addressing the unique behavioral health needs of children and families in the child welfare system...
TRANSCRIPT
Addressing the Unique Behavioral Health Needs of Children and Families
in the Child Welfare System
Institute #24
Caraleen Fawcett, Jan McCarthy,Frank Rider, Steve Sparks and Robin Trush
2006 Training InstitutesJuly 2006
Addressing the Unique Behavioral Health Needs of Children and Families in the Child Welfare
System – A National Perspective
Jan McCarthy
National TA Center for Children’s Mental Health
Georgetown University Center for Child and Human Development

Who are the children and families?
Reports of Child Abuse and Neglect
Total reports FY 03 2,900,000
2/3 were investigated 1,914,000
1/3 were confirmed 906,000
10% resulted in child placement 297,000
In placement more than 2 years 40%
Source:AFCARS Report 4/2/05, US DHHS, ACF, ACYF, CB http://www.acf.hhs.gov/programs/cb/stats_research/afcars/tar/report10.htm
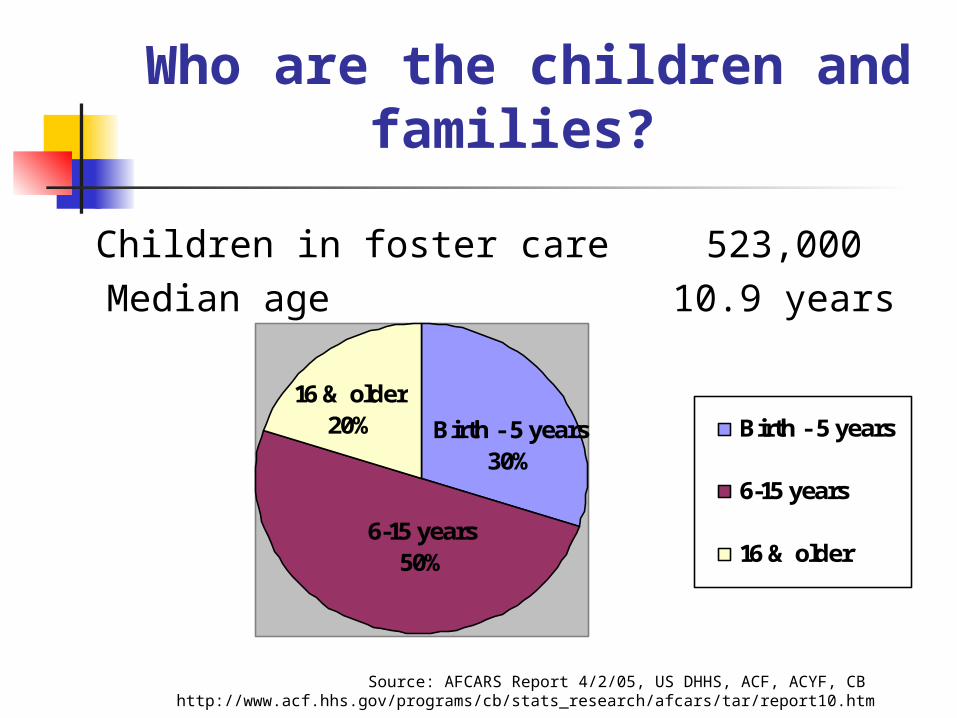
Who are the children and families?
Children in foster care 523,000 Median age 10.9 years
16 & older20%
6-15 years50%
Birth - 5 years30%
Birth - 5 years
6-15 years
16 & older
Source: AFCARS Report 4/2/05, US DHHS, ACF, ACYF, CB http://www.acf.hhs.gov/programs/cb/stats_research/afcars/tar/report10.htm
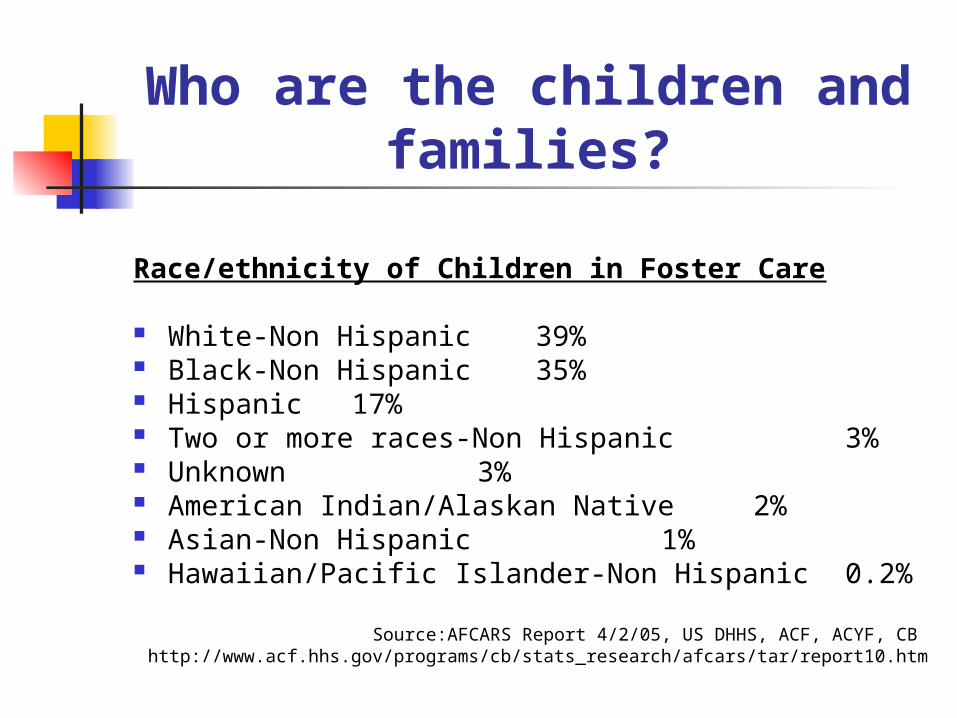
Who are the children and families?
Race/ethnicity of Children in Foster Care
White-Non Hispanic 39% Black-Non Hispanic 35% Hispanic 17% Two or more races-Non Hispanic 3% Unknown 3% American Indian/Alaskan Native 2% Asian-Non Hispanic 1% Hawaiian/Pacific Islander-Non Hispanic 0.2%
Source:AFCARS Report 4/2/05, US DHHS, ACF, ACYF, CB http://www.acf.hhs.gov/programs/cb/stats_research/afcars/tar/report10.htm
Representation of 5 Racial/
Ethnic Groups in Foster Care
Over-represented African American 2.43 Native American 2.16
Under-represented Latinos .79 Non-Latino Whites .76 Asian/Pacific Islanders .39
Source: 11/04 working paper by Robert B. Hill published in Race Matters Consortium, “Over-representation of Child of Color in Foster Care in 2000”
Living Arrangements of Children in Foster Care
Foster Family Home (non-relative) 46%
Foster Family Home (relative) 23%
Group Care (Institution/GH) 19%
Pre-Adoptive Home 5%
Trial Home Visit 4%
Runaway 2%
Supervised Independent Living 1%Source: AFCARS Report, FY 2003

Why Focus on Mental Health Issues?
Prevalent Need for Services children’s vulnerability and risk high prevalence of physical, behavioral,
developmental needs prior life experiences trauma of separation and placement experiences within foster care system parental service needs (MH, SA, DV +) relinquishing custody for treatment services difficulty in accessing services
National Data – MH Needs
National Survey of Child and Adolescent Well-Being (NSCAW)
Number of children studied 3,803 Ages 2 – 14 All involved with child welfare system:
Living in own homes 90% Living in foster, group,
or residential care 10%
SOURCE: Burns, B. et al. 2004 Mental health need and access to MH services by youths
involved with child welfare: A national survey. Journal of the American Academy of Child and Adolescent Psychiatry 43:8: 960-970.

National Data – MH Needs
47.9% of children/youth had significant emotional/
behavior problems (Need was defined by a clinical range score on the Child
Behavior Checklist)
Only 25% of children/youth with significant emotional/behavior problems received specialty mental health care in previous 12 months
SOURCE: Burns, B. et al. 2004 Mental health need and access to MH services by youths involved with child welfare: A national survey. Journal of the American Academy of
Child and Adolescent Psychiatry 43:8: 960-970.

National Data – MH Needs
NSCAW provides documentation of the magnitude of the problem:
• Large gap between service need and service use
• Failure of human service sectors to obtain mental health services needed by group of very high risk children and youth
National Data Demonstrates Need for Whole Family Approach
Children with a clinically significant externalizing score on the CBCL were more than twice as likely to have a caregiver with an alcohol, drug, or mental health problem.
Whole family approach to treatment can: address both child and caregiver needs
support interaction between the two
prevent children from being separated from their parents, e.g., drug and alcohol treatment facilities for the whole family.
Source: Anne M. Libby, University of Colorado, NSCAW data

National Data Shows Benefits
of Collaboration
Analysis of linkages between child serving systems in 92 sites:
Showed that increased coordination between MH and CW is associated with: greater use of services by children with
highest level of need decreased racial/ethnic disparities in receipt
of MH care
Source: Michael S. Hurlburt, CASRC, San Diego, NSCAW Data
Child and Family Services ReviewsCFSRs - Another Source of National Data
The CFSR Process and Mental Health: Focuses on well-being (PH, MH,
Education) Identifies need for MH reform Provides opportunity for reform Encourages participation of other
systems, c/b agencies, families
CFSR Findings2001-2004 Reviews (n = 52 States and
Territories)
PH and MH Needs Met (WB Outcome 3)• In substantial conformity 1 state• NOT in substantial conformity 51
states
MH Needs of the Child Met (Item 23)• Strength 4 states• Area Needing Improvement 48 states

CFSR FindingsAmong the primary reasons for case
openings(2001-04 - N = 2,416 children)
Child’s behavior (11% of all children; 41% of children age 13 +)
Parent’s behavior (including neglect, excluding child abuse)
Family’s mental and physical well being
CFSR Findings 2002-04 Content Analysis of Systemic Factors (N=35 states)
Service Array (for children placed in home and out-of-home) MH assessment and treatment services
are not sufficient to meet children’s needs 31 states Key services for parents lacking (including
substance abuse services) 30 states Lack of culturally appropriate services 18 states
CFSR FindingsStates are working on solutions to the
problems (N = 28 States): Program Improvement Plans (PIPs)
provide opportunity to correct problems identified in Final Reports
2/3 of PIPs identify strategies to improve assessment of MH needs and to expand service array and service capacity
All 28 PIPs mentioned MH issues and most (25) set goals and action steps to address them

CFSR Findings 2/3 of PIPs showed collaboration
across systems to address cross-system problems
1/3 of the PIPs proposed a comprehensive strategy for improving MH services
CFSR Findings Cultural competence – addressed in
very few Final Reports and PIPs in relation to MH and SA services – requires further study
Evidence based practices – very little data about concerted efforts to use evidence based MH practices

Some Trends in Child Welfare
Moving toward family-centered practice Use of child and family teams (including
multiple families in child’s life) Growth of kinship care Privatization Collaboration with other child-serving
systems – especially mental health; child welfare no longer seen as solely responsible
Addressing the Unique Behavioral Health Needs of
Children and Families in Arizona’s Child Welfare
System
Caraleen Fawcett, Pima County Community Network Team
Frank Rider, AZ Division of Behavioral Health Services
Steve Sparks, AZ Division for Children, Youth & Families
Robin Trush, System of Care Veteran, Maricopa County
…and who are you?

One Family’s Experience
Caraleen and Aliyah’s Story

Caraleen’s Themes
Pathologizing People We Serve, vs. Strength-Based, Needs-Driven
Overwhelming Families, vs. “One Family, One Team, One Plan”
Caraleen’s Themes
Parent Professional Partnerships – Equality and Respect
Hopelessness vs. Inspiring Hope
What Went “Right?” Only one caseworker Parent highly/self-motivated, resourceful
Pro-bono attorney friend - who happens to serves on the board of treatment center
Parent aide
Ponder this: How many families like Caraleen’s have experienced
comparatively poor outcomes, for their lack of any such fortunate factors?
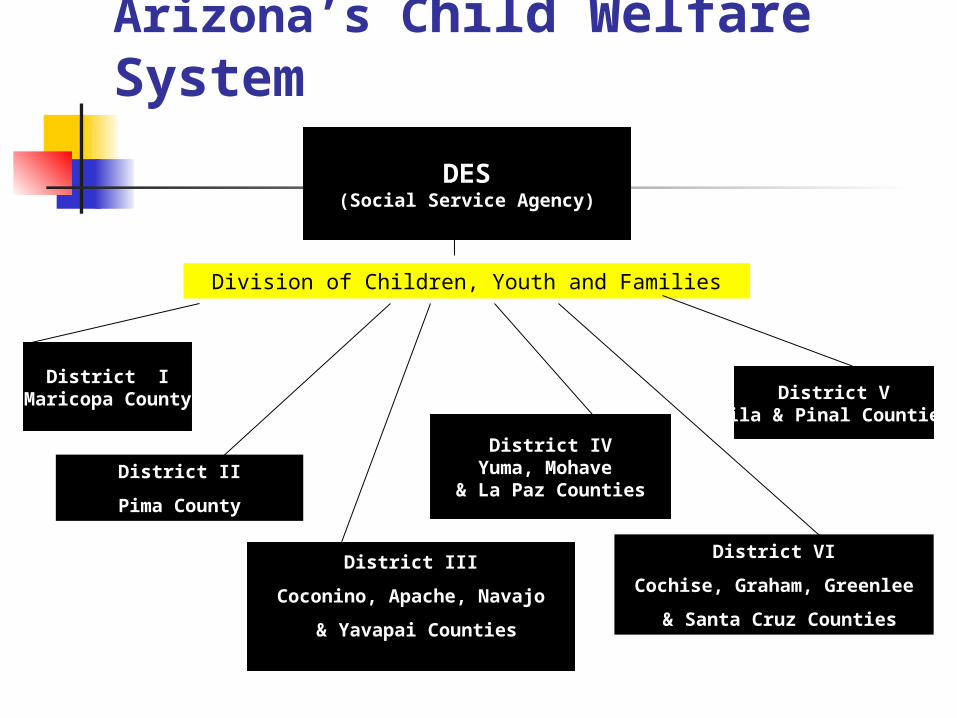
Arizona’s Child Welfare System
DES(Social Service Agency)
Division of Children, Youth and Families
District IMaricopa County
District II
Pima County
District III
Coconino, Apache, Navajo
& Yavapai Counties
District IVYuma, Mohave
& La Paz Counties
District VI
Cochise, Graham, Greenlee
& Santa Cruz Counties
District VGila & Pinal Counties

Arizona’s Child Welfare System
FEDERAL GOVERNMENT HEALTH AND HUMAN SERVICES ARIZONA STATE
GOVERNMENT (Appropriations)
ARIZONA DEPARTMENT OF ECONOMIC SECURITY DIVISION OF CHILDREN, YOUTH AND FAMILIES
District Offices
Field Offices
$
Administration for Children, Youth and Families
Children’s Bureau
$
$
$
SUBCONTRACTED PROVIDERS
$
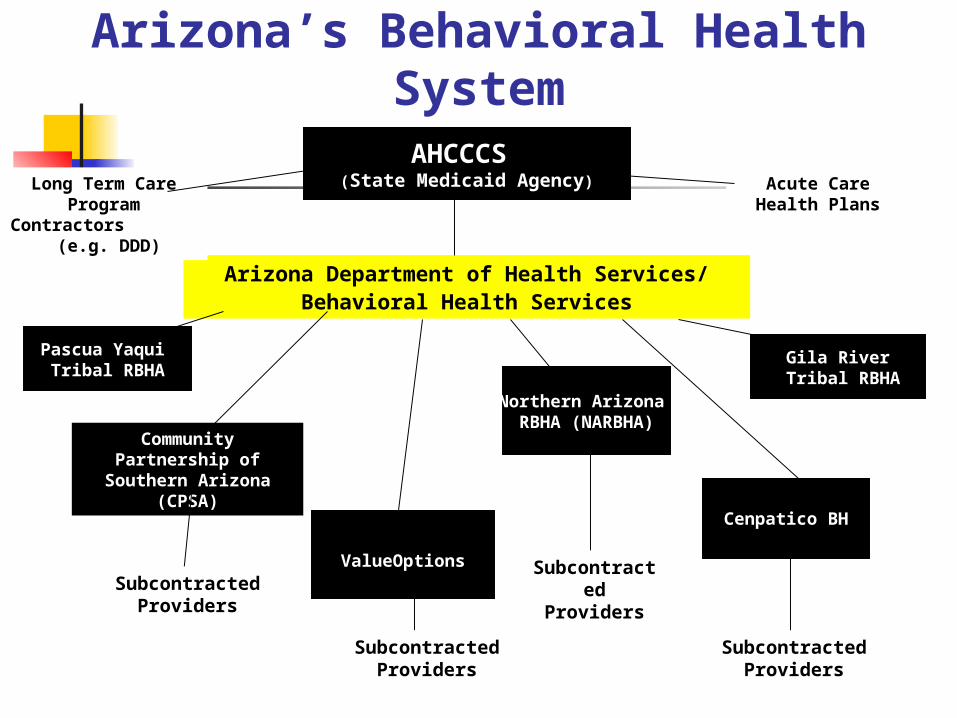
Arizona’s Behavioral Health System
AHCCCS (State Medicaid Agency)
Arizona Department of Health Services/Behavioral Health Services
Pascua Yaqui Tribal RBHA
Community Partnership of Southern Arizona
(CPSA)
ValueOptions
Northern Arizona RBHA (NARBHA)
Acute Care Health Plans
Cenpatico BH
Subcontracted Providers
Subcontracted Providers
Subcontracted Providers
Long Term Care Program Contractors
(e.g. DDD)
Gila River Tribal RBHA
Subcontracted Providers
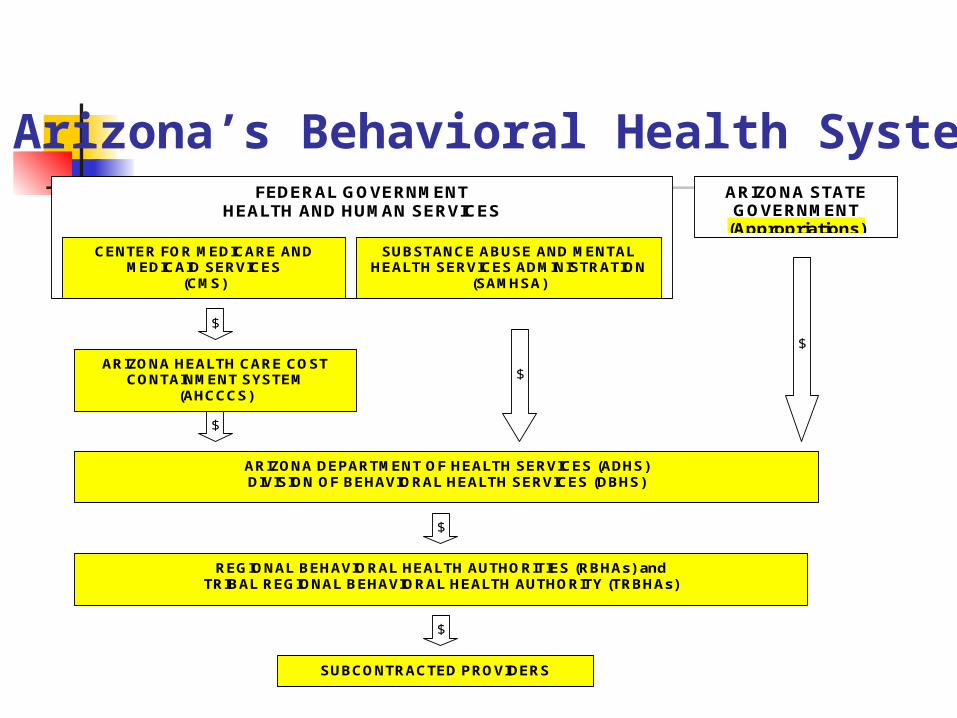
FEDERAL GOVERNMENT HEALTH AND HUMAN SERVICES
ARIZONA STATE GOVERNMENT
(Appropriations)
ARIZONA DEPARTMENT OF HEALTH SERVICES (ADHS) DIVISION OF BEHAVIORAL HEALTH SERVICES (DBHS)
ARIZONA HEALTH CARE COST CONTAINMENT SYSTEM
(AHCCCS)
REGIONAL BEHAVIORAL HEALTH AUTHORITIES (RBHAs) and TRIBAL REGIONAL BEHAVIORAL HEALTH AUTHORITY (TRBHAs)
SUBCONTRACTED PROVIDERS
SUBSTANCE ABUSE AND MENTAL HEALTH SERVICES ADMINISTRATION
(SAMHSA)
CENTER FOR MEDICARE AND MEDICAID SERVICES
(CMS)
$
$
$
$
$
$
Arizona’s Behavioral Health System

Arizona Behavioral Health and Child Welfare
Systems
Different expectations Different mandates and external
requirements Different funding streams and
approaches Different pace of work with family No common outcomes
Arizona Behavioral Health and Child Welfare
Systems
The child welfare system had developed its own de facto behavioral health system, to meet the unique needs of children and families it serves – needs that the public behavioral health system did not fully understand, or know how to address; and needs that the child welfare system was neither trained nor equipped to address.
Terrible outcomes for children: • Behavioral health needs going unmet• Limited permanency• Poor academic achievement by
children• Extremely high juvenile delinquency
among foster children• Family instability damaging children• Poor outcomes evident among
former foster children
Consequences of Misalignment of BH and CW Systems

Huge Costs to Families: “Mending the Damage”
Trust (“abandonment”) Triggering traumatic memories Guilt Etc.
Consequences of Misalignment of BH and CW Systems
Enormous Costs to Both Systems: Inadequately prepared, poorly supported
clinical staff Insufficient effort to heal families, which
might prevent or shorten removals of children to foster care
Lack of appropriate front loaded behavioral health services exacerbates family separations
Resentment, lack of understanding & mistrust between systems’ personnel
Consequences of Misalignment of BH and CW Systems
Enormous Costs to Both Systems: Lack of “shared care” evident Trauma-induced, situational and
substance-abuse related BH needs challenge both systems
Overworked personnel discouraged by poor results equates to high turnover and low morale
Consequences of Misalignment of BH and CW Systems
What Do Children Experience?
Separation from parents Separation from brothers and sisters Loss of pets Move from familiar
neighborhood/community Change of school Loss of friends Unfamiliar caretakers, routine, expectations Loss of comfort objects Sadness, anger, fear, guilt, shame,
differentness
“We Gotta Get Outta This Mess…”
But How?? How to optimize the existing expertise and resources within each system to meet a common success with a shared family?
Impetus for Change
Community Initiatives High Profile Tragedy CFSR Findings Legislation – Executive
Order System of Care Grant
Program Litigation

Arizona’s Reform Journey
JK Litigation (1991-1997) “Discovery” (1997-2000)
Governor’s Task Force on Behavioral Health and Child Welfare (2000)
JK Settlement Agreement (2001) Governor’s CPS Reform (2003)
The 12 Arizona Principles
Collaboration with the Child and Family Functional Outcomes Collaboration with Others Accessible Services Best Practices Most Appropriate Setting Timeliness Services Tailored to the Child and Family Stability Respect for the Child and Family’s Unique
Cultural Heritage Independence Connection to Natural Supports
Leadership – Being a Change Agent
Leadership Qualities: Philosophical Buy-In Early Innovators Sense of Urgency Commitment to Action

Being a Change Agent Through Parent/Professional Partnerships
Partnering at All Levels Voice, Access and Ownership Mirrors Successful Business
Practices Family is the Constant in
Communities Shared Burden with Change
Building A Common Vision
“In collaboration with the child and family and others, Arizona will provide accessible behavioral health services designed to aid children to:
achieve success in school live with their families avoid delinquency become stable and productive adults.
Services will be tailored to the child and family and provided in the most appropriate setting, in a timely fashion, and in accordance with best practices, while respecting the child’s and family’s cultural heritage.”
J.K. vs. Eden et al. No. CIV 91-261 TUC JMR, Paragraph 18
Building A Common Vision
Arizona Children’s Executive Committee: Collaborative Implementation of JK
Actions Family Involvement A Primary Value
(2001) Memorandum of Understanding (2002) Barriers Identification and Resolution
(2003) Commitment to Support CPS Reform
(2004)
Developing a Common Language
12 Arizona Principles Child Welfare Values and
Principles (Safety, Permanence, Well-Being)
Crosswalk #1 - Values and Principles
Crosswalk #2 - Child and Family Teams/ Family Group Conferencing
Developing a Common Language
Awareness Sensitization Empathy Understanding Learning Community

Creating Change in Arizona
Structure Process Outcomes
Structure to Address Unique Needs of Children
and Families Funding Policies: Example – AZ’s Urgent
Response for Children Entering Foster Care
Letters of Agreement/Detailed Protocols
Clinical Guidelines: “How to Operationalize Our Common Work”
Targeted Programming
Funding Maximizing Medicaid – One Single
System Risk-Adjusted Capitation (7/1/04) Program Development to Address
Needs Direct Supports to Caregivers Birth to Five Substance Abuse Specialty Skills and Services Expanded Provider Networks

Policies – Example:Arizona’s Urgent BH
Response for Children Entering Foster Care
One Simple Sentence…
“An urgent response should be initiated in a punctual manner, within a timeframe indicated by the person’s clinical needs, but no later than 24 hours from the initial identification of need. Urgent responses must be initiated upon notification by DES/CPS that a child has been, or will be, removed from their home.”
ADHS Policy 3.2: Appointment Standards and Timeliness of Services
[Effective August 15, 2003]

Arizona’s “Urgent BH Response,” and its Five
PurposesUrgent responses must be initiated upon notification by DES/CPS that a
child has been, or will be, removed from their home.” ADHS Policy 3.2: Appointment Standards and Timeliness of Services
[Effective August 15, 2003]
1. Identify immediate safety needs and presenting problems
2. Provide direct therapeutic support to each child3. Provide direct support to each child’s new
caregiver4. Initiate development of a Child and Family Team5. Provide CPS caseworker and Court with findings
and recommendations to inform the caseplan
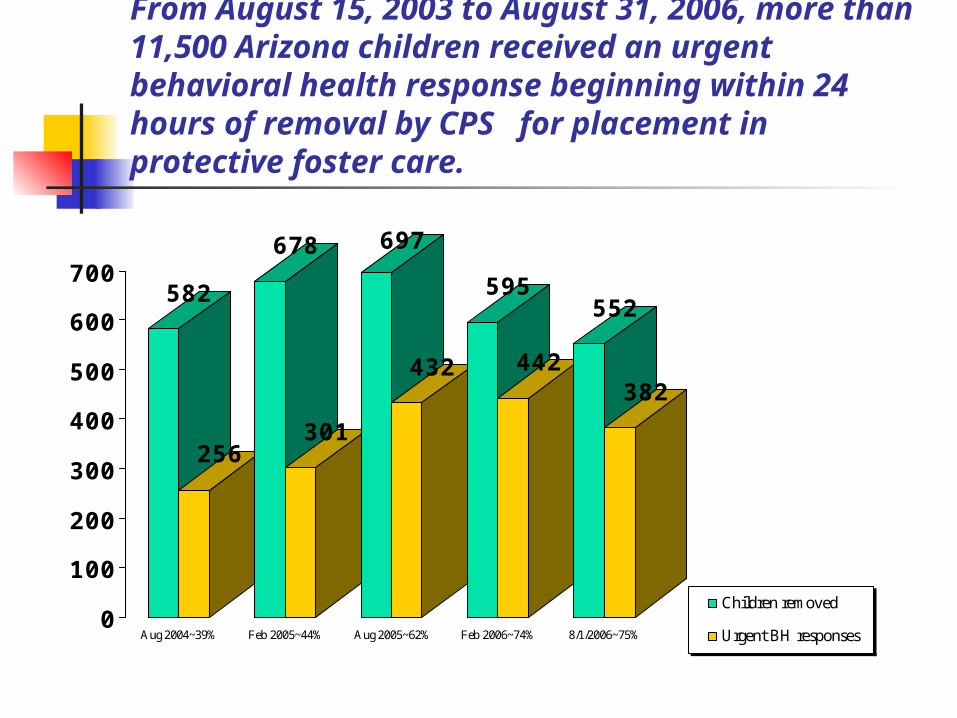
From August 15, 2003 to August 31, 2006, more than 11,500 Arizona children received an urgent behavioral health response beginning within 24 hours of removal by CPS for placement in protective foster care.
582
256
678
301
697
432
595
442
552
382
0
100
200
300
400
500
600
700
Aug 2004~39% Feb 2005~44% Aug 2005~62% Feb 2006~74% 8/1/2006~75%
Children removed
Urgent BH responses
The Unique BH Needs of Children Involved with
CPS
1. Services to the Child2. Services to the Family3. Services to Support Temporary
Protective Caregivers
ADHS Practice Improvement Protocol #15: Addressing the Unique Behavioral Health Needs of Children Involved with CPS
1. Working in Partnership2. Addressing Needs in the Context
of Each Child’s Family3. When the Child Remains with
His/Her Family4. When the Child Is Removed to
Protective Foster Care

ADHS Practice Improvement Protocol #15: Addressing the Unique Behavioral Health Needs of Children Involved with CPS
5. When the Child Returns Home to His/Her Family of Origin from Foster Care
6. When the Child Achieves Permanency through Guardianship or Adoption
7. Special Considerations for Infants, Toddlers and Pre-School Aged Children
8. Preparing the Adolescent for Independent Living
[See www.azdhs.gov/bhs/guidance/unique_cps.htm]
Trauma-Informed Clinical Approaches:
On-Line CEU-Credited Training
Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) – Medical University of South Carolina -- http://tfcbt.musc.edu
2. National Center on Substance Abuse and Child
Welfare (NCSACW) -- http://www.ncsacw.samhsa.gov/tutorials/
3. Bonding and Attachment in A Maltreated Child – Bruce Perry MD, Child Trauma Academy - http://
www.childtraumaacademy.com/bonding_attachment/index.html
Trauma-Informed Clinical Approaches
Cognitive Behavioral Intervention for Trauma in Schools (CBITS) ® Manual (Lisa H. Jaycox Ph.D., 2004) www.sopriswest.com or [email protected]
Seeking Safety: A Treatment Manual for PTSD and Substance Abuse
(Najavits, Guilford Press, 2002) www.seekingsafety.org Trauma Adaptive Recovery Group Education & Therapy Model for
Adolescents (TARGET-A; Ford et al., 2000; Ford, Mahoney & Russo, 2004) from www.ptsdfreedom.org or [email protected]
Dialectical Behavior Therapy for Adolescents, Rathus, Miller & Linehan (in
press) School-Based Trauma/Grief Group Psychotherapy Program
(SPARCS; Layne, Saltzman, Pynoos, et al., 2000) from [email protected]
Source: Jorielle R. Brown Ph.D, SAMHSA/CSAT, Treating Co-Occurring Disorders (June 2006)

Therapeutic Foster Care: A Programming Success
Story Early Efforts – An Alternative to Congregate
Care Braiding Medicaid and Title IV-E Resources ADHS Practice Improvement Protocols:
#12: Therapeutic Foster Care Services for Children
#14: Out of Home Care Services Recruitment, Licensing and Certification TFC Capacity: From 9 (09/03) to 404 (05/06) PS-MAPP and PS-MAPP TFC Curriculum

Processes Promoting Change
Child and Family Teams/Wraparound
Casey Family – Team Decision Making
Co-location of Behavioral Health with Child Welfare Personnel
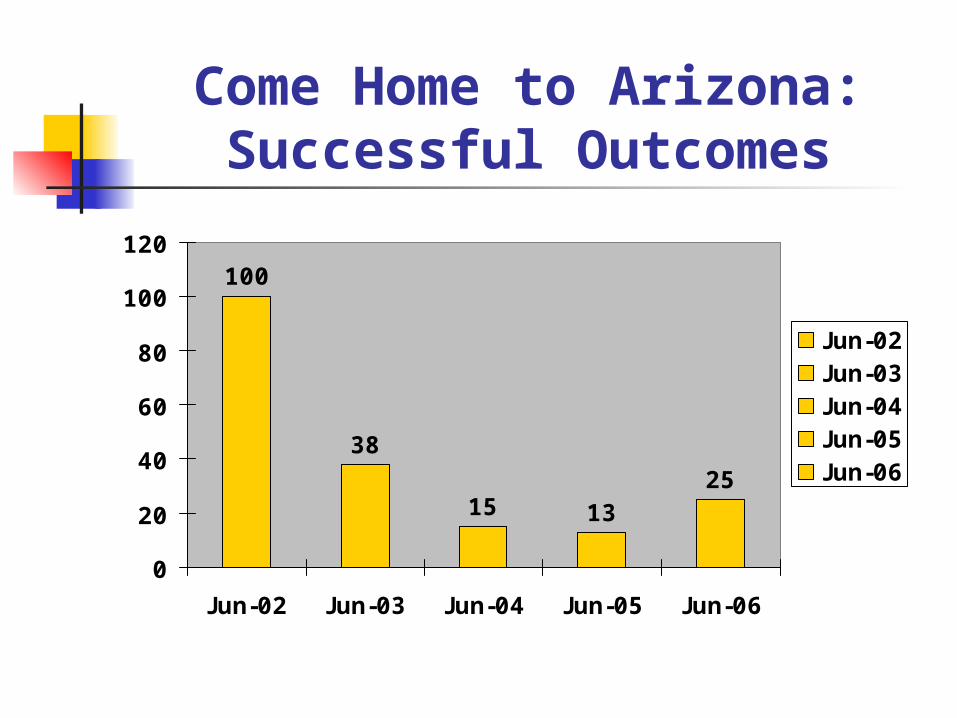
Come Home to Arizona:Successful Outcomes
100
38
15 1325
0
20
40
60
80
100
120
Jun-02 Jun-03 Jun-04 Jun-05 Jun-06
Jun-02Jun-03Jun-04Jun-05Jun-06
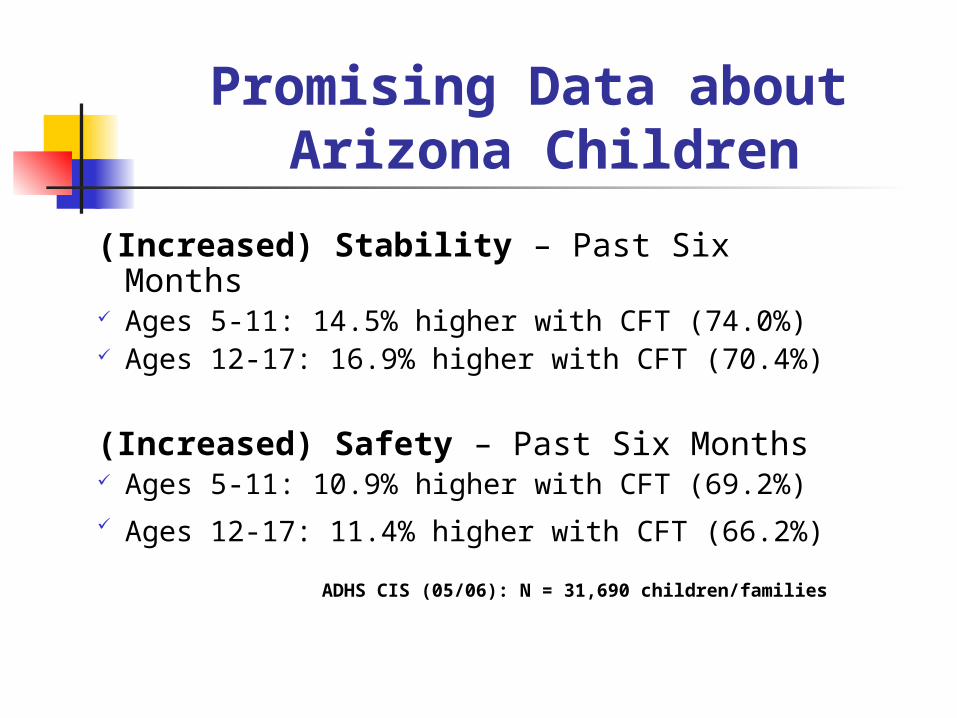
Promising Data about Arizona Children
(Increased) Stability – Past Six Months Ages 5-11: 14.5% higher with CFT (74.0%) Ages 12-17: 16.9% higher with CFT (70.4%)
(Increased) Safety – Past Six Months Ages 5-11: 10.9% higher with CFT (69.2%) Ages 12-17: 11.4% higher with CFT (66.2%)
ADHS CIS (05/06): N = 31,690 children/families
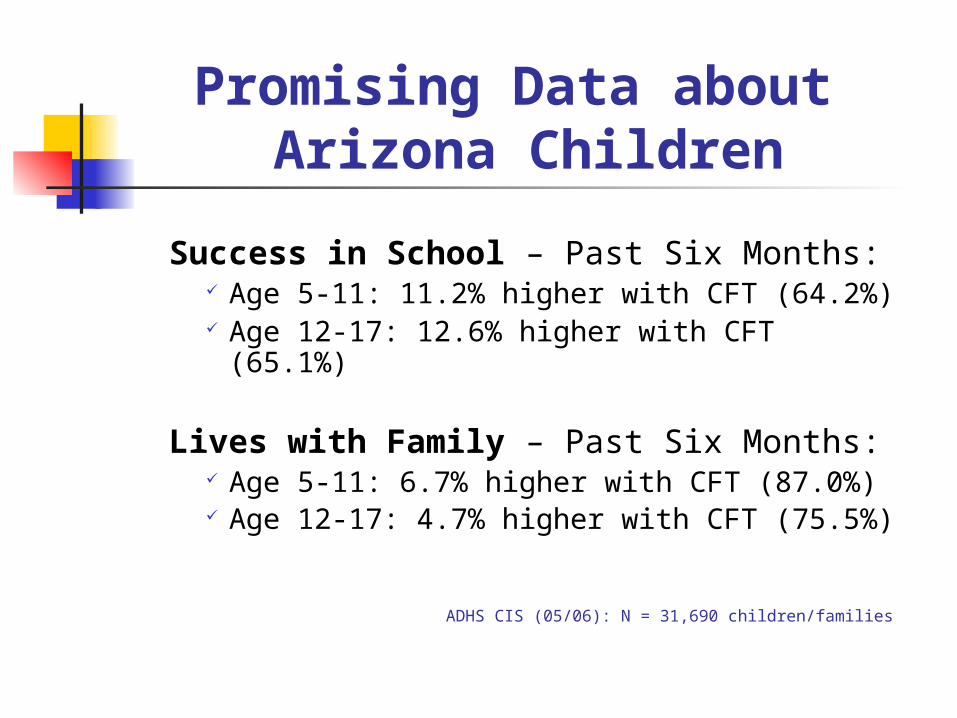
Promising Data about Arizona Children
Success in School – Past Six Months: Age 5-11: 11.2% higher with CFT (64.2%) Age 12-17: 12.6% higher with CFT (65.1%)
Lives with Family – Past Six Months: Age 5-11: 6.7% higher with CFT (87.0%) Age 12-17: 4.7% higher with CFT (75.5%)
ADHS CIS (05/06): N = 31,690 children/families
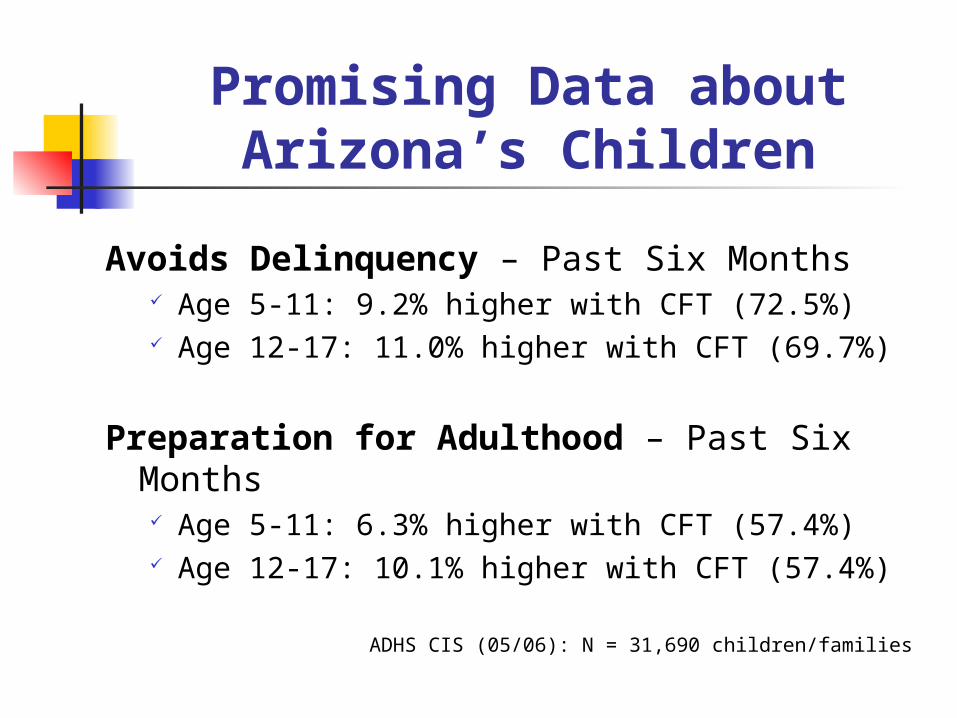
Promising Data aboutArizona’s Children
Avoids Delinquency – Past Six Months Age 5-11: 9.2% higher with CFT (72.5%) Age 12-17: 11.0% higher with CFT (69.7%)
Preparation for Adulthood – Past Six Months Age 5-11: 6.3% higher with CFT (57.4%) Age 12-17: 10.1% higher with CFT (57.4%)
ADHS CIS (05/06): N = 31,690 children/families

Comparing Outcomes for Arizona Children with and without Child and
Family Teams (Ages 5-11)
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
CFT
No CFT
CFT 74.6% 69.2% 77.9% 62.9% 77.9% 88.8%
No CFT 59.5% 55.5% 65.1% 52.3% 65.1% 83.3%
Increased Stability
Increased Safety
Avoids Deliquency
Prep for Adulthood
Success in School
Lives with Family
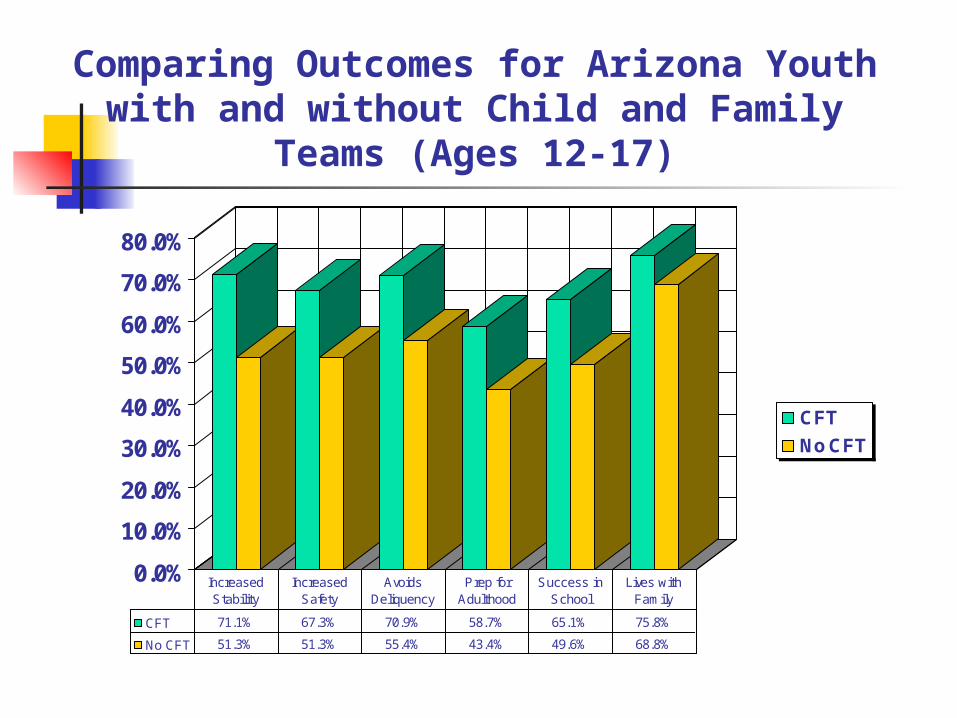
Comparing Outcomes for Arizona Youth with and without Child and
Family Teams (Ages 12-17)
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
CFT
No CFT
CFT 71.1% 67.3% 70.9% 58.7% 65.1% 75.8%
No CFT 51.3% 51.3% 55.4% 43.4% 49.6% 68.8%
Increased Stability
Increased Safety
Avoids Deliquency
Prep for Adulthood
Success in School
Lives with Family
Taking It to the Next Level
Service Integration: “One Family, One Team, One Plan”
AssessmentPlanningThe Whole FamilyFamily to Family
Taking It to the Next Level
Service Delivery Capacity Capability Strengthening and Preserving
Families Service Integration – System Level IV-E Waiver: Expedited Reunification

Taking It to the Next Level
“It Takes A Village”
Community Network Teams

Questions?
Thank you for your attention!