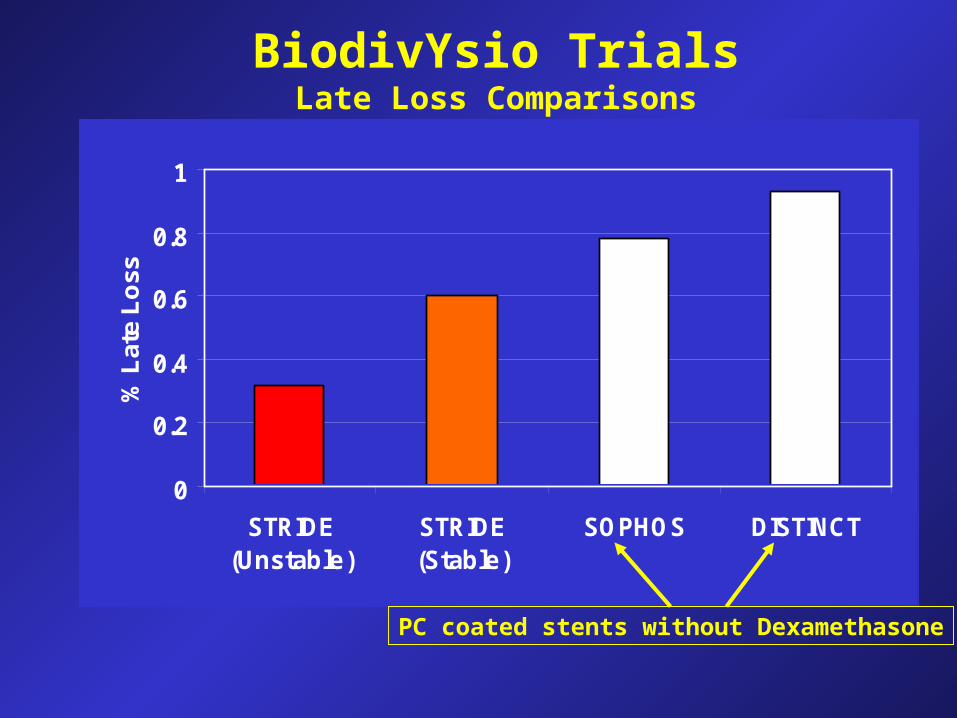
BiodivYsio TrialsLate Loss Comparisons
0
0.2
0.4
0.6
0.8
1
STRIDE(Unstable)
STRIDE (Stable)
SOPHOS DISTINCT
% L
ate
Lo
ss
PC coated stents without Dexamethasone

- A multi-centre registry with DexametTM & Dexamet SV
- PI: Dr Pieter Stella, Utrecht, Netherlands
- 1000 “Real-world” patients with no specific inclusion/exclusion criteria - patients must meet the indications specified in the Directions For Use
- 66 centres over 16 countries in Europe, Middle-East, Africa and Asia-Pacific- Endpoints are in-hospital, 30-day and 6-month MACE
- Results available at JIM 2004
First registry of DexametTM : SAFE
DEXAMETHASONE-ELUTING STENTS IMPROVE SIGNS OF INFLAMMATION IN PATIENTS
WITH UNSTABLE CORONARY SYNDROMES UNDERGOING PERCUTANEOUS CORONARY
INTERVENTION
G. Patti, A. D’Ambrosio, A. Carcagni’, M. Cortes-Morichetti,P. Carminati, G. Di Sciascio
CAMPUS BIOMEDICO UNIVERSITY OF ROME

Study design: case-control study with prospective evaluation
Population: 60 pts receiving dexamethasone-eluting stent (Dexamet, N=30) or Biodivysio phosphorylcholine-coated stent (N=30)
Inclusion criteria: - unstable angina (IIB-IIIB) or angina post recent (< 1 mo) myocardial infarction
- angiographic evidence of “complex” coronary lesions that could be covered by a single stent
Plasma levels of CRP were measured at: - 3 to 6 hours before PCI - 6, 24, 48 hours and 7 days after PCI
Follow-up assessment: occurrence of MACE (myocardial infarction, death, repeat revascularization)
DEXAMETHASONE-ELUTING STENTS IN UNSTABLE CORONARY SYNDROMES
Methods



3.7**5.4 * 3.6
5.2
2.8
2.33.2
5.8
9.8
11.4
0
3
6
9
12
15
18
Pre 6 h post 24 h post 48 h post 7 days post
CR
P m
g/l
DexametTM
Non DES
* P=0.041 vs non DES** P=0.026 vs non DES
DEXAMETHASONE-ELUTING STENTS
IN UNSTABLE CORONARY SYNDROMES
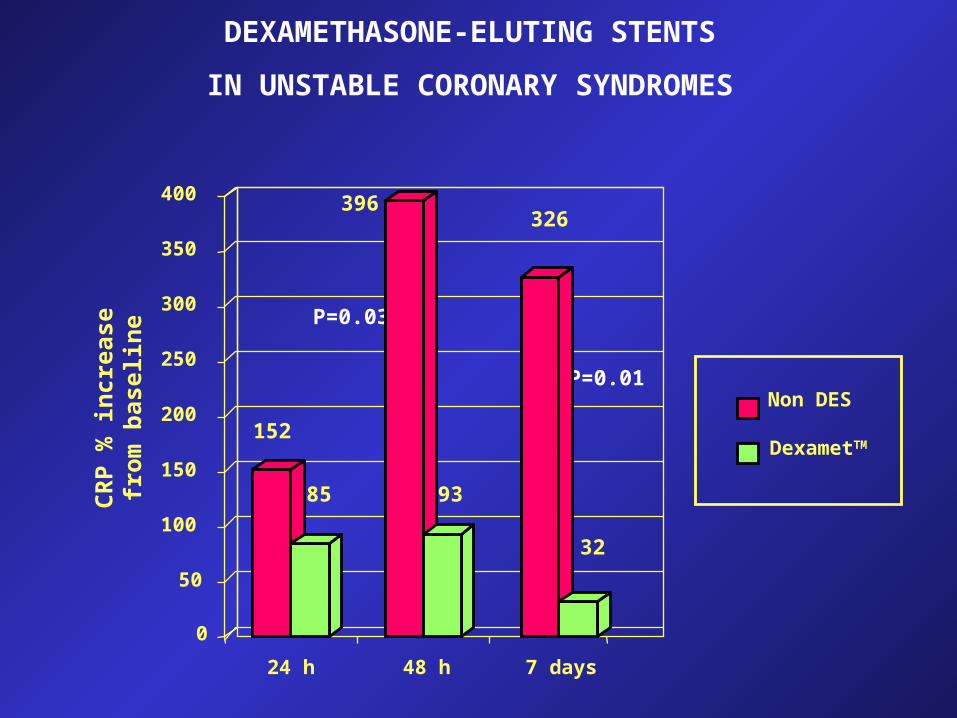
0
50
100
150
200
250
300
350
400
24 h 48 h 7 days
Non DES
DexametTM152
85
396
93
326
32
P=0.03
P=0.01
CR
P %
incr
ease
from
bas
elin
e
DEXAMETHASONE-ELUTING STENTS
IN UNSTABLE CORONARY SYNDROMES

Baseline CRP <3 mg/l
(N=19)
Baseline CRP 3 mg/l (N=11)
0
40
80
120
160
200
24 h 48 h 7 days
CR
P p
e rc e
n t i n
c re a
s efr
om b
a se l
ine
P=0.009
121
69
199
40
96
14
DEXAMETHASONE-ELUTING STENTS
IN UNSTABLE CORONARY SYNDROMES

0
20
40
60
80
100
0 1 2 3 4
% o
f pa
tien
ts
Dexamet Non DES
months after stenting
6
P=0.06
Event-free survival curves
DEXAMETHASONE-ELUTING STENTS
IN UNSTABLE CORONARY SYNDROMES

CONCLUSIONS
Dexamethasone-eluting stents improve early inflammatoryresponse after PCI; this effect is more evident in pts with higher baseline CRP status
The sustained attenuation of CRP values at 7 days may suggestearly plaque stabilization with dexamethasone-eluting stentsin pts with unstable coronary syndromes
Clinical follow-up at 6 months shows a trend towards favorableintermediate-term results
Will steroid-eluting stents be the treatment of choice for ptswith unstable coronary syndromes?
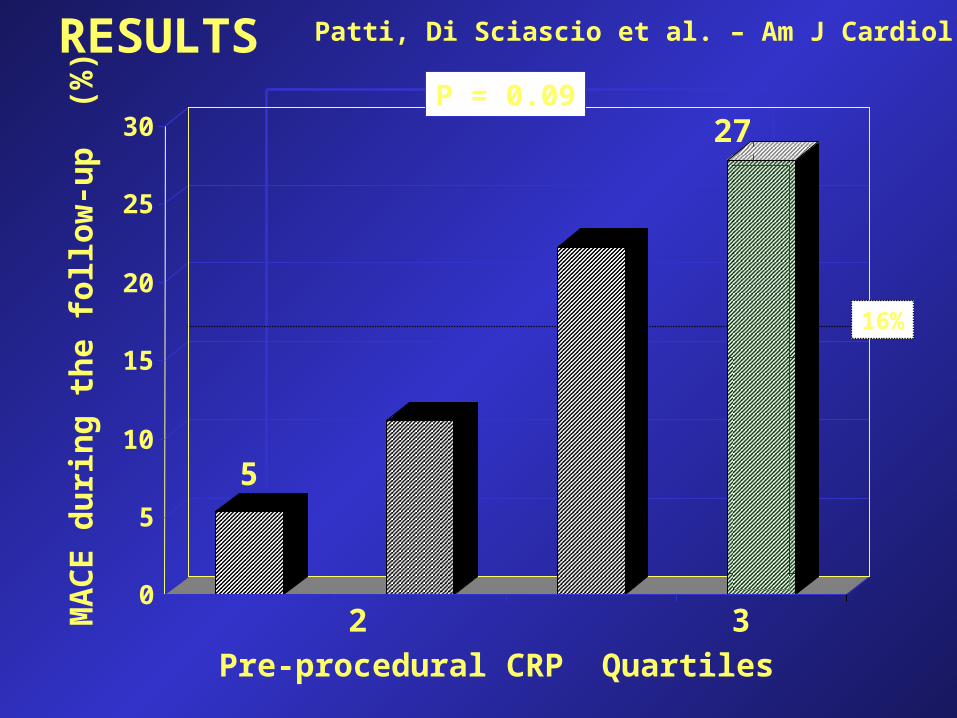
MA
CE
du
rin
g th
e fo
llow
-up
(%
)
1 2 3 4
Pre-procedural CRP Quartiles
0
5
10
15
20
25
30
16%
P = 0.09
5
27
RESULTS Patti, Di Sciascio et al. – Am J Cardiol

From morphology ................ To plaque “biology”


CR
P (
mg
/dl)
0
0,40
0,80
1,20
ControlsN=12
Stable anginaN=49
Unstable anginaN=57
P=0.046
P=0.66
P=0.07
Distribution of CRP plasma levels
Patti, Di Sciascio et al. – IL-1Ra: a sensitive marker of instability in patients with coronary artery disease J Thromb Thrombol 2002; 14: 139
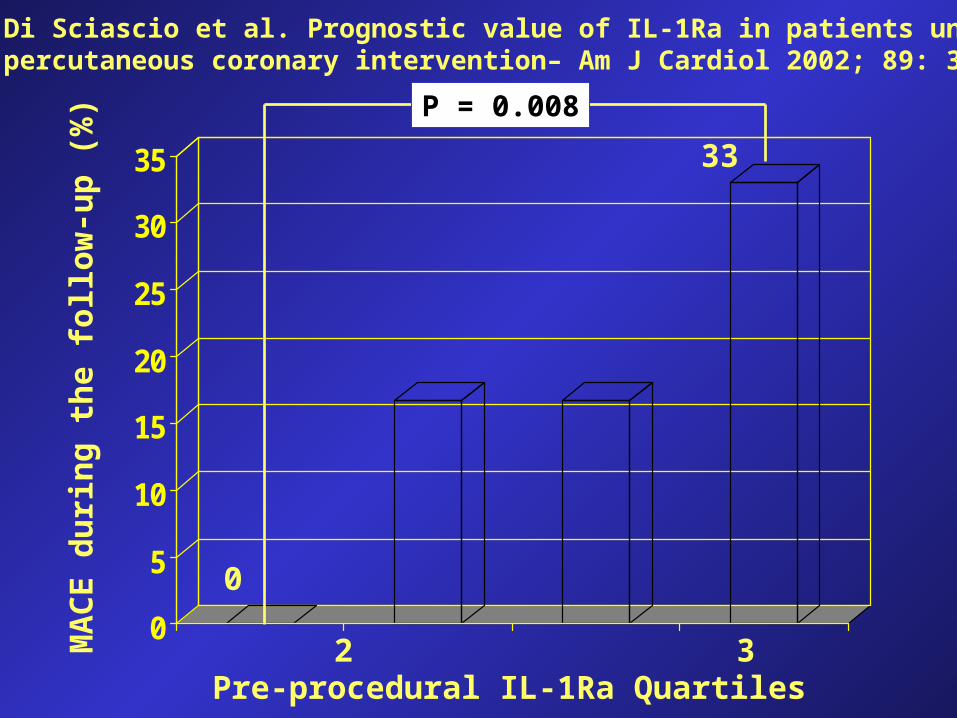
0
5
10
15
20
25
30
35
MA
CE
du
rin
g th
e fo
llow
-up
(%
)
1 2 3 4 Pre-procedural IL-1Ra Quartiles
P = 0.008
33
0
Patti, Di Sciascio et al. Prognostic value of IL-1Ra in patients undergoing percutaneous coronary intervention– Am J Cardiol 2002; 89: 372


SMC ProliferationSMC Proliferation
MigrationMigration Matrix secretionMatrix secretion
SMC receptors
Arterial injuryArterial injury
Growth Factors & cytokinesGrowth Factors & cytokines
ThrombusThrombus InflammationInflammation
G0 G1 G2
S
M
Smooth muscle cell (SMC)Smooth muscle cell (SMC)
Signal transduction
Cell cycle
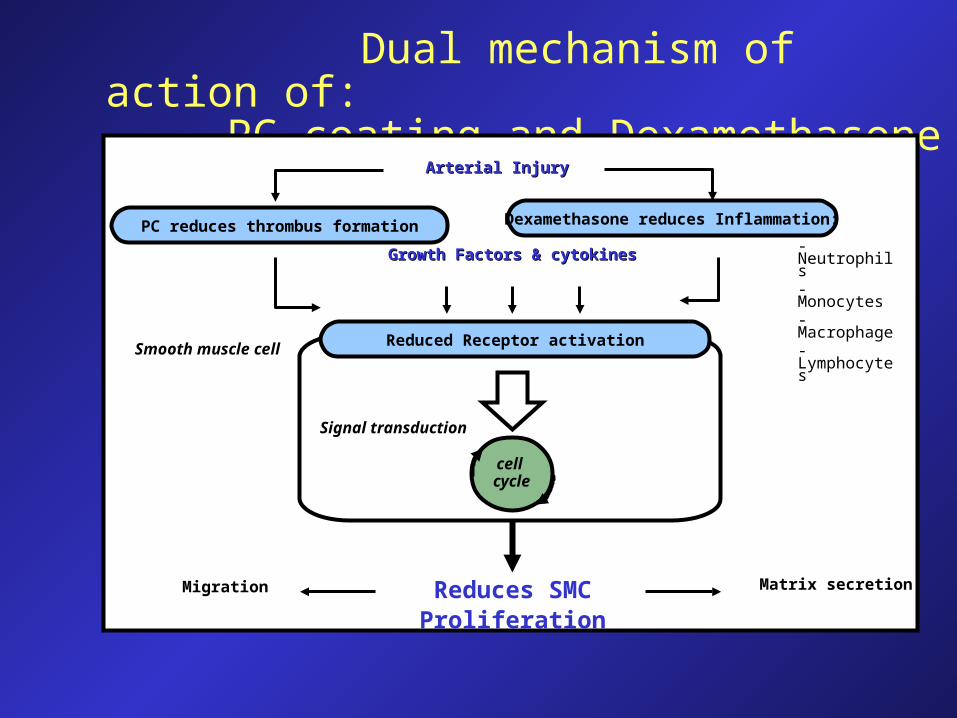
Dual mechanism of action of: PC coating and Dexamethasone
cell cycle
Smooth muscle cell
Growth Factors & cytokinesGrowth Factors & cytokines
Arterial InjuryArterial Injury
- Neutrophils- Monocytes- Macrophage- Lymphocytes
Reduces SMC Proliferation
Matrix secretionMigration
Reduced Receptor activation
PC reduces thrombus formation Dexamethasone reduces Inflammation:
Signal transduction

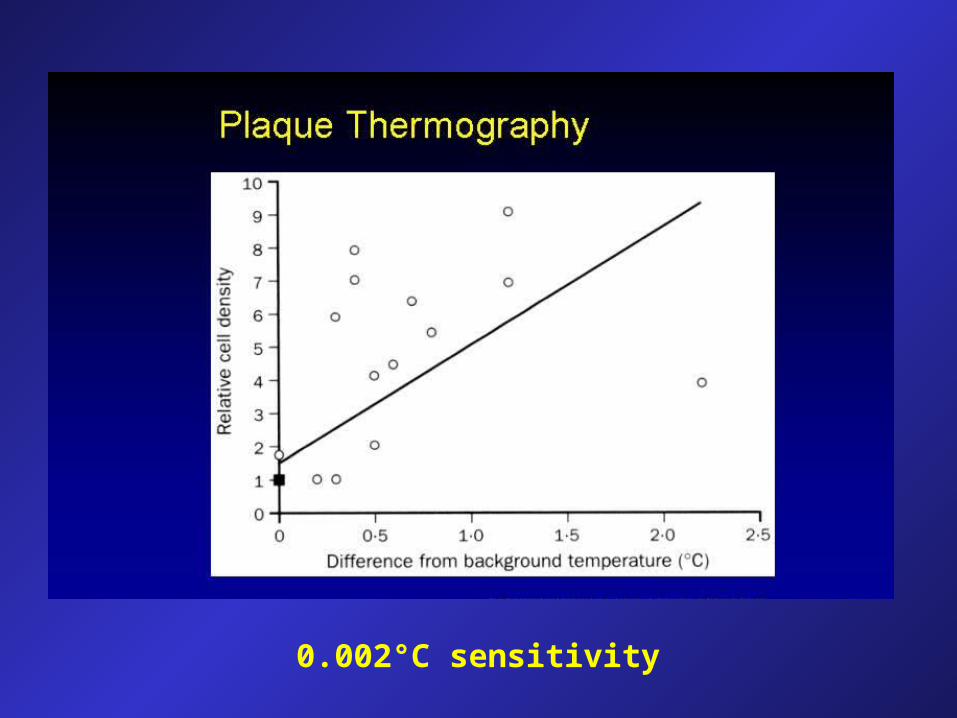
THERMOGRAPHY in ACUTE CORONARY SYNDROMES
• Temperature of the plaque is inversely correlated to cap thickness (Casscells W, Lancet 1996)
• Pts presenting with AMI and unstable angina have significantly more temperature heterogeneity in their coronary atherosclerotic plaques than pts with stable angina (Stefanadis C, Circulation 1999).
• Temperature was found to be the most powerful predictor of outcome (Stefanadis C, Circulation 2000) and to have a significant correlation with CRP levels (Stefanadis C, J Mol Cell Cardiol 2000)
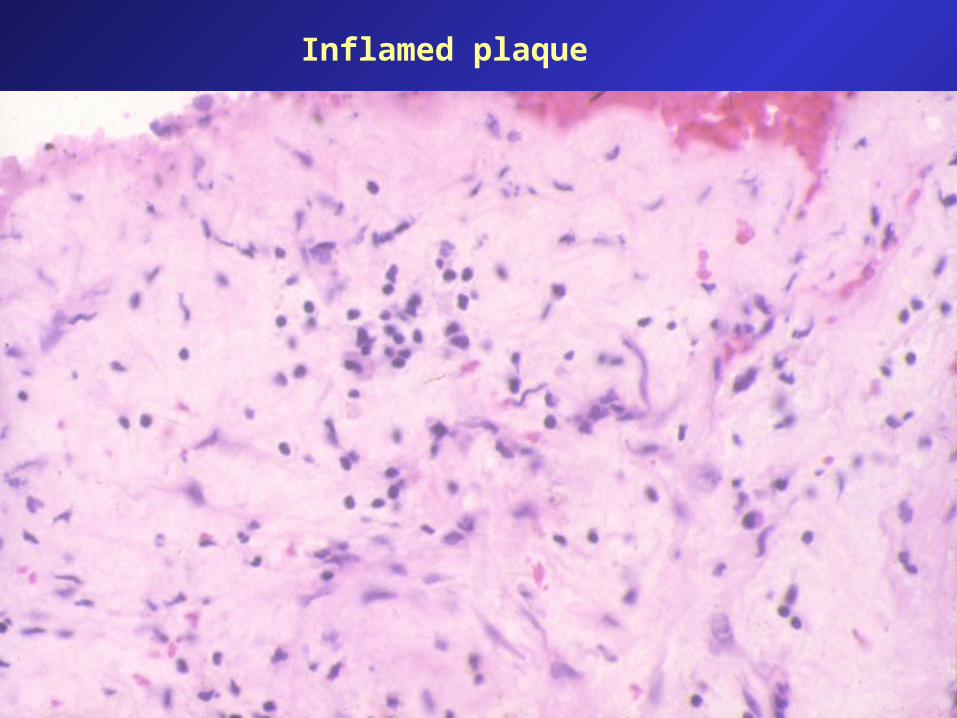
Inflamed plaque
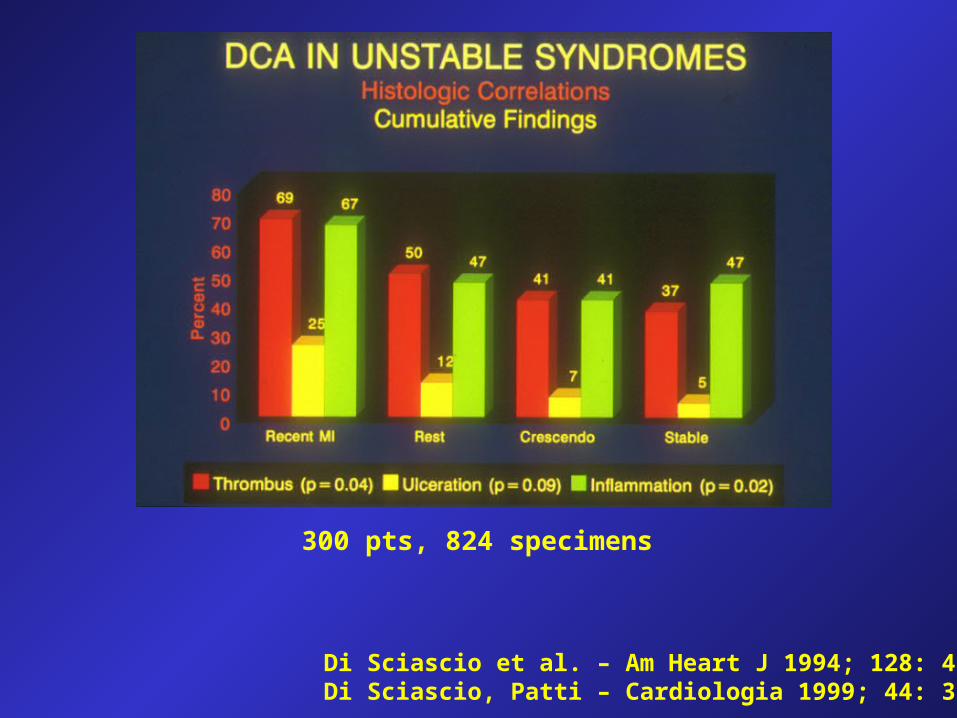
Di Sciascio et al. – Am Heart J 1994; 128: 419-26Di Sciascio, Patti – Cardiologia 1999; 44: 333-9
300 pts, 824 specimens


0
10
20
30
40
50
60
70
80
90%
Recurrent ischemia In-hosp. MACE
UA and CRP<0.3 mg/dl
UA and CRP>0.3 mg/dl
Liuzzo, Maseri et al. The prognostic value of CRP and serum amyloid A protein in severe unstable angina. N Engl J Med 1994; 331: 417

IL1-
Ra
(pg/
ml)
ControlsN=12
Stable anginaN=49
Unstable anginaN=47
0
100
200
300
400
500
P=0.038
P=0.002
P=0.99
IL-1Ra in ischemic syndromes
Patti, Di Sciascio et al. – IL-1Ra: a sensitive marker of instability in patients with coronary artery disease J Thromb Thrombol 2002; 14: 139
0
20
40
60
80
100
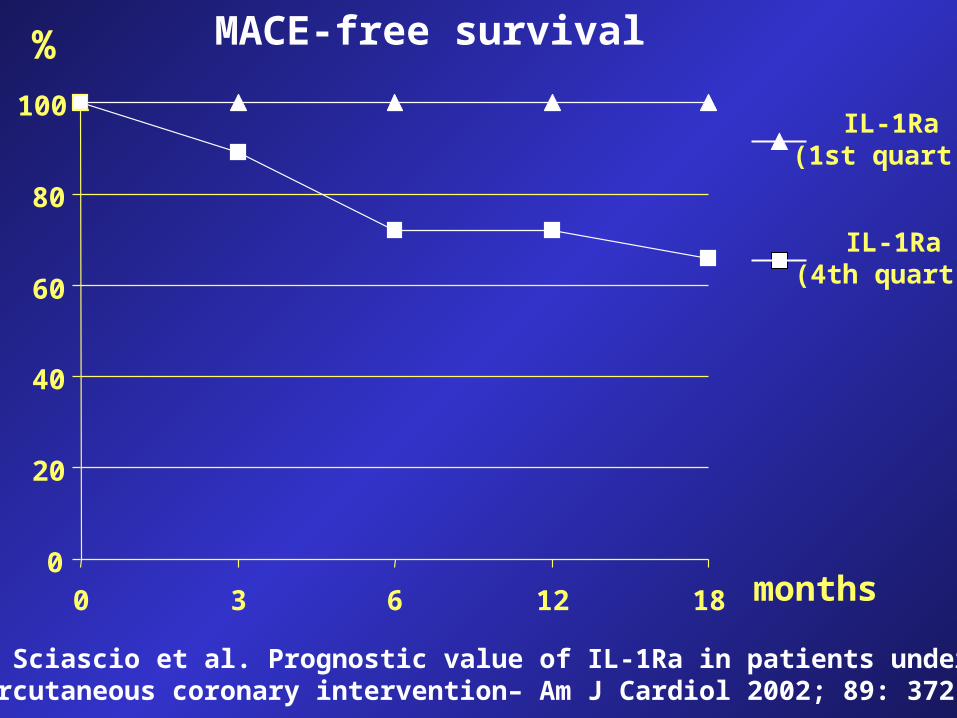
0 3 6 12 18 months
IL-1Ra (1st quart.)
IL-1Ra (4th quart.)
MACE-free survival%
Patti, Di Sciascio et al. Prognostic value of IL-1Ra in patients undergoing percutaneous coronary intervention– Am J Cardiol 2002; 89: 372

Drug Eluting Stent Trials
0,45
0,60
0,32 0,30
0,17
0,30
0,94
0
0,2
0,4
0,6
0,8
1
Stride Stride Stride Aspect Sirius TAXUS II Distinct(stable AP)(unstable AP) (Non-drug)
Late Loss (mm)
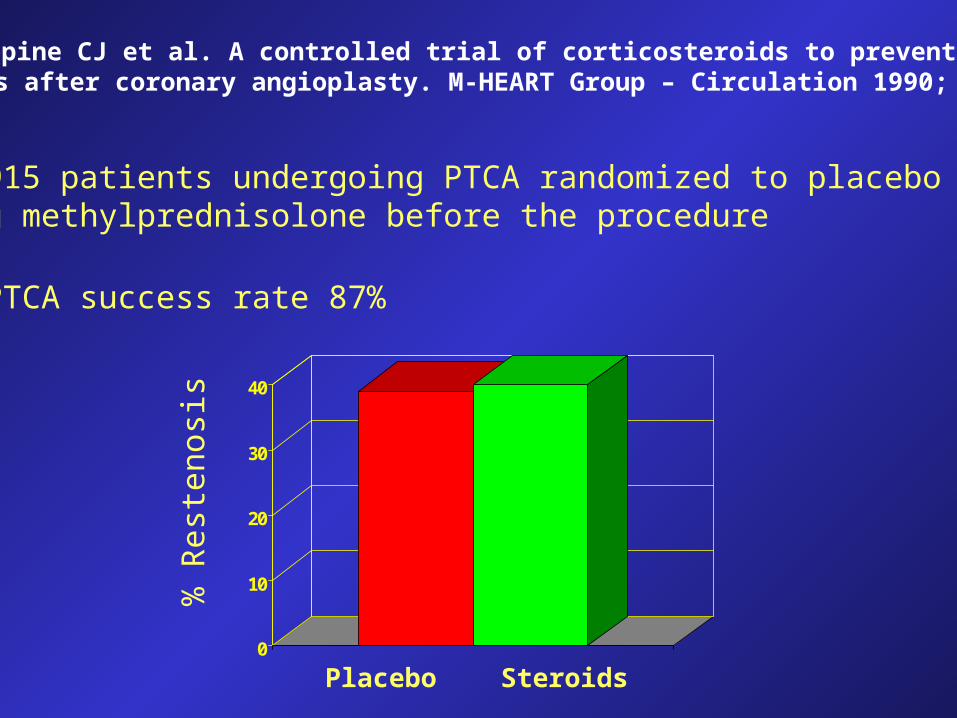
Pepine CJ et al. A controlled trial of corticosteroids to prevent restenosis after coronary angioplasty. M-HEART Group – Circulation 1990; 81: 1753
- 915 patients undergoing PTCA randomized to placebo or 1 g methylprednisolone before the procedure
- PTCA success rate 87%
0
10
20
30
40
Placebo Steroids
% R
este
nosi
s

Versaci et al. Immunosuppressive therapy for the prevention of restenosis after coronaryArtery stent implantation (IMPRESS study) – JACC 2002; 40: 1935
Oral prednisone therapy for 45 days in pts with elevated (>0.5 mg/dl) CRP levels 72 hours post PCI