adult in-patient services (nursing unit)
TRANSCRIPT

Adult In-Patient Services (Nursing Unit)
Prof (Col) Dr R N Basu
• The answer is difficult because there is a continuously changing need of healthcare delivery system
• Some of these are:
• Changing business need resulting in shorter and shorter length of stay
• Rapidly changing technology
• Changes in patient demographic profile
• Changes in disease profile
• Variability of acuity levels of the disease even during the same period of hospitalisation
• More and more complex operative procedures performed
2

• The NICE guidelines on safe nurse staffing does not recommend any universally applicable nurse staffing level that is applicable to the entire hospital
• It says that each ward has to determine its own nursing staff requirements to ensure safe patient care
• Instead the guidance makes recommendations about the factors that should be systematically assessed at ward level to determine nursing staff establishment
• Then it recommends on-the-day assessment of nursing staff requirements to ensure that the nursing needs of individual patients are met throughout a 24-hour period
3

• Factors to determine nursing staff requirements
• Patient factors:
• Use individual patient’s nursing needs as the main factor for calculating the nursing staff requirements for a ward
• Nursing needs include both patient acuity and patient dependency
• Make a holistic assessment of each patient’s nursing needs and take account of specific nursing requirements and disabilities, as well as other patient factors that may increase nursing staff requirements
• Difficulties with cognition or confusion
• End-of-life care
4
• Increased risk of clinical deterioration
• Need for the continuous presence of a member of nursing team (specialingcare)
• Ward factors
• Expected patient turnover in the ward during a 24-hour period (including both planned and unscheduled admissions, discharges and transfers
• Ward layout and size
• This includes the need to ensure the safety of patients who cannot be easily observed, and the distance needed to travel to access resources within the ward
5

• Nursing staff factors
• Nursing activities and responsibilities, other than direct patient care
• These include:
• Communicating with relatives and carers
• Managing the nursing team and the ward
• Professional supervision and mentoring of nursing staff, (student nurses are considered supernumerary)
• Communicating with and providing nursing client support to all healthcare staff involved with the care of patients on the ward
• Undertaking audit, and staff appraisal and performance reviews
6

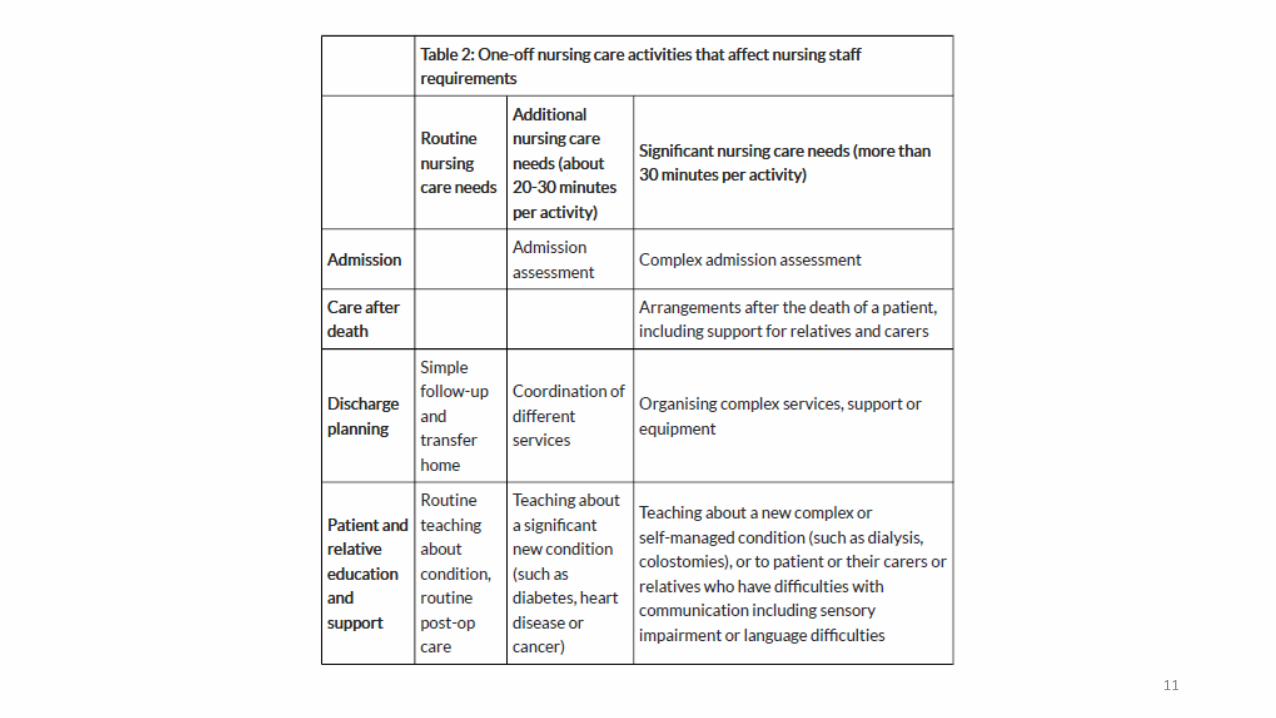
• Ongoing nursing care activities that affect nursing staff requirement
7
Routine Nursing care Needs Additional nursing care needs (about 20-30 minute per activity
Significant nursing care needs (more than 30 minutes per activity)
Care planning Simple condition and care plan
Complex condition or care plan (such as multiple comorbities)
Attending mulridisciplinary meetings
Direct contact and communication
Providing information and support to patients, including all emotional and spiritual support
Complex multiple health needs
Difficulties with communication including sensory impairment or language difficulties

8
9

10
11

12

• Patient reported outcome measures:
• Adequacy of meeting nursing care needs
• Adequacy of provided pain management
• Adequacy of communication with nursing team
• Safety outcome measures
• Falls:
• Record any fall that a patient has experienced
• Severity of fall could be further defined
• No harm, low harm, severe harm, death
13
• Pressure ulcer:
• Record pressure ulcers developed or worsened 72 hours or more after admission
• The patient’s worst new ulcer could be categorised as grade 2,3, or 4
• Medication administration errors
• Record any error in the preparation, administration or omission of medication by nursing staff
• The severity of error also be recorded
14

• Staff reported measures
• Missed breaks
• Record the proportion of expected breaks that were unable to be taken by nursing staff working in inpatient hospital wards
• Nursing overtime
• Record the proportion of nursing staff on inpatient hospital wards working extra hours (both paid and unpaid)
15
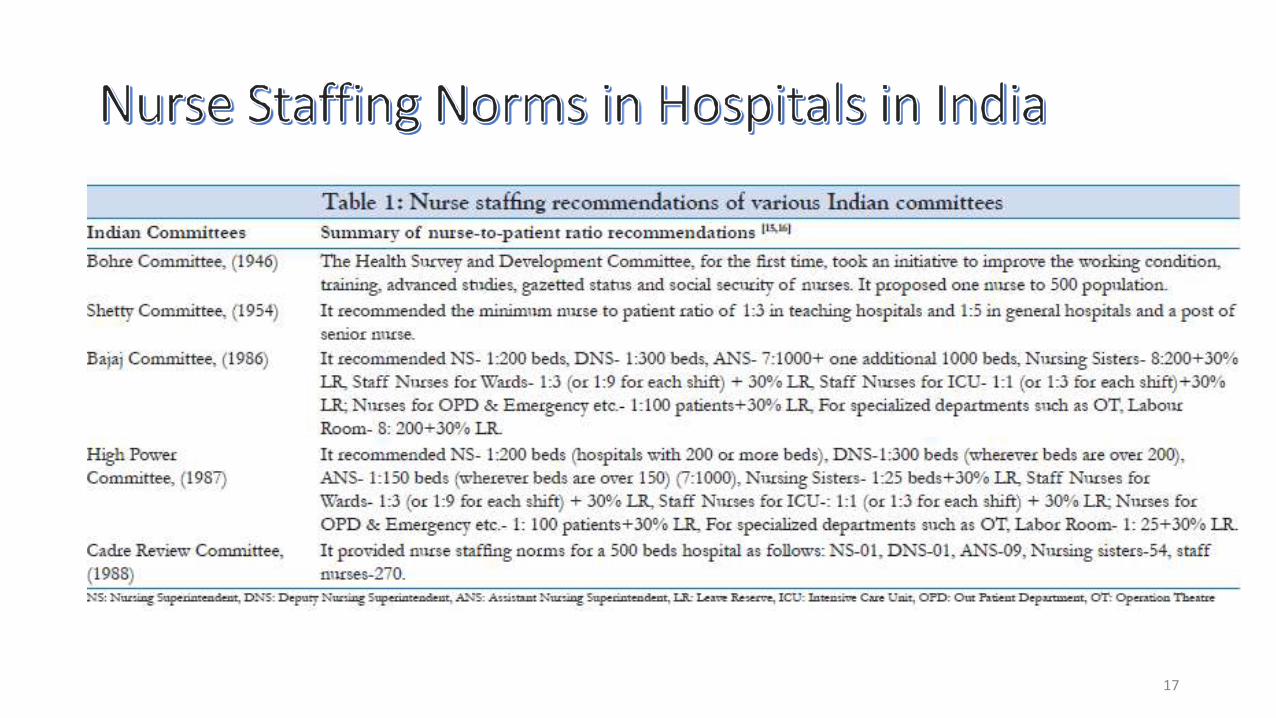
• Various Indian committees and regulatory bodies have provided recommendations on bench marks of the nurse-to patient ratio
• There is no evidence that these bodies critically analysed the various factors that contribute to safe patient care
• Various international guidelines have scientifically analysed the different factors that are required to decide on a norm
• The hospitals in India take these norms as sacrosanct and adopt them without considering the complex and dynamic nature of nurse staffing
16
17

• Recommendations of the various statutory bodies
• Indian Nursing Council (1985) recommendation
• Chief nursing officer 1:500 beds
• NS 1:400 beds
• DNS 1:300 beds, 1 additional for every 200 beds
• Nursing sisters 1:25 – 30 beds
• Staff nurses 1:3 beds in teaching and 1:5 in non-teaching+ 30% leave reserve
• For OPD & emergency 1:100 patients + 30% Leave reserve
18

• For ICU 1:1 (or 1:3 for each shift) + 3)% LR
• For specialised departments 1:25 + 30% LRsuch as OT /LR
• Infection control nurse 1 for each 250 beds
• Medical Council of India for teaching hospital
• Nursing Superintendent (NS) 01
• Deputy Nursing Superintendent 01
• Asst. Nursing Superintendent 02 (Additional 1 for every 50 beds)
• For wards
• DNS/ANS 01
• nursing sister 1 per ward/shift
• Staff nurses 1:3 (for 24 hours)
19

• For specialised units (cardiology, neurology etc)
• DNS/ANS 01 for 3 to 4 units
• Sister 1 per shift
• Staff nurses 1:1 for 24 hours
• For OT
• DNS/ANS 1 for 4-5 operating rooms
• Sister 1 per shift
• Staff nurses 3 per table (24 hours). For .minor OT 1 for every 13 patients
20

• Casualty & Emergence
• NS.ANS 1 for each unit
• Sister 1 per shift
• Staff nurse 2-3 (depending on beds)
• Out Patient Department
• Surgical OPDs
• Staff nurse 1 for every 120 patients
• Medical
• Staff nurse 1 for every 140 patients
21
• Gynaecology
• Staff nurse 1 for every 35 patients
• Paediatrics
• Staff nurse 1 for every 85 patients
• Skin
• Staff nurse 1 for every 100 patients
• Injection room & Eye OPD
• Staff nurse 1 for every 85 patients
• Leave reserve 30% in all categories of nurses
22
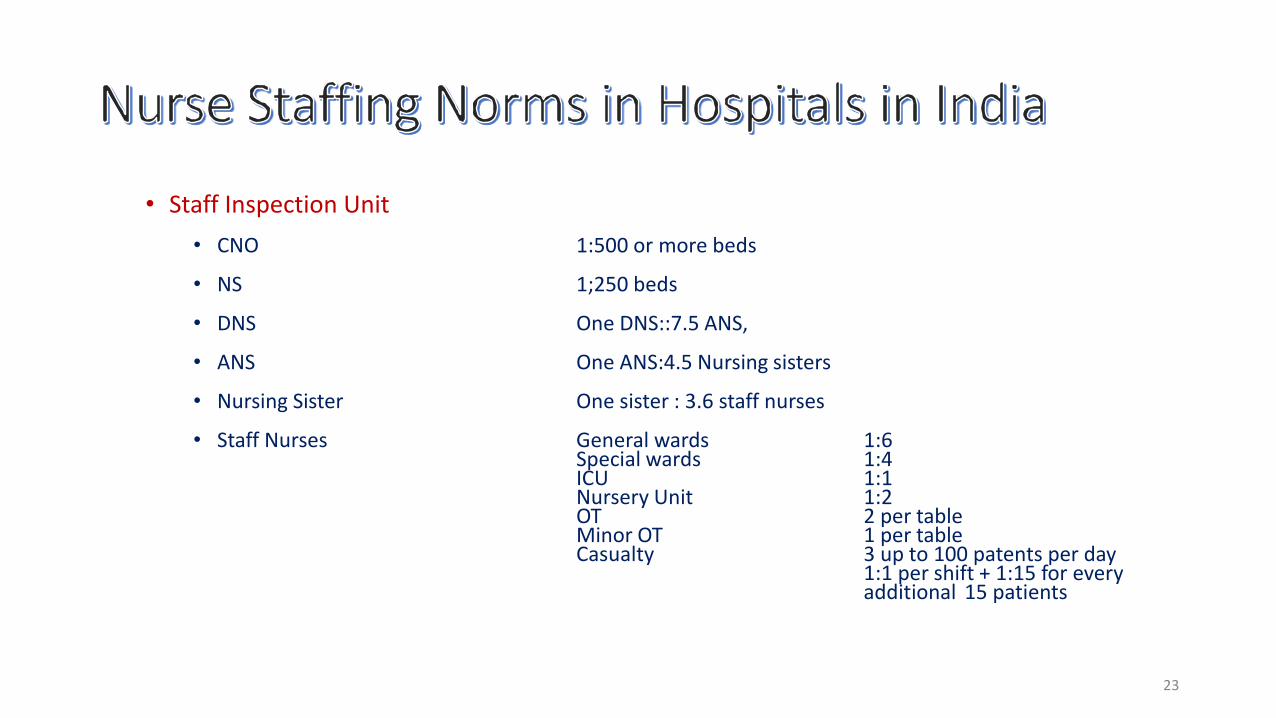
• Staff Inspection Unit
• CNO 1:500 or more beds
• NS 1;250 beds
• DNS One DNS::7.5 ANS,
• ANS One ANS:4.5 Nursing sisters
• Nursing Sister One sister : 3.6 staff nurses
• Staff Nurses General wards 1:6Special wards 1:4ICU 1:1Nursery Unit 1:2OT 2 per tableMinor OT 1 per tableCasualty 3 up to 100 patents per day
1:1 per shift + 1:15 for every additional 15 patients
23

•SNs (contd.) OBG (up to 40 patient/day) = 3
SNs1:1 per shift + 1:15 (for every additional patients
Burns (up to 15 pts per day) 3 SNs for 24 h; 1:1 per shift + 1:15 (for every additional 10 patients
Ortho (up to 45 Pts/day) 03 SNs/sisters for 24 hour;1;1 per shift + 1:15 (for every addl. 15 Pts
OPD 1:3 SNs, Injection 1:100 Pts, 2: 120-220 Pts3:221-320 Pts, 4:321-420 Pts45% additional as leave reserve
• ICU 1:1 (ventilator beds), 1:2 (non ventilated beds)each shift
HDU 1:3 each shift
24

• SNs (contd.) OTs 2 SNs per tableER 1:1 (ventilated), 1:4 (other beds)/shift)LR 01 nurse per table/shiftICN 01 for 100 bedsSuper Visor staff as applicable
• Indian standards are much lower than all international standards. In addition, there are other ancillary staff to help the staff nurses in these advanced countries
• The lower standard compromises on patient safety. Moreover, the nurse now somehow want to finish the tasks allotted to them.
• Thus patient’s emotional needs cannot be taken care of
25

• In-patient nursing unit (Ward) is the hub of activities where most services of the hospital converge
• Nurses are the linchpin of hospital care delivery
• The prime function of the inpatient unit is:• To provide appropriate accommodation for the delivery of
healthcare services to inpatients
• The unit also provide:
• facilities and conditions to meet the needs of patients and visitors as well as the workplace requirements of staff
27

• Inpatient Accommodation unit is for general medical and surgical patients
• In larger health facilities, this unit includes specialist medical and surgical patients
• For example this includes:
• cardiac,
• neurology,
• neurosurgery,
• obstetrics
• cardiothoracic surgery
28

• In-patient accommodation is provided in:• General Wards
• Intensive care wards patients
• Isolation wards/rooms
• Burn unit / Other special care areas
• Patients who are admitted are often quite sick needing close observation• This need for observation determines size and shape of the in-patient
accommodation
• Need for privacy, infection control, patient safety and nurse fatigue factor also determines type of accommodation provided
29

• External
–Principal relationships with other Units include:
• Easy access from the Main Entrance of a facility
• Access to one unit should not be through another
• Ready access to diagnostic facilities
• Ready access to Critical Care Units
• Surgical Units require ready access to OT
• Ready access to staff amenities
30

• Internal
–Optimum internal relationships include:
• Patient occupied areas as the core of the unit
• Staff Station need direct access and observation of patient areas
• Utility and Storage areas need ready access to patient and staff work areas
• Public areas should be on the outer edge of the unit
• Shared Areas should be easily accessible from the Units served
31
• Environmental Considerations–Acoustics
• Ambient noise level and transmission of sound between patient areas, staff areas and public areas should be minimum
• Acoustic treatment is required to the following:
– Patient bedrooms
– Interview and meeting rooms
– Consult rooms
– Staff rooms
– Toilet and showers
32
• Two types of wards pattern
• Nightingale
• The configuration is rectangular with the nursing station at the centre, curved out of the horizontal circulation
• Typically accommodates 24 – 32 beds arranged perpendicular lo the long wall
• Sanitary facility is at one end of the ward
33
• Riggs Pattern Ward
– It was first made in Rigg hospital in 1910 in Copenhagen
– Ward unit is divided into small compartments separated from each other
– Each compartment has 1,2,4 and 6 beds arranged parallel to the longitudinal wall
– In this pattern there is difficulty in communication between the nurse and the patient.
– It also reduces visibility and observation of the patient
– Wards become longer, consequently the nurse has to walk more
• Increased number of nurses required.
34
• Space standards and Components
–Room Capacity and Dimensions• Maximum capacity shall be four patients
• In USA, the recommendation is that all patients should be accommodated in single rooms
• Maximum dimensions, excluding such items as ensuites, built-in robes, alcoves, alcoves, entrance lobbies and floor mounted mechanical equipment shall be:
• Single Bed Room 120 SqFt
• Two bed room 220 SqFt
• Four bed room 420 SqFt
– In Nightingale pattern ward 100 SqFt/bed
35
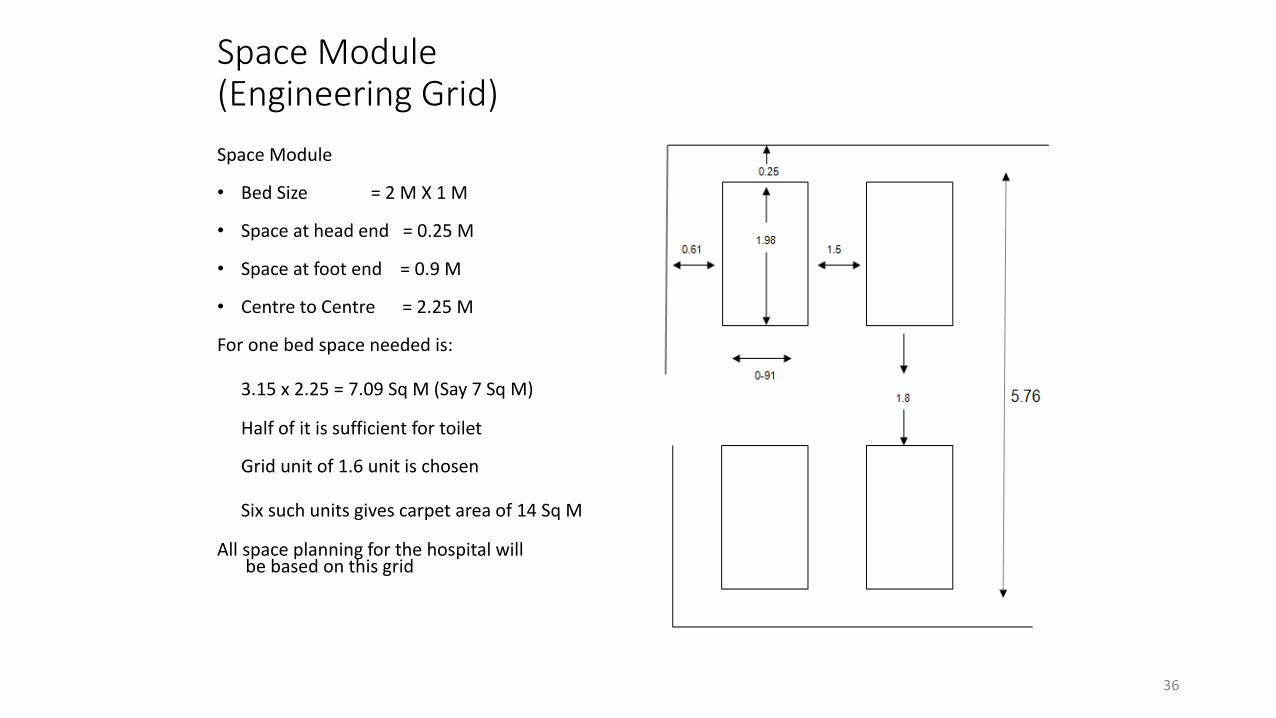
Space Module (Engineering Grid)
Space Module
• Bed Size = 2 M X 1 M
• Space at head end = 0.25 M
• Space at foot end = 0.9 M
• Centre to Centre = 2.25 M
For one bed space needed is:
3.15 x 2.25 = 7.09 Sq M (Say 7 Sq M)
Half of it is sufficient for toilet
Grid unit of 1.6 unit is chosen
Six such units gives carpet area of 14 Sq M
All space planning for the hospital willbe based on this grid
36
• Sufficient space in clinical areas, particularly for each bed space is a prime requirement in planning
• Ergonomics has shown that:
–Most activities carried out at bed side need a space with the dimensions 3600 mm (width) x 3700 mm (depth)
–This represents clear bed space
–Does not include space for fixed storage, preparation and worktops
37

– Natural Light
• Should be maximised
• Should be available in all bed rooms
– Observation and Privacy
• The design needs to consider the contradictory requirement of privacy and visibility
– Factors to be considered are:
» Use of windows in internal walls and/or doors
» Location of beds that may affect direct staff visibility
» Provision of bed screens
» Location of sanitary facilities to provide privacy for patients while not preventing observation by staff
38

An example of good observation into a single-bed room
39Department of Health UK HBN 04-01: Adult in-patient Facility
40