acute traumatic first-time anterior shoulder dislocation : post-reduction and rehabilitation (ebm...
TRANSCRIPT
Acute Traumatic First-time Anterior Shoulder
Dislocation : Post-reduction and Rehabilitation
(EBM Appraisal)
Nadhaporn SaengpetchDivision of Sports Medicine,
Department of Orthopaedics, Faculty of Medicine Ramathibodi Hospital
Mahidol University
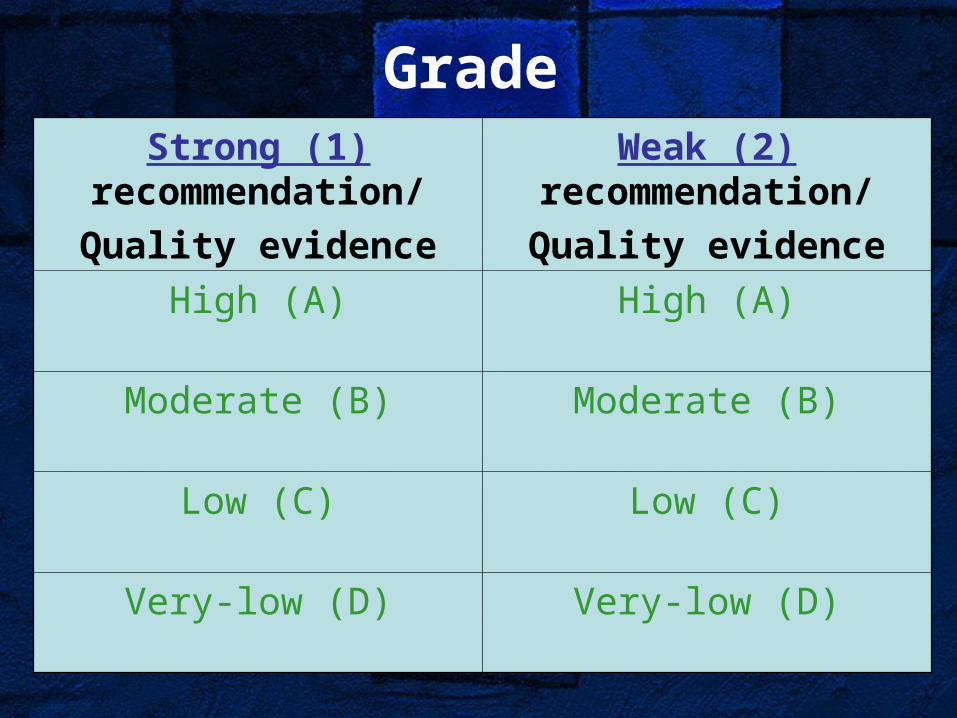
GradeStrong (1)
recommendation/Quality evidence
Weak (2) recommendation/Quality evidence
High (A) High (A)
Moderate (B) Moderate (B)
Low (C) Low (C)
Very-low (D) Very-low (D)

The Points of View
•Immobilization techniques•Duration of immobilization•Post-reduction rehabilitation•Functional outcomes and risk factors

Raymond A. Sachs, MD,Southern California Permanente Medical Group, El
Cajon, CA
…Like other surgeons, we love to operate and feel that we can “fix” almost anyone. It takes restraint to allow the natural history of shoulder instability to play out….

Immobilization Techniques

Sling VS No-sling
•questionable benefit•no difference in the recurrence rate and did not change the prognosis
•N=257 •Sling immobilization (the torso bandage) 3-4 weeks VS early motion•25-year follow-up•DASH questionnaire + x-ray both shoulders•Recurrence, GT fracture, age, activity, gender, contralateral dislocation

•Recurrence occurred in the first 15 years•Become stable overtime (stabilized spontaneously) in the last 10 years•Immobilization after the primary dislocation did not change the prognosis•Prognostic Level 1•Weak recommendation, high-quality evidence(Hovelius L J Bone Joint Surg Am 2008;90:945-52)

Types of Sling
•Better coaptation of the Bankart lesion with the shoulder in external rotation than internal rotation
(Itoi E JBJS Am 2001;83(5): 661-7)

•Evaluation 4 commercial braces which maintain in external rotation•Healthy subjects•Initial external rotation measurement, simulated ADL, reapplication of brace, rate of the comfort

•Rigid orthoses were most successful•dj Ultrasling ER: the most comfortable •No brace was successful in achieving its anticipated degree of external rotation
•Therapeutic Level IV•Weak recommendation, moderate quality evidence
$82 $52
$405 $284
(Sullivan LG Arthroscopy 2007;23(2):129-34)

Position: cadaver
•10 human cadaveric shoulders•Measuring contact force between the labrum and the glenoid•Humeral arc of rotation from IR 60º-neutral-ER 45º

•No contact force with the arm in IR•Forces increased as the arm passed to neutral and reached a maximum at ER 45º (83.5g)•ER significantly increased the labrum-glenoid contact force and may influence the healing of a Bankart lesion•Prognostic Level IV•Weak recommendation, low quality of evidence(Miller BS J Shoulder Elbow Surg 2004;13:589-92)

Position: MRI
•19 shoulders (first time=6, recur=13)•Plain MRI: fast-spin-echo T2 weighted axial images•MR arthrography: spin-echo T1 weighted axial images•Assessed the coaptation by measurement of the detached area, opening angle and detached length

•D and S were both lesser with ER than IR
•A detached area, angle and length were significantly lesser with ER
Displacement & separation
Detached area, angle & length

(Itoi E J Bone Joint Surg Am 2001; 83(5):661-7)
•ER immobilization better approximates the Bankart lesion to the glenoid neck than does the conventional•Prognostic Level I•Weak recommendation, high quality of evidence

Position
•159 shoulders (ER=85, IR=74)•Immobilized for 3 weeks, F/U >2 yrs•Recurrent rate, compliance, return to sports, complication•Subgroup analysis: younger pts (<30 yrs) with early immobilization had significantly lower recurrence rate

•ER immobilization had lesser recurrence rate (esp. perform in day1), return to pre-injury sports activity level, better compliance •ER immobilization reduces the risk of recurrence and particularly beneficial for pts < 30 yrs old •Therapeutic Level II•Weak recommendation, moderate quality of evidence (Itoi E J Bone Joint Surg Am 2007;89:2124-31)

AlcareTM, Tokyo, Japan

Duration of Immobilization

Fact
•The Bankart lesion has an ability to heal•Controversial for duration of immobilization•Position is more important than duration

•216 pts, prospective study 2 yrs•Sling/swathe 3-4 wks/sling 1-3 wks/sling 1 wk + avoid ABER 3 wks •Age group (<22, 23-29,30-40), recurrence rate, associated fractures

• Recurrence varied in 3 age groups but did not vary according to methods
• Recurrence depends on age more than duration of immobilization
• Prognostic Level II• Strong recommendation,
moderate quality of evidence
(Hovelius L J Bone Joint Surg Am 1983;65: 343-9)

Post-reduction Protocol

Physiotherapy
•Shoulder muscles contribute to both mobility and stability of the joint•Instability is specific to certain end-range positions•To improve treatment, we should focus the contribution of the muscles to glenohumeral joint stability in clinically relevant position.

Concavity-compression Mechanism
•Compression of the humeral head against the concave glenoid allows concentric rotation of the humeral head on the glenoid•Mid range: Muscles may be the primary stabilizers of the shoulder joint while the capsuloligamentous structures are lax•End range: Muscles act to protect the capsuloligamentous structures by limit the joints motion & decrease strain in these structures
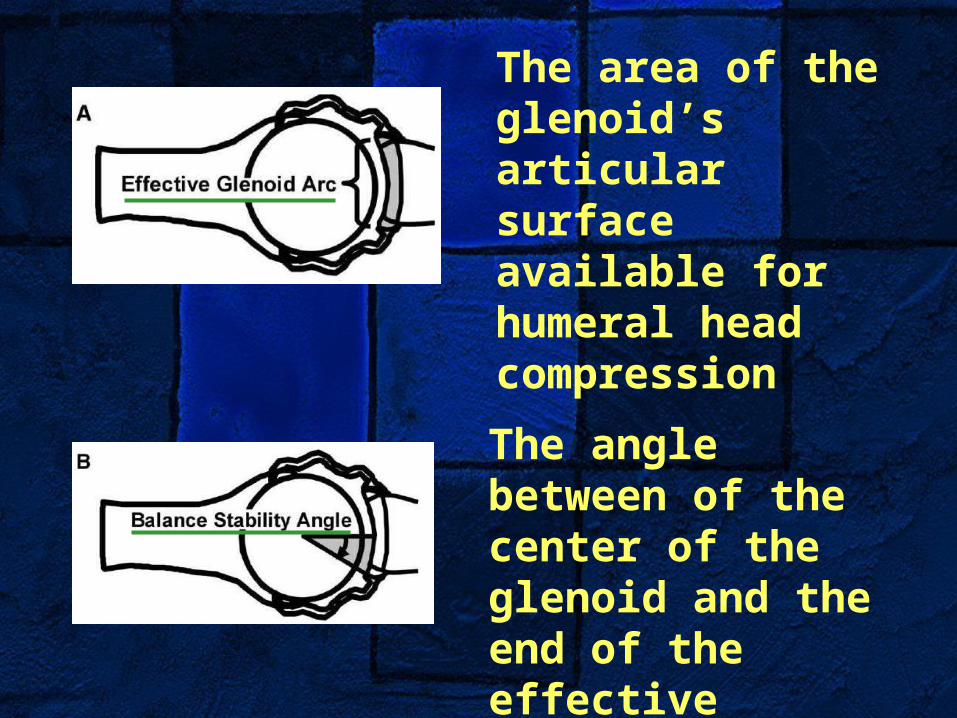
The area of the glenoid’s articular surface available for humeral head compression
The angle between of the center of the glenoid and the end of the effective glenoid arc
Shoulder Muscle andGlenohumeral Stability
• 50% decrease in the rotator cuff muscle 50% increase displacement of the head in all joint positions
(Wuelker N J Shoulder Elbow Surg 1998;7:43-52)
• Deltoids and pectoralis major decrease stability of the shoulder joint
• Bench-press: anterior deltoid and p. major spasm and led to dislocate
(Arciero RA J Shoulder Elbow Surg 1997;6:318-20)

•To determine the effect of increasing magnitude of individual muscle forces on the line of resultant forces•Lines of action were less anteriorly directed when magnitude of SST, IST or TMi were increased, tending to improve the stability
(Labriola JE J Shoulder Elbow Surg 2004;14(1S):32S-38S)
Shoulder Muscles Training

•In end-range: simulated in RC forces tended to improve stability whereas increased deltoid or p. major tended to decrease stability•Therapeutic Level IV•Strong recommendation, moderate quality of evidence

Modality Uses
•30 in-season athletes (first time =21)•Early mobilization, physical therapy and bracing•26/30 returned to their sports for the complete season at 10.2 days•Average 1.4 recur episodes/season/pts

•Range of motion exercises•wand exercises, strengthening the RC with free-weight•Periscapular strengthening
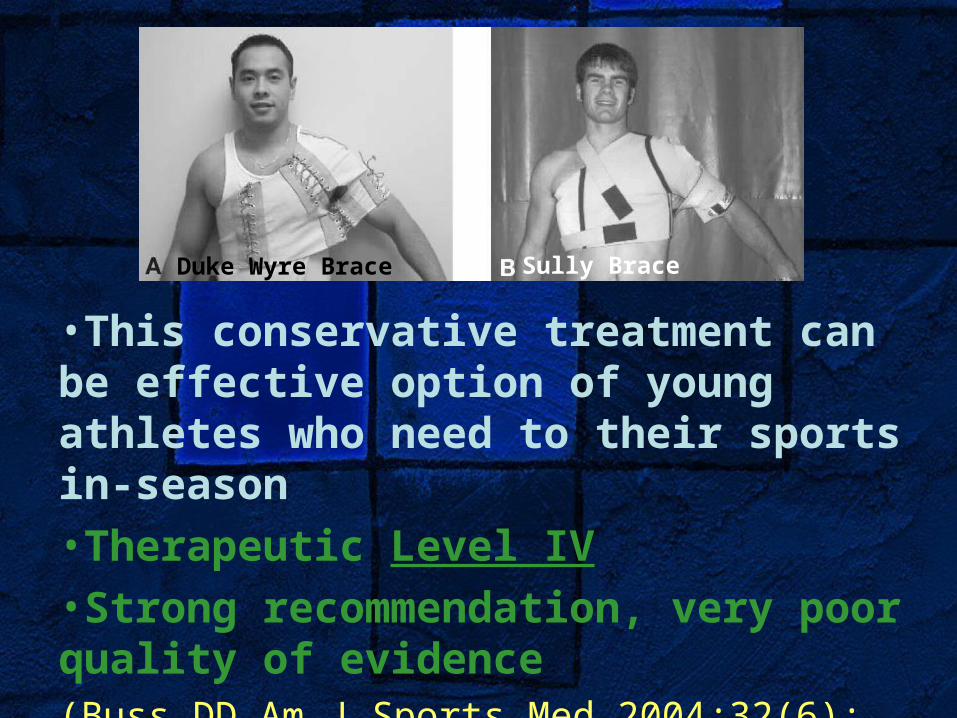
•This conservative treatment can be effective option of young athletes who need to their sports in-season•Therapeutic Level IV•Strong recommendation, very poor quality of evidence(Buss DD Am J Sports Med 2004;32(6): 1430-3)
Duke Wyre Brace Sully Brace

Prognostic Factors

Prognostic Factors
•Subcoracoid is a worse prognosis compare to axillary dislocation•Age on first-time dislocation•Associated disruption of soft-tissue envelope or osseous restraints
(Hovelius L J Bone Joint Surg Am 2008;90:945-52)

•538 pts, prospective observational cohort study, follow-up 3 yrs•3.2% sustained early redislocation within 6 wks•High energy injury(13.7), neurologic deficit(2.0), large RC tear(29.8), glenoid rim(7.0)/GT fracture(33.5)

•First-time dislocators who have severe disruption of RC (tear) or fracture of glenoid/humeral head is high risk for redislocation•Prognostic Level III•Strong recommendation, moderate quality of evidence (Robinson CM J Bone Joint Surg Am 2002;84:1552-9)

Conclusion•Immobilization: many evidence suggested that conventional position could not reach the best anatomic healing
immobilization in ER is more hazardous and awkward for people
need a good quality RCT study and independent investigators for ER/IR immobilization

Conclusion
•Duration: inconclusive for exact time of immobilization but shorter period is preferable•Post-reduction: selective shoulder muscles training is advisable

Thank you