addressing the “special cause” increase in pediatric clabsis: a
TRANSCRIPT

Addressing the “Special Cause” Increase in Pediatric CLABSIs:
A Quality Improvement Approach

Getting on the Telephone:• Your GoTo Navigation pane should be on the right of your screen• Expand the “audio” box• Click Telephone option• Dial the phone number• Enter the access code, then press #• You will be prompted to enable audio and enter your audio pin• Please remember to mute yourself
If you are having trouble getting onto the telephone, please enter your concerns in the question box ‐ we’ll be happy to help!
Questions and Comments:Should you have any questions and/or comments during the webinar, please enter them into the question box, and we will address them during the open discussion portion.
Webinar Logistics

CLA-BSI Pediatric Webinar
Mike Gutzeit, MDMargie McCaskey, RNJeff Hord, MD
Friday, January 29, 20163:30pm ‐ 4:30pm EST

Our CLA-BSI Leaders
Margie McCaskey, RN, DNPClinical Outcomes & Quality AdvisorChildren’s of Alabama
Jeff Hord, MDDirector of Hematology/OncologyAkron Children’s Hospital
Mike Gutzeit, MDChief Medical OfficerChildren’s Hospital of Wisconsin
Holly O'Brien, MSN RN CPPSSafety Program ManagerChildren’s Hospital of Wisconsin

Agenda
Friday, January 29, 2016 3:30pm ‐ 4:30pm ESTAgenda Item: Presenter: Time:
Welcome and Objectives Erin Goodman 3 minutes
About SPS Emily Oehler 5 minutes
Unique Circumstances of Pediatrics CLABSIs Mike Gutzeit 8 minutes
Prevention Bundle and High‐Reliability Theory Mike Gutzeit 8 minutes
Approach to Special Cause Margie McCaskey 8 minutes
Initial Learning from the Pediatric CLABSI Increase Jeff Hord 8 minutes
Open Discussion Emily Oehler 15 minutes
Adjourn Anyah Land 2 minutes

Session Objectives
• Understand Pediatric CLABSIs – Central Line Associated Blood Stream Infections
• Understand the Root Cause Testing Theory and the Method to Verify Suspected Cause
• Learn from SPS experience in responding to special cause within Pediatric CLABSIs

About SPS
Emily OehlerProject Manager

Children’s Hospitals’ Solutions for Patient Safety (SPS) Network Map

Working together to eliminate serious harm across all
children’s hospitals
OUR MISSION:
Children’s Hospitals’ Solutions for Patient Safety

Our 2015‐2016 Goals
40 percent reduction in hospital‐acquired conditions (HACs)
10 percent reduction in readmissions
25 percent reduction in serious safety events (SSEs)

Unique Circumstances ofPediatrics CLABSIs
Mike Gutzeit, MDChief Medical OfficerChildren’s Hospital of Wisconsin

Estimated Attributable Costs
• $1000 CAUTI• $3000 OBAE• $5000 ADE• $13,000 Falls• $35,000 CLABSI• $43,000 PU• $51,000 VAP

CLABSIs AreUnique for Children
Children have different needs than adults. They require special attention for many reasons such as…• Age diversity • Challenges with immune function• Concerns about deploying the usual
hygiene agents due to potential toxicity
• Variability in home care standards• Maintenance vs. insertion• Kids are Kids!
• Constant motion• Hygiene

Conditions generating unique pediatric safety risk:• Size: Catheters are smaller & more prone to complication; anatomy is smaller leading to difficulties with dressings and location of insertion sites in close proximity to other things (trachs, GT’s ostomies, etc.)
• High potential for extravasation / effusion due to thinner vasculature
• Greater challenges with PIV access• Greater potential for line migration
Defining the HAC Problem in Pediatrics
Prevention Bundle and High‐Reliability Theory
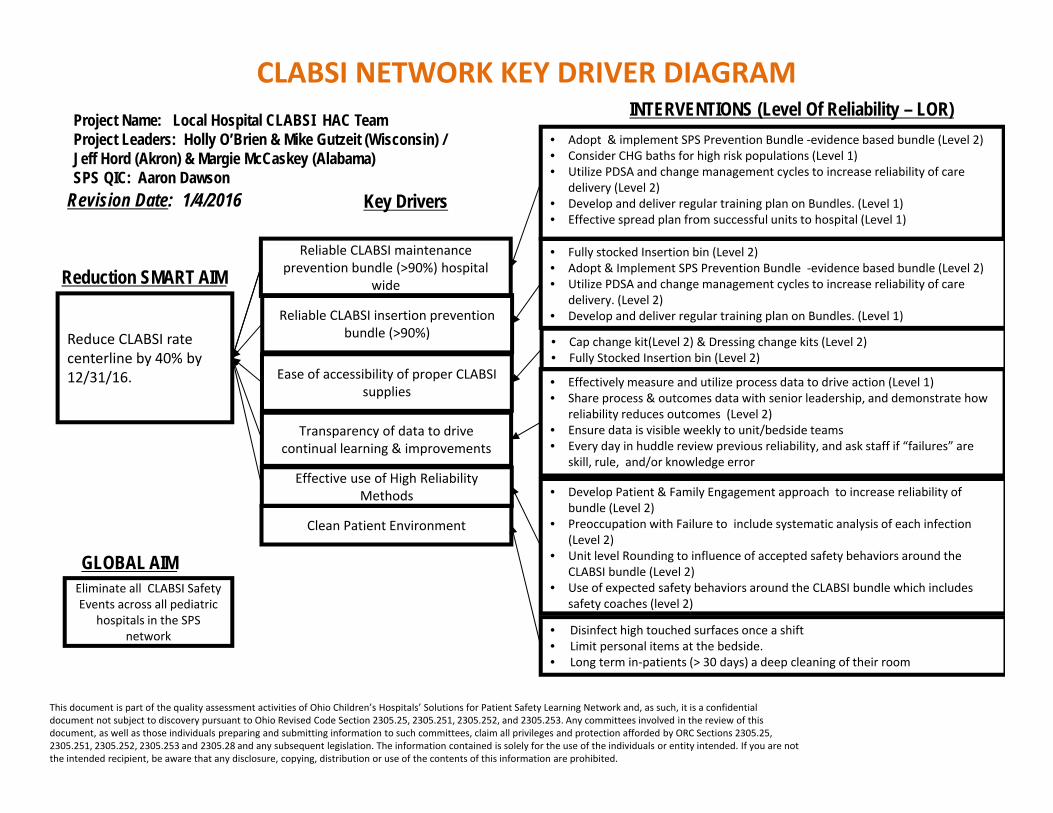
CLABSI NETWORK KEY DRIVER DIAGRAM Project Name: Local Hospital CLABSI HAC Team Project Leaders: Holly O’Brien & Mike Gutzeit (Wisconsin) / Jeff Hord (Akron) & Margie McCaskey (Alabama)SPS QIC: Aaron Dawson
Reliable CLABSI insertion prevention bundle (>90%)
Ease of accessibility of proper CLABSI supplies
Transparency of data to drive continual learning & improvements
Revision Date: 1/4/2016
Eliminate all CLABSI Safety Events across all pediatric
hospitals in the SPS network
GLOBAL AIM
Reliable CLABSI maintenance prevention bundle (>90%) hospital
wide
Effective use of High Reliability Methods
Reduction SMART AIM
Reduce CLABSI rate centerline by 40% by 12/31/16.
INTERVENTIONS (Level Of Reliability – LOR)• Adopt & implement SPS Prevention Bundle ‐evidence based bundle (Level 2)• Consider CHG baths for high risk populations (Level 1)• Utilize PDSA and change management cycles to increase reliability of care
delivery (Level 2)• Develop and deliver regular training plan on Bundles. (Level 1)• Effective spread plan from successful units to hospital (Level 1)
Clean Patient Environment
• Fully stocked Insertion bin (Level 2)• Adopt & Implement SPS Prevention Bundle ‐evidence based bundle (Level 2)• Utilize PDSA and change management cycles to increase reliability of care
delivery. (Level 2)• Develop and deliver regular training plan on Bundles. (Level 1)
• Cap change kit(Level 2) & Dressing change kits (Level 2)• Fully Stocked Insertion bin (Level 2)
• Effectively measure and utilize process data to drive action (Level 1)• Share process & outcomes data with senior leadership, and demonstrate how
reliability reduces outcomes (Level 2)• Ensure data is visible weekly to unit/bedside teams• Every day in huddle review previous reliability, and ask staff if “failures” are
skill, rule, and/or knowledge error
• Develop Patient & Family Engagement approach to increase reliability of bundle (Level 2)
• Preoccupation with Failure to include systematic analysis of each infection (Level 2)
• Unit level Rounding to influence of accepted safety behaviors around the CLABSI bundle (Level 2)
• Use of expected safety behaviors around the CLABSI bundle which includes safety coaches (level 2)
• Disinfect high touched surfaces once a shift• Limit personal items at the bedside.• Long term in‐patients (> 30 days) a deep cleaning of their room
Key Drivers
This document is part of the quality assessment activities of Ohio Children’s Hospitals’ Solutions for Patient Safety Learning Network and, as such, it is a confidential document not subject to discovery pursuant to Ohio Revised Code Section 2305.25, 2305.251, 2305.252, and 2305.253. Any committees involved in the review of this document, as well as those individuals preparing and submitting information to such committees, claim all privileges and protection afforded by ORC Sections 2305.25, 2305.251, 2305.252, 2305.253 and 2305.28 and any subsequent legislation. The information contained is solely for the use of the individuals or entity intended. If you are not the intended recipient, be aware that any disclosure, copying, distribution or use of the contents of this information are prohibited.

2016 Focus for SPS Pediatric CLABSIs
• Prevention Bundle Reliability• Hematology/Oncology Population• Environmental Contamination

PROCESS OUTCOME
What should be standardized?
SPS Pediatric CLABSIPrevention Bundles

Nomenclature
• SPS Prevention Bundle ‐ Terminology selected following input from the SPS Clinical Steering Team
– SPS Standard Element : Strong evidence suggests that implementation of this element is associated with a significant decrease in patient harm; all SPS hospitals should implement and measure reliability of this element.
– Recommended Element: Preliminary data and clinical expert opinion support the implementation of this element; SPS hospitals should strongly consider implementing and measuring reliability of this element.
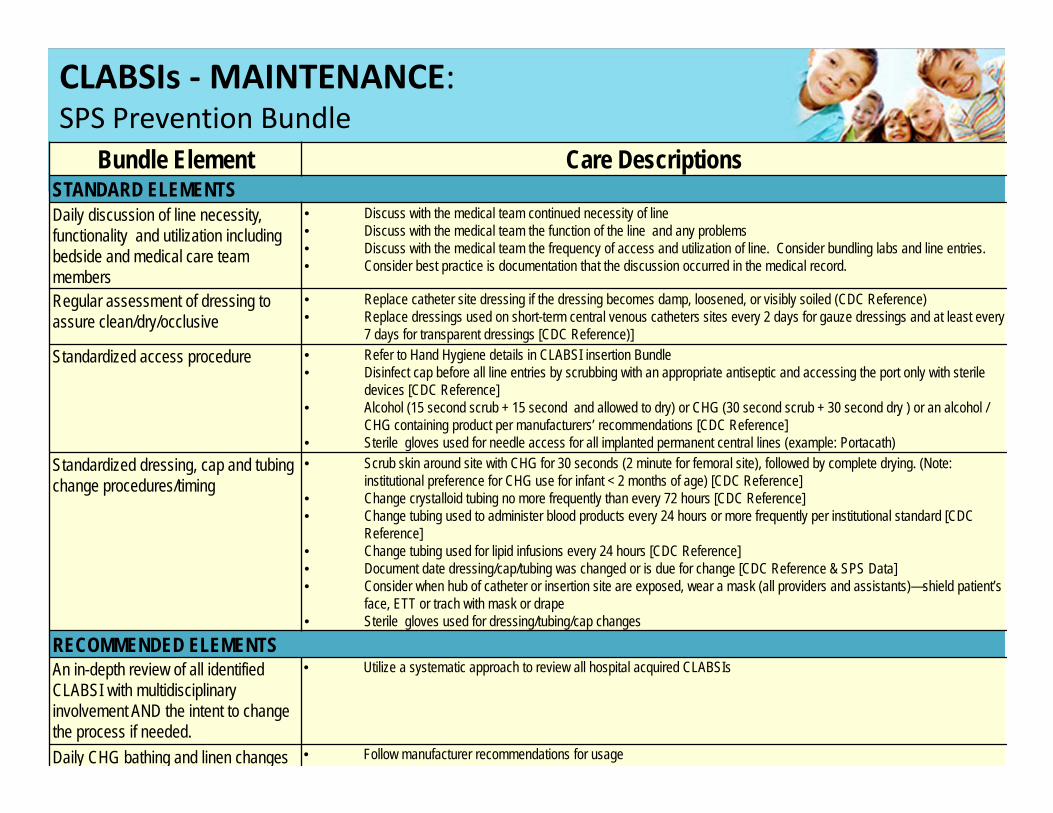
Bundle Element Care DescriptionsSTANDARD ELEMENTSDaily discussion of line necessity, functionality and utilization including bedside and medical care team members
• Discuss with the medical team continued necessity of line• Discuss with the medical team the function of the line and any problems • Discuss with the medical team the frequency of access and utilization of line. Consider bundling labs and line entries.• Consider best practice is documentation that the discussion occurred in the medical record.
Regular assessment of dressing to assure clean/dry/occlusive
• Replace catheter site dressing if the dressing becomes damp, loosened, or visibly soiled (CDC Reference)• Replace dressings used on short-term central venous catheters sites every 2 days for gauze dressings and at least every
7 days for transparent dressings [CDC Reference)]Standardized access procedure • Refer to Hand Hygiene details in CLABSI insertion Bundle
• Disinfect cap before all line entries by scrubbing with an appropriate antiseptic and accessing the port only with sterile devices [CDC Reference]
• Alcohol (15 second scrub + 15 second and allowed to dry) or CHG (30 second scrub + 30 second dry ) or an alcohol / CHG containing product per manufacturers’ recommendations [CDC Reference]
• Sterile gloves used for needle access for all implanted permanent central lines (example: Portacath)Standardized dressing, cap and tubing change procedures/timing
• Scrub skin around site with CHG for 30 seconds (2 minute for femoral site), followed by complete drying. (Note: institutional preference for CHG use for infant < 2 months of age) [CDC Reference]
• Change crystalloid tubing no more frequently than every 72 hours [CDC Reference]• Change tubing used to administer blood products every 24 hours or more frequently per institutional standard [CDC
Reference]• Change tubing used for lipid infusions every 24 hours [CDC Reference]• Document date dressing/cap/tubing was changed or is due for change [CDC Reference & SPS Data]• Consider when hub of catheter or insertion site are exposed, wear a mask (all providers and assistants)—shield patient’s
face, ETT or trach with mask or drape• Sterile gloves used for dressing/tubing/cap changes
RECOMMENDED ELEMENTSAn in-depth review of all identified CLABSI with multidisciplinary involvement AND the intent to change the process if needed.
• Utilize a systematic approach to review all hospital acquired CLABSIs
Daily CHG bathing and linen changes • Follow manufacturer recommendations for usage
CLABSIs ‐MAINTENANCE: SPS Prevention Bundle

Prevention Bundle and High‐Reliability Theory

Prevention Bundle and High‐Reliability Theory

Approach to Special Cause
Margie McCaskey, RN, DNPClinical Outcomes &Quality AdvisorChildren’s of Alabama
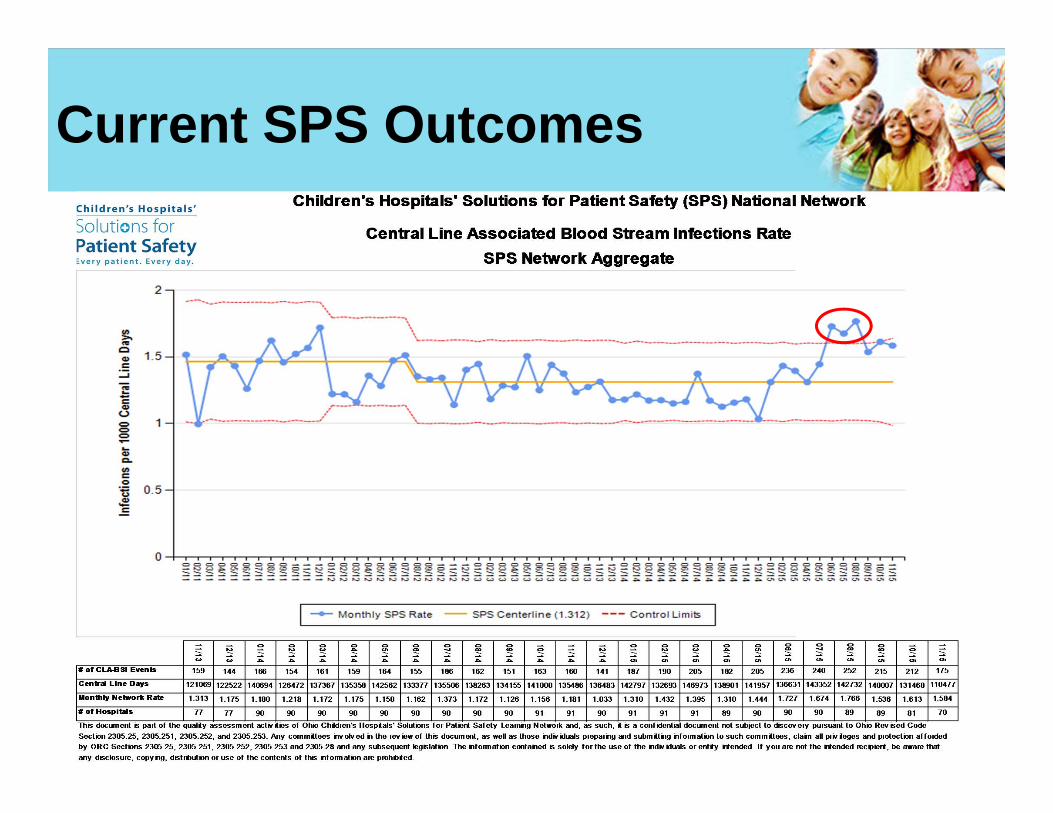
Current SPS Outcomes

Special Cause Process Map
• Products• Alcohol caps• Tubing ‐ the way tubings are set up; cracked tubing; quads on quads; are there hairline cracks in any of the tubing that could be causing this?
• Z‐flo pillows
• Human Factors• Changing staff workflows• Dress code compliance (jewelry, nails, Fitbits)• Keeping linens clean• Competency in staff – practice with line maintenance, keeping environment clean, following bundle elements
• Populations• Medically complex – short gut & MBI• NICU • Oncology – changes in COG protocol
Initial Findings During Focus Groups

Smart OBJECTIVE
Suspected Cause
Method to Verify Suspected Cause
To vigilantly a) identify, b) verify and c) mitigate the root cause(s) of the CLABSI special cause affecting SPS hospitals in 2015
Change in the Jan 2015 NHSNoperational definition change
Change in patient population
Change in product or device
Compare similarities and differences between special cause hospitals and stable hospitals: utilize multi-disciplinary team,
random in-person audits
Quantify the op def changes in stable hospitals: sample unchanged hospitals asking them to evaluate their 2015 events
through the ‘lens’ of the 2014 definition and 2015 definition
Change in organisms
KeyYellow = Active investigationWhite = Future investigation
SPS CLA-BSI Special Cause 2015Root Cause Testing Theory
Revision Date: 11/18/2015
Spread special cause learning to the SPS Network to prevent
future CLA-BSI harm
Global OBJECTIVE
Quantify the op def changes in hospitals with special cause (26): ask special cause hospitals to evaluate their 2015 events through the ‘lens’ of the 2014 definition and 2015 definition
Investigate and document (multi-site) credible event timeline linkage between change and special cause
Ask special cause hospitals (26) permission to engage the CDC to explore microbiologic epidemiology of the rate increase
Clear learning objectives and timeline with CDC
Change in prevention bundle process execution at the bedside (undetected by process reliability measurement system)
e.g. line access procedures
Sub-groups of hospitals investigating credible categories of suspected special cause
Rapid cycle PDSA testing to gather data and test hypothesis
Real-time sharing of lessons learned and recommendations across the network
Theory of Special Cause

Jeff Hord, MDDirector of Hematology/OncologyAkron Children’s Hospital
Initial Learning from thePediatric CLABSI Increase

Potential suspects of special cause• Product / device changes
• Alcohol caps• Flush syringes• Dressing changes
• Linen change frequency• Changes in organisms
• Reported increases• Reported new cases that had not been seen prior
• Changes in patient population• Short gut & MBI
Causes Identified from theNetwork Investigation

• Unit Acuity• Need for ongoing education• Organizational factors• Belief some BSIs are not preventable with bundle care interventions only
• Staffing (Turnover, New Staff, etc)• Adding/Stopping Bundle Elements
Unlikely Causes of Network Special Cause

• Renewed focus on bundle reliability – let’s get to 90%!
• Changes to the operational definition may have had a larger impact
than anticipated.
• The special cause served as a catalyst to form workgroups (in 2016)
in the following areas:
• Reducing Pediatric CLABSI’s in Hem/Onc population
• Reducing Pediatric CLABSI’s in the NICU population
• Investigating changes in products or device across the network
• Investigating changes in prevention bundle process execution at
the bedside
Learning and Next Steps for SPS Pediatric CLABSIs

Open Discussion
Emily OehlerProject Manager

More Information on Preventing Pediatric HACs• CEO Steering Team• Clinical Leadership Group – 2‐3 HAC Leaders for each HAC and SMEs
• Culture Council• Learning Council• Clinical Steering Team• Research and Publications
• Publicly available information:– www.solutionsforpatientsafety.org

More Information on Preventing Pediatric HACs• CEO Steering Team• Clinical Leadership Group – 2-3 HAC Leaders
for each HAC and SMEs• Culture Council• Learning Council• Clinical Steering Team• Research and Publications
• Publicly available information:– www.solutionsforpatientsafety.org
Results on Our Website
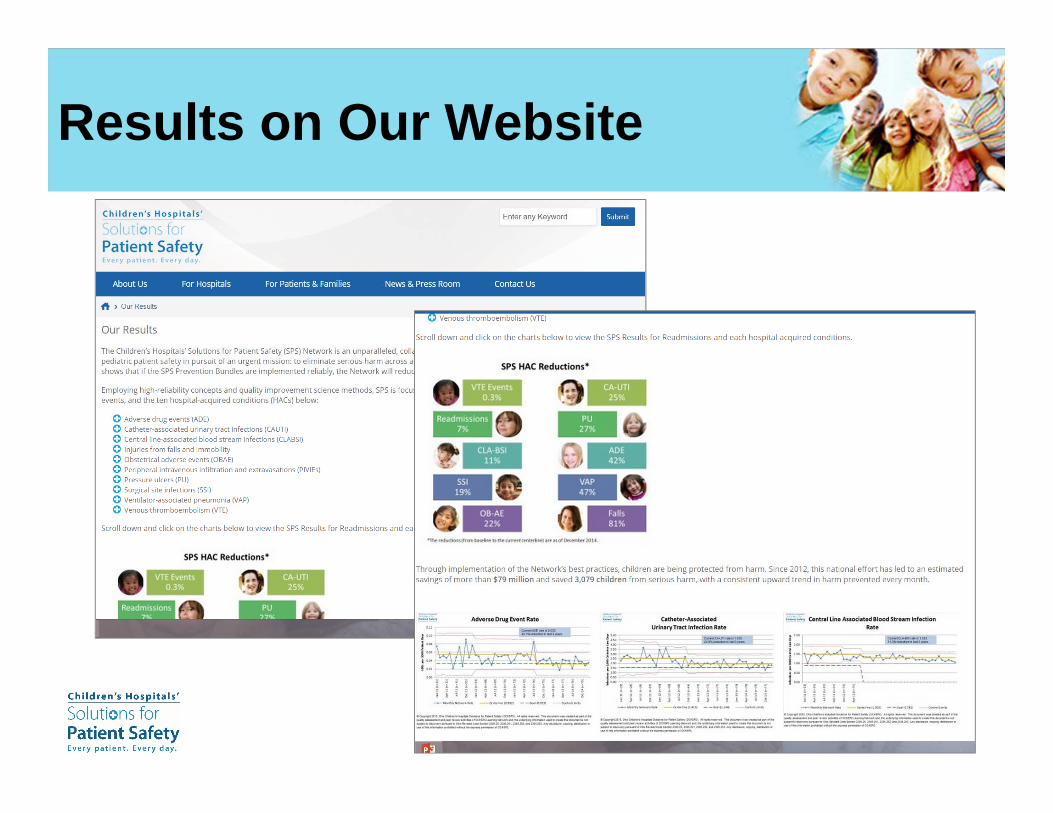
Results on Our Website
Thank you!


Follow us on Twitter ‐@sps4kids
Like us on Facebook
Share what you’re learning here using the hashtag #sharesafety
SPS is on Twitter & Facebook!
#