adjuvant-antigen requirements for active - cancer research
TRANSCRIPT

[CANCER RESEARCH 40, 4197-4203, November 1980]
Adjuvant-Antigen Requirements for Active Specific Immunotherapy of
Microscopic MétastasesRemaining after Surgery
Michael P. Ashley,1 Berton Zbar, James T. Hunter, Herbert J. Rapp, and Tohru Sugimoto
Laboratory of Immunobiology, National Cancer Institute, NIH. Bethesda, Maryland 20205
ABSTRACT
We studied the conditions required for eradication by immunization of occult lymph node métastaseswhich remainedafter surgical removal of an ¡ntradermally transplanted cavianhepatoma. Guinea pigs that received no postsurgical treatmentall died with progressively growing lymph node métastases.The growth of these métastases could be prevented in asignificant proportion of the animals by postsurgical treatmentwith vaccines containing oil-in-water emulsions of Mycobacte-rium bow's strain Bacillus Calmette-Guérin (BCG) cell walls
admixed with live or irradiated tumor cells. Vaccines containingliving tumor cells cured most of the guinea pigs but producedtumors at the vaccine sites in a few animals. Irradiated tumorcell vaccines were not tumorigenic but required more tumorcells for successful therapy. Therapy was dependent both onthe dose of tumor cells and on that of BCG cell walls. Microgramdoses of BCG cell walls were required for a therapeutic effect;milligram doses of BCG cell walls inhibited the therapeuticresponse. Animals rendered tumor free by postsurgical vaccinetherapy rejected an intradermal challenge with living tumorcells.
INTRODUCTION
Active specific immunotherapy is under investigation as amethod for eradication of occult métastases remaining aftersurgical removal of solid tumors. This form of cancer treatmenthas the potential of eradicating microscopic métastaseswithoutdamaging normal cells. Several animal models have been developed to analyze the factors required for successful activeimmunotherapy (4, 5, 8, 10, 11, 16). These animal modelsusually consist of transplantable syngeneic rodent tumors;animals are given injections of tumor cells and subsequentlyimmunized with tumor cells or tumor cell products. In a fewinstances, animals with autochthonous tumors have beentreated by surgical removal of primary tumors followed byimmunization with tumor cells or tumor cell extracts (21, 24).Factors identified as affecting the response to active specificimmunotherapy include residual tumor burden (4, 8, 10), tumorimmunogenicity (4), dose and form of tumor antigen (10, 11),dose and type of adjuvant (5, 11, 12, 27), and routes andschedules of immunization (8). Generalizations that haveemerged from a study of these animal models include: (a)vaccines containing adjuvants and tumor cells are generallymore effective in therapy than are vaccines containing eithercomponent alone (5, 10, 11); (b) treatment is antigenicallyspecific (5, 10, 11, 16); and (c) intact, metabolically activetumor cells are the best source of immunogen (14).
We previously reported that microscopic métastasesremaining after surgical removal of an i.d.2 implanted cavian hepatoma
could be eradicated by immunization with mycobacterial vaccines and tumor cells (27). In that report, it was establishedthat: (a) injection of adjuvant alone adjacent to the site of tumorexcision (regional injection) had a weak inhibitory effect ongrowth of lymph node métastases; (b) injection of adjuvantalone contralateral to the site of tumor excision (remote injection) had no inhibitory effect on growth of lymph node métastases; (c) remote or regional treatment with nonliving immuno-
stimulants admixed with tumor cells was effective treatmentagainst microscopic métastases;(d) BCG CW functioned effectively as adjuvant while living BCG was less effective; and (e)treatment was antigenically specific and devoid of gross systemic toxicity. In this report, we present information on theinfluence of dose and form of immunogen and dose of adjuvanton the success of therapy.
MATERIALS AND METHODS
Animals. Male Sewall-Wright strain 2 guinea pigs were obtained from the Laboratory Aids Branch, Division of ResearchServices, NIH, and from the Experimental Animal BreedingFacility of the National Cancer Institute, Frederick CancerResearch Center, Frederick, Md. They were caged in groupsof 6 and given water and NIH guinea pig ration ad libitum. Allanimals were used when 3 to 4 months old and weighed 500to 600 g.
Tumor Line. We used the L10 hepatocellular carcinomawhich was derived from a diethylnitrosamine-induced hepatoma in a male strain 2 guinea pig. The tumor has beenconverted to ascites form and is maintained by i.p. passage inmale weanling strain 2 guinea pigs. The in vivo passaged tumorline was restarted periodically with ascites cells stored in liquidnitrogen so that the cells used in experiments were in the 9thto the 18th i.p. passage generations. Suspensions containinggreater than 90% trypan blue-excluding cells were used in
experiments.Preparations of Oil-in-Water Emulsions Containing CW.
BCG CW (Lots 278 and 286) prepared as described previously(1 ) were obtained from Dr. Edgar Ribi (Rocky Mountain Laboratory, Hamilton, Mont.). The preparation of a mineral oil-in-water emulsion containing BCG CW in the oil phase has beendescribed (27). Briefly, light mineral oil (Drakeol 6-VR; Pen-reco, Butler, Pa.) was added to BCG CW and ground to asmooth paste in a tissue grinder. This paste was then emulsifiedin sterile NaCI solution (8.5 g/liter) containing Tween 80 (2 /il/ml) to produce a well-dispersed oil-in-water emulsion. Fordoses of CW up to and including 1.88 mg per ml, emulsions
1To whom requests for reprints should be addressed.
Received May 19, 1980; accepted July 31. 1980.
2 The abbreviations used are: i.d., intradermal(ly); BCG. Bacillus Calmette-
Guérinstrain of Mycobacterium bows; CW, cell walls; L10, tumor line 10; SDA.superficial distal axillary; EAE, experimental allergic encephalomyelitis.
NOVEMBER 1980 4197
Research. on January 2, 2019. © 1980 American Association for Cancercancerres.aacrjournals.org Downloaded from

M. P. Ashley et al.
contained 30 ¿iloil per ml; for doses of CW greater than 1.88mg per ml, emulsions contained 100 /¿Ioil per ml.
Composition of Mixtures Used for Treatment. Vaccinescontaining BCG CW plus L10 cells were prepared immediatelybefore use. A suspension of living or irradiated tumor cellsplaced in a 17 x 100 mm polypropylene tube 2059 (FalconPlastics, Oxnard, Calif.) was centrifuged at 140 x g; the volumeof the cell pellet was noted. Tumor cells were resuspended inBCG CW emulsion by dropwise addition of the emulsion to thetumor cell slurry; after each addition of emulsion, the slurrywas agitated with a Vortex mixer (Scientific Industries, Inc.,Springfield, Mass.). The injection volume for an individualguinea pig was the sum of the CW emulsion volume (0.4 ml)and the volume of a single dose of live or irradiated tumor cells.Vaccines were injected i.d. on the right thoracic flank with thetotal volume divided equally between 4 injection sites in avertical line down the flank.
Irradiation. L10 cells were irradiated with a dose of 20,000rads. The radiation was initially delivered with an X-ray sourcebut, in later experiments, a 137Csy-ray source was used. No
difference was observed in immunogenicity of cells irradiatedwith an X-ray source or with a 137Cs -y-ray source. For X-irradiation, L10 cells (30 ml, 30 x 106/ml) ¡nMedium 199
were placed in a 250-ml No. 3023 plastic tissue culture flask
(Falcon Plastics, Cockeysville, Md). The flask was irradiated ina horizontal position between 2 vertically opposed Philips RT250 therapeutic X-ray tubes. These were operated at 235 kV
and 15 ma with 0.25 mm copper and 0.55 mm aluminum filters(half-value layer, 0.9 mm aluminum). The source to target
distance was 25 cm, and the dose rate was 662 rads/min(30.2 min for 20,000 rads). For y-irradiation, L10 cells (50 ml,30 x 106/ml) were placed in a 50-ml No. 25335 polypropylene
centrifuge tube (Corning Glass Works, Corning, N. Y.). Duringy-irradiation, the test tube was rotated while in a vertical posi
tion in the center of the irradiation chamber of a Gammator M137Cs irradiator (Isomedix Inc., Parsippany, N. J.). The dose
rate was 1,790 rads/min (11.2 min for 20,000 rads). Afterirradiation, the cell concentration and viability of the cells weredetermined by the trypan blue exclusion test; no decrease inviability was observed after irradiation. To test whether irradiation had eliminated tumorigenicity, tumor cells (107) were in
jected i.p. into weanling strain 2 guinea pigs. No ascites tumorsformed after i.p. injection of L10 cells irradiated with 20,000rads. One viable L10 cell is capable of initiating ascites tumorgrowth in this test.3
Tumor Excision. Dermal tumors were excised with a 1-cmmargin of skin under pentobarbital anesthesia supplementedwith ether inhalation as previously described (28).
Animal Model for Evaluating the Effects of PostoperativeImmunotherapy. Tumor cells (106) were injected i.d. into each
guinea pig on Day 0. Seven days after i.d. injection, dermaltumors (9 to 10 mm in diameter) were excised. Immunotherapywas administered 2 days after surgery. Virtually all of theanimals treated by tumor excision alone developed progressively growing tumors in the regional lymph nodes. Thesemétastases developed first in the SDA lymph node whichbecame palpable after 20 to 30 days. Death occurred after 60to 90 days.
Measurements. Animals were examined at weekly intervals
after surgery to detect tumor growth. Since métastases appeared first in the left SDA lymph node, this lymph node waspalpated to estimate its size. For 20 to 30 days after L10injection, it was not possible to distinguish between lymph nodeenlargement due to tumor growth and lymphadenopathy resulting from immunostimulation. Axillary adenopathy detected30 days after immunostimulant treatment was a reliable indicator of tumor progression. Animals were observed for a minimum of 90 days; the usual observation period was 120 to 150days. Recurrence of tumors after Day 90 was rare. Significanceof differences between groups was determined with the Fisherexact test (1 tailed) and the x2 analysis.
RESULTS
Previously, we showed that a single treatment with a vaccineof live L10 cells and BCG CW could prevent the growth ofmicroscopic lymph node métastaseswhich remained after excision of dermal tumors (27). Vaccine therapy could preventthe growth of métastases in a high proportion of the treatedanimals whether administered adjacent to the site of excisionor on the contralateral flank. Adjuvant alone could protect asmall proportion of the animals but only if given as a regionaltreatment. To avoid these regional effects, vaccines were injected contralateral to the site of the primary tumor inoculationin the experiments in this study. In this way, we could investigate some of the conditions affecting vaccine therapy of distantoccult métastases.
Immunotherapy with Live Tumor Cell Vaccines
The previous study showed that postoperative immunother-
apy with a vaccine containing BCG CW (750 ¿tg)and living L10cells (6 x 106 cells) significantly reduced the incidence of
palpable lymph node métastases. Our experience with thisvaccine treatment over a series of 10 experiments includingthe 3 previously reported is summarized in Table 1. Vaccinetreatment was highly effective in preventing the growth ofmétastases. When vaccines contained 6 x 106 living tumor
cells, 60% of the treated animals were protected. The proportion of animals cured in individual experiments varied from 0 to89% but ¡nonly 2 of the experiments was it less than 50%(data not shown). In an attempt to improve the therapeuticefficacy of the vaccine, the dose of tumor cells was increased5-fold. Treatment with vaccines containing 30 x 106 living
tumor cells cured 74% of the treated animals and appeared to
Table 1
Summary of experiments with vaccines containing living tumor cellsAll animals received 106 L10 cells i.d. on Day 0 and had their dermal tumors
excised on Day 7. Vaccine treatment was given on Day 9. The dose of adjuvantwas 750 fig for all animals treated with 6 x 106 living tumor cells and for 54 of85 animals treated with 30 x 106 living tumor cells. Animals treated with 450 figBCG CW admixed with 30 x 106 living tumor cells had a response (24 of 31 ) that
was not significantly different from animals treated with 750 fig BCG CW admixedwith 30 x 106 living tumor cells (39 of 54). Consequently, the responses of
animals treated with 450 and 750 fig of CW have been pooled. Of 180 animalstreated with surgery alone, 179 died with progressive tumor growth.
' J. T. Hunter, unpublished data.
Dose of livingtumor cells
(X10~6)6
30No.
of animalsalive and tumor
free/totalp69/115 (60)"
63/85 (74) <0.05No.
of animalswith tumor
growth at vaccinesite/total5/115(4)
12/85 (14)P<0.02' Numbers in parentheses, percentage.
4198 CANCER RESEARCH VOL. 40
Research. on January 2, 2019. © 1980 American Association for Cancercancerres.aacrjournals.org Downloaded from

Immunotherapy of Lymph Node Métastases
give more consistent results than were obtained with the lowertumor cell dose. At least 50% of the animals were cured inevery experiment (data not shown). However, the improvementin therapeutic activity achieved by increasing the dose of livingtumor cells was counterbalanced by an increase in the tumor-
igenicity of the vaccine.
Occurrence of Tumor Growth at Vaccination Sites Containing Living Tumor Cells
The vaccine used in these experiments contained live tumorcells and so was potentially tumorigenic. Since the host's
reaction to BCG CW suppressed the growth of admixed tumorcells (29), tumor growth at the vaccine sites was rare. Instead,a vigorous inflammatory reaction developed at the vaccine sitewhich eventually healed. Tumor grew out from one or more ofthe vaccine sites and metastasized to the draining lymph nodein 4% of the animals treated with 6 x 106 live tumor cells
(Table 1). When the tumor cell dose was increased to 30 X106 cells, tumor grew at the vaccine sites in 14% of the animals.
Tumor growth occurred at the vaccine sites almost exclusivelyin animals in which therapy failed to prevent the growth of thelymph node métastases.A higher incidence of tumor growth atvaccine sites was observed in experiments in which vaccinetreatment was attempted in animals with more advanced tumorsor with disseminated BCG infection.4
Comparison of Vaccines Containing Live or Irradiated TumorCells
In order to eliminate the risks associated with live tumor cellvaccines, we tested vaccines containing L10 cells renderednontumorigenic by irradiation. To completely eliminate the tu-
morigenicity of the L10 cells, we irradiated tumor cells with adose of 20,000 rads (16). Vaccines containing irradiated tumorcells have been shown to be active against small deposits ofL10 cells in the skin or lungs (10, 16). Since irradiation mayreduce the immunogenicity of tumor cells (2, 6, 18, 25), wecarried out a series of experiments to compare the therapeuticefficacy of vaccines containing live or irradiated L10 cells.Vaccines containing living or irradiated tumor cells were compared under 3 conditions: (a) over a range of L10 doses; (£>)over a range of treatment times; and (c) in repeated experiments at a single dose level of tumor cells.
Chart 1, A and B, shows the results of 2 experiments comparing vaccines containing live or irradiated L10 cells over arange of tumor cell doses. The success of vaccine therapydiffered between the 2 experiments. Nevertheless, it was clearfrom both experiments that the efficacy of the vaccines increased with the dose of live or irradiated tumor cells. At eachtumor cell dose tested, the live L10 vaccine protected moreanimals than did the corresponding irradiated L10 vaccine.
Experiments were carried out to test the effect of varying thetime interval between i.d. tumor implantation and treatment(Chart 1C). Dermal L10 tumors were excised 4, 7, or 9 daysafter implantation. Vaccines containing live or irradiated L10cells (30 x 106) were injected 2 days after surgery. Lymph
node mestastases grew in all of the animals treated by surgeryalone, showing that tumor cells had reached the SDA lymph
100
0 03 1 3 10DOSE OF L10 CELLS (10-6 x
30DOSE!
UJccILXo
DI—
D
50
1 3 10 30DOSE OF L10 CELLS (10-6 x DOSE)
100
50
4 79DAY OF TUMOR EXCISION
Chart 1. Comparison of the ability of vaccines containing live or irradiatedtumor cells to eradicate métastasesremaining after surgery. Animals were treated2 days after surgery with CW (750 fig) plus live L10 cells (O) or CW plus irradiatedL10 cells (•).A, Surgery alone. The experiments were terminated on Days 133(A), 147 (B), and 159 (C). A, varying dose of tumor cells in the vaccine (firstexperiment); B, varying dose of tumor cells in the vaccine (second experiment);C, constant dose of tumor cells in the vaccine (30 x 106). Varying time between
tumor implantation and surgery.
node within the first 4 days of tumor growth. At each of thetimes tested, postsurgical vaccine therapy prevented thegrowth of métastasesin a significant proportion of the animalstreated. The success of vaccine therapy decreased slightly asthe time of treatment was delayed, although this trend was notstatistically significant5 with either of the vaccines. The only
significant difference attributable to treatment time was between the groups treated with live L10 vaccine following surgery on Day 4 and Day 7 (12 of 12 tumor-free versus 6 of 11,p < 0.05). No significant differences were observed in thisexperiment between vaccines containing live or irradiated tumor cells.
Table 2 summarizes our comparisons between vaccinescontaining live or irradiated cells (27 to 30 x 106 cells). Six
experiments with direct comparisons between the vaccines areshown, together with the results from another 7 experiments.The live vaccines cured 74% (63 of 85) of the animals in theseexperiments and cured at least 50% in each experiment. Thiscontrasted with the irradiated vaccines which cured the majority of the animals in only 6 of 12 experiments and cured 48%(76 of 158) overall. The superiority of the live cell vaccine wasstatistically significant over the series of experiments (p <0.001) and in 2 of the direct comparisons.
4 M. P. Ashley, J. T. Hunter, B. Zbar, and H. J. Rapp, unpublished data.
NOVEMBER 1980
1By the Cochran-Armitage x1 test for significance of observed trends (13).
4199
Research. on January 2, 2019. © 1980 American Association for Cancercancerres.aacrjournals.org Downloaded from

M. P. Ashley et al.
Table 2
Summary of comparisons of vaccines containing live or irradiated tumor cells
Vaccine treatment
None CW + liveLIO
Experiment123I3ii45678910111213TotalNo.
of animals aliveand tumor free/
total0/200/90/110/150/120/190/100/120/110/100/160/11NT0/156(0)No.of animals alive
and tumorfree/total9/10"NT9/1065/106NT6/11bNT6/11"NT9/12*NT14/15"NT5/663/85
(74)No.
of animals withtumors at vaccine
sites/total1/101/102/101/113/113/121/150/612/85(14)uw
+ irradiated LIuNo.
of animals aliveand tumorfree/total3/5"7/9"0/92/99/10"NT2/127/11"0/122/122/1212/15"28/36"2/6"76/158(48)p
(live vs. irradiated)NSC0.005NSNS0.006NSNS<0.001e
a Vaccines containing live or irradiated L10 cells (27 to 30 x 106)admixed with a mineral oil emulsion of BCG CW. The dose of CW was 750/jg in Experiments 3ii, 4, and 6 to 13 and 450 /ig in Experiments 1, 2, 3i, and 5. Vaccine treatment was given 2 days after excision of 7-daydermal L10 tumors.
" Significantly different from no vaccine (p < 0.05 by Fisher exact test).0 NS. not significant; NT, not tested.d Numbers in parentheses, percentage.8p < 0.001 whether comparing the totals from all 13 experiments (76 of 158 vs. 63 of 85), the totals from the 6 experiments in which both
live and irradiated vaccines were tested (29 of 67 versus 57 of 74) or the paired comparison in these 6 experiments by the method of Cochran(13).
Factors Affecting the Success of Vaccines Containing Irradiated Tumor Cells
Chart 2 summarizes 19 experiments undertaken to analyzesome of the factors influencing the success of vaccines containing irradiated tumor cells. This chart is in effect a 3-dimen-sional graph showing the degree of protection that resultedfrom immunization with different combinations of irradiatedtumor cells and BCG CW. Each of the 78 single-digit numbersin Chart 2 represents the proportion of tumor-free guinea pigsin an individual group of 9 to 12 guinea pigs. So that eachgroup can be represented by a single-digit number, the resultshave been expressed as 9 x (no. tumor-free/no, tested)rounded off to a whole number. For example, 0/12, 7/12, and12/12 are shown as 0, 5, and 9, respectively.
Certain conclusions can be drawn from the data, (a) BCGCW were a necessary component of vaccines used for eradication of métastases remaining after surgery. Vaccines containing irradiated tumor cells alone (6 to 100 x 106 cells) failed
to cure any guinea pigs, (b) A supraoptimal dose of BCG CWwas defined. Vaccines containing 3 mg of BCG CW wereineffective in postoperative immunotherapy. (c) BCG CW functioned effectively as adjuvants over a dose range of 47 to 750jug. (d) A minimum dose of about 30 x 106 irradiated tumor
cells was required in the presence of adjuvant to lead todestruction of lymph node métastases. The percentage ofanimals that were cured when treated with 30 x 106 irradiated
tumor cells varied from 0 to 100% with an average of 48%.Guinea pigs treated with 1 to 1.2 x 10s irradiated tumor cells
were cured in 55 to 88% of cases. A plateau in the irradiatedtumor cell dose-response curve was not found in individual
experiments (Chart 3) but, from interpolation, appeared to bein the region of 108 irradiated tumor cells, (e) No supraoptimal
dose of irradiated tumor cells was found.
108
COoQ
<O<
10? -
106-
9 = 100% TUMOR FREE
0 = 0% TUMOR FREE
337??aoo
30 100 300 1000 3000
BCG CW (Mg)
Chart 2. Influence of dose of BCG CW and of irradiated tumor cells onoutcome of active specific immunotherapy. The results are a summary of 19experiments (843 animals). Each of the 78 single-digit numbers represents theproportion of tumor-free animals in an individual group of 9 to 12 guinea pigs.Each result is expressed as 9 x (no. tumor-free/no, tested) rounded off to awhole number. Numbers with an underline indicate treatment with vaccinescontaining 10% (v/v) oil emulsion. All other vaccines contained 3% (v/v) oilemulsion.
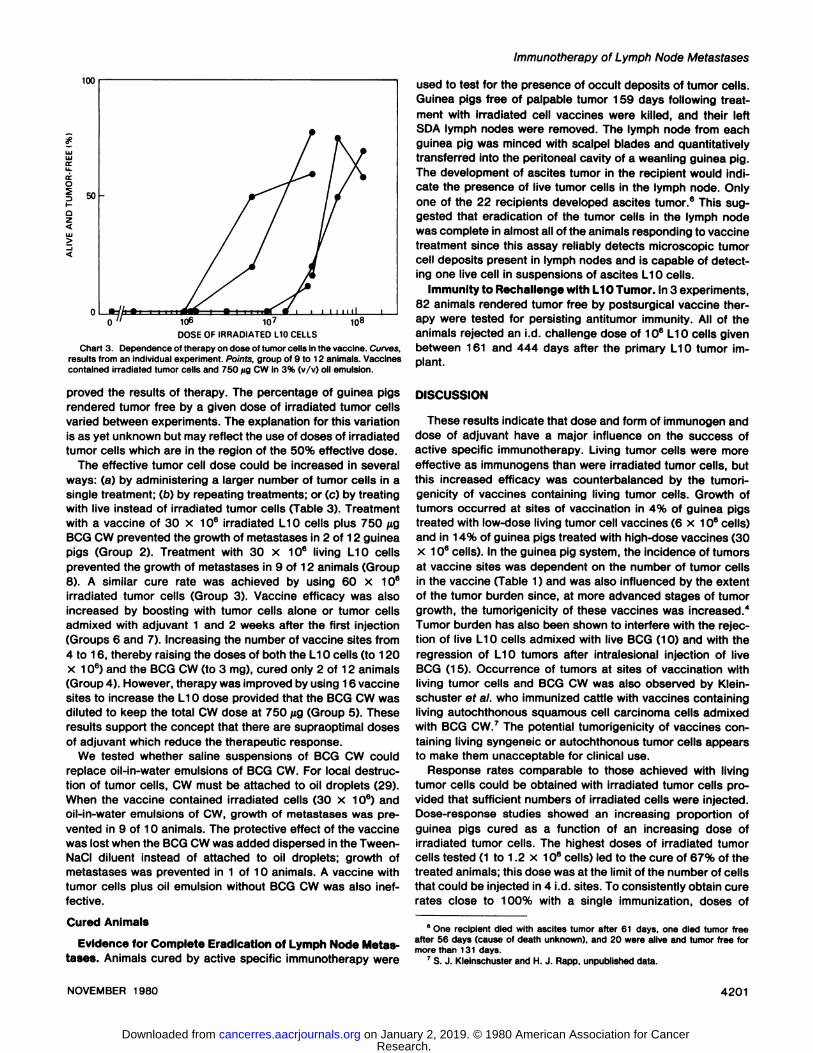
Five individual experiments illustrating the effects of increasing the dose of irradiated tumor cells are presented in Chart 3.Increasing the dose of irradiated tumor cells consistently im-
4200 CANCER RESEARCH VOL. 40
Research. on January 2, 2019. © 1980 American Association for Cancercancerres.aacrjournals.org Downloaded from
Immunotherapy of Lymph Node Métastases
106 io?DOSE OF IRRADIATED L10 CELLS
108
Chart 3. Dependence of therapy on dose of tumor cells in the vaccine. Curves,results from an individual experiment. Points, group of 9 to 12 animals. Vaccinescontained irradiated tumor cells and 750 jig CW in 3% (v/v) oil emulsion.
proved the results of therapy. The percentage of guinea pigsrendered tumor free by a given dose of irradiated tumor cellsvaried between experiments. The explanation for this variationis as yet unknown but may reflect the use of doses of irradiatedtumor cells which are in the region of the 50% effective dose.
The effective tumor cell dose could be increased in severalways: (a) by administering a larger number of tumor cells in asingle treatment; (b) by repeating treatments; or (c) by treatingwith live instead of irradiated tumor cells (Table 3). Treatmentwith a vaccine of 30 x 106 irradiated L10 cells plus 750 /¿g
BCG CW prevented the growth of métastasesin 2 of 12 guineapigs (Group 2). Treatment with 30 x 106 living L10 cells
prevented the growth of métastasesin 9 of 12 animals (Group8). A similar cure rate was achieved by using 60 x 106
irradiated tumor cells (Group 3). Vaccine efficacy was alsoincreased by boosting with tumor cells alone or tumor cellsadmixed with adjuvant 1 and 2 weeks after the first injection(Groups 6 and 7). Increasing the number of vaccine sites from4 to 16, thereby raising the doses of both the L10 cells (to 120x 106) and the BCG CW (to 3 mg), cured only 2 of 12 animals
(Group 4). However, therapy was improved by using 16 vaccinesites to increase the L10 dose provided that the BCG CW wasdiluted to keep the total CW dose at 750 ¿ig(Group 5). Theseresults support the concept that there are supraoptimal dosesof adjuvant which reduce the therapeutic response.
We tested whether saline suspensions of BCG CW couldreplace oil-in-water emulsions of BCG CW. For local destruc
tion of tumor cells, CW must be attached to oil droplets (29).When the vaccine contained irradiated cells (30 x 106) andoil-in-water emulsions of CW, growth of métastaseswas pre
vented in 9 of 10 animals. The protective effect of the vaccinewas lost when the BCG CW was added dispersed in the Tween-NaCI diluent instead of attached to oil droplets; growth ofmétastaseswas prevented in 1 of 10 animals. A vaccine withtumor cells plus oil emulsion without BCG CW was also ineffective.
Cured Animals
Evidence for Complete Eradication of Lymph Node Métastases. Animals cured by active specific immunotherapy were
used to test for the presence of occult deposits of tumor cells.Guinea pigs free of palpable tumor 159 days following treatment with irradiated cell vaccines were killed, and their leftSDA lymph nodes were removed. The lymph node from eachguinea pig was minced with scalpel blades and quantitativelytransferred into the peritoneal cavity of a weanling guinea pig.The development of ascites tumor in the recipient would indicate the presence of live tumor cells in the lymph node. Onlyone of the 22 recipients developed ascites tumor.6 This sug
gested that eradication of the tumor cells in the lymph nodewas complete in almost all of the animals responding to vaccinetreatment since this assay reliably detects microscopic tumorcell deposits present in lymph nodes and is capable of detecting one live cell in suspensions of ascites L10 cells.
Immunity to Rechallenge with L10 Tumor. In 3 experiments,82 animals rendered tumor free by postsurgical vaccine therapy were tested for persisting antitumor immunity. All of theanimals rejected an i.d. challenge dose of 106 L10 cells given
between 161 and 444 days after the primary L10 tumor implant.
DISCUSSION
These results indicate that dose and form of immunogen anddose of adjuvant have a major influence on the success ofactive specific immunotherapy. Living tumor cells were moreeffective as immunogens than were irradiated tumor cells, butthis increased efficacy was counterbalanced by the tumori-genicity of vaccines containing living tumor cells. Growth oftumors occurred at sites of vaccination in 4% of guinea pigstreated with low-dose living tumor cell vaccines (6 x 106 cells)
and in 14% of guinea pigs treated with high-dose vaccines (30x 106 cells). In the guinea pig system, the incidence of tumors
at vaccine sites was dependent on the number of tumor cellsin the vaccine (Table 1) and was also influenced by the extentof the tumor burden since, at more advanced stages of tumorgrowth, the tumorigenicity of these vaccines was increased.4
Tumor burden has also been shown to interfere with the rejection of live L10 cells admixed with live BCG (10) and with theregression of L10 tumors after intralesional injection of liveBCG (15). Occurrence of tumors at sites of vaccination withliving tumor cells and BCG CW was also observed by Klein-schuster ef al. who immunized cattle with vaccines containingliving autochthonous squamous cell carcinoma cells admixedwith BCG CW.7 The potential tumorigenicity of vaccines con
taining living syngeneic or autochthonous tumor cells appearsto make them unacceptable for clinical use.
Response rates comparable to those achieved with livingtumor cells could be obtained with irradiated tumor cells provided that sufficient numbers of irradiated cells were injected.Dose-response studies showed an increasing proportion of
guinea pigs cured as a function of an increasing dose ofirradiated tumor cells. The highest doses of irradiated tumorcells tested (1 to 1.2 x 108 cells) led to the cure of 67% of the
treated animals; this dose was at the limit of the number of cellsthat could be injected in 4 i.d. sites. To consistently obtain curerates close to 100% with a single immunization, doses of
6 One recipient died with ascites tumor after 61 days, one died tumor free
after 56 days (cause of death unknown), and 20 were alive and tumor free formore than 131 days.
7 S. J. Kleinschuster and H. J. Rapp, unpublished data.
NOVEMBER 1980 4201
Research. on January 2, 2019. © 1980 American Association for Cancercancerres.aacrjournals.org Downloaded from

M. P. Ashley et al.
Table 3Increasing efficacy of vaccine therapy by different methods of raising the tumor cell dosage
All animals received 106 L10 cells i.d. (Day 0) and had their dermal tumors excised (Day 7). Experiment terminated on Day 181.
Vaccine(Day9)No
vaccineCW
+ irradiated L1ObCW
+ live L10Sites
injected/ Boosted withGroup vaccination8 (Days 16 and23)1234567B4416164
CW + irradiated L104Irradiated L10only4L10
cellsOd"6 xdose)306012012030
(3times)30(3times)30BCGCW0*g>7507503000750750
(3times)750750No.
of animals tumorfree/total0/112/129/12°2/127/1
2C11/12°8/1
2C9/12c'd
'' All vaccine injections were i.d. on the right (contralateral) thoracic flank." Cells irradiated with 20,000 rads -^irradiation.c Significantly different (p < 0.05) to no vaccine controls and to Group 2.tf Tumor growth occurred at vaccine sites in 3 of 12 animals.
irradiated tumor cells greater than 108 may be required. Alter
natively, a series of booster immunizations with lower doses ofirradiated tumor cells may improve therapeutic results (Table3). No supraoptimal dose of irradiated tumor cells was detectedin dose-response studies. This observation is similar to observations of the induction of EAE in inbred guinea pigs in whichno supraoptimal dose of spinal cord or brain tissue was found(22).
Active specific immunotherapy required larger numbers oftumor cells than did immunoprophylaxis. Vaccines containing1.5 x 106 living tumor cells or less were sufficient to enable tothe host to reject a subsequent i.d. challenge with 106 livingtumor cells (26); vaccines containing a minimum of 6 x 106
living tumor cells were required to eradicate occult métastasesremaining after surgery. One concept suggested by theseresults is that the rate of formation of effector cells as well asthe number of effector cells formed are critical factors in thesuccess of active specific immunotherapy. A primary functionof the large doses of tumor cells used in vaccines for immunotherapy may be to accelerate the formation of large numbersof specifically sensitized cells. Studies of the rate of formationand properties of these cells are in progress.
A supraoptimal dose for CW was detected; /ig doses of CWwere effective immunostimulants, but mg doses of CW inhibitedthe ability of optimal doses of irradiated tumor cells to immunizethe host. This effect was similar to the dose response formycobacteria in the induction of EAE in guinea pigs (22). Thesimilarity in dose requirements for adjuvant in the induction ofEAE and in successful active specific immunotherapy raisesthe possibility that the optimal dose range for an immu-nostimulant may be a constant for the guinea pig and perhapsfor other species as well. Doses of living BCG (7, 9, 12) andkilled Corynebacterium parvum (5, 11, 25) have been foundthat inhibited the ability of tumor cells to immunize the host.
The mechanism for the inhibition by CW of the immunizingcapacity of optimal doses of irradiated tumor cells is unknown.It is possible that the intense granulomatous reaction inducedby high doses of adjuvant resulted in rapid destruction of tumorcells, thereby reducing the antigen dose (23), or resulted infunctional disruption of the draining lymph nodes. Meltzer andLeonard (17) demonstrated that mg doses of mycobacteria inmineral oil impaired the ability of guinea pigs to reject tumorline 10 at the site of BCG infection and inhibited the spontaneous regression of tumor line 1. Since animals pretreated with
mycobacteria in mineral oil functioned effectively as recipientsof transfusions of effector cells, these authors concluded thatthe block in the Freund's complete adjuvant-treated animals
was at the level of formation of effector cells. This block mightbe mediated by suppressor T-cells. Reinisch ef al. (19) foundthat i.p. injection of C57BL/6 mice with Freund's complete
adjuvant induced suppressor T-cells which inhibited in vitroresponses to allogeneic tumor cells. Schrier ef al. (20) foundthat i.v. injection of C57BL/6 mice with killed BCG on oildroplets led to the formation of macrophages that inhibitedgeneration of delayed hypersensitivity to sheep erythrocytes.
Several animal models have been developed to study activespecific immunotherapy. Tumor cell vaccines have been shownto eradicate tumor cell deposits established by prior s.c. or i.v.injection of tumor cells (11,16). There have been few studieson the use of tumor-specific vaccines in therapy of métastasesfrom primary tumor grafts. Bartlett and Kreider (5) treated micewith the LSTRA lymphoma with irradiated tumor cells plus C.parvum. It was not established in that study that the tumor haddisseminated from the site of inoculation by the time of treatment. Baldwin and Pimm (3) found that immunization withirradiated tumor cells and BCG did not eradicate lung métastases which remained after surgical removal of a transplantedrat epithelioma. The present report differs from those discussedabove since it describes successful postoperative therapy ofmétastasesarising from a primary tumor graft by remote treatment with a tumor cell-containing vaccine. This model shouldpermit analysis of the components of mycobacteria that arerequired as adjuvants in postoperative immunotherapy andshould facilitate studies on the cellular basis of active specificimmunotherapy.
ACKNOWLEDGMENTS
We thank Kevin Rice for typing the manuscript.
REFERENCES
1. Azuma, I., Ribi, E., Meyer, T. J., and Zbar, B. Biologically active componentsfrom mycobacterial cell walls. I. Isolation and composition of cell wallskeleton and component P3. J. Nati. Cancer Inst., 52: 95-100, 1974.
2. Baldwin, R. W., and Pimm, M. V. BCG immunotherapy of a rat sarcoma. Br.J. Cancer, 28. 281-287, 1973.
3. Baldwin. R. W., and Pimm, M. V. BCG immunotherapy of local subcutaneousgrowths and post-surgical pulmonary métastasesof a transplanted ratepithelioma of spontaneous origin. Int. J. Cancer, 12: 420-427, 1973.
4. Baldwin, R. W., and Pimm, M. V. BCG in tumor immunotherapy. Adv. Cancer
4202 CANCER RESEARCH VOL. 40
Research. on January 2, 2019. © 1980 American Association for Cancercancerres.aacrjournals.org Downloaded from

Immunotherapy of Lymph Node Métastases
Res.. 28:91-147, 1978.5. Bartlett, G. L., and Kreider, J. W. Active specific immune-therapy of murine
leukemia. II. Adjuvant effect of Corynebacterium parvum. Int. J. Cancer, 24.636-643. 1979.
6. Bartlett, G. L., Kreider, J. W., and Purnell, 0. M. Development of a vaccinefor immunotherapy of murine leukemia. Fed. Proc., 35: 225, 1976.
7. Bartlett, G. L., Kreider, J. W., and Purnell, D. M. Potentiation of immunity tomurine leukemia (LSTRA) by Bacillus Calmette-Guérin. Cancer Res., 38.4401 -4408, 1978.
8. Bartlett, G. L., Kreider, J. W., and Purnell, D. M. Active specific immunotherapy of murine leukemia. I. Irradiated tumor cell vaccine. Int. J. Cancer,24: 629-635, 1979.
9. Bartlett, G. L., Purnell, D. M.. and Kreider, J. W. BCG inhibition of murineleukemia: local suppression and systemic tumor immunity require differentdoses. Science (Wash. D. C.), Õ9Õ.299-301, 1976.
10. Bartlett, G. L., and Zbar, B. Tumor-specific vaccine containing Mycobacte-rium bow's and tumor cells: safety and efficacy. J. Nati. Cancer Inst., 48:
1709-1726, 1972.11. Bomford, R. Active specific immunotherapy of mouse methylcholanthrene
induced tumours with Corynebacterium parvum and irradiated tumour cells.Br. J. Cancer, 32: 551-557, 1975.
12. Davies, M., and Sabbadini. E. Dose-dependent adjuvant effects of BacillusCalmette-Guérin on tumor immunity in Lewis rats. Cancer Res., 39: 959-965, 1979.
13. Fleiss, J. L. Statistical Methods for Rates and Proportions, pp. 98-99, 112-115. New York: John Wiley & Sons, Inc., 1973.
14. Hanna, M. G., Jr. Active specific immunotherapy of residual micrometastasis:mechanisms of action of BCG-tumor cell vaccines in the generation of
systemic tumor immunity. Proc. Am. Assoc. Cancer Res., 27: 240, 1980.15. Hanna, M. G., Jr., and Peters, L. C. Efficacy of intralesional BCG therapy in
guinea pigs with disseminated tumor. Cancer (Phila.), 36: 1298-1304,1975.
16. Hanna, M. G., Jr., and Peters, L. C. Specific immunotherapy of establishedvisceral micrometastases by BCG-tumor cell vaccine alone or as an adjunctto surgery. Cancer (Phila.), 42: 2613-2625, 1978.
17. Meltzer, M. S., and Leonard, E. J. Enhanced tumor growth in animalspretreated with complete Freund's adjuvant. J. Nati. Cancer Inst., 50: 209-
218, 1973.18. Prager, M. D., and Baechtel, F. S. Methods for modification of cancer cells
to enhance their antigenicity. Methods Cancer Res., 9. 339-400, 1973.19. Reinisch, C. L., Gleiner, N. A., and Schlossman, S. F. Adjuvant regulation of
T cell function. J. Immunol., 776: 710-715, 1976.20. Schrier, D. J., Sternick, J. L., Allen, E. M.. and Moore. V. L. Control of BCG-
induced macrophage-mediated suppression of delayed hypersensitivity bygenes within the lg-1 complex. Fed. Proc., 39: 938, 1980.
21. Sedlacek, H. H., Weise, M., Lemmer, A., and Seiler, F. R. Immunotherapy ofspontaneous mammary tumors in mongrel dogs with autologous tumor cellsand neuraminidase. Cancer Immunol. Immunother., 6 47-58, 1979.
22. Shaw, C. M., Alvord, E. C., Fahlberg, W. J., and Kies, M. W. Adjuvant-antigen relationships in the production of experimental "allergic" encepha-
lomyelitis in the guinea pig. J. Exp. Med.. 775: 169-179, 1962.
23. Titus, M. J., Bartlett, G. L., and Kreider, J. W. Local effects in the preventionof tumor cell immunization by supraoptimal doses of admixed Corynebacterium parvum. Proc. Am. Assoc. Cancer Res., 27: 217, 1980.
24. Weiden, P. L., Storb, R., Tsoi, M.-S., Deeg, H. J., and Graham, T. C. Canineosteosarcoma: results of amputation with or without adjuvant immunotherapy. Cancer Immunol. Immunother., 5: 181-186, 1978.
25. Woodruff, M. F. A., Ghaffar, A., Dunbar, N., and Whitehead, V. L. Effect ofC. parvum on immunization with irradiated tumour cells. Br. J. Cancer, 33.491-495. 1976.
26. Zbar, B., Bernstein, I. D., and Rapp, H. J. Suppression of tumor growth atthe site of infection with living Bacillus Calmette-Guérin. J. Nati. CancerInst., 46.; 831-839, 1971.
27. Zbar, B., Canti, G., Ashley, M. P., Rapp, H. J., Hunter, J. T., and Ribi, E.Eradication by immunization with mycobacterial vaccines and tumor cells ofmicroscopic métastasesremaining after surgery. Cancer Res., 39. 1597-
1603, 1979.28. Zbar, B., Hunter, J. T., Rapp, H. J., and Canti, G. F. Immunotherapy of
bilateral lymph node métastases in guinea pigs by intralesional or parale-sional injection of Mycobactenum bovis (BCG). J. Nati. Cancer Inst., 60:1163-1168, 1978.
29. Zbar, B., Rapp, H. J., and Ribi, E. Tumor suppression by cell walls ofMycobacterium bovis attached to oil droplets. J. Nati. Cancer Inst., 48. 831 -
835, 1972.
NOVEMBER 1980 4203
Research. on January 2, 2019. © 1980 American Association for Cancercancerres.aacrjournals.org Downloaded from

1980;40:4197-4203. Cancer Res Michael P. Ashley, Berton Zbar, James T. Hunter, et al. SurgeryImmunotherapy of Microscopic Metastases Remaining after Adjuvant-Antigen Requirements for Active Specific
Updated version
http://cancerres.aacrjournals.org/content/40/11/4197
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/40/11/4197To request permission to re-use all or part of this article, use this link
Research. on January 2, 2019. © 1980 American Association for Cancercancerres.aacrjournals.org Downloaded from