acute!lower!gastrointestinal!bleeding!in!the! …
TRANSCRIPT

! 1!
!ACUTE!LOWER!GASTROINTESTINAL!BLEEDING!IN!THE!
UNITED!KINGDOM!!
!!
Candidate:!Miss!Kathryn!Oakland!MBBS!BSc!MRCS!!!!!
Imperial!College!London,!National!Heart!and!Lung!Institute!!
AND!!
NHS!Blood!and!Transplant,!Oxford!!!!!!
Submitted!for!MD(Res)!!!!
!!!!!!!!!!!!!!!!!!!!!!!
! 2!
Declaration!of!originality!!!!
The!work! contained! in! this! thesis,! unless! otherwise! referenced,! is! entirely!my!
own.! Statistical! advice! for! chapters! 3O5!was! provided! by! Frances! Seeney! (NHS!
Blood! and! Transplant)! although! I! performed! the! associated! analyses.! Where!
specialist! statistical! analysis!was! required,! this!was! conducted! by! Gary! Collins!
(Professor! of! Statistics,! Centre! for! Statistics! in!Medicine,! University! of! Oxford)!
and!Paul!Bassett!(independent!statistical!consultant)!and!this!is!referenced!in!the!
methods!sections!of!chapters!6!and!7,!respectively.!
!
!Copyright!declaration!!!!The!copyright!of!this!thesis!rests!with!the!author!and!is!made!available!under!a!
Creative! Commons! Attribution! NonOCommercial! No! Derivatives! license.!
Researchers!are! free! to!copy,!distribute!or! transmit! the! thesis!on! the!condition!
that! they!attribute! it,! that! they!do!not!use! it! for! commercial!purposes!and! that!
they! do! not! alter,! transform! or! build! upon! it.! For! any! reuse! or! redistribution,!
researchers!must!make!clear!to!others!the!license!terms!of!this!work.!
!
!
!
!
!
!
!

! 3!
Abstract!!
Introduction!
Lower!gastrointestinal!bleeding!(LGIB)!is!a!common!medical!emergency.!Despite!
this,! there! are! few! data! on! presentations,! interventions! and! patient! outcomes.!
The!aim!of! this! research! is! to!describe! the! epidemiology!of! LGIB! in! the!United!
Kingdom,! appraise! clinical! interventions! and! develop! a! risk! score! to! optimise!
patient!triage.!
!
Methods!
A!systematic!review!(SR)!of!common!interventions!for!LGIB!was!undertaken.!A!
prospective!national!observational! study!of!LGIB!presentations! to!UK!hospitals!
during!two!months!in!2015!was!conducted,!collecting!data!on!demographics!and!
outcomes! (reObleeding,! death,! reOadmission).! Frequency! of! intervention! was!
compared!to!that!identified!in!the!SR.!Multivariable!logistic!regression!was!used!
to! develop! a! risk! score! to! predict! need! for! hospitalisation,! and! independently!
validated! using! cases! collected! by! two! additional! acute! hospitals! using! CO
statistics.!
!
Results!
The! SR! identified! that! colonoscopy! within! 24! hours! of! presentation! was!
associated!with!a!higher!diagnostic!yield!and!a!reduced!length!of!hospitalisation.!
In! total! 143/174! (82.2%)! acute! hospitals! in! the! UK! participated! in! the!
observational! study,!providing!data!on!2528!cases!of!LGIB.!Most!patients!were!
elderly!(median!age!74!years)!with!major!coOmorbidities,!including!29.4%!taking!

! 4!
antiplatelets!drugs.!Only!52%!patients!underwent! inpatient! investigation,!3.9%!
receiving! colonoscopy.!Median! length! of! stay!was! 3! days! and! 85/2528! (3.4%)!
died!during!admission.!Data!from!2336!acute!admissions!were!used!to!develop!
the! risk! score,! identifying! that! >60%! patients! could! avoid! hospital! admission.!
Age,! gender,! previous!LGIB!admission,! blood!on! rectal! examination,! heart! rate,!
systolic!blood!pressure!and!haemoglobin!strongly!discriminated!safe!discharge!
(cOstatistic!0·84,!95%!confidence!interval!0·82!to!0·86).!!
!
Conclusion!
Few! patients! admitted! with! LGIB! require! treatment! for! bleeding,! or! come! to!
harm.! Many! could! safely! be! managed! as! an! outpatient.! We! developed! and!
validated!a!clinical! risk!score!with!good!discriminative!performance! to! identify!
these!patients.!!
!
!
!
!
!
!
!
!
!
!
!
!

! 5!
Acknowledgements!
The!idea!for!a!national!study!of!lower!gastrointestinal!bleeding!was!conceived!by!
Prof.!Mike!Murphy! and!Dr! Vipul! Jairath!without!whom! this! project!would! not!
have! been! possible.! Mike! offered! continuous! support,! encouragement! and!
moderation!when!needed.!No!one!replies!faster!to!emails!(even!whilst!abroad),!
meaning!that!I!always!had!direction,!and!was!the!envy!of!the!other!postOgraduate!
students.!!Vip!was!a!great!mentor!and!role!model.!He!was!full!of!inspiration!and!
encouragement! to! aim! high.! The! reputation! of! NHSBT! opened! doors! for! this!
project!that!would!have!remained!shut!for!simpler!studies,!and!even!kindled!the!
interest! of! busy! general! surgical! teams,! who!would!much! rather! be! operating!
than! trawling! the! wards! for! ‘PR! bleeders’.! I! was! able! to! make! full! use! of! the!
logistical! support! offered! by! the! NHSBT! team,! notably! John! GrantOCasey,! who!
offered!unending!patience.!!Mike!Schachter!provided!a!welcome!external!opinion!
and!Mike!Desborough!was! the! invaluable!sounding!board! I!was!able! to!bounce!
ideas! off! throughout! this!work.! Lastly! I!must! thank!my!partner!Bill!Hemstock.!
Never!has!a!professional!golfer!known!so!much!about!endoscopy,!metaOanalysis!
and!diverticular!disease.!!
!

! 6!
Contents!!!List!of!publications!and!presentations!arising!from!this!thesis………………………..8!List!of!abbreviations……………………………………………………………………………………10!List!of!tables………………………………………………………………………………………………..11!List!of!figures………………………………………………………………………………………………13!
1. Introduction!i. What!is!known!about!acute!lower!gastrointestinal!bleeding?......14!ii. Aims!of!the!thesis..…………………………………………………………………32!iii. Outline!of!thesis…………………………………………………………………….32!
2. Systematic!review!i. Introduction………………………………………………………………………….33!ii. Methods………………………………………………………………………………..34!iii. Characteristics!of!reviewed!studies………………………………………..41!iv. Choice!of!investigation…………………………………………………………..48!v. Timing!of!first!line!investigation…………………………………………….51!vi. Choice!of!treatment!………………………………………………………………57!vii. Assessment!of!methodological!quality……………………………………59!viii. Implications!for!practice!in!the!United!Kingdom…………………….63!
3. National!observational!study!methods!i. Recruitment!of!sites………………………………………………………………68!ii. Case!identification!and!Pilot!Study!1………………………………………69!iii. Data!collection………………………………………………………………………72!iv. Pilot!Study!2………………………………………………………………………….74!v. Data!analysis…………………………………………………………………………76!vi. Definitions…………………………………………………………………………….79!vii. Ethical!considerations……………………………………………………………80!
4. National!observational!study:!patient!results!i. Introduction,!aims!and!objectives…………………………………………..81!ii. Sample!size…………………………………………………………………………...82!iii. Patient!characteristics……………………………………………………………84!iv. Use!of!blood!components……………………………………………………….87!v. Endoscopy!and!endoscopic!haemostasis…………………………………90!vi. Radiology………………………………………………………………………………92!vii. Surgery…………………………………………………………………………………93!viii. Clinically!significant!bleeding…………………………………………………95!ix. Patients!undergoing!no!inpatient!investigations……………………..95!x. Outcomes……………………………………………………………………………...96!xi. Discussion…………………………………………………………………………..104!
5. National!observational!study:!organisation!of!services!i. Endoscopy………………………………………………………………………….110!ii. Interventional!radiology……………………………………………………..112!iii. Specialist!elderly!care…………………………………………………………113!iv. Guidelines…………………………………………………………………………..114!v. Discussion………………………………………………………………………….115!
6. Risk!score!i. Introduction……………………………………………………………………….120!ii. Additional!methods…………………………………………………………….121!

! 7!
i. Study!design!and!participants…………………………………121!ii. Study!outcomes………………………………………………………122!iii. Statistical!analysis…………………………………………………..122!iv. Comparative!assessment!with!previously!described!
scores…………………………………………………………………….124!iii. Results!
i. Demographics!and!presenting!features……………………126!ii. Predicting!safe!discharge…………………………………………129!iii. Comparison!of!the!new!score!with!previously!published!
scores…………………………………………………………………….135!iv. Discussion……………………………………………………………………………136!
7. Antiplatelet!and!anticoagulant!agents!!i. Introduction…………………………………………………………………………144!ii. Additional!methods………………………………………………………………146!iii. Management!of!antiplatelets!and!anticoagulants……………………152!iv. Antiplatelets!and!cardiovascular!outcomes……………………………159!v. Discussion……………………………………………………………………………163!
8. Conclusions…………………………………………………………………………………….169!i. Suggestions!for!future!work………………………………………………….175!
References……………………………………………………………………………………………..…178!Appendices……………………………………………………………………………………………….190!Publisher!permissions……………………………………………………………………………….197!!!!!!

! 8!
Publications!and!presentations!arising!from!this!thesis!!!Chapter!2:!Oakland!K,!Isherwood!J,!Lahiff!C,!Goldsmith!P,!Desborough!M,!Colman!KS,!Guy!R,!Uberoi!R,!Murphy!MF,!East!JE,!Hopewell!S,!Jairath!V.!Diagnostic!and!therapeutic!treatment!modalities!for!acute!lower!gastrointestinal!bleeding:!a!systematic!review.!Accepted!for!publication,!Endoscopy)International)Open.)!Chapter!3:!Oakland!K,!Guy!R,!Uberoi!R,!Seeney!F,!Collins!G,!GrantOCasey!J,!Mortensen!N,!Murphy!M,!Jairath!V!on!behalf!of!the!National!Comparative!Audit!in!Blood!Transfusion!Lower!Gastrointestinal!Bleeding!Working!Group.!Study!Protocol:!First!nationwide!comparative!audit!of!acute!lower!gastrointestinal!bleeding!in!the!United!Kingdom.!BMJ)Open.!2016!Aug!4;6(8):e011752.!doi:!10.1136/bmjopenO2016O011752.!!Chapter!4:!Oakland!K,!Guy!R,!Uberoi!R,!Hogg!R,!Mortensen!N,!Murphy!MF,!Jairath!V!on!behalf!of!the!UK!Lower!GI!Bleeding!Collaborative.!Acute!lower!gastrointestinal!bleeding!in!the!UK:!patient!characteristics,!interventions!and!outcomes!in!the!first!nationwide!audit.!Gut.!2017!Feb!1.!doi:!10.1136/gutjnlO2016O313428.!!Chapter!6:!Oakland!K!and!Jairath!V,!Uberoi!R,!Guy!R,!Ayaru!L,!Mortensen!N,!Murphy!MF,!!Collins!GS.!Safe!discharge!after!acute!lower!gastrointestinal!bleeding:!derivation!and!validation!of!a!novel!risk!score.!Lancet)Gastroenterology)and)Hepatology,!2017!Jun!23!doi:!10.1016/S2468O1253(17)30150O4! )Plenary)Lectures))Achieving!clinical!excellence!with!PR!bleeding!patients.!2nd!Emergency!Surgery!Conference,!Oxford,!16th!September!2016!!Lessions! Learned! from! the! National! Lower! Gastrointestinal! Bleeding! Audit.!Research! and! audit! in! the! emergency! setting! session,! Association! of!Coloproctology! of! Great! Britain! and! Ireland! Annual! Meeting,! Edinburgh,! July!2016!!!Oral)Presentations))Oakland!K,!Babra!P,!GrantOCasey!J,! Jairath!V,!Guy!R,!Mortensen!N,!Murphy!MF,!Uberoi!R.!The!use!of!radiology!for!haemorrhage!control!in!lower!gastrointestinal!bleeding:! results! from! a! national! comparative! audit.! British! Society! of!Interventional!Radiology,!Manchester,!15O17th!November!2016!)
! 9!
)Poster)Presentations)!Oakland!K,!GrantOCasey!J,!Jairath!V,!Guy!R,!Mortensen!N,!Murphy!MF,!Uberoi!R.!The! provision! of! interventional! radiology! for! the! treatment! of! lower!gastrointestinal! bleeding:! results! from! a! nationwide! audit.! British! Society! of!Interventional!Radiology,!Manchester,!15O17th!November!2016!!Oakland!K,!Guy!R,!Uberoi!R,!GrantOCasey!J,!Mortensen!N,!Jairath!V,!Murphy!MF!on! behalf! of! the! National! Comparative! Audit! in! Blood! Transfusion! Lower!Gastrointestinal! Bleeding! Working! Group.! Blood! Transfusion! in! Lower!Gastrointestinal!Bleeding:!Results!From!a!National!Study!in!the!United!Kingdom.!AABB!International!meeting,!Orlando,!October!2016!!Oakland!K,!Guy!R,!Uberoi!R,!GrantOCasey!J,!Mortensen!N,!Murphy!MF,!Jairath!V.!Outcomes!of!acute!lower!gastrointestinal!bleeding:!data!from!a!large!nationwide!audit.!United!European!Gastroenterology!Week,!Vienna,!October!2016!
!Oakland!K,!Uberoi!R,!GrantOCasey!J,!Murphy!MF,!Jairath!V,!Mortensen!N,!Guy!R.!The!use!of!surgery!in!the!management!of!acute!lower!gastrointestinal!bleeding:!results! from! a! large! national! audit.! European! Society! of! Coloproctology,!Milan,!30th!September!2016!!Oakland! K,! GrantOCasey! J,! Jairath!V,! Guy!R,! Mortensen!N,! Murphy!M,! Uberoi!R.!Provision! of! interventional! radiology,! endoscopy! and! surgery! for! acute! lower!gastrointestinal! bleeding! in! the! United! Kingdom:! preliminary! results! of! a!national! comparative! audit.! Cardiovascular! and! Interventional! Radiological!Society!of!Europe!(CIRSE),!Barcelona,!September!2016!!!

! 10!
List!of!abbreviations!!!CI!–!confidence!interval!CTA!–!computerised!tomographic!angiography!DAPT!–!dual!antiplatelet!drug!therapy!DOAC!–!direct!oral!anticoagulant!DRE!–!digital!rectal!examination!EUA!–!examination!under!anaesthesia!EBL!–!endoscopic!band!ligation!FFP!–!fresh!frozen!plasma!Hb!O!haemoglobin!HctO!haematocrit!HES!–!hospital!episode!statistics!HRO!heart!rate!ICD!–!International!Classification!of!Diseases!ICU!–!intensive!care!unit!INR!–!international!normalised!ratio!IQR!–!interquartile!range!IR!–!interventional!radiology!LGIB!–lower!gastrointestinal!bleeding!LOS!–!length!of!stay!MA!–!mesenteric!angiography!NCEPOD!–!National!Confidential!Enquiry!into!Patient!Outcomes!and!Death!MD!–!mean!difference!MI!–!myocardial!infarction!NHS!–!national!health!service!NICEO!National!Institute!of!Health!and!Care!Excellence!NRSI!–!nonOrandomised!studies!of!intervention!NSAID!–!nonOsteroidal!antiOinflammatory!drug!OGDO!oesophagogastroduodenoscopy!OR!–!odds!ratio!PCC!–!prothrombin!complex!concentrate!PH!–!proportional!hazards!RBC!–!red!blood!cell!RCT!–!randomised!controlled!trials!RR!–!risk!ratio!SBP!–!systolic!blood!pressure!SD!–!standard!deviation!UGIB!–upper!gastrointestinal!bleeding!UK!–!United!Kingdom!!!!!!!!!
! 11!
List!of!tables!!!Table!1:!! Summary!of!evidence!by!comparison!investigated!and!study!
methodology!!Table!2:! !Study!characteristics!!Table!3:!! InterOstudy!variability!of!the!definition!of!reObleeding!
Table!4:!! Assessment! of! methodological! quality;! Cochrane! risk! of! bias! for!RCTS,!NewcastleOOttawa!for!NRSI!
!Table!5:! !Pilot!case!identification!tool!!Table!6:!! Study!definitions!!Table!7:!! Presenting!features!and!demographics!of!patients!admitted!with!or!
who!developed!LGIB!whilst!an!established!inpatient!!Table!8:!! Inpatient!Interventions!for!LGIB!!Table!9:!! The!frequency!of!shock!and!transfusion!by!admitting!Hb!!Table!10:! !Patients!who!required!emergency!laparotomy!for!LGIB!!Table!11:!! Discharge!diagnoses!by!age!!Table!12:!! Outcomes! and! cause! of! death! in! patients! admitted! with! or! who!
developed!LGIB!whilst!an!established!inpatient!!Table!13:!! The!availability!of! in!and!out!of!hours! lower!GI!endoscopy! in! the!
UK!!Table!14:!! The!availability!of! in!and!out!of!hours! interventional!radiology! in!
the!UK!!Table!15:!! Demographic!data!for!candidate!variables!in!the!development!and!
validation!cohort!!Table!16:!! Sources!of!bleeding!!Table!17:!! Diagnostic!and!therapeutic!interventions!!Table!18:!! Final!prediction!model!for!safe!discharge!!Table!19:!! A!score!to!predict!the!safe!discharge!of!patients!presenting!with!a! ! cute!LGIB!!

! 12!
Table!20:!! Probability!of!safe!discharge!by!total!score!!Table!21:!! Number!of!patients!safely!discharged!by!score!!Table!22:! !COstatistics!for!the!new!model!against!existing!models!for!safe!
discharge!and!adverse!clinical!outcomes.!!POvalues!are!from!the!DeLong!test,!with!reference!to!the!new!model.!
!Table!23:!! Patient!characteristics!by!drug!group!!Table!24:!! Interventions!for!LGIB!by!antiplatelet!and!anticoagulant!exposure!!Table!25:!! Sources!of!LGIB!by!drug!exposure!!Table!26:!! Unadjusted!patient!outcomes!!Table!27:!! Univariate!and!multivariate!regression!models!for!reObleeding,!reO
admission!with!bleeding,!mortality!and!adverse!cardiovascular!outcomes!
!Table!28:!! Unadjusted!patient!outcomes!in!patients!who!were!receiving!a!
single!antiplatelet!and!had!it!continued!and!those!that!had!it!interrupted!
!Table!29:! Univariate!and!multivariate!regression!models!for!reObleeding,!reO
admission!with!bleeding,!mortality!and!adverse!cardiovascular!outcomes!in!patients!receiving!a!single!antiplatelet!drug!
!!!!!!!!!!!!!!!!!!!!!!
! 13!
List!of!figures!!!Figure!1:!! PRISMA!flowOchart!of!eligible!studies!
Figure!2:!! Forest!plot!of!comparison!of!NRSI!a)!presumptive!diagnoses,!b)!definite!diagnoses.!95%!CI,!95%!confidence!interval!
!Figure!3:!! Forest!of!plot!of!comparison!of!NRSI!a)!therapeutic!yield,!b)!length!
of!stay.!95%!CI,!95%!confidence!interval!!Figure!4:!! Flow!chart!of!excluded!and!included!cases!!Figure!5:!! The!relationship!between!Charlson!CoOmorbidity!Index!and!death!
and!reObleeding!!Figure!6:!! Calibration!plot!of!the!final!prediction!model!for!safe!discharge!in!
the!validation!cohort.!95%!CI!around!the!observed!predictions!(triangle)!at!tenths!of!predicted!risk.!
!Figure!7:!! The!distribution!of!scores!and!associated!proportion!of!safe!
discharges!!!Figure!8:!! FlowOchart!of!cases!! !Figure!9:!! KaplanOMeier!graph!of!time!to!inOhospital!reObleeding!!
!!!!!!!!!!!!!!!!!!!!

! 14!
CHAPTER!ONE:!INTRODUCTION!!!1.1!What!is!known!about!acute!lower!gastrointestinal!bleeding?!!!
Acute! lower! gastrointestinal! bleeding! (LGIB)! is! a! common! acute! medical! and!
surgical!emergency.!In!contrast!to!upper!gastrointestinal!bleeding!(UGIB),!which!
has!several!published!guidelines,1!is!well!researched!and!has!seen!improvements!
in! clinical! outcomes,2! LGIB! has! not! been! a! focus! for! clinical! or! scientific!
investigation.!In!the!United!Kingdom!(UK)!LGIB!is!a!leading!indication!for!red!cell!
(RBC)! transfusion,3! but! unlike!UGIB,!most! cases! are! considered! to! resolve! and!
stop!bleeding!without!intervention.4!5!In!2015!the!National!Confidential!Enquiry!
in! Patient! Outcomes! and! Death! (NCEPOD)! published! a! report! on! severe!
gastrointestinal!bleeds!that!found!that!only!44%!of!patients!received!good!care.6!
This! is! at! least! partly! the! result! of! the! lack! of! high! quality! research! into! the!
management!of!patients!that!present!with!LGIB,!a!problem!that!this!thesis!aims!
to!address.!
!
Definition)
!
Traditionally!UGIB!and!LGIB!have!been!distinguished!by!the!origin!of!bleeding!in!
relation! to! the! ligament! of! Treitz.! UGIB! corresponds! to! bleeding! in! the!
oesophagus,!stomach!and!duodenum,!whereas!LGIB!encompasses!bleeding!in!the!
small! bowel,! colon! and! anorectum.! Developments! in! options! for! investigating!
bleeding! in! the! small! bowel!have! lead! to! the! emergence!of! a! the! term! ‘midOGI’!
bleeding,7! corresponding! to! bleeding! originating! in! the! jejunum! and! ileum.! At!
! 15!
presentation! LGIB! can! cause! bright! rectal! bleeding,! clots,! blood!mixed! in!with!
stool! as!well! as!melaena,! although! the! latter!may! indicate! an!upperO!or!midOGI!
source.!!
)
Global)Incidence)
!
Although!LGIB! is! common!condition,! there! are! limited! studies!documenting! its!
incidence.!A!population!based!study!in!ten!hospitals!in!Spain!compared!patients!
discharged!with!hospital!codes!consistent!with!GI!complications!over!ten!years.!
It!was! found! that! in! comparison! to! the! upper! GI! tract,!where! the! incidence! of!
complications!fell!from!87/100,000!to!47/100,000!over!ten!years,!the!incidence!
of! complications! in! the! lower! GI! tract! increased! from! 20/100,000! to!
33/100,000.2!The!results!of!the!aforementioned!study!are!limited!by!its!sample!
size;! results! were! extrapolated! from! ten! hospitals! to! calculate! a! national!
incidence.!Additionally!cases!were!captured!using!discharge!codes!that!included!
GI! complications! not! related! to! bleeding.! A! group! in! Iceland! calculated! an!
incidence! of! 87/100,000! for! LGIB! by! multiplying! the! number! of! endoscopy!
referrals!for!the!investigation!of!rectal!bleeding!or!melaena!to!a!single!hospital!in!
2010.8! This! method! also! comprised! a! small! number! of! patients! and! may! be!
inaccurate!as!endoscopy!is!not!the!sole!mode!of!investigation!of!LGIB.!Historical!
studies!estimate!the!incidence!of!LGIB!as!20.5/100,000!but!again!this!is!based!on!
data!from!a!single!centre.9!
!
There!are!no!data!on!the!incidence!of!LGIB!in!the!UK.!A!systematic!review!of!the!
literature!and!hospital!episode!data!was!unable!to!quantify!the!incidence!of!LGIB!
! 16!
but! did! report! that! it! accounts! for! 20%!of! all! GI! bleeding.10! In! the!UK,! LGIB! is!
typically!managed!by!surgeons!and!represents!3%!of!surgical!referrals.11!
!
Patient)Demographics,)CoCmorbidity)and)Pharmacotherapy)
!
Studies!of!hospital!registries!have!shown!that!patients!that!develop!LGIB!tend!to!
be! elderly,! with! a!mean! age! of! 63O69! years.11!12! CoOmorbid! illness! is! common,!
78%!admitted!patients!have!>1!coOmorbid!conditions,13!33%!have!≥2.12!Aspirin!
for!secondary!prevention!is!used!in!20O33%,13!clopidogrel!in!3.2%!and!warfarin!
in! 6%! patients.14! There! are! no! published! data! on! the! number! of! patients!
admitted!with!LGIB!who!are!receiving!a!direct!oral!anticoagulant!(DOAC).!!
!
PopulationObased!database!studies!suggest!an!increased!risk!of!developing!LGIB!
with! aspirin8! or! longOterm! oral! nonOsteroidal! antiOinflammatory! drug! (NSAID)!
use.15!16!Inhibition!of!cycloOoxygenase!1!by!NSAIDs!and!aspirin!is!associated!with!
reduced! levels! of! protective!mucosal! prostaglandins17!which! induces! intestinal!
ulceration.18!Unlike!the!upper!GI!tract!where!this!effect!may!be!mitigated!by!the!
concomitant!use!of!proton!pump!inhibitors,!in!the!lower!GI!tract!these!drugs!may!
lead! to! an! increase! in! bleeding.19! 20! In! the! colon,! animal! studies! suggest! that!
NSAIDs! and! aspirin! are! additionally! associated! with! derangements! in! the!
microbiome!leading!to!mucosal!inflammation!and!a!propensity!for!bleeding.21!
!
Vitamin!K!antagonists!are!also!associated!with!developing!of!LGIB,16!22!increased!
severity!of!bleeding!when!it!occurs,8!and!are!a!risk!factor!for!mortality.12!Unlike!
NSAIDs!and!aspirin,! the!effects!of!oral!anticoagulants!are!most! likely! limited!to!

! 17!
disruption!of!coagulation!as!opposed!to!local!effects!on!the!intestine.!DOACs!are!
increasingly! used! as! alternatives! to! warfarin! due! to! their! more! predictable!
pharmacodynamics!and!improved!side!effect!profiles.!However,!pooled!analyses!
from! randomised! controlled! trials! indicate! that! in! comparison! to! warfarin,!
patients!receiving!DOACs!have!an!increased!risk!of!GIB.23!24!There!are!currently!
no! published! data! on! the! outcomes! of! DOAC! patients! who! develop! LGIB,! and!
guideline! recommendations! on! the! management! of! DOAC! associated! LGIB! are!
based!on!preclinical!information!and!expert!opinion.25!
!
Retrospective! database! studies! have! also! suggested! links! between!
bisphosphonates!and! selective! serotonin! reOuptake! inhibitors!and!an! increased!
risk!of!LGIB,26!27!but!whether!this!risk!is!clinically!significant!remains!unclear.!!
!
Transfusion)
!
RBC! transfusion! is!employed! in!21O40%!patients!admitted!with!LGIB.8!12! In! the!
UK,! GIB! is! the! second! most! common! indication! for! RBC! transfusion! after!
haematological!malignancy,!LGIB!accounting!for!half!of!all!transfusions!for!GIB.3!!
!
In! certain! settings! such!as! critical! care!and!cardiac! surgery,! there! is! increasing!
evidence! that! liberal! RBC! transfusion!may! have! no! advantage! over! restrictive!
transfusion,28! and! that! in! some! patients! it! may! be! harmful,! reducing! 30Oday!
survival.29!In!its!2015!transfusion!guideline,!the!National!Institute!for!Health!and!
Care! Excellence! (NICE)! recommended! using! restrictive! RBC! transfusion! in! all!

! 18!
patients! who! require! transfusion! without! major! bleeding,! acute! coronary!
syndrome!or!chronic!anaemia!requiring!regular!transfusions.30!!
!
In!the!GIB!setting,!evidence!for!liberal!transfusion!is!less!clear.!In!UGIB!there!are!
three! major! trials! of! restrictive! and! liberal! RBC! transfusion.! Villarejo! et) al!
randomised! 60! stable! UGIB! patients! to! receive! RBC! transfusion! once! their!
haematocrit!(Hct)!reached!<28%!(liberal!arm)!or!<21%!(restrictive!arm).31!The!
authors!reported!no!difference!between!the!groups!in!terms!of!length!of!stay!or!
‘organ! failure’,! although! 33! patients! were! lost! to! followOup.! Villanueva! et) al)
conducted! a!much! larger! trial,! randomising! 889! patients! to! receive! single! unit!
transfusions! at! a! haemoglobin! (Hb)! threshold! of! <70g/L,! with! further!
transfusions! to! maintain! a! target! of! 70O90g/L! (restrictive! arm),! or! to! receive!
single!unit!transfusions!at!a!Hb!threshold!of!<90g/L,!with!a!target!of!90O100!g/L!
(liberal!arm).32!Patients!were!enrolled!from!a!single!centre!after!being!admitted!
with! UGIB! of! any! aetiology.! Exclusions! included! massive! exsanguinating!
haemorrhage,!mild!bleeding!(signified!by!a!Blatchford!score!of!0)!and!a!history!of!
ischaemic!cardiovascular!disease.!Overall!mortality!data!demonstrated!improved!
45Oday! survival! with! a! restrictive! strategy.! The! effect! was! most! marked! in!
patients!with!chronic!liver!disease!(ChildOPugh!class!A!or!B)!with!a!hazard!ratio!
of!0.30!(95%!confidence!interval,!CI,!0.11!to!0.85).!In!patients!with!peptic!ulcer!
bleeding,! which! is! more! akin! to! aetiologies! seen! in! LGIB,! there! was! no! effect!
(hazard!ratio!0.70,!95%!CI!0.26!to!1.25).!Similar!results!were!seen!in!reObleeding,!
with!an!overall!reduction!in!further!bleeding!in!the!restrictive!arm!(hazard!ratio!
0.62,!95%!CI!0.43!to!0.91),!which!was!most!marked!in!cirrhotic!patients!(hazard!
ratio! 0.49,! 95%! CI! 0.27! to! 0.90)! and! not! seen! in! patients! with! peptic! ulcer!
! 19!
bleeding! (hazard! ratio! 0.63,! 95%!CI! 0.37! to! 1.07).! There! are! limitations! to! the!
generalisability!of!this!trial.!All!patients!received!oesophagogastroduodenoscopy!
(OGD)!within!six!hours,!which!is!not!feasible!in!many!hospitals.!Variceal!bleeds!
represented!24%!of!the!study!population,!which!is!not!representative!of!the!UK,!
where! they! represent! 11%.33! Jairath!et)al)attempted! to! reproduce! this! in! a!UK!
population! in! a! cluster! randomised,! feasibility! trial.34! Across! six! hospitals! 941!
patients!with!UGIB!of!any!aetiology!were!randomised!to!receive!RBC!at!a!Hb<80!
g/L!with!a!target!of!81O100g/L!(restrictive)!or!Hb<100g/L!with!a!target!of!101O
120g/L! (liberal).! Exclusions! included! only! exsanguinating! haemorrhage.! There!
was! no! significant! difference! between! treatment! arms! in! terms! of! further!
bleeding,! allOcause! mortality,! frequency! of! intervention! or! length! of! stay.! This!
trial!also!has!limitations.!This!was!a!pilot!feasibility!trial!so!was!not!adequately!
powered!to!assess!clinical!outcomes.!There!were!many!protocol!violations,!up!to!
17%!in!the!liberal!arm,!suggesting!a!reluctance!of!clinicians!to!commit!to!a!liberal!
transfusion!strategy.!!
!
Restrictive! transfusion! may! not! be! suitable! for! all! patients.! Murphy! et) al)
randomised!2003!patients!undergoing!elective!cardiac!surgery! to!restrictive!or!
liberal! transfusion! and! found! that! there!were! significantly!more! deaths! in! the!
restrictive!arm.35!The!question!of!whether!patients!with!cardiovascular!disease!
are! suitable! for! restrictive! transfusion! has! been! investigated! in! a! recent!
systematic! review.36! This! review! included! randomised! controlled! trials! in!
patients!with!cardiovascular!disease!in!a!nonOcardiac!surgery!setting,!identifying!
11! trials! of! 3033! participants.! Clinical! settings! included! orthopaedics,! UGIB,!
cardiology,! critical! care! and! vascular! surgery.! Pooled! estimates! suggested! no!

! 20!
effect! on! 30Oday! mortality! (risk! ratio,! RR,! 1.15! 95%! CI! 0.88! to! 1.50)! but! an!
increased!risk!of!myocardial!infarction!and!cardiac!arrest!(RR!1.78,!95%!CI!1.18!
to!2.70)!with!restrictive!transfusion.36!
!
There!are!no!randomised!controlled!trials!on!restrictive!RBC!transfusion!in!LGIB.!
Although!it!is!known!how!many!RBC!transfusions!are!used!in!LGIB,3!there!are!no!
published!data!on!the!transfusion!thresholds!or!targets!that!are!being!employed!
by! clinicians.!Given! the! findings! that! restrictive! transfusion!may!not! be! safe! in!
patients! with! acute! coronary! syndrome! and! other! types! of! cardiovascular!
disease,!whether!it!should!be!adopted!in!LGIB!patients,!who!are!known!to!have!a!
high!burden!of!cardiovascular!coOmorbidity,12!is!not!known.!!
!
Investigation)and)Treatment)
!
Interventions! may! include! upper! and! lower! GI! endoscopy,! diagnostic! or!
therapeutic!radiological!studies,!nuclear!medicine!studies!and!surgery.!In!the!UK!
there! are! no! contemporary! published! data! on! the! most! common! modes! of!
investigation,! although! a! report! by! the! NCEPOD! report! on! GIB! patients! with!
severe! bleeding! (≥4! units! RBC! transfusion)! reported! that! the! most! common!
investigation!of!rectal!bleeding!was!flexible!sigmoidoscopy,!although!it!was!only!
undertaken! in! 23%! cases.6! This! is! in! contrast! to! the!United! States! (US)!where!
colonoscopy! is! the! most! common! investigation! (46%),! flexible! sigmoidoscopy!
being! performed! in! only! 4%.12! Colonoscopy! enables! visualisation! of! the! large!
bowel!in!its!entirety,!but!requires!bowel!preparation!and!may!not!be!tolerated!by!
elderly! patients.37! Flexible! sigmoidoscopy! allows! only! visualisation! of! the! left!
! 21!
sided! of! the! colon,! but! can! be! performed! following! less! invasive! bowel!
preparations.!The!diagnostic!yields!for!each!modality!in!LGIB!are!not!known.!!!
!
As! well! as! identifying! the! cause! of! bleeding,! colonoscopy! and! flexible!
sigmoidoscopy!can!be!used! to!deliver!endoscopic! therapy.!Therapeutic!options!
include! adrenaline! injection,! thermocoagulation,! clipping! and! banding.! Case!
series! have! suggested! efficacy! of! clips! or! bands! in! diverticular! bleeding,38! 39!
argon!laser!in!angiodysplasia40!and!combination!therapies!for!postOpolypectomy!
bleeding.41! There! are! no! randomised! controlled! trials! comparing! these!
modalities,!nor!are!there!data!on!their!longOterm!efficacy.!This!is!reflected!in!the!
low!utilisation!of!endoscopic!therapy!as!a!treatment!option,!used!in!only!2O4.6%!
acute!LGIB!in!the!US!and!Australia.5!12!42!
!
A! bleeding! source! may! also! be! identified! using! computerised! tomographic!
angiography! (CTA)! or!mesenteric! angiography! (MA).! If! active! extravasation! of!
contrast! is! visualised! on! angiography,! mesenteric! embolisation! offers! a!
minimally! invasive! method! to! control! haemorrhage! avoiding! the! need! for!
surgery.!Embolic!agents!include!coils,!gelfoam!and!polyvinyl!particles.!Although!
there! is! potential! risk! of! developing! associated! colonic! ischaemia! after!
embolisation,! the! development! of! superOselective! embolisation! may! to! reduce!
this.43!44!Embolisation!is!reportedly!used!in!only!1O6%!LGIB!cases,5!6!but!whether!
its! uptake! has! resulted! in! a! reduction! in! requirements! for! major! abdominal!
surgery!and!its!associated!complications!is!not!known.!!
!

! 22!
Historically,! nuclear! bleeding! scanning! has! been! used! when! the! origin! of!
bleeding! is! beyond! the! reach! of! the! endoscope.! Its! use! is! limited! by! its!
requirement!for!specialised!staff!and!radioOlabelled!tracers!and!in!the!US,!nuclear!
scans!are!generally!being!replaced!by!CTA.45!However,!it!continues!to!have!a!role!
in! the! investigation! of! small! bowel! bleeding,! such! as! that! associated! with! a!
Meckel’s! diverticulum.! Additional! modalities! for! examining! the! small! bowel!
include! capsule! endoscopy! and! push! enteroscopy.! Capsule! endoscopy! is! well!
tolerated! by! patients! but! is! not! therapeutic! and! biopsy! is! not! possible.! Push!
enteroscopy! is! reported! to! have! a! superior! diagnostic! yield! to! that! of! capsule!
endoscopy46!but!is!limited!by!the!need!for!deep!sedation!or!anaesthesia.!!
!
Surgery!for!acute!haemorrhage!control!in!LGIB!is!now!usually!reserved!for!cases!
where! endoscopic! or! radiological! therapies! fail.47! There! are! limited! reports! on!
the!number!of!cases!that!require!emergency!surgery,!case!series!reporting!its!use!
in! 4.8%! LGIB! admissions.5! Indications! include! diverticular! disease,! bleeding!
colorectal! cancers! and! angiodysplasia.48! Complications! and! mortality! are!
reported! in! 60.3%! and! 15.9%! cases,! respectively.48! This! warrants! further!
concern!considering! that! those! that! survive!an!emergency! laparotomy!(for!any!
pathology)!face!a!1Oyear!mortality!of!25%.49!
!
Diagnoses)
)
Multicentre! database! studies! in! the! US! and! Europe! suggest! that! the! most!
common! sources! of! bleeding! are! diverticular! disease! (32.0O33.1%),!
haemorrhoids! (10.0O20.0%),! colonic! polyps! (13.1%)! and! colitis! (11.7%).12! 50!

! 23!
There!are!no!equivalent! studies! in! the!UK,! although!a! single! centre! case! series!
suggested!similar!findings,!with!diverticular!disease!and!haemorrhoids!being!the!
most!common!diagnoses.11!
!
Although! diverticular! disease! is! the! most! common! cause! of! LGIB,! two!
longitudinal! studies! in! the! US! suggest! that! between! the! years! 2000! and! 2010!
overall!hospitalisations!due!to!diverticular!bleeding!decreased.51!52!In!contrast,!a!
multicentre!study!in!Spain!suggested!that!the!frequency!of!diverticular!bleeding!
increased!between!1996!and!2005.52!The!authors! from!the!US!based!study!did!
not! provide! a! hypothesis! for! this! reduction! in! incidence,52! although! they! did!
suggest! that! the! difference! in! findings! compared! to! the! Spanish! study!was! the!
use! of! different!methods! for! classifying! unspecified! cases! of! GIB.52! Lanas! et)al)
suggested!that!an!increase!in!diverticular!bleeding!may!be!due!to!the!increased!
use! of! anticoagulants,! antiplatelets! and! NSAIDs,! as! seen! in! an! ageing!
population.53!
!
Haemorrhoids! are! a! common! problem! globally,! with! reported! international!
frequencies!of!4.4O14.4%!of!the!adult!population.54!55!There!are!no!contemporary!
data!on!the!incidence!of!haemorrhoids!in!the!UK,!but!estimates!of!the!size!of!the!
problem! can! be! drawn! from! the! number! of! patients! undergoing! elective!
haemorrhoidal! surgery;! 23,000! in! England! in! 2004O2005.56! Haemorrhoids! are!
dilatations!of!the!vascular!cushions!that!surround!the!anus!and!most!commonly!
result! from! constipation.! In! the! US,! presentations! to! Emergency! Departments!
due!to!constipation!increased!by!46%!between!2006!and!2011.57!The!authors!of!
this! study! suggested! that! the! reasons! for! this! were! multifactorial,! related! to!

! 24!
health! service! utilisation! by! elderly! patients,! the! cost! of! over! the! counter!
laxatives!and!increasing!use!of!constipating!medications!such!as!opiates.57!
!
Longitudinal! studies! also! suggest! the! incidence! of! angiodysplasia,53! colonic!
polyps58! and! colorectal! cancer! is! increasing.59! This! trend! is! likely! due! to! the!
introduction!of!bowel!screening!and!adenoma!surveillance!programmes!leading!
to!increased!rates!of!diagnosis.60!Any!effect!on!polyp!and!cancer!related!LGIB!is!
unknown.!!
!
Determining!the!source!of!bleeding!can!be!difficult!and!20.8O50%5!12!patients!are!
discharged! without! a! diagnosis.! This! reduces! to! 9.2%! in! cohorts! where! all!
patients!receive!colonoscopy.8!Often!patients!are!discharged!with!a!diagnosis!of!
‘nonOspecific! gastrointestinal! haemorrhage’! or! ‘acute! haemorrhagic! anaemia’.12!
This! variability! in! the! coding! of! diagnoses! has! implications! for! the!
epidemiological!study!of!LGIB,!particularly!comparison!of!trends!over!time.!!
!
Outcomes)
!
In!comparison!to!UGIB,!LGIB!is!thought!to!have!a!more!benign!course.!Database!
studies!estimate!inOhospital!mortality!of!3.9O8.8%,2!12!but!most!deaths!are!due!to!
medical!morbidity,!such!as!sepsis!and!cardiac!events.5!11!13!Deaths!due!to!severe!
haemorrhage!occur!in!as!little!as!1%!cases.8!11!!
!
Single!centre!case!series!suggest!that!reObleeding!occurs!in!4.3O8.0%!cases!during!
admission,13!61!12.4%!at!3!months62!and!9%!at!one!year.9!The!highest!rates!of!reO
! 25!
bleeding! are! reported! in! patients! diagnosed! with! diverticular! bleeding! and!
angiodysplasia,!found!in!19.2%50!and!16.7%!patients!respectively.63!There!are!no!
large! multicentre! studies! detailing! the! frequency! of! reObleeding! in! the! UK,! or!
comparing!rates!of!reObleeding!across!a!standardised!population.!!
!
In!the!UK!there!no!contemporary!reports!of! the!average! length!of!hospital!stay!
for! patients! admitted! with! LGIB! and! there! are! widely! varying! reports! in! the!
literature!of!averages!between!3O10!days.12!64!Single!centre!retrospective!studies!
report!reOadmission!rates!of!4O7.5%.11!61!65!!
!
Risk)Assessment)
!
Unlike! UGIB,! there! are! no! widely! accepted! risk! assessment! tools! for! LGIB.! In!
UGIB! the! Rockall66! and! Blatchford67! scores! were! both! developed! in! UK!
populations,! and! have! been! extensively! validated! across! many! healthcare!
settings.!!Rockall!and!Blatchford!scores!are!used!to!predict!death,!reObleeding!or!
need!for!intervention.!There!have!been!attempts!to!do!this!in!LGIB!with!varying!
results.12! 68O70! One! database! study! of! 9,391! cases! of! LGIB! identified! that! age,!
intestinal! ischaemia,! coOmorbidity,! inpatient! bleeding,! coagulopathy,!
hypovolaemia,! RBC! transfusion! and! male! sex! were! predictive! of! inOhospital!
mortality.12! A! different! database! study! of! 4044! cases! agreed! that! age! and! coO
morbidity!were!predictive,!but!not!inpatient!bleeding,!transfusion!or!male!sex.70!!
!
The!usual!approach!of!modelling!risk!factors! is!hindered!by!the!paucity!of!data!
captured!about!LGIB.!There!are!several! reasons! for! this.!Research! into!GIB!has!

! 26!
typically! focussed!on!UGIB,! as! it! the!more! severe! type!of!GIB.6!To!develop!and!
validate! risk! assessment! tools! requires! at! least! two! sufficiently! large! and!
complete!sets!of!patient!data,!which!simply!do!not!exist!in!LGIB.!Database!studies!
often!use!hospital!codes!to! identify!patients,!but!as!described!previously,!many!
patients! are! discharged!with! a! nonOspecific! bleeding! or! anaemia! code.12! There!
are! often! geographical! differences! in! the! approach! to! hospital! coding,! for!
example! the! most! frequent! diagnosis! of! exclusion! in! the! US! is! diverticular!
bleeding,! whereas! in! Spain! it! is! anorectal! sources.52! This! means! that! risk!
profiling!based!on!data!from!coding!national!databases!may!not!be!applicable!to!
other! healthcare! settings! where! coding! is! applied! differently.! Additionally,!
treatment!strategies!may!differ!between!healthcare!settings,!which!may!reduce!
the!ability!of!a!risk!score!to!predict!need!for!intervention!in!other!geographical!
areas.! Critically,! a! prediction! tool! that! has! been! developed! in! an! American!
dataset!may! not! be! translatable! to! UK! practice,! where!management! strategies!
differ.!!
!
An!additional!limitation!is!the!focus!on!adverse!outcomes.!The!UGIB!risk!scores!
were! able! to! predict! adverse! outcomes! from! smaller! databases! as! these!
outcomes!are!more!common!in!UGIB!than!LGIB;!mortality!10%!versus!3.9%!and!
reObleeding! 13%! versus! 8%.12!13!33! To! adequately! power! a! statistical!model! to!
accurately! predict! these! outcomes! in! LGIB! would! require! a! larger! number! of!
cases.! The! Blatchford! score! uses! features! that! can! be! identified! at! initial!
assessment!to!predict!reObleeding,! including!features!of!hypovolaemic!shock.!In!
LGIB!these!features!are!much!less!common,!retrospective!studies!demonstrating!
a!frequency!of!shock!of!8%,11!13!making!this!approach!more!difficult.!

! 27!
!
The! lack! of! risk! scoring! has! important! implications! in! LGIB.! Other! than! using!
clinical! experience,! clinicians! have! no! standardised! approach! when! assessing!
LGIB!patients.!This!clinical!ambiguity!means!that!modifiable!risk!factors!may!not!
be!identified!and!in!a!climate!where!uncertainty!is! less!well!tolerated,!this!may!
lead! to! unnecessary! hospital! admissions.! This! has! financial,! social! and!
organisational!consequences.!!
!
Organisational)Requirements)and)Resource)Utilisation)
!
The! investigation! and! treatment! of! LGIB! may! involve! endoscopy,! radiology,!
interventional! radiology! and! surgery.! These! options! are! provided! by! different!
clinical!teams!and!departments!within!a!hospital!and!may!not!be!available!in!all!
hospitals.!!
!
The!2015!NCEPOD!report!into!GIB!found!that!only!55%!hospitals!could!provide!
24/7!onOsite!colonoscopy!and!70%!could!provide!24/7!access!to!interventional!
radiology.6!The!availability!of!endoscopists!who!are!able!to!provide!endoscopic!
haemostasis! in!the! lower!GI!tract! is!unknown.!Additionally,! the!NCEPOD!report!
did! not! collect! detail! on! how! hospitals! without! 24/7! access! to! these! services!
managed! their! patients.! In! response! to! findings! in! their! report,! the! NCEPOD!
made!several!organisational!recommendations.!!
• ‘Patients! with! any! acute! GI! bleed! should! only! be! admitted! to! hospitals!
with!24/7!access! to!onOsite!endoscopy,! interventional! radiology! (onOsite!

! 28!
or! covered! by! a! formal! network),! onOsite! GI! bleed! surgery! and! onOsite!
critical!care!and!anaesthesia.’6!
• ‘The!traditional!separation!of!care!for!UGIB!and!LGIB!in!hospitals!should!
stop.!All! acute!hospitals! should!have! a! lead! clinician!who! is! responsible!
for! local! integrated! care! pathways! for! both! UGIB! and! LGIB! and! their!
clinical! governance,! including! identifying! named! consultants,! ideally!
gastroenterologists,!who!would!be!responsible!for!the!emergency!and!onO
going!care!of!all!major!bleeds.’6!
!
Implementing!these!recommendations!would!require!significant!changes!to!the!
way! the!National!Health!Service! (NHS)! cares! for!GIB.!The!UK! is!unusual! in! the!
ownership!of!LGIB!patients!by!surgeons,!not!gastroenterologists.!Investing!in!the!
provision!of!comprehensive!endoscopy!and!interventional!radiology!would!have!
important! financial! consequences! and! other! than! sensible! expert! opinion,! this!
recommendation!has! little! evidence! supporting! it.! In! the!UK! it! is! currently! not!
known! how! many! LGIB! patients! require! endoscopy.! In! the! literature,! studies!
investigating!benefits!of!performing!all!colonoscopies!for!LGIB!on!an!urgent!basis!
have!had!conflicting!results.!One!cohort! study!demonstrated! increased!rates!of!
diagnosis!if!colonoscopy!was!performed!within!24!hours!of!admission,61!whereas!
a! randomised! controlled! trial! demonstrated! no! benefit.71! Evidence! supporting!
widespread!access!to!intervention!radiology!is!lacking,!but!reports!suggest!that!it!
is! only! used! in! a! minority! of! cases.5! 6! There! are! questions! on! the! use! and!
outcomes! of! both! endoscopy! and! interventional! radiology! that! should! be!
investigated!before!widespread!changes!to!hospital!services.!
!
! 29!
Health)Economics))
!
The!economic!burden!of!LGIB!in!the!UK!is!unknown.!In!the!US,!median!admission!
costs! are! estimated! at! $7,890.72! The! median! cost! of! an! UGIB! admission! is!
estimated!at!$9,548!in!the!US72!and!£2458!in!the!UK.73!A!retrospective!analysis!in!
the!US!found!that!40%!costs!related!to!GIB!were!incurred!following!discharge,74!
suggesting!significant!onOgoing!resource!utilisation!beyond!the!hospital!stay.! In!
the!current!climate!of!close!scrutiny!of!NHS!finances!and!a!drive!towards!proven!
efficiency! and! value! for!money,! any! new! strategy! in! the!management! of! LGIB!
requires! sound! economic! modelling! as! well! as! appraisal! of! its! safety! and!
effectiveness.!
!
Limitations)to)studying)LGIB)in)the)UK)
!
The! NHS! is! in! a! unique! position! where! hospitals! can! collaborate! on! research.!
Numerous! research! collaboratives! and! audit! programmes! have! enabled! the!
collection!data!on!clinical!across!many!different!NHS!Trusts,!providing!a!wealth!
of! observational! data! about! a! range! of! diseases.75! This! is! in! contrast! to!many!
other! countries!where!healthcare! is! fragmented,!hospitals! compete! for! funding!
and!consumers,!which!is!likely!to!limit!coOoperation!between!hospitals.!!
!
Studying!LGIB!does!have!limitations.!Previous!multicentre!studies!of!LGIB!from!
Europe! and! the! US2! 12! rely! on! hospital! codes! to! identify! patients.! The! same!
clinical!codes!are!used!in!the!Hospital!Episode!Statistics!(HES)!data!collected!by!
hospitals!in!the!UK,!but!their!use!has!many!drawbacks.!As!described!previously,!
! 30!
many!codes!are!nonOspecific,!allowing!a!patient!to!be!discharged!with!codes!such!
as!‘nonOspecific!gastrointestinal!haemorrhage.’!This!problem!is!more!of!a!burden!
for! LGIB! than!UGIB.! For! example,! in! the! International! Classification! of! Disease!
(ICD,! version! 10)! there! are!multiple! codes! that! can! be! used! for! UGIB,! such! as!
‘haematemesis’!and!‘melaena’.76!The!sole!equivalent!for!LGIB!is!‘haemorrhage!of!
the! anus! or! rectum’,! which! by! definition! excludes! diverticular! disease,! which!
studies! have! suggested! is! the! most! common! cause! of! LGIB.12! 50! Diverticular!
disease! is! included! in! several! ICD! codes,! but! is! limited! to! perforation! or!
abscess;76!there!is!no!code!for!diverticular!bleeding!per!se.!Similarly!there!is!no!
code!for!haemorrhoidal!bleeding.!!
)The!lack!of!investigation!or!inconclusive!investigations!as!often!found!in!LGIB,5!12!
also! causes! problems! when! attempts! at! validating! hospital! codes! are! made.!
Researchers!have!attempted!to!improve!the!identification!of!LGIB!patients!from!
coded!databases!by!using!classification!trees!and!machine!learning!algorithms,77!
but!these!are!cumbersome!and!have!limited!applicability!in!clinical!research.!To!
start!addressing!the!many!questions!relating!to!LGIB,!a!different!approach!will!be!
required!to!provide!the!level!of!detail!required!to!provide!meaningful!answers.!
!
Discussion:)outstanding)questions)in)LGIB)
!
There!are!several!key!areas!in!LGIB!that!require!research.!There!are!a!global!lack!
of! high! quality! epidemiological! data! that! can! be! used! to! track! trends! in!
diagnoses,! management! and! outcomes.! This! has! implications! for! the! critical!
! 31!
appraisal! of! new! interventions,! as! there! are! limited! baseline! data! to! use! for!
comparison.!
!
Outcomes! of! patients! admitted! to! NHS! hospitals! with! LGIB! are! currently!
unknown.!Without! these! data,! we! are! unable! to! determine! factors! influencing!
outcome,!and!how!risk!factors!for!adverse!outcome!could!be!modified.!The!use!of!
diagnostic! and! therapeutic! intervention! is! likely! to! be! influenced! by! its!
availability!as!opposed!to!clinical!evidence!for!efficacy.!
!
Resource!utilisation!remains!unquantified!in!the!UK!and!estimates!from!around!
the!world!often! include!UGIB,!which!has!a!different! clinical! course.!The! lack!of!
epidemiological!and!resource!data!means!that!appraisal!of!current!management!
strategies!often!relies!on!expert!opinion,!not!rigorous!scientific!study.!The!close!
scrutiny!of!healthcare!delivery!by!consumers!and!providers!means!that!this!is!no!
longer!accepted!as!adequate.!!
!
!
!
!
!
!
!!!!!!!
! 32!
1.2!Aims!of!the!thesis!!
In!the!UK!there!are!no!national!guidelines!on!optimal!standards!of!care!for!LGIB,!
no! large!epidemiological!studies!and! limited!reports!on!patient!outcomes.6!The!
work! in! this! thesis! aims! to! critically! appraise! the! literature! on! optimal!
investigation!and!treatment,!and!provide!unprecedented!national!data!on!acute!
LGIB!in!the!UK.!These!observational!data!will!be!used!to!identify!organisational!
and! patientOrelated! factors! that! influence! patient! outcome! and! to! design! a!
strategy!to!modify!them.!Presenting!features!will!be!used!to!develop!a!model!to!
identify! features! that! predict! adverse! outcomes! that! can! be! used! to! triage!
patients!on!initial!clinical!assessment.!
!
!
1.3!Outline!of!the!thesis!!
Chapter! 2! is! a! systematic! review! of! diagnostic! and! therapeutic! treatment!
modalities!for!acute!LGIB,!aiming!to!identify!the!best!diagnostic! intervention!to!
identify! the! source!of! bleeding,! and! the!optimum! treatment! to! arrest! bleeding.!
Interventions! are! appraised! using! diagnostic! yield,! rates! of! reObleeding,! RBC!
transfusion!and!complications.!Chapters!3,!4!and!5!detail! the!methodology!and!
results!of!the!first!national!observational!study!of!patients!presenting!with!acute!
LGIB.! Chapter! 6! describes! a! risk! score! to! aid! the! triage! of! LGIB! at! initial!
assessment,!and!Chapter!7!described!an!analysis!of!patients!who!develop!LGIB!
whilst!receiving!antiplatelet!and!anticoagulant!medications.!
!
!

! 33!
CHAPTER!2!
!
SYSTEMATIC! REVIEW:! DIAGNOSTIC! AND! THERAPEUTIC! TREATMENT!
MODALITIES!FOR!ACUTE!LOWER!GASTROINTESTINAL!BLEEDING!
!
2.1!Introduction!
The!treatment!of!LGIB!involves!determining!the!site!and!source!of!bleeding,!and!
choosing!the!most!appropriate! interventions!to!achieve!haemostasis.!There!are!
several!possible!interventions!including!colonoscopy,!computerised!tomographic!
angiography!(CTA),!mesenteric!angiography!(MA)!and!nuclear!scintigraphy.!The!
diagnostic! and! subsequent! therapeutic! yields!of! each!modality! are!unclear! and!
are!likely!to!be!influenced!by!timing,78!pathology,79!haemodynamic!status80!and!
patient!related!factors.37!There!is!little!evidence!in!the!literature!informing!their!
optimal! use,! hence! the! development! of! recommendations! in! guidelines! is!
limited.47!!
!
As! well! as! diagnosis,! endoscopy! offers! endotherapy,! including! adrenaline!
injection,!thermocoagulation!or!clipping.!Extravasation!of!contrast!on!CTA!or!MA!
may! identify! bleeding! that! is! amenable! to! embolisation.! In! comparison! to!
colonoscopy,!CTA!is!better!tolerated!by!patients!but!may!only! identify!a!source!
where!there!is!active!bleeding.81!Delays!between!CTA!and!angiography!may!lead!
to! a! blush! on! CTA! becoming! nonOapparent! on! a! subsequent! mesenteric!
angiogram.82!!
!

! 34!
Given! uncertainties! around! the! optimum! approach! to! investigation! and!
management! of! LGIB,!we! conducted! a! systematic! review! of! the! diagnostic! and!
therapeutic! yields! of! colonoscopy,! CTA! and!MA.!This! takes! the! form!of! several!
direct!head!to!head!comparisons!between!modalities,!each!of!which!is!reported!
separately,! aiming! to! mirror! the! clinical! questions! encountered! by! clinicians!
involved!in!the!acute!management!of!LGIB.!!
!
2.2!Methods!
This! review! was! registered! on! the! PROSPERO! register! of! systematic! reviews!
(CRD42016025100)!and!conducted!in!accordance!with!the!Preferred!Reporting!
Items! for! Systematic! Reviews! and! MetaOAnalyses! (PRISMA)! statement83! and!
MetaOAnalysis!of!Observational!Studies!in!Epidemiology!(MOOSE)!group.84!
)
Search)strategy)
MEDLINE,! PubMed,! EMBASE,! CDSR,! CENTRAL,! DARE,! HTA! &! NHSEED,! the!
Transfusion! Evidence! Library,! ClinicalTrials.gov! and! the! WHO! International!
Clinical! Trials! Registry! Platform!were! searched! for! articles! published! between!
2000!and!12th!November!2015!without!language!restrictions!(Appendix!2).!The!
search!was!limited!to!publications!since!2000!due!to!the!more!recent!adoption!of!
CTA! and! therapeutic! endoscopy,! reflective! of! modern! day! practice.! Any! nonO
English! language! articles! were! translated.! References! that! were! likely! to! be!
related! to! UGIB! were! also! identified! and! preOscreened! by! one! reviewer! (KO).!!
Any!potentially!relevant!references!were!added!to!the!results!and!underwent!full!
screening!with!the!other!identified!studies.!I!also!hand!searched!reference!lists!of!
relevant!narrative!and!systematic!reviews.!

! 35!
)
Study)eligibility)
As!recent!guidelines!on!this!topic!have!demonstrated!a!lack!of!randomised!data!
in!this!area,6!47!cohort!studies!(nonOrandomised!studies!of!intervention,!NRSI)!as!
well!as!randomised!controlled!trials!(RCTs)!were!included.!Studies!were!eligible!
if! they!included!at! least!two!different! interventions!for!LGIB.!Those!reported!in!
conference! proceedings! were! also! included.! Case! reports! and! series! were! not!
eligible.!!
!
Screening!criteria!were!as!follows:!
• Participants! had! a! diagnosis! of! acute! LGIB! that! required! hospital!
admission,!(including!exclusive!subgroups!such!as!diverticular!bleeds)!
• Participants!aged!≥!16!years!
• One!group! in! the! study! received! colonoscopy,!CTA,!MA,! embolisation!or!
endoscopy!therapy!(surrogate!terms!such!as!haemorrhoid!banding!were!
also!eligible)!!
• Published!in!year!2000!or!later!
• Study! compared! two! interventions,! timing! of! intervention! or! shocked!
status!of!the!patient!
• Study! reported! at! least! one! of! diagnostic! yield,! therapeutic! yield,! RBC!
transfusion,! length!of! stay! (LOS),!mortality,! complications! related! to! the!
intervention,!need!for!further!procedure!
!
Pairs! of! authors! screened! all! search! results.! Where! a! decision! regarding!
eligibility! could!not!be!made!on! title! and!abstract! screen!alone,! full! texts!were!

! 36!
retrieved.! As! there! is! considerable! variation! in! the! reporting! quality! of! nonO
randomised! studies,! those! that! contained! two! comparator! groups! but! lacked!
transparently! reported!methodology! or! that! reported! a! cohort! design!without!
methodological! concordance! were! screened! to! determine! whether! they! met!
criteria!to!truly!be!categorised!as!a!cohort!study!as!described!by!Dekkers!et)al.85!
!
Participants))Adult! patients! (≥16! years)! hospitalized! with! acute! LGIB! of! any! cause! were!
eligible.! Studies! of! obscureOovert! GI! bleeding! (defined! as! clinical! evidence! of!
bleeding! without! an! obvious! aetiology! after! endoscopic! and! radiologic!
evaluation)7!were! only! eligible! if! participants!were! hospitalised!with! bleeding.!
Patients!with!obscureOoccult!GI!bleeding! (defined!as!bleeding! from!the!GI! tract!
without!an!obvious!aetiology!in!the!absence!of!clinically!evident!bleeding7)!
or!UGIB!were!excluded.!!
!
Interventions)and)comparisons)
Interventions! included! flexible! sigmoidoscopy,! colonoscopy,! CTA,! MA,!
therapeutic!endoscopy!and!mesenteric!embolisation.!Comparisons!comprised!of:!
colonoscopy/sigmoidoscopy! versus! CTA;! colonoscopy/sigmoidoscopy! versus!
other! (e.g.! standard! care);! CTA! versus! other;! timing! of!
colonoscopy/sigmoidoscopy,! CTA! and! MA! in! relation! to! presentation! with!
bleeding.! Modes! of! haemostasis! were! also! compared:! endoscopic! haemostasis!
versus! embolisation;! endoscopic! haemostasis! versus! other! and! embolisation!
versus! other.! Specific! types! of! endoscopic! therapy! (including! adrenaline!
! 37!
injection,! banding,! haemoclipping,! thermocoagulation! and! snare! polypectomy)!
were!also!compared.!!
!
)
Outcomes)
Primary! outcomes! were! diagnostic! or! therapeutic! yield.! Diagnostic! yield! was!
defined!as!identification!of!the!source!of!bleeding.!Therapeutic!yield!was!defined!
as! the! proportion! of! participants! that! received! haemostatic! therapy,! either!
during! or! after! the! intervention.! Secondary! outcomes! were! reObleeding,! red!
blood! cell! (RBC)! transfusion,! length! of! hospital! stay! (LOS),! mortality! and!
complications! related! to! the! intervention! (perforation! at! lower! GI! endoscopy,!
complications!of!sedation,!contrast!reactions,!vascular!entry!site!complications,!
nonOtarget!embolisation,!mesenteric!ischaemia).!!
!
Data)extraction)
Two!independent!review!authors!extracted!the!following!data!from!each!study:!
1. General! study! information:! study! ID,! publication! type,! publication! date,!
funding!source,!conflict!of!interest!statement!
2. Study!methods:!country,!setting,!recruitment!dates,!recruitment!or!cohort!
allocation! method,! randomisation,! blinding,! methods! of! matching! or!
adjusting!for!confounders,!specified!primary!outcome!
3. Intervention:! number! of! treatment! arms! or! cohorts,! description! of!
intervention,! any! coOinterventions! (such! as! method! of! bowel!
preparation),! timing! of! intervention,! person! performing! or! interpreting!
intervention,!criteria!to!treat!bleeding!

! 38!
4. Participants:! age! gender,! baseline! haemodynamic! status,! baseline!
antiplatelet,!anticoagulant!and!NSAID!use!
5. Outcomes:! diagnostic! yield! and! study! specific! definition! of! diagnostic!
yield,! therapeutic! yield! and! treatment!methods! available! for! use! in! the!
study,! reObleeding! and! definition! of! reObleeding,! participants! requiring!
RBC! transfusion,! volume!of! red! cell! transfusion,! length!of! intensive! care!
(ICU)! stay,!LOS,!mortality! (inpatient! and!up! to!30!days),! cause!of!death,!
number!of! participants! requiring! a! further!procedure! and! rationale! and!
number!of!participants!with!a!complication!related!to!the!intervention.!
!
If!studies!included!upper!and!lower!GIB!extraction!was!limited!to!data!pertaining!
only! to! LGIB.! Study! screening! and! data! extraction! was! performed! using!
Covidence!Systematic!Review!Software!(Veritas!Heath!Innovation!Ltd,!Australia).!!
)
Quality)of)evidence)
Risk!of!bias!in!RCTs!was!assessed!using!the!Cochrane!risk!of!bias!tool,86!using!the!
following!seven!domains:!
• Sequence!generation!(selection!bias)!
• Allocation!concealment!(selection!bias)!
• Blinding!of!participants!and!personnel!(performance!bias)!
• Blinding!of!outcome!assessors!(detection!bias)!
• Incomplete!outcome!data!(attrition!bias)!
• Selective!outcome!reporting!(reporting!bias)!
• Other!sources!of!bias!
!
! 39!
NRSI!were!assessed!using!the!NewcastleOOttawa!Scale87!using!the!following!eight!
domains:!
• Representativeness!of!exposed!cohort!
• Selection!of!nonOexposed!cohort!
• Ascertainment!of!exposure!
• Demonstration!that!outcome!of!interest!was!not!present!at!the!start!of!the!
study!
• Comparability:! study! controls! for! haemodynamic! status,! study! controls!
for!any!additional!factor!
• Ascertainment!of!outcome!
• Was!follow!up!long!enough!for!outcomes!to!occur?!
• Adequacy!of!follow!up!
!
Statistical)analysis)
Continuous! outcomes! were! recorded! as! mean,! standard! deviation! (SD)! and!
number!of!participants!and!compared!using!mean!difference!(MD)!and!95%!CI.!
Dichotomous!outcomes!were!recorded!as! the!number!of!events!and!number!of!
participants!and!analysing!using!RR!and!95%!CI! for!RCTs!and!odds!ratios!(OR)!
and!95%!CI!for!NRSI.!Where!the!number!of!observed!events!was!small!(less!than!
5%!of!the!sample)!Peto!ORs!and!95%!CI!were!used.!!
!
RCTs! and! NRSI! were! analysed! seperately88.! Statistical! heterogeneity! was!
analysed! using! I2! statistics! and! values! >50%! were! considered! significantly!
heterogeneous.89! If! heterogeneity! between! RCTs! was! not! significant,! metaO
analysis! was! undertaken! using! fixedOeffect! metaOanalysis,! otherwise! randomO

! 40!
effects! metaOanalysis! was! undertaken.90! To! aid! clinical! interpretation,! effect!
estimates!from!RCTs!were!reported!as!RRs.88!!
!
Due!to!the!nonOrandomised!nature!of!NRSI,!these!studies!are!likely!to!be!at!risk!
of!bias,!particularly!selection!and!reporting!bias.86!For!this!reason,!metaOanalysis!
of!NRSI!was!restricted! to! randomOeffects!metaOanalysis!and!estimates! reported!
as!OR,!regardless!of!heterogeneity.!NRSIs!were!deemed!comparable!if!they!had!a!
NewcastleOOttawa! score! ≥891.! No! tests! for! funnel! plot! asymmetry! were!
undertaken!as! the!number!of! studies! in!each!comparison!was! fewer! than!1088.!
MetaOanalysis! was! undertaken! using! Review! Manager! 5.3! (Cochrane!
Collaboration,!Denmark).!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!

! 41!
2.3!Characteristics!of!reviewed!studies!
Searches! identified! 5839! records! potentially! eligible! references! and! 40! from!
2410!preOscreened!records.!The!flowchart!of!the!search!is!shown!in!Figure!1.!On!
review! of! full! texts,! 507! studies!were! excluded,! including! 193!with! the!wrong!
design,! 47! without! the! interventions! of! interest! and! 165! with! the! wrong!
comparison.!41!studies!did!not!differentiate!lower!from!UGIB.!!
Figure!1:!PRISMA!flowOchart!of!eligible!studies!
!
Records(iden+fied(through(other(sources((n=2)(
Records(excluded,(did(not(meet(eligibility(criteria(
(n=5353)(
Studies(assessed(for(full@text(eligibility((n=528)(
Full@text(studies(excluded((n=507)(
Wrong(study(design((n=193)(Wrong(comparator(or(no(comparator((n=165)(
Wrong(interven+on((n=47)(Pa+ents(not(hospitalised(
(n=37)(UGIB(or(unable(to(classify(
(n=41)(Includes(paediatric(popula+on((n=19)(
Wrong(outcomes((n=5)((
Records(iden+fied(in(databases(search((n=5879)(
Eligible'studies'(n=21)'
Mul+ple(reports(of(same(study(excluded(
(n=5)(
Non4randomised'studies'(cohort'studies)'
(n=13)'
Randomised'controlled'trials'(n=3)'(

! 42!
There!was!a!paucity!of!data!across!all!interventions!and!comparators;!3!RCT,!13!
NRSI! and! 3! onOgoing! studies! met! the! criteria! for! inclusion,! including! six!
conference!abstracts92O97.!Eleven!studies!compared!at! least!two!different!modes!
of! investigation! or! treatment! and! five! examined! different! timings! of! the! same!
intervention!(Table!1).!!No!studies!reported!subgroups!based!on!haemodynamic!
status!of!the!participant.!We!found!no!studies!of!flexible!sigmoidoscopy.!

! 43!
Table!1:!Summary!of!evidence!by!comparison!investigated!and!study!methodology!
!
Comparator! RCTs! NRSIs! OnUgoing!trials!Colonoscopy!vs!CTA!!
! Nagata!2015!Yabutani!2014!
!
Colonoscopy!vs!other!(eg!standard!care)!!
Green!2005!! Yamaguchi!2006!!!
!
CTA!vs!other!(inc!standard!care)!
! Ketwaroo!2012!!Sun!2011!!Jacovides!2015!!
!
Diagnostic!MA!vs!other! Leung!2012!! ! Chen!NCT02069262!
Timing!of!colonoscopy!A) Early!(<24!hours)!
vs!late!(>24!hours)!
!Laine!2010!!
!Abeldawi!2014!Nagata!2016!Strate!2003!RodriguezOMoranta!2007!
!!
Timing!of!radiology!A)!Urgent!CTA!vs!nonOurgent!B)!Urgent!MA!vs!nonOurgent!
!!!!
!!!
!
Therapeutic!endoscopy!vs!mesenteric!embolisation!
! ! !
Therapeutic!endoscopy!vs!other!
! Jensen!2000!! Matsuhashi!!JPRNOUMIN000008287!
Embolisation!vs!other! ! ! !Endoscopic!agent!A!vs!B! ! Nakano!2015!!
Ishii!2011!!Barkun!NCT02135627!
!!!The!characteristics!of!each!study!are!included!in!Table!2.!Although!eligibility!was!
restricted!to!publication!since!2000,!several!studies!were!conducted!years!before!
publication.!Jensen!et)al)included!a!historical!control!that!was!captured!between!
1986! and! 199298! and! Green! et) al) published! their! results! 10! years! after!
recruitment!had!finished78.!The!case!definitions!of!LGIB!are!included!in!Table!2.!
Eleven!studies!included!patients!with!LGIB!of!any!cause45!61!64!71!78!93O95!99O101,!four!
were!limited!to!patients!with!diverticular!bleeding92!96O98!and!one!was!limited!to!

! 44!
obscureOovert! bleeding102.! The! number! of! participants! enrolled! in! each! study!
was!small,!ranging!from!60O100!in!the!RCTs!and!27O326!in!the!NRSI.!!
!
Most!trials!were!conducted!in!older!patients!and!where!reported,!anticoagulant,!
NSAID! and! particularly! antiplatelet! use! was! common.! Five! studies! reported!
baseline! haemodynamic! status64! 71! 78! 101! 102.! The! RCTs! included! a! higher!
proportion!of!shocked!patients!than!the!NRSIs.!!
!
!
!
!
!
!
!
!
!
!
!

! 45!
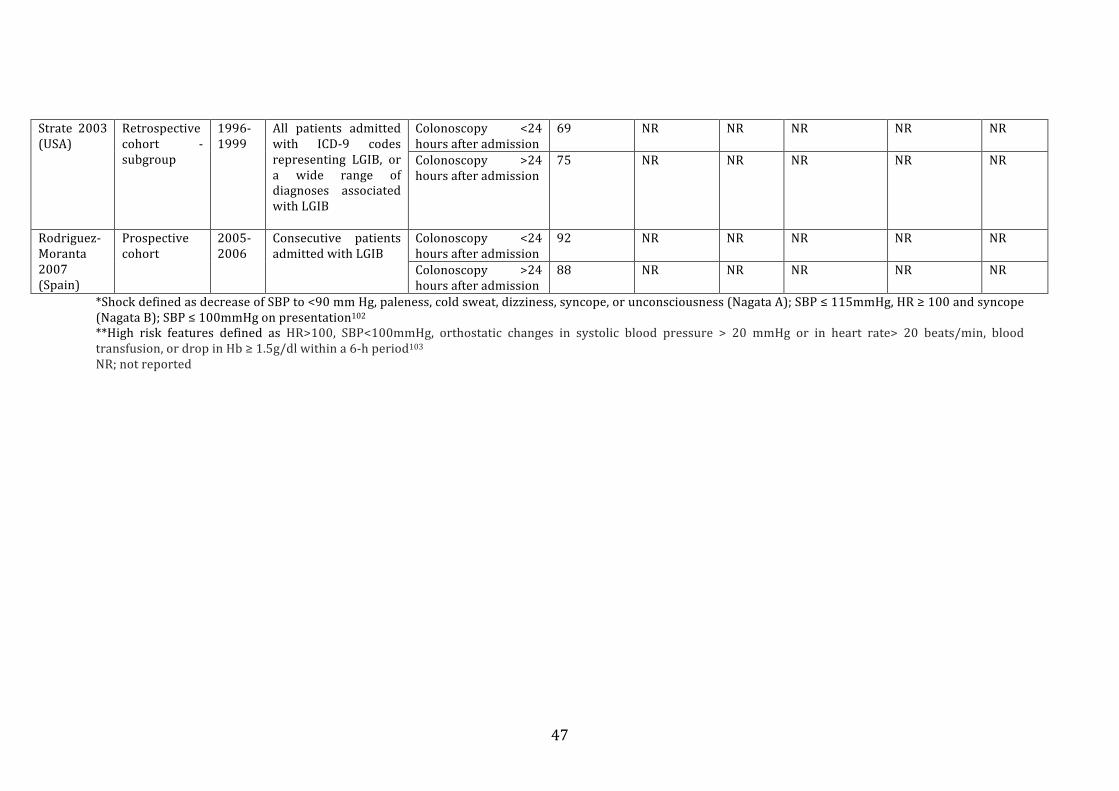
Table!2:!Study!characteristics!!
Study! Design!! Study!years!
Study!population! Interventions! Total!Participants!(N)!
Age! (mean!±SD)!
Shock*!N!(%)!
Medications!on!admission,!N!(%)!Anticoagulants! Antiplatelets! NSAIDs!
Green! 2005!(USA)!
RCT! 1993P1995!
Patients! admitted!with! haematochezia!with! clinical! or!laboratory!evidence!of!significant!blood!loss!
Colonoscopy!<8!hours!after!admission!
50! 68±3! 30!(60.0)!
NR! NR! 29!(60.0)!
Standard! care:! red!cell! scan! if! ongoing!bleeding,!colonoscopy!
50! 71±4! 34!(68.0)!
NR! NR! 26!(52.0)!
Laine! 2010!(USA)!
RCT! 2002P2008!
Patients! admitted!with! haematochezia!with! a! high! risk!feature**!
Colonoscopy! <12!hours!after!admission!
36! 52±3! 27!(75.0)!
NR! NR! NR!
Colonoscopy! 36P60h!hours!after!admission!
36! 52±2! 31!(86.1)!
NR! NR! NR!
Leung! 2012!(USA)!
RCT! 2005P2009!
Patients! admitted!with! melena! or!hematochezia! with!nonPdiagnostic! upper!GI! endoscopy! and!colonoscopy!
Capsule!endoscopy! 30! 58.6±19.9! 10!(33.3)!
1!(3.3)! 6!(20.0)! 6!(20.0)!
Angiography! 30! 53.3±20.9! 9!(30.0)! 0! 8!(26.7)! 3!(10.0)!
Albeldawi!2014!(USA)!
Retrospective!cohort!
2011P2012!
All!acute!LGIB!! Colonoscopy! <24!hours!after!admission!!
24! 66.8±!13.8! NR! 2!(8.3)! 13!(54.2)! 2!(8.3)!
Colonoscopy! >24!hours!after!admission!!
33! 69.3±11.1! NR! 7!(21.2)! 19!(57.6)! 3!(9.1)!
Ishii! 2011!(Japan)!
Retrospective!cohort!
2004P2010!and!2009P2010!
Patients! with! colonic!diverticular!haemorrhage!!
EBL! 16! NR! NR! NR! NR! NR!EC! 48! NR! NR! NR! NR! NR!
Jacovides!2015!(USA)!
Historical!control!
2005P2012!
All! patients!hospitalised! with!LGIB!!
Historical! protocol:!red! cell! scan,! CTA! or!colonoscopy!
78! 68±15!!
NR! NR! NR! NR!
New! protocol:! CTA,!colonoscopy!
83! 70±15! NR! NR! NR! NR!

! 46!
Jensen!2000!(USA)!
Historical!control!!
1986P1992!and!1994P1998!
Patients! with!haematochezia! and!diverticulosis!
Medical! and! surgical!intervention!
17! 66±3!!
NR! NR! NR! 3!
Medical! and!endoscopic!therapy!
10! 67±4! NR! NR! NR! 3!
Nagata!2016!(Japan)!
Retrospective!cohort!
2009P2014!
All! patients! admitted!with!acute!overt!LGIB!
Colonoscopy! <24!hours!after!admission!
163! 67.9±17.4!!
17!(10.4)!
9!(5.5)! 63!(38.7)! 23!(14.1)!
Colonoscopy! >24!hours!after!admission!!
163! 66.4±16.9!!
19!(11.7)!
6!(11.7)! 54!(33.1)! 20!(12.3)!
Nagata!2015!(Japan)!
Retrospective!Cohort!
2008P2013!
Patients! admitted!with! LGIB! who!underwent!colonoscopy!!
Urgent! CTA! then!colonoscopy!
126! 68.3±16.5!!
5!(4.0)! 7!(5.6)! 55!(43.7)! 33!
Colonoscopy! <24!hours!after!admission!
97! 67.7±16.5!!
1!(1.0)! 4!(4.1)! 36!(37.1)! 13!(13.4)!
Nakano!2015!(Japan)!
Retrospective!cohort!
2004P2014!
Patients! undergoing!endoscopic! therapy!for! colonic!diverticular!haemorrhage!!
EBL! 50! 67±13!!
NR! NR! 15! 4!
EC! 39! 64±13! NR! NR! 13! 3!
Sun! 2011!(USA)!
Retrospective!cohort!
2007P2008!and!2008P2010!
All! patients!hospitalised! with!acute!GIB!!
CTA! 53! NR! NR! NR! NR! NR!Red!cell!scan! 46! NR! NR! NR! NR! NR!
Yabutani!2006!(Japan)!
Single!retrospective!cohort!
2010P2012!
Patients! diagnosed!with! diverticular!bleeding!!
CTA!and!colonoscopy! 57! NR! NR! NR! NR! NR!
Yamaguchi!2006!(Japan)!
Single!retrospective!cohort!
1999P2004!
Consecutive! patients!with!haematochezia!!
Ultrasound! and!colonoscopy!
111! 58! (range!18P96)!
NR! NR! NR! NR!
Ketwaroo!2012!(USA)!
Retrospective!cohort!!!!
2010P2011!
Suspected!acute!LGIB!! CTA! 46! 68.2±17! NR! NR! NR! NR!Red!cell!scan! 46! 70±15!
!NR! NR! NR! NR!
! 47!
Strate! 2003!(USA)!!!!!!
Retrospective!cohort! P!subgroup!
1996P1999!
All! patients! admitted!with! ICDP9! codes!representing! LGIB,! or!a! wide! range! of!diagnoses! associated!with!LGIB!
Colonoscopy! <24!hours!after!admission!
69! NR! NR! NR! NR! NR!
Colonoscopy! >24!hours!after!admission!
75! NR! NR! NR! NR! NR!
RodriguezP!Moranta!2007!(Spain)!
Prospective!cohort!
2005P2006!
Consecutive! patients!admitted!with!LGIB!
Colonoscopy! <24!hours!after!admission!
92! NR! NR! NR! NR! NR!
Colonoscopy! >24!hours!after!admission!
88! NR! NR! NR! NR! NR!
*Shock!defined!as!decrease!of!SBP!to!<90!mm!Hg,!paleness,!cold!sweat,!dizziness,!syncope,!or!unconsciousness!(Nagata!A);!SBP!≤!115mmHg,!HR!≥!100!and!syncope!(Nagata!B);!SBP!≤!100mmHg!on!presentation102!**High! risk! features! defined! as! HR>100,! SBP<100mmHg,! orthostatic! changes! in! systolic! blood! pressure! >! 20! mmHg! or! in! heart! rate>! 20! beats/min,! blood!transfusion,!or!drop!in!Hb!≥!1.5g/dl!within!a!6Ph!period103!!!!!NR;!not!reported
! 48!
2.5$Choice$of$investigation$of$acute$lower$gastrointestinal$bleeding$
Colonoscopy)versus)CTA))
No! RCTs! compared! colonoscopy! with! CTA.! The! two! eligible! NRSIs! were!
retrospective,! one! comparing! early! colonoscopy! and! CTA! (within! 24! hours! of!
admission)! with! early! colonoscopy! alone! in! 223! participants64,! and! one!
comparing!early!colonoscopy!with!CTA!(timings!not!defined)!in!a!single!cohort!of!
114!patients!with!diverticular!bleeding!that!had!both!tests92.!!
!
The!was!no!difference!in!the!diagnostic!yield!of!CTA!combined!with!colonoscopy!
versus!colonoscopy!alone!(OR!1.31,!95%!CI!0.26!to!6.63)!although!the!diagnosis!
of!lesions!with!active!bleeding,!adherent!clot!or!visible!vessels!was!higher!in!the!
CTA! group! (OR! 2.14,! 95%! CI! 1.16! to! 3.95,! 223! participants).! Patients! in! this!
group! subsequently! received! more! endoscopic! haemostasis! (OR! 3.47,! 95%! CI!
1.74!to!6.91),!but!there!was!no!difference!in!terms!of!rePbleeding!(OR!1.08,!95%!
CI!0.51!to!2.28)!or!participants!receiving!RBC!transfusion!(OR!1.71,!95%!CI!0.86!
to! 3.39).! Mortality,! LOS! and! complications! were! not! reported.! The! study! by!
Yabutani! et) al! described! only! diagnostic! yield,! demonstrating! no! difference!
between!CTA!and!colonoscopy!(OR!1.36,!95%CI!0.63!to!2.95,!114!participants).!!
$
Colonoscopy)versus)other))
We!identified!one!RCT78!that)randomised!100!patients!to!colonoscopy!within!8!
hours!or!standard!care!(red!cell!scanning,!angiography!or!elective!colonoscopy).!
The!diagnostic!yield!was!higher!in!the!group!randomised!to!urgent!colonoscopy!
(RR!1.91,!95%!CI!1.03!to!3.53),!but!there!was!no!difference!in!therapeutic!yield!
(endoscopic!haemostasis!or!vasopressin!infusion,!RR!1.7!95%!CI!0.87!to!3.34)!or!

! 49!
rePbleeding!(RR!0.73,!95%!CI!0.37!to!1.44),!although!volume!of!RBC!transfusion!
was!smaller!in!the!colonoscopy!group!(mean!difference!P0.8!units,!95%!CI!P0.62!
to!P0.98).!We!identified!one!NRSI;99!a!study!of!111!participants!who!underwent!
ultrasound! followed! by! colonoscopy.! The! diagnostic! yield! of! colonoscopy! was!
superior!to!that!of!ultrasound!(OR!3.78!95%!CI!2.07!to!6.91).!
!
CTA)versus)other)
No!RCTs!were!identified.!The!three!eligible!NRSIs!all!compared!CTA!with!nuclear!
scintigraphy;!two!retrospective!cohort!studies!of!92P99!participants94!95!and!one!
before! and! after! study! of! a! protocol! that! prioritised! CTA! over! nuclear!
scintigraphy!in!161!participants45.!CTA!demonstrated!a!higher!diagnostic!yield!in!
the!study!by!Ketwaroo!et)al)but!there!was!no!difference!in!the!study!by!Sun!et)al)
(OR!4.03,!95%!CI!1.67!to!9.72,!92!participants!and!OR!0.49!95%!CI!0.20!to!1.21,!
99!participants,!respectively).!Neither!study!reported!therapeutic!yield!for!both!
study!arms!or!any!of!the!secondary!outcomes.!The!protocol!study!by!Jacovides!et)
al)demonstrated!no!difference!in!diagnostic!yield!(OR!0.85!95%!CI!0.33!to!2.19),!
therapeutic!yield!(defined!as!embolisation!during!first!MA,!OR!1.10,!95%!CI!0.55!
to!2.20)!or!LOS!(MD!3!days,!95%!CI!P16.58!to!22.58).!
$
Diagnostic)MA)versus)other))
We! identified! one! RCT! comparing!MA! to! capsule! endoscopy,102! and! no! NRSIs.!
The!study!by!Leung!et)al)was!conducted!in!patients!with!obscurePovert!bleeding!
(defined! as! those! presenting! with! melaena! or! haematochezia! with! a! nonP
diagnostic!upper!GI!endoscopy!and!colonoscopy)!randomising!60!participants!to!
MA! or! capsule! endoscopy.! Initially! capsule! endoscopy! was! superior! to! MA! in!

! 50!
terms!of!diagnostic!yield!(RR!2.67,!95%!CI!1.21!to!5.88),!however!in!the!capsule!
endoscopy! arm! 4! patients! had! active! bleeds! from! the! small! bowel,! which! if!
regarded!as!negative!findings,!rendered!the!diagnostic!yield!nonPsignificant!(RR!
2.00,! 95%! CI! 0.86! to! 4.63).! Therapy! was! limited! to! surgery! (there! was! no!
angiographic! intervention)! and! there! was! no! significant! difference! between!
patients! that! received! MA! versus! those! that! received! capsule! endoscopy! (RR!
0.67,! 95%! CI! 0.12! to! 3.71).! ! There! was! also! no! difference! in! the! risk! of! reP
bleeding!(RR!0.50!95%!CI!0.19!to!1.29),!transfusion!(RR!1.0,!95%!CI!0.22!to!4.56)!
or! death! (RR! 1.0,! 95%! CI! 0.28! to! 3.63)! in! the!MA! group! compared! to! capsule!
endoscopy.!!!
!
We!found!one!onPgoing!trial,!again!in!overtPobscure!GIB,!randomising!patients!to!
receive!MA!or!MA!in!combination!with!laparoscopy!(Chen!et)al,!NCT02069262).!!
!
! 51!
2.5$Timing$of$first$line$investigation$
Colonoscopy)
One!RCT,71!one!prospective93!and! three!retrospective!NRSI61!93!100!101! compared!
early! and! late! colonoscopy.! Laine! et) al) randomised! 72! patients! and! the! NRSI!
ranged! from! 57P326! participants.! One! study! defined! early! colonoscopy! to! be!
within! 12! hours,71! three! studies! defined! early! colonoscopy! to! be! within! 24!
hours93! 100! 101! and! one! subdivided! their! cohort! into! consecutive! 12! hours!
groups61.! For! the! purpose! of! this! comparison! early! colonoscopy! is! defined! as!
within!24!hours!of!admission.!!
$
For! diagnostic! yield,! three! studies! categorised! diverticula61! 71! 101! or!
haemorrhoids! 61! 71! as! definite! (based! on! the! presence! of! active! bleeding! or!
stigmata! of! recent! haemorrhage)! or! presumptive! sources! (presence! of!
diverticulosis! or! haemorrhoids! without! bleeding! in! absence! of! other! potential!
bleeding!sources).!RodriguezPMoranta!et)al)reported!only!definite!diagnoses,!but!
did!not!define!this,!and!Albeldawi!et)al)did!not!define!diagnosis.!
!
When! presumptive! and! definite! diagnoses! are! included! in! diagnostic! yield,! no!
difference!was!observed!between!early!versus! late!colonoscopy!in!the!RCT!(RR!
1.17,!95%!CI!0.87!to!1.56)!or!pooled!analysis!of!the!NRSI!(OR!0.68,!95%!CI!0.31!
to!1.49,!3!studies,!527!participants,!I2=9%,!Figure!2a).!When!diagnostic!yield!was!
limited! to! definite! diagnoses,! early! colonoscopy! was! associated! with! a! higher!
diagnostic! yield! in! the! NRSI! (OR! 1.86,! 95%! CI! 1.21! to! 2.86,! 3! studies,! 650!
participants!I2=42%,!Figure!2b)!although!this!was!not!significant!in!the!RCT!(RR!
1.12,!95%!CI!0.70!to!1.78).!!

! 52!
!
!
!
!
!
!
!
!!!!!!!!!!!Figure!2:!Forest!plot!of!comparison!of!NRSI!a)!presumptive!diagnoses,!b)!definite!diagnoses.!95%!CI,!95%!confidence!interval!!
!
!
All#studies#employed#endoscopic#haemostasis#with#a#minimum#of#three#available#
modalities# (clipping,# banding,# thermocoagulation,# argon# plasma# coagulation,#
epinephrine# injection),# the# specific# type# depending# on# pathology# and#
endoscopist’s# preference.# The# therapeutic# yield# was# superior# in# the# early#
colonoscopy#group# in#the#pooled#analysis#of# the#NRSI#(OR#3.08,#95%#CI#1.93#to#
4.90,#4#studies,#707#participants#I2=7%,#Figure#3a),#but#not#significant#in#the#RCT#
(RR#1.0,#95%#CI#0.36#to#2.81).##
#
Mean# LOS# was# reported# in# three# studies# 71# 93# 101.# Early# colonoscopy# was#
associated#with#a#shorter#LOS#in#NRSI#(MD#2.64#days,#95%#CI#1.54#to#3.73,#two#
studies,#506#participants,#I2=0%)#and#in#the#RCT#(MD#0.40#days,#95%#CI#0.06#to#
0.74,#72#participants)#(Figure#3b).##
#######################
53#
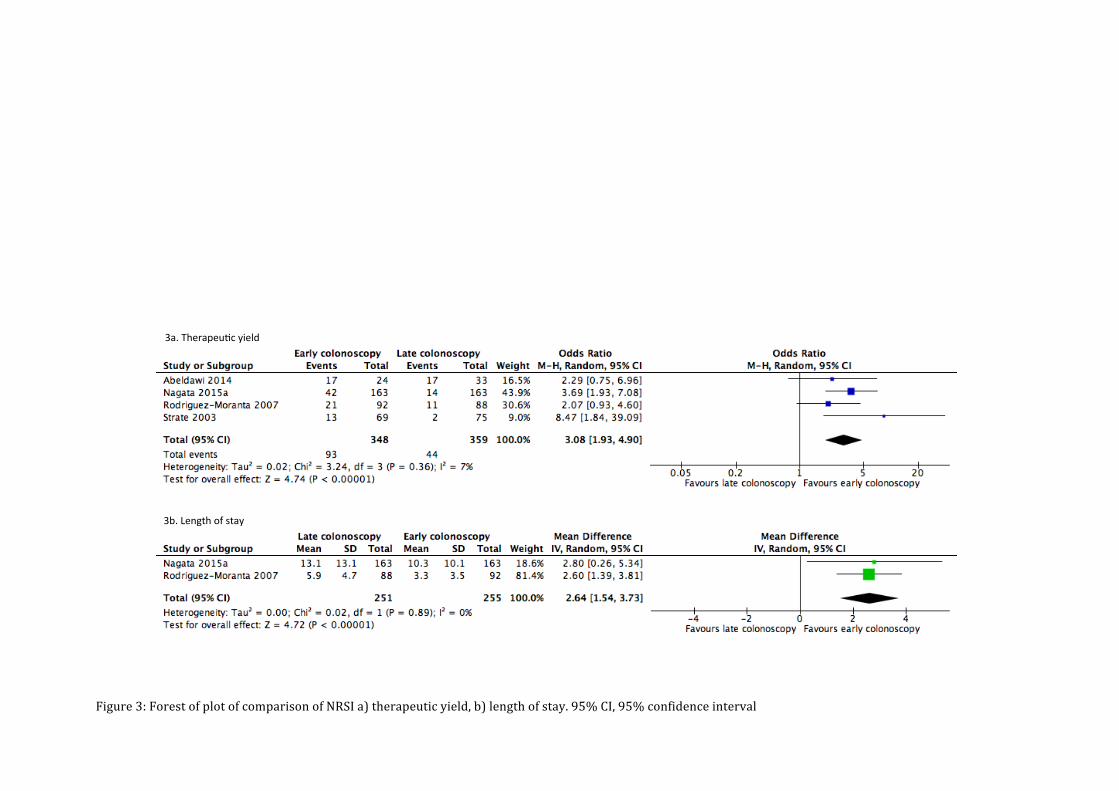
! 54!
!
!
!
!
!!!!!!!!!!!!!!!!!Figure!3:!Forest!of!plot!of!comparison!of!NRSI!a)!therapeutic!yield,!b)!length!of!stay.!95%!CI,!95%!confidence!interval!!
!
!
3a.$Therapeu+c$yield$
3b.$Length$of$stay$

! 55!
Re%bleeding!was!reported!in!the!RCT!and!two!NRSI100!101,!but!all!varied!in!their!
definition!(Table!3)!so!were!not!pooled.!There!was!no!difference!in!re%bleeding!
between!early!and!late!colonoscopy!in!the!RCT!(RR!1.6,!95%!CI!0.58!to!4.43,!72!
participants),! or! the! NRSI! (Nagata! et# al# OR! 1.96,! 95%! CI! 0.94! to! 4.11,! 326!
participants,!and!Albeldawi!et#al#OR!0.7,!95%!CI!0.2!to!2.44,!57!participants).!!
!
Table!3:!Inter%study!variability!in!the!definition!of!re%bleeding!
Study!! Definition!of!re%bleeding!
Green!2005! Haematochezia!!(defined!as!any!one!of!!>3!bloody!bowel!movements!in!<8!h,! ICU! admission,! >5%! decrease! in! Hct! in! <12! h,! transfusion! of! >3! units!RBC,!hemodynamic! instability! in!previous!6h!defined!as! angina,! syncope,!pre%syncope,! orthostatic! vital! signs,! MAP! <80! mmHg! or! HR>110)! after!clinical!cessation!of!the!index!bleeding!event!!
Laine!2010! Haematochezia! persisting! for>24h,! recurrent! haematochezia! after! initial!resolution! (e.g,! brown! stool! followed! by! haematochezia),! HR>! 100! or!SBP<100mmHg!after!hemodynamic!stability!for!≥1h,!or!hemoglobin!drop>!2g/dl!after!stable!hemoglobin!values≥!3h!apart!
Nagata!2016! Significant! amounts! of! fresh! bloody! or! wine%coloured! stools! after! index!colonoscopy!with! unstable! vital! signs;! SBP≤90!mmHg! or! HR≥110! or! the!need!for!blood!transfusion!
Strate!2003! Blood! per! rectum! after! 24! h! of! stability! accompanied! by! a! drop! in!Hct≥20%,!and/or!a!requirement!of!additional!blood!transfusions!
Abeldawi!2014! After!clinical!cessation!of!index!bleeding!event!during!hospitalization!
Nagata!2015! Significant! fresh!bloody!or!wine! coloured! stool! accompanied!by!unstable!vital! signs;! SBP≤90! mmHg! or! HR≥110! and! non%response! to! ≥2! units!transfused!blood!!
Jensen!2000! Self%limited! or! recurrent! haematochezia! that! required! no! more! than! an!additional! 2! units! of! packed! red! cells! or! continued! or! recurrent!haematochezia!that!required!at!least!3!units!of!packed!red!cells!
Ishii!2011! Clinical!evidence!of!recurrent!bleeding!
*Hct,!haematocrit.!
!
RBC!transfusion!was!reported!in!the!RCT71!and!one!NRSI101;!patients!in!the!early!
group!of!the!RCT!received!more!transfusions!(mean!difference!0.8!units,!95%!CI!
0.65! to! 0.95,! 72! participants),! but! in! the! NRSI! there! was! no! difference! in! the!
! 56!
number!of!participants!receiving!RBC!transfusion!(OR!1.00,!95%!CI!0.62!to!1.63,!
326!participants).!
#
Adverse! events! were! reported! in! two! studies71! 101.! Laine! et# al! reported! one!
perforation!in!the!late!colonoscopy!group!(RR!0.33,!95%!CI!0.01!to!7.92).!Nagata!
et# al# reported! no! major! colonoscopy%related! adverse! events! in! either! cohort.!
Mortality!was!reported!in!two!studies71!100.!There!were!no!deaths!in!the!study!by!
Albeldawi!et#al,!but!there!were!two!deaths!in!the!urgent!colonoscopy!arm!in!the!
RCT!by!Laine!et#al!(RR!5.00,!95%!CI!0.25!to!1.00).!One!patient!developed!a!fatal!
intracranial!haemorrhage!and!the!other!had!a!prolonged!hospitalisation!due! to!
medical!co%morbidities!and!died!after!a!cardio%respiratory!arrest.!!
!
CTA#and#MA#
To!maximise!study!eligibility!we!did!not!pre%specify!definitions!of!urgent!or!non%
urgent!CTA!or!MA.!No!studies!were!identified.!

! 57!
2.6!Choice!of!treatment!for!acute!lower!gastrointestinal!bleeding!
#
Therapeutic#endoscopy#versus#mesenteric#embolization#
We!identified!no!RCTs,!NRSIs!or!on%going!trials.!!
#
Therapeutic#endoscopy#versus#other#
One! prospective! cohort! study! compared! endoscopic! therapy! (adrenaline! or!
thermocoagulation)!to!a!historical!control!comprising!of!conservative!or!surgical!
treatment! in! patients! with! diverticular! bleeding.98! Patients! that! received!
endoscopic! treatment!were! less! likely! to!require!surgery! for!bleeding!(Peto!OR!
0.14,!95%!CI!0.02!to!0.88,!27!participants),!re%bleed!(Peto!OR!0.10!95%!CI!0.02!to!
0.51)!or! receive!a!RBC! transfusion! (Peto!OR!0.10!95%!CI!0.02! to!0.51).!An!on%
going! RCT! is! comparing! endoscopic! therapy! with! barium! impaction! for!
diverticular!bleeding!(Matsuhashi!et#al,#JPRN%UMIN000008287).!!
!
Mode#of#Endoscopic#haemostasis##
No!RCTs!were!identified.!Two!retrospective!cohort!studies!were!identified,!both!
comparing! endoscopic! band! ligation! (EBL)! with! endoclipping! in! diverticular!
bleeding.96!97! The! primary! outcome! in! both! studies!was! re%bleeding;! Ishii! et#al!
reporting! 60! day! rates! of! 1/16! (6.2%)! and! 16/48! (33.3%)! for! EBL! and!
endoclipping!respectively,!although!this!was!not!significantly!different!(OR!7.50,!
95%!CI!0.91!TO!61.94,!64!participants).!Seven!patients!in!the!endoclipping!group!
required!radiological!control!of!bleeding!versus!none!in!the!EBL!group!however!
this! was! non%significant! (Peto! OR! 4.37,! 95%! CI! 0.72! to! 26.37).! Nakano! et# al!
followed!patients!for!two!years!and!also!found!that!large!numbers!of!patients!re%

! 58!
bled! in! each! group! (EBL! 24/50,! 48.0%;! endoclipping! 18/39,! 46.2%)! although!
there!was! no! difference! between! the! two!modalities! (OR! 0.93! 95%! CI! 0.40! to!
2.15,! 89! participants).! No! patient! experienced! complications! related! to!
endoscopy!in!either!study.!!
!
One!on%going!RCT!comparing!TC%325! (Hemospray)!monotherapy!at! endoscopy!
to!standard!endoscopic!therapy!in!patients!with!UGIB!or!LGIB!due!to!malignancy!
was!identified!(Barkun!et#al,!NCT02135627).!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!

! 59!
2.7!Assessment!of!methodological!quality!
The!RCTs!were!all!deemed!at!high!or!unclear!risk!of!bias!due!to!blinding!(Table!
4).!Laine!et#al#stated!that!their!trial!was!not!blinded.!Green!et#al#also!stated!that!
the! physicians! caring! for! the! patients!were! not! blinded! and! gave! no! detail! on!
blinding!of!outcome!assessors.!Leung!at#al#stated!that!patients!and!investigators!
were# unaware! of! the! randomisation! sequence! but! patients! were! assigned! to!
physically!different!interventions!(capsule!endoscopy!or!MA)!so!blinding!is!likely!
to!have!been!broken.!The!nature!of!the!interventions!used!in!these!studies!makes!
blinding!difficult.! For! some!objective! outcomes,! this!may!be! acceptable! but! for!
other! more! subjective! outcomes! such! as! diagnostic! yield! this! may! introduce!
significant!bias.!!
!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!

! 60!
Table!4:!Assessment!of!methodological!quality;!Cochrane!risk!of!bias!for!RCTS,!Newcastle%Ottawa!for!NRSI!!
RCT! Sequence!generation!
Allocation!concealment!
Blinding!of!participants! and!personnel!!
Blinding!of!outcome!assessors!
Incomplete!outcome!data!
Selective!outcome!reporting!
Other!!
Green!2005!
Low! Unclear! High! Unclear! Low! Unclear! Low!
Laine!2010!
Low! Low! High! High! Low! Low! High!
Leung!2012!
Low! Low! High! Unclear! Low! High! Low!
NRSI! Representativeness!(1)!
Selection!of! non%exposed!(1)!
Ascertainment! of!exposure!(1)!
Outcome! of!interest!not!present!at! start!of! study!(1)!
Comparability!(2)!
Assessment! of!outcome!(1)!
Follow! up!long!enough!and!adequate!(2)!
Adeldawi!2014!
1! 1! 1! 1! 1/0! 1! 1/1!
Ishii!2011!
0! 1! 1! 1! 0/0! 1! 1/1!
Jacovides!2015!
1! 1! 1! 0! 0/1! 1! 1/1!
Jensen!2000!
0! 1! 1! 1! 0/0! 1! 1/1!
Nagata!2016!
1! 1! 1! 1! 1/1! 1! 1/1!
Nagata!2015!
1! 1! 1! 1! 1/0! 1! 1/1!
Nakano!2015!
0! 1! 1! 1! 0/0! 1! 1/0!
Sun!2011!
0! 0! 1! 1! 0/0! 1! 1/1!
Yabutani!2006!
0! 1! 1! 0! 1/1! 1! 1/1!
Yamaguchi!2006!
1! 1! 1! 1! 1/1! 1! 1/1!
Ketwaroo!2012!
0! 0! 1! 1! 0/0! 1! 1/1!

! 61!
Strate!2003!
1! 1! 1! 1! 1/1! 1! 1/1!
Rodriguez%!Moranta!2007!
1! 1! 1! 1! 1/1! 1! 1/1!
!!
Re%bleeding! may! also! be! subject! to! bias! due! to! lack! of! blinding.! Additionally,!
there! was! considerable! inter%study! variation! in! the! definition! re%bleeding.!!
Several!studies!characterised!re%bleeding!by!the!persistence!of!on%going!signs!of!
bleeding71! 101! 102! but! these! definitions! may! have! also! captured! patients! with!
failed! haemostatic! intervention,! not! true! re%bleeding.! Most! studies! used! a!
definition! that! included! a!period!of! clinical! stability61!78! although! some!did!not!
define!the!criteria!that!would!need!to!be!met!to!establish!a!new!bleeding!event97!
100!(Table!3).!!
!
The!trial!by!Leung!et#al!was!deemed!to!be!at!high!risk!of!bias!as!not!all!outcomes!
pre%specified! in! the! study!protocol!were! reported,!particularly!LOS.!Due! to! the!
nature! of! the! procedure,! LOS!may!be! longer! for! capsule! endoscopy,!which! has!
implications!for!its!use!in!the!acute!inpatient!setting.!The!study!by!Laine!et#al#was!
subject!to! ‘other’!source!of!bias!as! it!was!terminated!early!because!the!hospital!
changed!its!protocol!on!allowing!colonoscopy!in!the!emergency!room,!although!
the!reasons!for!this!are!not!given.!!
!
Risk!of!bias!in!the!NRSI!was!assessed!using!the!Newcastle%Ottawa!scale.!The!two!
most! common! areas! of! poor! performance! in! the! NRSI! were! selection! of!
participants,! particularly! representativeness! of! the! exposed,! and! the!
! 62!
comparability! of! cohorts.! Six! studies! scored! no! stars! for! representativeness! of!
LGIB!as! they!studied!a!single!pathology92!96%98!or!a!single! intervention! that!was!
related!to!severity!of!bleeding94!95.!This!limits!the!generalisability!of!these!results!
to!the!LGIB!population!as!a!whole.!!
!
Three!studies!included!no!data!on!whether!they!adjusted!for!confounders94!95!97,!
one! study!provided!no!data! on! confounders! and! also!populated!one! treatment!
arm! using! an! intervention! that! is! likely! to! be! related! to! severity! of! bleeding!
(endoscopic!haemostasis)98!and!one!study!compared!baseline!demographics!for!
each! group,! but! did! not! include! cardiovascular! parameters! or! baseline!
transfusion!requirements.96!There!is!likely!to!be!significant!baseline!imbalances!
between!the!cohorts!in!these!studies.!None!were!deemed!of!sufficient!quality!to!
permit!data!synthesis.!
!
!
!
!
!
!
!
!
!
!
!
!
! 63!
2.8!Implications!for!practice!in!the!United!Kingdom!
!
LGIB! presents! a! significant! healthcare! burden! in! the! UK10! but! there! is!
considerable! uncertainty! regarding! its! optimal! management.6! This!
comprehensive! review! of! the! diagnostic! and! therapeutic! yield! of! treatment!
modalities!demonstrates!a!paucity!of!evidence!across!the!majority!of!diagnostic!
and!therapeutic!techniques.!!
!
Colonoscopy! is! recommended!as! the! first%line!diagnostic!procedure! for!LGIB! in!
international! guidelines47! but! questions! remain! regarding! its! timing! and!
suitability! for! all! patients.! The! limited! studies! comparing! interventions!
demonstrate! higher! diagnostic! rates! with! colonoscopy! compared! to! standard!
care! algorithms,! but! that! identification! of! lesions!with! active! bleeding!may! be!
enhanced!by!the!concomitant!use!of!CTA.!However,!this!did!not!translate!into!an!
increase! in! therapy,! and! when! haemostasis! was! undertaken,! most! studies!
showed! no! or!minimal! impact! upon! clinically! important! outcomes! such! as! re%
bleeding!or!RBC!transfusion.!!
!
The!area!with! the!greatest! evidence!was! timing!of! colonoscopy,! although!most!
studies!were!non%randomised.!Early! colonoscopy!was! associated!with! a!higher!
diagnostic!yield,!rate!of!haemostasis!and!a!reduction!in!LOS.!However,!there!was!
no!evidence!that!earlier!colonoscopy!had!any!impact!upon!death!or!re%bleeding.!
Paradoxically!there!was!higher!RBC!transfusion! in!the!early!colonoscopy!group!
of!the!RCT,!although!this!may!represent!baseline!imbalances!between!the!groups,!
as! the! initial! haemoglobin! was! also! lower! in! the! early! arm.71! It! is! not! known!

! 64!
whether! colonoscopy!within! 24! hours! of! presentation! is! routinely! available! in!
hospitals!in!the!UK.!!
!
In!contrast!to!OGD!in!UGIB,!colonoscopy!in!the!acute!setting!can!be!challenging!to!
perform,! requires!rapid!bowel!preparation!and!may!be!poorly! tolerated!by! the!
patient.!Only!two!studies!reported!complications,!but!overall!early!colonoscopy!
appeared!safe.!In!one!RCT,#two!patients!who!received!urgent!colonoscopy!died.71#
Although!neither!was!attributed!to!the!intervention,!the!potential!to!cause!harm!
in!patients!with!extensive!co%morbidities!should!not!be!underestimated.!!
!
The!impact!of!early!colonoscopy!on!length!of!hospital!stay!has!clear!benefits.!A!
micro%costing!analysis!of!UGIB!admissions!reported!an!average!cost!of!£2458!per!
patient,!most!of!which!was!due!to!the!cost!of!the!hospital!bed.73!Outcomes!other!
than! LOS! must! also! be! considered;! there! was! no! difference! in! re%bleeding! or!
death.!The!value!of!investment!in!24%hour!lower!GI!endoscopy!services!therefore!
requires!further!assessment.!
!
Most!of!these!studies!on!timing!of!colonoscopy!were!conducted!in!patients!who!
were! subsequently! diagnosed! with! diverticular! bleeding,! limiting! the!
generalizability!of!these!findings!to!other!sources!of!bleeding.!The!proportion!of!
patients!admitted!with!LGIB!due!to!diverticular!bleeding!in!the!UK!is!not!known.!!
!
Timing! of! colonoscopy! has! been! the! focus! of! three! recent! systematic! reviews.!
Kouanda!et#al! and! Seth!et#al! included!RCTs! and! cohort! studies,! but! differed! in!
their! classification! of! several! large! database! studies! that! we! rejected! as! case!

! 65!
series,! or! restricted! their! search! to! English! language! studies.104!105! Regardless,!
the! authors! reported! similar! findings;! there! was! no! difference! in! rates! of! re%
bleeding,! death! or! transfusion.! In! contrast! to! the! present! review,! Seth! et! al!
reported! that! there! was! no! difference! in! therapeutic! yield! or! LOS! with! early!
colonoscopy.! For! therapeutic! yield,! the! authors! did! not! include! data! from!
Albeldawi!et! al! in! the!meta%analysis,! but! the! reasons! for! this! are!not! clear.! For!
LOS,! the! authors! pooled! estimates! from! RCTs! with! NRSI,! which! contravenes!
Cochrane!guidance,88! and!may!account! for! the!different! findings! to! the! current!
review.!Sengupta!et#al!used!a!similar!study!classification!system!to! the!present!
review,! and! also! pooled! estimates! from! RCTs! and! NRSI,! but! also! reported! no!
difference!in!clinical!outcomes!with!early!colonoscopy.91!
!
We! found! only! minimal! studies! examining! therapeutic! intervention! at!
colonoscopy.! These! studies! included! combinations! of! clipping,! banding,! argon!
laser,!heater!probe!or! forceps,!adrenaline! injection!or!snare!polypectomy.!Only!
banding! and! clipping!were! examined! in! their! own! right.!Re%bleeding! following!
endoscopic! haemostasis! was! reported! as! 6%48%! in! the! cohort! studies,96! 97! 101!
raising! questions! regarding! the! efficacy! of! endoscopic! haemostasis.! This! is!
important! given! the! absence! of! evidence! comparing! it! to! other! treatment!
options,!notably!embolisation.!This!uncertainty!is!reflected!in!the!infrequent!use!
of! endoscopic!haemostasis! reported! in!population! studies!of! LGIB,8!12! although!
its!utilisation!in!the!UK!is!not!known.!!
!
In! the! acute! setting! CTA! may! be! an! alternative! to! colonoscopy,! although! we!
found! only! two! studies! directly! comparing! these! two! interventions.! 64! 92! Pre%
! 66!
colonoscopy! CTA! was! associated! with! higher! diagnosis! of! vascular! lesions! in!
comparison! to! colonoscopy! alone.! There! were! no! studies! to! inform! optimum!
timing!or!patient!selection!with!regard!to!severity!of!bleeding.!Studies!on!upper!
and!lower!GIB!have!reported!that!CTA!has!a!comparable!diagnostic!yield!to!that!
of!MA79!but! further!research!comparing! it!with!other! first%line! investigations! is!
required.! The! quoted! minimum! 0.4ml/min! required! volume! of! blood! loss! to!
demonstrated! extravasation! of! contrast! is! based! on! animal! studies106.! Further!
areas! of! research! should! focus! on! the! clinical! outcomes! of! endotherapy! and!
embolization,!and!the!role!of!CT.!
!
There!are!several!limitations!to!this!review.!Most!evidence!originates!from!NRSI,!
with! significant! bias,! which! limits! the! strength! of! the! conclusions! that! can! be!
drawn! from! this! review.! More! randomised! data! particularly! on! the! timing! of!
colonoscopy! is! urgently! required.! Systematic! review!of!NRSIs! is! limited!by! the!
variable! description! of! study!methodology,!making! their! classification! difficult.!
This! is! evidenced! by! the! different! studies! that! are! included! in! reviews! of! the!
same!topic!with!similar!inclusion!criteria.91!104!105!
!
In! summary,! whilst! there! was! a! paucity! of! high! quality! evidence! across! all!
interventions!we!found!that!colonoscopy!within!24!hours!had!higher!diagnostic!
and! therapeutic! yields,! and! shorter! LOS.! Chapters! 3,! 4! and! 5! present! the! first!
national! study! of! LGIB! undertaken! in! the! UK,! and! provide! data! on! current!
practice!in!the!UK,!including!the!frequency!and!timing!of!inpatient!colonoscopy,!
and!diagnostic! yields! in! a!UK!population!of! acute!admissions.!The! study!of! the!

! 67!
organisation!of!services!provides!data!on!whether!the!provision!of!colonoscopy!
within!24!hours!is!currently!feasible!in!the!NHS.!!
!

! 68!
CHAPTER!3!
NATIONAL!OBSERVATIONAL!STUDY!OF!ACUTE!LOWER!
GASTROINTESTINAL!BLEEDING:!METHODOLOGY!
!
This! chapter! describes! how! the! observational! study! process! was! piloted,! how!
hospitals!were!recruited,!cases!identified!and!data!collected!and!analysed.!!
!
3.1!Recruitment!of!sites!
All!NHS!Trusts!in!England!admitting!acute!surgical!and!medical!admissions!were!
contacted! directly! in! June! 2015! and! invited! to! participate.! Letters! and! emails!
explaining! the! rationale! and! aims! were! sent! to! the! Medical! Director,! Chief!
Executive,! Clinical! Audit! Department! and! the! haematologist! with! primary!
responsibility! for! transfusion,! as! well! as! transfusion! practitioners! within! each!
acute!hospital.! If! there!was!no!response,!a! further!two!written!invitations!were!
sent! in! July! and! August! 2015.! If! there! was! no! response! after! three! formal!
requests! it!was! assumed! that! the! hospital!would! not! be! participating.!Medical!
Directors!were!asked!to!give!permission!for!their!hospital! to!participate!and!to!
provide! the! contact!details! of! their!Clinical! Lead! for! Surgery.!The!Clinical! Lead!
was!then!provided!with!information!about!the!methodology!and!timeline!of!the!
study!and!asked!to!nominate!a!local!lead!to!co%ordinate!the!project.!!
!
This!study!was!offered!to!NHS!hospitals!in!Scotland,!Wales!and!Northern!Ireland!
via! their! national! blood! services.! Independent! hospitals! were! not! invited! to!
participate!since!GI!bleeds!are!predominantly!managed!in!the!NHS.!In!June!2015!
! 69!
there!were!140!eligible!NHS!trusts!in!England,!and!the!aim!was!to!recruit!80%!of!
these.!!
!
3.2!Case!Identification!
Eligible! cases! included! all! unselected! patients! that! presented! with! LGIB! that!
resulted! in!an!admission! to!hospital!or!developed!whilst!patients!were!already!
admitted! for!another!reason.!There!are!no!hospital!diagnostic!codes!specific! to!
LGIB,! limiting! case! identification! from! hospital! registries.! Methods! aimed! at!
identifying!LGIB!cases!by!mapping!to!‘classification!trees’!using!codes!such!as!the!
ICD76! have! been! shown! to! have! varying! performance.77! A! previous! large!
prospective!audit!on!UGIB! successfully! addressed! this! constraint!by! contacting!
clinical! teams.33! Cases! were! therefore! identified! by! clinical! teams,! using!
presenting! symptoms! as! opposed! to! examination! findings! or! discharge!
diagnoses.! Cases! were! identified! prospectively! and! followed! until! death,!
discharge!or!28th!day!of!admission.!Central!data!collectors!monitored!each!case!
for!28!days!post%discharge!for!re%admission.!!
!
Pilot#study#1#
To! establish! a! pattern! of! hospital! admission! locations! for! patients! with! acute!
LGIB,! five! hospitals! (including! a! tertiary! referral! centre! for! interventional!
radiology! and! a! small! district! general! hospital)! were! asked! to! describe! their!
referral! pathways! and! pilot! the! process! of! case! identification.! Eleven! potential!
departments!and!wards!were!identified!as!likely!to!accommodate!patients!with!
LGIB.! Over! a! two! week! period,! each! hospital! was! instructed! to! contact! each!

! 70!
location! multiple! times! to! identify! locations! with! the! highest! and! lowest! case!
yield!by!recording!the!number!of!identified!cases!per!department!(Table!5).!!
Table!5:!Pilot!case!identification!tool!!Location! Present! in!
your!hospital!(Y/N)!
Frequency!of!contact!
Number! of!cases!identified!Week!1!
Number! of!cases!identified!Week!2!
Comment!
Surgical! Assessment!Unit!
! Daily! ! ! !
Endoscopy!unit! ! Daily! ! ! !On%call! Surgical!Registrar!
! Daily! ! ! !
A&E!Nurse!in!Charge! ! Daily! ! ! !Medical! Assessment!Unit!
! Daily! ! ! !
Blood!Bank!!
! X3!per!week! ! ! !
Adults!Wards!!
! X3!per!week! ! ! !
Emergency!theatre! ! X2!per!week! ! ! !GI!Bleed!Unit! ! Daily!! ! ! !Interventional!Radiology!Suite!
! X3!per!week! ! ! !
Death!Certificates! ! Weekly! ! ! !!!Feedback! on! ease! of! case! identification,! time! spent! and! suggestions! for! other!
locations!were!collected.!Of!the!five!hospitals,!only!one!site!was!able!to!provide!
data!for!the!complete!time!period,!identifying!28!cases!of!LGIB.!The!low!response!
rate!of! the!other!hospitals! indicates! that! this!kind!of! case!ascertainment! is!not!
reproducible! or! reliable.! A! recent! national! audit! of! severe! gastrointestinal!
haemorrhage!demonstrated! that!unlike!UGIB,!which!may!present! to!a! range!of!
departments! and! specialities,! LGIB! presents! to! a! more! limited! selection! of!
locations6,! namely! surgery,! gastroenterology! and!general!medicine!wards.!This!
was!also!demonstrated!by!the!28!cases!identified!in!this!pilot!study;!all!but!one!
case!was!identified!by!daily!contact!with!the!admitting!surgical!team!and!acute!
medical!admissions!unit.!To!maximise!case!ascertainment!in!this!national!study,!
study!leads!were!asked!to!have!daily!contact!with!surgical!admission!units!and!

! 71!
the!surgical!on%call!team,!daily!contact!with!medical!admission!units!and!on%call!
team!and!to!visit!the!gastroenterology!wards!three!times!per!week.!!
!!!Cases!were!eligible!if!they!fulfilled!the!following!criteria:!!
• Age!≥!16!years!
• History! of! bright! or! dark! blood! per! rectum,! maroon! coloured! stool! or!
blood!mixed!in!with!stool,!clots!per#rectum!or!passage!of!melaena!without!
haematemesis.!!
!
Melaena! without! haematemesis! was! included! so! that! cases! of! small! bowel!
bleeding!were!unlikely!to!be!missed.!Previous!reports!have!shown!that!it!can!be!
difficult! to!distinguish!upper! from!lower!GI!sources!of!bleeding6!so! to!optimise!
the! identification! of! LGIB! the! inclusion! criteria! were! deliberately! broad.!
Inevitably! a! small! number! of! patients! with! UGIB! would! be! captured! in! the!
dataset,!but!this!reflects!the!uncertainties!that!may!exist!in!routine!clinical!care.!
Once!data!collection!was!complete,!UGIB!cases!were!identified!using!presenting!
features!and!findings!at!OGD.!The!following!cases!were!excluded:!!
• Definite!UGIB!(proven!stigmata!of!UGIB!on!OGD)!
• Probable!UGIB!(no!stigmata!of!haemorrhage!but!abnormal!OGD)!
• !Suspected! UGIB! (presentations!with!melaena! only! but! no! confirmatory!
OGD)!
!
!
!
! 72!
3.3!Data!Collection!!Over!two!months!between!1st!September!2015!and!31st!October!2015,!two!broad!
categories!of!data!were!collected;!organisational!and!individual!patient!data.!!
#
Organisation#data:#
Organisational!data!recorded!the!availability!of!services!for!the!investigation!and!
treatment! of! LGIB.! The! questionnaire!was! available! as! a! paper! version! and! an!
electronic! survey.! Outcomes! included! the! in%! and! out%of%hours! availability! of!
endoscopy,!interventional!radiology!and!surgery.!Data!on!how!patients!accessed!
these! investigations! and! treatment! in! hospitals! without! onsite! services! were!
collected.!Each!hospital!was!asked!to!complete!one!copy!of!this!questionnaire.!
!
Individual#patient#data:#
This!dataset!captured!the!clinical!characteristics!and!outcomes!of!patients!with!
acute! LGIB.! The! data! collection! questionnaire! included! questions! on! clinical!
examination! findings,! the! timing! and! results! of! endoscopy,! radiology! and!
surgery,! the!prevalence!of!different!aetiologies!of!LGIB!and!the!use,! timing!and!
volume! of! blood! products.! Outcomes! included! length! of! stay,! in%hospital!
morbidity! and! mortality,! 28%day! re%admission! rates,! re%bleeding! rates! and!
transfusion! requirements.! Data! on! anticoagulation! and! antiplatelets! were!
collected,! including! methods! of! their! reversal.! All! data! were! obtained!
prospectively!from!patient!notes!and!electronic!hospital!records.!
!!In! each! hospital,! a! team! consisting! of! a! study! lead,! case! identifier! and! several!
data!enterers!collected!the!data! in!each!NHS!trust.!The! lead!ensured!that!cases!

! 73!
are!being!identified!and!entered!and!that!the!data!were!complete!and!accurate.!
The! leads! were! predominantly! colorectal! or! general! surgical! consultants! or!
registrars,! although! gastroenterologists! and! transfusion! practitioners! also!
participated.! I! co%ordinated! the! leads! and!worked!with! the! case! identifier! and!
case!enterers!in!each!site!as!needed.!!
!!#!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!

! 74!
3.4!Pilot!Study!2!!!The! questionnaires! were! subject! to! an! extensive! pilot! process.! First,! I! piloted!
both!questionnaires!on%site!at!three!NHS!hospitals.!I!worked!with!a!study!lead!at!
each!site!to!trial!the!organisational!questionnaire!and!the!patient!questionnaire!
on! real! cases! of! LGIB! that! they!had! identified! that!week.! The! terminology!was!
checked! to! ensure! applicability! across! sites! and! to!make! sure! that! all! required!
data!were!readily!reported!in!medical!notes!and!electronic!records.!!
!
!Secondly,! ten!NHS!hospitals!were! asked! to!pilot! the!questionnaires! externally.!
Each!site!was!asked! to!review!the!questionnaires!and!record! feasibility!of!data!
collection!for!each!question!via!a!grading!system!of!1%3!to!represent!agreement!
or!disagreement!with!validity!and! feasibility!both!of!question!content,!wording!
and!availability!of!information!
!
Seven! sites! returned! the! organisational! questionnaire! pilot! and! all! but! two!
questions! were! answered! as! expected.! The! questions! found! to! be! difficult! to!
complete! asked! for! a! recording! of! the! availability! of! guidelines! on! the!
management! of! LGIB,! which! were! uniformly! unanswered.! On! review! it! was!
decided!that!the!data!collected!by!these!questions!were!not!essential!and!time%
consuming!to!capture.!These!questions!were!removed!from!the!dataset.!!
!
Six!hospitals!were!asked!to!identify!and!complete!patient%specific!questionnaires!
on!five!cases!of!LGIB!to!determine!the!feasibility!of!collecting!the!data!in!a!clinical!
setting.! The! questionnaires! took! 30%40! minutes! to! complete! per! case." All!

! 75!
mandatory!questions!were!deemed!feasible!and!accessible.!The!remainder!of!the!
questions! were! reviewed! and! clarified.! No! questions! were! excluded.! Wording!
and! phrasing! was! amended! for! questions! deemed! ambiguous! based! upon! the!
pilot! exercise.! Answers! were! reviewed! to! ensure! data! was! interpretable! and!
reproducible.!
!!Electronic#Data#Entry#Pilot##An!electronic!version!of!the!questionnaire!was!created!which!was!incorporated!
into! a! password! protected! website.! The! website! was! trialled! on! true! cases! of!
LGIB!as!identified!in!the!pilot!study!and!any!coding!problems!addressed.!!
!
#!!!!!!!!!!!!!!!!!!!!!!!!!!

! 76!
3.5!Data!Analysis!!Data!were!entered! into!an!online!questionnaire,!which!was!accessed!by!a! site%
specific,!password%protected!website.!Paper!versions!of!the!questionnaire!were!
posted! to! sites! to! facilitate! the! collection! of! data! for! those! sites! with! limited!
computer!access.!Cases!and!sites!were!given!a!unique!code!to!enable!data!entry!
without!using!any!patient!or!hospital!identifiers.!!
!
Throughout! the!data! capture!period,! the!website!automatically!downloaded!all!
data!into!a!central!database!regardless!of!whether!the!site!had!indicated!that!the!
data!were! complete.!This! allowed!monitoring!of! the!participants’!progress! and!
regular!counts!of! the!registered!cases.!Once!a!site! indicated!that! it!had!entered!
complete!data! for! a! case,! the! central! study! team!were! alerted,! and! the!dataset!
checked!for!any!missing!mandatory!data!or!nonsensical!responses.!Study!Leads!
within! each! hospital! were! contacted! to! provide! additional! or! corrected! data!
where!necessary.!This!happened!on!a!daily!basis!throughout!and!after!the!study!
period! to!ensure!data!were!as! complete!as!possible.!Whilst! the! study!was! live,!
the! central! project! team! also! reviewed! any! cases! that! were! incomplete! but!
inactive! for! more! than! one! week! and! contacted! the! hospital! study! lead! to!
encourage!their!completion.!!
!Once! all! datasets!were! indicated! as! finished! by! the! local! site,! checked! for! any!
missing! data! and! incorrect! entries! amended! they! were! downloaded! into! one!
unifying!database.!Any!duplicates!were! removed.!Variations! in! spelling!of!drug!
names,!abbreviations!and!treatments!were!standardised.!!
!

! 77!
Although!most! questions! required! a! single! fixed! response,! there! were! several!
with!an!‘other’!option.!Where!appropriate!these!were!recoded!as!one!of!the!other!
fixed!responses!or!compiled!into!an!appendix.!!
!
Data!were!collected!on!several!baseline!co%morbidities,!including!those!listed!in!
the!Deyo!modification107!of! the!Charlson!Co%Morbidity! Index.108!This! is! a! score!
based! on! combinations! of! co%morbidity,! which! can! be! used! to! predict! 1%year!
mortality.108!The!Charlson!index!has!been!used!in!administrative!datasets!but!its!
application! to! clinical! data! is! more! difficult! as! some! of! the! definitions! are!
subjective.! To! enable! its! use! in! a! clinical! setting! we! made! the! following!
amendments;! (1)! mild! or! and! moderate! liver! disease! was! stratified! into! non%
cirrhotic! and! cirrhotic! respectively! for! ease! of! categorisation! using! medical!
notes;!(2)!Congestive!cardiac!failure!is!usually!classified!by!the!New!York!Heart!
Association!criteria109!but!these!criteria!may!not!be!reproducible!in!a!review!of!
surgical!notes.!This!was!changed!to!include!patients!on!pharmacotherapy!or!with!
clinical! examination! findings! consistent! with! heart! failure;! (3)! Peptic! ulcer!
disease!was!classified!by!the!use!of!pharmacological!acid!suppression;!(4)!Renal!
disease! was! re%classified! as! chronic! kidney! disease! stage! 2%3! and! stage! 4! to!
represent! moderate! and! severe! respectively110! (Appendix! 1).! A! Charlson! Co%
morbidity! index! was! calculated! for! each! case.! A! retrospective! review! of! a!
national! database! showed! that! a! Charlson! index! ≥! 2! was! independently!
associated!with!in%hospital!mortality!in!patients!admitted!with!LGIB.12!
!!!

! 78!
The! discharge! diagnosis!was! determined! by! using! the! following! hierarchy:! (1)!
diagnostic! CT,! endoscopy,! proctoscopy,! examination! under! anaesthesia! (EUA),!
laparoscopy!or! laparotomy,! (2)!diagnostic!digital! rectal!examination!(DRE),! (3)!
diagnosis!as!documented!in!medical!notes!or!discharge!papers.!These!were!then!
mapped!to!the!ICD%10:!Classification!of!diseases!of!the!digestive!system.76!!
!!Calculating!the!hospital!resources!required!by!patients!admitted!with!acute!LGIB!
requires!estimates!of!bed!occupancy!and! frequency!of! inpatient!and!outpatient!
investigation! and! treatment.! ! Hospital! bed! requirements!were! described! using!
data!on!LOS,!new!discharge! to!a!nursing!home!or!rehabilitation! facility!and!re%
admission! rates.! Patients! were! only! included! in! re%admission! rates! if! they!
survived!to!discharge.!
!
The! frequency! and! waiting! time! for! investigations! were! calculated! and!
comparisons!by!type!of!investigation!were!made.!LOS!for!patients!who!received!
inpatient! treatment!(as!well!as! investigation)!were!compared!to! those!who!did!
not.!!
!!Statistical#Methods###Missing! data! are! reported! for! each! variable!within! each! corresponding! results!
table.! Data! are! reported! as! numerator! and! percentage,! and! as! median! and!
interquartile! range! (IQR)! as! appropriate.! Categorical! data! are! compared! using!
Chi! square! test! and! continuous! data! by! Wilcoxon! rank! sum.! The! ability! of!
Charlson! Co%morbidity! Index! to! discriminate! mortality,! re%bleeding! and! re%
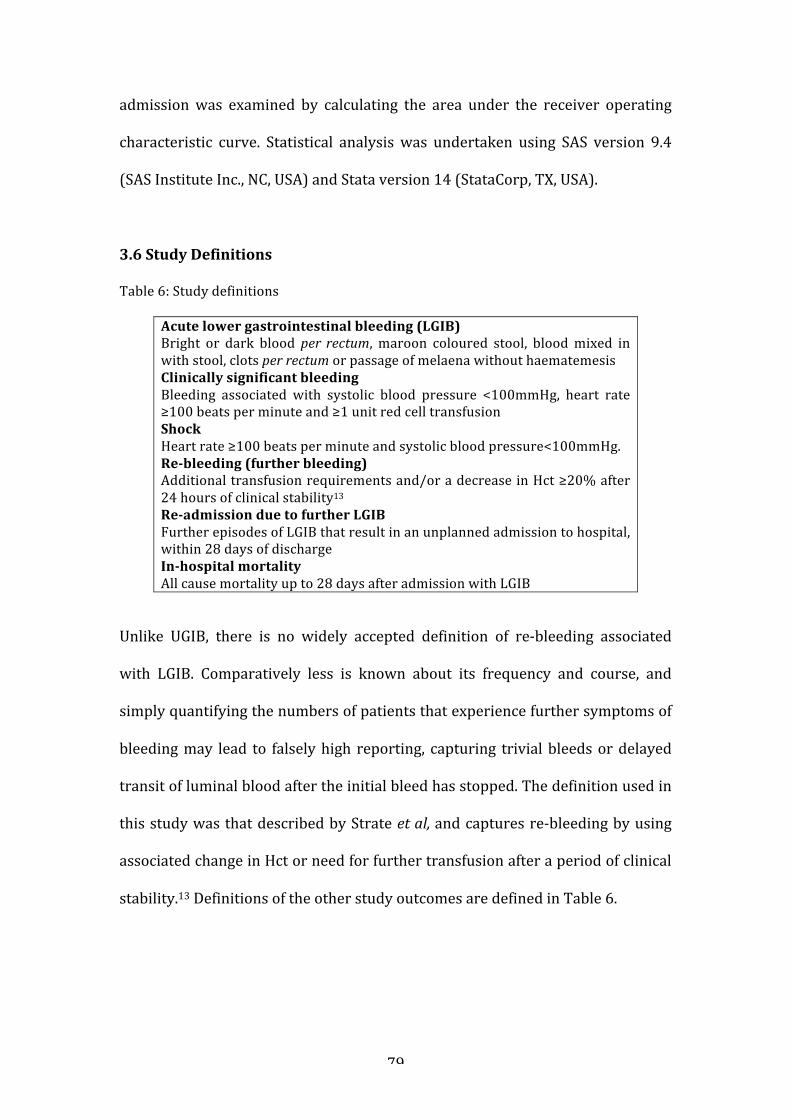
! 79!
admission!was! examined! by! calculating! the! area! under! the! receiver! operating!
characteristic! curve.! Statistical! analysis! was! undertaken! using! SAS! version! 9.4!
(SAS!Institute!Inc.,!NC,!USA)!and!Stata!version!14!(StataCorp,!TX,!USA).!
!
3.6!Study!Definitions!
Table!6:!Study!definitions!!
Acute!lower!gastrointestinal!bleeding!(LGIB)!Bright! or! dark! blood! per# rectum,! maroon! coloured! stool,! blood!mixed! in!with!stool,!clots!per#rectum!or!passage!of!melaena!without!haematemesis!Clinically!significant!bleeding!Bleeding! associated! with! systolic! blood! pressure! <100mmHg,! heart! rate!≥100!beats!per!minute!and!≥1!unit!red!cell!transfusion!Shock!Heart!rate!≥100!beats!per!minute!and!systolic!blood!pressure<100mmHg.!ReZbleeding!(further!bleeding)!Additional!transfusion!requirements!and/or!a!decrease!in!Hct!≥20%!after!24!hours!of!clinical!stability13!ReZadmission!due!to!further!LGIB!Further!episodes!of!LGIB!that!result!in!an!unplanned!admission!to!hospital,!within!28!days!of!discharge!InZhospital!mortality!All!cause!mortality!up!to!28!days!after!admission!with!LGIB!
!
Unlike! UGIB,! there! is! no! widely! accepted! definition! of! re%bleeding! associated!
with! LGIB.! Comparatively! less! is! known! about! its! frequency! and! course,! and!
simply!quantifying!the!numbers!of!patients!that!experience!further!symptoms!of!
bleeding!may! lead! to! falsely!high! reporting,! capturing! trivial!bleeds!or!delayed!
transit!of!luminal!blood!after!the!initial!bleed!has!stopped.!The!definition!used!in!
this!study!was!that!described!by!Strate!et#al,#and!captures!re%bleeding!by!using!
associated!change!in!Hct!or!need!for!further!transfusion!after!a!period!of!clinical!
stability.13!Definitions!of!the!other!study!outcomes!are!defined!in!Table!6.!
!!!!!
! 80!
3.7!Ethical!Considerations!!!This! study!was! carried!out! as!part!of! the!National!Comparative!Audit!of!Blood!
Transfusion!programme,!which!is!supported!by!the!National!Blood!Transfusion!
Committee!in!England.!This!study!details!routine!observational!data!collected!to!
support!the!audit!findings.!The!audit!examined!established!methods!of!care!and!
did! not! influence! patient! management! whilst! it! was! being! conducted,! it! is!
therefore! not! subject! to! ethical! consideration! by! the! NHS! Research! Ethics!
Committee.111!As!stated! in! the!NHS#Code#of#Practice#(2003)!patient! information!
may! be! collected! for! clinical! audit! without! prior! patient! consent.! No! patient!
identifiers!are!collected!as!part!of!this!audit.112!!
"
!!!!!!!!!!!!!!!!!!!!!!!!
! 81!
!CHAPTER!4:!NATIONAL!OBSERVATIONAL!STUDY!OF!ACUTE!LOWER!
GASTROINTESTINAL!BLEEDING:!RESULTS!!!4.1!Patient!Data!!!4.1.Aims!and!Objectives!!The! overall! objective! was! to! characterise! the! clinical! characteristics,!
management!strategies!and!outcomes!of!patients!with!acute!LGIB!presenting!to!
UK!hospitals.!Specific!objectives!included:!
1. Description! of! the! use! of! inpatient! investigations! (lower! GI! endoscopy,!
CTA,! interventional! radiology,! nuclear! medicine! and! surgery)! and! their!
associated! diagnostic! yield! (including! factors! associated! with! failed!
investigation),!complications!and!effect!on!LOS,!re%admissions,!morbidity!
and!mortality.!
2. Evaluation! of! therapeutic! modalities! (endoscopic! haemostasis,!
embolisation!and!surgery)!focussing!on!indication,!therapeutic!yield!with!
regard! to! re%bleeding,! need! for! further! procedures! and! the! associated!
impact!on!outcomes.!
3. Quantification!of!blood!product!transfusion!!
4. Identification!of!patient!specific! risk! factors! for!poor!outcome!to!aid! the!
triage!of!patients!presenting!with!LGIB.!!
!
Reporting!contemporaneous!data!on!presenting!characteristics,! requirement!of!
inpatient! investigation! and! success! of! treatment! will! allow! the! future!
development!of!guidelines!on!the!optimal!management!of!LGIB!with!the!aim!of!

! 82!
improving!patient!care,!reducing!variation!in!practice!and!ultimately!improving!
outcomes.!
!
4.2!Sample!Size!!!Of! 174! hospitals! invited,! 143! (82.2%)! participated,! identifying! 2781! potential!
cases!of!LGIB.!Of!these,!41!were!excluded,!as!they!were!incomplete,!duplicate!or!
cases! of! haematemesis.! There! were! 212! patients! with! proven,! probable! or!
suspected!UGIB!who!were!also!excluded,!leaving!2528!cases!of!LGIB!for!analysis!
(Figure!4).!!
!Figure!4:!Flow!chart!of!excluded!and!included!cases!!
!!!!Estimates! of! the! incidence! of! lower! GI! bleeding! are! scarce,! since! there! are! no!
previous! population! based! studies! of! lower! GI! bleeding! in! the! UK.! The! largest!
study!arising!from!Europe!is!by!Lanas!et#al!who!collected!data!from!10!Spanish!
hospitals!over!a!period!of!10!years!using!hospital!discharge!codes,!and!reported!
2781"cases"iden.fied"
Incomplete"(n=22),""duplicates"(n=9),"
haematemesis"(n=10)"
41"cases"excluded"
Proven"UGIB"(n=107),"probable"UGIB"(n=37),"suspected"UGIB"(n=68)"
212"cases"excluded"2528"cases"LGIB"
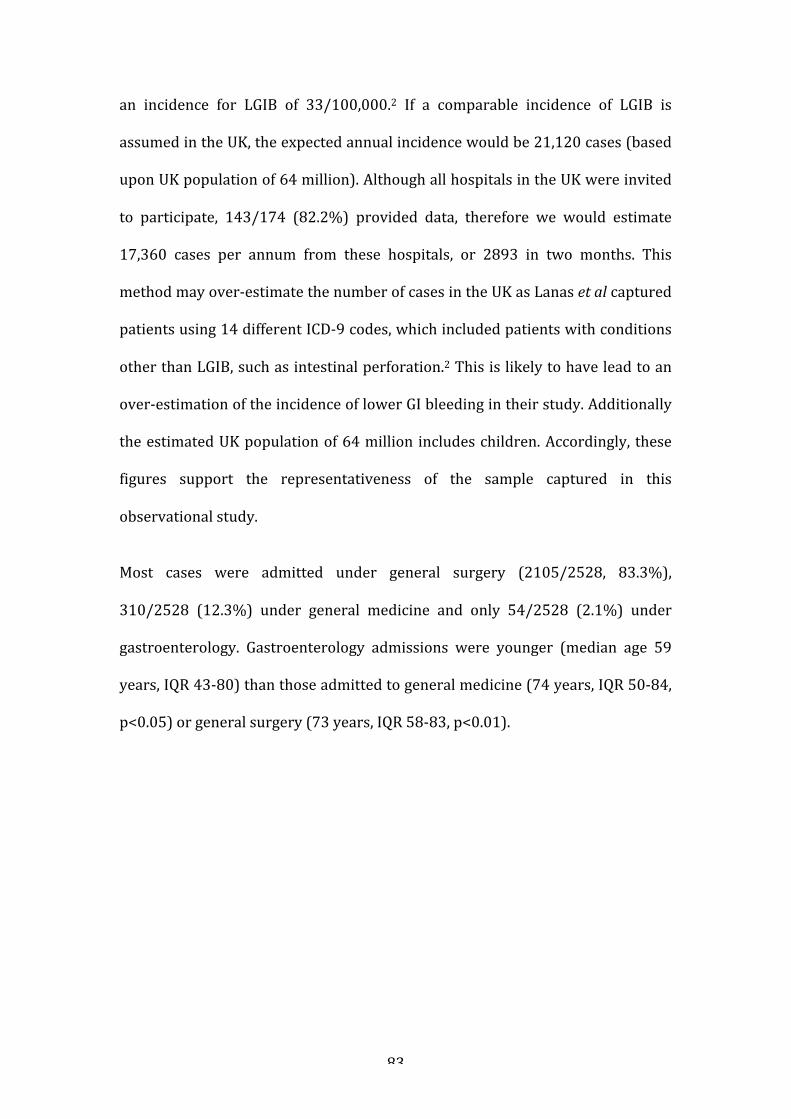
! 83!
an! incidence! for! LGIB! of! 33/100,000.2! If! a! comparable! incidence! of! LGIB! is!
assumed!in!the!UK,!the!expected!annual!incidence!would!be!21,120!cases!(based!
upon!UK!population!of!64!million).!Although!all!hospitals!in!the!UK!were!invited!
to! participate,! 143/174! (82.2%)! provided! data,! therefore! we! would! estimate!
17,360! cases! per! annum! from! these! hospitals,! or! 2893! in! two! months.! This!
method!may!over%estimate!the!number!of!cases!in!the!UK!as!Lanas!et#al!captured!
patients!using!14!different!ICD%9!codes,!which!included!patients!with!conditions!
other!than!LGIB,!such!as!intestinal!perforation.2!This!is!likely!to!have!lead!to!an!
over%estimation!of!the!incidence!of!lower!GI!bleeding!in!their!study.!Additionally!
the!estimated!UK!population!of!64!million! includes!children.!Accordingly,! these!
figures! support! the! representativeness! of! the! sample! captured! in! this!
observational!study.!
!Most! cases! were! admitted! under! general! surgery! (2105/2528,! 83.3%),!
310/2528! (12.3%)! under! general! medicine! and! only! 54/2528! (2.1%)! under!
gastroenterology.! Gastroenterology! admissions! were! younger! (median! age! 59!
years,!IQR!43%80)!than!those!admitted!to!general!medicine!(74!years,!IQR!50%84,!
p<0.05)!or!general!surgery!(73!years,!IQR!58%83,!p<0.01).!
!
!
!
!!!!!!!!

! 84!
4.3!Patient!Characteristics!!!!The! median! age! of! patients! was! 74! years! (57%83);! 1319/2528! (52.2%)! were!
female! and! 1455! (57.6%)! had! a! Charlson! Co%morbidity! Index! ≥1.! Malignancy,!
diabetes!and!myocardial!infarction!(MI)!were!the!most!common!co%morbidities,!
reported!in!392!(15.5%),!377!(14.9%)!and!285!(11.3%)!cases,!respectively.!!
!
Patients!who!developed!LGIB!whilst! hospitalised! for! another! reason! (inpatient!
bleeds)! represented!185/2528! (7.3%)!of!LGIB!cases.!They!were!older! (median!
age! 73! vs! 78! years,! p<0.001)! with!more! co%morbid! illness,! including! diabetes!
(21.6%! vs! 14.4%),! stroke! (16.2%! vs! 8.0%)! and! MI! (16.2%! vs! 10.9%)! in!
comparison!to!new!admissions.!!
!
Bright! red! blood! per# rectum! was! the! most! common! presenting! symptom,!
reported! in! 1836/2528! (72.6%)! cases! and!more! common! in! acute! admissions!
than!inpatient!bleeds.!Inpatients!were!more!likely!to!present!with!melaena,!clots!
per#rectum#and!shock.!Presentation!with!haemodynamic!shock!was!uncommon,!
reported! in! just! 58/2528! (2.3%)! cases.! Anaemia!was! also! uncommon! (median!
Hb! 122g/l,! full! range! 36%192);! a! minority! presented! with! Hb! ≤80g/l! (272,!
10.8%).!A!total!of!408!(16.1%)!patients!had!previously!been!admitted!with!LGIB,!
with!95/408!(23.3%)!in!the!preceding!28!days!!(Table!7).!
!!!!!!!!

! 85!
Table! 7:! Presenting! features! and! demographics! of! patients! admitted! with! or! who!developed!LGIB!whilst!an!established!inpatient!!! Acute!admissions!
N!=!2331!N!(%)!
Inpatients!N!=!185!N!(%)!
All!patients!§!Total!N!=!2528!N!(%)!
Median!Age!(IQR)! 73!(56%83)! 78!(66%85)! 74!(57%83)!Gender!Female!(Missing)!
!1204!(51.7)!6!
!112!(60.5)!0!
!1319!(52.2)!7!
Charlson!CoZmorbidity!index!0!1!≥2!(Missing)!!Cardiac!failure!Myocardial!Infarction!Diabetes!Stroke!Chronic!respiratory!disease!Colorectal!cancer!Non%colorectal!cancer!Liver!disease!Dementia!
!!1016!(43.6)!530!(22.7)!778!(33.4)!7!!136!(5.8)!255!(10.9)!335!(14.4)!186!(8.0)!268!(11.5)!108!(4.6)!234!(10.0)!50!(2.1)!136!(5.8)!!
!!42!(22.7)!39!(21.1)!104!(56.2)!0!!22!(11.9)!30!(16.2)!40!(21.6)!30!(16.2)!30!(16.2)!20!(10.8)!29!(15.7)!5!(2.7)!14!(7.6)!!
!!1066!(42.2)!570!(22.5)!885!(35.0)!7!!159!(6.3)!285!(11.3)!377!(14.9)!217!(8.6)!298!(11.8)!128!(5.1)!264!(10.4)!55!(2.2)!150!(5.9)!!
Presenting!features!Bright!red!blood!per#rectum#Clots!per#rectum#Melaena!Abdominal!pain!(Missing)!
!1723!(73.9)!313!(13.4)!99!(4.2)!474!(20.3)!5!
!110!(59.5)!29!(15.7)!20!(10.8)!17!(9.2)!0!
!1836!(72.6)!344!(13.6)!120!(4.7)!492!(19.5)!6!
Haemodynamic!Status*!Normal!Isolated!tachycardia!Shock!(Missing)!
!1851!(79.4)!368!(15.8)!48!(2.1)!64!
!144!(77.8)!19!(10.3)!9!(4.9)!13!
!2004!(79.3)!388!(15.3)!58!(2.3)!78!
Admitting!Hb!!Median!(IQR)!!Hb!≤!70!Hb!71%80!Hb!81%90!Hb!91%100!Hb!101%110!Hb!111%120!Hb!≥!121!(Missing!data)!
!!124!(101%139)!!127!(5.4)!118!(5.1)!137!(5.9)!181!(7.8)!210!(9.0)!291!(12.5)!1253!(53.8)!14!
!!107!(88%124)!!13!(7.0)!14!(7.6)!29!(15.7)!20!(10.8)!28!(15.1)!23!(12.4)!57!(30.8)!1!
!!122!(100!%138)!!140!(5.5)!132!(5.2)!166!(6.6)!201!(8.0)!240!(9.5)!314!(12.4)!1320!(52.2)!15!
Previous! admission! with!LGIB!(Missing)!
396!(17.0)!!443!
11!(5.9)!!50!
408!(16.1)!!495!
Medications!Aspirin!Clopidogrel!Dual#antiFplatelet#Warfarin!
!532!(22.8)!203!(8.7)!65!(2.8)!249!(10.7)!
!51!(27.6)!32!(17.3)!10!(5.4)!21!(11.4)!
!584!(23.1)!235!(9.3)!75!(3.0)!270!(10.7)!
! 86!
DOACs!(total)!Apixaban#Dabigatran#Rivaroxiban#(Missing)!NSAIDs!(Missing)!
122!(5.2)!35#(1.5)#15#(0.6)#72#(3.1)#1!130!(5.6)!0!
7!(3.8)!3#(1.6)#1#(0.5)#3#(1.6)#11!15!(8.1)!0!
131!(5.2)!38#(1.5)#16#(0.6)#77#(3.0)#12!146!(5.8)!0!
§! Includes! 10! patients! classified! as! ‘other’! presentation! and! 2! with! missing! data! on! mode! of!presentation.!*On!admission!or!first!set!of!observations!after!developing!LGIB.!Shock!defined!as!HR≥100! and! SBP<100mmHg.! 24! (0.9%)! patients! appeared! twice! in! the! dataset! as! they! were!admitted!with!further!LGIB!during!the!audit!period.!!!!Medications#
At! the! time! of! presentation! with! bleeding,! 742/2528! (29.4%)! patients! were!
taking! antiplatelet! agents;! 584! (23.1%)! of! all! patients! were! taking! aspirin.!
Warfarin! use!was! reported! in! 270! (10.7%)! patients! and!DOACs! in! 131! (5.2%)!
patients!(Table!7).!Aspirin!was!withheld!in!417/584!(71.4%,!missing!data!in!21!
cases),! and! clopidogrel! in! 167/235! (71.1%,!missing! data! in! 13)! patients.!Most!
patients!had! their!DOAC!stopped! (116/131,!88.5%),! five!patients!also! received!
prothrombin!complex!concentrate!and!3!fresh!frozen!plasma!(FFP).!!
!
Most! patients! had! normal! coagulation! profiles! on! presentation! (median!
international! normalised! ratio,! INR! 1.1,! IQR! 1.0%1.2).! There! were! 267/2528!
(10.6%)!cases!presenting!with!an!INR!>1.5,!and!58!(2.3%)!with!an!INR!≥5!(INR!
missing! in!404).!Of! those!presenting!with! an! INR!>1.5,! 195/267! (73.0%)!were!
taking!warfarin,!26!were!taking!a!DOAC,!3!had!liver!disease!with!cirrhosis!and!1!
had!a!congenital!bleeding!disorder.!!
!!!!!!!!

! 87!
4.4.Use!of!Blood!Components!!Red! blood! cell! transfusion!was! administered! in! 666/2528! (26.3%)! cases!with!
258!(10.2%)!receiving!≥4!units!during!admission!(Table!8).!!
Table!8:!Inpatient!Interventions!for!LGIB!!! All!patients,!N!=!2528!
N!(%)!Transfusion!Red!cell!transfusion!(all)!Received�≥4#units#Median!units!(range)!(Missing!data)!FFP!Platelets!(Missing!data)!
!666!(26.3)!258!(10.2)!3!(1%17)!35!56!(2.2)!44!(1.7)!30!
Endoscopy!Colonoscopy!Flexible!sigmoidoscopy!Rigid!sigmoidoscopy!or!proctoscopy!TOTAL!(Missing!data)!Endoscopic!Haemostasis!(Missing!data)!OGD!(Missing!data)!Other!endoscopy**!(Missing!data)!
!99!(3.9)!543!(21.5)!84!(3.3)!726!(28.7)!47!54!(2.1)!141!285!(11.3)!39!10!(0.4)!58!
Radiology!CT!Abdomen/pelvis!CT!Angiography!TOTAL!(Missing!data)!
!507!(20.1)!149!(5.9)!656!(25.9)!77!
Interventional!Radiology!Mesenteric!Angiography!Mesenteric!Embolisation!(Missing!data)!
!37!(1.5)!19!(0.8)!61!
Nuclear!medicine!Red!cell!scan!(Missing!data)!
!1!(0.04)!42!
No!inpatient!investigation*!(Missing!data)!
1213!(48.0)!55!
Surgery!Laparotomy!for!bleeding!Transanal!surgery!for!bleeding!(Missing!data)!
!6!(0.2)!26!(1.0)!53!
*Inpatient! investigation! includes! rigid! sigmoidoscopy,! proctoscopy,! flexible!sigmoidoscopy,! colonoscopy,! OGD,! CT! abdomen/pelvis,! CTA,! mesenteric! angiography!and!red!cell!scanning!**!Other!endoscopy:!capsule!endoscopy,!push!enteroscopy!
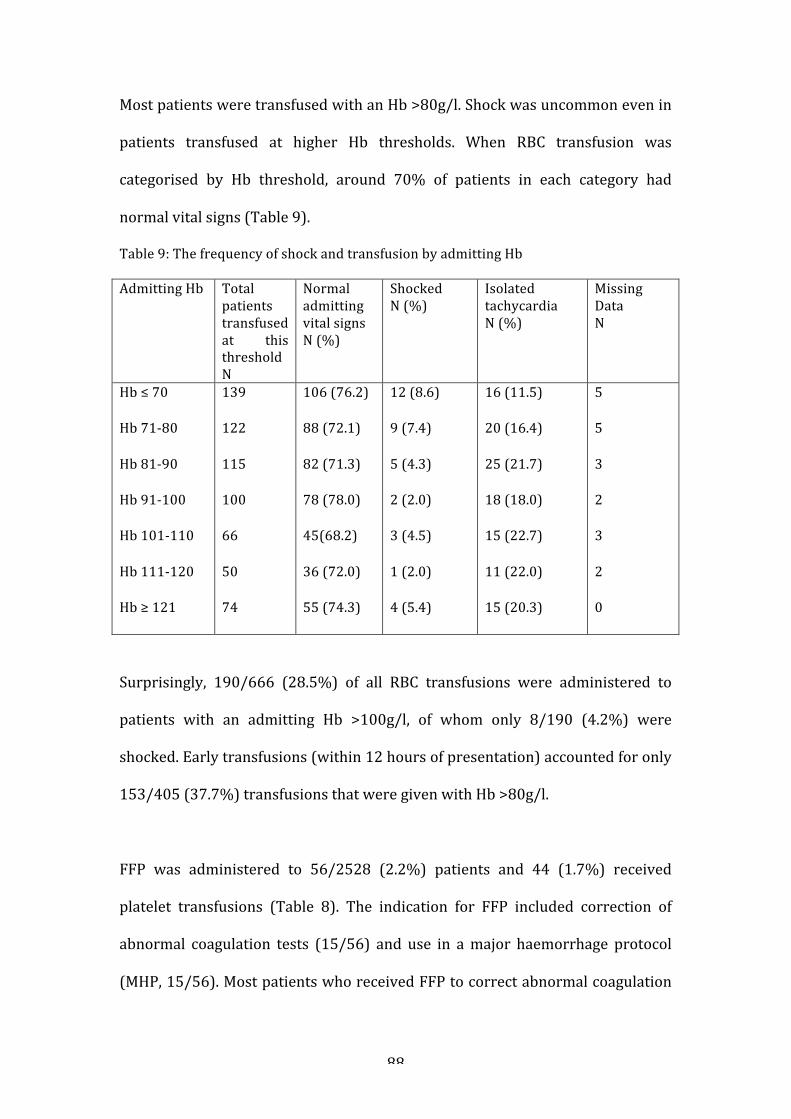
! 88!
Most!patients!were!transfused!with!an!Hb!>80g/l.!Shock!was!uncommon!even!in!
patients! transfused! at! higher! Hb! thresholds.! When! RBC! transfusion! was!
categorised! by! Hb! threshold,! around! 70%! of! patients! in! each! category! had!
normal!vital!signs!(Table!9).!
Table!9:!The!frequency!of!shock!and!transfusion!by!admitting!Hb!!Admitting!Hb! Total!
patients!transfused!at! this!threshold!N!!
Normal!admitting!vital!signs!N!(%)!
Shocked!N!(%)!
Isolated!tachycardia!N!(%)!
Missing!Data!N!!
Hb!≤!70!!Hb!71%80!!Hb!81%90!!Hb!91%100!!Hb!101%110!!Hb!111%120!!Hb!≥!121!!
139!!122!!115!!100!!66!!50!!74!
106!(76.2)!!88!(72.1)!!82!(71.3)!!78!(78.0)!!45(68.2)!!36!(72.0)!!55!(74.3)!
12!(8.6)!!9!(7.4)!!5!(4.3)!!2!(2.0)!!3!(4.5)!!1!(2.0)!!4!(5.4)!
16!(11.5)!!20!(16.4)!!25!(21.7)!!18!(18.0)!!15!(22.7)!!11!(22.0)!!15!(20.3)!
5!!5!!3!!2!!3!!2!!0!
!
Surprisingly,! 190/666! (28.5%)! of! all! RBC! transfusions! were! administered! to!
patients! with! an! admitting! Hb! >100g/l,! of! whom! only! 8/190! (4.2%)! were!
shocked.!Early!transfusions!(within!12!hours!of!presentation)!accounted!for!only!
153/405!(37.7%)!transfusions!that!were!given!with!Hb!>80g/l.!!
!
FFP! was! administered! to! 56/2528! (2.2%)! patients! and! 44! (1.7%)! received!
platelet! transfusions! (Table! 8).! The! indication! for! FFP! included! correction! of!
abnormal! coagulation! tests! (15/56)! and! use! in! a!major! haemorrhage! protocol!
(MHP,!15/56).!Most!patients!who!received!FFP!to!correct!abnormal!coagulation!

! 89!
tests!were! taking! anticoagulants;! 8! taking!warfarin! and!3! a!DOAC.! For!platelet!
transfusions,! 8/44! patients! were! thrombocytopenic! with! a! platelet! count!
<30x109/l,! 15! received! platelets! to! reverse! antiplatelet! drugs! and! 12! received!
platelets! as! part! of! a! major! haemorrhage! protocol.! A! major! haemorrhage!
protocol!was!administered! to!53/2528! (2.1%)!patients! in!whom!FFP,!platelets!
and! cryoprecipitate! were! given! in! 21! (39.6%),! 12! (22.6%)! and! 6! (11.3%)!
respectively.!!
!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!
! 90!
!4.5!Endoscopy!and!Endoscopic!Haemostasis!!!The!most! frequent! inpatient! investigation!was! flexible! sigmoidoscopy,! used! in!
543/2528! (21.5%)! cases.!OGD! (285,! 11.3%)! and! colonoscopy! (99,! 3.9%)!were!
used!less!frequently.!Capsule!endoscopy!and!push!enteroscopy!were!rarely!used!
(Table!8).!!
!
The!highest!diagnostic!yields!were!on!flexible!sigmoidoscopy!(418/543,!77.0%)!
and!colonoscopy! (71/99,!71.7%).! !Bedside!proctoscopy!or! rigid! sigmoidoscopy!
was!undertaken!in! just!73/2528!(2.9%)!patients.! In!the!group!of!2455!patients!
that! did! not! undergo! proctoscopy! or! rigid! sigmoidoscopy,! 526/2455! (21.4%)!
had! an! inpatient! flexible! sigmoidoscopy,! with! readily! identifiable! anorectal!
pathologies! (anal! cancer,! anal! fissures,! haemorrhoids! and! rectal! prolapse)!
identified!in!69/526!(13.1%)!of!these.!!In!the!patients!that!underwent!inpatient!
colonoscopy! the! most! common! diagnoses! were! diverticular! bleeds! (34/99,!
34.3%),! haemorrhoids! (13/99,! 13.1%),! colitis! (7/99,! 7.1%),! colorectal! cancers!
(5/99,! 5.1%)! and! angiodysplasia! (4/99,! 4.0%).! Evidence! of! bleeding! with! no!
identifiable!source!was!found!in!13/99!(13.1%)!of! inpatient!colonoscopies,!and!
7/99!(7.1%)!were!reported!as!normal!investigations.!!
!
The!median!time!to!procedure!was!3!days!(IQR!2%5)!for!flexible!sigmoidoscopy,!2!
days! (IQR! 1%4)! for! OGD! and! 4! days! (IQR! 2%7)! for! colonoscopy.! Overall! 14/99!
(14.1%,!missing!data! in!6)!patients!who!had!a! colonoscopy!had! the!procedure!
performed! within! 24! hours! of! admission.! The! majority! of! flexible!
sigmoidoscopies! and! colonoscopies! were! performed! in! the! endoscopy!

! 91!
department! (475/543,! 87.5%,! missing! data! in! 17,! and! 85/99,! 85.9%,! missing!
data!in!1,!respectively),!with!39/543!(7.2%)!flexible!sigmoidoscopies!and!10/99!
(10.1%)!colonoscopies!performed!in!emergency!theatre.!44!patients!underwent!
a! repeat! lower! GI! endoscopy:! 14! for! further! bleeding,! 10! due! to! poor! bowel!
preparation,! six! patients! had! a! full! colonoscopy! after! an! initial! non%diagnostic!
flexible! sigmoidoscopy! and! three! were! repeated! to! allow! therapeutic!
intervention!(missing!data!in!11).!!
!
Endoscopic! haemostasis!was! very! infrequently! used,! reported! in! just! 54/2528!
(2.1%)! of! the! total! cohort! and! 54/642! (8.4%)! of! the! cases! undergoing!
endoscopy:! 36/54! endoscopic! therapies! were! delivered! at! flexible!
sigmoidoscopy,!14!at!colonoscopy,!3!at!proctoscopy!and!one!unknown.!The!most!
frequent!methods!were!banding!(n=13),!argon!laser!(n=11)!and!clipping!(n=9).!
Two! modalities! were! used! in! 12/54! cases! and! three! in! 3/54.! Re%bleeding!
following!endotherapy!occurred!in!7/54!(13.0%)!patients,!of!whom!one!required!
embolisation,! one! underwent! angiography! that! did! not! demonstrate! contrast!
extravasation!and!two!required!further!endoscopic!haemostasis.!No!cases!of!re%
bleeding! required! surgical! intervention.! Two! perforations! were! reported! at!
endoscopy,! both! requiring! surgical! intervention.! Both! followed! flexible!
sigmoidoscopy,! one! showing! pseudomembranous! colitis! and! one! multiple!
colonic!ulcers.!Neither!had!attempted!endoscopic!haemostasis.!!
!!
Overall!77!patients!were!admitted!with!LGIB!following!an!endoscopic!procedure,!
49/77!(66.6%)!of!which!were!indicated!as!post%polypectomy!bleeds.!Of!these!49!

! 92!
post%polypectomy!bleeds,!only!six!underwent!inpatient!lower!GI!endoscopy,!four!
receiving! endotherapy.! An! additional! four! underwent! CTA! and! two! were!
successfully!embolised.!
!
!!4.6!Radiology!!CT! abdomen/pelvis!was! undertaken! in! 507/2528! (20.1%)! cases,! but! CTA!was!
used!in!only!149!(5.9%)!and!formal!angiography!in!just!37!(1.5%)!(Table!8).!CT!
abdomen/pelvis! and! CTA! lead! to! a! diagnosis! of! the! source! of! bleeding! in!
283/507! (55.8%)! and! 74/149! (49.7%)! scans! respectively.! The! most! frequent!
diagnoses! found! on! CT! abdomen/pelvis! were! colitis! (170/507,! 33.5%)! and!
diverticular! disease! (123/507,! 24.2%).! Colorectal!mass! lesions!were! identified!
on! 42/507! (8.9%)! scans,! whereas! no! source! of! bleeding! was! identified! on!
138/507!(27.2%).!The!median!time!to!procedure!was!2!(1%3)!days!and!1!(0%2)!
day!for!CT!abdomen/pelvis!and!CTA!respectively.!!
!
Of! the! 37! patients! that! underwent! mesenteric! angiography,! only! 19! (51.3%)!
went!on!to!have!embolisation.!Re%bleeding!following!embolisation!was!reported!
in! 7/19! patients,! of! whom! one! underwent! successful! re%embolisation! and! one!
required! surgical! control.! Two! patients! developed! mesenteric! ischaemia!
following! embolisation,! one! requiring! surgical! resection.! Both! survived! to!
hospital!discharge.!
!
!!!

! 93!
!4.7!Surgery!!Six! (0.2%)! patients! underwent! laparotomy! for! bleeding,! one! following!
embolisation.! Three! patients! had! pre%operative! CTA! identifying! an! actively!
bleeding!rectal!cancer!and!two!had!diverticular!bleeds.!Both!diverticular!bleeds!
were!demonstrated!by!extravasation!of!contrast,!but!these!patients!proceeded!to!
surgery! without! angiography.! Another! patient! had! a! CT! abdomen/pelvis! that!
identified!angiodysplasia.!Another!had!no!pre%operative! investigations.!Surgery!
was!conducted!between!8pm!and!8am! in!3/6!cases!and!all!were!performed!or!
supervised! by! a! consultant! surgeon.! Three! of! six! patients! who! underwent!
laparotomy!for!bleeding!died;!all!had!significant!co%morbidities!(Table!10).!!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!!

! 94!
!Table!10:!Patients!who!required!emergency!laparotomy!for!LGIB!!Patient!characteristics!(age)!
PreDoperative!investigation!
Charslon!Index!
ASA*! Time! to!laparotomy**!(hours)!
Source! of!bleeding!
Procedure! Outcome!
Male!(79)!!!Male!(51)!!!Female!(89)!!!Male!(72)!!!!Male!(69)!!!!Male!(68)!!!
CTA!–!no!blush!!!CT!Abdomen/pelvis!!CTA!–!blush!!!None!!!!MA!blush!–!embolisation!–!further!bleeding!!CTA!D!blush!
0!!!0!!!0!!!3!!!!2!!!!3!!!
2!!!2!!!4!!!3!!!!Not!known!!!4!
23!!!40!!!6!!!72!!!!28!!!!72!
Rectal!cancer!!!Angiodysplasia!!!Diverticular!bleed!!Suspected!diverticular!bleed!!NonDhodgkins!lymphoma!!!Diverticular!bleed!!
Anterior!resection!!!Right!hemicolectomy!!!Right!hemicolectomy!!!Subtotal!colectomy!!!!Subtotal!colectomy!!!!Laparotomy!!
LOS!28!days!!!LOS!21!days!!!LOS!24!days!!!PostDoperative!death!!!PostDoperative!death!!!IntraDoperative!death!
*!American!Society!of!Anaesthestiologists!physical!status!classification!**Time!between!presentation!and!start!of!surgery.!!!
! 95!
4.8$Clinically$significant$bleeding$$Only! 36/2528! (1.4%)! patients! met! the! pre<defined! criteria! for! clinically!
significant!bleeding.!The!most!common!investigations!were!CT!abdomen/pelvis!
(8/36),! CTA! (7/36)! and! flexible! sigmoidoscopy! (7/36).! Angiography! was!
undertaken! in! two,! one! receiving! embolisation.! None! underwent! endoscopic!
haemostasis!or!laparotomy!for!bleeding,!14!received!no!inpatient!investigation.!
$
$4.9$Patients$undergoing$no$inpatient$investigations$!Nearly!one!half!of!patients! (1213/2528,!48.0%)!had!no! investigations! for!LGIB!
during! their! admission.! Of! these,! 210/1213! (17.3%)! received! RBC! transfusion!
and! 126/1213! (10.4%)!were! re<admitted! by! 28! days;! 59/126! (46.8%)! due! to!
further!LGIB.!!Hospitals!reported!that!105/1213!(8.7%)!patients!did!not!warrant!
further!inpatient!investigation!as!they!had!been!investigated!previously.!A!total!
of!93/1213!(7.7%)!had!an!anorectal!source!that!was!identified!on!digital!rectal!
examination.!Outpatient! investigation!was!planned! in!518/1213!(42.7%)!cases,!
the!most! frequent!being! flexible!sigmoidoscopy!or!colonoscopy!(490!requests),!
CT!colonography!(25!requests)!and!CT!abdomen/pelvis!(16!requests).!
!
Hospitals!were!asked!why! the! remaining!497/1213! (41.0%)!patients!were!not!
scheduled! for! outpatient! investigation.! Frequent! reasons! were! ‘trivial,! self<
limiting!bleeding!with!no!change! in!haemodynamic!status’,!and! ‘unknown’.!Ten!
patients!refused!investigation,!and!62!(5.1%)!were!considered!to!be!for!palliative!
care!only.!!
!

! 96!
Compared!to!patients!that!underwent!inpatient!investigation,!patients!who!were!
not! investigated! were! less! likely! to! be! transfused! (445/1254,! 35.5%,! missing!
data! in! 61! vs! 210/1211,! 17.3%,!missing! data! in! 2,! respectively! p<0.0001)! and!
had! a! shorter! length! of! stay! (median! 5! days,! IQR! 3<9! vs! 2! days! IQR! 1<4,!
respectively! p<0.001)! although!no! difference!was! seen! in! in<hospital!mortality!
(mortality! in! the! investigated! group! 42/1248,! 3.4%,! missing! data! in! 67,! vs!
42/1210,! 3.4%,!missing! data! in! 3,! p=0.89)! or! re<admission! due! to! re<bleeding!
(investigated! group! 51/1261,! 4.0%,! missing! data! in! 54,! vs! 59/1212,! 4.9%,!
missing!data!in!1,!p=0.32).!!
!4.10$Outcomes$!!Diagnoses)
The! most! commonly! reported! sources! of! bleeding! were! diverticular! disease!
(668/2528,! 26.4%),! benign! anorectal! disorders! (422,! 16.7%)! and! colitis! (344,!
13.6%).!Haemorrhoids!were!reported!as!the!source!of!bleeding!in!305!(12.1%).!
Angiodysplasia! accounted! for! only! 1%! of! cases.! Bleeding! due! to! diverticulosis!
and! ischaemic! colitis! increased! with! age,! but! other! pathologies! were! largely!
constant!!(Table!11).!!!
!In!576/2528!(22.8%)!cases,!patients!were!discharged!with!no!formal!diagnosis.!
In! this! ‘unknown’! group,! 248/576! (43.1%)! had! investigations! that! were! non<
diagnostic!and!the!remainder!had!no!investigations!(328/576,!56.9%).!!
!!!

! 97!
Table!11:!Discharge!Diagnoses!by!age!!
! Age!<!60!N=699!N!(%)!
Age!60>79!N=938!N!(%)!
Age!≥!80!N=889!N!(%)!
All!patients !Total!N!=!2528*!N!(%)!
Diverticular+Disease+ 94+(13.4)+ 259+(27.6)+ 315+(35.4)+ 668+(26.4)+Colitis+Infective)Ischaemic))Inflammatory)bowel)disease)Undetermined)
163+(23.3)+20!(2.9)!12!(1.7)!43!(6.2)!88!(12.6)!
116+(12.4)+16!(1.7)!44!(4.7)!8!(0.9)!48!(5.1)!
65+(7.3)+5!(0.6)!29!(3.3)!11!(1.2)!20!(2.2)!
344+(13.6)+41!(1.6)!85!(3.4)!62!(2.5)!156!(6.2)!
Malignancy+Colon)Rectum)Anal)Othera)
18+(2.6)+5!(0.7)!10!(1.4)!2!(0.3)!1!(0.1)!
71+(7.6)+19!(2.0)!37!(3.9)!6!(0.6)!9!(1.0)!
65+(7.3)+37!(4.2)!24!(2.7)!1!(0.1)!3!(0.3)!
154+(6.1)+61!(2.4)!71!(2.8)!9!(0.4)!13!(0.5)!
Benign+anorectal+disordersb+Haemorrhoids)
171+(24.5)+126!(18.0)!
127+(13.5)+86!(9.2)!
124+(13.9)+93!(10.5)!
422+(16.7)+305!(12.1)!
Polyp(s)+ 11+(1.6)+ 28+(3.0)+ 24+(2.7)+ 64+(2.5)+Angiodysplasia+ 5+(0.7)+ 11+(1.2)+ 9+(1.0)+ 25+(1.0)+PostFendoscopyc+ 18+(2.6)+ 46+(4.9)+ 13+(1.5)+ 77+(3.0)+PostFoperatived+ 23+(3.3)+ 15+(1.6)+ 5+(0.6)+ 43+(1.7)+Small+bowel+sourcee+ 2+(0.3)+ 11+(1.2)+ 3+(0.3)+ 16+(0.6)+Drugs+(presumed+aetiology)f+ 9+(1.3)+ 21+(2.2)+ 13+(1.5)+ 43+(1.7)+Otherg+ 10+(1.4)+ 13+(1.4)+ 6+(0.7)+ 29+(1.1)+Unknown+ 160+(22.9)+ 194+(20.7)+ 222+(25.0)+ 576+(22.8)+(Missing!data)+ 9! 28! 30! 67!
*Includes!2!patients!where!age!unknown!aOther! malignancy:! acute! myeloid! leukaemia,! non>hodgkin’s! lymphoma,! post>transplant! lymphoproliferative! disorder,! bladder! or! gynaecological! origin,!neuroendocrine!tumour,!pancreatic,!prostate,!urothelial,!disseminated!intra>abdominal!malignancy!bBenign!anorectal:!anal!fissure,!solitary!rectal!ulcer,!fistulae,!rectal!prolapse,!proctitis,!perianal!haematoma,!rectal!varices,!anorectal!trauma!

! 98!
cPost>endoscopy:! diagnostic,! post>polypectomy,! transrectal! ultrasound! biopsy! of! the! prostate! and! other! biopsy,! haemorrhoid! banding,! endoscopic! mucosal!resection!dPost>operative:!colorectal!resection,!EUA!rectum,!haemorrhoidectomy,!prolapse!surgery,!haemorrhoidal!artery!ligation,!trans>anal!minimally!invasive!surgery!eSmall!bowel!source:!Meckel’s,!small!bowel!ischaemia,!intussusception,!obstruction,!small!bowel!tumour!fDrugs:!!warfarin,!DOAC,!aspirin,!clopidgrel,!laxatives,!low!molecular!weight!heparin,!mycophenolate!mofetil,!steroids!gOther:!chronic!anastomotic!ulcer,!arterioenteric!fistula,!arteriovenous!malformation,!caecal!varices,!chronic!anastomotic!dehiscence,!chronic!perineal!sinus,!colon!perforation,!decompensated!liver!disease,!endometriosis,!stoma!granulation!tissue,!HHT,!intussusception,!large!bowel!obstruction,!pouchitis,!volvulus!+!!

! 99!
Re#bleeding*
Continued* bleeding! was! reported! in! 279/2528! patients! (11.0%,! 135! cases!
missing!data)!during!the!first!24!hours!of!admission!(defined!as!the!requirement!
of! ≥2! units! red! cell! and/or! a! decrease! in! haematocrit! ≥20%13).! ! Re#bleeding!
(defined!by!additional!blood!transfusion!requirements!and/or!a!further!decrease!
in!haematocrit!≥20%!after!24!hours!of!clinical!stability13!occurred!in!343/2528!
patients!(13.6%,!missing!data!in!126).!283!(11.2%)!patients!had!one!episode!of!
reHbleeding,!43!(1.7%)!had!two!(each!preceded!by!24!hours!of!clinical!stability)!
and!17!had! three!or!more.!ReHbleeding!occurred!a!median!of!3!days! (IQR!2H5)!
after! presentation! with! the! index! bleed.! ReHbleeding! was! more! common! in!
inpatients! (26.5%! vs! 12.6%),! and! patients! taking! aspirin! (107/552,! 19.4%,!
p<0.0001,! 32! cases! missing! data),! versus! those! taking! no! antiplatelet! or!
anticoagulant!agents!(156/1365,!11.4%).!There!was!no!difference!in!reHbleeding!
in!patients!taking!warfarin!(38/254,!15.0%!p=0.11,!16!cases!missing!data).!The!
relationship!between!Charlson!CoHmorbidity! Index!and!reHbleeding! is!shown! in!
Figure! 5.! The! area! under! the! receiver! operator! characteristic! curve! was! nonH
discriminative!at!0.59.!
!
!
!
!
!
!
!

! 100!
Figure! 5:! The! relationship! between! Charlson! CoHmorbidity! Index! and! death! and! reH
bleeding!
!
!
!
The!highest!rate!of!reHbleeding!was!seen!in!angiodysplasia!(9/25),!but!significant!
numbers! of! patients! diagnosed! with! diverticular! bleeding! (98/668,! 14.7%,! 21!
cases! missing! data),! haemorrhoids! (30/305,! 9.8%,! 16! cases! missing! data)! or!
inflammatory,! infective! or! undetermined! colitis! (33/344,! 9.6%)! also! reHbled!
during!admission.!
!
In#hospital*mortality*
InHhospital!mortality!was!85/2528!(3.4%),!although!was!considerably!higher!for!
inpatients! compared! to! new! admissions! (33/185,! 17.9%! vs! 51/2296,! 2.2%,!
p<0.0001)!and!in!patients!who!reHbled!(24/338,!7.0%,!p<0.0001,!missing!data!in!

! 101!
5! cases).! In! four! (0.2%)! patients! the! cause! of! death! was! attributed! to!
uncontrollable!haemorrhage,!most!deaths!were!attributed!to!comorbidity!(Table!
12).!!
Table! 12:! Outcomes! and! cause! of! death! in! patients! admitted! with! or! who! developed!
LGIB!whilst!an!established!inpatient!
!
! Acute&admissions&N&=&2331&N&(%)&
Inpatients&&N&=&185&N&(%)&
All&patients&&Total&N&=&2528&N&(%)&
In&hospital&mortality&All!
Due!to!LGIB!
(Missing)!
!
Primary&cause&of&death*&GI!malignancy!
NonHGI!malignancy!
IntraHabdominal!Sepsis!
Pneumonia!
Myocardial!infarction!
and!heart!failure!
Stroke!
Frailty!
Other§!
Unknown**!
!
51!(2.2)!
3!(0.1)!
34!
!
!
!
7!
2!
10!
4!
4!
!
0!
0!
4!
17!
!
33!(17.8)!
1!(0.5)!
1!
!
!
!
3!
2!
7!
3!
3!
!
2!
1!
1!
10!
!
85!(3.4)!
4!(0.2)!
36!
!
!
!
10!
4!
17!
7!
7!
!
2!
1!
5!
28!
ReCbleeding &(Missing)!&
293!(12.6)!
113!
49!(26.5)!
12!
343!(13.6)!
126!
Median&length&of&stay&(IQR)&(Missing)!
3!(1H6)!
!
115!
9!(5H21)!
!
39!
3!(1H7)!
!
156!
ReCadmission&within&28&days&All!
Due!to!further!LGIB!
Unknown&
!
!
244!(10.5)!
107!(4.6)!
505!
!
!
16!(8.6)!
4!(2.2)!
26!
!
!
260!(10.3)!
111!(4.4)!
535!
All!patients!includes!12!cases!where!mode!of!presentation!was!unclassified!
*As!documented!on!the!primary!cause!of!death!on!the!death!certificate!
**Unknown:!death!certificate!not!available.!
§Other:! decompensated! liver!disease,! infective! endocarditis,! status! epilepticus,! chronic!
obstructive!pulmonary!disease,!dementia!
ReHbleeding! defined! as! additional! blood! transfusion! requirements! and/or! a! further!
decrease!in!Hct!≥20%!after!24!hours!of!clinical!stability13!
!
!
!

! 102!
The! four! patients! that! died! due! to! haemorrhage! also! had! significant! coH
morbidities;! two! had! metastatic! colorectal! cancers! that! were! the! source! of!
bleeding!and!two!had!severe!aortic!stenosis.!The!latter!two!did!not!have!a!source!
of!LGIB!localised.!
!
Figure! 5! shows! the! relationship! between! Charlson! CoHmorbidity! Index! and!
mortality.!The!area!under! the!receiver!operating!characteristic!curve!was!0.75,!
reflecting! reasonable! ability! of! Charlson! CoHmorbidity! Index! to! discriminate!
between!patients! that!survived! to!discharge!and!those! that!did!not.! In!contrast!
the!CHstatistic!for!Charlson!Index!and!reHadmission!was!0.57.!
!
Length*of*Stay*and*Hospital*Transfer*
The!median!LOS!was!3!days!(IQR!1H7)!and!was!longer!for!patients!that!developed!
LGIB!as!an!inpatient!(9!days,!IQR!5H21!vs!3!days,!IQR!1H6,!Table!12).!136/2528!
patients! (5.4%,! missing! data! in! 344)! were! discharged! to! a! nursing! home! or!
rehabilitation! facility,!which! added!on! average! an! extra!2!days! to! total! LOS.! In!
total,! 56/2528! (2.2%)! patients! required! transfer! to! another! hospital! for!
treatment.! Only! 6! cases! were! transferred! for! interventional! radiology!
procedures!(Table!13).!
!
!
!
!
!
!
!
!
!
!
!
!

! 103!
Table!13:!Transfer!Status!
!
! All&patients &Total&N&=&2528&N&(%)!
Requiring&transfer&to&another&hospital&(Missing)!
!
For!ITU!
For!endoscopy!
For!surgical!input!
For!radiology!input!(non!interventional)!
For!interventional!radiology!input!
Other!
!
56&(2.2)&(11)!
!
0!
7!(0.3)!
40!(1.6)!
0!
6!(0.2)!
3!(0.1)!
!
!
&
Re#admission*
ReHadmission! occurred! in! 260/2528! (10.3%)! patients! by! 28! days,! and! in! 111!
(4.4%)! cases! this!was! attributed! to! further! LGIB.! ReHadmission! due! to! further!
bleeding!was!highest!for!patients!diagnosed!with!haemorrhoidal!or!diverticular!
bleeding!(18/305,!5.9%,!missing!data! in!50,!and!38/668,!5.5%,!missing!data! in!
155,!respectively).!The!majority!of!patients!reHadmitted!with!further!LGIB!had!no!
inpatient!investigations!during!their!index!admission!(59/111,!53.2%).!
!
!
!
!
!
!
!
!
!
!

! 104!
4.11&Discussion&!
!
This! is! the! largest!and!most!comprehensive!study!of!LGIB!conducted!to!date! in!
the!UK!and!has!defined!its!causes,!interventions,!processes!of!care!and!outcomes.!
Patients!were!elderly!with!a! large!burden!of! coHmorbidity,! such! that!over!oneH
third! had! a! Charlson! coHmorbidity! index! ≥2.! At! the! time! of! presentation,! 28%!
were! taking! aspirin,! clopidogrel! or! a! nonHsteroidal! antiHinflammatory,! with! an!
additional! 16%! taking! either! warfarin! or! a! DOAC.! Overall! 16%! had! been!
admitted!with! LGIB! before,! 14%! reHbled! during! admission! and! 4.4%!were! reH
admitted! with! further! bleeding.! Over! half! of! the! latter! were! not! investigated!
during!their!index!admission.!!
!
Haemodynamic! instability!was!present! in!only!18%!of! cases,! the!majority!with!
just!an!isolated!tachycardia!and!normal!blood!pressure.!Thus!it!is!surprising!that!
RBCs! were! transfused! to! over! one! quarter! of! patients,! despite! only! 11%!
presenting! with! a! Hb! <80! g/L.! ! This! indicates! a! liberal! approach! to! RBC!
transfusion!in!realHlife!practice!which!is!contrary!to!guideline!recommendations!
for!transfusion.30!Randomised!data!from!UGIB!and!other!critically!ill!populations!
indicate! a! causal! relationship! between! transfusion! above! Hb! >70H80! and! reH
bleeding! and! death.32!34!113!114
! Thus!many! transfusions! in! this! study! would! be!
considered! inappropriate!and!require!critical!review!of! institutional!practice! in!
line!with!patient!blood!management!initiatives.115!
!
This! study! showed! that! case! fatality! rates! following! LGIB! are! low! and!
considerably!lower!than!those!reported!from!other!populationHbased!studies.!In!

! 105!
a! study! from! 10! Spanish! hospitals,! Lanas! et* al! reported! mortality! of! 8.8%,!
although! the! ICDH10! coding! for! LGIB! case! ascertainment! may! have! captured!
cases!of!UGIB.2!The!reported!inHhospital!mortality!in!the!present!study!is!limited!
by!the!duration!of!hospital!admission!(3!days)!so!may!not!be!directly!comparable!
to! studies! with! a! longer! follow! up.! Although,! another! database! study! of! LGIB!
reported! a! similar! inHhospital!mortality! of! 3.9%.12! The! present! study! confirms!
that! death! due! to! uncontrolled! bleeding! is! very! rare,! with! a! strong! observed!
association! between! increasing! comorbidity! and! mortality.! The! almost! 8Hfold!
increase!in!unadjusted!mortality!seen!in!inpatient!bleeds!is!also!likely!to!reflect!a!
greater! burden! of! comorbidity,! but! may! also! reflect! more! severe! bleeding,! as!
previously!noted!for!UGIB.33!116
!!
!
Decisions! regarding!withholding! antiplatelets! in! patients! presenting!with! LGIB!
are!difficult!since!continued!antiplatelet!use!is!associated!with!reHbleeding117!but!
withholding!them!may!lead!to!increased!cardiovascular!morbidity.103!Guidelines!
recommend!that!patients!receiving!aspirin!for!secondary!prevention!of!high!risk!
cardiovascular! disease! should! not! have! this! drug! stopped.47! This! study!
demonstrates! that! this!principle! is!not!being!adhered! to! in!many!patients!with!
LGIB! suggesting! uncertainty! as! to! optimal! management.! DOACs! can! also! be! a!
challenging,!as!most!have!no!specific!antidote!at!this!time.!This!is!a!key!area!for!
further!research!and!will!be!examined!in!Chapter!7.!
!
It!was! surprising! that! just! 29%! cases! underwent! lower! GI! endoscopy! (flexible!
sigmoidoscopy,! colonoscopy! and! anoscopy),! 8.4%! resulting! in! therapeutic!
intervention! to! arrest! bleeding,! given! guideline! recommendations.47! Studies!

! 106!
examining! the! role! of! colonoscopy! have! not! demonstrated! that! inpatient!
endoscopy! improves! clinical! outcomes,61! although! the! systematic! review!
(Chapter!2)! suggests! that! if!undertaken!as!an! inpatient,! colonoscopy!within!24!
hours! is! associated!with! a! higher! diagnostic! and! therapeutic! yield! and! shorter!
LOS.!Whether!hospitals!have!the!facilities!to!support!this!is!examined!in!Chapter!
5.!!
!
Hospitals! reported! that!outpatient! investigations!were!planned! for!only!half! of!
the!48%!that!were!not!investigated!for!LGIB!as!an!inpatient.!In!the!primary!care!
setting,! there! is! clear! guidance! from! NICE! that! patients! aged! 50! or! over! with!
unexplained!rectal!bleeding!should!be!referred!for!specialist!assessment!within!
two!weeks.118!The!proportion!of!patients!discharged!without!reported!plans!for!
endoscopic! evaluation! therefore! raises! concerns! regarding! the! potential! for!
missed!lesions.!In!addition,!considering!that!more!than!half!of!the!4.4%!that!were!
reHadmitted!due!to!further!bleeding!had!not!been!investigated!during!their!index!
admission,! this! may! suggest! that! early! discharge! without! investigation! was!
inappropriate.! Indeed,! the! proportion! of! patients! undergoing! flexible!
sigmoidoscopy! or! colonoscopy!was! lower! than! reports! of! 34.7H46.3%! in! other!
observational!studies!of!LGIB,5!12!and!raises!the!question!of!how!diagnoses!such!
as!diverticular!bleeding!or!angiodysplasia!were!confidently!made.!!
!
The!most!common!discharge!diagnosis!was!diverticular!bleeding,!and!across!all!
age! groups! benign! anorectal! conditions!were! the! second!most! common! cause.!
This! is! consistent! with! other! populationHbased! studies! from! Europe! and! the!
USA.8!12!Angiodysplasia!accounted!for!only!1%!LGIB,!which!is!less!frequent!than!
! 107!
previously! reported.53! The! proportion! of! LGIB! attributed! to! polyps! and! colon!
cancer! is! also! lower,8! 12
! but! this! may! be! due! to! the! use! of! hospital! codes! or!
endoscopy!referrals!to!identify!cases!in!previous!studies.!!
!
Mesenteric! embolisation! and! surgical! intervention!were! used! in! just! 0.8%!and!
0.2%! cases! respectively.! Embolisation! is! often! reserved! for! severe! bleeds! to!
avoid!surgery,!or!where!endoscopic!investigation!fails.47!It!is!recommended!that!
hospitals! have! 24/7! access! to! interventional! radiology! for! this! purpose,! either!
onHsite!or!through!a!network;6!although!just!6!cases!required!transfer!to!another!
institution! to! access! this! facility.! ! Whether! the! low! frequencies! of! both!
endoscopic! haemostasis! and! embolisation! are! due! to! lack! of! availability! are!
examined! in!Chapter!5.!Regardless,! the!case! fatality! rates!were! low,! suggesting!
that!most!patients!who!did!not!have!haemostatic! intervention!did!not! come! to!
harm.!!
!
The!sources!of!bleeding!requiring!emergency!laparotomy!were!varied,!although!
the!number!was!small.!Ideally,!laparotomy!should!be!last!resort!and!carried!out!
only!after!attempts!at! colonoscopic!or! interventional! radiological!management,!
although! only! one! patient! who! required! laparotomy! underwent! attempted!
embolisation.!Considering!laparotomy!was!performed!more!than!24!hours!after!
presentation!in!4/6!cases,!a!reHbleeding!plan!may!have!been!useful!to!allow!the!
organisation! and! planning! of! minimally! invasive! treatment! should! further!
bleeding!occur.!Consultant!staff!should!be!involved!with!the!decisionHmaking!and!
surgery!in!this!rare!and!highly!coHmorbid!group!of!patients,!as!evidenced!by!the!
50%!surgical!mortality!rate.!!

! 108!
ReHbleeding! is! frequently! encountered! after! UGIB,! is! well! defined119! and!
associated! with! poor! prognosis.33! Comparatively! less! is! known! about! its!
frequency! and! course! after! LGIB! and! there! are!no! accepted!definitions.! Simply!
quantifying! the! numbers! of! patients! that! experience! further! symptoms! of!
bleeding!may! lead! to! falsely!high! reporting,! capturing! trivial!bleeds!or!delayed!
transit!of!luminal!blood!after!the!initial!bleed!has!stopped.!The!definition!used!in!
this!study!was!that!described!by!Strate!et*al,*and!captures!reHbleeding!by!using!
associated!change!in!Hct!or!need!for!further!transfusion!after!a!period!of!clinical!
stability.13!Accordingly,! 13.6%!patients! reHbled!during! admission! and! a! further!
4.4%!were!reHadmitted!for!further!LGIB!by!28!days.!This!is!higher!than!previous!
reports!of!reHbleeding!of!8%!during!index!admissions.13!Sites!were!instructed!to!
check!each!patient’s!status!at!28!days!using!their!own!electronic!patient!records,!
although! it! is! possible! that! reHadmissions! to! other! institutions!may! have! been!
missed,!thus!this!is!a!conservative!estimate.!
!
Limitations! of! this! study! should! be! acknowledged.! Sites! were! instructed! to!
capture! consecutive! cases! in! order! to! represent! an! unselected! caseHmix! of!
presentations,! although! it! is! inevitable! that! some! cases!will! have! been!missed.!
However,!we!followed!the!same!methodology!of!case!ascertainment!used!in!the!
previous!BSG/NHSBT!study!of!UGIB33!and!that!was!shown!to!have!captured!over!
85%!of!cases!when!compared!with!national!hospital!episode!statistics!data!over!
the!same!time!period.120!Using!European!data!reporting!an!incidence!of!33/100!
000,2!we!estimate!an!annual!UK!incidence!of!21!120!cases.!Limiting!this!figure!to!
the! 82.2%! UK! hospitals! that! participated! would! equate! to! 17360! cases! per!
annum,!or!2893!in!2!months,!which!is!very!close!to!the!case!ascertainment!in!this!

! 109!
study.!To!explore!whether!data!were!skewed!by!a!few!large!centres,!the!largest!
5%!hospitals!(identified!by!the!number!of!acute!beds!in!2015!as!reported!by!NHS!
England)121!were!removed!and!mortality!recalculated.!The!overall!mortality!was!
unchanged!(3.41%).!A!further!limitation!is!that!the!lack!of!investigation!in!many!
patients! renders!many!of! the!diagnoses!presumptive,! although! the! frequencies!
are!consistent!with!other!studies.!8!12!
&
In! summary,! this! is! the! first! nationwide! study! of! LGIB! and! one! of! the! most!
detailed! of! its! kind.! Most! patients! had! minor! bleeding,! only! oneHquarter! of!
patients!underwent!inpatient!lower!GI!endoscopy,!which!infrequently!resulted!in!
the!use!of!endotherapy.!Radiological!or!surgical!intervention!was!rarely!required!
to! control! bleeding.! Further! research! into! risk! stratification! is! needed! to! allow!
avoidance!of!admission!or!facilitation!of!early!discharge!of!low!risk!patients,!this!
is! described! in! Chapter! 6.! The! optimal! management! of! patients! who! develop!
bleeding!whilst!receiving!anticoagulants,!DOACs!or!antiplatelets!is!a!critical!area!
for! further! exploration,! and! this! is! discussed! in! Chapter! 7.! Critical! review! of!
excessive!transfusion!practice!is!also!needed!as!is!research!informing!the!role!of!
colonoscopy!in!the!acute!setting.!!
&&&&&&&&&&&&&
! 110!
CHAPTER&5&!
THE& ORGANISATION& OF& SERVICES& FOR& THE& INVESTIGATION& AND&
MANAGEMENT&OF&LOWER&GASTROINTESTINAL&BLEEDING&!
!
Data!on!the!organisation!of!services!for!LGIB!was!provided!by!138!hospitals.!Of!
these,! two! (1.4%)! indicated! that! they! did! not! routinely! admit! LGIB! (a! tertiary!
centre! for! oncology! and! a! heart! and! lung! specialist! hospital).! These! hospitals!
were!therefore!excluded!from!any!analysis!of!results!that!apply!to!routine!LGIB!
admissions.!!
*5.1&Endoscopy&**24/7!access!to!endoscopy!was!investigated!both!in!hours!(defined!as!9amH5pm!
Monday! to! Friday)! and! out! of! hours! (defined! as! 5.01pmH8.59am! Monday! to!
Friday! and! throughout! the!weekend).! These!were! examined! separately! (Table!
13).!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!

! 111!
Table!13:!the!availability!of!in!and!out!of!hours!lower!GI!endoscopy!in!the!UK!
!
! UK!hospitals!
N=!136*!!
n!(%)!!
Does! your! hospital! provide! inHhours**!
colonoscopy! or! flexible! sigmoidoscopy! for!
lower!GI!bleeding?!
*****Yes******No******Unknown*
!
!
!
134!(98.5)!
2!(1.5)!
0!
Does! your! hospital! provide! outHofHhours**!
colonoscopy! or! flexible! sigmoidoscopy! for!
lower!GI!bleeding?!
*****Yes******No******Unknown!
!
!
!
99!(72.8)!
37!(27.2)!
0!
*Hospitals!that!do!not!routinely!admit!LGIB!were!excluded!
**! Defined! in! hours! (defined! as! 9amH5pm! Monday! to! Friday)! and! out! of! hours! (defined! as!
5.01pmH8.59am!Monday!to!Friday!and!throughout!the!weekend)!
!
!
Of! the! 136! sites! that! routinely! admit! LGIB,! 134/136! (98.5%)! stated! that! they!
provided! inHhours! colonoscopy! and! flexible! sigmoidoscopy.! This! reduced! to!
99/136! (72.8%)! in! the! out! of! hours! period.! In! total! only! 99/136! (72.8%)!
hospitals!are!able!to!provide!24/7!access!to!onHsite!lower!GI!endoscopy!for!LGIB.!!
!
Hospitals!that!did!not!provide!24/7!access!to!lower!GI!endoscopy!were!asked!to!
report!how!they!would!manage!patients!who!may!require!this!service,!only!one!
reported! that! they! had! an! agreed! referral! protocol! to! another! hospital,! 8/136!
(5.9%)!reported!ad!hoc!arrangements,!5/136!(3.7%)!reported!no!arrangements!
at!all!and!four!reported! ‘other!arrangements’!(missing!data! in!19/136!(14.0%).!
The!‘other!arrangements’!included!a!service!limited!to!mornings!at!the!weekend!
and!a!lower!GI!endoscopy!service!that!was!only!available!in!emergency!theatre,!
depending!on!the!speciality!of!the!onHcall!surgeon.!!
!

! 112!
Hospitals!that!provided!out!of!hours!lower!GI!endoscopy!for!LGIB!were!asked!to!
report!the!competency!of!their!endoscopists;!82/99!(82.8%)!reporting!that!all!of!
the! endoscopists! on! their! rota! were! proficient! at! haemostatic! therapy! during!
colonoscopy! or! flexible! sigmoidoscopy.! Additionally,! 77/136! (56.6%)!hospitals!
reported! that! they! had! defined! emergency! slots! that! could! be! used! to! provide!
urgent!lower!GI!endoscopy!for!LGIB!during!the!day.!!
*****5.2&Interventional&Radiology&*!
Overall,!73/136!(53.7%)!hospitals!reported!that!they!provided!onHsite! inHhours!
interventional! radiology! (IR)!but! this! reduced! to!50/136! (36.8%)! in! the!out!of!
hours!setting.!The!greatest!changes!between!inH!and!out!of!hours!IR!were!seen!in!
the!number!of!hospitals!reporting!‘ad!hoc!arrangements’!and!‘no!arrangements’!
(Table!14).!No!arrangements!were!reported!by!8/136!(5.9%)!hospitals!in!hours,!
but!this!increased!to!17/136!(12.5%)!in!the!out!of!hours!setting.! ‘Other’!and!‘ad!
hoc’!arrangements!included!the!transfer!of!patients!to!other!hospitals!without!a!
formalised!pathway!and!the!reliance!on!a!small!number!of!radiologists!(1H2)!who!
were!not!always!available.!!
!
!
!
!
!
!
!

! 113!
Table!14:!The!availability!of!in!and!out!of!hours!interventional!radiology!in!the!UK!
!
! UK!hospitals!
N=!136*!!
n!(%)!
What!are!the!arrangements!for!inHhours*!
interventional!radiology!for!lower!GI!
bleeding?!
*****On#site*service******Agreed*referral*protocol*to*another********hospital******Ad*hoc*arrangements******No*arrangements*in*place******Other*****
!
!
!
73!(53.7)!
19!(14.0)!
!
34!(25.0)!
8!(5.9)!
2!(1.5)!
!
What!are!the!arrangements!for!outHofH
hours*!IR!for!lower!GI!bleeding?!******
*****On#site*service******Agreed*referral*protocol*to*another********hospital******Ad*hoc*arrangements******No*arrangements*in*place******Other*****
!
!
50!(36.8)!
22!(16.2)!
!
44!(32.4)!
17!(12.5)!
3!(2.2)!
!
*Defined!as! in!hours,!9amH5pm!Monday! to!Friday!and!out!of!hours,!5.01pmH8.59am!Monday! to!
Friday!and!throughout!the!weekend,!!
!
!
Of! the! 50! hospitals! that! provided! out! of! hours! onsite! IR,! 27/50! (54%)! also!
provided!cover!for!external!sites,!7/50!providing!it!for!three!or!more!sites.!
The!median!number!of!consultant!radiologists!on!rotas!in!these!hospitals!was!5!
(range!1H9,!50!hospitals).!Out!of!hours!support!staff!such!as!radiographers!and!
specialised!IR!nurses!were!available!in!29/50!(58%)!of!these!hospitals.!
&&&5.3&Specialist&elderly&care&*Only! 28/136! (20.6%)! hospitals! reported! that! elderly! patients! admitted! with!
LGIB!under!the!care!of!general!surgeons!were!routinely!reviewed!by!Care!of!the!
Elderly!doctors.!
! 114!
5.4&Guidelines&
All!hospitals!that!participated!in!the!study,!regardless!of!whether!they!routinely!
admit! patients! with! LGIB! were! included! in! this! analysis! (n=138).! Overall!
133/138! (96.4%)! hospitals! reported! providing! separate!written! guidelines! for!
blood!transfusion!in!patients!with!major!haemorrhage.!Written!guidelines!on!the!
management! of! GI! bleeding! were! provided! by! 100/138! (72.5%)! hospitals,!
although!only!43/138!(31.2%)!included!LGIB.!!
&
&
&
&
&
&
&
&
&
&
&
&
&
&
&
&
&
&

! 115!
5.5&Discussion&
!
In! the! UK! 24/7! lower! GI! endoscopy! and! interventional! radiology! are! only!
available!in!72.8%!and!36.8%!hospitals!that!routinely!admit!patients!with!LGIB,!
respectively.! Overall,! 82/136! (60.3%)! hospitals! had! out! of! hours! endoscopy!
rotas! that!were! exclusively! staffed! by! endoscopists! trained! in! the! provision! of!
endoscopic! haemostasis.! ! Most! hospitals! that! provided! out! of! hours! onsite! IR!!
also!covered!external!sites,!the!median!number!of!interventional!radiologists!on!
an!out!of!hours!rota!was!5,!and!only!58%!had!oncall!support!staff!available.!The!
majority! of! hospitals! provided!written! guidance! on!blood! transfusion! in!major!
haemorrhage,! but! only! 31.2%! had! a! guideline! on! LGIB.! Only! 20.6%! hospitals!
provided! routine! specialist! elderly! care! for! older! patients! admitted! under!
surgical!teams.!
!
In!their!2015!report,!the!NCEPOD!recommended!that!‘patients!with!any!acute!GI!
bleed!should!only!be!admitted!to!hospitals!with!24/7!access!to!onsite!endoscopy,!
IR! (onsite! or! covered! by! a! formal! network).’6! This! study! demonstrated!
deficiencies! in! the! provision! of! endoscopy! and! IR! in! hospitals! that! routinely!
admit!LGIB!in!the!UK.!To!rectify!this!would!require!considerable!investment.!In!
UGIB,! economic! modelling! suggests! that! in! high! volume! centres,! the! cost! of!
providing!out!of!hours!endoscopy!would!be!offset!by!savings!achieved!through!a!
reduction!in!LOS.122!In!LGIB,!this!may!be!supported!by!the!association!between!
colonoscopy!within! 24! hours! and! reduced! LOS! as! demonstrated! in! Chapter! 2.!
However,! in! the! observational! patient! study,! inpatient! flexible! sigmoidoscopy!
and!colonoscopy!were!undertaken!in!only!21.5%!and!3.9%!cases,!with!a!median!
! 116!
waiting!time!of!3!and!4!days,!respectively.!Despite!the!low!numbers!of!patients!
receiving!endoscopy!and! the! long!waiting! time! in! those! that!did,!most!patients!
did! not! come! to! harm.! This! raises! questions! whether! a! blanket! investment! in!
endoscopy!provision!for!all!comers!with!LGIB!is!economically!justified.!!
!
Centralisation!of!specialist!services!has!meant!that!many!hospitals!have!lost!their!
onsite!IR!services.!The!most!frequently!absent!mode!of!treatment!for!LGIB!was!
IR,! and! embolisation! was! the! least! common! minimally! invasive! mode! of!
haemostasis!in!the!observational!study.!!The!lack!of!IR!provision!was!particularly!
notable!out!of!hours,!with!only!36.8%!hospitals!providing!on!an!onsite!service.!It!
might!be!expected!that!the!difference!is!accounted!for!by!an!increase!in!the!use!
of! formal!referral!protocols!out!of!hours,!but!this!was!not!the!case.!The!biggest!
increases!were!seen!in! ‘ad!hoc’!and! ‘no!arrangements.’!Additionally,! the!patient!
study! demonstrated! that! only! 0.2%! patients! admitted! with! LGIB! required!
transfer!for!IR!treatment.!!
!
Embolisation! is! not! suitable! for! all! causes! of! LGIB.! Multifocal! or! postHsurgical!
anastomosis! bleeds! may! not! be! amenable! due! to! the! risk! of! ischaemic!
complications.43! Previously,! anorectal! bleeds! were! also! thought! to! be! at!
particular! risk! of! ischaemia,! but! recent! evidence! on! the! safety! and! efficacy! of!
embolisation! in! the! treatment! of! bleeding! haemorrhoids123! has! started! to!
challenge!this.!In!the!observational!patient!study!12.1%!of!all!LGIB!was!reported!
to! be! due! to! hemorrhoids! so! this! may! greatly! extend! the! role! of! IR! in! LGIB,!
although! whether! embolisation! is! superior! to! endoscopic! management! of!
haemorrhoids!remains!unclear.!!

! 117!
Like! endoscopy,! improving! access! to! IR! services!will! also! require! considerable!
investment,! both! in! equipment! and! trained! personnel.! European! guidelines!
recommend! a! minimum! of! 6! consultant! radiologists! on! an! out! of! hours! rota!
covering!<1,000,000!population,124!which!we!have!demonstrated! is!not!current!
practice! in!most! IR!units! in! the!UK.!There! are!no!health! economic!data! on! the!
extension!of!IR!services,!but!as!embolisation!was!only!used!in!a!minority!of!LGIB!
patients,!like!endoscopy,!it!may!not!be!justified.!!
!
In! Chapter! 4.2! we! demonstrated! that! LGIB! patients! tend! to! be! elderly! with!
extensive! coHmorbidities! and! that! the! majority! are! admitted! under! general!
surgeons.! The! organisational! data! show! that! only! 20.6%! hospitals! provide!
routine! specialist! elderly! care! for! these! patients.! In! orthopaedic! surgery! the!
involvement!of!specialist!elderly!care!physicians! is!routine!and!associated!with!
reduced!complications,!mortality!and!LOS.125!A!similar!effect!has!been!reported!
in! elderly! patients! undergoing! urological! or! gastrointestinal! surgery,126! and!
elective! nonHcardiac! surgery.127! Although! the! benefit! of! routine! care! of! the!
elderly! review!has!not!been! studied! in!LGIB,! the!number!of! elderly!patients! in!
this!population!may!justify!an!intervention!targeted!at!this!group.! !Additionally!
as! most! hospitals! already! have! inHhouse! care! of! the! elderly! services,! the!
implementation!of!a!routine!assessment!protocol!may!be!less!costly!to!introduce!
than!the!other!organisational!interventions!for!LGIB.!!
!
!
Despite! the! almost! standard! provision! of!major! haemorrhage! protocols! across!
the! UK,! many! patients! with! LGIB! receive! potentially! unnecessary! RBC!

! 118!
transfusions.128!The!observational! study!demonstrated! that! shock!and!anaemia!
were! very! uncommon,! so!most! patients! will! not! trigger! a!major! haemorrhage!
protocol! and! therefore! will! not! be! covered! by! these! with! these! guidelines.!
Although! there! is! national! guidance! on! RBC! transfusion,30! the! deviation! from!
restrictive!transfusion!practice!may!be!due!to!the!lack!of!guidance!that!is!specific!
to! LGIB.! As! well! the! economic! considerations,! overHtransfusion! may! be!
associated! with! harm,! as! demonstrated! in! UGIB.32! The! lack! of! specific! LGIB!
guidance!that!includes!transfusion!should!be!addressed!as!a!priority.!!
!
!
Limitations! of! this! study! should! be! acknowledged.! The! study! lead! in! each! site!
was!asked!to!complete!the!organisational!questionnaire,!and!these!were!mostly!
surgeons.!Although!they!were!asked!to!visit!different!departments!it!is!likely!that!
some!of!the!responses!regarding!alternative!care!areas,!such!as!IR!may!not!be!as!
accurate!as!if!they!were!completed!by!a!specialist!in!that!area!e.g.!a!radiologist.!
Despite! this,! the! findings!on! the! in!and!out!of!hours!provision!of!services!were!
very!similar!to!those!found!by!the!NCEPOD!in!2013.6!Drawing!conclusions!on!the!
tailoring!of!resources!for!LGIB!is!difficult,!as!even!though!a!hospital!may!have!the!
provision!for!a!certain!intervention,!it!may!not!used.!This!is!particularly!relevant!
to! interventions! that! are! dependent! on! operator! skill,! such! as! endoscopic!
haemostasis.!An!endoscopist!will!need!to!perform!a!minimum!number!of! these!
procedures! to! maintain! their! skills,! but! only! 54! patients! received! endoscopic!
haemostasis!across!the!whole!study.!The!reported!82.8%!of!endoscopists!being!
proficient! at! haemostasis! in! LGIB! may! not! be! an! accurate! reflection! of!
endoscopists’! skills! and! their! confidence! at! undertaking! this! complex!
intervention.!!

! 119!
!
In! conclusion,!many!hospitals! do! not! have! comprehensive! lower!GI! endoscopy!
services! and! the!majority!do!not!have! comprehensive! IR! support.!Despite! this,!
most! patients! do! not! come! to! harm.! Further! research! into! identifying! which!
interventions!may! have! the! greatest! benefit,! such! as! the! institution! of! routine!
care! of! the! elderly! specialist! input! is! required.! Another! key! area! for! further!
research! is! appropriate! triage,! specifically! identifying! low! risk! patients,!where!
admission! and! inHhospital! intervention! can! be! avoided.! This! is! discussed! in!
Chapter!6.!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!

! 120!
!
CHAPTER&6:& SAFE&DISCHARGE&AFTER&ACUTE&LOWER&GASTROINTESTINAL&BLEEDING:&DERIVATION&AND&VALIDATION&OF&A&NOVEL&RISK&SCORE!&&
6.1&Introduction!
The! prediction! of! adverse! outcomes! such! as! severe! bleeding,! need! for!
intervention!or!death!is!a!research!priority!of!the!clinicians!who!care!for!patients!
with! LGIB.! In! Chapter! 4! we! identified! that! the! majority! of! patients! neither!
required!endoscopic,!radiological!or!surgical! intervention,!nor!suffered!adverse!
events!such!as!reHbleeding!or!death.!Of!the!patients!that!were!hospitalised!with!
LGIB,!48%!received!no!inpatient!investigation.!!
!
There! are! several! extensively! validated! risk! stratification! scores! for! UGIB,66!67
!
but! there! is! no! equivalent! for! LGIB.! Risk! scores! or! severity! indicators! have!
previously!been!proposed,13!69!129
!but!have!been!found!to!be!not!predictive11!130
!
or! remain!unvalidated! in!wider!populations.!Most!scoring! tools!seek! to!predict!
adverse! outcomes,! but! the! results! of! the! observational! study! described! in!
Chapter!4!found!that!severe!bleeding!and!inHhospital!death!are!uncommon,12!131
!
and! thus! many! patients! could! be! safely! discharged! at! presentation! and!
investigated!as!an!outpatient.!The!aim!of!this!risk!score!is!to!identify!this!latter!
group! of! patients,! therefore! avoiding! unnecessary! admission! and! diverting!
hospital!resources!to!patients!that!would!derive!greater!benefit.!!
!
Data!were!used!from!the!observational!study!to!develop!a!clinical!risk!score!to!
identify! patients! that! could! be! safely! discharged! from! the! emergency!

! 121!
department.!The!risk!score!was!externally!validated!and!compared!to!previously!
published!risk!scoring!systems!for!LGIB!as!well!as!scores!specific!to!UGIB.!
!
6.2&Methods&
&
6.2.1.&Study&design&and&participants&
!
Data! used! to! derive! the! prediction! model! were! identified! from! the! national!
observational! study! of! acute! LGIB! as! described! in! Chapter! 4.131! As! this! is! a!
secondary! analysis! of! routine! anonymous! data! collected! for! an! audit,! ethical!
approval!was!not!required,132!as!confirmed!by!the!Joint!Research!Office!at!Oxford!
University!Hospitals!NHS!Foundation!Trust.!!
!
Since! the! aim! of! the! score! was! to! aid! decisions! about! admission! to! hospital,!
patients! who! developed! LGIB! whilst! already! hospitalised,! or! who! were!
transferred! between! hospitals! or! other! treatment! facilities! were! excluded,!
leaving! data! from! 2336! acute! admissions! to! develop! the! model.! External!
validation!was!performed!using!a!cohort!of!288!patients!admitted!with!LGIB!to!
two! hospitals! within! Imperial! College! NHS! Healthcare! NHS! Trust! in! an!
observational! study! that! was! unrelated! to! the! national! study! described! in!
Chapter! 4.133! These! hospitals! did! not! participate! in! the! national! observational!
study.!This!cohort!was!chosen!as,!to!our!knowledge,!it!was!the!largest!available!
database!reporting!all!elements!of!the!composite!outcome!and!those!of!all!of!the!
other! six! scores! that!were!assessed! for! comparative!performance.!This!dataset!
was! retrospectively! populated! using! electronic! health! data! from! consecutive!

! 122!
presentations! to! the! emergency! department! in! each! hospital! with! a! primary!
diagnosis! of! LGIB! over! 5! years,! between! 2007! and! 2011.! Inpatient! bleeds! and!
cases! transferred! from! other! hospitals! were! excluded.! Cases! of! UGIB! were!
excluded!using!presenting!features,!OGD!and!angiography!findings.133!!
!
6.2.2.Outcomes&
Our!primary!objective!was!to!develop!and!validate!a!riskHscoring!tool!to!identify!
patients! that! could! be! safely! discharged! after! presentation! with! LGIB.! Safe*
discharge!was!defined!as! the!absence!of!all!of! the! following!after!presentation:!
reHbleeding,! defined! as! additional! blood! transfusion! requirements! and/or! a!
further! decrease! in! Hct! ≥20%! after! 24! hours! clinical! stability13;! any! RBC!
transfusion! during! the! episode! of! LGIB;! therapeutic! intervention! to! control!
bleeding,!defined!as!endoscopic,!radiological,!or!surgical!haemostasis;!inHhospital!
death,!all!cause;!reHadmission!with!further!LGIB!within!28!days.!
!
6.2.3&Statistical&Analysis&
Model*development*
Prior! to!any!statistical!modelling,!we!selected!18!candidate!predictor!variables!
that! were! considered! to! be! biologically! and! clinically! plausibly! related! to! the!
outcome! of! safe! discharge:! age,! gender,! previous! admission! with! LGIB,!
cardiovascular!disease,!active!malignancy,! liver!disease,!renal!disease,!blood!on!
DRE,! heart! rate! (HR),! systolic! blood! pressure! (SBP),! regular! use! of! oral!
antiplatelet! or! NSAIDS,! use! of! oral! anticoagulants,! Hb,! (g/L),! platelet! count!
(109/L),! white! cell! count! (10
9/L),! INR,! serum! urea! (mmol/L),! and! creatinine!
(μmol/L)!at!initial!assessment.!!The!list!of!candidate!variables!was!also!limited!to!
! 123!
those! routinely! collected! during! hospital! admission.! Variables! with! large!
amounts!of!missing!data!were!omitted,!as!it!was!likely!they!would!be!missing!in!
clinical! practice.! Data! on! coHmorbidities! were! defined! using! the! Charlson! coH
morbidity! index,108! which! we! previously! amended! to! allow! application! to!
medical!notes!(Appendix!1).134!
!
To! develop! a! risk! score,! the! suggested! sample! size! requirements! to! avoid!
overfitting! are! between! 5H10! events! per! candidate! variable.135! Based! on! 10!
eventsHperHvariable,! a! dataset! comprising! 180! events! is! required.! In! the!
development!cohort,!1599/2336!patients!were!safely!discharged,!737!not!safely!
discharged,!both!substantially!larger!than!the!minimum!180!events!required.!To!
validate! a! risk! score,! a! minimum! of! 100! events! are! required! for! calibration!
purposes,! and! much! lower! sample! sizes! are! required! for! calculating!
discrimination! (i.e.! the! cHstatistic).136! The! validation! cohort! included! >! 100!
events,!and! therefore!meeting!recommended!sample!sizes! for!model!validation!
for!the!outcome!of!safe!discharge.!
!
The! following! multivariate! logistic! regression! modelling,! multiple! imputation!
and! bootstrapping! was! performed! by! Professor! Gary! Collins.! Fractional!
polynomials137!were!used! to!explore! the!presence!of!nonlinear!relationships!of!
continuous! predictors! (age,!HR,! SBP,!Hb,! platelet! count,!white! cell! count,! urea,!
creatinine,! INR),! however! a! linear! relationship! was! found! to! be! a! good!
approximation.!We! assumed!missing! data! occurred! at! random! and! performed!
multiple! imputation! using! chained! equations! using! the! aregImpute! function! in!
the!R!statistical!software!package!for!imputing!missing!data!in!the!development!

! 124!
cohort!(R!Foundation!for!Statistical!Computing,!Vienna,!Austria).!!The!validation!
cohort!had!complete!data!on!all!necessary!predictors.!We!used!a!multivariable!
logistic!regression!model!with!backwards!elimination!to!select!predictors!using!
the!Akaike!Information!Criteria!(P=0·157).!Missing!values!were!predicted!on!the!
basis!of!all!other!predictors!as!well!as!the!outcome.!!Fifty!imputed!data!sets!were!
generated! with! imputed! values! reflecting! the! uncertainty! associated! with! the!
imputations.!!The!internal!validity!of!the!prediction!model!to!obtain!an!unbiased!
and! optimism! corrected! estimation! of!model! performance!was! assessed! using!
bootstrapping.! The! entire! modelling! process,! including! variable! selection,! was!
repeated!in!each!of!the!200!bootstrap!samples.!Performance!measures!evaluated!
include! the! discrimination! (cHstatistic),! with! 95%! confidence! intervals! (CI),!
where! a! value! of! 0·5! indicates! no! discrimination! and! a! value! of! 1! indicates!
perfect!discrimination.!!
!
To! increase! the! uptake! and! usability! of! the! model,! we! created! a! simplified!
scoring!system!following!the!approach!by!Sullivan!et*al.138!Values!are!assigned!to!
risk!factor!categories,!and!their!total!sum!assigned!predicted!probabilities!of!safe!
discharge.!
!
Model*Validation*
The! predicted! probabilities! were! calculated! for! each! patient! in! the! validation!
cohort! using! the! regression! coefficients! from! the! model! obtained! on! the!
development! cohort.!Discrimination!was! assessed!by! calculating! the! cHstatistic.!
Using! the! val.prob.ci.2! package! in! R,! a! calibration! plot,! with! 95%! confidence!
bands,!was!constructed!to!assess!the!agreement!between!the!observed!outcome!
! 125!
of! safe! discharge! with! the! predicted! probabilities! from! the!model.139! A!model!
with!perfect!calibration!should!lie!on!the!line!at!45Hdegrees!for!agreement!with!
the!outcome.!!
*
6.2.4&Comparative&assessment&with&previously&described&scores&
Previously!developed!scores!for!LGIB;!BLEED,129!NOBLADS,
69!and!Strate
13!were!
calculated!for!each!patient!(methodology!in!Appendix!3).!Although!Blatchford67,!
Rockall66! and! AIMSH65
140! scores! have! been! designed! for! UGIB! there! is! some!
evidence! that! they! have! predictive! value! in! LGIB.141! 142
! These! were! also!
calculated,!although!Rockall!was!limited!to!preHendoscopy!variables!as!several!of!
the! endoscopic! findings! are! specific! to! UGIB.! To! compare! the! discriminative!
ability!of!these!scores,!the!cHstatistic!for!each!was!calculated!for!safe!discharge.!CH
statistics! were! also! calculated! for! adverse! outcomes! (inHhospital! death,! reH
bleeding,! RBC! transfusion,! haemostatic! intervention,! and! reHadmission! with!
further!bleeding)!in!comparison!to!the!new!model.!The!DeLong!test!was!used!to!
compare!cHstatistics!for!each!model!and!each!outcome!against!the!new!model.143!
We! followed! the!TRIPOD!statement! for!reporting! this!clinical!prediction!model!
study.144
&
&
&
&
&
&
&

! 126!
6.3&Results&
6.3.1.&Demographics&and&presenting&features&
The!mean!age!was!68±19!years!in!the!derivation!cohort!and!66±19!years!in!the!
validation! cohort.! CoHmorbidity! was! common,! the! most! frequent! being!
cardiovascular! disease! in! both! cohorts.! Oral! antiplatelet! or! NSAID! use! was!
common,! found! in!over!40%!cases,! although!a!higher!proportion!of!patients! in!
the! derivation! dataset! were! receiving! oral! anticoagulants! (Table! 15).! In! the!
derivation!cohort!1599/2336!(68.5%)!patients!were!safely!discharged.!Patients!
that! required! admission! did! so! for! the! following! reasons:! 576/2336! (24.7%)!
received!RBC!transfusion,!323/2336!(13.8%)!reHbled,!58/2336!(2.5%)!required!
therapeutic! intervention! to! control! bleeding,! 52/2336! (2.2%)! died! and!
107/2284! (4.7%)! were! reHadmitted! with! further! LGIB.! In! both! cohorts,!
diverticular! disease! was! the! most! common! source! of! bleeding! (Table! 16).! As!
missing!data!accounted!for!38%!INR!values!this!predictor!was!excluded!from!any!
further!analysis.!!
!

! 127!
Table!15:!Demographic!data!for!candidate!variables!in!the!development!and!validation!cohort!
Variable( label( in(development(dataset((
Development(data((n=2336)( External(validation(data((n=288)(
Not(safely(discharged((n(=(737)( Safely(discharged((n(=(1599)( Not(safely(discharged((n(=(104)( Safely(discharged((n(=(184)(
Summary( Missing(data( Summary( Missing(data( Summary( Missing(data( Summary( Missing(data(
Mean( (SD)( [IQR];(n((%)(
n((%)(Mean( (SD)([IQR];(n((%)(
n((%)(Mean( (SD)([IQR];(n((%)(
n((%)(Mean( (SD)([IQR];(n((%)(
n((%)(
Age$ 72'46$(17'37)$ 0$ 66'48$(19'00)$ 0$ 69'50$(17'19)$ 0$ 64'49$(20'56)$ 0$Male$Gender$ 381$(51'7%)$ 0$ 748$(46'8%)$ 0$ 58$(55'8%)$ 0$ 93$(50'5%)$ 0$Previous$ LGIB$admission1$
187$(25'4%)$ 139$(18'9%)$ 208$(13'0%)$ 304$(19'0%)$ 42$(40'4%)$ 0$ 49$(26'6%)$ 0$
CVS$disease2$ 420$(57'0%)$ 0$ 733$(45'8%)$ 7$(0'4%)$ 62$(59'6%)$ 0$ 103$(56'0%)$ 0$Cancer3$ 138$(18'7%)$ 0$ 190$(11'9%)$ 7$(0'4%)$ 24$(23'1%)$ 0$ 37$(20'1%)$ 0$Liver$disease4$ 23$(3'1%)$ 0$ 27$(1'7%)$ 7$(0'4%)$ 2$(1'9%)$ 0$ 8$(4'3%)$ 0$Renal$disease5$ 87$(11'8%)$ 0$ 85$(5'3%)$ 7$(0'4%)$ 12$(11'5%)$ 0$ 11$(6'0%)$ 0$Blood$on$DRE$$ 451$(61'2%)$ 96$(13'0%)$ 843$(52'7%)$ 185$(11'6%)$ 61$(58'7%)$ 4$(3'8%)$ 82$(44'6%)$ 12$(6'5%)$HR$ 85.84$(17'93)$ 16$(2'17%)$ 83'11$(16'80)$ 45$(2'8%)$ 86'24$(17'54)$ 0$ 86'58$(16'92)$ 0$BP$ 123.71$(24'78)$ 15$(2'04%)$ 136'82$(40'45)$ 41$(2'6%)$ 132'19$(28'97)$ 0$ 141'91$(50'49)$ 0$Oral$ antiplatelet$ or$NSAID$
390$(52'9%)$ 2$(0'3%)$ 703$(44'0%)$ 7$(0'4%)$ 44$(42'3%)$ 0$ 72$(39'1%)$ 0$
Oral$anticoagulant$ 132$(17'9%)$ 2$(0'3%)$ 243$(15'2%)$ 7$(0'4%)$ 5$(4'8%)$ 0$ 6$(3'3%)$ 0$Hb$ 97'04$(28'35)$ 2$(0'3%)$ 129'50$(19'15)$ 12$(0'8%)$ 97'86$(24'43)$ 0$ 123'23$(22'38)$ 0$Platelet$count$ 274'42$(124'37)$ 4$(0'5%)$ 259'09$(88'87)$ 17$(1'1%)$ 247'71$(98'60)$ 0$ 233'70$(81'06)$ 0$WBC$(median,$IQR)$ 9'2$(6'80,$12'48)$ 7$(1'0%)$ 9'5$(7'10,$12'80)$ 19$(1'2%)$ 7'5$(5'45,$10'85)$ 1$ 7'10$(5'20,$9'70)$ 1$Urea$(median,$IQR)$ 7'35$(5'20,$10'30)$ 19$(2'6%)$ 5'90$(4'50,$8'00)$ 53$(3'3%)$ 6'25$(4'48,$8'80)$ 0$ 5'60$(3'75,$8'30)$ 1$Creatinine$ 107'94$(82'87)$ 16$(2'2%)$ 88'57$(54'68)$ 34$(2'1%)$ 115'39$(88'29)$ 0$ 98'72$(70'64)$ 0$INR$(median,$IQR)$ 1'10$(1'00,$1'30)$ 266$(36'1%)$ 1'10$(1'00,$1'20)$ 629$(39'3%)$ 1'10$(0'10,$1'10)$ 0$ 0'1$(0'1,$1'10)$ 8$
1. Any!episode!LGIB!resulting!in!hospital!admission!2. Myocardial!infarction,!angina,!congestive!heart!failure,!hypertension!3. Any!active!cancer!excluding!basal!cell!and!squamous!cell!carcinomas!of!the!skin!4. Chronic!liver!disease!with!or!without!cirrhosis!!5. Chronic!kidney!disease!stage!≥2!(eGFR!≤!60

! 128!
Table 16: Sources of bleeding !
! Development*Cohort*N=2336**N*(%)*
Validation*Cohort*N=288*N*(%)*
Diverticular!disease!Colitis!Colorectal!cancer!Haemorrhoids!and!other!benign!anorectal!disorders!Polyps!Post<polypectomy!Angiodysplasia!Small!bowel!bleeding!Unknown!Other*!(missing)!
645!(27.6)!268!(11.5)!106!(4.5)!390!(16.7)!!!55!(2.4)!50!(2.1)!23!(1.0)!8!(0.3)!550!(23.5)!131!(5.6)!93!
84!(29.2)!37!(12.8)!13!(4.5)!38!(13.2)!!!7!(2.4)!3!(1.0)!12!(4.2)!3!(1.0)!68!(23.6)!26!(9.0)!2!
*Aortoenteric fistula, drug induced LGIB, caecal varices, arteriovenous malformation, colonic perforation, colonic endometriosis, intussusception, Meckel’s diverticulum, post-endoscopic biopsy, stenting, post-trans anal endoscopic microsurgery
!The! most! common! interventions! were! flexible! sigmoidoscopy! in! the!
development! cohort! (487/2336,! 20.8%)! and! colonoscopy! in! the! validation!
cohort! (67/288,! 23.3%).! OGD! was! undertaken! in! 256/2336! (11.0%)! of! the!
development! cohort! and! 37/288! (12.8%)! of! the! validation! cohort.! Mesenteric!
angiography!was!rarely!undertaken!(Table!17).!!
*
Table 17: Diagnostic and therapeutic interventions ! Development Cohort
N=2336 N (%)
Validation Cohort N=288 N (%)
OGD (missing) Colonoscopy (missing) Flexible sigmoidoscopy (missing) Capsule endoscopy (missing) Endoscopic haemostasis (missing) Mesenteric angiography ± embolisation (missing)
256 (11.0) 37 92 (3.9) 46 487 (20.8) 44 8 (0.3) 49 41 (1.8) 153 32 (1.4) 57
37 (12.8) 9 67 (23.3) 8 43 (14.9) 8 1 (0.3) 0 13 (4.5) 0 15 (5.2) 0
!
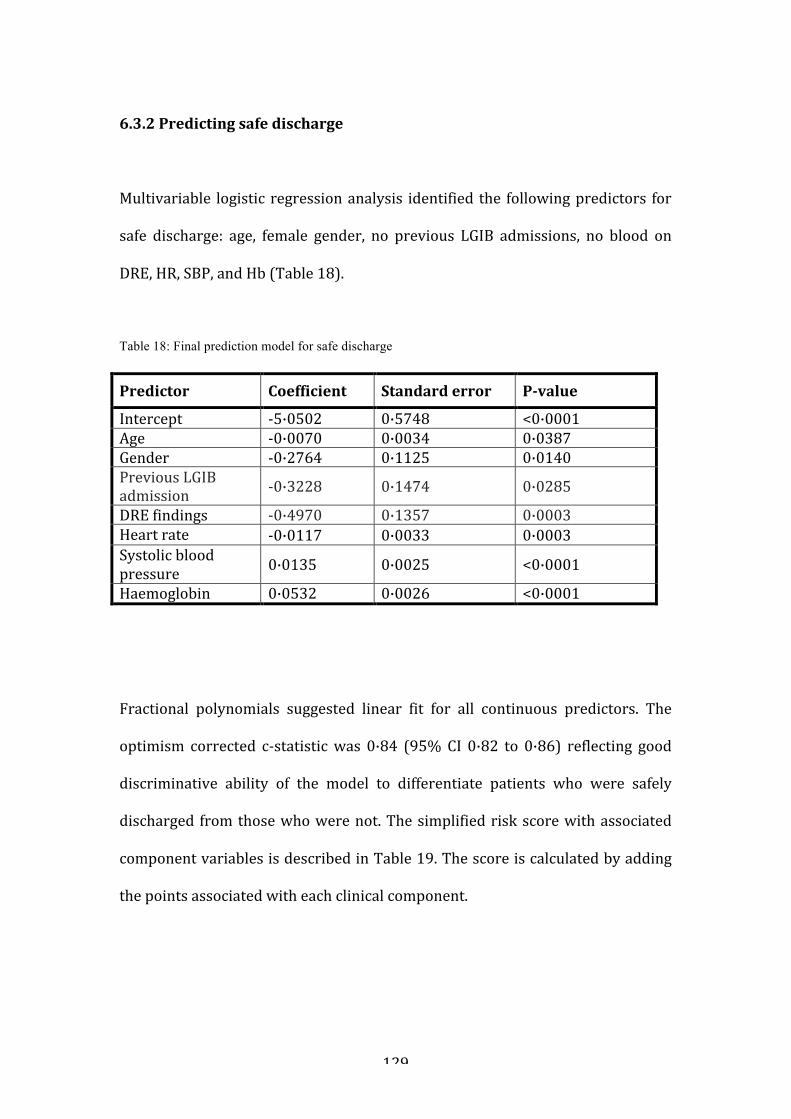
! 129!
!6.3.2*Predicting*safe*discharge*
!
Multivariable! logistic! regression!analysis! identified! the! following!predictors! for!
safe! discharge:! age,! female! gender,! no! previous! LGIB! admissions,! no! blood! on!
DRE,!HR,!SBP,!and!Hb!(Table!18).!!
!
Table 18: Final prediction model for safe discharge !Predictor** Coefficient* Standard*error* PBvalue*
Intercept! <5·0502! 0·5748! <0·0001!Age! <0·0070! 0·0034! 0·0387!Gender! <0·2764! 0·1125! 0·0140!Previous!LGIB!admission! <0·3228! 0·1474! 0·0285!
DRE!findings! <0·4970! 0·1357! 0·0003!Heart!rate! <0·0117! 0·0033! 0·0003!Systolic!blood!pressure! 0·0135! 0·0025! <0·0001!
Haemoglobin! 0·0532! 0·0026! <0·0001!!!
!
Fractional! polynomials! suggested! linear! fit! for! all! continuous! predictors.! The!
optimism! corrected! c<statistic!was! 0·84! (95%!CI! 0·82! to! 0·86)! reflecting! good!
discriminative! ability! of! the! model! to! differentiate! patients! who! were! safely!
discharged! from!those!who!were!not.!The!simplified!risk!score!with!associated!
component!variables!is!described!in!Table!19.!The!score!is!calculated!by!adding!
the!points!associated!with!each!clinical!component.!!
*
!!!
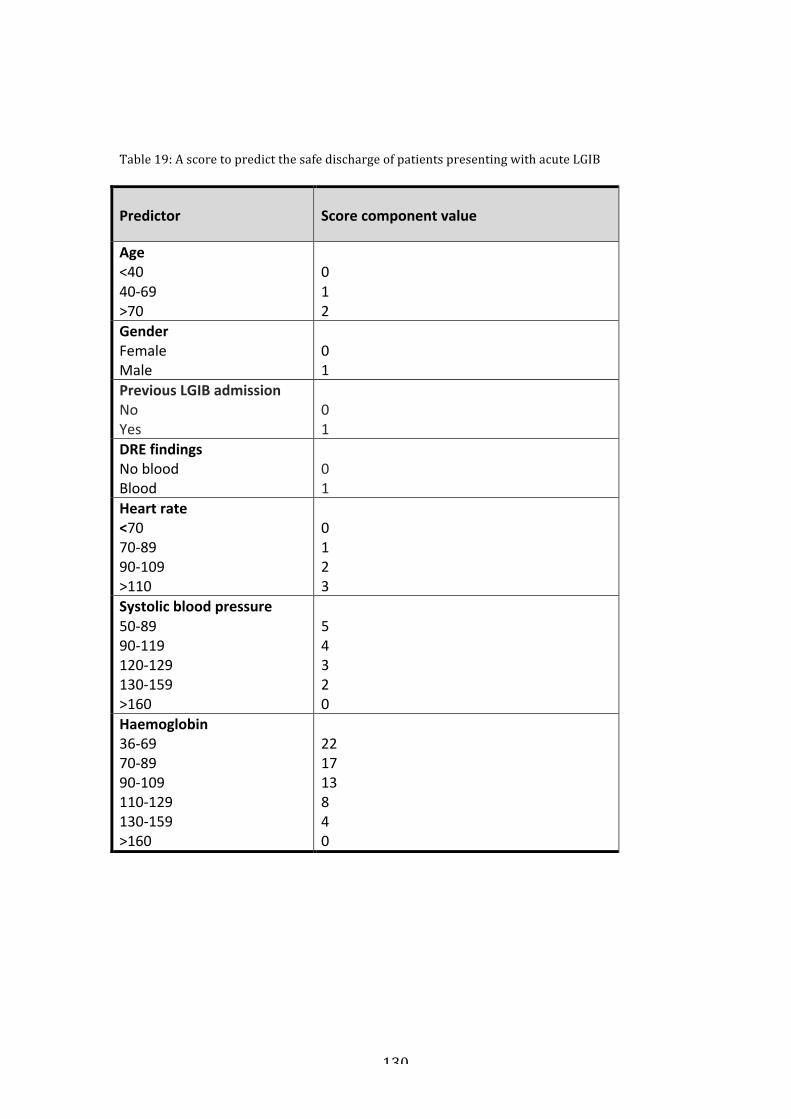
! 130!
!!!Table!19:!A!score!to!predict!the!safe!discharge!of!patients!presenting!with!acute!LGIB!!
Predictor)) Score)component)value)
Age)<40$40%69$>70$
$0$1$2$
Gender)Female$Male)
$0$1$
Previous)LGIB)admission)No$Yes)
$0$1$
DRE)findings)No$blood$Blood)
$0$1$
Heart)rate)<70$70%89$90%109$>110)
$0$1$2$3$
Systolic)blood)pressure)50%89$90%119$120%129$130%159$>160)
$5$4$3$2$0$
Haemoglobin)36%69$70%89$90%109$110%129$130%159$>160$
$22$17$13$8$4$0$
!!!!!
!
!

! 131!
The!c<statistic!of!the!validation!model!was!0·79!(95%!CI!0·73!to!0·84)!with!good!
calibration!(Figure!6).!
Figure 6: Calibration plot of the final prediction model for safe discharge in the validation cohort. 95% CI around the observed predictions (triangle) at tenths of predicted risk. *
!
!
!
!
!
!
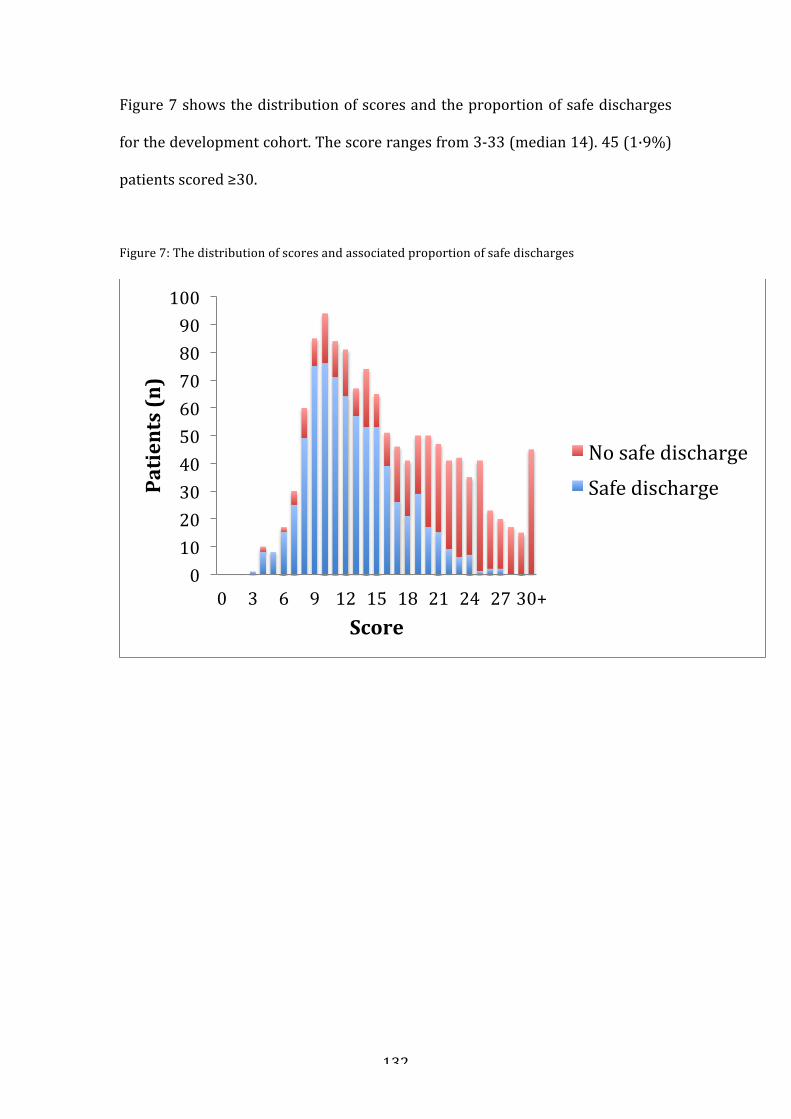
! 132!
Figure!7!shows!the!distribution!of!scores!and!the!proportion!of!safe!discharges!
for!the!development!cohort.!The!score!ranges!from!3<33!(median!14).!45!(1·9%)!
patients!scored!≥30.!!
!
Figure!7:!The!distribution!of!scores!and!associated!proportion!of!safe!discharges!!
!
!
!
!
!
!
!
!
!
0!10!20!30!40!50!60!70!80!90!100!
0! 3! 6! 9! 12! 15! 18! 21! 24! 27!30+!
Patients*(n)*
Score*
No!safe!discharge!Safe!discharge!

! 133!
Table!20!shows!the!probability!of!safe!discharge!at!each!score.!A!patient!with!a!
score! of! eight! has! a! 95%! chance! of! safe! discharge.! In! total! 191/2336! (8.2%)!
patients!scored!8!or!less!and!20!were!unsafe!discharges.!!
Table!20:!probability!of!safe!discharge!by!total!score!!
Total!score! Probability! of! safe!discharge!
0!1!2!3!4!5!6!7!8!9!10!11!12<13!14<15!16<17!
0·99!0·99!0·99!0·98!0·98!0·97!0·96!0·96!0·95!0·93!0·91!0·89!0·87<0·89!0·77<0·81!0·67<0·72!
18<20! 0.50<0.62!21<23! 0.33<0.45!24<26! 0.20<0.28!27<29! 0.11<0.16!≥30! <0.1!
!$
For!absolute!numbers!of!patients!safely!discharged!at!each!score!see!Table!21.!
The!mean!length!of!stay!in!patients!scoring!≤8!was!4±5.5!days,!and!5±6.1!days!in!
patients!that!scored!>8.*
!
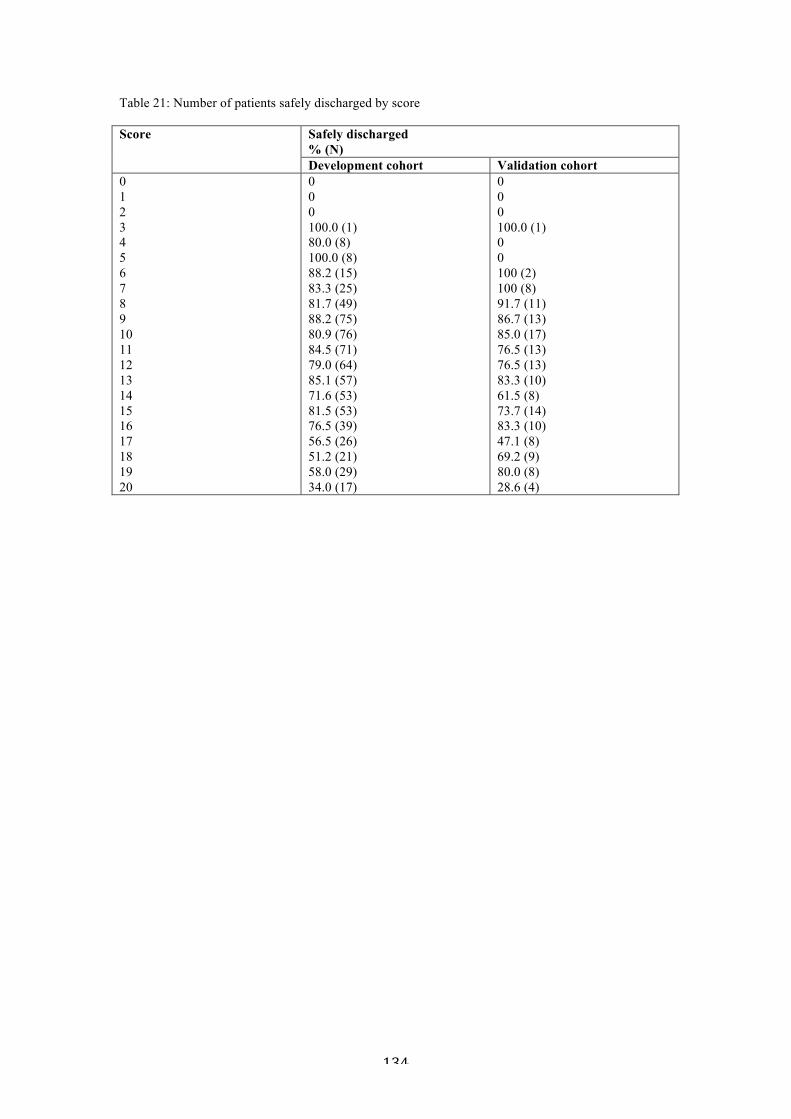
! 134!
Table 21: Number of patients safely discharged by score! Score Safely discharged
% (N) Development cohort Validation cohort
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
0 0 0 100.0 (1) 80.0 (8) 100.0 (8) 88.2 (15) 83.3 (25) 81.7 (49) 88.2 (75) 80.9 (76) 84.5 (71) 79.0 (64) 85.1 (57) 71.6 (53) 81.5 (53) 76.5 (39) 56.5 (26) 51.2 (21) 58.0 (29) 34.0 (17)
0 0 0 100.0 (1) 0 0 100 (2) 100 (8) 91.7 (11) 86.7 (13) 85.0 (17) 76.5 (13) 76.5 (13) 83.3 (10) 61.5 (8) 73.7 (14) 83.3 (10) 47.1 (8) 69.2 (9) 80.0 (8) 28.6 (4)
!!!!
!
!
!
!
*
*
*
*
*
*

! 135!
6.3.3*Comparison*of*the*new*score*with*previously*published*scores*
!
In!comparison!to!Blatchford,!Rockall,!AIMS<65,!BLEED,!Strate,!and!NOBLADS!the!
new! model! demonstrated! superior! ability! to! discriminate! patients! who! were!
safely! discharged! (Table! 22).! For! adverse! outcomes,! the! most! discriminative!
score! for! in<hospital! death!was! AIMS<65! (c<statistic! 0·78),! for! re<bleeding!was!
the! new! model! and! the! Blatchford! score! (c<statistics! 0·74! and! 0·74),! for!
therapeutic!intervention!was!BLEED!(c<statistic!0·65)!and!for!re<admission!with!
further!bleeding!was! the!new!model! (c<statistic!0·68).!No!score!had!a! superior!
performance! across! all! adverse! outcomes,! although! the! new! model!
demonstrated! superior! predictive! ability! for! RBC! transfusion! (c<statistic! 0·92),!
re<bleeding!and!re<admission!with!bleeding!as!well!as!safe!discharge!
!!Table!22:!C<statistics! for!the!new!model!against!existing!models! for!safe!discharge!and!adverse!clinical!outcomes.!!P<values!are!from!the!DeLong!test,!with!reference!to!the!new!model.!!
Model*
Death*(n=52;*2.2%)*
ReBbleeding*(n=323;*13.8%)*
Haemostatic*Intervention*(n=58;*2.5%)*
RBC*Transfusion*(n=576;*24.7%)*
ReBadmission*(n=107;*4.7%)*
Safe*Discharge*(n=1599;*68.5%)*
New!model! 0·67! 0·74! 0·61! 0·92! 0·68! 0·84!
Blatchford! 0·73!(p=0·02)!
0·74!(p=0·71)!
0·59!(p=0·23)!
0·86!(p<0·001)!
0·62!(p<0·001)!
0·80!(p<0·001)!
Aims65! 0·78!(p=0·02)!
0·63!(p<0·001)!
0·60!(p=0·53)!
0·63!(p<0·001)!
0·53!(p<0·001)!
0·64!(p<0·001)!
BLEED! 0·68!(p=0·85)!
0·63!(p<0·001)!
0·65!(p=0·28)!
0·66!(p<0·001)!
0·54!(p<0·001)!
0·65!(p<0·001)!
STRATE! 0·67!(p=0·53)!
0·66!(p<0·001)!
0·59!(p=0·68)!
0·73!(p<0·001)!
0·58!(p<0·001)!
0·69!(p<0·001)!
NOBLADS! 0·72!(p=0·12)!
0·62!(p<0·001)!
0·50!(p=0·04)!
0·66!(p<0·001)!
0·57!(p<0·001)!
0·64!(p<0·001)!
ROCKALL! 0·75!(p=0·06)!
0·61!(p<0·001)!
0·62!(p<0·05)!
0·64!(p<0·001)!
0·53!(p<0·001)!
0·64!(p<0·001)!
!!*****

! 136!
6.4*Discussion**!
This! chapter! has! described! the! derivation! of! an! externally! validated! clinical!
prediction!model! and! simple! risk<scoring! tool! comprising! seven! variables! that!
can!be!routinely!used!to!discriminate!between!LGIB!patients!who!can!be!safely!
managed!as! an!outpatient! and! those!who!will! benefit! from!hospital! admission.!
This!risk!score!is!created!from!a!large!prospectively!acquired!national!database!
of!LGIB!in!the!UK.!It!uses!simple!demographic!and!physical!examination!findings!
in!combination!with!a!single!blood!test!so!is!easily!applicable!by!the!bedside.!!A!
patient! scoring! ≤8! points! at! presentation! has! a! 95%! chance! of! safe! discharge!
from!the!emergency!department.!We!would!advocate!the!use!of!this!threshold!in!
patients!with!no!other!indications!for!hospital!admission.!
!
LGIB! is!widely!recognised!as!a!clinical!area!with!paucity!of!data! to! inform!care!
pathways!and!treatment!guidelines.145!146!In!comparison!to!UGIB,!which!has!seen!
improvements! in! outcomes,2! hospitalisations! due! to! LGIB! are! increasing! and!
mortality!has! remained! constant.2!53!A! risk! score! that! allows!accurate! triage! at!
initial! assessment!has!potential! to!avoid!hospitalisation! in! favour!of!outpatient!
management.!!
!
The! prediction! model! was! built! from! several! constructs! that! were! defined! a!
priori,! which!we! anticipated!would! identify! the! cohort! of! patients! who!would!
come!to!no!harm!following!presentation!with!LGIB.!One!construct!was!to!ensure!
there!was!no! re<bleeding! (for!which!we!used!a!previously!described!definition!
that!required!24!hours!of!stability13).!RBC!transfusion!and!need!for!endoscopic,!
! 137!
radiological! or! surgical! intervention! to! control! bleeding! were! incorporated! to!
capture!adverse!events! that!occurred!within! the!24!period!not! captured! in! the!
re<bleeding! definition,! as! well! as! throughout! the! patient’s! admission.! Re<
admission! with! LGIB! was! included! to! ensure! no! patient! was! subsequently!
readmitted!with!LGIB!within!28!days.!The!data!used!in!this!study!were!collected!
over!two!separate!periods;!2007!to!2011!for!the!validation!cohort,!and!2015!for!
the! development! cohort.! Although! there! are! no! obvious! differences! in! the!
management!of!LGIB!between!the!two!periods,!this!interval!could!have!resulted!
in!differences!between! these! two!populations.!This!may!be!beneficial!however,!
as!the!score!demonstrates!efficacy!in!different!patient!populations.!
!
In!both!the!derivation!and!validation!cohorts!over!60%!patients!presenting!with!
LGIB! were! safely! discharged.! The! estimated! number! of! admissions! to! UK!
hospitals! annually!with!LGIB! is!21,120!cases.131!The!use!of! this! risk! score!may!
avoid! admission! in! many! of! these,! provided! there! is! a! clear! plan! and! prompt!
access!to!outpatient!tests.!This!has!benefits!in!terms!of!reducing!the!exposure!to!
unnecessary!inpatient!stay,!financial!advantages!and!the!prioritising!of!access!to!
inpatient! beds! to! other! more! acutely! unwell! patients.! In! the! UK! the! median!
length!of! stay! is!3!days! for!LGIB.131!Whilst! there! are!no! costs! for!LGIB,! a! large!
micro<costing!study!in!UGIB!demonstrated!a!mean!cost!per!patient!of!£2458,!of!
which!60%!is!attributed!to!the!expense!of!the!inpatient!bed.73!Assuming!similar!
costs!for!LGIB,!avoiding!admission!in!60%!would!equate!to!an!estimated!saving!
of! £18·7m! per! year,! across! NHS! hospitals! in! the! UK,! although! patients! will!
require!outpatient!resources.!

! 138!
Previous!studies!have!identified!that!advancing!age,!unstable!vital!signs,!markers!
of! anaemia,! and!blood!on!DRE!are!predictive! of! adverse!outcomes.11!13!69!129!133!
We! have! additionally! identified! gender! and! previous! hospital! admission! with!
LGIB! as! risk! factors.! The! predictive! value! of! male! gender! is! consistent! with!
another!study!of!LGIB12!and!may!be!due!to!a!higher!burden!of!co<morbid!illness.!
Recurrent!admission! is! likely! to!be!a!marker!of!pathologies! that!are!difficult! to!
manage,! and! prone! to! re<bleeding,! such! as! diverticular! bleeding.147! Use! of!
anticoagulant!and!antiplatelet!drugs!were!included!in!the!model!but!found!not!to!
be!statistically!predictive!of!safe!discharge!and!thus!do!not!feature!in!the!score.!
Given!previous!observational!evidence!that!these!drugs!may!be!associated!with!
increased! severity! of! bleeding131! 13! 133! this! was! unexpected.! However,! even! a!
small!derangement!in!vital!signs,!such!as!SBP!90<120mmHg,!HR!90<109!and!Hb!
130<159g/dL!which!might!be!found!with!these!drugs,!reaches!the!recommended!
threshold!score!of!>8!for!admission.!The!impact!of!anticoagulant!and!antiplatelet!
drugs!on!clinical!outcomes!is!discussed!further!in!Chapter!7.!
!
Although!there!have!been!previous!attempts!at!designing!a!risk!score!for!LGIB,69!
129!13!these!studies!were!limited!by!a!reliance!on!endoscopy!referrals69!or!disease!
classification!codes! for!case!ascertainment.13!Reliance!on!endoscopy! to! identify!
LGIB!cases!may!introduce!unnecessary!investigation!and!delay!in!the!assessment!
of!these!cases.!Accounting!for!bowel!preparation,!it!would!take!a!minimum!of!48!
hours! from! presentation! to! perform! a! colonoscopy! (in! those! hospitals! able! to!
provide!a!7!day!service),! limiting!the!use!of!a!score!that!relies!on!endoscopy!at!
initial! assessment.! Important! subgroups! presenting! with! LGIB! such! as!
inflammatory!bowel!disease13!or!post<endoscopy!bleeds129!were!often!excluded!

! 139!
in!the!previous!scores,!limiting!their!generalizability!to!an!unselected!population.!
Prior!scores!sought!to!predict!severe!haemorrhage!or!mortality,13!69!129!which!we!
have!previously! shown!occurs! in! only!1·4%!and!4·3%!cases! respectively.131! In!
the! present! study,! cases! were! identified! by! clinical! teams! using! presenting!
features! and! the! predicted! outcome! was! safe! discharge,! which! is! much! more!
common.!!
!
Strate! et# al# designed! a! score! comprising! seven! predictors! of! severe! LGIB!
(continued!bleeding,! re<bleeding,! or! re<admission!within! one!week)!using!data!
from!252!patients.13!In!our!current!study,!this!score!performed!well!at!predicting!
RBC! transfusion,! but!was! less! discriminative! for! re<bleeding! and! re<admission.!
The!different!performance!may!be!accounted!for!by!the!differing!rates!of!severe!
bleeding,! which!was! found! in! 49%! cases! in! their! original! data,! but! only! 1·4%!
patients! in!the!current!study.131!A!similar!study!of!132!patients!who!also!had!a!
lower!frequency!of!severe!LGIB!demonstrated!no!significant!association!between!
the!Strate!score!and!severe!bleeding.130!!
!
Aoki!et#al#developed!the!NOBLADS!score,!using!data!from!439!patients!with!LGIB!
confirmed!on!colonoscopy,!identifying!eight!predictors!of!severe!bleeding.69!The!
score!was! validated! using! prospectively! collected! data! from! 161! patients!who!
also!received!colonoscopy.!In!the!current!study,!the!NOBLADS!score!did!predict!
re<bleeding!and!RBC!transfusion,!although!was!not!as!discriminative!as!the!new!
score.!It!is!also!limited!by!the!exclusive!use!of!colonoscopy!to!identify!cases.!!
!

! 140!
The!BLEED!score!was!originally!developed!in!an!intensive!care!population!of!103!
patients!with!GI!bleeding.129!It!was!designed!to!predict!in<hospital!complications!
and!mortality! but! in! the! present! study! was! the! best! predictor! of! haemostatic!
intervention! (albeit! a!weak! effect)! and! did! not! discriminate! the! other! adverse!
outcomes.!This!is!consistent!with!another!study!that!did!not!validate!this!score.11!
!
The!scores!that!have!been!developed!for!UGIB,!Rockall,!Blatchford!and!AIMS<65!
have! been! shown! to! have! some! ability! to! predict! in<hospital!mortality! or! RBC!
transfusion! in! LGIB.141!142! The! current! study! supports! these! findings,! although!
none! of! the! scores! consistently! discriminated! all! of! the! adverse! outcomes! that!
were! studied.! These! scores! did! predict! safe! discharge,! but! were! not! as!
discriminative!as!the!new!score.!Overall!the!best!predictor!for!adverse!outcomes!
in! LGIB!was! the! Blatchford! score,67!with! c<statistics! consistently! above! 0·7! for!
death,!re<bleeding!and!RBC!transfusion.!In!combination!with!the!new!score,!this!
may!be!clinically!useful!when!assessing!patients!who!are!not!safe!for!discharge.!
As!UGIB! tends! to! have! a!more! severe! course! than!LGIB,! if! there! is! any! clinical!
uncertainty!about!the!origin!of!the!GI!bleed,!the!Blatchford!score!should!be!used!
in!preference!to!the!new!score.!
!
Triaging!patients!for!outpatient!management!of!LGIB!raises!important!questions!
about! timing! and! access! to! resources.! There! are! currently! limited! data!
supporting! the!optimum!timing!of! investigation148!although! it! is! recommended!
that! patients! aged! 50! or! over! with! unexplained! rectal! bleeding! should! have!
specialist!assessment!within!two!weeks.149!Gastrointestinal!malignancy!accounts!
for! only! 6%! of! LGIB! admissions,131! so! whether! other! groups! of! patients! also!
! 141!
require! rapid! assessment! requires! further! study.! There! is! urgent! need! for!
randomised! data! comparing! the! diagnostic! yields! of! urgent! and! elective!
outpatient! colonoscopy,! as! an! increase! in! outpatient! endoscopy! service!
requirements!may!have!significant!organisational!implications.!
!
There!are!several!limitations!to!this!study.!Two!components!of!the!safe!discharge!
outcome! relied! on! the! presence! of! RBC! transfusion! (re<bleeding! as! well!
transfusion!itself),!which!may!be!imprecise,!as!many!of!the!transfusions!may!be!
deemed! unnecessary,! when! stratified! by! vital! signs! and! anaemia.131! However,!
this!may!have!led!to!an!under<estimation!of!the!proportion!of!patients!that!could!
have!been!safely!discharged.!The!effect!of!liberal!RBC!transfusion!on!the!number!
of!patients! classified!as!not! safe! for!discharge!could!be! further!explored!by! re<
classifying! the! transfusions! as! necessary! or! potentially! unnecessary.! The! latter!
could!be! identified! as! transfusions! that!were! given! at! a!Hb! trigger! of! >100!g/l!
and! no! haemodynamic! stability.! Further! study! could! look! to! include! these!
patients! in! the! safe! discharge! group! (if! these! patients! were! admitted! for!
transfusion!only),!and!further!analysis!undertaken!to!determine!the!probability!
of! safe! discharge! at! different! points! thresholds,! in! an! attempt! to! increase! the!
proportion!of!patients!classified!as!safe!for!discharge!identified!by!the!score.!!
!
The! composite! outcome! of! safe! discharge! included! death! which! occurred! in!
hospital,! but! not! out! of! hospital! death.! Patients! who! had! unremarkable! index!
admissions!(no!transfusion,!re<bleeding,!or!intervention!to!control!bleeding)!but!
died!out!of!hospital!after!discharge!would!not!have!been!identified.!Both!cohorts!
included!only!patients!that!were!admitted,!therefore!assessment!of!the!safety!of!

! 142!
clinical!decisions!in!patients!that!were!not!admitted!is!beyond!the!scope!of!this!
paper.!
!
In!both!cohorts,!only!25<38%!patients!received!endoscopic!evaluation,!and!a!lack!
of!blood!on!DRE!or!lower!GI!endoscopy!may!suggest!that!some!patients!did!not!
have!true!LGIB.!However,!all!cases!were! identified!by!clinicians!at!presentation!
and!assessed!to!have!LGIB!based!upon!clinical!signs!and!symptoms,!as!opposed!
to!retrospective!review!of!hospital!records!or!from!administrative!databases.!In!
clinical!practice!cases!do!present!with!a!history!of!LGIB,!without!demonstrable!
bleeding! on!DRE! or! colonoscopy,! since! bleeding! can! be! intermittent! in! nature.!!
INR!was!missing!in!895!cases!in!the!development!cohort.!Of!these,!207!patients!
did!not!have!a!clotting!screen!taken,!511!LGIB!patients!had!only!an!APTT!(no!PT!
or!INR),!but!not!an!APTT!ratio!(and!it!was!not!possible!calculate!this!as!we!did!
not! have! data! on! the! normal! range,! which! differs! between! analyser)! and! the!
remaining! 177! patients! had! truly! missing! data! on! coagulation! testing.! The!
variability! in!coagulation!screen!is!reflective!of!real<life!practice!and!in!keeping!
with!a!similar!UK!study!of!4478!cases!of!non<variceal!UGIB,!which!also!found!that!
INR!was!not!routinely!checked!in!40%!cases.150!
!
Sites! were! instructed! to! capture! all! consecutive! cases! but! it! is! inevitable! that!
some! cases! will! have! been! missed.! We! are! unable! to! provide! a! ratio! of!
hospitalized!cases!to!non<hospitalized!cases,!as!there!are!no!national!registries!of!
GP! referrals! or! prospective! ED! registries.! The! latter! are! populated! by! hospital!
codes,! which! use! the! ICD<10! classification! trees.! ICD<10! is! inaccurate! in!
identifying!LGIB!patients,!as!there!are!no!pathology<specific!codes.!!

! 143!
!
Although!the!validation!cohort!originated!from!an!external!database!of!cases,!like!
the! development! cohort,! it! was! sampled! from! a! UK! population! of! patients.!
Different! racial! groups!do!display!different! trends! in!LGIB!diagnoses,51! but! the!
frequency! of! clinical! outcomes,! such! as! mortality! are! consistent! between!
geographically!diverse!populations.12!131! It!would!be!beneficial! to!prospectively!
validate! the! new! score! in! populations! with! different! risk! profiles.! Although! a!
substantial! undertaking,! an!RCT!would! be! a! useful!way! to! further! validate! the!
score.!
!
In!summary,!the!new!score!has!been!developed!using!one!of!the!largest!and!most!
comprehensive!databases!of!LGIB,! and!externally!validated.! It!uses! seven!basic!
predictors!that!are!easily!quantifiable!and! is!simple!to!calculate.! In!comparison!
to!six!other!risk!scores,! it!was!the!best! in!predicting!safe!discharge.! It!could!be!
routinely! incorporated! into! triage! pathways! for! acute! medical! and! surgical!
admissions! to! identify! LGIB! patients! who! can! be! safely! discharged.! Further!
independent!validation!in!external!cohorts!and!in!differing!healthcare!systems!is!
welcomed.!
*
*
*
*
*
*!!

! 144!
CHAPTER* 7:* ACUTE* LOWER* GASTROINTESTINAL* BLEEDING* IN* PATIENTS*RECEIVING*ANTICOAGULANT*OR*ANTIPLATELET*DRUGS**!7.*1*Introduction*
!
In! Chapter! 4,! the! observational! study! demonstrated! that! 29.4%! patients! who!
present!with!LGIB!are!receiving!antiplatelet!drugs,!10.7%!are!receiving!warfarin!
and! 5.2%! are! receiving! DOACs.! Similar! frequencies! are! reported! in! large!
database! studies! of! LGIB.16! 13! Despite! the! frequent! use! of! these! medications,!
there! is! paucity! of! data! to! inform! the! clinical! course! and! outcomes! of! patients!
with!LGIB!who!are!taking!these!drugs,!as!well!as!uncertainty!as!to!whether!they!
should!be!temporarily!halted!or!continued.!Single!centre!studies!have!indicated!
an!increased!risk!of!severe!bleeding!with!aspirin,!clopidogrel!and!warfarin<use,13!
16!117! but! is! not! known!whether! the! use! of! DOACs! also! has! an! adverse! impact!
upon!clinical!outcomes.!
!
The!ability!to!reverse!the!effect!of!drugs!which!promote!bleeding!is!important!in!
the! acute! setting.! The! anticoagulant! effect! of!warfarin! can! be! rapidly! reversed!
with!prothrombin!complex!concentrates!(PCC)!and!vitamin!K.!DOACs!have!short!
half<lives,! and! can! usually! be! managed! by! discontinuing! the! drug! although!
antidotes! are! becoming! available.151! 152! Platelet! dysfunction! associated! with!
antiplatelet!drugs!is!less!easily!managed;!there!is!no!drug!that!directly!reverses!
their! effects.! Antiplatelet! drugs! bind! irreversibly! to! platelets,! the! duration! of!
effect!dependent!on! the! lifespan!of! the!platelet! (4<10!days).153!Withholding! the!
drug! for! a! shorter! time! is! unlikely! to! have! an! appreciable! effect! on! platelet!

! 145!
function.! Simply! transfusing! platelets! may! have! a! limited! beneficial! effect! on!
outcomes!due!to!the!short!half<life!of!transfused!platelets.154!!
!
The! increased! risk! of! bleeding! seen! with! anticoagulant! and! antiplatelet! drugs!
must!be!balanced!against!the!risk!of!cardiovascular!complications!if!the!drug!is!
stopped.! For! this! reason,! the! American! College! of! Gastroenterology! LGIB!
Guideline! recommends! continuing! aspirin! for! secondary! prevention.155! It! also!
recommends!withholding!non<aspirin!antiplatelets!for!up!to!7!days,155!although!
evidence! for! this! is! inferred! from! studies! of! UGIB156! or! patients! undergoing!
gastrointestinal!procedures157!as!opposed!to!patients!with!LGIB.!
!
This!chapter!describes! the!clinical! course!of!patients!admitted!with!acute!LGIB!
who!are!taking!warfarin,!antiplatelets!and!DOACs!and!compare!their!risk!profiles!
to! a! control! group! of! patients!with! LGIB!who!were! not! receiving! any! of! these!
medications.! The! outcomes! of! interest! are! re<bleeding! during! admission,! in<
hospital! mortality,! adverse! cardiovascular! outcomes! and! re<admission! with!
further! bleeding.! In! addition! the! impact! of! withholding! antiplatelets! during!
admission!on!re<bleeding!and!adverse!cardiovascular!events!is!explored.!!
!
!
!
!
!
!
!
! 146!
7.2*Methods*
This! is!a!post<hoc!analysis!of!the!prospectively!collected!data!from!the!national!
observational!study!described!in!Chapter!4.!Anticoagulant!and!antiplatelet!drug!
use! was! established! from! medical! notes! and! drug! charts.! Patients! receiving!
single! or! dual! antiplatelet! therapy! (DAPT),! warfarin! or! DOACs! as! a! regular!
medication! upon! presentation! with! bleeding! were! identified.! Patients! taking!
concurrent! oral! NSAIDs! (n=146)! or! combinations! of! antiplatelet! drugs! with!
warfarin,! DOACs,! or! parenteral! anticoagulation! were! excluded! (n=237).! The!
latter! group! were! excluded! from! this! analysis,! as! due! to! the! number! of! drug!
combinations! it! was! not! possible! to! classify! them! into! discrete! groups! of! a!
meaningful!size.!A!control!group!of!patients!within! the!same!study!cohort!who!
were!taking!no!antiplatelet!drugs,!anticoagulants!or!NSAIDs!was!also!identified.!!
!
7.2.1*Study*definitions*
Re<bleeding! was! defined! as! additional! transfusion! requirements! and/or! a!
decrease!in!Hct!≥20%!after!24!hours!of!clinical!stability.13!Need!for!intervention!
was!defined!as!the!need!for!a!procedure!to!arrest!bleeding,!including!endoscopic!
haemostasis,!mesenteric!embolisation!or!laparotomy!for!bleeding.!Re<admission!
with!bleeding!was!defined!as!re<bleeding!up!to!28!days!post<discharge.!!
!
Adverse! cardiovascular! outcome! was! defined! as! in<hospital! acute! coronary!
syndrome,! ischaemic! stroke,! other! ischaemic! vascular! event! or! cardiovascular!
death.! Cardiovascular! death!was! defined! as! fatal! ischaemic! stroke,!myocardial!
infarction!(MI)!or!death!from!an!ischaemic!event.!
!
! 147!
7.2.2*Statistical*methods*
Continuous!data!are!presented!as!mean!and!SD!or!median!and!IQR.!Categorical!
data!are!compared!using!Fisher’s!exact!test.!
!
Kaplan%Meier$curves$of$time$to$ in%hospital$re%bleeding$for$each$group$were$plotted$
(GraphPad$ Prism$ v7,$ San$ Diego,$ USA).$ Cox$ proportional$ hazards$ (PH)$ regression$
models$ were$ then$ used$ to$ analyse$ the$ in%hospital$ re%bleeding$ outcome.$ For$ each$
patient,$time$to$event/censoring$was$derived$as$follows:$
• For$ those$ patients$ who$ experienced$ re%bleeding:$ number$ of$ days$ after$
admission$when$the$re%bleeding$event$occurred.$$
• For$those$patients$who$are$censored:$number$of$days$they$were$followed$up$
for$until$death,$discharge$or$the$study$end%point$of$28$days$post%discharge$$
Paul!Bassett!(independent!statistics!consultant)!performed!the!following!cox!and!
multivariate! logistic! regression! modelling.! Univariate! and! multivariate! cox! PH!
regression! models! were! used! to! analyse! the! association! between! group! of!
patients!and!time!to!re<bleeding.!The!hazard!ratio!and!95%!CI!for!re<bleeding!are!
presented!for!the!groups!of!patients!compared!to!the!control!group.!The!baseline!
covariates! included! in! the!multivariate! cox! regression!model! are;! age,! gender,!
Charlson!co<morbidity! index,!HR! (beats!per!minute),! SBP! (mmHg),! frank!blood!
on!DRE,!Hb,! reversal! of! antiplatelet! or! anticoagulant! drug! (reversal! versus!no<
reversal! versus! no! drug)! and! admission! status! (new! presentation! versus!
established! inpatient!versus!other).!These! covariates!were!determined!a!priori!
upon!clinical!plausibility.!
!

! 148!
The$remaining$outcomes$(adverse$cardiovascular$outcome,$in%hospital$mortality$and$
28%day$re%admission)$were$analysed$using$logistic$regression$models.$Univariate$and$
multivariate$ logistical$ regression$ models$ were$ fitted$ and$ the$ OR$ and$ 95%$ CI$ are$
presented$ for$ the$ antiplatelet$ and$ anticoagulant$ groups$ compared$ to$ the$ control$
group.$ The$ risk$ factors$ included$ in$ the$multivariate$ logistic$ regression$models$ are$
described$ above$ in$ the$ cox$ PH$ regression$models.$ Cases$with$missing$ data$ on$ the$
study$ outcomes$ were$ excluded$ from$ both$ the$ cox$ PH$ and$ multivariate$ logistic$
regression$models.$
!
Finally! the! cox! PH! regression! analyses! for! re<bleeding! was! repeated! on! a!
subgroup! of! single! antiplatelet! users! who! had! complete! data! on! whether! the!
antiplatelet!drug!was! stopped!during!admission.!The!purpose!of! this! subgroup!
analysis! was! to! assess! for! an! association! between! continuing! the! antiplatelet!
during!admission!with!LGIB!and!re<bleeding.!HR!and!95%!CI!are!presented! for!
the!patients!who!had!their!antiplatelet!withheld! for!<5!days!and!for! those!who!
had!it!withheld!for!≥!5!days,!in!comparison!to!a!group!of!patients!who!had!their!
antiplatelet!continued!after!presentation!with!bleeding.!A!threshold!of!five!days!
was! chosen! as! this! is! the! average! time! to! normal! platelet! function! after!
antiplatelet!drug!discontinuation.158!
!
!
*
*
*

! 149!
*
7.3*Results**
We! identified! 504! patients! taking! a! single! antiplatelet! drug,! 79! taking! DAPT!
drugs,! 232!patients! taking!warfarin,! 102!patients! taking! a!DOAC! and! a! control!
group!of!1218!patients! taking!none!of! these!drugs!(Figure!8).!The!DOAC!group!
included! 63! patients! taking! rivaroxaban,! 26! taking! apixaban! and! 13! taking!
dabigatran.! Most! patients! taking! an! antiplatelet! drug! were! taking! aspirin! or!
clopidogrel,!only!16!were! receiving! ticagrelor,!6!dipyridamole!and!1!prasugrel.!
No!patients!were!receiving!abciximab.!!
!
Figure!8:!Flow<chart!of!cases!!
!
!
!
2528$pa'ents$with$LGIB$
Control$$
(n=1218)$
Single$an'platelet$$
drug$(n=504)$
Dual$an'platelet$
$drug$(n=79)$
Warfarin$(n=232)$
DOAC$$
(n=102)$
NSAIDs$excluded$(n=146)$
Combina'ons$of$an'coagulants,$
an'platelets$or$DOACs$excluded$(n=237)$Missing$data$on$
an'coagulant,$an'platelet$or$DOAC$status$excluded$(n=10)$

! 150!
!
7.3.1.Characteristics* of* patients* taking* antiplatelet* or* oral* anticoagulant*
drugs*
!
Patients! taking! antiplatelet! or! oral! anticoagulant! drugs! were! elderly;! patients!
receiving! DOACs! represented! the! oldest! group! of! patients! (79.9! years! ±10.8,!
Table!23).!Patients!in!the!DAPT!group!had!the!highest!burden!of!cardiovascular!
co<morbidities! such! as!MI! and! peripheral! vascular! disease! (47/79,! 59.5%! and!
11/79,!13.9%!respectively)! although! the!highest! rates!of!previous! stroke!were!
seen!in!patients!taking!DOACs!(21/102,!20.6%).!!
!!!!!!!!!!!!!!!!!!!!!!!!!!!!!

! 151!
!!Table!23:!Patient!characteristics!by!drug!group!!! Control!
!!N=1218!N!(%)!
Single!antiplatelet!user!N=504!N!(%)!
Dual!antiplatelet!user!N=79!N!(%)!
DOAC!!!N=102!N!(%)!
Warfarin!!!N=232!N!(%)!
Age!(years)! 61.4!±!20.47! 77.9!±!10.91! 73.4!±!11.37! 79.9!±!10.77! 78.6!±!10.11!! ! ! ! ! !! ! ! ! ! !Female!Gender! 662!(54.5%)! 245!(48.7%)! 34!(43.6%)! 56!(54.9%)! 124!(53.5%)!! ! ! ! ! !! ! ! ! ! !Charlson! Co<morbidity!Index!!
! ! ! ! !
0! 700!(57.8%)! 123!(24.4%)! 10!(12.7%)! 27!(26.5%)! 75!(32.3%)!1! 200!(16.5%)! 174!(34.5%)! 29!(36.7%)! 25!(24.5%)! 56!(24.1%)!2+! 312!(25.7%)! 207!(41.1%)! 40!(50.6%)! 50!(49.0%)! 101!(43.5%)!! ! ! ! ! !! ! ! ! ! !Hypertension! 356!(29.4%)! 266!(52.8%)! 40!(50.6%)! 54!(52.9%)! 121!(52.2%)!MI! 39!(3.2%)! 102!(20.2%)! 47!(59.5%)! 12!(11.8%)! 29!(12.5%)!CCF! 37!(3.1%)! 32!(6.4%)! 6!(7.6%)! 20!(19.6%)! 33!(14.2%)!Peripheral!vascular!disease!
21!(1.7%)! 27!(5.4%)! 11!(13.9%)! 1!(1.0%)! 10!(4.3%)!
Stroke! 33!(2.7%)! 74!(14.7%)! 11!(13.9%)! 21!(20.6%)! 27!(11.6%)!Diabetes! 133!(10.9%)! 97!(19.3%)! 15!(19.0%)! 5!(4.9%)! 44!(19.0%)!! ! ! ! ! !! ! ! ! ! !HR! 85.5!±!16.86! 82.0!±!17.20! 78.9!±!15.67! 81.6!±!17.33! 81.3!±!16.07!! ! ! ! ! !SBP!(mmHg)! 132.1!±!24.78! 133.7!±!26.66! 129.1!±!22.93! 125.0! ±!
20.54!131.8!±!27.96!
! ! ! ! ! !Shocked!participant*!
27!(2.3%)! 11!(2.2%)! 0!(0.0%)! 4!(4.1%)! 4!(1.8%)!
! ! ! ! ! !! ! ! ! ! !Admitting!Hb! 121.7!±!27.96! 116.8!±!26.08! 111.5!±!23.36! 106.5! ±!
30.38!114.4!±!24.07!
! ! ! ! ! !*!Shock!defined!as!HR>100!and!SBP<100mmHg!Missing!data:!age!0,!gender!0.3%,!co<morbidities!0.3%,!HR!2.5%,!SBP!2.2%,!shocked!status!2.6%,!admitting!Hb!0.5%.!!DOAC,!direct!oral!anticoagulant;!MI,!myocardial! infarction;!CCF,!congestive!cardiac! failure;!HR,!heart!rate;!SBP,!systolic!blood!pressure;!Hb,!haemoglobin.!$!$Presentation!with! haemodynamic! shock!was! uncommon! across! all! groups! and!
there! was! no! difference! in! patients! taking! antiplatelet! drugs! (single! p=1.00,!
DAPT! p=0.41),! warfarin! (p=0.81)! or! DOACs! (p=0.09)! in! comparison! to! the!
control! group.! In! comparison! to! the! control! group,! patients! taking! DOACs!
! 152!
(p<0.0001),! single! antiplatelet! drugs! (p<0.001)! or! warfarin! (p<0.0001)!
presented!with!significantly!lower!Hb!concentrations,!with!the!lowest!presenting!
mean! Hb! observed! in! the! DOAC! group.! Clinically! significant! anaemia!
(Hb<80g/dL)!was!found!in!22/102!(21.6%)!of!the!DOAC!group,!24/232!(10.3%)!
of!the!warfarin!group,!50/504!(9.9%)!of!the!single!antiplatelet!drug!group,!8/79!
(10.1%)!of!the!DAPT!group!and!119/1218!(9.8%)!of!the!control!group.!
!
7.3.2*Management*of*warfarin,*antiplatelets*and*DOACs*
!
In! the! warfarin! group,! 210/232! (90.5%)! patients! had! their! warfarin! stopped!
during! admission! and! 99/232! (42.7%)! had! it! reversed! either! with! vitamin! K!
alone! (81! patients),! PCC! alone! (3! patients)! or! both! (15! patients).! In! the!DOAC!
group! 92/102! (90.2%)! patients! had! their! drug! stopped! during! admission! but!
only! 6/102! (5.9%)! received! treatment! in! an! attempt! to! reverse! its! effect;! 4!
patients!receiving!PCC!and!2!FFP.!No!patient!received!a!specific!antidote!to!the!
DOAC,!although!this!study!was!performed!before!the!widespread!availability!of!
idarucizumab.151! In! the! antiplatelet! drug! groups,! 376/504! (74.6%)! patients!
taking!a!single!antiplatelet!drug!had!their!antiplatelet!drug!withheld!and!58/79!
(73.4%)!patients!taking!DAPT!had!at!least!one!antiplatelet!drug!withheld.!Only!8!
patients!receiving!an!antiplatelet!drugs!received!a!platelet!transfusion,!6!of!these!
were! in! the! single! antiplatelet! drug! group.! Of! the! 376! patients! who! had! their!
single! antiplatelet! withheld,! 166/376! (44.2%)! restarted! it! before! or! upon!
discharge.!In!the!DAPT!group,!this!figure!was!30/79!(38.0%).!
!
!
! 153!
Although!DOAC!patients! tended! to! present!with! the! lowest!Hb! concentrations,!
proportionally! more! patients! taking! antiplatelet! drugs! received! a! RBC!
transfusion,!the!highest!proportion!being!seen!in!the!patients!taking!DAPT!drugs!
(34/79,!43%!vs!256/1213,!21.1%!control!group,!p!<0.0001,!Table!24).!Patients!
taking!single!antiplatelet!drugs!or!DOACs!were!also!more!likely!than!those!in!the!
control! group! to! receive! RBC! transfusion! (160/499,! 32.1%,! p<0.0001! and!
32/102,!30.5%,!p<0.05),!respectively.!There!was!no!difference!in!the!number!of!
patients! that! received! RBC! transfusion! in! the!warfarin! group! compared! to! the!
control!(60/231,!26.0%!vs!256/1213,!21.1%!p=0.118).!!
!
!
!
!
!
!
!
!
!
!
!
!
!
!
!

! 154!
Endoscopic!haemostasis,!mesenteric! embolisation!and! laparotomy! for!bleeding!
were! uncommon! across! all! groups! (Table! 24).! Despite! proportionally! more!
patients!on!single!or!dual!antiplatelet! therapy! receiving!RBC! transfusion,! there!
was! no! difference! in! the! proportion! of! patients! requiring! intervention! for!
bleeding!when!compared!to!the!control!(control!34/1145,!3.0%;!single!10/472,!
2.1%!p=0.40;!dual!3/74,!4.1%,!p=0.49).!!
!!!Table!24:!Interventions!for!LGIB!by!antiplatelet!and!anticoagulant!exposure!!! Control!
!!N=1218!N!(%)!
Single!antiplatelet!exposed!N=504!N!(%)!
Dual!antiplatelet!exposed!N=79!N!(%)!
DOAC!exposed!!N=102!N!(%)!
Warfarin!exposed!!N=232!N!(%)!
Red!cells! ! ! ! ! !Transfused?! 256!(21.1%)! 160!(32.1%)! 34!(43.0%)! 32!(31.4%)! 60!(26.0%)!! ! ! ! ! !Volume! 0.67!±!1.648! 1.01!±!1.774! 1.41!±!2.245! 1.11!±!1.903! 0.88!±!1.825!(missing!data)! ! ! ! ! !! ! ! ! ! !Endoscopic!haemostasis!
26!(2.2%)! 6!(1.3%)! 1!(1.3%)! 1!(1.0%)! 6!(2.7%)!
! ! ! ! ! !! ! ! ! ! !Mesenteric!embolisation!
7!(0.6%)! 4!(0.8%)! 2!(2.6%)! 2!(2.0%)! 1!(0.5%)!
! ! ! ! ! !! ! ! ! ! !Laparotomy! for!bleeding!
3!(0.3%)! 0!(0.0%)! 0!(0.0%)! 0!(0.0%)! 0!(0.0%)!
! ! ! ! ! !! ! ! ! ! !Combined!intervention*!
34!(3.0%)! 10!(2.1%)! 3!(4.1%)! 3!(3.0%)! 7!(3.2%)!
(missing!data)! ! ! ! ! !! ! ! ! ! !!*!Patients!may!have!had!more!than!one!intervention!!Missing! data:! transfused! participants! 0.5%,! RBC! transfusion! volume! 2.3%,! endoscopic! haemostasis! 3.8%,! mesenteric!embolisation!2.1%,!laparotomy!for!bleeding!1.4%,!combined!intervention!2.7%.!!DOAC,!direct!oral!anticoagulant!
!!
*

! 155!
7.3.3.Diagnoses*
The!most!common!source!of!LGIB!was!diverticula!across!all!groups,!the!highest!
frequency! seen! in! the! single! antiplatelet! drug! group! (188/504,! 37.3%).! In!
comparison! to! the! control,! fewer!patients! in! the! antiplatelet! and! anticoagulant!
groups! were! diagnosed! with! benign! anorectal! causes! or! inflammatory! bowel!
disease.!At!least!20%!patients!in!each!group!were!discharged!without!a!diagnosis!
(Table!25).!!
!
Table!25:!Sources!of!LGIB!by!drug!exposure!!! !
Control!N=1218!N!(%)!
Single!antiplatelet!exposed!N=504!N!(%)!
Dual!antiplatelet!exposed!N=79!N!(%)!
DOAC!exposed!!N=102!N!(%)!
Warfarin!exposed!!N=232!N(%)!
Diverticular!bleed!IBD!Other!colitis!Ischaemic#colitis#Benign!anorectal!conditions!Colorectal!cancer!Angiodysplasia!Unknown!Other!!
280!(23.0)!48!(3.9)!137!(11.2)!36!(3.0)!239!(19.6)!!70!(5.7)!14!(1.1)!324!(26.6)!127!(10.4)!!
188!(37.3)!5!(1.0)!29!(5.8)!24!(4.8)!56!(11.1)!!24!(4.8)!3!(0.6)!129!(25.6)!45!(8.9)!!
19!(24.1)!1!(1.3)!3!(3.8)!2!(2.5)!6!(7.6)!!5!(6.3)!1!(1.3)!24!(30.4)!17!(21.5)!!
31!(30.4)!1!(1.0)!2!(2.0)!2!(2.0)!16!(15.7)!!9!(8.8)!0!(0)!22!(21.6)!19!(18.6)!!
67!(28.9)!3!(1.3)!7!(3.0)!7!(3.0)!32!(13.8)!!12!(5.2)!2!(0.9)!52!(22.4)!55!(23.7)!
*!Patients!may!have!had!more!than!one!diagnosis!Missing!data:!control!2.3%,!single!antiplatelet!2.2%,!dual!1.3%,!DOAC!0%,!warfarin!4.7%.!!**
*
*
*
*
*
*
*

! 156!
7.3.4.*ReBbleeding*
Time!to!in<hospital!re<bleeding!for!all!groups!is!shown!in!Figure!9.!!
Figure!9:!Kaplan<Meier!graph!of!time!to!in<hospital!re<bleeding!!
!
!
Most! re<bleeding!occurred!within! the! first! 5!days! (Figure!9).! In! comparison! to!
the!control!group,!the!highest!rates!of! in<hospital!re<bleeding!were!observed!in!
the!DAPT!group!(38.0%,!95%!CI!22.3!to!52.7,!p=0.0005)!followed!by!the!single!
antiplatelet!group!(28.2%,!95%!CI!22.8!to!33.6,!p=0.04).!!Re<bleeding!rates!in!the!
DOAC!(20.0%,!95%!CI!0.5! to!30.5,!p=0.52)!and!warfarin!group!(23.1%,!95%!CI!
15.1! to! 31.1,! p=0.99)!were! similar! to! the! control! group! (19.4%,! 95%!CI! 16! to!
22.8).!
!
!!!!!
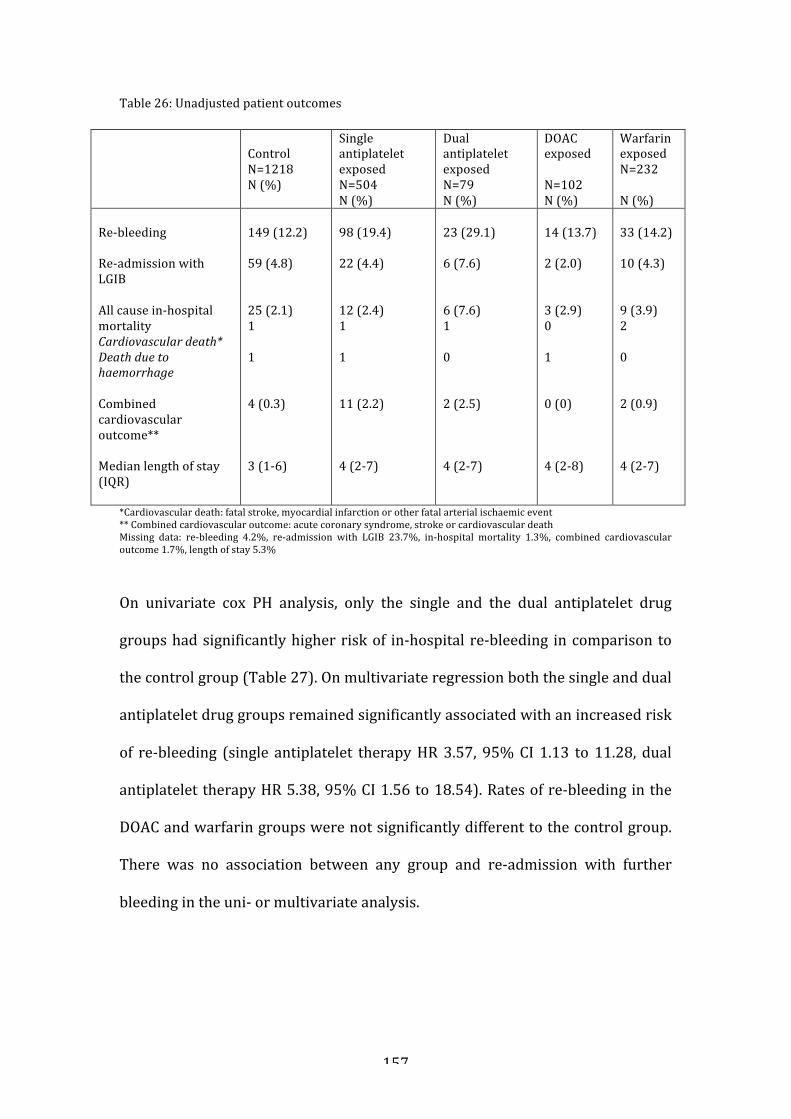
! 157!
Table!26:!Unadjusted!patient!outcomes!!
! !Control!N=1218!N!(%)!
Single!antiplatelet!exposed!N=504!N!(%)!
Dual!antiplatelet!exposed!N=79!N!(%)!
DOAC!exposed!!N=102!N!(%)!
Warfarin!exposed!N=232!!N!(%)!
!Re<bleeding!!Re<admission!with!LGIB!!All!cause!in<hospital!mortality!Cardiovascular#death*#Death#due#to#haemorrhage#!Combined!cardiovascular!outcome**!!Median!length!of!stay!(IQR)!!
!149!(12.2)!!59!(4.8)!!!25!(2.1)!1!!1!!!4!(0.3)!!!!3!(1<6)!!!
!98!(19.4)!!22!(4.4)!!!12!(2.4)!1!!1!!!11!(2.2)!!!!4!(2<7)!!!
!23!(29.1)!!6!(7.6)!!!6!(7.6)!1!!0!!!2!(2.5)!!!!4!(2<7)!!!
!14!(13.7)!!2!(2.0)!!!3!(2.9)!0!!1!!!0!(0)!!!!4!(2<8)!
!33!(14.2)!!10!(4.3)!!!9!(3.9)!2!!0!!!2!(0.9)!!!!4!(2<7)!
*Cardiovascular!death:!fatal!stroke,!myocardial!infarction!or!other!fatal!arterial!ischaemic!event!**!Combined!cardiovascular!outcome:!acute!coronary!syndrome,!stroke!or!cardiovascular!death!Missing! data:! re<bleeding! 4.2%,! re<admission! with! LGIB! 23.7%,! in<hospital! mortality! 1.3%,! combined! cardiovascular!outcome!1.7%,!length!of!stay!5.3%!!*On! univariate! cox! PH! analysis,! only! the! single! and! the! dual! antiplatelet! drug!
groups!had!significantly!higher!risk!of! in<hospital! re<bleeding! in!comparison! to!
the!control!group!(Table!27).!On!multivariate!regression!both!the!single!and!dual!
antiplatelet!drug!groups!remained!significantly!associated!with!an!increased!risk!
of! re<bleeding! (single! antiplatelet! therapy!HR!3.57,! 95%!CI! 1.13! to!11.28,! dual!
antiplatelet!therapy!HR!5.38,!95%!CI!1.56!to!18.54).!Rates!of!re<bleeding!in!the!
DOAC!and!warfarin!groups!were!not!significantly!different!to!the!control!group.!
There! was! no! association! between! any! group! and! re<admission! with! further!
bleeding!in!the!uni<!or!multivariate!analysis.!!
!
!!

! 158!
Table! 27:! Univariate! and! multivariate! regression! models! for! re<bleeding,! re<admission! with!bleeding,!mortality!and!adverse!cardiovascular!outcomes!!
! Univariate!regression!! Multivariate*!regression!
OR! (95%! CI,! HR!for! cox!regression)!
P<value! OR! (95%! CI,! HR!for! cox!regression)!
P<value!
InBhospital*reBbleeding***Control!
!!1!
!!0.003!
!!1!
!!0.001!
Single!antiplatelet!! 1.40!(1.08,!1.80)! ! 3.57!(1.13,!11.28)! !Dual!antiplatelet!! 2.19!(1.40,!3.42)! ! 5.38!(1.56,!18.54)! !DOAC!! 0.85!(0.49,!1.47)! ! 1.72!(0.49,!6.02)! !Warfarin!!!! 0.99!(0.68,!1.45)! ! 2.00!(0.56,!7.17)! !!ReBadmission*with*further*bleeding*Control!Single!antiplatelet!Dual!antiplatelet!DOAC!Warfarin!!Mortality*Control!Single!antiplatelet!Dual!antiplatelet!DOAC!Warfarin!!Adverse*cardiovascular*outcome*Control!Single!antiplatelet!Dual!antiplatelet!DOAC!Warfarin!!!
!!!!1!0.88!(0.53,!1.45)!1.68!(0.69,!4.08)!0.39!(0.09,!1.61)!0.91!(0.46,!1.82)!!!1!1.16!(0.58,!2.33)!3.93!(1.56,!9.89)!1.43!(0.42,!4.82)!1.76!(0.78,!3.95)!!!!!1!6.75!(2.14,!21.29)!8.20!(1.48,!45.50)!<!2.72!(0.50,!14.94)!
!!!0.41!!!!!!!!0.11!!!!!!!!!0.03!
!!!!1!0.49!(0.02,!10.78)!0.88!(0.04,!21.52)!0.19!(0.01,!5.55)!0.70!(0.03,!16.94)!!!1!0.10!(0.01,!1.04)!0.35!(0.03,!4.27)!0.09!(0.01,!1.31)!0.10!(0.01,!1.32)!!!!!!<!<!<!<!<!
!!!0.41!!!!!!!!0.08!!!!!!!!!!
*!Adjusted! for!age,!gender,!Charlson!co<morbidity! index!(0!versus!1!versus!2+),!HR,!SBP,! frank!blood! on! rectal! examination,! Hb,! reversal! of! antiplatelet/anticoagulant! agent! and! admission!status!!**!All!analyses!employ!logistic!regression!modelling!except!in<hospital!re<bleeding!which!is!a!cox!regression!with!hazard!ratios!!
*
! 159!
7.3.5*Mortality*
The! highest! unadjusted! rates! of! in<hospital! mortality! were! seen! in! the! dual!
antiplatelet! drug! group! (Table! 26).! Mortality! due! to! severe! haemorrhage! was!
very!uncommon!across!all!groups.!There!was!no!significant!association!between!
antiplatelet! or! anticoagulant! group! and! all<cause! mortality! in! the! uni<! or!
multivariate!analysis!(Table!27).!!
!
7.3.6*Adverse*cardiovascular*outcomes*
Cardiovascular!death!was!uncommon!across!all!groups.!Adverse!cardiovascular!
outcomes!were! infrequent!and!as! follows;! the! control!group! included!one! fatal!
MI,! two! cases!of!ACS!and!an! ischaemic! limb,! the! single! antiplatelet!drug!group!
included! one! fatal!MI,! seven! ACS! and! three! strokes,! the! dual! antiplatelet! drug!
group! included!one! fatal! stroke! and!one!ACS,! the!warfarin! group! included!one!
fatal! MI! and! one! fatal! ischaemic! gut.! There! were! no! adverse! cardiovascular!
outcomes! in! the! DOAC! group.! Univariate,! unadjusted! analysis! suggested! a!
significant!association!between!single!and!dual!antiplatelet!drug!use!and!adverse!
cardiovascular! outcomes! in! comparison! to! the! control! (single! antiplatelet!
therapy!OR!6.75,!95%!CI!2.14!to!21.19,!dual!antiplatelet!therapy!OR!8.20,!95%!CI!
1.48! to! 45.50).! The! number! of! events! was! too! few! to! perform! meaningful!
multivariate!analysis!(Table!27).!
!
*
*
*
*

! 160!
7.3.7*Withholding*antiplatelets*during*admission*
In! the! single! antiplatelet! drug! group! 385/504! (76.4%)! cases! had! data! on!
whether! the! antiplatelet! drug! was! withheld! during! admission;! in! 140/385!
(36.4%)! the!antiplatelet!drug!was!withheld! for!<5!days,! in!134/385!(34.8%)! it!
was!withheld! for! ≥! 5! days,! and! in! 111/385! (28.8%)! cases! it!was! not!withheld!
(Table!28).!!
!
Table!28:!Unadjusted!patient!outcomes!in!patients!who!were!receiving!a!single!antiplatelet!and!had!it!continued!and!those!that!had!it!interrupted!!
! Antiplatelet!user,!N=!385**!Continued!N=111!N!(%)!
Stopped!<5!days!!N=140!N!(%)!
Stopped!≥5!days!N=!134!N!(%)!
Re<bleeding! 11!(10.2%)! 14!(10.5%)! 38!(29.0%)!(missing!data)! (3)! (6)! (3)!! ! ! !Combined! cardiovascular!outcome!
1!(0.9%)! 3!(2.2%)! 5!(3.7%)!
(missing!data)! (1)! (2)! (0)!! ! ! !Cardiovascular#death*! 1!(0.9%)! 0!(0.0%)! 2!(1.5%)!(missing!data)! (1)! (1)! (0)!! ! ! !All<cause! in<hospital!mortality!
4!(3.6%)! 1!(0.7%)! 4!(3.0%)!
(missing!data)! (0)! (1)! (0)!! ! ! !Re<admission!with!LGIB! 3!(3.8%)! 8!(7.0%)! 5!(4.7%)!(missing!data)! (32)! (25)! (27)!
*!In<hospital!death!due!to!stroke,!MI!or!other!ischaemic!event!**119!patients!no!data!on!duration!of!single!antiplatelet!therapy!!
No!difference!was!observed! in!re<bleeding!rates!between!patients!who!had!the!
antiplatelet! drug! stopped! for! <5! days! compared! to! those! who! continued! it!
throughout! their!admission!on!univariate! (14/140,!10.5%!cases!of! re<bleeding,!
versus!11/111,!10.2%,!respectively,!HR!0.98,!95%!CI!0.45!to!2.17,!Table!29)!or!
multivariate!cox!regression!analysis!(HR!0.95,!95%!CI!0.41!to!2.21).!
*
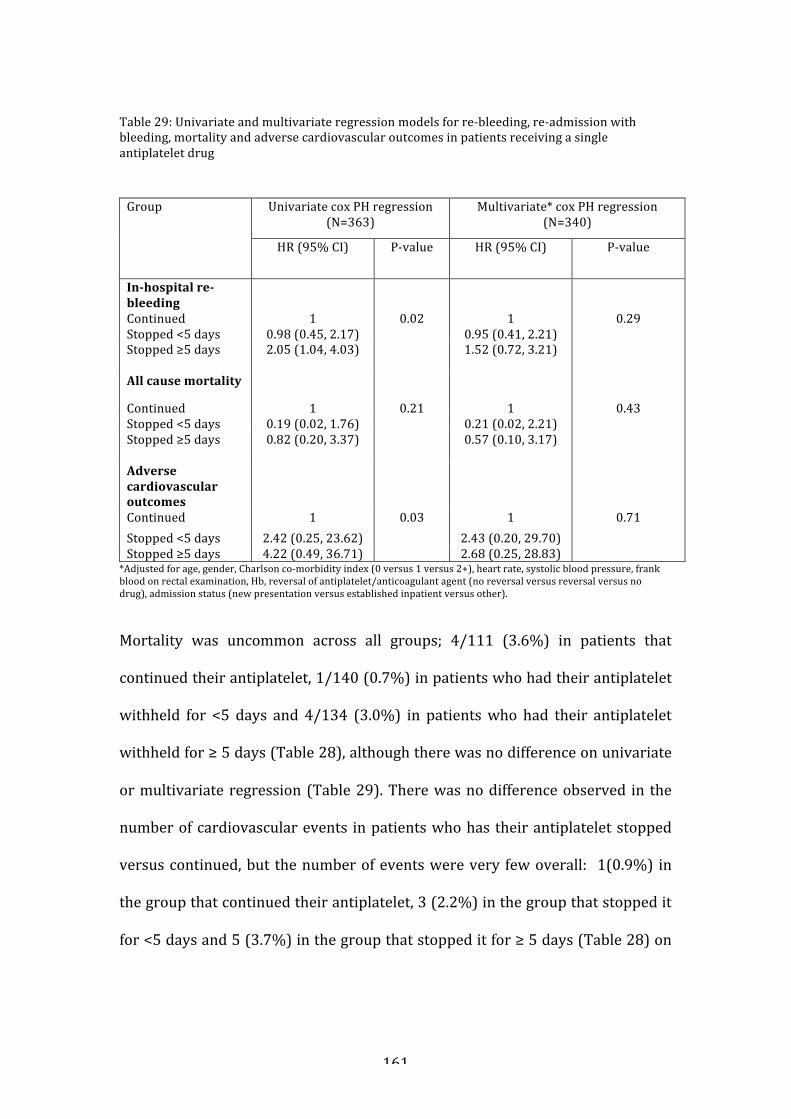
! 161!
!Table!29:!Univariate!and!multivariate!regression!models!for!re<bleeding,!re<admission!with!bleeding,!mortality!and!adverse!cardiovascular!outcomes!in!patients!receiving!a!single!antiplatelet!drug!**Group! Univariate!cox!PH!regression!
(N=363)!Multivariate*!cox!PH!regression!
(N=340)!
HR!(95%!CI)! P<value! HR!(95%!CI)! P<value!
InBhospital*reBbleeding*Continued!
!!1!
!!
0.02!
!!1!
!!
0.29!Stopped!<5!days!! 0.98!(0.45,!2.17)!! ! 0.95!(0.41,!2.21)! !Stopped!≥5!days! 2.05!(1.04,!4.03)! ! 1.52!(0.72,!3.21)! !! ! ! ! !All*cause*mortality* ! ! ! !
Continued! 1! 0.21! 1! 0.43!Stopped!<5!days! 0.19!(0.02,!1.76)!! ! 0.21!(0.02,!2.21)! !Stopped!≥5!days! 0.82!(0.20,!3.37)! ! 0.57!(0.10,!3.17)! !! ! ! ! !Adverse*cardiovascular*outcomes*
! ! ! !
Continued! 1! 0.03! 1! 0.71!Stopped!<5!days! 2.42!(0.25,!23.62)!! ! 2.43!(0.20,!29.70)! !Stopped!≥5!days! 4.22!(0.49,!36.71)!! ! 2.68!(0.25,!28.83)! !
*Adjusted!for!age,!gender,!Charlson!co<morbidity!index!(0!versus!1!versus!2+),!heart!rate,!systolic!blood!pressure,!frank!blood!on!rectal!examination,!Hb,!reversal!of!antiplatelet/anticoagulant!agent!(no!reversal!versus!reversal!versus!no!drug),!admission!status!(new!presentation!versus!established!inpatient!versus!other).!!*Mortality! was! uncommon! across! all! groups;! 4/111! (3.6%)! in! patients! that!
continued!their!antiplatelet,!1/140!(0.7%)!in!patients!who!had!their!antiplatelet!
withheld! for! <5! days! and! 4/134! (3.0%)! in! patients!who! had! their! antiplatelet!
withheld!for!≥!5!days!(Table!28),!although!there!was!no!difference!on!univariate!
or!multivariate!regression!(Table!29).!There!was!no!difference!observed! in! the!
number!of!cardiovascular!events! in!patients!who!has! their!antiplatelet!stopped!
versus!continued,!but! the!number!of!events!were!very! few!overall:! !1(0.9%)! in!
the!group!that!continued!their!antiplatelet,!3!(2.2%)!in!the!group!that!stopped!it!
for!<5!days!and!5!(3.7%)!in!the!group!that!stopped!it!for!≥!5!days!(Table!28)!on!

! 162!
univariate!or!multivariate!regression,!although!the!small!number!of!events!limits!
conclusions!from!this!model!(Table!29).!
!
!
* *

! 163!
7.4*Discussion**
!
To!my!knowledge,!this!is!the!first!study!to!use!a!prospectively!collected!national!
sample! to! describe! the! clinical! course! of! patients! admitted!with! overt! LGIB! in!
relation!to!the!use!of!antiplatelet!or!anticoagulant!medications,!including!DOACs.!
The!key!finding!was!that,!compared!to!patients!not!taking!these!drugs,!patients!
taking!a!single!antiplatelet!agent!had!a!three<fold! increase! in!risk!of! in<hospital!
re<bleeding!and!those!taking!DAPT!had!a!five<fold!increase!in!risk.!This!did!not!
translate! into! an! increased! use! of! interventions! to! treat! bleeding,! or! increased!
risk! of! in<hospital! mortality,! however.! There! was! no! increased! risk! of! re<
bleeding,!need!for!therapeutic! intervention!or!in<hospital!mortality!observed!in!
patients!taking!warfarin!or!DOACs!in!comparison!to!the!control!group.!When!re<
bleeding!did!occur,!most!events!occurred!within!5!days!of! the! index!event!and!
plateaued!after!7!days!of!presentation.!
!
In! Chapter! 6,! although! we! included! use! of! antiplatelet! drugs! in! the! model! to!
develop! the! risk! score,! this! variable!was! not! found! to! be! associated!with! safe!
discharge!(including!negatively).!The!findings!of!the!present!study!are!therefore!!
unexpected.!Using!the!presenting!data!from!the!antiplatelet!groups!it!is!possible!
to!estimate!the!score!of!an!average!single!antiplatelet!patient!and!a!DAPT!patient.!
In!the!single!antiplatelet!group,!a!mean!age!of!77.9!years,!mean!HR!of!82,!mean!
SBP!of!133.7!and!a!mean!Hb!of!116.8!scores!13,!higher!than!the!suggested!score!
of!≥8! for!safe!discharge.!This! is!without! the! inclusion!of! the!sex,!previous!LGIB!
admission! and! DRE! findings! variables.! Using! the! equivalent! mean! data! for! a!
DAPT!patient!also!scores!13.!

! 164!
!
Previous!single!centre!studies!have!demonstrated!that!aspirin!is!associated!with!
an! increased! risk!of!developing!LGIB,16! increased!bleeding! severity13! and! long<
term!recurrence!of!bleeding.103!117!A!previous!study!has!compared! the!effect!of!
withholding! aspirin! after! discharge,! also! finding! that! patients! who! continued!
their!aspirin!post<discharge!experienced!a!three<fold!increase!in!re<bleeding,!but!
importantly!a!1.6<fold!reduction!in!the!risk!of!adverse!cardiovascular!events,!and!
a!three<fold!reduction!in!all<cause!mortality.103!Arguably!a!more!pressing!clinical!
dilemma! is! what! to! do! with! antiplatelet! medications! during! a! patient’s! acute!
admission!with!LGIB.!Clinical!guidelines!state! that! ‘in!patients!with!established!
high!risk!cardiovascular!disease!and!a!history!of!LGIB,!aspirin!used!for!secondary!
prevention!should!not!be!discontinued.’47!The!present!study!is!the!first!study!to!
compare! the! outcomes! of! patients! who! had! their! antiplatelet! drug! withheld!
during! their! hospital! admission! and! the! findings! support! this! guideline!
recommendation:! there! was! no! difference! in! re<bleeding! in! patients! that! had!
their! antiplatelet!withheld! for! less! than! 5! days,! versus! those! that! continued! it.!
These! findings! are! not! unexpected! considering! that! aspirin! and! clopidogrel!
irreversibly! bind! to! platelets,! so! their! effects! are! seen! for! 5<7! days! after!
ingestion.159!160!!!
!
Unlike! the! paper! by! Chan! et! al,! there!were! insufficient! adverse! cardiovascular!
events! to! explore! the! association! between! a! short! interruption! to! antiplatelet!
therapy!and!adverse!outcomes.!This!is!likely!due!to!the!short!follow!up!period!in!
the! present! study,! where! the! median! length! of! stay! was! 3<4! days.! In! UGIB,! a!
small,!single!centre!RCT!found!a!large!increase!in!cardiovascular!risk!with!even!a!

! 165!
short<term! interruption! to!antiplatelet! therapy.156!However,! a! randomised! trial!
of!4000!high!risk!cardiovascular!patients!undergoing!non<cardiac!surgery!found!
that! in! comparison! to! placebo,! peri<operative! aspirin! did! not! prevent! MI.161!
Given! the! potential! risk! of! adverse! cardiovascular! events! and! the! lack! of!
increased!risk!of!haemorrhage!related!death,!we!find!no!benefit! in! interrupting!
antiplatelet!drugs!in!the!short<term!in!LGIB.$This!represents!a!change!in!practice,!
as! in! the! current! national! study,! antiplatelet! drugs! were! withheld! in! >70%!
patients,!despite!guideline!recommendations.!!
!
!
In!some!patients!with!LGIB!there!may!be!a!need!to!withhold!antiplatelet!drugs,!
such!as! those!undergoing! emergency!procedures!or! surgery.!Guidelines!on! the!
management!of!antiplatelets!in!patients!undergoing!emergency!surgery!suggest!
the!use!of!tranexamic!acid,!and!if!there!is!excessive!bleeding!despite!this,!platelet!
transfusion!can!be!considered.162!Currently!these!recommendations!are!based!on!
non<randomised! data,! but! the! HALT<IT! trial163! will! assess! the! benefit! of!
tranexamic!acid!in!GI!bleeding!and!will!provide!the!first!randomised!evidence!for!
its!use!in!LGIB.!Evidence!supporting!platelet!transfusion!originates!from!a!pilot!
study!of! patients! undergoing! surgery.164! In! contrast,! a! case<control! study!of!GI!
bleeding! (including! 161! cases! LGIB)! found! that! platelet! transfusion! did! not!
improve! clinical! outcomes.154! These! findings! are! consistent! with! other!
therapeutic! areas! such! as! intra<cranial! bleeding.165! Antidotes! for! specific!
antiplatelet!drugs!are!also!being!developed!and!vasopressin!analogues!may!also!
have!a!role.166!
!

! 166!
The!risks!of! severe!bleeding!associated!with!novel!anticoagulant!drugs! in!LGIB!
have!been!demonstrated! in! administrative!databases.8!12! In! this! study,!patients!
receiving! DOACs! had! a! lower! presenting! Hb! concentration,! although!were! not!
more! likely! to! be! shocked,! require! haemostatic! intervention! or! develop! re<
bleeding.!Most!patients! receiving!DOACs!were!managed!by! simply!withholding!
the!drug!and!this!raises!questions!as!to!whether!antidotes!would!have!a!role!in!
this! setting.! Additionally,! as! most! patients! had! their! DOAC! withheld,! the! risk!
associated!with!their!continuation!is!unknown.!!
!
There! are! conflicting! reports! on! the! risks! of! LGIB! with! warfarin,! with! some!
studies! indicating! an! association!between!warfarin<use! and!bleeding! severity16!
167!and!others!finding!no!such!association.69!In!comparison!to!the!control!group,!
we!found!no!increased!risk!of!shock,!RBC!transfusion!or!re<bleeding.!The!current!
study!has!a!much!larger!sample!of!patients!taking!warfarin!than!previous!studies!
and! is! sufficiently! large! to! report! on!mortality,! finding! no! increased! risk! with!
warfarin!use.!These!findings!may!be!in!part!be!explained!by!the!relative!ease!of!
warfarin<reversal!with!vitamin!K!or!PCC,!which!was!used!in!over!40%!patients.!!
!
Strengths!of!the!study!include!its!size!and!prospective!data!collection!by!clinical!
teams.! Previous! large! studies! of! LGIB! have! used! administrative! databases! or!
colonoscopy! referrals! to! identify! cases,8!13!117! but! this! is! has! limited! efficacy! in!
LGIB,!as!codes!for!some!frequent!causes!of!LGIB!such!as!diverticular!bleeding!are!
not!widely!used,! and!most!patients!do!not!undergo! colonoscopy.131!The!use!of!
contemporaneous!medical! records!allowed! the!collection!of!detailed!data,! such!
! 167!
as! the! mode! and! timing! of! drug! reversal.! This! allowed! us! to! include! this!
important!variable!in!the!regression!models!used!in!this!study.!
!
There! are! several! limitations! to! this! study.! As! the! data! derive! from! an!
observational! study,! any! associations! are! susceptible! to! confounding,!
particularly! comparisons!between!groups!of!patients! that!had!drugs! continued!
or! withheld.! In! the! analysis! of! continuing! or! withholding! single! antiplatelets,!
rates!of! re<bleeding!may!have!been!higher! in! the!group! that!withheld! the!drug!
for!five!days!or!more!as!patients!were!followed!up!for!longer!than!those!that!had!
it!withheld! for!<5!days.! Further! studies!may!need! to!analyse! this! variable! as! a!
time<varying! covariate.! The! definition! of! the!main! outcome! re5bleeding,#used! a!
period! of! 24! hours! to! identify! a! recurrent! bleeding! event.! This!means! that! re<
bleeding! that! occurred! within! 24! hours! of! admission! may! not! have! been!
captured,! underestimating! the! frequency! of! severe! bleeding.! Mortality! data!
corresponded! to! the! entire! admission! though,!which!was!no!different!between!
drug!groups,!even! if! there!may!have!been!differences! in!severe!bleeding! in! the!
first! 24! hours! of! admission.! Missing! data! accounted! for! 23.7%! of! the! re<
admission!with!further!bleeding!outcome,!so!re<admission!rates!may!actually!be!
higher! than! reported! in! this! study.! Patients!were! identified! as! having! LGIB! by!
clinicians,! using! presenting! features,! but! only! 52%! in! the! original! study!
underwent! inpatient! investigation! of! the! source! of! bleeding.! It! is! therefore!
possible!that!a!proportion!of!the!remaining!patients!may!not!have!had!true!LGIB.!
Additionally,! it! is! not! possible! to! tell! whether! patients! who! experienced! re<
bleeding! bled! from! the! initial! lesion! or! from! a! difference! lesion.! This! is!
particularly!relevant!to!diverticular!bleeding,!which!was!the!most!common!cause!

! 168!
of!LGIB! in! this!study.!We!were!able! to!compare!outcomes!of!patients! receiving!
single! antiplatelet! therapy! who! discontinued! or! continued! the! drug,! but! not!
patients!who!were! receiving!DAPT,! as! the! total! number! of! the! latter!were! too!
few.!This!remains!a!key!area!for!further!research.!Additional!studies!should!aim!
to!determine!factors!that! influence!the!decision!to!withhold!antiplatelet!agents,!
such! as! type! and! timing! of! previous! ischaemic! events! to! further! explore! the!
rationale!for!continuing!or!withholding!these!drugs.!
!
In! summary! this! is! the! first! prospectively! designed! study! to! compare! the!
outcomes! of! patients! taking! antiplatelet! drugs! or! anticoagulants! at! the! time! of!
presentation! with! LGIB.! We! have! identified! that! patients! taking! antiplatelets!
have! the! greatest! risk! of! re<bleeding,! and! demonstrated! that! withholding! the!
drug! has! no! impact! on! rates! of! re<bleeding! and! may! expose! the! patient! to!
unnecessary!cardiovascular!risk.!When!triaging!LGIB!patients!the!increased!risk!
of! re<bleeding!with! antiplatelet! drugs!may!need! to! be! anticipated! and!patients!
managed! accordingly.! This! may! consist! of! having! a! lower! threshold! for!
investigation,! haemostatic! intervention! or! a! longer! period! of! observation! in!
hospital.!!
!
!
!
!******
! 169!
CHAPTER*8:*CONCLUSIONS**!
This! project! provides! the! first! national,! epidemiological! data! on! LGIB! in! a! UK!
population.!These!LGIB!data!provide!a!unique!basis!to!identify!trends!in!patient!
demographics,! presenting! features! and! outcomes,! which! has! implications! for!
organisational! level! services! as!well! as! individual! clinicians!managing! patients!
with!LGIB.!!
!
The! systematic! review! appraised! and! pooled! the! best! available! evidence! on!
modes!of!diagnostic!and!therapeutic!intervention.!Although!evidence!from!RCTs!
is! lacking,! the! systematic! review! identified! that! the! greatest! evidence! base!
related!to!colonoscopy!and!that!access!to!early!colonoscopy!may!have!benefits!to!
patients.!The!review!of!existing!service!organisation!demonstrated!which!areas!
of!care!are!currently!deficient!in!the!NHS.!The!size!of!the!LGIB!patient!database!
enabled!detailed!analysis!of!patient!risk! factors! for!adverse!outcomes,!allowing!
the!development!of!a!risk!score!to!aid!patient!triage!at!initial!assessment.!For!the!
first!time,!patients!can!be!reliably!identified!as!suitable!for!immediate!discharge!
and!outpatient!management,!with!associated!benefits!to!the!patient!and!the!NHS.!!
!
In!the!UK,!the!typical!LGIB!patient!is!elderly!and!co<morbid!illness!is!a!frequent!
finding.! The! challenge! in!managing! these! patients! lies! not!with! the! severity! of!
haemorrhage,! but! with! the! complex! interaction! with! their! co<existing! medical!
problems!and!medications.!Previous!population!based!studies!have!also!found!a!
high! burden! of! co<morbidity8! but! the! proportion! of! patients! developing! LGIB!
whilst!receiving!antiplatelets!(26.1%)!or!oral!anticoagulants!(15.9%)!was!higher!

! 170!
than!found!in!recent!previous!studies;!20.5<23.2%!and!5.7<11.4%,!respectively.69!
70!This!difference!is!possibly!accounted!for!by!the!timing!of!data!capture!between!
these!two!studies!and!the!current!study;!Sengupta!et#al!collected!data!from!2008<
2015,!Aoki!et#al!2009<2015.!This!reflects!the!trend!towards!increased!aspirin!and!
anticoagulant! prescriptions! particularly! in! the! elderly! population.168! 169! Data!
from! the!observational! study! (Chapter!4)! suggested! that!patients!who!develop!
LGIB!whilst!taking!aspirin!have!higher!rates!of!re<bleeding,!and!that!re<bleeding!
may! be! a! risk! factor! for! in<hospital!mortality.! This!was! further! investigated! in!
Chapter!7,!demonstrating!an!association!between!single!antiplatelet!and!DAPT<
use! and! re<bleeding! when! potential! confounders! were! controlled! for.!
Retrospective! studies! have! also! demonstrated! an! association! between! aspirin!
and! immediate13! and! long<term! re<bleeding! in! LGIB.103!However,! there!was!no!
association! between! antiplatelet! use! and! mortality! in! the! regression! analysis.!
Additionally!antiplatelet<use!does!not!appear!in!the!risk!score.!This!may!be!due!
to!an!association!between!antiplatelets!and!other!variables!that!are!included!in!
the!risk!score,!such!as!abnormal!vital!signs,!although!there!was!no!difference!in!
the! proportion! of! shocked! patients! between! the! antiplatelet! and! anticoagulant!
groups,!and!the!control!group!in!Chapter!7.!!
!
In!patients! taking!antiplatelet!medications,! it! is!plausible! that! in!comparison!to!
adverse! cardiovascular! events,! re<bleeding! is! not! an! important! determinant! of!
outcome.! Chan! et#al#conducted! a! retrospective! study! of! 295! aspirin<users!who!
developed! LGIB103! grouping! patients! into! those! that! discontinued! aspirin! on!
discharge! and! those! who! continued! it.! The! latter! group! experienced! more!
episodes! of! re<bleeding,! but! fewer! adverse! cardiovascular! events! and! deaths!

! 171!
over!5!years.!Although!the!study!reported!in!this!thesis!is!larger,!I!was!unable!to!
demonstrate! an! association! between! withholding! aspirin! during! the! index!
admission!and!adverse!cardiovascular!outcomes!because! the!number!of!events!
was!too!small,!possibly!due!to!the!short!period!of!follow!up.!Despite!this,!(and!in!
keeping!with!the!study!by!Chan!et#al),!the!conclusion!was!that!antiplatelet!drugs!
should!not!be!withheld!during!an!acute!admission!with!LGIB.!This!is!at!odds!with!
current! guideline! recommendations! that! imply! that! antiplatelets! should! be!
withheld,! stating! that! ‘non<aspirin! antiplatelet! therapy! should! be! resumed! as!
soon!as!possible!and!at!least!within!7!days.’47!However,!the!findings!of!the!study!
reported!in!this!thesis!are!limited!by!its!design;!prospective!observational!study.!
An!RCT!randomising!patients! to!continue!or! interrupt! their!antiplatelet!drug! is!
required!to!fully!address!this!question.!!
!
The! descriptive! data! on! the! outcomes! of! patients! taking! anticoagulants! is! an!
important! addition! to! the! evidence<base! surrounding! the! effect! of! these! drugs!
(including!DOACs)!on!GIB.!Previous!studies!were!small!and!often!did!not!capture!
enough!detail! regarding! the! type!and! timing!of! cardiovascular! events!or!major!
bleeds.!The!recent!multicentre!COMPASS!trial!randomised!27,395!patients!with!
stable!atherosclerotic!disease!to!aspirin!alone,!rivaroxaban!alone!or!combination!
therapy.170! In! comparison! to! aspirin! alone,! patients! treated! with! aspirin! plus!
rivaroxaban!had!a!24%!reduction! in! rates!of! cardiovascular! events,! but! a!70%!
increase!in!rates!of!major!bleeding.!The!leading!site!of!bleeding!was!the!GI!tract.!
If! this!study!does! lead!to!a!change!in!practice,!physicians!may!see!a!substantial!
increase!in!the!volume!of!drug<associated!LGIB.!!
!

! 172!
A!key!finding!from!the!observational!study!was!the!lack!of!intervention!in!most!
patients.!The!most!frequent!investigation!was!flexible!sigmoidoscopy,!performed!
in!21.5%!cases,!whereas!colonoscopy!was!performed!in!only!3.9%.!This!pattern!
of!investigation!is!at!odds!with!the!published!evidence!in!the!systematic!review!
(Chapter!2);!no!studies!comparing!flexible!sigmoidoscopy,!whereas!colonoscopy!
was!the!intervention!with!the!most!evidence.!This!may!be!because!most!studies!
originated!in!the!US,!where!colonoscopy!is!favoured!over!flexible!sigmoidoscopy.!
In! the! observational! study,! patients! waited! a! median! of! 4! days! for! their!
colonoscopy,!and!only!14%!patients!undergoing!colonoscopy!had!the!procedure!
within!24!hours.!Although!guidelines!recommend!that!‘in!patients!with!high<risk!
clinical! features! and! signs! or! symptoms! of! on<going! bleeding,! a! rapid! bowel!
purge! should! be! initiated! following! hemodynamic! resuscitation,! and! a!
colonoscopy!performed!within!24!h!of!patient!presentation,’47!evidence!from!the!
systematic! review! found! no! difference! in! important! clinical! outcomes! (re<
bleeding!or!RBC!transfusion)!between!early!and!late!colonoscopy.!The!guideline!
recommendations! may! therefore! not! be! justified,! although! results! of! the!
systematic!review!are!limited!by!the!quality!of!evidence!available!on!this!topic.!!
!
In! total! 48%!patients! admitted!with! LGIB! in! the! observational! study!were! not!
investigated! as! an! inpatient,! and! only! a! small! minority! of! patients! received!
endoscopic,! radiological! or! surgical! treatment.! Overall! mortality! was! low,! at!
3.4%.!The!group!of!non<investigated!patients!received!fewer!blood!transfusions!
and!there!was!no!difference!in!in<hospital!mortality!or!re<admission!with!further!
bleeding!in!comparison!to!the!group!that!were!investigated,!suggesting!that!they!
did!not!come!to!harm!(although!this!may!be!confounded!by!indication).!The!low!
! 173!
frequency! of! intervention! questions! the! rationale! for! patient! admission.! This!
finding!changed!the!initial!focus!of!the!risk!score!from!the!prediction!of!adverse!
outcomes,! to! the! identification!of! patients! that! could! safely! avoid! admission! in!
favour! of! outpatient! investigation! (Chapter! 6).! This! strategy! differs! from!
previous!attempts!by!other!groups!at!designing!a!risk!score!for!LGIB,!which!have!
aimed! to! predict! severe! haemorrhage,! complications! and! death.13! 68<70! 140! The!
clinical!usefulness!of!these!scores!is!limited!by!the!infrequency!of!the!events!they!
seek! to! identify! and! they! give! little! prognostic! information! on! the!majority! of!
patients!who!will!not!come!to!harm.!!
!
The!new!risk!score!aims!to!identify!the!large!group!of!patients!with!a!remote!risk!
intervention!or!adverse!events.!The! frequency!of!patients!who!met! the!criteria!
for!safe!discharge!was!unexpected;!68%!in!the!development!cohort!and!64%!in!
the!validation!cohort.!The!widespread!use!of!this!risk!score!has!the!potential!to!
transform! the!management! of! patients! admitted!with! LGIB.! In! the! preliminary!
paper!arising! from!Chapter!6171! it! is! recommended!that!a!score!of!≤8!points!at!
initial!assessment!can!be!used!as!the!threshold!for!hospital!discharge,!as!this!is!
associated!with!a!95%!chance!of! safe!discharge.!However,!only!11.9%!patients!
who!met! the!criteria! for!safe!discharge!scored!≤8!points.!Although! the!score! is!
externally! validated,! it! is! yet! to! be! validated! in! healthcare! systems!beyond! the!
UK,! and! in! populations! outside! of! study! conditions.!With! this! consideration! in!
mind,! a! conservative!points! threshold!was! selected! to!maximise!patient! safety,!
but! it! sacrificed! the! volume! of! patients! that! could! otherwise! be! discharged.!
Further!studies!may!demonstrate!that!higher!points!thresholds!are!safe,!in!which!
case!a!greater!proportion!of!patients!may!be! identified!by! the!score!as!safe! for!

! 174!
outpatient! management.! The! observational! study! may! serve! as! a! comparison!
dataset!for!rates!of!admission,!inpatient!and!outpatient!investigation,!should!the!
score!be!widely!adopted.!!
!
Increasing! the! outpatient! management! of! LGIB! patients! has! important!
considerations.!The!systematic!review!was!designed!to!include!all!studies!on!the!
timing! of! investigation,! but! we! found! only! studies! that! compared! inpatient!
elective! colonoscopy! with! that! performed! within! 24! hours.! There! were! no!
studies! examining! the! optimum! timing! of! outpatient! investigation.! The!
observational! study! demonstrated! that! 70%! of! outpatient! endoscopies! were!
scheduled!to!be!performed!more!than!two!weeks!post<discharge.!Whether!this!is!
adequate! requires! further! study,! but! it! is! plausible! that! many! stigmata! of!
haemorrhage! may! have! disappeared! by! this! time.! If! the! colonoscopy! is! being!
performed! for! the! diagnosis! of! cancer,! NICE! recommends! that! endoscopy! is!
performed!within!two!weeks.118!
!
Reducing!the!number!of!patients!admitted!with!LGIB!is!likely!to!have!a!beneficial!
impact! on! inpatient! resources,! but! the! trade<off! is! increased! demand! on!
outpatient! resources.! The! study! of! the! organisation! of! services! (Chapter! 5)!
identified! that! 24/7! inpatient! lower! GI! endoscopy! was! available! in! 75%!
hospitals.!Additionally! there!was!a!deficit! in!endoscopists’! skills!with!regard! to!
the!ability!to!provide!therapy!at!colonoscopy.!The!current!volume!of!referrals!for!
outpatient!endoscopy!is!unknown!and!the!gap!in!endotherapy!skills!is!also!likely!
to! apply! in! the! outpatient! setting.! Quantifying! the! potential! increased! demand!

! 175!
associated!with!more! outpatient<based! care! requires! detailed! health! economic!
analysis.!
!
The! risk! score! can! also! be! used! to! predict! need! for! RBC! transfusion! and! re<
bleeding.! The! systematic! review! was! unable! to! identify! which! interventions!
reduced!these!outcomes!though;! there!was!no!difference! in!re<bleeding!or!RBC!
transfusion!with!colonoscopy!versus!CTA,!and!there!were!no!studies!comparing!
the!efficacy!of!endotherapy!with!that!of!mesenteric!embolisation.!The!optimum!
management! approach! to! patients! that! do! require! admission! remains! unclear!
therefore,!and!greatly!hindered!by!the!lack!of!evidence!in!this!area.!
!
Although!adverse!events!were!uncommon,! the!observational! study!did! identify!
that!patients!who!developed!LGIB!as!an!established!inpatient!were!at!increased!
risk.!During!hospital!admission,!17.9%!of!these!patients!died,!versus!2.2%!of!the!
de!novo!admissions!with!LGIB.!This!group!represents!an!opportunity!to!improve!
outcomes.! In! comparison! to! new! admissions,! the! inpatient! bleeds! were! older!
with! more! co<morbid! illness.! Early! assessment! by! the! medical! team! that!
normally!treats!GIB!and!involvement!of!Care!of!the!Elderly!physicians!may!help!
optimise!these!patients!and!initiate!prompt!minimally!invasive!treatment!where!
appropriate.!!
!
Suggestions*for*Future*Work*
The!risk!score!model!indicated!that!patients!scoring!≤8!points!on!the!risk!score!
can! be! safely! discharged.! Future! work! should! aim! to! address! the! question! of!
further!management.! NICE! recommends! performing! a! colonoscopy!within! two!

! 176!
weeks! for! patients! aged! over! 50! with! unexplained! rectal! bleeding.118! The!
national!bowel! cancer! screening!programme!reports!a! cancer!detection! rate!of!
7.8<11.6%.172! By! definition! LGIB! patients! already! have! a! potential! symptom!of!
cancer,! so! the! detection! rate! may! be! higher.! A! large! observational! study!
reporting! the!diagnostic! yield!of!outpatient! colonoscopy! could!provide!data!on!
the!utility! of! this! investigation! in!LGIB.!These!data! could!be!used! to! inform!an!
RCT,! randomising! patients! to! colonoscopy! within! two! weeks,! or! colonoscopy!
beyond!this!(current!practice).!In!younger!patients!with!a!low!risk!of!cancer,!this!
could! be! a! non<inferiority! trial,! comparing! no! investigation! or! flexible!
sigmoidoscopy!with!outpatient!colonoscopy.!!
!
Patients!who!score!>8!may!benefit! from!hospital!admission,!although!currently!
there! are! no! RCTs! comparing! CTA! with! colonoscopy! or! endotherapy! with!
embolisation.! These! are! both! required.! Chapter! 5! identified! deficiencies! in! the!
provision! of! all! of! these! interventions,! requiring! considerable! investment! in!
services,!which!will!require!clinical!justification.!!
!
Lastly,!the!area!of!work!that!is!most!likely!to!see!immediate!benefit!to!patients!is!
the!publication!and!adoption!of!a!national!guideline!on!the!management!of!LGIB.!
This! will! allow! standardisation! of! management! between! hospitals! and! also!
clearly!define!what! is!expected!with!regard!to!the!availability!of!care.!Although!
the!evidence!base!supporting!optimal!care! is!poor,! there!are!groups!of!patients!
where! improvements! can! be! made,! as! identified! in! this! thesis.! These! groups!
include!patients!with!severe!bleeding!who!may!benefit!from!improved!access!to!
IR! or! interventional! colonoscopy,! patients! who! develop! LGIB! whilst! receiving!

! 177!
antiplatelet! or! anticoagulant! drugs,! and! patients! who! develop! bleeding! as! an!
inpatient.! This! guideline! is! currently! being! developed! by! the!British! Society! of!
Gastroenterology!and!is!expected!to!be!completed!in!2018.!
!
In!summary,!this!thesis!describes!the!management!of!LGIB!patients!in!the!UK!in!
an! unprecedented! number.! The! observational! study! is! also! one! of! the! largest!
epidemiological! studies!of!LGIB!worldwide.!Although! its!aims!were! to! improve!
the! inpatient! management! of! these! patients! by! identifying! the! optimum!
approach! to! management! and! therapy,! and! designing! a! risk! score! to! predict!
adverse!outcomes,!the!paucity!of!evidence!for!the!optimum!management!meant!
that! identifying! patients! at! low! risk! of! harm! had! greater! clinical! value.! By!
reducing! the! number! of! hospital! admissions! with! LGIB,! clinicians! can! focus!
resources! on! the! small! group! of! patients! who! will! benefit! from! inpatient!
investigation!and!treatment.!!

! 178!
References**1.!National!Institute!for!Health!and!Care!Excellence.!Clinical!Guideline!141.!Acute!
upper!gastrointestinal!bleeding!in!over!16s.!2012.!2.!Lanas!A,!Garcia<Rodriguez!LA,!Polo<Tomas!M,!et!al.!Time!trends!and!impact!of!
upper!and!lower!gastrointestinal!bleeding!and!perforation!in!clinical!practice.!The!American!journal!of!gastroenterology!2009;104(7):1633<41.!
3.!Tinegate!H,!Pendry!K,!Murphy!M,!et!al.!Where!do!all!the!red!blood!cells!(RBCs)!go?!Results!of!a!survey!of!RBC!use!in!England!and!North!Wales!in!2014.!Transfusion!2016;56(1):139<45.!
4.!Hoedema!RE,!Luchtefeld!MA.!The!management!of!lower!gastrointestinal!hemorrhage.!Diseases!of!the!colon!and!rectum!2005;48(11):2010<24.!
5.!Soares!DN,!Kheng<Seong;!Nassar,!Natasha;!Gladman,!Marc.!Incidence!and!Outcomes!of!Patients!Presenting!to!the!Emergency!Department!With!Acute!Lower!Gastrointestinal!Hemorrhage.!Gastroenterology!2013;144(5):S<783.!
6.!National!Confidential!Enquiry!into!Patient!Outcomes!and!Death!(NCEPOD).!Time!to!get!control?!A!review!of!the!care!received!by!patients!who!had!a!severe!gastrointestinal!haemorrhage.!2015.!
7.!Raju!GS,!Gerson!L,!Das!A,!et!al.!American!Gastroenterological!Association!(AGA)!Institute!technical!review!on!obscure!gastrointestinal!bleeding.!Gastroenterology!2007;133(5):1697<717.!
8.!Hreinsson!JP,!Gumundsson!S,!Kalaitzakis!E,!et!al.!Lower!gastrointestinal!bleeding:!incidence,!etiology,!and!outcomes!in!a!population<based!setting.!European!journal!of!gastroenterology!&!hepatology!2013;25(1):37<43.!
9.!Longstreth!GF.!Epidemiology!and!outcome!of!patients!hospitalized!with!acute!lower!gastrointestinal!hemorrhage:!a!population<based!study.!The!American!journal!of!gastroenterology!1997;92(3):419<24.!
10.!Williams!JG,!Roberts!SE,!Ali!MF,!et!al.!Gastroenterology!services!in!the!UK.!The!burden!of!disease,!and!the!organisation!and!delivery!of!services!for!gastrointestinal!and!liver!disorders:!a!review!of!the!evidence.!Gut!2007;56*Suppl*1:1<113.!
11.!Newman!J,!Fitzgerald!JE,!Gupta!S,!et!al.!Outcome!predictors!in!acute!surgical!admissions!for!lower!gastrointestinal!bleeding.!Colorectal!disease!:!the!official!journal!of!the!Association!of!Coloproctology!of!Great!Britain!and!Ireland!2012;14(8):1020<6.!
12.!Strate!LL,!Ayanian!JZ,!Kotler!G,!et!al.!Risk!factors!for!mortality!in!lower!intestinal!bleeding.!Clinical!gastroenterology!and!hepatology!:!the!official!clinical!practice!journal!of!the!American!Gastroenterological!Association!2008;6(9):1004<10;!quiz!955<.!
13.!Strate!LL,!Orav!EJ,!Syngal!S.!Early!predictors!of!severity!in!acute!lower!intestinal!tract!bleeding.!Archives!of!internal!medicine!2003;163(7):838<43.!
14.!Nagata!N,!Niikura!R,!Aoki!T,!et!al.!Colonic!diverticular!hemorrhage!associated!with!the!use!of!nonsteroidal!anti<inflammatory!drugs,!low<dose!aspirin,!antiplatelet!drugs,!and!dual!therapy.!Journal!of!gastroenterology!and!hepatology!2014;29(10):1786<93.!
! 179!
15.!Chang!CH,!Lin!JW,!Chen!HC,!et!al.!Non<steroidal!anti<inflammatory!drugs!and!risk!of!lower!gastrointestinal!adverse!events:!a!nationwide!study!in!Taiwan.!Gut!2011;60(10):1372<8.!
16.!Hreinsson!JP,!Palsdottir!S,!Bjornsson!ES.!The!Association!of!Drugs!With!Severity!and!Specific!Causes!of!Acute!Lower!Gastrointestinal!Bleeding:!A!Prospective!Study.!Journal!of!clinical!gastroenterology!2016;50(5):408<13.!
17.!Tanaka!A,!Hase!S,!Miyazawa!T,!et!al.!Up<regulation!of!cyclooxygenase<2!by!inhibition!of!cyclooxygenase<1:!a!key!to!nonsteroidal!anti<inflammatory!drug<induced!intestinal!damage.!The!Journal!of!pharmacology!and!experimental!therapeutics!2002;300(3):754<61.!
18.!Somasundaram!S,!Sigthorsson!G,!Simpson!RJ,!et!al.!Uncoupling!of!intestinal!mitochondrial!oxidative!phosphorylation!and!inhibition!of!cyclooxygenase!are!required!for!the!development!of!NSAID<enteropathy!in!the!rat.!Alimentary!pharmacology!&!therapeutics!2000;14(5):639<50.!
19.!Washio!E,!Esaki!M,!Maehata!Y,!et!al.!Proton!Pump!Inhibitors!Increase!Incidence!of!Nonsteroidal!Anti<Inflammatory!Drug<Induced!Small!Bowel!Injury:!A!Randomized,!Placebo<Controlled!Trial.!Clinical!gastroenterology!and!hepatology!:!the!official!clinical!practice!journal!of!the!American!Gastroenterological!Association!2016;14(6):809<15.e1.!
20.!Endo!H,!Sakai!E,!Taniguchi!L,!et!al.!Risk!factors!for!small<bowel!mucosal!breaks!in!chronic!low<dose!aspirin!users:!data!from!a!prospective!multicenter!capsule!endoscopy!registry.!Gastrointestinal!endoscopy!2014;80(5):826<34.!
21.!Reuter!BK,!Davies!NM,!Wallace!JL.!Nonsteroidal!anti<inflammatory!drug!enteropathy!in!rats:!role!of!permeability,!bacteria,!and!enterohepatic!circulation.!Gastroenterology!1997;112(1):109<17.!
22.!Lanas!A,!Carrera<Lasfuentes!P,!Arguedas!Y,!et!al.!Risk!of!upper!and!lower!gastrointestinal!bleeding!in!patients!taking!nonsteroidal!anti<inflammatory!drugs,!antiplatelet!agents,!or!anticoagulants.!Clinical!gastroenterology!and!hepatology!:!the!official!clinical!practice!journal!of!the!American!Gastroenterological!Association!2015;13(5):906<12.e2.!
23.!Patel!MR,!Mahaffey!KW,!Garg!J,!et!al.!Rivaroxaban!versus!warfarin!in!nonvalvular!atrial!fibrillation.!The!New!England!journal!of!medicine!2011;365(10):883<91.!
24.!Eikelboom!JW,!Wallentin!L,!Connolly!SJ,!et!al.!Risk!of!bleeding!with!2!doses!of!dabigatran!compared!with!warfarin!in!older!and!younger!patients!with!atrial!fibrillation:!an!analysis!of!the!randomized!evaluation!of!long<term!anticoagulant!therapy!(RE<LY)!trial.!Circulation!2011;123(21):2363<72.!
25.!Heidbuchel!H,!Verhamme!P,!Alings!M,!et!al.!Updated!European!Heart!Rhythm!Association!Practical!Guide!on!the!use!of!non<vitamin!K!antagonist!anticoagulants!in!patients!with!non<valvular!atrial!fibrillation.!Europace!:!European!pacing,!arrhythmias,!and!cardiac!electrophysiology!:!journal!of!the!working!groups!on!cardiac!pacing,!arrhythmias,!and!cardiac!cellular!electrophysiology!of!the!European!Society!of!Cardiology!2015;17(10):1467<507.!
26.!Peng!YL,!Hu!HY,!Luo!JC,!et!al.!Alendronate,!a!bisphosphonate,!increased!upper!and!lower!gastrointestinal!bleeding:!risk!factor!analysis!from!a!nationwide!population<based!study.!Osteoporosis!international!:!a!journal!
! 180!
established!as!result!of!cooperation!between!the!European!Foundation!for!Osteoporosis!and!the!National!Osteoporosis!Foundation!of!the!USA!2014;25(5):1617<23.!
27.!Cheng!YL,!Hu!HY,!Lin!XH,!et!al.!Use!of!SSRI,!But!Not!SNRI,!Increased!Upper!and!Lower!Gastrointestinal!Bleeding:!A!Nationwide!Population<Based!Cohort!Study!in!Taiwan.!Medicine!2015;94(46):e2022.!
28.!Carson!JL,!Stanworth!SJ,!Roubinian!N,!et!al.!Transfusion!thresholds!and!other!strategies!for!guiding!allogeneic!red!blood!cell!transfusion.!The!Cochrane!database!of!systematic!reviews!2016;10:Cd002042.!
29.!Hebert!PC,!Wells!G,!Blajchman!MA,!et!al.!A!multicenter,!randomized,!controlled!clinical!trial!of!transfusion!requirements!in!critical!care.!Transfusion!Requirements!in!Critical!Care!Investigators,!Canadian!Critical!Care!Trials!Group.!The!New!England!journal!of!medicine!1999;340(6):409<17.!
30.!National!Institute!for!Health!and!Care!Excellence.!NICE!Guideline!NG24!<!Transfusion!2015.!
31.!Villarejo!F,!Rizzolo!M,!Lopez!E,!et!al.![Acute!anemia!in!high!digestive!hemorrhage.!Margins!of!security!for!their!handling!without!transfusion!of!red!globules].!Acta!gastroenterologica!Latinoamericana!1999;29(4):261<70.!
32.!Villanueva!C,!Colomo!A,!Bosch!A,!et!al.!Transfusion!strategies!for!acute!upper!gastrointestinal!bleeding.!The!New!England!journal!of!medicine!2013;368(1):11<21.!
33.!Hearnshaw!SA,!Logan!RF,!Lowe!D,!et!al.!Acute!upper!gastrointestinal!bleeding!in!the!UK:!patient!characteristics,!diagnoses!and!outcomes!in!the!2007!UK!audit.!Gut!2011;60(10):1327<35.!
34.!Jairath!V,!Kahan!BC,!Gray!A,!et!al.!Restrictive!versus!liberal!blood!transfusion!for!acute!upper!gastrointestinal!bleeding!(TRIGGER):!a!pragmatic,!open<label,!cluster!randomised!feasibility!trial.!Lancet!(London,!England)!2015;386(9989):137<44.!
35.!Murphy!GJ,!Pike!K,!Rogers!CA,!et!al.!Liberal!or!restrictive!transfusion!after!cardiac!surgery.!The!New!England!journal!of!medicine!2015;372(11):997<1008.!
36.!Docherty!AB,!O'Donnell!R,!Brunskill!S,!et!al.!Effect!of!restrictive!versus!liberal!transfusion!strategies!on!outcomes!in!patients!with!cardiovascular!disease!in!a!non<cardiac!surgery!setting:!systematic!review!and!meta<analysis.!BMJ!(Clinical!research!ed)!2016;352:i1351.!
37.!Cardin!F,!Andreotti!A,!Martella!B,!et!al.!Current!practice!in!colonoscopy!in!the!elderly.!Aging!clinical!and!experimental!research!2012;24(3!Suppl):9<13.!
38.!Kaltenbach!T,!Watson!R,!Shah!J,!et!al.!Colonoscopy!with!clipping!is!useful!in!the!diagnosis!and!treatment!of!diverticular!bleeding.!Clinical!gastroenterology!and!hepatology!:!the!official!clinical!practice!journal!of!the!American!Gastroenterological!Association!2012;10(2):131<7.!
39.!Ishii!N,!Setoyama!T,!Deshpande!GA,!et!al.!Endoscopic!band!ligation!for!colonic!diverticular!hemorrhage.!Gastrointestinal!endoscopy!2012;75(2):382<7.!
40.!Kwan!V,!Bourke!MJ,!Williams!SJ,!et!al.!Argon!plasma!coagulation!in!the!management!of!symptomatic!gastrointestinal!vascular!lesions:!experience!in!100!consecutive!patients!with!long<term!follow<up.!The!American!journal!of!gastroenterology!2006;101(1):58<63.!

! 181!
41.!Huang!R,!Pan!Y,!Hui!N,!et!al.!Polysaccharide!hemostatic!system!for!hemostasis!management!in!colorectal!endoscopic!mucosal!resection.!Digestive!endoscopy!:!official!journal!of!the!Japan!Gastroenterological!Endoscopy!Society!2014;26(1):63<8.!
42.!Ron<Tal!Fisher!O,!Gralnek!IM,!Eisen!GM,!et!al.!Endoscopic!hemostasis!is!rarely!used!for!hematochezia:!a!population<based!study!from!the!Clinical!Outcomes!Research!Initiative!National!Endoscopic!Database.!Gastrointestinal!endoscopy!2014;79(2):317<25.!
43.!Tan!KK,!Strong!DH,!Shore!T,!et!al.!The!safety!and!efficacy!of!mesenteric!embolization!in!the!management!of!acute!lower!gastrointestinal!hemorrhage.!Annals!of!coloproctology!2013;29(5):205<8.!
44.!Adusumilli!S,!Gosselink!MP,!Ctercteko!G,!et!al.!The!efficacy!of!selective!arterial!embolization!in!the!management!of!colonic!bleeding.!Techniques!in!coloproctology!2014;18(6):529<33.!
45.!Jacovides!CL,!Nadolski!G,!Allen!SR,!et!al.!Arteriography!for!Lower!Gastrointestinal!Hemorrhage:!Role!of!Preceding!Abdominal!Computed!Tomographic!Angiogram!in!Diagnosis!and!Localization.!JAMA!surgery!2015;150(7):650<6.!
46.!Ma!JJ,!Wang!Y,!Xu!XM,!et!al.!Capsule!endoscopy!and!single<balloon!enteroscopy!in!small!bowel!diseases:!Competing!or!complementary?!World!journal!of!gastroenterology!2016;22(48):10625<30.!
47.!Strate!LL,!Gralnek!IM.!ACG!Clinical!Guideline:!Management!of!Patients!With!Acute!Lower!Gastrointestinal!Bleeding.!The!American!journal!of!gastroenterology!2016;111(4):459<74.!
48.!Czymek!R,!Kempf!A,!Roblick!UJ,!et!al.!Surgical!treatment!concepts!for!acute!lower!gastrointestinal!bleeding.!Journal!of!gastrointestinal!surgery!:!official!journal!of!the!Society!for!Surgery!of!the!Alimentary!Tract!2008;12(12):2212<20.!
49.!Watt!DG,!Wilson!MS,!Shapter!OC,!et!al.!30<Day!and!1<year!mortality!in!emergency!general!surgery!laparotomies:!an!area!of!concern!and!need!for!improvement?!European!journal!of!trauma!and!emergency!surgery!:!official!publication!of!the!European!Trauma!Society!2015;41(4):369<74.!
50.!Lorenzo!DCG,!Lahmek!P,!Lesgourgues!B,et!al.!Middle<term!mortality!and!re<bleeding!after!initial!diverticular!bleeding:!A!nationwide!study!of!365!mostly!elderly!French!patients!United!European!Gastroenterology!Journal!2016;5(1):119<27.!
51.!Wheat!CL,!Strate!LL.!Trends!in!Hospitalization!for!Diverticulitis!and!Diverticular!Bleeding!in!the!United!States!From!2000!to!2010.!Clinical!gastroenterology!and!hepatology!:!the!official!clinical!practice!journal!of!the!American!Gastroenterological!Association!2016;14(1):96<103.e1.!
52.!Laine!L,!Yang!H,!Chang!SC,!et!al.!Trends!for!incidence!of!hospitalization!and!death!due!to!GI!complications!in!the!United!States!from!2001!to!2009.!The!American!journal!of!gastroenterology!2012;107(8):1190<5;!quiz!96.!
53.!Lanas!A,!Garcia<Rodriguez!LA,!Polo<Tomas!M,!et!al.!The!changing!face!of!hospitalisation!due!to!gastrointestinal!bleeding!and!perforation.!Alimentary!pharmacology!&!therapeutics!2011;33(5):585<91.!
54.!Johanson!JF,!Sonnenberg!A.!The!prevalence!of!hemorrhoids!and!chronic!constipation.!An!epidemiologic!study.!Gastroenterology!1990;98(2):380<6.!

! 182!
55.!Lee!JH,!Kim!HE,!Kang!JH,!et!al.!Factors!associated!with!hemorrhoids!in!korean!adults:!korean!national!health!and!nutrition!examination!survey.!Korean!journal!of!family!medicine!2014;35(5):227<36.!
56.!Burch!J,!Epstein!D,!Baba<Akbari!A,!et!al.!Stapled!haemorrhoidectomy!(haemorrhoidopexy)!for!the!treatment!of!haemorrhoids:!a!systematic!review!and!economic!evaluation.!Health!technology!assessment!(Winchester,!England)!2008;12(8):iii<iv,!ix<x,!1<193.!
57.!Sommers!T,!Corban!C,!Sengupta!N,!et!al.!Emergency!department!burden!of!constipation!in!the!United!States!from!2006!to!2011.!The!American!journal!of!gastroenterology!2015;110(4):572<9.!
58.!Visovan,!II,!Tantau!M,!Ciobanu!L,!et!al.!Increasing!prevalence!of!right<sided!colonic!adenomas!in!a!high<volume!endoscopy!department!in!Romania:!implications!for!colorectal!cancer!screening.!Journal!of!gastrointestinal!and!liver!diseases!:!JGLD!2014;23(2):147<51.!
59.!Office!for!National!Statistics.!Cancer!registrations.!2014.!60.!Brenner!H,!Schrotz<King!P,!Holleczek!B,!et!al.!Declining!Bowel!Cancer!
Incidence!and!Mortality!in!Germany.!Deutsches!Arzteblatt!international!2016;113(7):101<6.!
61.!Strate!LL,!Syngal!S.!Timing!of!colonoscopy:!impact!on!length!of!hospital!stay!in!patients!with!acute!lower!intestinal!bleeding.!The!American!journal!of!gastroenterology!2003;98(2):317<22.!
62.!Schmulewitz!N,!Fisher!DA,!Rockey!DC.!Early!colonoscopy!for!acute!lower!GI!bleeding!predicts!shorter!hospital!stay:!a!retrospective!study!of!experience!in!a!single!center.!Gastrointestinal!endoscopy!2003;58(6):841<6.!
63.!Redondo<Cerezo!E,!Gomez<Ruiz!CJ,!Sanchez<Manjavacas!N,!et!al.!Long<term!follow<up!of!patients!with!small<bowel!angiodysplasia!on!capsule!endoscopy.!Determinants!of!a!higher!clinical!impact!and!rebleeding!rate.!Revista!espanola!de!enfermedades!digestivas!:!organo!oficial!de!la!Sociedad!Espanola!de!Patologia!Digestiva!2008;100(4):202<7.!
64.!Nagata!N,!Niikura!R,!Aoki!T,!et!al.!Role!of!urgent!contrast<enhanced!multidetector!computed!tomography!for!acute!lower!gastrointestinal!bleeding!in!patients!undergoing!early!colonoscopy.!Journal!of!gastroenterology!2015;50(12):1162<72.!
65.!Sengupta!N,!Tapper!EB,!Patwardhan!VR,!et!al.!Risk!Factors!for!Adverse!Outcomes!in!Patients!Hospitalized!With!Lower!Gastrointestinal!Bleeding.!Mayo!Clinic!proceedings!2015;90(8):1021<9.!
66.!Rockall!TA,!Logan!RF,!Devlin!HB,!et!al.!Risk!assessment!after!acute!upper!gastrointestinal!haemorrhage.!Gut!1996;38(3):316<21.!
67.!Blatchford!O,!Murray!WR,!Blatchford!M.!A!risk!score!to!predict!need!for!treatment!for!upper<gastrointestinal!haemorrhage.!Lancet!(London,!England)!2000;356(9238):1318<21.!
68.!Kollef!MH,!Canfield!DA,!Zuckerman!GR.!Triage!considerations!for!patients!with!acute!gastrointestinal!hemorrhage!admitted!to!a!medical!intensive!care!unit.!Critical!care!medicine!1995;23(6):1048<54.!
69.!Aoki!T,!Nagata!N,!Shimbo!T,!et!al.!Development!and!Validation!of!a!Risk!Scoring!System!for!Severe!Acute!Lower!Gastrointestinal!Bleeding.!Clinical!gastroenterology!and!hepatology!:!the!official!clinical!practice!journal!of!the!American!Gastroenterological!Association!2016;14(11):1562<70.e2.!

! 183!
70.!Sengupta!N,!Tapper!EB.!Derivation!and!Internal!Validation!of!a!Clinical!Prediction!Tool!for!30<Day!Mortality!in!Lower!Gastrointestinal!Bleeding.!The!American!journal!of!medicine!2017.!
71.!Laine!L,!Shah!A.!Randomized!trial!of!urgent!vs.!elective!colonoscopy!in!patients!hospitalized!with!lower!GI!bleeding.!The!American!journal!of!gastroenterology!2010;105(12):2636<41;!quiz!42.!
72.!Whelan!CT,!Chen!C,!Kaboli!P,!et!al.!Upper!versus!lower!gastrointestinal!bleeding:!a!direct!comparison!of!clinical!presentation,!outcomes,!and!resource!utilization.!Journal!of!hospital!medicine!2010;5(3):141<7.!
73.!Campbell!HE,!Stokes!EA,!Bargo!D,!et!al.!Costs!and!quality!of!life!associated!with!acute!upper!gastrointestinal!bleeding!in!the!UK:!cohort!analysis!of!patients!in!a!cluster!randomised!trial.!BMJ!open!2015;5(4):e007230.!
74.!Cryer!BL,!Wilcox!CM,!Henk!HJ,!et!al.!The!economics!of!upper!gastrointestinal!bleeding!in!a!US!managed<care!setting:!a!retrospective,!claims<based!analysis.!Journal!of!medical!economics!2010;13(1):70<7.!
75.!Bhangu!A,!Kolias!AG,!Pinkney!T,!et!al.!Surgical!research!collaboratives!in!the!UK.!Lancet!(London,!England)!2013;382(9898):1091<2.!
76.!World!Health!Organisation.!International!Statistical!Classification!of!Diseases!and!Related!Health!Problems!10th!Revision!(ICD<10).!
77.!Siddique!J,!Ruhnke!GW,!Flores!A,!et!al.!Applying!Classification!Trees!to!Hospital!Administrative!Data!to!Identify!Patients!with!Lower!Gastrointestinal!Bleeding.!PloS!one!2015;10(9):e0138987.!
78.!Green!BT,!Rockey!DC,!Portwood!G,!et!al.!Urgent!colonoscopy!for!evaluation!and!management!of!acute!lower!gastrointestinal!hemorrhage:!a!randomized!controlled!trial.!The!American!journal!of!gastroenterology!2005;100(11):2395<402.!
79.!Yoon!W,!Jeong!YY,!Shin!SS,!et!al.!Acute!massive!gastrointestinal!bleeding:!detection!and!localization!with!arterial!phase!multi<detector!row!helical!CT.!Radiology!2006;239(1):160<7.!
80.!Scheffel!H,!Pfammatter!T,!Wildi!S,!et!al.!Acute!gastrointestinal!bleeding:!detection!of!source!and!etiology!with!multi<detector<row!CT.!Eur!Radiol!2007;17(6):1555<65.!
81.!Strate!LL,!Naumann!CR.!The!role!of!colonoscopy!and!radiological!procedures!in!the!management!of!acute!lower!intestinal!bleeding.!Clinical!gastroenterology!and!hepatology!:!the!official!clinical!practice!journal!of!the!American!Gastroenterological!Association!2010;8(4):333<43;!quiz!e44.!
82.!Koh!FH,!Soong!J,!Lieske!B,!et!al.!Does!the!timing!of!an!invasive!mesenteric!angiography!following!a!positive!CT!mesenteric!angiography!make!a!difference?!International!journal!of!colorectal!disease!2015;30(1):57<61.!
83.!Moher!D,!Liberati!A,!Tetzlaff!J,!et!al.!Preferred!reporting!items!for!systematic!reviews!and!meta<analyses:!the!PRISMA!statement.!International!journal!of!surgery!(London,!England)!2010;8(5):336<41.!
84.!Stroup!DF,!Berlin!JA,!Morton!SC,!et!al.!Meta<analysis!of!observational!studies!in!epidemiology:!a!proposal!for!reporting.!Meta<analysis!Of!Observational!Studies!in!Epidemiology!(MOOSE)!group.!Jama!2000;283(15):2008<12.!
85.!Dekkers!OM,!Egger!M,!Altman!DG,!et!al.!Distinguishing!case!series!from!cohort!studies.!Annals!of!internal!medicine!2012;156(1!Pt!1):37<40.!

! 184!
86.!Higgins!JGS.!Cochrane!Handbook!for!Systematic!Reviews!of!Interventions!Cochrane!Book!Series!2008;Chapter*13.!
87.!Stang!A.!Critical!evaluation!of!the!Newcastle<Ottawa!scale!for!the!assessment!of!the!quality!of!nonrandomized!studies!in!meta<analyses.!European!journal!of!epidemiology!2010;25(9):603<5.!
88.!Higgins!JGS.!Cochrane!Handbook!for!Systematic!Reviews!of!Interventions.!Cochrane!Book!Series!2008(Part!3):392<432.!
89.!Higgins!JP,!Thompson!SG,!Deeks!JJ,!et!al.!Measuring!inconsistency!in!meta<analyses.!BMJ!(Clinical!research!ed)!2003;327(7414):557<60.!
90.!DerSimonian!R,!Laird!N.!Meta<analysis!in!clinical!trials.!Controlled!clinical!trials!1986;7(3):177<88.!
91.!Sengupta!N,!Tapper!EB,!Feuerstein!JD.!Early!Versus!Delayed!Colonoscopy!in!Hospitalized!Patients!With!Lower!Gastrointestinal!Bleeding:!A!Meta<Analysis.!Journal!of!clinical!gastroenterology!2016.!
92.!Yabutani!AT,!K.;!Teramoto,!A.;!Kondou,!A.;!Nakamura,!S.;!Iraha,!A.;!Matsukawa,!S.;!Nakamura,!M.;!Kobashikawa,!K.;!Nakayoshi,!T.;!Uchima,!N.;!Kinjo,!F.!Possible!utility!of!contract!enhanced!computed!tomography!for!detecting!colonic!diverticular!bleeding!by!emergent!colonoscopy.!Journal!of!Gastroenterology!and!Hepatology!(Australia)!2014;29:pp!307<08.!
93.!Rodriguez<Moranta!FB,!A.;!Botargues,!JM.;,!Soriano<Izquierdo!AC,!N.;!Biondo,!S.;,!Guardiola!J.!Colonoscopy!Delay!in!Lower!Gastrointestinal!Bleeding:!Influence!On!Diagnostic!Accuracy,!Endoscopic!Therapy!and!Hospital!Stay.!Gastrointestinal!Endoscopy!2007;65(5):AB261.!
94.!Ketwaroo!GAT,!S.!K.;!Kheraj,!R.;!Raptopoulos,!V.;!Leffler,!D.!A.;.!Mesenteric!ct!angiography!in!the!evaluation!and!management!of!acute!lower!gi!bleeding.!Gastroenterology!2012;142(5!suppl!1):S581.!
95.!Sun!JK,!N.;!Wong,!R.!CT!angiography!is!superior!to!tagged!red!blood!cell!scanning!for!localizing!GI!bleeding!and!for!guiding!management!The!American!journal!of!gastroenterology!2011;106:ppS82.!
96.!Nakano!K,!Ishii,!N.;!Fujita,!Y.;.!Long<Term!Outcomes!of!Endoscopic!Band!Ligation!Versus!Endoscopic!Clipping!for!Treatment!of!Colonic!Diverticular!Hemorrhage.!Gastrointestinal!Endoscopy!2015;81(5S):AB370.!
97.!Ishii!NF,!Y.!Endoscopic!treatment!for!colonic!diverticular!hemorrhage:!From!endoscopic!clipping!to!endoscopic!band!ligation.!Gastrointestinal!Endoscopy!2011;73(4!supp!1):AB292.!
98.!Jensen!DM,!Machicado!GA,!Jutabha!R,!et!al.!Urgent!colonoscopy!for!the!diagnosis!and!treatment!of!severe!diverticular!hemorrhage.!The!New!England!journal!of!medicine!2000;342(2):78<82.!
99.!Yamaguchi!T,!Manabe!N,!Hata!J,!et!al.!The!usefulness!of!transabdominal!ultrasound!for!the!diagnosis!of!lower!gastrointestinal!bleeding.!Alimentary!pharmacology!&!therapeutics!2006;23(8):1267<72.!
100.!Albeldawi!M,!Ha!D,!Mehta!P,!et!al.!Utility!of!urgent!colonoscopy!in!acute!lower!gastro<intestinal!bleeding:!a!single<center!experience.!Gastroenterology!report!2014;2(4):300<5.!
101.!Nagata!N,!Niikura!R,!Sakurai!T,!et!al.!Safety!and!Effectiveness!of!Early!Colonoscopy!in!Management!of!Acute!Lower!Gastrointestinal!Bleeding!on!the!Basis!of!Propensity!Score!Matching!Analysis.!Clinical!gastroenterology!and!hepatology!:!the!official!clinical!practice!journal!of!the!American!Gastroenterological!Association!2016;14(4):558<64.!

! 185!
102.!Leung!WK,!Ho!SS,!Suen!BY,!et!al.!Capsule!endoscopy!or!angiography!in!patients!with!acute!overt!obscure!gastrointestinal!bleeding:!a!prospective!randomized!study!with!long<term!follow<up.!The!American!journal!of!gastroenterology!2012;107(9):1370<6.!
103.!Chan!FK,!Leung!Ki!EL,!Wong!GL,!et!al.!Risks!of!Bleeding!Recurrence!and!Cardiovascular!Events!With!Continued!Aspirin!Use!After!Lower!Gastrointestinal!Hemorrhage.!Gastroenterology!2016;151(2):271<7.!
104.!Kouanda!AM,!Somsouk!M,!Sewell!JL,!et!al.!Urgent!colonoscopy!in!patients!with!lower!GI!bleeding:!a!systematic!review!and!meta<analysis.!Gastrointestinal!endoscopy!2017;86(1):107<17.e1.!
105.!Seth!A,!Khan!MA,!Nollan!R,!et!al.!Does!Urgent!Colonoscopy!Improve!Outcomes!in!the!Management!of!Lower!Gastrointestinal!Bleeding?!The!American!journal!of!the!medical!sciences!2017;353(3):298<306.!
106.!Kuhle!WG,!Sheiman!RG.!Detection!of!active!colonic!hemorrhage!with!use!of!helical!CT:!findings!in!a!swine!model.!Radiology!2003;228(3):743<52.!
107.!Deyo!RA,!Cherkin!DC,!Ciol!MA.!Adapting!a!clinical!comorbidity!index!for!use!with!ICD<9<CM!administrative!databases.!Journal!of!clinical!epidemiology!1992;45(6):613<9.!
108.!Charlson!ME,!Pompei!P,!Ales!KL,!et!al.!A!new!method!of!classifying!prognostic!comorbidity!in!longitudinal!studies:!development!and!validation.!Journal!of!chronic!diseases!1987;40(5):373<83.!
109.!New!York!Heart!Association.!Nomenclature!and!Criteria!for!Diagnosis!of!Diseases!of!the!Heart!and!Great!Vessels.!.!Boston:!Little,!Brown!&!Co!1994:253–56.!
110.!The!Renal!Association.!Chronic!Kidney!Disease!Stages.!www.renal.org!111.!Health!Research!Authority!(HRA).!Determining!whether!your!study!is!
research!wwwhranhsuk.!112.!Department!of!Health.!NHS!Code!of!Practice:!Confidentiality.!
https://wwwgovuk/government/uploads/system/uploads/attachment_data/file/200146/Confidentiality_<_NHS_Code_of_Practicepdf!2003.!
113.!Jairath!V,!Hearnshaw!S,!Brunskill!SJ,!et!al.!Red!cell!transfusion!for!the!management!of!upper!gastrointestinal!haemorrhage.!Cochrane!Database!Syst!Rev!2010(9):CD006613.!
114.!Hopewell!S,!Omar!O,!Hyde!C,!et!al.!A!systematic!review!of!the!effect!of!red!blood!cell!transfusion!on!mortality:!evidence!from!large<scale!observational!studies!published!between!2006!and!2010.!BMJ!open!2013;3(5).!
115.!Murphy!MF.!The!Choosing!Wisely!campaign!to!reduce!harmful!medical!overuse:!its!close!association!with!Patient!Blood!Management!initiatives.!Transfusion!medicine!(Oxford,!England)!2015;25(5):287<92.!
116.!Jairath!V,!Thompson!J,!Kahan!BC,!et!al.!Poor!outcomes!in!hospitalized!patients!with!gastrointestinal!bleeding:!impact!of!baseline!risk,!bleeding!severity,!and!process!of!care.!Am!J!Gastroenterol!2014;109(10):1603<12.!
117.!Aoki!T,!Nagata!N,!Niikura!R,!et!al.!Recurrence!and!mortality!among!patients!hospitalized!for!acute!lower!gastrointestinal!bleeding.!Clinical!gastroenterology!and!hepatology!:!the!official!clinical!practice!journal!of!the!American!Gastroenterological!Association!2015;13(3):488<94.e1.!
118.!National!Institute!for!Health!and!Care!Excellence.!Guideline!NG12:!Suspected!cancer:!recognition!and!referral.!2015.!
! 186!
119.!Laine!L,!Spiegel!B,!Rostom!A,!et!al.!Methodology!for!randomized!trials!of!patients!with!nonvariceal!upper!gastrointestinal!bleeding:!recommendations!from!an!international!consensus!conference.!The!American!journal!of!gastroenterology!2010;105(3):540<50.!
120.!Crooks!CJ,!West!J,!Hearnshaw!SA,!et!al.!Hospital!admission!database!or!specialist!national!audits!for!monitoring!gastrointestinal!bleeding?!both!are!vital!to!monitoring!our!clinical!practice.!Gut!2011;60:A187<A88.!
121.!NHS!England.!Bed!availability!and!occupancy!data:!Quarter!2,!2015.!2015.!www.digital.nhs.uk!
122.!National!Institute!for!Health!and!Care!Excellence.!Acute!upper!gastrointestinal!bleeding!costing!report.!2012.!
123.!Zakharchenko!A,!Kaitoukov!Y,!Vinnik!Y,!et!al.!Safety!and!efficacy!of!superior!rectal!artery!embolization!with!particles!and!metallic!coils!for!the!treatment!of!hemorrhoids!(Emborrhoid!technique).!Diagnostic!and!interventional!imaging!2016;97(11):1079<84.!
124.!Tsetis!D,!Uberoi!R,!Fanelli!F,!et!al.!The!Provision!of!Interventional!Radiology!Services!in!Europe:!CIRSE!Recommendations.!Cardiovasc!Intervent!Radiol!2016;39(4):500<6.!
125.!Tarazona<Santabalbina!FJ,!Belenguer<Varea!A,!Rovira!E,!et!al.!Orthogeriatric!care:!improving!patient!outcomes.!Clinical!interventions!in!aging!2016;11:843<56.!
126.!Ellis!G,!Spiers!M,!Coutts!S,!et!al.!Preoperative!assessment!in!the!elderly:!evaluation!of!a!new!clinical!service.!Scottish!medical!journal!2012;57(4):212<6.!
127.!Macpherson!DS,!Lofgren!RP.!Outpatient!internal!medicine!preoperative!evaluation:!a!randomized!clinical!trial.!Medical!care!1994;32(5):498<507.!
128.!NHS!Blood!and!Transplant.!National!comparative!audit!of!lower!gastrointestinal!bleeding!and!the!use!of!blood.!2016.!www.hospitals.blood.co.uk!
129.!Kollef!MH,!O'Brien!JD,!Zuckerman!GR,!et!al.!BLEED:!a!classification!tool!to!predict!outcomes!in!patients!with!acute!upper!and!lower!gastrointestinal!hemorrhage.!Crit!Care!Med!1997;25(7):1125<32.!
130.!Xavier!S,!Firmino<machado,!Magalhaes!J,!et!al.!Acute!Gastrointestinal!Bleeding:!Are!STRATE!and!BLEED!Scores!Valid!to!Clinical!Practice?!Gastrointestinal!endoscopy!2016;83(5):AB282.!
131.!Oakland!K,!Guy!R,!Uberoi!R,!et!al.!Acute!lower!GI!bleeding!in!the!UK:!patient!characteristics,!interventions!and!outcomes!in!the!first!nationwide!audit.!Gut!2017.$Feb$1. 132.!Health!Research!Authority.!Ethical!review!of!research!databases.!2016.!133.!Ayaru!L,!Ypsilantis!PP,!Nanapragasam!A,!et!al.!Prediction!of!Outcome!in!
Acute!Lower!Gastrointestinal!Bleeding!Using!Gradient!Boosting.!PloS!one!2015;10(7):e0132485.!
134.!Oakland!K,!Guy!R,!Uberoi!R,!et!al.!Study!protocol:!first!nationwide!comparative!audit!of!acute!lower!gastrointestinal!bleeding!in!the!UK.!BMJ!open!2016;6(8):e011752.!
135.!Moons!KG,!Altman!DG,!Reitsma!JB,!et!al.!Transparent!Reporting!of!a!multivariable!prediction!model!for!Individual!Prognosis!or!Diagnosis!(TRIPOD):!explanation!and!elaboration.!Annals!of!internal!medicine!2015;162(1):W1<73.!
! 187!
136.!Collins!GS,!Ogundimu!EO,!Altman!DG.!Sample!size!considerations!for!the!external!validation!of!a!multivariable!prognostic!model:!a!resampling!study.!Statistics!in!medicine!2016;35(2):214<26.!
137.!Royston!P!AD.!Regression!using!fractional!polynomials!of!continuous!covariates:!parsimonious!parametric!modelling.!Applied!Statistics!1994;43(3):429<67.!
138.!Sullivan!LM,!Massaro!JM,!D'Agostino!RB,!Sr.!Presentation!of!multivariate!data!for!clinical!use:!The!Framingham!Study!risk!score!functions.!Statistics!in!medicine!2004;23(10):1631<60.!
139.!Van!Calster!B,!Nieboer!D,!Vergouwe!Y,!et!al.!A!calibration!hierarchy!for!risk!models!was!defined:!from!utopia!to!empirical!data.!Journal!of!clinical!epidemiology!2016;74:167<76.!
140.!Saltzman!JR,!Tabak!YP,!Hyett!BH,!et!al.!A!simple!risk!score!accurately!predicts!in<hospital!mortality,!length!of!stay,!and!cost!in!acute!upper!GI!bleeding.!Gastrointestinal!endoscopy!2011;74(6):1215<24.!
141.!Zakko!LL,!S.;!Stanley,!A.;!Dalton,!H.;!Jing,!N.;!Schultz,!M.;!Laine,!L.!Do!Upper!Gastrointestinal!Bleeding!Scores!Predict!Outcomes!for!Patients!Presenting!With!Hemodynamically!Significant!Hematochezia?!Gastrointestinal!endoscopy!2016;83(5):AB281.!
142.!Nakamura!S,!Matsumoto!T,!Sugimori!H,!et!al.!Emergency!endoscopy!for!acute!gastrointestinal!bleeding:!prognostic!value!of!endoscopic!hemostasis!and!the!AIMS65!score!in!Japanese!patients.!Digestive!endoscopy!:!official!journal!of!the!Japan!Gastroenterological!Endoscopy!Society!2014;26(3):369<76.!
143.!DeLong!ER,!DeLong!DM,!Clarke<Pearson!DL.!Comparing!the!areas!under!two!or!more!correlated!receiver!operating!characteristic!curves:!a!nonparametric!approach.!Biometrics!1988;44(3):837<45.!
144.!Collins!GS,!Reitsma!JB,!Altman!DG,!et!al.!Transparent!Reporting!of!a!multivariable!prediction!model!for!Individual!Prognosis!or!Diagnosis!(TRIPOD):!the!TRIPOD!statement.!Annals!of!internal!medicine!2015;162(1):55<63.!
145.!Stewart!BT,!Groen!RS,!Kamara!TB,!et!al.!Rectal!bleeding!and!endoscopy!need!in!Sierra!Leone:!results!of!a!nationwide,!community<based!survey.!Lancet!(London,!England)!2015;385*Suppl*2:S4.!
146.!National!Confidential!Enquiry!into!Patient!Outcomes!and!Death.!Time!to!get!control?!A!review!of!the!care!received!by!patients!who!had!severe!gastrointestinal!haemorrhage.!NCEPOD!2015.!
147.!Cirocchi!R,!Grassi!V,!Cavaliere!D,!et!al.!New!Trends!in!Acute!Management!of!Colonic!Diverticular!Bleeding:!A!Systematic!Review.!Medicine!2015;94(44):e1710.!
148.!Kouanda!AM,!Somsouk!M,!Sewell!JL,!et!al.!Urgent!colonoscopy!in!patients!with!lower!gastrointestinal!bleeding:!A!systematic!review!and!meta<analysis.!Gastrointest!Endosc!2017.!
149.!National!Institute!for!Health!and!Care!Excellence.!Guideline!NG12:!Suspected!cancer:!recognition!and!referral.!
150.!Jairath!V,!Kahan!BC,!Stanworth!SJ,!et!al.!Prevalence,!management,!and!outcomes!of!patients!with!coagulopathy!after!acute!nonvariceal!upper!gastrointestinal!bleeding!in!the!United!Kingdom.!Transfusion!2013;53(5):1069<76.!

! 188!
151.!Pollack!CV,!Jr.,!Reilly!PA,!Eikelboom!J,!et!al.!Idarucizumab!for!Dabigatran!Reversal.!The!New!England!journal!of!medicine!2015;373(6):511<20.!
152.!Connolly!SJ,!Milling!TJ,!Jr.,!Eikelboom!JW,!et!al.!Andexanet!Alfa!for!Acute!Major!Bleeding!Associated!with!Factor!Xa!Inhibitors.!The!New!England!journal!of!medicine!2016;375(12):1131<41.!
153.!Li!C,!Hirsh!J,!Xie!C,!et!al.!Reversal!of!the!anti<platelet!effects!of!aspirin!and!clopidogrel.!Journal!of!thrombosis!and!haemostasis!:!JTH!2012;10(4):521<8.!
154.!Zakko!L,!Rustagi!T,!Douglas!M,!et!al.!No!Benefit!From!Platelet!Transfusion!for!Gastrointestinal!Bleeding!in!Patients!Taking!Antiplatelet!Agents.!Clinical!gastroenterology!and!hepatology!:!the!official!clinical!practice!journal!of!the!American!Gastroenterological!Association!2016.!
155.!Strate!LL,!Gralnek!IM.!ACG!Clinical!Guideline:!Management!of!Patients!With!Acute!Lower!Gastrointestinal!Bleeding.!The!American!journal!of!gastroenterology!2016;111(5):755.!
156.!Sung!JJ,!Lau!JY,!Ching!JY,!et!al.!Continuation!of!low<dose!aspirin!therapy!in!peptic!ulcer!bleeding:!a!randomized!trial.!Annals!of!internal!medicine!2010;152(1):1<9.!
157.!Becker!RC,!Scheiman!J,!Dauerman!HL,!et!al.!Management!of!platelet<directed!pharmacotherapy!in!patients!with!atherosclerotic!coronary!artery!disease!undergoing!elective!endoscopic!gastrointestinal!procedures.!Journal!of!the!American!College!of!Cardiology!2009;54(24):2261<76.!
158.!Makris!M,!Van!Veen!JJ,!Tait!CR,!et!al.!Guideline!on!the!management!of!bleeding!in!patients!on!antithrombotic!agents.!British!journal!of!haematology!2013;160(1):35<46.!
159.!Awtry!EH,!Loscalzo!J.!Aspirin.!Circulation!2000;101(10):1206<18.!160.!Weber!AA,!Braun!M,!Hohlfeld!T,!et!al.!Recovery!of!platelet!function!after!
discontinuation!of!clopidogrel!treatment!in!healthy!volunteers.!British!journal!of!clinical!pharmacology!2001;52(3):333<6.!
161.!Devereaux!PJ,!Mrkobrada!M,!Sessler!DI,!et!al.!Aspirin!in!patients!undergoing!noncardiac!surgery.!The!New!England!journal!of!medicine!2014;370(16):1494<503.!
162.!Keeling!D,!Tait!RC,!Watson!H.!Peri<operative!management!of!anticoagulation!and!antiplatelet!therapy.!British!journal!of!haematology!2016;175(4):602<13.!
163.!Roberts!I,!Coats!T,!Edwards!P,!et!al.!HALT<IT<<tranexamic!acid!for!the!treatment!of!gastrointestinal!bleeding:!study!protocol!for!a!randomised!controlled!trial.!Trials!2014;15:450.!
164.!Thiele!T,!Sumnig!A,!Hron!G,!et!al.!Platelet!transfusion!for!reversal!of!dual!antiplatelet!therapy!in!patients!requiring!urgent!surgery:!a!pilot!study.!Journal!of!thrombosis!and!haemostasis!:!JTH!2012;10(5):968<71.!
165.!Baharoglu!MI,!Cordonnier!C,!Al<Shahi!Salman!R,!et!al.!Platelet!transfusion!versus!standard!care!after!acute!stroke!due!to!spontaneous!cerebral!haemorrhage!associated!with!antiplatelet!therapy!(PATCH):!a!randomised,!open<label,!phase!3!trial.!Lancet!(London,!England)!2016;387(10038):2605<13.!
166.!Buchanan!A,!Newton!P,!Pehrsson!S,!et!al.!Structural!and!functional!characterization!of!a!specific!antidote!for!ticagrelor.!Blood!2015;125(22):3484<90.!

! 189!
167.!Nagata!N,!Niikura!R,!Aoki!T,!et!al.!Risk!factors!for!adverse!in<hospital!outcomes!in!acute!colonic!diverticular!hemorrhage.!World!journal!of!gastroenterology!2015;21(37):10697<703.!
168.!Baker!D,!Wilsmore!B,!Narasimhan!S.!Adoption!of!direct!oral!anticoagulants!for!stroke!prevention!in!atrial!fibrillation.!Internal!medicine!journal!2016;46(7):792<7.!
169.!Narayan!SW,!Tordoff!JM,!Nishtala!PS.!Temporal!trends!in!the!utilisation!of!preventive!medicines!by!older!people:!A!9<year!population<based!study.!Archives!of!gerontology!and!geriatrics!2016;62:103<11.!
170.!Eikelboom!JW,!Connolly!SJ,!Bosch!J,!et!al.!Rivaroxaban!with!or!without!Aspirin!in!Stable!Cardiovascular!Disease.!New!England!Journal!of!Medicine;0(0):null.!
171.!Oakland!K,!Jairath!V,!Uberoi!R,!et!al.!Derivation!and!validation!of!a!novel!risk!score!for!safe!discharge!after!acute!lower!gastrointestinal!bleeding:!a!modelling!study.!The!lancet!Gastroenterology!&!hepatology!2017.!
172.!Logan!RF,!Patnick!J,!Nickerson!C,!et!al.!Outcomes!of!the!Bowel!Cancer!Screening!Programme!(BCSP)!in!England!after!the!first!1!million!tests.!Gut!2012;61(10):1439<46.!
!!!******************APPENDICES**Appendix!table!1:!modified!Charlson!Co<morbidity!Index!for!use!in!a!Clinical!Dataset!!Co<morbidities!were!collated!using!the!Deyo!modification!of!Charlson!Co<Morbidity!Index,108!which!links!definitions!of!the!conditions!used!in!the!Charlson!co<morbidity!index!to!ICD<9!criteria!to!aids!application!in!non<administrative!datasets.!The!application!of!the!Charlson!index!is!difficult!as!some!of!the!definitions!are!subjective.!To!enable!its!use!in!a!clinical!setting!we!made!the!following!amendments.*!Assigned!weight!
Charlson!weighted!condition!
Deyo!description! Amended!definition!

! 190!
1! Myocardial!Infarction!!Congestive!Heart!Failure!!Peripheral!Vascular!Disease!!!!!Stroke!without!hemiplegia!!Dementia!!!Chronic!Pulmonary!Disease!!!!Connective!Tissue!Disease!!!!!Peptic!Ulcer!Disease!!!Mild!Liver!Disease!!!!!Diabetes!!
Acute!or!old!!Heart!failure!!!Intermittent!claudication,!gangrene,!resection!and!replacement!of!lower!limb!arteries,!blood!vessel!replaced!by!prosthesis,!gangrene,!aortic!aneurysm!!!!Senile!or!presenile!dementias!!COPD,!pneumoconeosis,!chronic!repiratory!conditions!due!to!inhaled!fumes!and!vapours!!SLE,!systemic!sclerosis,!polymyositis,!adult!rheumatoid!arthritis,!rheumatic!lung,!polymyalgia!rheumatica!!Gastric,!duodenal,!gastrojejunal!ulcers!!alcoholic!cirrhosis,!cirrhosis!without!alcohol,!biliary!cirrhosis,!chronic!hepatitis!!!Includes!those!with!peripheral!circulatory!disorders!!
!!On!pharmacotherapy!or!clinical!examination!findings!consistent!with!congestive!heart!failure!!!!!!!!!Formally!diagnosed!dementia!!Addition!of!Asthma!!!!!!!!!!!Requiring!acid!suppression!with!PPI!or!H2!receptor!antagonist!Liver!disease!but!absence!of!hepatic!coma,!portal!hypertension,!other!sequelae!of!chronic!liver!disease,!oesophageal!varices!!!!!
2! Stroke!with!Hemiplegia!!Moderate!or!Severe!Renal!Disease!!!!!!Diabetes!with!End<
!!Chronic!glomerulonephritis,!nephritis!and!nephropathy,!chronic!renal!failure,!unspecified!renal!failure,!disorders!resulting!from!impaired!renal!function!!!Renal,!opthalmic!or!
!!!eGFR!≤!60!(renal!association!stage!2)!

! 191!
organ!Damage!!Any!Tumour,!leukaemia!or!lymphoma!
neurological!complications!
3! Moderate!or!Severe!Liver!Disease!
Hepatic!coma,!portal!hypertension,!other!sequelae!of!chronic!liver!disease,!oesophageal!varices!
*
6! Metastatic!Solid!Tumour!AIDS!
! !
!!!!!!!!!!!!!!!!!!!!!!!!!!!***********

! 192!
Appendix*2:*Systematic*review*search*terms**The!following!databases!were!searched!for!systematic!reviews,!RCTs!and!observational!(cohort)!studies,!from!2000!onwards,!on!12.11.15:!MEDLINE!(OvidSP,!1946!onwards)!PubMed!(epublications!only)!Embase!(OvidSP,!1974!onwards)!CDSR,!CENTRAL,!DARE,!HTA!&!NHSEED!(The!Cochrane!Library!2015,!Issue!3)!!Transfusion!Evidence!Library!!Ongoing!Trials:!ClinicalTrials.gov!!159!refs!WHO!International!Clinical!Trials!Registry!Platform:!36!refs!!!Searches!retrieved!10,667!references!plus!195!ongoing!trials,!which!were!reduced!to!8,260!refs!plus!87!ongoing!trials!when!duplicates!had!been!removed.!!!SEARCH!STRATEGIES!!MEDLINE!(OvidSP)!1.!exp!Lower!Gastrointestinal!Tract/!2.!exp!Intestines/!3.!Gastrointestinal!Tract/!4.!exp!Mesenteric!Arteries/!5.!(lower!gastrointestinal!tract*!or!lower!gastro<intestinal!tract*!or!lower!GI!tract*!or!large!intestin*!or!small!intestin*!or!mesenteric!arter*).tw,kf.!6.!or/1<5!7.!(h?emorrhag*!or!bleed*!or!re<bleed*!or!rebleed*!or!blood!loss*).mp.!8.!6!and!7!9.!exp!Gastrointestinal!Hemorrhage/!10.!((anal!or!anus!or!rectum!or!rectal!or!colon!or!colonic!or!colorectal!or!cecum!or!caecum!or!jejunum!or!cloaca!or!gut!or!ileum!or!diverticula*!or!lower!intestin*!or!large!intestin*!or!small!intestin*!or!bowel!or!lower!gastrointestinal!or!lower!gastro<intestinal!or!lower!GI!or!mesenteric)!adj6!(h?emorrhag*!or!bleed*!or!re<bleed*!or!rebleed*!or!blood!loss*)).tw,kf.!11.!(hematochezia!or!mel?ena!or!colonic!angiodysplasia!or!proctorrhagi*!or!rectocolic*!or!rectorrhagi*).tw,kf.!12.!or/8<11!13.!exp!Colonoscopy/!14.!Proctoscopy/!15.!(colonoscop*!or!coloscop*!or!sigmoidoscop*!or!proctoscop*!or!rectoscop*!or!enteroscop*!or!anuscop*).tw,kf.!16.!Endoscopy,!Gastrointestinal/!17.!Capsule!Endoscopy/!18.!(endoscop*!adj3!(capsule!or!video!or!lower!or!mesenteric!or!colon*!or!bowel)).tw,kf.!19.!pillcam.tw,kf.!20.!or/13<19!21.!Colonography,!Computed!Tomographic/!22.!((CT!or!computed!or!tomograph*!or!virtual)!adj2!(colonograph*!or!colonoscop*!or!pneumocolon*)).tw,kf.!23.!Tomography,!X<Ray!Computed/!24.!Radiology,!Interventional/!25.!(tomograph*!angiogra*!or!CTA!or!CT!angiogra*!or!mesenteric!angiogra*!or!GI!angiogra*!or!(radiolog*!adj2!(diagnos*!or!intervention*))).tw,kf.!26.!Angiography/!27.!or/21<26!28.!Hemostasis,!Endoscopic/!29.!((therap*!or!treatment*!or!h?emosta*!or!epinephrine!or!adrenaline!or!cyanoacrylate!or!inject*!or!band*!or!electrocauter*!or!argon!plasma!or!thermal!coagulat*!or!thermocoagulat*!or!
! 193!
thermo<coagulat*!or!heater!probe*!or!argon!coagulat*!or!laser!coagulat*!or!YAG!laser!or!ablat*!or!h?emoclip*!or!h?emospray!or!sclerotherap*)!adj10!endoscop*).tw,kf.!30.!(endotherap*!or!endoclip*!or!over<the<scope!clip*).tw,kf.!31.!20!or!28!or!29!or!30!32.!Embolization,!Therapeutic/!33.!(emboli?ation!or!emboli?ed!or!embolotherap*!or!angioemboli*!or!microemoboli*).tw,kf.!34.!27!or!32!or!33!35.!12!and!(31!or!34)!36.!limit!35!to!yr="2000!<Current"!!EMBASE!(OvidSP)!1.!exp!Large!Intestine/!2.!exp!Small!Intestine/!3.!exp!Anus/!4.!exp!Mesenteric!Artery/!5.!Intestine/!6.!Gastrointestinal!Tract/!7.!(lower!gastrointestinal!tract*!or!lower!gastro<intestinal!tract*!or!lower!GI!tract*!or!large!intestin*!or!small!intestin*!or!mesenteric!arter*).tw.!8.!1!or!2!or!4!or!5!or!6!or!7!9.!(h?emorrhag*!or!bleed*!or!re<bleed*!or!rebleed*or!blood!loss*).mp.!10.!Bleeding/!11.!9!or!10!12.!8!and!11!13.!Gastrointestinal!Hemorrhage/!or!Colon!Hemorrhage/!or!Hemorrhagic!Colitis/!or!Intestinal!Bleeding/!or!Intestine!Hematoma/!or!Large!Intestine!Hemorrhage/!or!Melena/!or!Rectum!Hemorrhage/!or!Small!Intestine!Hemorrhage/!14.!((anal!or!anus!or!rectum!or!rectal!or!colon!or!colonic!or!colorectal!or!cecum!or!caecum!or!jejunum!or!cloaca!or!gut!or!ileum!or!diverticula*!or!lower!intestin*!or!large!intestin*!or!small!intestin*!or!bowel!or!lower!gastrointestinal!or!lower!gastro<intestinal!or!lower!GI!or!mesenteric)!adj6!(h?emorrhag*!or!bleed*!or!re<bleed*!or!rebleed*!or!blood!loss*)).tw.!15.!(hematochezia!or!mel?ena!or!colonic!angiodysplasia!or!proctorrhagi*!or!rectocolic*!or!rectorrhagi*).tw.!16.!or/12<15!17.!Intestine!Endoscopy/!or!Capsule!Endoscopy/!or!Colonoscopy/!or!Push!Enteroscopy/!or!Rectoscopy/!or!Sigmoidoscopy/!18.!Gastrointestinal!Endoscopy/!19.!(colonoscop*!or!coloscop*!or!sigmoidoscop*!or!proctoscop*!or!rectoscop*!or!enteroscop*!or!anuscop*!or!pillcam*).tw.!20.!(endoscop*!adj3!(capsule!or!video!or!lower!or!mesenteric!or!colon*!or!bowel)).tw.!21.!or/17<20!22.!*Endoscopy/!and!*Hemostasis/!23.!((therap*!or!treatment*!or!h?emosta*!or!epinephrine!or!adrenaline!or!cyanoacrylate!or!inject*!or!banded!or!banding!or!electrocauter*!or!argon!plasma!or!thermal!coagulat*!or!thermocoagulat*!or!thermo<coagulat*!or!heater!probe*!or!argon!coagulat*!or!laser!coagulat*!or!YAG!laser!or!ablat*!or!h?emoclip*!or!h?emospray!or!sclerotherap*)!adj10!endoscop*).tw.!24.!(endotherap*!or!endoclip*!or!over<the<scope!clip*).tw.!25.!or/21<24!26.!Computed!Tomographic!Colonography/!27.!((CT!or!computed!or!tomograph*!or!virtual)!adj2!(colonograph*!or!colonoscop*!or!pneumocolon*)).tw.!28.!Computer!Assisted!Tomography/!29.!Interventional!Radiology/!30.!(tomograph*!angiogra*!or!CTA!or!CT!angiogra*!or!mesenteric!angiogra*!or!GI!angiogra*!or!(radiolog*!adj2!(diagnos*!or!intervention*))).tw.!31.!Abdominal!Angiography/!or!Superior!Mesenteric!Angiography/!32.!Pelvic!Angiography/!33.!or/26<32!34.!Artificial!Embolism/!

! 194!
35.!(emboli?ation!or!emboli?ed!or!embolotherap*!or!angioemboli*!or!microemoboli*).tw.!36.!or/33<35!37.!16!and!(25!or!36)!!PubMed!(epublications!only)!!#1!!!(lower!gastrointestinal!tract*!OR!lower!gastro<intestinal!tract*!OR!lower!GI!tract*!OR!large!intestin*!OR!small!intestin*!OR!mesenteric!arter*)!AND!(hemorrhag*!OR!haemorrhag*!OR!bleed*!OR!re<bleed*!OR!rebleed*!OR!blood!loss*)!#2!!!((anal!OR!anus!OR!rectum!OR!rectal!OR!colon!OR!colonic!OR!colorectal!OR!cecum!OR!caecum!OR!jejunum!OR!cloaca!OR!gut!OR!ileum!OR!diverticula*!OR!lower!intestin*!OR!large!intestin*!OR!small!intestin*!OR!bowel!OR!lower!gastrointestinal!OR!lower!gastro<intestinal!OR!lower!GI!OR!mesenteric)!AND!(hemorrhag*!OR!haemorrhage*!OR!bleed*!OR!re<bleed*!OR!rebleed*!OR!blood!loss*))!#3!!!(hematochezia!OR!melena!OR!melaena!OR!colonic!angiodysplasia!OR!proctorrhagi*!OR!rectocolic*!OR!rectorrhagi*)!#4!!!#1!OR!#2!OR!#3!#5!!!!(colonoscop*!OR!coloscop*!OR!sigmoidoscop*!OR!proctoscop*!OR!rectoscop*!OR!anuscop*!OR!pillcam!OR!endotherap*!OR!endoclip*!OR!over<the<scope!clip*)!#6!!!((capsule!OR!video!OR!lower!OR!mesenteric!OR!colon!OR!colonic!OR!bowel!OR!hemosta*!OR!haemostat*!OR!epinephrine!OR!adrenaline!OR!cyanoacrylate!OR!inject*!OR!banded!OR!banding!OR!electrocauter*!OR!argon!plasma!OR!thermal!coagulat*!OR!thermocoagulat*!OR!thermo<coagulat*!OR!heater!probe*!OR!argon!coagulat*!OR!laser!coagulat*!OR!YAG!laser!OR!ablat*!OR!hemoclip*!OR!hemospray!OR!sclerotherap*)!AND!endoscop*)!#7!!!#5!OR!#6!#8!!((CT!OR!computed!OR!tomograph*!OR!virtual)!AND!(colonograph*!OR!colonoscop*!OR!pneumocolon*))!#9!!(tomograph*!angiogra*!OR!CTA!OR!CT!angiogra*!OR!mesenteric!angiogra*!OR!GI!angiogra*!OR!(radiolog*!AND!(diagnos*!OR!intervention*)))!#10!(embolization!OR!embolized!OR!embolization!OR!embolised!OR!embolotherap*!OR!angioemboli*!OR!microemoboli*)!#11!!#8!OR!#9!OR!#10!#12!!#4!and!(#7!OR!#11)!#13!!((random*!OR!blind*!OR!"control!group"!OR!placebo*!OR!controlled!OR!cohort*!OR!nonrandom*!OR!observational!OR!retrospective*!OR!prospective*!OR!comparative!OR!comparator!OR!groups!OR!trial*!OR!"systematic!review"!OR!"meta<analysis"!OR!metaanalysis!OR!"literature!search"!OR!medline!OR!cochrane!OR!embase)!AND!(publisher[sb]!OR!inprocess[sb]!OR!pubmednotmedline[sb]))!#14!!#12!and!#13!!TRANSFUSION!EVIDENCE!LIBRARY!Clinical!Specialty:!Gastrointestinal!Disorders!Subject!Area:!Red!Cells!!ClinicalTrials.gov!Conditions/Search!Terms:!GI!bleeding!OR!lower!gastrointestinal!hemorrhage!OR!colorectal!bleeding!OR!colonic!bleeding!OR!intestinal!bleeding!OR!rectal!bleeding!OR!mesenteric!bleeding!OR!hematochezia!OR!melena!OR!bowel!bleeding!OR!diverticular!bleeding!Interventions:!endoscopy!OR!colonoscopy!OR!CT!OR!tomography!OR!proctoscopy!OR!endoclip!OR!colonography!OR!angiography!OR!embolization!OR!capsule!OR!pillcam!!!ICTRP!Conditions/Search!Terms:!GI!bleeding!OR!lower!gastrointestinal!hemorrhage!OR!colorectal!bleeding!OR!colonic!bleeding!OR!intestinal!bleeding!OR!rectal!bleeding!OR!mesenteric!bleeding!OR!hematochezia!OR!melena!OR!bowel!bleeding!OR!diverticular!bleeding!Interventions:!endoscopy!OR!colonoscopy!OR!CT!OR!tomography!OR!proctoscopy!OR!endoclip!OR!colonography!OR!angiography!OR!embolization!OR!capsule!OR!pillcam!!Results!!

! 195!
Relevant!references:!5850!Possibly!irrelevant!references:!2410!(contain!one!or!more!of!the!following!words!in!the!title:!upper!(not!lower),!abdominal!aortic!aneurysm,!cancer,!malignan*,!carcinoma*,!esophageal,!duodenal,!hepatic,!cirrho*,!stomach,!liver,!transplant*,!varice*,!pancreat*)!These!have!been!screened!by!one!reviewer!(KO)!and!identified!40!possible!relevant!references.!These!have!been!added!to!the!‘relevant!references’!for!full!screening!by!two!reviewers.!!!!!!!!

! 196!
Appendix 3: Previously described risk scores for upper and lower gastrointestinal bleeding !
!* Severe haemorrhage defined as requirement of >= 2 units red cells OR decrease in Hct of >=20% in first 24 hours, OR additional transfusion OR further decrease in Hct >=20% after 24 hours of clinical stability OR re-admission with LGIB within one week7
!!!!!!!
Score PRE-ENDOSCOPY ROCKALL66
BLATCHFORD67 BLEED129 AIMS65140 STRATE61 NOBLADS69
Variables Age <60 6-79 >80 Shock No shock HR>100 and SBP>100 SBP<100 Co-morbidity Nil major CHF, IHD, any major morbidity renal failure, liver failure, metastatic cancer
Urea 6.5-8 8-10 10-25 >25 Hb M 12.0 F 10.0-11.9 M 10.0-11.9 (no F) M <10 SBP 100-109 90-99 <90 Other HR>=100 Melaena Syncope Hepatic disease Cardiac failure
On-going bleeding SBP<100 PT>1.2 Erratic mental status Unstable co-morbid disease (defined as organ derangement requiring ICU admission)
Albumin <30g/l INR>1.5 Altered mental status SBP ≤90 Age>65
HR ≥100 SBP ≤115 Syncope Non-tender abdominal examination Bleeding per rectum in first 4 hours of presentation Aspirin use >2 active Charslon co-morbid conditions
NSAIDs No diarrhoea No abdominal tenderness SBP ≤100 Non-aspirin antiplatelet Albumin <30g/l >2 active Charslon co-morbid conditions
Predicted Outcomes
Death and re-bleeding Need for intervention In-hospital complications and mortality
LOS and mortality Severe haemorrhage* used a surrogate marker of patients that will ‘require substantial support and early interventions’*
Severe haemorrhage*, transfusion, LOS, need for intervention

Publishers’+Permissions++Chapter(2:(
Oakland+K,(Isherwood(J,(Lahiff(C,(Goldsmith(P,(Desborough(M,(Colman(KS,(Guy(R,(Uberoi(R,(Murphy(MF,(East(JE,(Hopewell(S,(Jairath(V.(Diagnostic(and(therapeutic(
treatment(modalities(for(acute(lower(gastrointestinal(bleeding:(a(systematic(
review.(Accepted(for(publication,(Endoscopy)International)Open.)(
(
(
(
Chapter(3:(
Oakland+K,(Guy(R,(Uberoi(R,(Seeney(F,(Collins(G,(GrantMCasey(J,(Mortensen(N,(Murphy(M,(Jairath(V(on(behalf(of(the(National(Comparative(Audit(in(Blood(
Transfusion(Lower(Gastrointestinal(Bleeding(Working(Group.+Study(Protocol:(First(nationwide(comparative(audit(of(acute(lower(gastrointestinal(bleeding(in(
the(United(Kingdom.(BMJ)Open.(2016(Aug(4;6(8):e011752.(doi:(10.1136/bmjopenM2016M011752.(
(
‘This&article&was&published&under&a&CC&BY&NC&agreement&meaning&it&can&be&reused,&in&any&non<commercial&way,&without&acquiring&permission&from&BMJ.&The&author&licence&you&agreed&to&also&permits&reuse&in&your&thesis&without&permission.’&&&(
(
(
(
(
(
(

Chapter(4:(
Oakland+K,(Guy(R,(Uberoi(R,(Hogg(R,(Mortensen(N,(Murphy(MF,(Jairath(V(on(behalf(of(the(UK(Lower(GI(Bleeding(Collaborative.(Acute(lower(gastrointestinal(
bleeding(in(the(UK:(patient(characteristics,(interventions(and(outcomes(in(the(
first(nationwide(audit.(Gut.(2017(Feb(1.(doi:(10.1136/gutjnlM2016M313428.((
(
(
07/08/2017 11:31RightsLink Printable License
Page 1 of 4https://s100.copyright.com/App/PrintableLicenseFrame.jsp?publisherID=5…d889e7b5-9566-489d-8528-45319b7ff90c%20%20&targetPage=printablelicense
BMJ PUBLISHING GROUP LTD. LICENSETERMS AND CONDITIONS
Aug 07, 2017
This Agreement between Miss. Kathryn Oakland ("You") and BMJ Publishing Group Ltd.("BMJ Publishing Group Ltd.") consists of your license details and the terms and conditionsprovided by BMJ Publishing Group Ltd. and Copyright Clearance Center.
License Number 4163580507227
License date Aug 07, 2017
Licensed Content Publisher BMJ Publishing Group Ltd.
Licensed Content Publication Gut
Licensed Content Title Acute lower GI bleeding in the UK: patient characteristics,interventions and outcomes in the first nationwide audit
Licensed Content Author Kathryn Oakland,Richard Guy,Raman Uberoi,Rachel Hogg,NeilMortensen,Michael F Murphy,Vipul Jairath
Licensed Content Date Feb 1, 2017
Type of Use Dissertation/Thesis
Requestor type Author of this article
Format Electronic
Portion Figure/table/extract
Number offigure/table/extracts
4
Descriptionoffigure/table/extracts
tables 1, 2, 3, 4
Will you be translating? No
Circulation/distribution 10
Title of your thesis /dissertation
ACUTE LOWER GASTROINTESTINAL BLEEDING IN THE UNITEDKINGDOM
Expected completion date Aug 2017
Estimated size(pages) 150
Requestor Location Miss. Kathryn Oakland63 Horton Road
London, SL59HDUnited KingdomAttn: Miss. Kathryn Oakland
Publisher Tax ID GB674738491
Billing Type Invoice
Billing Address Miss. Kathryn Oakland63 Horton Road

(
Chapter(6:(
Oakland+K+and(Jairath(V,(Uberoi(R,(Guy(R,(Ayaru(L,(Mortensen(N,(Murphy(MF,((Collins(GS.(Safe(discharge(after(acute(lower(gastrointestinal(bleeding:(derivation(
and(validation(of(a(novel(risk(score.(Lancet)Gastroenterology)and)Hepatology,(2017(Jun(23(doi:(10.1016/S2468M1253(17)30150M4(
(
(
07/08/2017 11:36Doctors.net.uk Webmail :: RE: THELANCETGASTROHEP-D-17-00175R2: Your manuscript for The Lancet Gastroenterology & Hepatology
Page 1 of 3https://webmail.doctors.org.uk/?_task=mail&_action=print&_uid=22244&_mbox=INBOX&_safe=1&_extwin=1
Subject RE: THELANCETGASTROHEP-D-17-00175R2: Your manuscript for The Lancet Gastroenterology & HepatologyFrom Brierley, Robert (ELS-LOW) <[email protected]>To Kate Oakland <[email protected]>Date 2017-07-07 12:49
Dear Kate
Apologies for the delay in getting back to you; I had to run this past a couple of the other Lancet editors. This is absolutely fine—good luck with the writeup!
Best wishes
Rob
Rob BrierleyEditor-in-Chief, The Lancet Gastroenterology & Hepatologyhttp://www.thelancet.com/gastrohephttps://twitter.com/LancetGastroHep
From: Kate Oakland [mailto:[email protected]]Sent: 06 July 2017 14:22To: Brierley, Robert (ELS-LOW)Subject: Re: THELANCETGASTROHEP-D-17-00175R2: Your manuscript for The Lancet Gastroenterology & Hepatology
Hi Rob,
Apologies for being unclear. The thesis will contain the original word version of the submitted article (minus corrections, journal edits, etc as I cannot claim these as my own work), plus an expanded methods section. It will also reference the journal article in full, including the URL.
Is this permissible?
Many thanks
KateSent from my iPhone
On 6 Jul 2017, at 13:55, Brierley, Robert (ELS-LOW) <[email protected]<mailto:[email protected]>> wrote:Dear Kate
Sorry, I am still not entirely clear on the requirements here – and apologies if I’m just missing something obvious! Hosting the word document of the paper on the Imperial server will require it to be identical in terms of text to the main paper (rather than having shared content). We will provide the document for you, exporting it direct from our production software. However, the posted word document should be independent from any upload of your thesis (although you can obviously cite both the published paper and the URL for the word version in the thesis).
Best,
Rob
Rob BrierleyEditor-in-Chief, The Lancet Gastroenterology & Hepatologyhttp://www.thelancet.com/gastrohephttps://twitter.com/LancetGastroHep
From: Kate Oakland [mailto:[email protected]]Sent: 06 July 2017 13:25To: Brierley, Robert (ELS-LOW)Subject: Re: THELANCETGASTROHEP-D-17-00175R2: Your manuscript for The Lancet Gastroenterology & Hepatology
Thanks Rob,
I can confirm it will be latter: word document, not identical to the original PDF, but some shared content.
BW
KateSent from my iPhone
On 6 Jul 2017, at 11:41, Brierley, Robert (ELS-LOW) <[email protected]<mailto:[email protected]>> wrote:Dear Kate
Thank you for your email. By “reprint”, do you mean actually include the laid out, final PDF version of the paper in the thesis? If so, I’m afraid the copyright agreement for the article means that this is not permitted. You are entitled to post a word-processed document (not the published journal article as PDF) of the peer-reviewed, accepted, and edited article on personal or institutional websites any time after publication in print or online, provided the word document also contains a link to the paper on thelancet.com<
Best wishes
Rob
Rob BrierleyEditor-in-Chief, The Lancet Gastroenterology & Hepatologyhttp://www.thelancet.com/gastrohephttps://twitter.com/LancetGastroHep
From: Hook, Kayleigh (ELS-LOW)
From: [email protected]<mailto:[email protected]> [mailto:[email protected]]Sent: 05 July 2017 12:33To: Hook, Kayleigh (ELS-LOW) <[email protected]<mailto:[email protected]>>Subject: RE: THELANCETGASTROHEP-D-17-00175R2: Your manuscript for The Lancet Gastroenterology & Hepatology
Thanks Kayleigh!
I am currently writing my MD thesis at Imperial, and our risk score paper is a feature of this work. It is possible to be granted permission to reprint the article in my thesis?
The thesis will be added to Spiral, Imperial's institutional repository http://spiral.imperial.ac.uk/ and made available to the public under a Creative Commons Attribution-NonCommercial-NoDerivs licence.
I hope this is ok?

(
(
+(
(
(
(