ad-a263 559 - defense technical information center · ad-a263 559 iiiii ad_____ report no tn93-4...
TRANSCRIPT
AD-A263 559iIIII AD_____________________
REPORT NO TN93-4
MEDICAL ASPECTS OF COLDWEATHER OPERATIONS:
A Handbook for Medical Officers
U S ARMY RESEARCH INSTITUTEOF
ENVIRONMENTAL MEDICINE
Natick, Massachusetts01760-5007
DTI
APR30 93
App,*ovod I*, pub, "l l ,P)OO distributio. niie
UNITED STATES ARMY
MEDICAL RESEARCH & DEVELOPMENT COMMAND
93-0917493 4 0• 30
The findings in this report are not to be construed as anofficial Department of the Army position, unless so designated byother authorized documents.
DTIC AVAILABILITY NOTICE
Qualified requestors may obtain copies of this document fromCormmander, Defense Technical Information Center (DTIC), CameronStation, Alexandria, VA 22314.
DISTRIBUTION UNLIMITED
DISPOSITION INSTRUCTIONS
Destroy this report when no longer needed.
Do not return to the originator.

( Form ApprovedREPORT DOCUMENTATION PAGE 0MS No. 0704-0188
P-bi reoort,.rg ourden for 'hI,:CfeCtion cif nfo~ratior' is el rated to. 4erage I rr oer r.worse, ncl-oing tt'e inhe for rey'ewrng instru.ctions. searchi~ng ex~strrg data sources.lather,,ig and m ,.nt,rit,rrr the data needed. and corni'Oetinq and reviewing the <atecton of informtation Send comments rNqarding this burden estimate or any )ttrer asibent of ttisCollection ,'If I i:) at Cnt. nclI 'nq Suggestions for too tiog ths ioi~roen to Ni~shr r'qon Headoruarters Services. Direclorate for In for m.tion Qoerattons and Rpoorts. 121 is etfersonDavis H~qr.av. Su.te 42C4 Olrg~ton, iA a 2202-4 302 and to the Officeo .)t anagement ar'd Sudget P~oerwork Reduction ficlect(0704.0188). NaShingion, DC 20503
1. AGENCY USE ONLY (Leave blank) 2. REPORT DATE 3. REPORT TYPE AND DATES COVERED
I April 1993 ITechnical Note4.TTLE AND SUBTITLE 5. FUNDING NUMBERS
On t M icle daa
6. AUTH4OR(S)
* R. E. Burr
7. PERFORMING ORGANIZATION NAME(S) AND ADDRESS(ES) B. PERFORMING ORGANIZATIONUS Army Research Institute of Environmental Medicine REPORT NUMBER
Kansas StreetNatick, MA 01760-5007
9. SPONSORINGý MONITORING AGENCY NAME(S) AND ADDRESS(ES) 10. SPONSORING /MONITORINGAGENCY REPORT NUMBER
Same as Block 7.
11. SUPPLEMENTARY NOTES
12a. DISTRIBUTION AVAILABILITY STATEMENT 121)b. DISTRIBUTION CODE
Approved for public release; distribution is unlimited. j____________13. ABSTRACT (Maximum 200 words)
Soldiers engaged in military operations in cold weather are at risk of cold weatherinjuries and illnesses. This technical note reviews the physiology of coldexposure, the prevention of cold injuries, the medical management of cold injuriesand provides briefing points for medical personnel to use in training.
14. SUBJECT TERMS 15. NUMBER OF PAGESSubject terms: cold injuries, accidental hypothermia, frostbite, 60trench foot, prevention, nm'¶ical surveillance, medical opera- 16. PRICE CODE
tions, cold environments WU 12717. SECURITY CLASSIFICATION I18. SECURITY CLASSIFICATION 19. SECURITY CLASSIFICATION 20. LIMITATION OF ABSTRACT
OF REPORT I OF THIS PAGE I OF ABSTRACTUnclassified Unclassified I Unclassified
NSN 7540-01 -280-5500 Standard Forti 298 (Rev 2-89)0-% bed bit 4Wt rtd '1.If$ U2

Approved for public release ADDistribution unlimited
TECHNICAL NOTENO. 93-4
MEDICAL ASPECTS OF COLDWEATHER OPERATIONS:
A HANDBOOK FOR MEDICAL OFFICERS
Prepared by
Robert E. Burr, LTC, MC, USA
March 1993
US Army Research Institute of Environmental MedicineNatick, Massachusetts 01760-50007

Table of ContentsPage
Acknowledgements ................. ....................... 1
Preface ...................... ............................ 2
Introduction ................... ......................... 3
Section 1. Physiologic Effects of Cold Exposure .... ....... 4
1.1 Heat Balance and Core Temperature ....... .......... 4
1.2 The Acute Response to Cold Exposure ..... ......... 5
1.3 Cold-Induced Vasodilation (CIVD) .................. 7
1.4 Human Adaptation to Cold .......................... 7
Section 2. Prevention of Illness and Injury in the Cold . . . 8
2.1 Preventing Cold Injuries:Role of the Medical Officer ..... ...............
2.2 Advice for the Commander .......................... 8
2.2.1 Soldier-Related Risk Factors ..... ......... 8
2.2.2 Environmental Risk Factors ....... .......... 9
2.2.3 Mission-Related Risk Factors ..... ........ 10
2.3 Training ................. ..................... 10
2.4 Medical Surveillance ........ ............... .. 12
2.5 Sustaining Health and Performance ... ......... ... 13
2.5.1 Medical Predeployment Preparation ..... ... 13
2.5.2 Nutrition .......... ................. ... 14
2.5.3 Hydration .......... ................. ... 14
2.6 Medical Soldiers Are Role Models ... ......... ... 15
2.7 Prevention of Illness and Injury from Other Hazards 15
2.7.1 Traumatic Injury and Falls ... ......... ... 15
2.7.2 Carbon Monoxide, Fires and Fumes ........ .. 15
i
2.7.3 Crowding and Infection .... ........... ... 16
2.7.4 Sun Exposure ......... ................ ... 16
2.7.5 Contact Freezing Injuries ... ......... ... 16
2.7.6 Alcohol ............ .................. ... 17
2.8 BE ALERT! .............. ..................... ... 17
Section 3. Illness and Injury Due to Cold ... ......... ... 18
3.1 Introduction ............ ................... ... 18
3.2 Freezing Injury (Frostbite) ..... ............ .. 18
3.2.1 Pathogenesis of Freezing Injuries ... ..... 19
3.2.2 Clinical Manifestations and Classification 19
3.2.3 First Aid and Field Management .... ....... 21
3.2.4 Hospital Management ...... ............ .. 22
3.2.5 Return to Duty and Physical Profiling . 25
3.3 Non-Freezing Cold Injury (NFCI) .... .......... .. 25
3.3.1 Pathogenesis ............. ................ 26
3.3.2 Clinical Manifestations .... .......... .. 26
3.3.3 Classification ....... ............... ... 27
3.3.4 First Aid and Field Management .... ....... 28
3.3.5 Hospital Management ...... ............ .. 29
3.3.6 Return to Duty and Physical Profiling . 30
3.4 Accidental Hypothermia ....... ............... .. 30
3.4.1 Pathophysiology of Hypothermia .... ....... 30
3.4.2 Accidental Hypothermia .... ........... ... 31
3.4.3 Clinical Manifestations of Hypothermia . 33
3.4.4 First Aid and Field Management of AccidentalHypothermia .............. ................ 33
3.4.5 Cardiopulmonary Resuscitation (CPR) . ... 34
ii
3.4.6 Sudden Death in Accidental Hypothermia . 36
3.4.7 Hospital Management ...... ............ .. 37
3.4.8 Return to Duty and Physical Profiling . 40
3.5 Other Medical Problems in Cold Environments . ... 41
3.5.1 Carbon Monoxide (CO) Poisoning ......... ... 41
3.5.2 Respiratory Tract Conditions ..... ........ 42
3.5.3 Cold Urticaria ....... ............... .. 42
3.5.4 Chilblains (Pernio) ....... ............ .. 43
3.5.5 Solar Keratitis (Snow Blindness) and Sunburn 43
3.5.6 Eczema (Winter Itch, "Eczema Craquele") 44
3.5.7 Lacerations ............................ .. 44
3.5.8 Intolerance of Cold Exposure ..... ........ 44
Section 4. Key Points and Reminders ...... ............ .. 45
4.1 Useful points to remember ..... ............. ... 45
4.2 Prevention .............. .................... .. 45
4.3 Rescue and Evacuation ....... ............... .. 46
4.4 Medical Operations in the Cold .... .......... .. 47
Appendices .................. ......................... .. 49
Appendix A: Wind Chill Chart ....... .............. .. 50
Appendix B: Cold Weather Training Guidelines .... ...... 52
Appendix C: Clinical Manifestations of Hypothermia . 54
References .................. ......................... .. 55
Bibliography ...... ................. ......... ___2_ 56Aooession For
NTIC TA&DTIC C...'i.•r~~ ...... DTIJ' T-':
By
iii Dist ributiton/Availatllity Cod-os
IAvail and/orDist Speolal
AcknowedgementsIn the preparation of this handbook, the author has had the
benefit of the unstinting help of a number of individuals.
First and foremost, COL Gerald Krueger, the USARIEMCommander, who originated the concept of an environmentalmedicine handbook series, has given continuous support, carefuland thorough editorial review and exhortation during every phaseof the preparation of this handbook. This handbook would notexist without his guidance and determination.
LTC Paul Rock, Dr. Andy Young and MAJ Sven Ljaamo of theUSARIEM staff contributed substantially to the content andorganization of the handbook with their several careful andcritical reviews. Dr. Don Roberts, LTC Katy Reynolds, LTCWilliam Curtis, MAJ Paul Amoroso, MAJ Marc Eisenmann, MAJ HaryModrow, CPT Barry Bickley and CPT Peter Boosalis providedadditional scientific, medical and practical review andcriticism. The USARIEM Technical Editor, Ms. Eileen Collins,reviewed many drafts, each time with care and patience, andprovided invaluable assistance with the references andbibliography.
The inprovement and evolution of the manuscript through itsmany drafts is due in large part to the conscientious andgenerous help of all these individuals. Whatever weaknessesremain are solely the responsibility of the author.
Robert E. BurrMedical AdvisorU. S. Army Research Institute of
Environmental Medicine
Si i i ii i1

Preface
This handbook is one of a series prepared at the U.S. ArmyResearch Institute of Environmental Medicine (USARIEM) formedical officers supporting units operating and training in harshclimatic conditions. It is intended for health care personnel asa review of those aspects of military medicine important for coldweather operations.
In addition to this medical handbook, USARIEM has preparedanother: Sustainina Health and Performance in the Cold: Environ-mental Medicine Guidance for Cold Weather Operations intended forall personnel, medical and non-medical, who may have to deploy tocold regions. This handbook is available in two formats, 8.5 x11 (USARIEM Technical Note 92-2, DTIC No. AD A254-328) and pocketsize (USARIEM Technical Note 93-2, DTIC No. AD A259-920). Thetwo handbooks are complementary. We believe medical personnelwill find useful information in both.
Most current practice in the management of illness andinjury due to cold exposure depends on limited clinical seriesand personal anecdote. It has little basis in modern clinicalinvestigation. To address the need for new contributions, wewelcome advice, anecdote, opinion, correction and clarification.
Correspondence concerning this handbook should be directedto:
ComnanderU.S. Army Research Institute of Environmental MedicineATTN: SGRD-UE-ZMKansas St.Natick, MA 0176G-3007
USARIEM POC is Medical Advisor at DSN 256-5059 (Commercial508-651-5059) or Telefax 256-5298.
The material in this handbook should not be taken to bedoctrinal guidance of either the Department of Defense,the U.S. Army or the U.S. Army Medical Department,unless so designated by appropriate authority.
2
Introduction
Of all the natural environmental hazards soldiers confrontin the course of their duties, cold is arguably the most diffi-cult and dangerous. Every medical officer has heard of the cata-strophic withdrawal of Napoleon's Grand Army from Moscow in thewinter of 1807 during which illness and injury due to cold causedthe death of thousands of French troops.
Casualties from cold exposure occur in all types of opera-tions. Cold is an effective weapon on the side of a militaryforce with initiative. Forces including the U.S. Cavalry, theRussians and the Finns used cold in this way by displacing theiropponent from shelter and allowing the environment itself toforce surrender. In the offense, rapid paced operations canoutrun supply trains and expose leading elements to unexpectedcold weather bivouacs and risk of cold injury.
It should not be surprising that the U.S. Army suffered coldweather casualties in almost all of our conflicts from theAmerican Revolution to Korea. Cold injuries remain a problem inmilitary operations and training exercises today (Barat, A.K.,Puri, H.C., Ray, N., 1978; Marsh. A.R., 1983; Orr, K.D. andFainer, D., 1952; Tek, D. and Mackey, S., 1993).
Because the U.S. Army is evolving into a CONUS-based rapiddeployment force, U. S. Army Medical Department officers must beprepared to assist commnanders to deal with any deploymentcontingency. Many cold regions throughout the world are poten-tial deployment destinations for the U.S. Army. This handbookwas written to help medical officers prepare for, and manage themedical needs of units confronted by deployment and operations incold environments.
This handbook is divided into four sections. The firstsection is a review of human physiologic and pathophysiologicreactions to cold. The second is an approach to the preventionof illness and injury during operations in the cold. The thirdis a clinical review, from the military medical perspective, ofthe presentation and management of the various forms of illnessand injury caused by cold exposure. Tho fourth sectionsummarizes particularly important or useful points to allow easyextraction for training.
3
Section 1.
Physiologic Effects of Cold Exposure
1.1 Heat Balance and Core Temperature
Humans require that the body core temperature stay withinnarrow limits for optimum functioning. Even small (2-3 0F) devia-tions frcm the average 990F (370C) temperature will impair physi-cal and mental performance.
Core temperature stability is maintained by balancing heatgain from the environment and metabolism with heat loss. If, onaverage, the two are equal, core temperature will remain con-stant, permitting optimum function. If heat gain exceeds heatloss, core temperature rises; conversely, if heat loss exceedsheat gain, core temperature will fall.
Heat balance can be expressed algebraically in the followingway: S=M±R±C-E
where: S = net change in heat content.
M = metabolic heat production; always positive.
R = radiation.
C = conduction/convection.
E = evaporation, always negative.
Metabolic heat production (M) varies with activity. Onaverage, an adult male at rest generates about 80-90 Cal per hour(roughly equivalent to a 100 W bulb). Maximum aerobic exerciseincreases metabolic heat production to about 10 times the restingrate (about 1000 Cal per hour) and can be sustained by mostindividuals for only brief periods. Individuals performingsustained hard physical work (digging, marching under a load) whocan control the rate of exertion will usually work at about 4-5times the resting metabolic rate. For comparison, shivering canincrease metabolic rate up to six times resting level.
4

Radiation (R) is the loss or gain of heat in the form ofelectromagnetic energy. The direction of heat energy transfer isfrom warmer to cooler objects. The warming we sense standing indirect sun or near a hot surface is produced by radiative heatgain. As "warm-blooded" mammals, in a cold environment, we arerelatively warm objects, and, so, radit, e heat energy. Radiantheat gain and loss can be moderated by material barriers whichare considered either "shade" or "insulation" depending on thedliect Ln of the radiant heat energy flow.
Conduction and convection (C) are the mechanisms of heatenergy transfer due to physical contact between two materials ofdifferent temperatures. Conductive heat transfer occurs when onematerial warms another adjacent material. Conductive bodily heatgain or loss is particularly significant when lying on hot orcold ground. If one of the materials is a fluid (water or air).then convection can occur which moves the warmed fluid away andreplaces it with unwarmed fluid sustaining the temperaturedifferential and conductive cooling. Wind increases convectionand is responsible for the greater apparent coldness of movingair. Convection is also an important component of cooling duringcold water inmmersion.
Evaporation (E) of sweat causes heat loss. Each liter ofsweat evaporated transfers 540 Cal to the environment. Sweatevaporation does NOT depend on the relative humidity, but ratherupon the difference between the vapor pressure of sweat on theskin and the vapor pressure of water in the air adjacent to theskin. Even in cool-wet environments of high relative humidity,sweat on warm skin can evaporate into the air because the vaporpressure of the sweat exceeds that of the water vapor in the airthat has been warmed by contact with skin. Sweating in the coldis an important form of heat loss.
1.2 The Acute Response to Cold Exposure
Humans have evolved two physiologic mechanisms to maintaincore temperature during cold exposure: 1) reducing skin temper-ature which reduces the differential between the skin temperatureand the environment and slows heat loss and 2) increasing heatproduction by shivering.
When the body is exposed to cold, blood is diverted awayfrom skin and extremities to the trunk by vasoconstriction.Consequently, a layer of relatively hypoperfused tissue is formedbetween the environment and the viscera. Deprived of the heatfrom the metabolically active core, this "shell" of tissue cools,thereby reducing the gradients for heat loss from the skinsurface by radiation, conduction and evaporation. This tissueinsulation has been estimated to be about the same as thatprovided by wearing a light business suit. In contrast, heavy
5
arctic clothing provides six to eight times as much insulation.
The diversion of blood away from the skin and extremities iscaused by arteriolar and venous vasoconstriction mediated by bothcutaneous and central temperature responsive reflexes. Directcooling of the skin or the core causes generalized cutaneousvasoconstriction. Central and peripheral receptors act synergis-tically, so, the degree of vasoconstriction depends on both skinand core body Cemperature. The lower the core temperature, themore intense and generalized the vasoconstriction.
Skin cold sensory receptors respond both to absolutetemperature and the rate of temperature change. Consequently,sudden exposure tc cold, such as walking from a warm buildinginto a cold wind, will trigger an acute response with vasocon-striction and even transient shivering. (Who hasn't experiencedthe brief frisson of shivering when going out into the cold?) Ascold exposure continues, the skin equilibrates at a new coldertemperature. As skin temperature stops changing, the response tothe cold stimulus wcierates and the acute shivering passes. Theskin gradually (over a period of two to three hours) acconrmnodatesto the cold and the sensation of cold becomes less uncomfortable.Conversely, if cold skin is warmed, the reflex response canproduce moderation of the insulating vasoconstrictive responseand increase heat loss from skin and extremities.
As a consequence of reducing blood flow and volume in skinand extremities, peripheral vasoconstriction causes an expansionin central blood volume. Although the effect is antagonized byipright posture, the expanded central volume can produce "colddiuresis." Cold diuresis can contribute to dehydration duringprolonged cold exposure, and particularly, to hypovolemia invictims of accidental hypothermia and irmmersion.
If the insulating effect of vasoconstriction is insufficientto protect the core temperature, the continuing fall in tempera-ture triggers the onset of heat production by muscle. Initially,muscle tone increases, which increases metabolic rate twofold.However, if temperature falls further, the muscular activitychanges to cycles of contraction and relaxation, producir4visible shivering. The core temperature at which maxima- shiver-ing develops differs among indiv:duals, but is almost alwaysbetween 94 and 970F. Maximal shivering increases heat productionto six times the resting level. Shivering, although an importantmechanism of emergency metabolic heat production in the cold, issustained only at considerable cost. First, it disables byinterfering with purposeful, coordinated muscular activity.Second, the increased muscular activity requires an increase inextremity blood flow, which diminishes the iisulating effect ofvasoconstriction.
6

1.3 Cold Induced Vasodilation (CIVD)Although vasoconstriction is beneficial and protects core
temperature, because it reduces the flow of blood from the coreto the periphery, it places the metabolically inactive acralregions of the body at risk of severe cooling and injury. "Coldinduced vasodilation" is a physiologic mechanism that appears toreduce the risk of injury when the hands or feet are exposed towater below 500F and air below 320F.
As the hands or feet cool, vasoconstriction initiallyreduces blood flow and volume. After a few minutes of lowdigital tenperature, arteriovenous anastomoses in the distalphalanx open and allow a rapid increase in digital blood flow (bybypassing the constricted precapillary arterioles). While thearteriovenous anastonoses remain open, the digits remain warm.The phenomenon is usually cyclic, producing alternating periodsof vasoconstriction and vasodilation 10-20 minutes long.Individuals vary in the magnitude of their CIVD response. Occa-sionally, individuals will sustain CIVD without cyclicity; otherindividuals have very limited CIVD and seem to have poor coldtolerance.
The magnitude and duration of the CIVD are dependent on coretemperature. When core temperature is low, the phenomenon issubstantially less prominent and, presumably, affords lessprotection to the hands and feet from cold injury.
Unless a fall in core temperature inhibits CIVD, it will in-crease heat loss, particularly in cold water. Loss rates of 40Cal per hour have been reported.
1.4 Human Adaptation to Cold.
Although apparently adaptive changes in metabolic rate, coretemperature, shivering threshold, vasoconstriction and CIVD havebeen demonstrated in experimental cold exposures, the magnitudeof these effects is small. Physiological adaptation to cold isnot a phenomenon of the same significance as adaptation to heator high altitude. Indeed, the successful use of clothing andshelter in cold environments prevents much of the cold stressthat might induce adaptation or habituation. Consequently, thereappears to be no practical means of significantly enhancingphysiological cold tolerance through training or predeploymentexercises.
Some canponent of the cold tolerance seen in soldiers duringcold weather exercises may be due to physiologic change, but,familiarization and skill-development are at least as importantto maintaining their well-being.
7

Section 2.
Prevention of Illness and Injury in theCold
2.1 Preventing Cold Injuries: Role of the Medical Officer.
Commanders are responsible for the prevention of cold injuryin their units. They take this responsibility seriously, butneed constructive advice from their medical staff to developeffective preventive measures compatible with mission accomplish-ment. Commanders, not medical officers, control the exposure ofsoldiers to cold. The principal role of the medical officer inthe prevention of injury is to advise his/her commander and unit,train unit leaders and members, and conduct injury surveillance.
2.2 Advice for the Commander.
During operations planning, medical officers have the wide-ranging responsibility of preparing analyses, recommendations andplans for the entire spectrum of health service support. Part ofthat responsibility consists of considering the risks due to theenviron.ent, recommending countermeasures to reduce the risk ofenvironmental injury and preserving the health and performance ofthe unit.
It is useful to analyze the risk of environmental injury asan interaction of three components: the soldier, the environmentand the mission. Each component has unique risk factors whichmust be assessed and controlled.
A careful consideration of the three risk components ofenvironmental injury will assist the medical officer in thepreparation of the health service estimate which should containrecomnmendations and plans to reduce injury risk. Since most ofthe conmonents of risk can be modified, explicit consideration ofeach risk conponent will allow the implementation of counter-measures to preserve the health of the unit.
2..1 Soldier-Related Risk Factors
Characteristics of soldiers that are generally accepted tobe risk factors for cold injury include: fatigue, dehydration,
8
undernutrition, lack of cold weather training and experience,lower rank, black race and tobacco use. The degree to whichthese factors are present in a unit will vary depending on thecomposition and circumstances of the unit. The medical officermust be completely familiar with the unit and monitor itcarefully in order to judge when particular risk factors are ofsufficient magnitude to require control measures.
Some of the soldier-related risk factors for cold injury arecommon consequences of operating in the field. Soldier fatigue,undernutrition and dehydration are encountered in every deploy-ment. These risk factors are controlled by ensuring commandattention to scheduled rest periods, complete consumption ofrations and enforced hydration. Nutrition and hydration areconsidered in more detail in 2.5.2 and 2.5.3.
With all the other training and readiness demands, unitsthat do not routinely train in cold environments will have feweropportunities to maintain or develop their cold-weather skills.Before operatinq in the cold, military units should plan toacquire appropriate skills and equipment. Units that trainregularly in the cold should ensure that new members of the unitare given individual cold-weather training and equipment to allowthem to function safely in the field.
Soldiers at particular risk of cold injury are: 1) those oflower rank who are exposed to cold most, 2) those with blackskin, which seems more susceptible to cold injury than white skinand 3) those who use tobacco, which vasoconstricts and may limitthe protective vascular response to cold. Unit leaders must beaware of the increased risk to these individuals and monitor themduring cold exposure.
2.2.2 Environmental Risk Factors
Cold environments are dangerous; however, with the oneexception of the Wind-Chill Index, the risks have been hard toexpress quantitatively. The medical officer must remain aware ofthe current and forecast conditions to enable him to estimaterisk of exposure and recommnend countermeasures.
Cold exposure can occur on land, in water or in aircraft.Cold land environments are generally classified as either wet-cold or dry-cold. Wet-cold environments have ambienttemperatures above freezing to about 60OF (16°C) with wetnessranging from fog to heavy rain. They are associated with non-freezing peripheral injuries, such as trench foot. Usually, manyhours to days of exposure are required to cause injury. Dry-coldenvironments have ambient temperatures below freezing(32 0F, 00C). Precipitation, if present, is in the form of drysnow. Dry-cold environments are associated with freezing
9
peripheral injuries, which can develop in a few minutes to hours.Aircrew exposed to the airstream around a flying aircraft throughan open hatch or port in the fuselage risk severe dry-coldexposure and can incur serious freezing injuries in seconds.
Accidental hypothermia can occur in any cold environment,water, wet-cold or dry-cold.
A quantitative index of risk to exposed skin, the "Wind-Chill Index", has been developed as an inportant tool for judgingenvironmental risk. A Wind Chill Table is included in thishandbook as Appendix A. It is important to remember the WindChill Index does not provide an index of hypothermic risk or ofrisk to covered skin. Effective cover will protect skin even inconditions of very "cold" wind-chill.
Changing weather conditions are associated with an increasedrisk of cold injury. Exhaustion hypothermia classically occurswhen individuals are caught in unexpected rain or snow. They mayhave to bivouac without adequate shelter or become lost ordelayed in cross-country movement, any of which leads toprolonged cold exposure. Freezing injuries commonly occur at theconclusion of a period of bitter cold when the slightly warmer,but still cold, temperatures do not produce their usual sensationof cold.
Z23 IEssloneateW Msk Factors
The mission will determine the exposure of soldiers to theenvironment and is an important component of the environmentalinjury risk. Risk factors associated with the mission include:prolonged cold exposure, hasty preparation, limited resupply andinadequate equipment.
Mission-related operations should be planned to protectsoldiers against environmental injury. In the cold, operationalplans should provide for adequate resupply of water, food and dryclothing. Cperational schedules must take into account thedifficulties of movement in the cold and provide for adequateopportunities for rewarming, rest and foot care. The possibilityof weather change should be anticipated and appropriate alterna-tives planned.
2.3 Training.Successful injury prevention ultimately rests on the skill
and knowledge of the soldiers conducting operations in coldenvironments. The medical officer is responsible for providingsome of that skill and knowledge, which addresses the cause,prevention, recognition and first aid of cold injury. Othermembers of the unit will be responsible for providing training on
10

cold weather survival, use of equipment and unit procedures inthe cold. The medical officer needs to provide his medicaltraining for three groups in the unit: unit medics, unit leadersand the soldiers themselves.
The unit medics should be thoroughly trained in the signs,symptoms, prevention and management of cold injuries and how tosurvey aggressively for illness and injury. They must understandthat early recognition of cold injuries is essential to minimizethe severity of the injury and to reduce the number of soldiersaffected. In addition to their usual medical supplies, theirmedical support plan should include adequate equipment to protectcasualties from the cold during evacuation.
Unit leaders should understand the causes and manifestationsof cold injury, both for their own benefit and that of theirsoldiers. They should understand that cold injury is insidious,that affected soldiers are often unaware of their injury and thatcold can adversely affect performance. They should understand theimportance of potable water, adequate rations, the "buddy" systemand cold weather clothing on preserving unit function in thefield. They should understand the importance of adequatepredeployment preparation for cold by conducting cold weathertraining, cold weather clothing and equipment inspections andassuring appropriate health maintenance and medical screeningmeasures. The USARIEM handbook "Sustaining Health and Perfor-mance in the Cold" is intended for small unit leaders and can beused both as a training aid and field guidance.
Leaders should understand the importance of adequatemateriel support in cold weather operations. Functional coldweather clothing, particularly dry warm socks, cold weatherfootwear and underwear are essential for adequate cold weatherprotection. Opportunities for exchange or cleaning and dryingsocks and underwear are essential. A supply of cold weatherboots must be available to replace immediately boots that becomedefective. If long intervals between resupply are anticipated,adequate supplies of these items must be included in the initialunit issue.
The most important control measure for preventing coldinjury during cold exposure is the provision of adequate time andfacilities for rest, rewarming and inspection of the face andextremities. The interval between rest and rewarming should bedetermined by the immediate circumstances of the unit and may beas frequent as every 20 or 30 minutes in very cold weather.
Soldiers should know the signs and symptoms of cold injuryin themselves and their buddy, and know what to do if theysuspect a medical problem. They should be alert to theconsequences of dehydration, undernutrition, fatigue and alcohol.
11
They should understand the importance and the techniques for footcare in the cold.
Effective techniques have been developed for preventing coldinjury in the lower extremities. Soldiers should be trained inthese techniques and leaders should understand the importance ofassuring that they are carried out when soldiers are exposed tocold. They are summarized below:
1. Assure the best possible fit of the boots with heavysocks.
2. Keep the body as warm as possible; avoid chilling.
3. Remove boots and socks at least twice a day; three timesis better. Wash, dry, massage and move the feet to restorecirculation and feeling. Allow enough time and provideappropriate shelter to complete this task. After massaging andwarming the feet, put on clean, dry socks, or, if dry socks arenot available, remove as much water from the wet socks aspossible before putting them back on.
4. Do not sleep with wet footgear. Remove wet boots andsocks for sleep. Protect the feet with as much dry cover aspossible to keep them warm.
5. Dry wet socks by keeping them in the sleeping bag duringsleep, or placing them inside the field jacket against the chestor across the shoulders.
6. In fixed positions, stand on rocks, boards or brush tokeep the feet out of water and mud.
7. Keep the feet and legs moving to stimulate warmingcirculation. Instead of crouching all the time to keep low in afixed position, try to sit or lie back periodically with the feetslightly elevated to reduce swelling of the feet and ankles.
8. Watch carefully for numbness or tingling. These areearly symptoms of injury. If these develop, immediately takemeasures to warm the feet.
9. Keep the clothing and footgear loose enough to permiteasy circulation.
2.4 Medical Surveillance.
Medical surveillance of the unit is the third component ofthe medical officer's role in preventing cold injuries. The goalof surveillance is 1) to identify risk factors for illness or
12
injury to permit preventive intervention and 2) detect illnessand injury as early as possible to allow interruption of thedisease process.
The medical officer should implement a formal medical sur-veillance plan tailored to the needs and mission of the unit.The surveillance is intended to monitor selected informationabout the health of the unit in order to detect emerging riskfactors and early manifestations of illness and injury.
A medical surveillance plan to support a program of coldinjury prevention starts before deployment by assuring that allmembers of the unit are optimally prepared for cold exposure.The plan should periodically assess the following medical data onall unit members: immunization status, past history of coldinjury and current coincident or cold-related illnesses. Amedical record review is important to identify individuals'coincidental medical condition that increase the risk of coldinjury. Examples of these latter conditions are Raynaud'sDisease or diabetes mellitus.
In the field, medical surveillance should assess frequently:hydration, fatigue, nutrition, coincident illnesses and theintensity of cold exposure. Cold injuries should be reportedimmediately and the circumstances of the injury determined.Inspection of unit work schedules for adequate rest periods,morning urine checks for hydration, and inspection for discardedrations can provide evidence of fatigue, dehydration orundernutrition.
Medical surveillance should be performed in an organizedfashion by all members of the health service support team.Regular written reports are an essential part of the disciplinethat successful medical surveillance requires. Without organizeddata collection, surveillance becomes anecdotal and loses asignificant amount of its sensitivity for early detection andsuccessful intervention.
2.5 Sustaining Health and Performance.
Predeployment immunization, nutrition and hydration arecritically important to preserving health in cold environments.Each is reviewed in more detail below.
2.5.1 Medical Prdpogymnt Preparation
The unit should have received appropriate immunization andprophylaxis. Influenza and tetanus vaccinations are particularlyimportant preparations for cold weather operations. In somecases, some soldiers may benefit from pneumonia vaccination. If
13
the unit has been exposed to streptococcal infection, bicillinprophylaxis should be provided.
Unit members who develop conditions that increase their risk ofcold injury should be formally evaluated for deployability.Medical conditions that are considered to increase the risk ofcold injury are: a history of prior cold injury, Raynaud'sphenomenon or Raynaud's disease, obstructive vasculopathies(venous and arterial), chronic pulmonary disease and peripheralneuropathies.
Z&2 N•fion
Maintaining nutrition is a difficult challenge in the field.Appetite and food intake decreases in the field, while energyrequirements increase. Voluntary undereating for weight control,dehydration, cold rations and unpredictable meal schedulescompound the problem. Consequently, weight losses of two tothree pounds per week are common for the first few weeks of acold weather deployment.
Countering the propensity to weight loss requires thatsoldiers eat sufficient rations to provide 4,000 to 5,000 Cal perday. Command emphasis on complete ration consumption isrequirea. F.uviding warm rations (A's or B's) at least once aday and a warm drink at each meal will enhance food consumption.A modified MRE ration specifically tailored to support coldweather operations (Ration - Cold Weather) has been developedand, if available, should be used when units cannot be provideddaily "A", "B" or "T" rations.
2.5.3 Hydration
Maintaining hydration is as difficult and important asmaintaining food intake. A number of factors contribute todehydration. In the field, soldierS exhibit voluntarydehydration, which is a moderate degree of dehydration (2% belownormal) that seems insufficient to trigger thirst. In addition,despite thirst, soldiers may further restrict water intake toreduce the need for urination in the cold. Since most water istaken with meals and is related to the amount of food eaten,incomplete consumption of rations tends to reduce water intake.The logistic problems of providing potable liquid water in thecold often restrict supply. Even if water is freely available,it is often cold and unpalatable.
Water requirements in the cold are high. Cold air is dryand increases respiratory losses. High work rates required incold weather operations increase water requirements. All thisadds to the dehydration due to restricted water intake.
14

Soldiers require a minimum of four quarts of liquid per dayto assure adequate hydration. The effort to supply water in acold environment req-'4res the same attention as water supply inthe desert. Once adequate water is provided, unit leaders mustensure that it is consumed. Squad leaders should check urinecolor daily to detect dehydration early and to emphasize thecomriander's concern about adequate hydration. Comnand directeddrinking may be required.
2.6 Medical Soldiers Are Role Models.
Soldiers will watch their medics to see if they put intopractice what has been provided in the unit's cold weathermedical training. The medical officer should assure that themedics understand that they will provide an important example tothe rest of the unit and that their behavior can either reinforceor weaken the training which the unit has received in sound coldweather preventive practice.
2.7 Prevention of Illness and Injury from Other Hazards.
Cold environments present hazards other than that of coldexposure such as: icy surfaces, long hours of darkness, openflame heating equipment and heavy clothing. The medical officermust be as vigilant to these other hazards as to cold itself.Several of these hazards and measures to control them are brieflyreviewed in this section.
2.7.1 Traumatic Injury and Falls
Wet or icy surfaces, long hours of darkness and heavy cloth-ing combine to make work and movement slow, difficult anduncertain and increase the risk of falling. Darkness and snowconceal trip and fall hazards during cross-country movement.Vehicles are more difficult to control in ice, snow and Tud.Their direction of travel is less predictable for both driver andpedestrian, increasing the risk of accident.
Control measures include 1) careful preparation, maintenanceand marking of paths, roads and load-handling areas, 2)separation of pedestrian and vehicular traffic, 3) one-wayvehicular traffic, 4) extra help for work-details and 5) work-area illumination.
2.7.2 Carbon Monoxide, Fires and Fumes
Fuel-fired heaters are ubiquitous equipment in coldenvironments and create a risk of carbon monoxide (CO) poisoning,burns, eye injuries and tent fires. In the cold, motor vehiclesare kept running for long periods, and are often close to troop
15
bivouacs. Soldiers sleeping in or near running vehicles are atrisk of CO poisoning.
Control measures include unrelenting attention to trainingsoldiers in the operation and maintenance of heaters, mandatoryfirewatch, placement of vehicle areas downwind from bivouacs andprohibition of sleeping in operating vehicles.
2.7.3 Crovwing and Infection
Soldiers sleeping in close, poorly ventilated quartersprovide an environment for the rapid dissemination of respiratoryillness. Viral and streptococcal respiratory infections areparticular hazards.
Control measures include appropriate predeploymentimrunization and prophylaxis, early detection of respiratoryinfection by examination and culture, head-to-toe sleeping, andadequate ventilation.
2.7.4 Sun Exposure
Sunlight, particularly when reflected off snow and ice, canproduce serious burns to exposed skin and eyes from its ultravio-et component. The risk of burns is increased in moderate
weather or at high altitude because the warming effect of the sunis particularly noticeable and inviting in these circumstances.
Solar keratitis (snow blindness) is profoundly disabling.Affected soldiers' vision is blocked or restricted for two orthree days by required protective eye covering and eye pain mayproduce substantial discomfort. They may not be able to toleratefull sun exposure for several days after the injury.
Sunburn is not a minor problem! It can prevent the wearingof cold weather uniform items, and consequently, significantlylimit availability for normal duty.
Control measures include clothing and sunscreen to protectskin, and sunglasses to protect the eyes. If sunglasses are notavailable, opaque eye covering (e.g., tape-covered eyeglasses)with narrow horizontal slits provide adequate field expedient eyeprotection.
2.7.5 Contact Freezing Injuries
In the cold, all materials in the environment should beconsidered to be at the ambient temperature. If cold materielcomes in contact with unprotected skin, it can produce localfrostbite in seconds. Particular hazards are: 1) vehicles (doorhandles, steering wheels), 2) metal surfaces (utility poles,
16

armored vehicles, weapons), 3) POL, antifreeze and alcohol (thesecan be liquid at temperatures many degrees below zero. Splasheson skin or mucous membrane can produce inmmediate severe injury)and 4) ice and snow.
Alcohol consumption increases the risk of all forms ofillness and injury in the cold. It inpairs judgement and coordi-nation which increases the risk of traumatic injury. Itshypnotic effect reduces the alertness to fire and carbon monoxidepoisoning. Alcohol increases the risk of hypothermia and frost-bite by a combination of effects: impaired self-protectivebehavior, reduced shivering and heat generation, reduced pain ofcold exposure, dehydration from diuresis and inhibited gluco-neogenesis.
There are no known beneficial effects of alcohol in theprevention or management of cold injury.
2.8 BE ALERT!Responses to operational contingencies will generate new
hazards. For example, during one winter exercise, whenunexpected subfreezing temperatures developed, soldiers trainingto conduct mass decontamination responded by preparing a field-expedient freeze-resistant shower solution by adding ANTIFREEZE.Only the last minute recognition that this shower solution wasnow actually below freezing itself prevented a large number ofacute cold injuries.
17

Section 3.
Illness and Injury Due to Cold
3.1 Introduction.
The following sections describe injuries and illnesses dueto cold exposure. Sections 3.2, 3.3 and 3.4 follow the tradi-tional classification of these conditions into peripheralinjuries of the freezing (3.2) and non-freezing types (3.3) andthe systemic injury of accidental hypothermia (3.4). Section 3.5discusses a variety of other medical conditions that commonlyoccur during military operations or training in the cold.
3.2 Freezing Injury (Frostbite).
Frostbite is currently the most common cold-induced injuryencountered in the U.S.Ar"y. It is endemic at a low rate in coldenvironments. Isolated episodes are usually associated with anepisode of carelessness or sudden weather change. Clusters offrostbite injuries occur in exercises and operations, frequentlythe result of poor planning or inattention to control measures.Fortunately, most frostbite injuries occurring during trainingare of low degree of severity and do not usually result inpermanent tissue loss. However, the prolonged recovery usuallymeans the loss of the injured soldier to field duties for theremainder of the cold season. In cold regions this can meanmonths of limited duty. For that reason, a unit that suffers acluster of freezing injuries may become ineffective.
Remember that freezing injuries are preventable. Preventionis a ccmmand responsibility that depends on advice, training andsurveillance by unit medical personnel (see Section 2).
Most freezing injuries occur in the field, consequently, themedical officer is often the last person to see and managefrostbite injuries. Most freezing injuries will be recognizedand initially managed by unit medics and other non-physicianmedical providers. Because the outcome of the frostbite dependson early detection and management, the medical officer mustassure that the unit medics are well trained in the recognitionand management of these injuries.
18

3.Z1 Pathogenesis of Freezing Inuies
Frostbite injury results when tissue is cooled sufficientlyto freeze. Tissues with large surface to mass ratios (ears) orwith restricted circulation (hands and feet) are particularlysusceptible to freezing. However, any tissue exposed to severecold can freeze.
Tissue does not freeze at 32°F; the high concentration ofelectrolytes and other solutes prevents freezing until tissue iscooled below 28 0F. At that point, ice crystals form whichsegregate some tissue water and cause concentration of theremainder into a progressively more hypertonic and harmfulsolution. Once solidly frozen, tissue injury is probablyarrested. Additional injury to frozen tissue occurs during andafter thawing, probably in two phases. First, upon restorationof blood flow, reperfusion tissue injury occurs. Second, markedendothelial swelling develops in the thawed tissue causinpsecondary loss of perfusion, ischemia and infarction of tissue.Despite freezing and reperfusion injury, some frostbitten tissueis able to recover. However, refreezing of injured tissue causesirredeemable injury, a phenomenon used therapeutically in cryo-surgery.
Pigmented cells seem to have greater susceptibility tofreezing than non-pigmented cells. The mechanism is not knownbut may be related to lower cytoskeletal tolerance to cold inpigmented cells (Post, P.W., Daniels, F. Jr. and Binford, R.T.Jr., 1975). To some extent, the higher incidence of freezinginjury among Afro-American soldiers may be explained by thisphenomenon.
3.2 Clinical Manifestations and Classmification
Initially, all frozen tissue has the same appearance: cold,hard and bloodless. Except in minor and severe cases, the degreeof injury will usually not beccme clear for 24-72 hours. Mostsignificant injuries include areas with different degrees offrostbite, usually more severe distally. Digits, ears andexposed facial skin are the most commnonly injured areas.
Frostbite is classified by depth of injury into four degreesof severity. The depth of the injury depends on the duration andintensity of the cold exposure. Very intense cold for a fewseconds will produce a superficial injury whereas prolongedmoderate freezing can freeze an entire extremity.
First dere frostbite is an epidermal injury. The affectedarea is usually limited in extent involving skin that has hadbrief contact with very cold air or metal (e.g., touching anoutside door handle). The frozen skin is initially a white or
19
yellow plaque. It thaws quickly becoming wheal-like, red andpainful. Since deep tissues are not frozen (though they may becold) mobility is normal. The affected area may become edematousbut does not blister. Desquamation of the frostbitten skin withcomplete clinical healing follows in 7-10 days.
Second degree frostbite involves the whole epidermis and mayalso affect superficial dermis. The initial frozen appearance isthe same as first degree injury. Since the freezing involvesdeeper layers and usually occurs in tissue with prolonged coldexposure, some limitation of motion is present early. Thawing israpid with return of mobility and appearance of pain in affectedareas. A bulla, with clear fluid, forms in the injured area overseveral hours after thawing. The blister fluid is extravasatedfrom the dermis. Usually, the upper layers of dermis are pre-served which permits rapid re-epithelialization after injury.Second degree injuries produce no permanent tissue loss. Healingis complete but takes three to four weeks. Some amount of firstdegree injury is frequently present in the immediate vicinity ofsecond degree frostbite. Frostbite should be looked for on allother exposed areas. Following second degree frostbite, coldsensitivity may persist in the injured area.
Third degree frostbite involves the dermis to at least thereticular layer. Initially, the frozen tissue is stiff andrestricts mobility. After thawing, mobility is restored briefly,but the affected skin swells rapidly and hemorrhagic bullaedevelop due to damage to the dermal vascular plexus. Theswelling restricts mobility. Significant skin loss followsslowly through mummification and sloughing. Healing is alsoslow, progressing from adjacent and residual underlying dermis.There may be slight permanent tissue loss. Residual coldsensitivity is common.
Fourth dearee frostbite involves the full thickness of theskin and underlying tissues, even including bone. Initially thefrozen tissue has no mobility. Thawing restores passivemobility, but intrinsic muscle function is lost. Skinreperfusion after thawing is poor. Bullae and edema do notdevelop. The affected area shows early necrotic change. Theinjury evolves slowly (weeks) to mummification, sloughing andautoanrputation. Whatever dermal healing occurs is from adjacentskin. Significant permanent anatomic and functional loss is therule.
Corneal frostbite is a rare, but profoundly disablinginjury. The evolution is similar to any deep ocular keratitis.Permanent corneal opacification requiring corneal transplant is acommon outcome.
20
3.2.3 First Aid and Field MIanagement
The first essential step in cold injury management isdetection. Frostbite injuries are insidious. Injured tissue,which was painful initially while getting cold, is anestheticwhen frozen and is often covered in a glove or boot. Detectionrequires direct inspection of at-risk tissue including the hands,feet, ears, nose and face.
When frostbite is suspected, the injured area must beimnmediately protected from further cold exposure and trauma bythe best available means. After protection is assured, adecision can be made regarding the method of warming.
It is important to remember that active warming of frozentissue should be deferred until there is no risk that the injuredtissue can be reexposed to freezing cold. Because refreezing ofa frostbite injury aggravates the injury so severely, currentpractice recorTnends that frozen parts not be actively rewarmeduntil protection from refreezing can be assured. Thisreco•Tnendation should NOT be interpreted to mean that the injuredpart should be deliberately kept frozen by packing in snow orcontinued cold exposure. To do so would extend the injury toadjacent tissue. Rather, expeditious evacuation and protectionof the casualty from further cold exposure is required. Ifadequate shelter and wraps are available, passive rewarming willoccur during a long evacuation. once tissue has thawed, it isabsolutely essential that it be protected from reexposure tocold.
If refreezing can be prevented during evacuation, thenfrozen tissue can be immediately warmed by contact with warmskin. The groin or axilla are particularly effective areas forwarming frozen tissue.
It is also important to remember that since the injuredtissue is as vulnerable to heat as to cold, whatever emergencytechnique is used for warming, the tissue must not be exposed totemperatures in excess of 102-1030 F, which will aggravate theinjury. Exposure to motor engine manifolds or exhaust, hotwater, open flames, stove tops, or incandescent bulbs isparticularly dangerous. Many frostbite injuries have beensubstantially worsened by exposure to inappropriate warmingtechniques.
Frostbitten tissue is vulnerable to trauma and should becarefully protected from physical injury during evacuation. Indesperate circumstances, frostbite casualties may need to walk onfrozen feet. In these circumstances, any available means shouldbe used to prevent additional injury to the frozen tissue (e.g.,extra wrapping, crutches or buddy assistance).
21

Victims of frostbite often have other, coincident medicalproblems (e.g., hypothermia, traumatic injury, dehydration andhypovolemia). To be sure other problems are found and managed,every frostbite casualty must be thoroughly examined andevaluated.
Since many frostbite injuries result in formalinvestigations, careful records should be made from the outset,includin, a complete description of the circumstances of theinjury, its initial extent and appearance, and the first steps ofmanagement.
3.2.4 Hospital Nbnagmnt
At the Medical Treatment Facility (MTF), management includeswarming of still-frozen tissue, treatment of various phases ofthe injury as it evolves, and evaluation for coincident injuryand illness. Frostbite injuries require meticulous record-keeping, which should include careful and complete descriptionsof the circumstances of the injury, its prehospital management,its extent, and all phases of its management. This documentationshould begin from the first contact with the casualty.
If tissue is still anesthetic and cold upon arrival at theMTF, active warming is usually appropriate. If the tissue hasalready thawed on arrival at the MTF, additional active warmingshould not be done.
Digits or entire hands or feet can be warmed in atemperature monitored water bath kept at 102-1050 F. Facialtissue or the ears can be warmed by towels kept wet with waterwarmed to 102-105'F. Warming should be continued until nofurther irrprovement in the return of circulation and mobility isnoted. This usually requires 15 to 45 minutes depending on theinitial temperature and size of the injured part. After warming,the frostbitten tissue should be carefully and atraumaticallydried, completely covered in bulky dry dressings, and keptslightly elevated to moderate swelling.
In addition to the immediate local treatment of the injuredpart, a corplete examination of the casualty is required todetect other frozen tissue (remember, while below 50°F theseareas are anesthetic), other traumatic injuries, hypovolemia, andhypothermia. Temperature should always be taken using a lowreading thermometer at a "core" (rectal or esophageal) site.Since dehydration and hypovolemia are so common with significantcold injuries and cold exposure, IV access should be establishedearly and rehydration begun.
After whatever stabilization is necessary and warming hasbegun, early management includes: tetanus prophylaxis as
22
appropriate, and analgesics. Frostbite is a tetanus-prone wound.If immunization status is unknown or incomplete, both tetanustoxoid and tetanus immune globulin should be given. If tetanusimmunization has been completed but more than five years havepassed since the last "booster", only the toxoid should be given.During warming, pain appears and is often intense. Analgesiashould be provided with NSAIDs and narcotics as needed. Inaddition to pain control, NSAIDs are believed by some to reducethe release of eicosanoids that may aggravate the post-injuryischemia. Ibuprofen is the NSAID most conmonly used.
Prophylactic antibiotics are frequently used as a routinepart of early management. Because wound anaerobes andstreptococci appear to be early causes of post-injury infection,penicillin is reconmmended (2-4 M units IV QD or 500 mg po QID).For the penicillin allergic, clindamycin is an alternative.There is no consensus on the appropriate duration of prophylacticantibiotic treatment. Courses longer than a few days clearlycarry the risk of selecting resistant organisms.
The continuing care of frostbite is intended to minimize theloss of tissue by providing the optimum environment for healing,avoiding additional injury and infection, and permittingspontaneous evolution of tissue loss. The injury must beabsolutely protected against exposure to excessive cold or heatand from physical trauma. When the casualty does not haveadequate housing or warm transportation, hospitalization may berequired for injuries involving only small amounts of tissue. Inthe case of third or fourth degree injuries, particularly in coldclimates, months of hospitalization may be needed to provideappropriate care and protection of the injury.
In second, third and fourth degree injuries, devitalizedtissue is usually removed by whirlpool debridement once or twicedaily in skin temperature saline or dilute betadine. Duringwhirlpool treatment, gentle active range of motion exercises aredone to minimize functional loss. Careful atraamatic drying andredressing is done after each whirlpool treatment. Some centershave begun to apply aloe vera ointments to the surface of bullaein an attempt to reduce the production of vasoconstrictiveeicosanoids and facilitate healing.
In injuries that appear severe, radioisotope scanning ofbone or soft tissue perfusion three to five days post-injury willprovide some evidence of the extent to which the deep tissues areinvolved and may allow earlier prognostic judgements. Digitalsubtraction angiography has been used as well, but it is notclear that it offers sufficient additional information to offsetits increased risk relative to scanning. In any case, sincecurrent practice permits the injury to evolve with minimalintervention, these diagnostic techniques would not be expectedto influence management or hospital stay.
23

Occasionally, significant arterial vasospasm may be presentin the first several days after injury. As a rule, use oftobacco is prohibited during healing of any cold injury to avoidany vasoconstriction due to nicotine. Alpha-blockade has beenreported anecdotally to reduce post-injury vasospasm. Based onths experience, when vasospasm seems to be limiting perfusionafter injury, a trial of alpha-blockade should be considered.The vascular response should be monitored with objectivetechniques such as skin temperature or Doppler flow measurements.The dose can be titrated upward to the appearance of sigrnificantnon-cutaneous side effects such as orthostatic hypotension ornasal stuffiness. If alpha-blockade appears to enhance flow, itshould be continued in the minimally effective dose for severaldays and, then, tapered over one to two days while watching forreturn of vasospasm. The practice of early sympathectomy orintraarterial injection of vasodilators has largely disappeared.
Heparin and aspirin have both been used in attempts toprevent microthrombi in injured arterioles without notablesuccess. Neither measure is used routinely in current practice.One anecdotal report of early use of thrombolysis has beenpublished. At this time, the role of thrombolytic therapy in theearly management of freezing injury is not clear and is a matterfor clinical investigation.
Infection during healing of deep frostbite injuries is anextremely serious complication. If uncontrolled, the infectioncan disseminate systemically or precipitate gangrene. Even ifthe infection does not disseminate or produce gangrene, localtreatment of infection often necessitates surgical debridement ofthe injury and loss of tissue that might otherwise have beenpreserved. At the earliest evidence of infection, afterculturing the wound, aggressive antibiotic therapy should beinitiated. The antibiotics should be directed at usual woundpathogens, including anaerobes, and the nosocomial organismscharacteristic of the particular MTF. If prophylacticarntibiotics have been used, antibiotics should be selected on theassumption that the infection is due to organisms resistant tothe prophylactic antibiotics.
The principal late complications of frostbite include tissueloss, contractures, persistent pain, cold sensitivity,susceptibility to reinjury and hyperhidrosis. The evaluation andmanagement of post-injury symptoms may be complicated bysecondary gain. Contractures and tissue loss should be managedby mechanical means such as orthotics and prostheses. There areno uniformly beneficial approaches to the management ofpersistent pain. Referral to a specialty pain management centeras early as possible is appropriate. Cold sensitivity can bemanaged by extra protection of the injured area. However,occasionally cold exposure of any portion of the skin canprecipitate symptoms in the area of a previous injury.
24
Relocation to a warm climate may be required if cold intoleranceis intractable. Tissues that have suffered a frostbite injury,are probably more susceptible to cold injury and should receiveextra protection and attention when exposed to cold. Post-frostbite hyperhidrosis of the feet can increase the incidence ofdermatophyte infection and maceration.
3.2.5 Retum to Duty and Physical Profilirn
Recovery from frostbite is slow. Soldiers with frostbiteare, as a rule, unable to participate in outdoor duties for atleast the remainder of the cold season. Even though mostfrostbite injuries are only first or second degree, persistentpost-healing functional symptoms are frequent and may be a causefor separation from military service.
Physical profiles should be based on each individualcircumstance and any established local, Department of the Army(DA) or U.S. Army Medical Department (AMEDD) policies. If nospecific policies have been established, the following profilingguideline is suggested:
1. If the frostbite injury has caused significant loss oftissue or persistent disabling symptoms, the soldier should beevaluated by a Medical Board (MPEBD) and referred, as appropriate,for further consideration.
2. For healed first degree frostbite: Following completehealing, issue a permanent P-2 profile permitting the use ofadditional cold weather protective clothing as needed. Non-regulation clothing items are permitted under the regulationouter uniform.
3. For healed second, third and fourth degree frostbite:Initially, issue a temporary P-3 profile prohibiting bothexposure to temrperatures below 321F and any physical activitieslimited by the injury itself. This temporary profile is renewedat three-month intervals for the remainder of the cold season.At the end of the cold season, issue a permanent P-2 profilesimilar to that for first degree injury providing there is noapparent residual difficulty. Reappearance of symptom upon thereturn of cold weather may require evaluation by a MEBD andappropriate further evaluation.
3.3 Non-Freezing Cold Injury (NFCI).Non-freezing cold injury is the result of prolonged (many
hours) exposure of the extremities to wet-cold, but above freez-ins, conditions. The feet are the most conmtn area of injury,which is reflected in the common names of the two principal typesof non-freezing injury: trench foo and inrmersion foot. Trench
25

foot occurs during ground operations and is due to the combinedeffects of sustained cold exposure and restricted circulation.Immersion foot is caused by continuous inmmersion of theextremities in cold water and usually occurs in survivors of shipsinkings. Trench foot is rare outside of military operations,but immersion injury is a risk of any venture on cold ocean.
3.3.1 Pathogmesis
NFCI is the result of prolonged (many hours) cooling of thelower extremities to temperatures above freezing but below 650F.The prolonged cooling produces some damage to all the softtissues; but peripheral nerves and blood vessels suffer theýnreatest injury. The vascular injury causes secondary ischemicijury which aggravates the direct effect of cold on othertissues. NFCI is initially reversible, but if cooling issustained, it becomes irreversible. Wet conditions increase therisk and accelerate the injury both because wet clothinginsulates poorly and water itself cools more effectively than airat the same temperature. Factors that reduce circulation to theextremities also contribute to the injury. In militaryoperations, these factors include constrictive clothing andboots, prolonged immobility, hypothermia and crouched posture.Maceration of the wet skin can complicate NFCI and predisposes toearly infection.
3.3.2 Clinical Manifestations
When first seen, the injured tissue is pale, anesthetic,pulseless and immobile, but not frozen. Trench foot or immersionfoot (depending on the environmental medium causing the injury)can be diagnosed when these signs DO NOT CHANGE AFTER WARMING.In addition, the skin is frequently macerated and slightly edema-tous. The degree of the injury is usually not completely apparentearly.
Initially, despite rest and warmth, the injured part remainspale, anesthetic and pulseless. After several hours(occasionally as long as 24-36 hours), a marked hyperemiadevelops associated with severe burning pain and reappearance ofsensation proximally, but not distally. The hyperemia representsa passive venous vasodilation and blanches with elevation.Edema, often sanguineous, and bullae develop in the injured areasas perfusion increases. Skin that remains poorly perfused afterhyperemia appears is likely to slough as the injury evolves.Persistence of pulselessness in an extremity after 48 hourssuggests severe deep injury and high likelihood of substantialtissue loss. The hyperemia lasts a few days to many weeksdepending on the severity of the injury.
26
Recovery from NFCI is slow due to its neuropathic component.Except in minor injuries, sharp, intermittent "lightning" painsdevelop in the second week after injury, which are in addition tothe burning and are described as reminiscent of tabes dorsalis.Improved sensitivity to light touch and pin in the area ofanesthesia within four to five weeks suggests reversible nerveinjury and less likelihood of persistent symptoms. Persistenceof anesthesia to touch beyond six weeks suggests neuronaldegeneration. Injury of that degree takes much longer to resolveand has a greater likelihood of persistent disabling symptoms.
Hyperhidrosis is a comTmon and prominent late feature of NFCIand seems to precede the recovery of sensation. A distinctadvancing hyperhidrotic zone can develop which is presumed tomark the point to which sudomotor nerves have regenerated(Guttmann. L., 1940). The excessive sweating may be permanent.It predisposes to blistering, maceration and dermatophyteinfection.
3.3.3 Classification
NFCI has been classified into four degrees of severity. Twoschemes of classification have been used based on clinical seriesfrom World War II. The Webster classification (Webster, D.R.,Woolhouse, F.M. and Johnston, J.L., 1942) is based on theclinical appearance of the foot two to three days after injury.The Ungley classification (Ungley, C.C., 1949) is based on thedistribution of anesthesia seven days after injury. These twosystems correlate well and provide useful prognostic information.
Minimal NFCI (Webster) or Grade A (Ungley). Hyperemia andslight sensory change remain two to three days after injury. Atseven days after injury, no objective findings or anesthesiaremain. Rapid re-amrbulation is the rule with only occasionalresidual cold sensitivity. Return to duty is possible within oneto two weeks.
Mild NFCI (Webster) or Grade B (Ungley). Edema, hyperemiaand definite sensory change are still present two to three daysafter injury. At seven days after injury, anesthesia is foundonly on the plantar surface of the foot and tips of the toes, andlasts four to nine weeks. This degree of injury is associatedwith one to three weeks of edema, two to four weeks ofneuropathic pain and three to seven weeks of hyperemia. Bullaeand skin loss are not seen. Hyperhidrosis and residual coldsensitivity occur in about half the injuries, althouqh notnecessarily in the same individuals. Re-ambulation is possiblewhen walking does not increase pain. Return to duty usuallyrequires three to four months.
27

Moderate NFCI (Webster) or Grade C (Ungley). Edema,hyperemia, bullae and mottling are present two to three daysafter injury. At seven days, anesthesia to touch is present onthe dorsum of the foot as well as the plantar surface and toes.In addition to anesthesia to touch, vibration and position senseare diminished and the intrinsic muscles of the foot becomeparetic and atrophic. Edema persists two to three weeks, painand hyperemia up to 14 weeks. Some of the skin affected byblistering sloughs, but loss of deep tissue does not occur.Hyperhidrosis and cold sensitivity occur in the majority ofcases. A significant number of cases will become permanentlydisabled and these soldiers will not be able to return to duty.
Severe NFd (Webster) or Grade D (Ungley). Severe edema,extravasation of blood and incipient gangrene are present two tothree days after injury. At seven days, complete anesthesia isfound in the entire foot with paralysis and wasting of theintrinsic muscles. The injury often extends proximal to thefoot. The injury produces significant loss of tissue throughautoamputation. Deep tissue, as well as superficial tissue islost. Gangrene is a constant risk until tissue loss is complete.Edema in tissue that is not lost lasts three to seven weeks;hyperemia and pain last up to four months. Prolongedconvalescence and permanent disability are the rule. Soldierswith these injuries rarely are able to return to duty.
3.3.4 First Aid and Field ManageUent
NFCI, like frostbite, is an insidious injury because theaffected tissue is cooled to the point of anaesthesia while theinjury is occurring. So, like frostbite, the first essential ofmanagement is detection. Foot inspection and care every eighthours under cold-wet condition will prevent most cases and allowdetection of early injury. Boots and socks should not bereplaced on the feet until the feet are warm and have normalfeeling. Residual anesthesia after warming is evidence of NFCI.Soldiers who suspect a NFCI should inspect and warm their feetimmediately.
If NFCI is suspected to have occurred, priority evacuationis appropriate. Because tissue injured by NFCI is as vulnerableto trauma and cold exposure as thawed freezing injuries, theinjured extremity must be carefully protected during evacuation.If the lower extremity is involved, the casualty must be moved bylitter, vehicle or aircraft; ambulation is not possible. Drycovering of the injured part and protection of the casualty fromcold may permit spontaneous warming of the injured tissue duringevacuation. If warming does occur during evacuation, severe painmay develop before arrival at a MTF. Consequently, if aprolonged evacuation is anticipated in a particular case, thesoldiers performing the evacuation should be equipped and trained
28
to provide adequate analgesia. The possibility that pain mayappear during evacuation is NOT a reason to keep an injuredextremity cool.
Active warming is not necessary for NFCI. The extremitieswill warm spontaneously when the casualty is removed from cold-wet conditions. Massaging the injury "to restore circulation"may worsen it.
NFCI, even in its mildest expression, evolves slowly, andso, requires time (> one week) for evaluation and recovery.Therefore, when a casualty is considered to have a NFCI, heshould be evacuated to a rear echelon hospital. Nothing is to begained from observation in forward echelons.
3.3.5 Hospital Management
The principal reguirements of initial hospital managementare tetanus prophylaxis, manamement of concomitant hypothermiaand dehydration, and pain relief. The casualty should be warmedand rehydrated, but the injured extremity should not be activelywarmed. Bed rest in a warm room is sufficient.
The injured extremity should be kept at the temperatureproviding the greatest comfort. After hyperemia appears, coolingby a fan usually provides some relief from the burning pain.External warming (as, e.g., a vascular light box) should not beused. Dry loose dressings can be used to cover the injury buteven the weight of bedclothes may aggravate the pain. Painrelief with acetaminophen, NSAIDs and opiate analgesics should beprovided as needed.
As the injury evolves, pain and infection present theprimary clinical challenges.
To minimize pain and avoid mechanical injury, weight bearingshould not be allowed until the circulation has been fullyrestored, edema has cleared, and any maceration or ulceration hashealed. Patients with areas of indolent dry gangrene in the toesmay walk if the other parts of the feet can be protected againstfurther injury. Deep pain on weight bearing may limit walkingfor periods of a few days in minimal injury to months in severeinjury.
Macerated and ulcerated skin increases the likelihood ofinfection. The skin should be assiduously protected with drydressings. Intact bullae should be left intact; ruptured bullaeshould be sharply debrided and dressed. Open bullae, ulcers andareas of necrosis should be periodically monitored withsurveillance aerobic cultures. If infection appears, it shouldbe treated immediately with antibiotics selected to be effective
29

against organisms detected by surveillance cultures. In severeinjuries, infection of deep tissues may develop. In thiscircumstance, the antibiotics selected must also be effectiveagainst anaerobes and pseudomonas (e.g., ampicillin sulbactam orimipenen cilistatin).
3.3.6 Retum to Duty and Physical Profiling
Anatomic defects and functional symptoms commonly causepersistent disability after NFCI. The more common of thesedefects and symptoms include: loss of toes and other forefoottissues, hammer toe deformities, flexion contracture of the greattoe, hyperhidrosis predisposing to skin maceration and dermato-phytosis, persistent pain, either spontaneous or when weightbearing, and cold intolerance.
Casualties with minimal or mild degrees of injury areusually able to return to duty. They should receive a medicalfitness profile appropriate for their symptoms and functionallimitation. Casualties who have suffered moderate or severeinjury should be evaluated by a MEBD at the completion ofclinical healing. Soldiers with persistent symptoms orfunctional impairment should be referred to a Physical EvaluationBoard (PEB).
3.4 Accidental Hypothermia.
3.41 Pathophysiology of Hypothrmia
The sequence of events during whole-body cooling and rewarm-ing is well known.
The initial response to a fall in core temperature isperipheral vasoconstriction, followed by an increase in muscletone and metabolic rate. With continued fall in coretemperature, shivering, tachypnea, tachycardia and hypertensiondevelop. These become maximal when the core temperature is about95OF (35 0C) .
Below a core temperature of 95°F (350C), the depressanteffect of hypothermia begins to offset the metabolic activation.As core temperature falls from 95°F to 860F (30 0C), metabolicrate, shivering, respiratory rate, heart rate and cognitive func-tion all decline. The individual may become quiet and withdrawnor confused and combative initially, but eventually becomesobtunded. Furthermore, since the metabolic depression ofhypothermia stops the hypermetabolic response to cold, theindividual loses a substantial defense against additional fall incore temperature. As core temperature declines, the rate of itsfall can accelerate.
30
Below 95 0F (350C) core tenperature, heart rate, blood pres-sure and respiratory rate decline roughly in parallel. Metabolicrate, oxygen consýumption and cardiac output are about half normalat 85°F (29 0C) and about 20% normal at 68 0F (200C) . At theselower temperatures, ventilation and perfusion do not quite keepup with metabolic requirements and a mixed respiratory andmetabolic acidosis develops.
When the core temperature falls below 860F (30 0C), atrialtachyarrhythmias and repolarization abnormalities ("Osbornewaves") appear. Below 82 0F (280C), the ventricular fibrillationthreshold declines, presumably due to inhibition of Purkinjefiber conduction velocity.
Peripheral voluntary muscle activity and reflexes disappearabout 80°F (27 0C). Brainstem reflexes disappear about 730F(23 0C). Below 68 0F (20°C), electrical activity disappears, firstin the brain and then in the heart. Despite the disappearance ofall objective evidence of life at these low core temperatures,resuscitation is possible.
3.4,2 Accidental Hy.wth-mIa
Hypothermia is the clinical syndrome that results fromreduced core temperature. By definition, hypothermia isconsidered to be present when the "core" temperature (clinicallyusually taken to be the same as rectal temperature) is below 950F (35 0C). Hypothermia is always the product of loss of heat tothe environment in excess of the rate of heat production by thebody.
Hypothermia that occurs outside the therapeutic setting iscalled accidental hypothermia to distinguish it from hypothermiadeliberately induced for therapeutic purposes. Individualsdevelop accidental hypothermia when the cooling effect of theirenvironment is greater than their thermoregulatory capacity.Individuals who have poor thermoregulatory responses to cold maybecome hypothermic even in relatively mild cold stress. Poorthermoregulatory responses to cold are found. in individuals withmetabolic illnesses (e.g., hypothyroidism or hypoadrenalism),malnutrition, severe trauma, extensive burns (which accelerateheat loss despite hypermetabolism), CNS lesions ofthermoregulatory centers, depressant intoxications (barbiturates,opiates, ethanol) and others.
Soldiers, unless injured, generally are healthy and havenormal thermoregulatory responses. In soldiers, accidentalhypothermia is usually the result of severe cold exposure. Insoldiers, accidental hypothermia is usually the result of eitherimrersion in cold water (immersion hypothermia) or prolonged
31
exposure in cold-wet ground environments (exhaustionhypothermia).
Immersion hypothermia is usually the result of boating, pondskating and automobile accidents. Airplane accidents andshipwreck can produce mass hypothermic casualties. The fall incore temperature during cold water iimmersion is rapid and steady.Several factors influence the rate and magnitude of core tempera-ture reduction including:
1) water temperature.
2) protective clothing.
3) body posture and movement. Increased exposedsurface area and movement increase the rate of heat loss.
4) body size and adiposity. Smaller, leanerindividuals cool heat more rapidly.
5) thermorecfulatory aggressiveness. There isindividual variation in the thermoregulatory response to coldwater irmmersion. Individuals with less vigorous vasoconstrictiveand shivering responses to cold will cool nrrre quickly thanindividuals with more vigorous responses.
Exhaustion hypothermia (sometimes called "exposure") resultswhen individuals exposed to cold conditions are unable because offatigue or injury to sustain a metabolic rate sufficient tobalance the loss of heat to the environment. Factors thatinfluence the rate of temperature fall during exposure to coldland environments are:
1) ambient temperature and wind.
2) clothing.
3) precipitation. Precipitation reduces the insulatingvalue of clothing and adds an additional source of cooling.
4) rate of physical activity. In contrast to imrmer-sion, physical activity is an important mechanism of maintainingcore temperature in cold conditions on land. The benefit ofphysical activity lasts only as long as activity is maintained.
5) shelter. Dry shelter moderates the cooling effectof wind and precipitation, and may allow an opportunity to rest.
The lethality and difficulty of management of hypothermiadepends on the degree of temperature depression. Consequently,hypothermia is classified into mild, moderate and severe, basedon core temperature. Mild hypothermia is defined as core
32
temperatures between 90 and 950F (32 to 350C). Casualties withmild hypothermia usually retain the ability to rewarmspontaneously and do not develop cardiac arrhythmias. Between90°F and 82 0F (320 to 28'C), the range of moderate hypothermia,atrial arrhythmias become coinon and metabolic rate is suffi-ciently depressed to significantly slow the rate of spontaneousrewarming. Below 82°F (28 0C), the range of severe hypothermia,spontaneous rewarming is markedly depressed and the risk of ven-tricular fibrillation becomes substantial.
3.4.3 Clinical Manifestations of Hypothermia
The clinical manifestations of mild to moderate hypothermiaare frequently insidious and subtle. Mild to moderatehypothermia may not be recognized unless it is suspected and coretemperature is measured. If oral temperature is not over 95°F(35 0C), rectal temperature should be measured with a low readingthermometer.
The principal manifestations of mild to moderate hypothermiaare shivering and mental status change. Persistent shivering isevidence of incipient hypothermia and should always be takenseriously. Shivering will diminish as hypothermia worsens. Theother significant early manifestation of hypothermia is a changein mental status. Mental status change may be the only clinicalevidence of significant hypothermia. Withdrawal and irritabilityare contain. As hypothermia worsens, subtle mental status changesprogress to frank confusion, lethargy and obtundation. Thedegree of mental status change is not a reliable guide to thedegree of hypothermia. For example, individuals have beenreported to remain conscious at core temperatures below 80°F(27 0C) .
The clinical manifestations of hypothermia become moredramatic and more obvious as core temperature falls. Cool, paleskin, obtundation, atrial arrhythmias, bradycardia and hypopneaare all prcsent at core temperatures in the 80-90°F (27-320C)range.
At core temperatures between 70 and 801F (21-270C), reflexesand vital signs become imperceptible, the skin is cold and waxyand musclular rigor may be present.
The brain and the heart become electrically silent at coretemperatures between 60 and 701F and the hypothermic casualtyappears clinically dead.
3.A4 First Aid and Field Management of Accidental Hypothermia
The diagnosis of hypothermia is confirmed by coretemperature measurement. However, clinical thermometers are
33

often unavailable in the field and first responders have to relyon their judgement of the clinical state of the casualty.
Anyone suspected of hypothermia should be considered to beat risk of sudden death from ventricular fibrillation orhypotension and steps should be taken to prevent thosecomplications. Handling should be minimal and gentle. Copiousinsulation to prevent heat loss should be placed around thecasualty at the same time wet clothinV is removed. Protectionfrom wind and wet is important. The insulation under thecasualty should be incompressible, otherwise it will rapidlybecome ineffective under the casualty's weight and allow signifi-cant heat loss. Airway heat loss should be prevented by anymeans available even if only a scarf or non-occlusive bandage isavailable.
If necessary, ventilation can be assisted by mask and bag.When indicateQ, endotracheal intubation is safe as it does notseem to increase the risk of ventricular fibrillation. Oxygensupplementation is usually not needed because of the low oxygenrequirements in hypothermia.
Since dehydration and hypovolemia are comnmon in hypothermiccasualties, an IV should be started with warmed fluid (LR, NS,D5/0.5NS). If hypoglycemia, alcoholism or opiate intoxicationare possible causes of hypothermia, naloxone (1-2 mg), thiamine(100 mg) and glucose (10-25 grams) should be administered IV.
An injury survey should be done and appropriate dressing,splinting and stabilization provided before transport/evacuation.
3.4.5 Cardiopulmonary Resuscitation (CPR)
Victims of severe hypothermia often appear to be in cardiacarrest; they are unconscious and without perceptible signs oflife. In the normothermic individual with these signs, CPR wouldbe initiated without hesitation beca:.,se there is no significantrisk of doing harm in excess of benefit. In the hypothermicindividual, however, there is a real risk of converting aperfusing quiet bradycardia into ventricular fibrillation byexternal massage. The lowered ventricular fibrillation thresholdis likely due to reduced conduction velocity in both the Purkinjesystem and myocardium allowing circus movement propagation ofaction potentials. Ventricular fibrillation greatly complicatesand reduces the likelihood of successful resuscitation fromhypothermia.
If possible, cardiac monitoring and Doppler flow probesshould be used in the field to determine the need for CPR. (Besure to warm metal elkctrodes before applying to avoid freezinginjury to the sKin.) if monitoring shows a regular ventricular
34

rhythm and arterial flow can be appreciated by Doppler, CPRshould not be performed, even if pulse and/or blood pressure areotherwise imperceptible. Ventricular fibrillation reguiresexternal massage. Wide complex ventricular rhythms withoutdetectable flow should probably also be given external massage.
If cardiac monitoring or flow probes are not available, thefollowing suggestion can be considered for implementation.
Remember to take more time for assessment in hypothermiccasualties. The slow pulse may be difficult to appreciate. Ifthe casualty meets the criteria for CPR, initiate CPR unless:
1) Any signs of life (respiratory effort, spontaneousmuscular movement) are present. These signs must becontinuously reassessed to assure they persist. Theirdisappearance may represent a failure of perfusion due toventricular fibrillation.
2) There are pre-existing orders not to resuscitate ora valid living will.
3) There are other obvious lethal injuries.
4) The chest is incompressible.
5) Performing CPR would be dangerous to the rescuers.
6) Core temperature is less than 420F (6°C).
7) Serum potassium is greater than 10 meq/l. (This maynot be the easiest measurement to obtain in the field, but is areliable criteria for resuscitative futility).
CPR should be continued until core temperature exceeds 90°Fand no evidence of effective cardiac function is present (i.e.,pulseless electrical activity, asystole or agonal rhythm).
Guidelines for discontinuing resuscitation after prolongedarrest in severe hypothermia have been developed at EmanualHospital in Portland, Oregon. These are:
Resuscitation can be discontinued if:
1) All of the following are true: Core temperature(measured at the right or left atrium) is between 42 and 79OF (6-
260 C), the victim has no vital signs, electrical asystole ispresent and the documented period of arrest has been greater thanfive hours.
OR
35

2) All of the following are true: Core temperature(measured at the right or left atrium) is between 79 and 90OF(26-320C), the victim has no vital signs, electrical asystole ispresent and the documented period of arrest has been greater than12 hours.
3.4.6 Sudden Death in Accidental Hypothermia
Sudden death is a cormmon complication of rescues ofhypothermic individuals. Examples abound of hypothermic victimsalive and alert at the start of crevasse extraction who diedwhile being moved. Even more striking are the reports of massdeaths among shipwreck survivors, who had been able to climbaboard rescuing ships, only to be found dead shortly thereafter.
Three factors are believed to contribute to sudden death inhypothermic individuals: ventricular irritability, hypovolemiaand orthostasis, and sudden intraventricular cooling.
The increased risk of ventricular fibrillation seems to bedue to changes in ventricular impulse conduction. Thehypothermic ventricle responds to mechanical stimuli with localaction potentials. Because the Purkinje system is relativelymore depressed than myocardium, action potentials are propagateddirectly by myocardium allowing establishment of circus movementarrhythmias.
Victims of accidental hypothermia are usually hypovolemicdue to minimal food or water intake and cold diuresis. Ininersionvictims have had an immersion diuresis (due to the displacementof blood volume into the central circulation by the outsidepressure on the legs and abdomen) in addition to cold diuresis.Hypothermia also depresses orthostatic reflexes causing venouspooling to occur in any upright posture. Muscular exerciseincreases blood flow to the exercising muscle, further reducingeffective blood volume. The ultimate consequence of thehypovolemia, orthostasis and redistribution of blood flow ishypotension.
Finally, exercise and warming of the skin in hypothermicindividuals increase blood flow to areas that have beenunderperfused during cold exposure. The stagnant blood in theseareas is acidotic, hyperkalemic and cold. If large amounts ofthis cold peripheral blood enters the central circulation, theventricle is exposed to metabolic and temperature conditions(called post-exposure cooling or "after-drop") that furtheraggravate the risk of fibrillation.
The risk of sudden death can be moderated during rescue byassuring that each of the risk factors above are controlled.Casualties should be kept quiet and supine. Sudden movements
36
during rescue should be avoided. The casualty should not beallowed to exert during rescue. Hypovolemia should be treatedearly.
3.4.7 Hospial Managemnt
The key to successful resuscitation from hypothermia is therestoration of normal core temperature without causingcomplications.
Many techniques have been used to accorplish rewarming.Techniques that take advantage of the casualty's own inherentmetabolic heat veneration (which is present to some degree inevery hypothermic patient) are called "passive rewarmang".Those that apply external sources of heat are called "activerewarmimg".
Passive rewarming techniques consist of providing sufficientinsulation to both the body and the airway to prevent furtherheat loss. Passive rewarming is effective even from coretenmperatures as low as 80OF (27 0C). Depending on theeffectiveness of the insulation, core temperature increases from0.25 to 1F per hour. Passive rewarming is appropriate only aslong as temperature is rising even though it may take 24 - 36hours to restore normothermia. Passive rewarming consumesrelatively few intensive care resources, allows for gradual re-equilibration during rewarming and avoids the complications ofthe invasive techniques. The principal disadvantages of passiverewarming are the long time to normothermia and the need forcontinued surveillance to assure that core temperature isincreasing.
Active rewErming techniques of several types have been used.Active "surface" rewarming techniques apply heat to the periphery(warm baths to trunk or extremities, heating blankets, warmtowels to groin and axilla). These techniques are nottechnically demanding and are probably helpful for mild andmoderate hypothermia. However, there are three caveats. First,they are not effective if cardiac arrest has occurred. Second,by increasing blood flow to skin and extremities before centralrewarming has occurred, they may increase the delivery of coldperipheral blood and precipitate hypotension and cardiac cooling.Third, since hypothermic skin is vulnerable to burning, carefulmonitoring of the temperature of the heat source is needed.
One technique of active surface rewarming is used to warmpatients after induced surgical hypothermia. In this techniquethe scalp is warmed by application of warm (1040F) water soakedtowels. The scalp has a low blood volume but high blood flow andrapid entry into the central circulation. Consequently, heat canbe delivered to the core without increasing the delivery of large
37

amounts of cold peripheral blood. There are no reports yet ofits efficacy in accidental hypothermia.
Active "core" rewarming is required for resuscitation ofhypothermic cardiac arrest and for most severely hypothermicpatients. There are four categories of core rewarmingtechniques: 1) intraluminal lavage, 2) heated air, 3) directvascular warming, and 4) radiant energy.
Although virtually every cavity in the body has been lavagedwith warm fluid for the treatment of hypothermia (stomach,urinary bladder, colon, abdomen and chest), the two in mostcom•on use are gastric lavage and intraperitoneal lavage usingperitoneal dialysis equipment. These techniques are effectiveand simple. They raise core temperature 0.5 to 1.5°F per hour.The principal risks of lavage are the procedures required to gainaccess (gastric intubation, insertion of intraperitonealcatheters, etc.) and aqgravation of edema due to fluid overload.Direct myocardial warmlng by mediastinal lavage using either tubethoracostomy or open techniques has been reported to haveresolved ventricular fibrillation and permitted resuscitationwhen less invasive techniques of core rewarming had failed.
Ventilation with heated air has been developed as an effec-tive technique for central rewarming. A variety of apparatushave been developed for use in the field and in the hospital. Anexcellent recent review of the technique and available apparatusis found in the Journal Of Wilderness Medicine (Lloyd, E.L.,1990).
Hemodialysis and cardiopulmonary bypass are very effectiverewarming techniques. Relatively rapid rewarming is possiblewith both. Cardiopulmonary bypass offers the additional advan-tage of assured perfusion during resuscitation. Because thesetechniques are only available in specialized centers, they areusually only applied in extraordinary circumstances of profoundhypothermia when other methods have failed.
Experimental devices for direct core rewarming usingelectromagnetic radiation in the microwave range have beenreported. Such devices have not yet become available forclinical practice.
The choice of technique for rewarming depends on: (1) thestate of the circulation and (2) the degree of hypothermia.
Casualties who have stable circulation and only mild tomoderate degrees of hypothermia can be given the chance to rewarmspontaneously. If they fail to rewarm spontaneously, then activerewarming should be started. They should be admitted to anintensive care unit, be given warmed, humidified oxygen andgradual re-hydration. They should have continuous cardiac and
38
temperature monitoring (rectal or esophageal). A thorough searchfor contributing causes of hypothermia should be done includingevaluations for intoxication (alcohol and depressants particu-larly), endocrine dysfunction and malnutrition. Sepsis and strokemust be ruled out, particularly in the elderly. Associatedinjuries (particularly frostbite) and complications (pneumonia,decubitus ulcer, thrombophlebitis, pancreatitis, renal failureand hyperosmolarity) should be identified and treated. Oralintake should be prohibited until rewarming is complete and cold-induced ileus has resolved.
Casualties in cardiac arrest or with severe hypothermia willneed more aggressive management. Ideally, medical treatmentfacilities will have a protocol which addresses both the need toprovide an adequate circulation and rewarming for resuscitatinghypothermic patients. Ad hoc management of this profound emer-gency cannot be as adequate as management guided by carefullyconceived and frequently reviewed treatment protocols.(Additional advice for hypothermia treatment protocols can befound in the clinical texts listed in the bibliography of thishandbook.)
The following steps are suggested for the management ofhypothermic cardiac arrest. Endotracheal intubation, if notalready done in the field, should be done and assistedventilation begun with heated humidified oxygen. Sincehypothermic resuscitation tends to be prolonged, earlyinstitution of mechanical compression and ventilation isappropriate. In the hypothermic casualty, oxygen requirements andcarbon dioxide production will be low. Ventilation needs to beguided by blood gas measurements to avoid excessive respiratoryalkalosis. Blood gas measurements can be interpreted as reportedby the laboratory; temperature "correction" is no longerconsidered appropriate.
There is usually no requirement for large amounts of paren-teral fluid. One or two liters during rescue is usuallysufficient to manage hypovolemia unless there is evidence ofhemorrhage or a severe diuresis (e.g. diabetic hyperosmolarcoma). Fluid is not retained in the vascular space in hypother-mia and dramatic edema appears early in resuscitation. The edemais not of great significance in the peripheral tissues except asa possible indicator that edema is a1so developing in the lungs.Pulmonary compliance monitoring during ventilation can be used toprovide early evidence of pulmonary edema and guide appropriateadjustment of ventilation and fluids to minimize the problem.
Hypoglycemia may be a cause of hypothermia or may be aconsequence. If hypoglycemia is found, dextrose (25 cc of D50/W)should be administered immediately. 100 mg of Thiamine IV shouldalways precede the dextrose.
39

As a general rule, antiarrhythmic and vasoactive drugs arenot useful during resuscitation from hypothermia until coretemperatures exceed 900F. Below that temperature, drug effectsare absent or unpredictable. Also, since drug metabolism ismarkedly slowed below 900F, applying American Heart AssociationAdvanced Cardiac Life Support (ACLS) drug protocols inhypothermia causes the accumulation of drugs which have nomanifest effect when administered, but which suddenly and drama-tically express themselves as they regain activity at higher coretemperatures. A possible exception is bretylium tosylate, whichhas been shown (Orts, A., Alcaraz, C., Delaney, K.A., Goldfrank,L.R., Turndorf, H. and Puig, M.M., 1992) to have some efficacyagainst ventricular fibrillation at depressed core temperatures.If drug therapy of ventricular fibrillation is required,bretylium at its usual doses would be the drug of choice.
During resuscitation, temperature should be continuouslymonitored either in the rectum, esophagus or centralvessels. Urine output should be monitored both as an index ofrenal perfusion, and as a guide for replacement of renal fluidlosses which can be substantial.
Coagulopathies of M ncertain etiology occur in some severelyhypothermic patients. Profuse bleeding may develop duringrewarming which may require massive replacement with red cells,fresh frozen plasma and platelets. Coagulopathies gradually re-solve after successful rewarming.
Until it is clear that the patient can maintain coretemperature, core temperature monitoring is required.
After rewarming, continuing management should be directed atany associated and underlying conditions. The principal post-warming conplications of accidental hypothermia are: pneumonia(including aspiration after inmnersion), pancreatitis,rhabdomyolysis, myoglobinuria and renal failure. Temporary leftventricular dysfunction has been seen after profound hypothermia.Late complications of hypothermia include prolonged, sometimespermanent, cold sensitivity and occasionally contractures in thehands and/or feet.
If a thorough evaluation does not reveal any underlyingconditions and the circumstances of the accident account for thehypothermia, permanent disability due to the hypothermic episodeis unusual.
3.4.8 Retum to Duty and Physical Profiling
Upon complete recovery from hypothermia and anyconplications, the soldier can return to his unit with atemporary P-2 profile, permitting the use of additional cold
40
weather protective clothing as needed. Non-regulation clothingitems are permitted under the regulation outer uniform. Unitleaders should be instructed to provide additional supervision tothe soldier during cold exposure. If a recovered soldierexhibits any tendency toward cold intolerance or inability toperform in the cold, the soldier should be referred to a PEB.
Since accidental hypothermia is frequently associated withother injuries (e.g., frostbite), those other injuries imay welldetermine the convalescent course and disposition of the soldier.
3.5 Other Medical Problems in Cold Environments.
The body surfaces directly exposed to cold (i.e., skin andrespiratory mucosa), suffer a variety of conditions that, if notprevented or* appropriately managed, will lead to discomfort andeven acute disability. All carry a risk of progression to moreserious conditions.
3.51! Carbon Monoxide (CO) Poisoning
During cold weather operations, the continuous running ofvehicle engines to prevent freezing and the use of fuel-firedheaters in tents and other closed spaces poses a risk of carbonmonoxide poisoning.
Carbon monoxide is extraordinarily toxic. Concentrations of100 parts per million in sea level air will produce carboxyhemo-globin (COHb)concentrations up to 20% and frank toxicity.Headache, vomitin¶ and change in mental status are typicalsyrrptoms of CO poisoning. "Cherry red skin", although freguentlymentioned as a specific physical finding, is unusual even insevere cases. Its absence should not be considered as excludingCO poisoning. (Note also, extremities below 50°F reduce theiroxygen utilization to low levels, so that the perfusing bloodretains its arterial color. Cold, bright red extremities are,therefore, not evidence of CO poisoning. The bright red color ofcarboxyhemoglobin should be looked for in warm tissue (e.g., oralmucosa).
Oxygen saturation measured by co-oximetry is a usefulscreening test for CO poisoning because CO reduces oxygensaturation. Oxygen saturation as reported by arterial blood gasanalysis is often calculated, not measured, and should not berelied on to rule out CO poisoning. Indeed, a difference betweenco-oximetric and calculated oxygen saturation is excellentevidence of CO poisoning. The definitive test is directmeasurement of carboxyhemoglobin in blood.
41
Management of C0 poisoning is inrmediate administration of100% oxygen by a close fitting mask or endotracheal tube.Hyperbaric oxygen will accelerate the clearance of CC. Generalindications for hyperbaric oxygen are: COHb is greater thaxu 25%,metabolic acidosis, angina or ECG change, or neurologic symptomsother than headache.
If air evacuation is necessary, the lowest possible altitudeshould be used to maintain the highest possible P0 2 .
3.5.2 Respiratory Tract Conditions
The nasal and bronchial mucosa respond to cold air byincreasing mucus production. Consequently, chronic nasal dis-charge and cough are a frequent acconpaniment of cold weatheroperations. Rhinorrhea and bronchorrhea are probably protectivebut can cause two principal complications. First, nasaldischarge causes wetting and chapping of the philtrum and nasa-labial sulcus which increases the risk of cold injury and localinfection. Second, the increased secretions may accumulate andinterfere with drainage of the sinuses leading to sinusitis.Decongestants may reduce nasal secretions, but commensuratelyreduce their protective effect. Careful local hygiene is abetter measure than decongestants to prevent chapping. Militaryarctic mittens are designed with a pad to wipe nasal secretionsfrom the face without taking off the mitten.
Crowding and poor ventilation in tents and other sheltersincrease dissemination of respiratory infections. Influenzavaccination is an essential preventive measure. Medical officersshould perform aggressive surveillance, particularly for strepto-coccal infection. Early intervention with appropriate infectioncontrol can curtail the spread of respiratory infection.
Some individuals will experience bronchospasm on exposure tocold dry air or fumes from fuel-fired heaters. These individualsshould be evacuated for evaluation.
3.5.3 Cold Urticara
Cold can precipitate a variety of local immunologic skinreactions in susceptible individuals involving a variety ofirmunoproteins.
Cold urticaria which is manifested as local or systemicurticaria on exposure to cold can be familial, congenital oracquired. Its onset is usually abrupt and distinctive. It canbe reliably induced by local application of ice or irnrersion ofan extremity in an ice bath which will reproduce local or system-ic symptoms. Although not cormon, cold urticaria is occasionally
42

associated with detectable cryoproteins (cryoglobulin, coldhemolysin and cryofibrinogen) . A rare "delayed" cold urticariahas been described that may depend on cellular immune mechanismsrather than circulating immune mediators. Cold urticaria ispotentially lethal either from systemic anaphylaxis or laryngealswelling upon exposure to cold liquids during drinking.
Immune mediators activated by cold can cause other reactionsbesides urticaria. Most cause symptoms and signs includingcyanosis, livedo reticularis, pruritus, paresthesia and Raynaud'sphenomenon in the acral regions of the body. Immune complexesdeposited in the microcirculation can cause distal ulceration,even frank gangrene. Cold hemolysin and agglutinins canprecipitate episodic hemolysis and hemoglobinuria. Individualswho develop symptoms or signs of cryoprotein-mediated diseaseshould be referred for evaluation.
3.5A Chilblains (Pemio)
Chilblains are small erythematous papules that appear mostcommonly on the extensor surface of the fingers, but can appearon any skin chronically exposed to above freezing cold. Ears,tace and exposed shins are other commonly mentioned locations.Multiple lesions are the rule. The lesion is pruritic andpainful, particularly after re-exposure to cold. It is indolentaid does not remit until cold exposure has ceased. Chilblainsfrequently recur upon the return of cold weather. Chilblainsoccasionally ulcerate.
The etiology of chilblains is unknown. Some cases may besecondary to cryoprotein or localized vasculitic processes("lupus pernio").
Management of chilblains is by protection from cold withsuitable clothing. Symptoms will remit when cold exposure iseliminated.
3.5.5 Solar Keratitis (Snow Blindness) and Sunburn
The dry air and brilliant reflectivity of snow combine tovenerate a risk of ultraviolet burns to skin and eyes. This riskis tremendously enhanced at altitude. The injury is not apparentuntil after exposure, so prevention by appropriate solarprotection is essential.
Management of both types of burn is symptomatic. Solarkeratitis is managed with topical ophthalmic antibiotics,cycloplegics and oral analgesics. If outdoor exposure is un-avoidable, the eyes must be protected by patching. Solarkeratitis is disabling for several days and injured eyes aresusceptible to reinjury.
43

Sunburn can be severe with blistering of the skin andintense pain. Treatment is conservative using oral analgesics andprotecting skin from further injury.
3.5.6 Eczema (.Mnter tch, "Eczema Craquele")
This condition is extremely conmnon on the hands in the coldand frequently will generalize to involve all the skin. It ismanifested by persistent painful itch, thickening and painfulcracking of the skin of the tingers and toes, and fine scaling ofthe skin on extremities and trunk. The cause appears to be lossof the neutral lipids from the stratum corneum which allowsdrying and irritation of the lower layers of skin. Frequentwashing appears to be the principal cause of the cutaneousdelipidation. The cracking and fissuring of skin on the digits ispainful and carries the risk of infection. The problem can beprevented and managed by moderating the frequency of washing (notusually much of a problem during cold weather training), avoidingharsh soaps and applying emollient creams to replace neutral skinlipids.
3.5.7 Lacrations
Untreated lacerations are prone to freezing injury. Theopen skin allows injury to both the wound margins (perhaps due tohemostatic vasoconstriction) and to deep tissue exposed to thecold environment. If a laceration becomes frostbitten, aninitially small injury can be transformed into a serious deepinjury prone to infection and slow to heal. Primary closure andadequate dressing prevents freezing injury in lacerations.
3.5.8 Intolerance of Cold Expore
Some individuals without any history or evidence of past orpresent cold injury complain of recurrent pain and burning oncold exposure. This phenomenon has not been well studied, butclinical impressions are that it seems to be more prevalent amongthose who have repeated, prolonged lower extremity exposures tomoderate cold. No objective findings have been identified.Occasionally, the symptoms seem to become manifest withprogressively less cold exposure.
There is, at present, no diagnostic term for this problemand no management plan beyond avoidance of cold exposure.Soldiers who develop this complaint may require evaluation by aMEBD and referral to a PEB if symptoms are disabling.
44

Section 4.
Key Points and Reminders*** The following secLion is a list of discrete points to beused as reminders and briefing points for training and planning.
4.1 Useful Points to Remember.1. Humans cannot sense core temperature. An individual
becoming hypothermic will usually shiver but will not beotherwise aware of lowered core temperature. Individuals who donot shiver may have no insight into how cold they are.
2. Skin is sensitive to cold and will be painful until itcools to 50OF (100C).
3. Skin accommodates to cold; exposure reduces both thesensation of cold and pain.
4. Skin is numb below 500F. The disappearance of pain in anextremity during cold exposure may indicate serious cold injury.Irmediate visual inspection for frostbite is mandatory.
5. Cold exposure causes diuresis which aggravates thevoluntary dehydration encountered routinely in the field.
6. Extremities below 501F (10 0C) are paralyzed. Individualswith significant hypothermia cannot help themselves.
7. The most important adaptation to cold is learning andapplying skills and equipment that permit living and working inthe cold in safety.
4.2 Prevention.
1. The best prevention against cold injury is a healthy,trained, equipped, well-fed and hydrated soldier.
2. In military operations and training, risk factors forfreezing injuries include: 1) dehydration, 2) weight loss, 3) un-planned or unduly prolonged exposures to cold, 4) undertrained orovertired soldiers and 5) poor or insufficient equipment.
45

3. If one freezing injury has occurred in an operation,remember that everyone in the unit was exposed to the sameconditions. Inspect everyone immediately.
4. Loss of sensation in the feet (they feel like "blocks ofwood' or "like walking on cotton") is an ominous symptom and mustbe immnediately evaluated by direct inspection of the feet.
5. Cold injuries in operations usually occur in clusters.
6. At the eariiest suspicion of hypothermia, the casualtyshould be provided warm shelter iimmediately. The presence ofhypothermia means that the individual is already unable tomaintain body temperature. The hypothermia will only worsen ifnot managed. An individual with mild hypothermia will warmspontaneously and fully recover if provided warm shelter, warmliquids and supervision.
7. No one in whom hypothermia is suspected should be leftalone.
8. Exercise is dangerous if significant hypothermia ispresent.
4.3 Rescue and Evacuation.1. In the cold, the advantage of vehicular evacuation
(!round ambulance, tracked vehicle or helicopter) over manuallitter evacuation is magnified. Movement of casualties by litteror sled is very slow, significantly delays their treatment andexposes them to significant risk of hypothermia. An entire squadof 10-12 soldiers is needed to move a casualty in the mountainsor in snow. Long nights in winter mean more movement must bedone in the dark, increasing the risk of injury to the rescuersand to the casualty. The techniques of movement and the coverrequired to keep the casualty warm on a litter make observationand medical intervention difficult during evacuation.
2. Fluids and medications may freeze and become useless ifcarried in packs or bags. For all practical purposes, a frozenbag of IV solution in the field is only excess weight. Carryingmedication and bags of IV fluid inside cold weather clothingduring evacuation will prevent freezing.
3. Medical units must develop medical support plans thatallow the earliest possible care and stabilization with the leastpossible risk to rescuers and casualties. Provision for initialmanagement in the field in portable shelter while waiting forvehicular evacuation is often preferable to an immediate attemptto move a casualty cross-country.
46

4. Whatever technique of evacuation is used, sufficientprotection from cold must be available for the casualty duringtransportation. Since the casualty will be at rest and oftendepressed by injury, two arctic sleeping bags may be barelysufficient insulation. Airway heat loss should be prevented.
5. It is very important to remember to prevent heat lossfrom beneath the casualty. The down or synthetic material ofsleeping bags is compressed and loses its effectiveness under thecasualty's weight. Additional incompressible insulation (e.g., afoam mattress) is required regardless of the surface beneath.
6. Critical points in rescue and early management ofaccidental hypothermia include:
* To avoid sudden death, hypothermic casualties must bekept absolutely quiet. They must not participate intheir own rescue. They must be kept supine or headdown.
* Prevent further heat loss by removal of wet clothing,copious insulation and protection of the airway.
* Ventilate with warm, humidified air. Endotrachealintubation is safe if needed. Oxygen supplementationis not required for hypothermia alone.
* Provide volume resuscitation (1-2 liters of LIR, NS orD5/0.5 NS) with warm fluid (carry next to the bodyduring approach to keep warm)
* If evacuation requires re-exposure or interruption ofresuscitation, consider rewarming in the field.
4.4 Medical Operations in the Cold.1. Helicopter landings may raise huge opaque clouds of snow,
blinding both the pilots and ground staff. Landing areas shouldbe cleared of snow and debris. If a clean landing site isimpossible, helicopter operations should be performed at adistance from the MTF. This would help to prevent injury in caseof a landing accident and avoid snow blowin[ into the hospitalinterior spaces. Patients awaiting evacuation should be kept inshelter until the rotorwash and blowing snow have cleared.
2. Even warm liquid fluids can freeze while running throughIV tubing in the cold. If necessary, an IV bag can be placedunder the casualty in the sleeping bag and the fluid infused bythe casualty's own weight. However, once begun, supervision of
47
the infusion is very difficult, requiring re-exposure of thecasualty.
3. Cormon IV solutions (LR, NS, D5/W or saline) can bethawed and used after freezing if no damage to the bag hasoccurred and the solutions are clear.
4. Certain medications are known to be damaged by freezingand should not be used after thawing (Weinberg, A.D., Hamlet,M.P., Paturas, J.L., McAninch, G.W. and White, R.W., 1990).These include epinephrine, NPH insulin, sodium bicarbonate,.magnesium sulfate, tetanus toxoid and mannitol. These must notbe used after freezing.
5. Hypothermia is a significant risk during resuscitativecare of burn and trauma casualties in forward areas, particularlyif surgery is required. These casualties often arrive alreadyhypothe- mic due to effect of shock and cooling during evacuation.Careful monitoring of temperature during and after resuscitationwill detect significant hypothermia and permit treatment beforeand during transportation to rear echelons.
6. Medical staff are as susceptible to cold injury as anyoneelse. Since medical areas are usually kept relatively warm, thebasic work uniform is light. Consequently, significant frostbitecan result frorn not takinW the time to dress appropriately foroutside exposure. Frostbite injury is also caused by hasty hand-ling of litters or equipment brought in from outside. Outsideair drafts during helicopter evacuation are particularly danger-ous because of the rapidity with which they can cause freezinginjury.
48
APPENDICES
Appendix A: Wind Chill Chart
Appendix B: Cold Weather Training Guidelines
Appendix C: Clinical Manifestations of Hypothermia
49
Appendix A: Wind Chill Chart
The "wind chill" temerature is an estimate of the still airtemperature that causes the same skin cooling as each of theparticular combinations of wind and temperature listed. Forexample, air at -10OF blowing on the skin at 10 MPH has about thesame cooling effect as -33 0F still air. The risk of freezing isbased on the estimated cooling rate and stratified into threezones of ascending risk.
The windchill temperature provides a roughly 9uantitativeindex of the risk of freezing injury to exposed skin. Theestimates in this table are based on the effect of wind and coldon dry skin in healthy individuals with normal skin. Wet skin orrestricted circulation will increase the susceptibility tofreezing.
The table is adapted from the Wind Chill Chart at Appendix Aof USARIEM Technical Note 92-2: Sustaining Health and Performancein the Cold.
Additional information about the Wind Chill Index can befound in Toner, M.M. and McArdle, W.D. "Physiological Adjustmentsof Man to the Cold", In: Pandolf, K.B., Sawka, M.N. andGonzalez, R.R. (eds.) Human Performance Physiology andEnvironmental Medicine at Terrestrial Extremes. Indianapolis,IN: Benchmark Press, 1988.
50
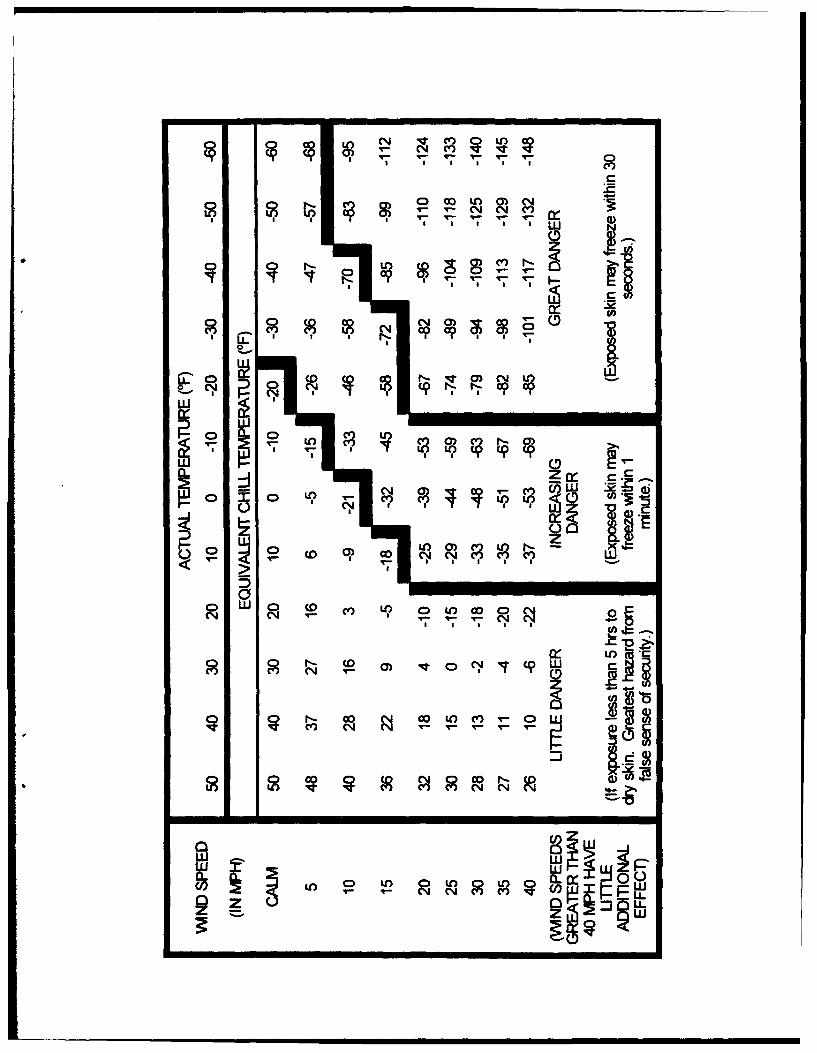
-" -"T-
) m) tn -
I S I I I
C)C
T4-
CD M L 0 LO0
&00
w w
zi

Appendix B: Cold-Weather Training Guidelines
The table in Appendix B was developed by CPT James Cook, MC,USA at USARIE4 as a straightforward set of guidelines for use byunits training in cold envirornments. The guidance is directed atunits that do not have special cold weather experience andtraining.
The table is designed to be copied and distributed to unitleaders for their continued reference.
To determine the recotrmended cold weather protection fortraining, first determine the Wind Chill risk category perAppendix A and estimate the work intensity of the soldiers. Thetable can then be consulted for appropriate protective measures.If the soldiers' work intensity or cold exposure is going to vary(e.g. periodically off-loading trucks), ensure appropriateprotection for each level of work intensity.
52
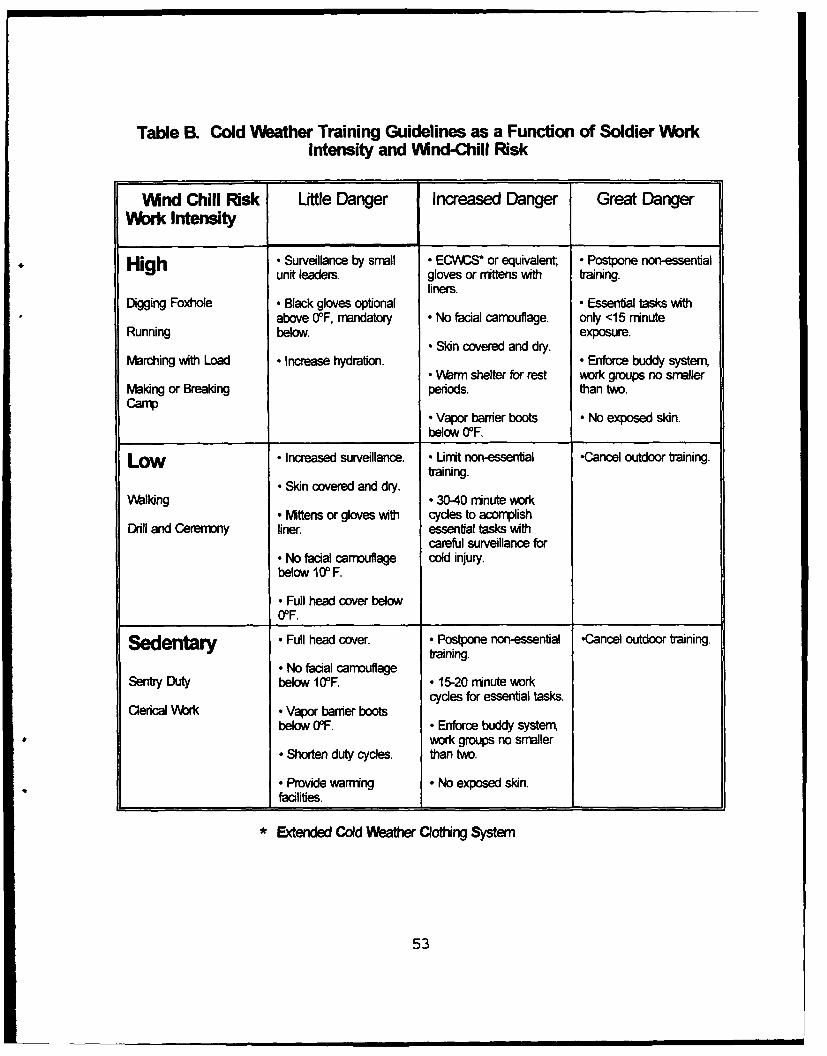
Table B. Cold Weather Training Guidelines as a Function of Soldier WorkIntensity and Wnd-Chill Risk
Wind Chill Risk Uttle Danger Increased Danger Great DangerWork Intensity
High • Surveillance by small • ECWACS* or equivalent • Postpone non-essentialunit leaders. gloves or mittens with training.
liners.Digging Foxhole • Black gloves optional • Essential tasks with
above 0°F, mandatory * No facial camouflage. only <15 ninuteRunning below, exposure.R Skin covered and dry.
Marching with Load * Increase hydration. - Enforce buddy systerr• Warm shelter for rest work groups no smaller
Making or Breaking periods. than two.Camp
C Vapor banier boots • No exposed skin.below 00F.
LOW * Increased surveillance. - Umit non-essential -Cancel outdoor training.training.• Skin covered and dry.
Walking * 30-40 ninute work• Mittens or gloves with cydes to acormplish
DrUll and Ceremony liner, essential tasks withcareful surveillance for
- No facial camnoutage cold injury.below `10 F.
• Full head cover below0OF.
Sedenta•' - Full head cover. Postpone non-essential -Cancel outdoor trainingtraining.• No facial camouflage
Sentry Duty below 10F. * 15-20 minute workcycles for essential tasks
Clenical Work * Vapor barrier bootsbelow 00F. * Enforce buddy systemn
work groups no smaller- Shorten duty cycles, than two.
• Provide warning * No exposed skin.facilities.
• Extended Cold Weather Clothing System
53

Appendix C: Clinical Manifestations of HypothermiaBODY CORE TIMEA• UI I M•AO
C° F0
10037
NomrntheniaIncreased Metabolic Rate
35 95Mild Maximal ShiveringHypothemua Confused-Cornbate-Dysarthric
32 90Obtunded
Moderate Shivering Ceases, Increased Muscle ToneHypotherma
30 85 Reduced Ventricular Fibrillation ThresholdAbtial FibrillationVital Signs Often Clinically Absent
80Coma
Survivor. 16 y/o Male. 1.5 Hour Rescusitaton25 Spontaneous Ventricular Fibrillation
Severe 75Hypotherria No Corneal Reflex
70 Survivor 67 y&o Male. 3 Hour Rescusitation20 Asystrle
65 No CNS Eetical Actvy
60Survivor 23 d/o Male. 6 Hour Rescusitation
15
55
10 50
45 Lowest Terrnerature of Survival from Induced Hypothernia
5
54
REFERENCES
Barat, A.K., Puri, H.C., Ray, N. Cold Injuries in Kashmir,December 1971. Annals of the Royal College of Surgeons ofE2land 60:332-5, 1978.
Guttmann. L. Topographic studies of the disturbances ofsweat secretion after coplete lesions of the peripheral nerves.Journal of Neurology and Psychiatry 3:197-210, 1940.
Lloyd, E.L. Airway warming in the treatment of accidentalA. hypothermia: a review. Journal of Wilderness Medicine 1:54-78,
"1990.
Marsh. A.R. A short but distant war - the Falklands cam-paign. Journal of the Royal Society of Medicine 76:972-82,1983.
Orr, K.D. and Fainer, D. Cold injuries in Korea in thewinter of 1950-51. Meiine (Baltimore) 31:177-220, 1952.
Orts, A., Alcaraz, C., Delaney, K.A., Goldfrank, L.R.,Turndorf, H. and Puig, M.M. Bretylium tosylate and electricallyinduced cardiac arrhythmias during hypothermia in dogs. AmericanJournal of Emergency Medicine 10:311-6, 1992.
Post, P.W., Daniels, F. Jr. and Binford, R.T. Jr. Coldinjury and the evolution of "white" skin. Laboratory experimentsdemonstrate that pigmentation influences the degree of coldinjury to the skin. Human Biol _y 47:65-80, 1975.
Tek, D. and Mackey, S. Non-freezing Cold Injury in a MarineInfantry Battalion. Journal of Wilderness Medicine ("inpress"), 1993.
Ungley, C.C. The Immersion foot syndrome In: Advances inS Vol 1 Andrus, W.D. (ed.) New York, NY: IntersciencePublishers, 269-336, 1949.
Webster, D.R., Woolhouse, F.M. and Johnston, J.L. IimmersionFoot. Journal of Bone and Joint Surgery 24:785-94, 1942.
Weinberg, A.D., Hamlet, M.P., Paturas, J.L., McAninch, G.W.and White, R.W. (eds.) Cold Weather Emergencies: Principles ofPatient Management. Branford, CN: American Medical Publishing,1990
55
BIBUOGRAPHY
Adam, J.M. and Goldsmith, R. Cold Climates. In: O.G. Edholmand A.L. Bacharach (eds) Exploration Medicine. Bristol, UK: JohnWright and Sons, 1965.
Department of the Army. Brigade and Division Surgeon's•. Washington, D.C.: U.S. Army Field Manual 8-10-5, 10
June 1991.
Burton, A.C. and Edholm, O.G. Man in a Cold Environment:Physiological and Pathological Effects of Exposure to LowT _ atu . London: Edward Arnold, 1955.
Daniels, F. Jr. Physiologic Factors in the Skin's Reactionto Heat and Cold. In: T.B. Fitzpatrick, A.Z. Eisen, K. Wolff,I.M. Freedberg, K.F. Austen (eds) Dermatoloay in GeneralM. (3rd edition). New York,NY: McGraw-Hill, 1987.
Danzl, D.F. Accidental Hypothermia. In: P. Rosen, F.J.Baker II, R.M. Barkin, G.R. Braen, R.H. Dailey and R.C. Levy(eds) Emergency Medicine. Concepts and Clinical Practice. St.Louis, MO: C. V. Mosby, 1988.
Danzl, D.F., Pozos, R.P., and Hamlet, M.P. AccidentalHypothermia. In: P.S. Auerbach and R.S. Geehr (eds) Mau |of Wilderness and Environmental Emergencies. (2nd ed.) St.Louis, MO: C. V. Mosbv, 1989.
Denny-Brown, D., Adams, R.D., Brenner, C., Doherty, M.M.Pathology of injury to nerve induced by cold. JNeuropathology and Experimental Neurology 40:305-23, 1945.
Dubas, F. and Valloton, J. (eds.) Color Atlas of MountainMedicine. St. Louis, MO: Mosby-Year Book, 1991.
Hamlet, M.P. Human Cold Injuries. In: K.B. Pandolf, M.N.Sawka and R.R. Gonzalez (eds.) Human Performance Physiology andEnvironmental Medicine at Terrestrial Extremes. Indianapolis,IN: Benchmark Press, 1988.
Kalant, H. and Le, A.D. Effects of Ethanol onThermoregulation. In: E. Schonbaum and P. Lomax (eds)Thermregulation: Pathology, Pharmacology and Therapy: Section132. International Encyclopedia of Pharmacology and Therapeutics.New York, NY: Pergamon Press, 1991.
56
Kennet, R.P. and Gilliatt, R.W. Nerve conduction studies inexperimental nonfreezing cold injury: II. Generalized nervecooling by limb inversion. Muscle and Nerve 14:960-967. 1991.
Lloyd, E.L. Hypothermia and Cold Stress. Rockville, MD:Aspen Systems Corporation, 1986.
McClellan, W.B. Work Under Low Temperatures and Reactionsto Cold Stress. In: Carl Zenz (ed.) Occupational Medicine (2nded.) Chicago, IL: Year Book, 1988.
Paton, B.C. Accidental Hypothermia. In: E. Schonbaum and P.Lomax (eds) Thermoregulation: Pathology. Pharmacology andery: Section 132. International Encyclopedia of Pharmacology
and Therapeutics. New York, NY: Pergamon Press, 1991.
Paton, B.C. Accidental Hypothermia - Update 1988. In:Schonbaum, E. and Lomax, P., (eds) Thermoregulation: PatholoQgyPharmacology and Therapy: Section 132. International Encyclopediaof Pharmacology and Therapeutics. New York, NY: Pergamon Press,1991.
Santee, W.R. and Gonzalez, R.R. Characteristics of theThermal Environment. In: K.B. Pandolf, M.N. Sawka and R.R.Gonzalez (eds.) Human Performance PhysioloQgy and EnvironmentalMedicine at Terrestrial Extremes. Indianapolis, IN: BenchmarkPress, 1988.
Shaw, J.F. Frostbite. Inz P. Rosen, F.J. Baker II, R.M.Barkin, G.R. Braen, R.H. Dailey and R.C. Levy (eds) EMedicine. Concepts and Clinical Practice. St. Louis, MO: C. V.Mosby, 1988.
Smith, D.J. Jr., Robson, M.C., and Heggers, J.P. Frostbiteand Other Cold Induced Injuries. In P.S. Auerbach and R.S. Geehr(eds) Management of Wilderness and Environmental Emergencies.(2nd ed.) St. Louis, MO: C. V. Mosby, 1989.
Steinmann, A.M. and Hayward, J.S. Cold-Water Immersion. In:P. S. Auerbach and E. S. Geehr (eds) Management of Wilderness andEnvironmental Emergencies (2nd ed.) St. Louis, MO: C. V. Mosby,"1989.
Stoner, H.B. and Randall, P.E. The Metabolic Aspects ofHypothermia. In: R. D. Cohen, B. Lewis, K. G. M. M. Alberti andA. M. Denman (eds) The Metabolic and Molecular Basis of AcquiredDisease. Philadelphia, PA: Bailliere Tindall, W. B. Saunders,1990.
57

Taylor, C.A. Surgical Hypothermia. In: E. Schonbaum and P.Lomax (eds) Thermoregulation: Pathology. Pharmacology andTherap•*. Section 132. International Encyclopedia of Pharmacologyand Therapeutics. New York, NY: Pergamon Press, 1991.
Toner, M.M. and McArdle, W.D. Physiological Adjustments ofMan to'the Cold. in K. B. Pandolf, M. N. Sawka and R. R. Gonzalez(eds) B=man Performance Physiology and Environmental Medicine atTerrestrial Extremes. Indianapolis, IN: Benchmark Press, 1988.
Winter Operations Manual. Fort Greely, AK: U.S. ArmyNorthern Warfare Training Center, Deprtment of the Army, 1October 1989.
Weinberg, A.D., Hamlet, M.P., Paturas, J.L., McAninch, G.W.and White, R.W. (eds.) Cold Weather Emergencies: Principles ofPatient Management. Branford, CN: American Medical Publishing,1990
Whayne, T.F. and DeBakey, M.E. Cold Injury. Ground Type, inWorld War II. Washington, D.C.: Office of the Surgeon General,Department of the Army, 1958.
Wilkerson, J.A., Bangs, C:C. and Hayward, J.S. HypQthermia.Frostbite and Other Cold Injuries. Seattle, WA: TheMountaineers, 1986.
Young, A.J. Human Adaptations to Cold. In: K.B. Pandolf,M.N. Sawka arid R.R. Gonzalez (eds.) Human Performance Physiologyand Environmental Medicine at Terrestrial Extremes.Indianapolis, IN: Benchmark Press, 1988.
Young, A.J., Roberts, D.E., Scott, D.P., Cook, J.E., Mays,M.Z., and Askew, E.W. Sustaining Health and Performance in theCold: Environmental Medicine Guidance for Cold Weather(nerations. Natick, MA: U.S. Army Research Institute ofEnvironmental Medicine, Technical Note 92-2, 1992. (AD A254 328)
Young, A.J., Roberts,D.E., Scott, D.P., Cook, J.E., Mays,M.Z., and Askew, E.W. Sustainina Health and Performance in theCold: A Pocket Guide to Environmental Medicine Aspects of ColdWeather Operations. Natick, MA: U.S. Army Research Institute ofEnvironmental Medicine, Technical Note 93-2, 1992. (AD A259 920)
58