acute stroke it’s not just t-pa the basics. nina t. gentile, md associate professor department of...
TRANSCRIPT

Acute StrokeAcute Stroke
It’s Not Just t-PA
The BasicsThe Basics

Nina T. Gentile, MDNina T. Gentile, MD
Associate Associate ProfessorProfessor
Department of Emergency Department of Emergency MedicineMedicine
Temple University Hospital Temple University Hospital & School of Medicine& School of Medicine
Philadelphia, PAPhiladelphia, PA
Nina T. Gentile, MD, FAAEM

Nina T. Gentile, MD, FAAEM
Stroke BasicsStroke Basics
• How important is blood pressure control? • How do early ischemic changes on CT
impact on decision-making and treatment?
• What roles do aspirin and heparin play?• Is hyperglycemia really a problem?• What are the indications for immediate
transfer?

Nina T. Gentile, MD, FAAEM
Case ExampleCase Example
• 72-year-old woman
• History: hypertension, diabetes
• Sudden slurred speech, left facial droop, left-sided weakness
• Family calls 911

Nina T. Gentile, MD, FAAEM
Case ExampleCase Example
• ACLS squad dispatched, evaluates, transports patient to nearest ED
• En route the squad notifies the receiving hospital of a possible stroke patient
• And asks….

““Hey Doc… Hey Doc… How About Aspirin?”How About Aspirin?”
“Isn’t it…
…the sooner the better?”
Nina T. Gentile, MD, FAAEM

Nina T. Gentile, MD, FAAEM
Aspirin in Stroke Meta-AnalysisAspirin in Stroke Meta-Analysis
• 41,399 subjects • Nine trials• For every 1,000 patients…
…7 fewer early recurrent strokes …13 fewer dead or dependent at 6
months…~ 2 intracerebral bleeds

Nina T. Gentile, MD, FAAEM
Aspirin Trials for StrokeAspirin Trials for Stroke
• International Stroke Trial (IST)
• Chinese Acute Stroke Trial (CAST)
• Treatment within 48 hours• IST time to treatment: 19 hours
• CAST time to treatment: 25 hours

Nina T. Gentile, MD, FAAEM
International Stroke TrialInternational Stroke Trial
• 19,435 patients
• 300 mg/d aspirin within 48 hours of stroke onset
• Slightly fewer deaths at 14 days: 9.0% vs 9.44%, p=.02, NNT =91

2.8%3.9%
0.9%
0.8%
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
Aspirin Avoid Aspirin
HemorrhagicIschemic
IST – 14 DAY OUTCOME
p=.05
p=.05

36.5%38.8%
2022242628303234363840
Aspirin Avoid Aspirin
Dead or Dependent
IST – 6 MONTH OUTCOME
p=.05

Nina T. Gentile, MD, FAAEM
Chinese Acute Stroke TrialChinese Acute Stroke Trial
• 21,106 patients
• 160 mg/d dose within 48 hours of stroke onset
• Primary end points:
• Death at 4 weeks
• Death or dependence at discharge
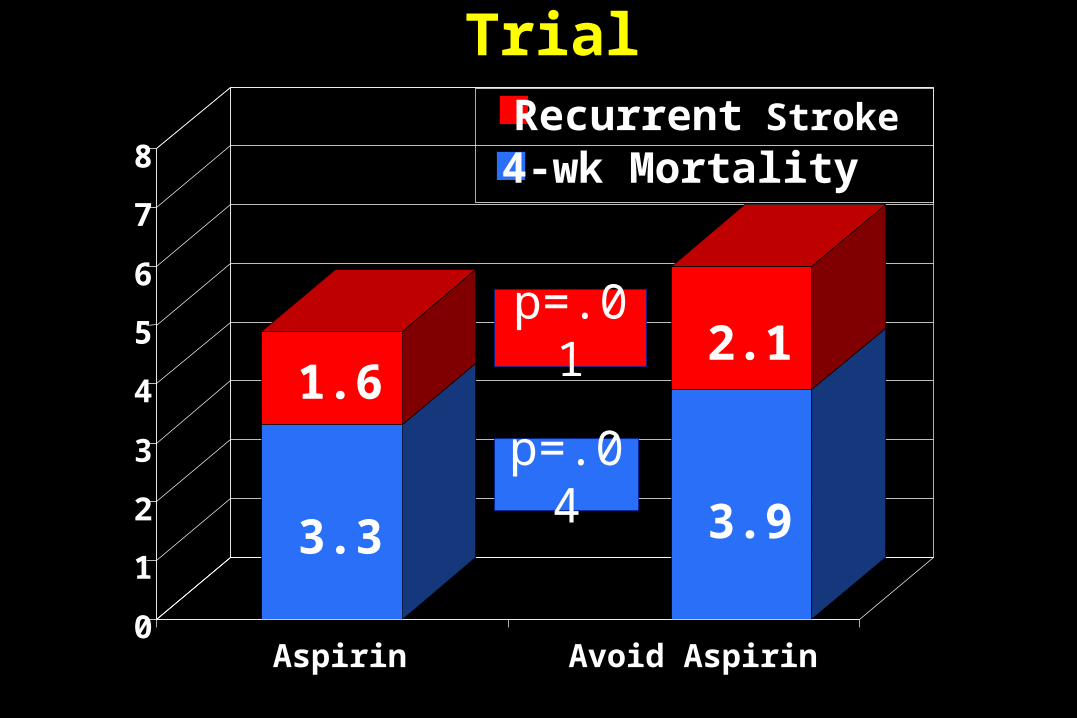
Chinese Acute Stroke TrialChinese Acute Stroke Trial
3.3
1.6
3.9
2.1
0
1
2
3
4
5
6
7
8
Aspirin Avoid Aspirin
Recurrent Stroke
4-wk Mortality
p=.01
p=.04

Chinese Acute Stroke TrialChinese Acute Stroke Trial
30.5% 31.6%
20
22
24
26
28
30
32
34
36
Aspirin Avoid Aspirin
Dead or Dependent
p=.08

Nina T. Gentile, MD, FAAEM
Aspirin in Acute Stroke: <6 HoursAspirin in Acute Stroke: <6 Hours
• Not studied ICH when used with lytic
• Early thrombolytic trials
• Phase IV trials

Nina T. Gentile, MD, FAAEM
Thrombolysis: Early StudiesThrombolysis: Early Studies
• ASK (1996): SK or Placebo plus ASA within 4 hours of symptom onset
SK +ASA ASA
Mortality 36% 20%
HT or Hematoma
32% 17%

Nina T. Gentile, MD, FAAEM
Thrombolysis: Early StudiesThrombolysis: Early Studies
• MAST- I (1995): within 6 hours of symptom onset• streptokinase,
• aspirin,
• both or
• neither

Nina T. Gentile, MD, FAAEM
Thrombolysis: MAST-IThrombolysis: MAST-I
Therapy 10-Day Mortality Streptokinase 27%Aspirin 12%Both 34%*Neither 13%
*OR 3.5; 95% CI 1.9-6.5; 2p < 0.00001OR 3.5; 95% CI 1.9-6.5; 2p < 0.00001

Nina T. Gentile, MD, FAAEM
Phase IV: IV t-PA in StrokePhase IV: IV t-PA in Stroke
The Cleveland Area Experience
• Symptomatic ICH: 15.7%
• Protocol violation: 50%• Received aspirin within 24 hours: 37%

Nina T. Gentile, MD, FAAEM
Phase IV: IV t-PA in StrokePhase IV: IV t-PA in Stroke
STARS 2000• Symptomatic ICH: 3.3%• Asymptomatic ICH: 8.2% • Protocol violation in 33%
• rt-PA >180 minutes: 13%• Received aspirin or anticoagulant
within 24 hours: 9%

Nina T. Gentile, MD, FAAEM
Aspirin in Acute StrokeAspirin in Acute Stroke
• Recommendation: 160 to 325 mg/day within 24 to 48 hours
• Avoid in potential candidates for thrombolytic therapy
• Delay for at least 24 hours after the administration of rt-PA
• Do not administer prehospital (i.e. pre-CT)

Nina T. Gentile, MD, FAAEM
Our Patient Arrives…Our Patient Arrives…
• Right gaze preference
• Left face droop
• Dysarthria
• Left arm paresis
• Mild left side neglect

Nina T. Gentile, MD, FAAEM
Three Questions…Three Questions…
• Is this a stroke?
• How would you quantify or describe the stroke?
• Would you give t-PA?

Nina T. Gentile, MD, FAAEM
Differential DiagnosisDifferential Diagnosis
• Intracerebral hemorrhage
• Hypoglycemia
• Hyperglycemia
• Seizure
• Migraine headache
• Hypertensive crisis
• Tumor
• Meningitis
• Encephalitis
• Brain abscess

Nina T. Gentile, MD, FAAEM
‘‘Misdiagnosis of Stroke’Misdiagnosis of Stroke’
• 821 patients admitted to acute stroke unit
• 108 (13%) incorrect diagnosis• Seizure: 39%
• Confusional states, syncope: 24%
Lancet. 1982 Feb 6;1(8267):328-31Lancet. 1982 Feb 6;1(8267):328-31

Nina T. Gentile, MD, FAAEM
Stroke Mimics: Libman 1995Stroke Mimics: Libman 1995
• Evaluator: stroke team• Studies: history, physical• Misdiagnosis: 19%• Mimics identified: seizure, infection, tumor,
metabolic, positional vertigo, cardiac syncope, subdural, C- spine fracture, transient amnesia, conversion disorder, MS, myasthenia gravis, parkinsonism, hypertensive encephalopathy

Nina T. Gentile, MD, FAAEM
Stroke Mimics: Kothari 1995Stroke Mimics: Kothari 1995
• Evaluator: emergency physician
• Studies: history, physical, CT
• Misdiagnosis: 4%
• Mimics identified: paresthesia, seizure, migraine, neuropathy, psychogenic, others

Nina T. Gentile, MD, FAAEM
Stroke Mimics: Allder 1999Stroke Mimics: Allder 1999
• Evaluator: neurologist
• Studies: history, physical, CT
• Misdiagnosis: 9%
• Mimics identified: metabolic, migraine, conversion disorder, withdrawal

Nina T. Gentile, MD, FAAEM
Stroke Mimics: Ay 1999Stroke Mimics: Ay 1999
• Evaluator: neurologists
• Studies: history, physical, CT
• Misdiagnosis: 1.2%
• Mimics identified: seizure, migraine, tumor, transient global amnesia

Nina T. Gentile, MD, FAAEM
NIH Stroke Scale (NIHSS)NIH Stroke Scale (NIHSS)
• Designed as research tool
• Widely used in clinical practice
• Good interobserver reliability
• Helps predict outcome

Nina T. Gentile, MD, FAAEM
NIH Stroke Scale (NIHSS)NIH Stroke Scale (NIHSS)
• Helps assess risk of hemorrhage after t-PA treatment
• Provides quantitative mechanism for following individual patient

Nina T. Gentile, MD, FAAEM
Our Patient’s NIHSS Score (Part 1)Our Patient’s NIHSS Score (Part 1)
00-4Motor Arm Right6
30-4Motor Arm Left5
20-3Facial Palsy4
00-3Best Visual3
10-2Best Gaze2
10-2LOC Commands1c
10-2LOC Questions1b
10-3Level of
consciousness1a
Pt scoreRangeDescriptionItem

Nina T. Gentile, MD, FAAEM
Our Patient’s NIHSS Score (Part 2)Our Patient’s NIHSS Score (Part 2)
00-3Best Language13
10-2Dysarthria12
10-2Neglect11
10-2Sensory10
00-2Limb Ataxia9
00-4Motor Leg Right8
10-4Motor Leg Left7
Pt scoreRangeDescriptionItem
Total = 13

Nina T. Gentile, MD, FAAEM
Would you Give t-PA?Would you Give t-PA?
• Potential Benefit
• Potential Risks
• Exclusion Criteria• Historical features
• CT findings

Nina T. Gentile, MD, FAAEM
IV t-PA: Potential BenefitIV t-PA: Potential Benefit
• 2775 patients in 6 trials
Odds of favorable 3-mo outcome
0-90 2.8 1.8-4.5
91-180 1.6 1.1-2.2
181-270 1.4 1.1-1.9
271-360 1.2 0.9-1.5
Lancet. 2004

Nina T. Gentile, MD, FAAEM
IV t-PA for Stroke: Meta-analysisIV t-PA for Stroke: Meta-analysis
Stroke. 2005

Nina T. Gentile, MD, FAAEM
Complete Resolution in 24 HoursComplete Resolution in 24 Hours
0
5
10
15
20
25
t-PA placebo
(NIHSS(NIHSS<<1)1)

Nina T. Gentile, MD, FAAEM
NINDS 1 Year Follow-up NINDS 1 Year Follow-up
01020304050607080
<9 10-14 15-20 >20
t-PAPlacebo
Favo
rabl
e O
utco
me
Presenting NIHSS Score

Nina T. Gentile, MD, FAAEM
IV t-PA: Potential RiskIV t-PA: Potential Risk
• Intracranial hemorrhage• Pooled analysis of 2775 patients
treated within 6 hours of sx onset
• rt-PA: 82 (5.9%)
• Placebo:15 (1.1%)

Nina T. Gentile, MD, FAAEM
Clinical Exclusion CriteriaClinical Exclusion Criteria
Bleeding Risk• Active GI or GU
bleeding • Bleeding Diathesis
• PLT < 100K• INR > 1.7 PTT
• Potential Major Bleeding Site
BP sys>185, dias >110
• Stroke Mimic• BS < 50, > 400• Seizure at onset
• Rapidly improving or minor symptoms

Nina T. Gentile, MD, FAAEM
CT Exclusion Criteria: Blood CT Exclusion Criteria: Blood

Nina T. Gentile, MD, FAAEM
Early Ischemic ChangesEarly Ischemic Changes
• Loss of insular ribbon
• Loss of gray-white interface
• Loss of sulci • Acute hypo density • Mass effect • Dense MCA sign

Nina T. Gentile, MD, FAAEM
Early Ischemic ChangesEarly Ischemic Changes
Sylvian Fissure
Insular Cortex

Nina T. Gentile, MD, FAAEM
Early Ischemic ChangesEarly Ischemic Changes
• Loss of insular ribbon
• Loss of gray-white interface
• Loss of sulci • Acute hypo density • Mass effect • Dense MCA sign

Nina T. Gentile, MD, FAAEM
Early Ischemic ChangesEarly Ischemic Changes
• Loss of insular ribbon • Loss of gray-white
interface
• Loss of sulci • Acute hypo density • Mass effect • Dense MCA sign

Nina T. Gentile, MD, FAAEM
• Loss of insular ribbon ()• Loss of gray-white
interface ()
• Loss of sulci ( )• Acute hypodensity • Mass effect • Dense MCA sign
Early Ischemic ChangesEarly Ischemic Changes

Nina T. Gentile, MD, FAAEM
Early Ischemic ChangesEarly Ischemic Changes
• Loss of insular ribbon • Loss of gray-white
interface • Loss of sulci
• Acute hypodensity
• Mass effect • Dense MCA sign

Nina T. Gentile, MD, FAAEM
Early Ischemic ChangesEarly Ischemic Changes
• Loss of insular ribbon • Loss of gray-white
interface • Loss of sulci • Acute hypo density • Mass effect
• Dense MCA sign

Nina T. Gentile, MD, FAAEM
“No hemorrhage…
…large area of hypoattenuation with edema….”
Would You Give t-PA to Our Patient?Would You Give t-PA to Our Patient?

Nina T. Gentile, MD, FAAEM
Review the FactsReview the Facts

Nina T. Gentile, MD, FAAEM
SignificanceSignificance
Early ischemic changes can…
…assist in decision-making
…predict outcome
…predict ICH

Nina T. Gentile, MD, FAAEM
EIC Assists Decision-MakingEIC Assists Decision-Making
…findings change over time
…are correlated with perfusion deficits

Nina T. Gentile, MD, FAAEM
Early Ischemic ChangesEarly Ischemic Changes
Nina T. Gentile, MD, FAAEM
EIC Predicts OutcomeEIC Predicts Outcome
43 patients, t-PA (30-100 mg)
PPV for death
• Hypodensity > 50% MCA: 85%
• Local brain swelling: 70%
• Hyperdense MCA: 32%
Amer J Neurorad 1994Amer J Neurorad 1994

Nina T. Gentile, MD, FAAEM
EIC Predict OutcomeEIC Predict OutcomeFavors tPAFavors Placebo
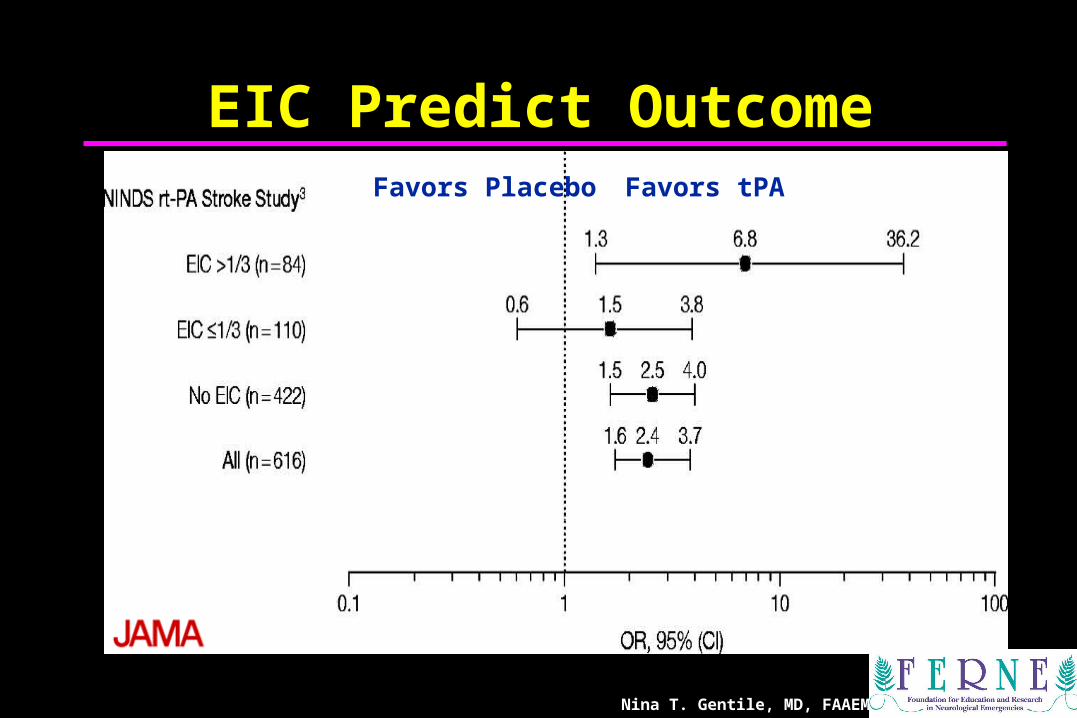
Nina T. Gentile, MD, FAAEM
EIC Predict OutcomeEIC Predict OutcomeFavors tPAFavors Placebo

Nina T. Gentile, MD, FAAEM
EIC Predicts ICHEIC Predicts ICH
ECASS I• If >1/3 MCA involvement: increased
risk of bleed• OR 3.6, 95% CI, 2.3 to 5.3
NINDS• Only CT exclusion: hemorrhage• No association with EIC extent

Nina T. Gentile, MD, FAAEM
What To Look For On CT What To Look For On CT
• Any signs of blood
• Hypodensity >1/3 MCA territory
• EICs difficult to appreciate • Should not dissuade use of
appropriate therapy
• Correlate with the history

Neurology Resident: Neurology Resident: “Oh no…she’ll be sure to bleed “Oh no…she’ll be sure to bleed
with t-PA….with t-PA….Let’s start Heparin instead.”Let’s start Heparin instead.”
We “have to do something”
Nina T. Gentile, MD, FAAEM

Nina T. Gentile, MD, FAAEM
Potential IndicationsPotential Indications
• Cardioembolic Stroke
• Progressing Stroke
• Stroke due to documented large-artery stenosis
• Arterial Dissection

Nina T. Gentile, MD, FAAEM
IV AdministrationIV Administration
• 225 patients• IV Heparin vs Placebo for 7 days• No difference at 7 days, 3 mos, 1yr
• stroke progression • functional activity
• More patients in heparin group died at 1 year
Ann Intern Med. 1986 Dec;105(6):825-8

Nina T. Gentile, MD, FAAEM
SubQ Heparin:IST
• 19,435 Patients
• 4 Groups: • ASA, Heparin 5,000U or 12,500U bid,
Both, or Neither
• 1o Outcome: • Death at 14 days
• Death or dependency at 6 mos

Nina T. Gentile, MD, FAAEM
IST
9.0 9.3
5
6
7
8
9
10
Heparin Avoid Heparin
14-Mortality (NS)

Nina T. Gentile, MD, FAAEM
IST
Heparin Avoid Heparin0
62.9 62.9
10203040506070
6-mo Dead/Dependent (NS)

Nina T. Gentile, MD, FAAEM
IST: No Net BenefitIST: No Net Benefit
0
2.93.8
1.40.4
1
2
3
4
5
Heparin Avoid Heparin
Ischemic Hemorrhagic
Nina T. Gentile, MD, FAAEM
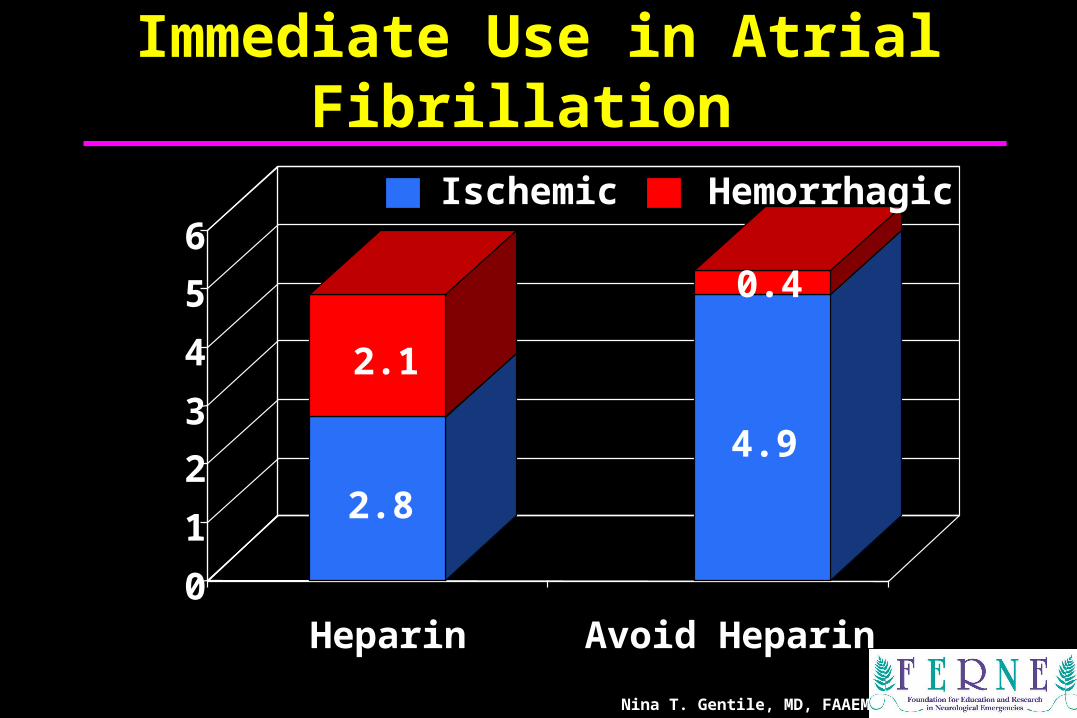
Immediate Use in Atrial Fibrillation Immediate Use in Atrial Fibrillation
0
1
2
3
4
5
6
Heparin Avoid Heparin
2.8
4.9
Ischemic
2.1
0.4
Hemorrhagic

Nina T. Gentile, MD, FAAEM
EUSI and AHA:EUSI and AHA:Heparin in StrokeHeparin in Stroke
1. No recommendation for general use of heparin, LMWH or heparinoids after
ischemic stroke (Level I)
2. Full dose heparin for selected indications such as AF, other cardiac sources with
high risk of re-embolism, arterial dissection, or high grade arterial stenosis (Level IV)
3. DVT-prophylaxis

Nina T. Gentile, MD, FAAEM
What are the Options?What are the Options?
• Intravenous t-PA
• Excluded from Thrombolytics• Nothing
• Aspirin
• Heparin
• Intra-arterial thrombolysis

Nina T. Gentile, MD, FAAEM
Neuroimaging Neuroimaging
• Assessment of blood flow and tissue viability• CT Angiography
• MRI with perfusion imaging

Nina T. Gentile, MD, FAAEM
MRIMRI
Acute CBFDWI

Nina T. Gentile, MD, FAAEM
72-yr-old Right MCA stroke72-yr-old Right MCA stroke• 5:05 Angiography reveals multiple thrombi
proximal MCA and segmental arteries• 5:25 Microangiocatheter IA t-PA
administration• 6:30 Patient goes to ICU

Nina T. Gentile, MD, FAAEM
10-day T2
MRIMRI
Acute CBF DWI

Nina T. Gentile, MD, FAAEM
72-yr-old S/P t-PA72-yr-old S/P t-PA
• Day 2: PT and speech therapy started
• Day 10: Hospital discharge to resume managing her brokerage company
Stroke Survivors.com

Nina T. Gentile, MD, FAAEM
Case #2Case #2
• 43 year old black male with headache, right sided face, arm, leg weakness and vertigo x 30 minutes
• PMH: Hypertension, diabetes
• Exam: Dysarthria, profound weakness and ataxia

Nina T. Gentile, MD, FAAEM
Initial Vital SignsInitial Vital Signs
• BP: 220/120 mm Hg
• Pulse: 64 regular
• Resp Rate: 24 regular
• Accucheck: 428 mg%

Nina T. Gentile, MD, FAAEM
Severe HypertensionSevere Hypertension
• What is the optimal BP?
…with fibrinolytic therapy?
• When to initiate treatment?
• Which antihypertensive?

Nina T. Gentile, MD, FAAEM
Severe HypertensionSevere Hypertension
• Worsens cerebral blood flow
• Decreases odds of full recovery
• Promotes hemorrhagic transformation and ICH after t-PA
Dutka, 1987
Chamorro,1998

Nina T. Gentile, MD, FAAEM
OptOptimal BP imal BP
• No controlled studies to guide
• “Permissive hypertension”• Target BP in patients with prior
hypertension: 180 / 100-105 mmHg• Target BP in previously normotonic
patients: 160-180 / 90-100 mmHg
• Avoid hypotension, drastic reductions in BP

Nina T. Gentile, MD, FAAEM
BP Management:BP Management:
• Systolic<220 or Diastolic<120• Observe
• Except with end-organ involvement (aortic dissection,AMI,pulmonary edema, hypertensive encephalopathy)
Not Eligible for Thrombolytic Therapy 1Not Eligible for Thrombolytic Therapy 1

Nina T. Gentile, MD, FAAEM
• Systolic>220 or Diastolic 121–140Labetalol 10–20 mg IV; may repeat Q 10 min (max 300 mg) Nicardipine 5 mg/hr IV initial dose;
increase 2.5 mg/hr Q 5 min (max 15 mg/hr)
• Diastolic>140Nitroprusside 0.5 µg/kg/min IV infusion
initial dose, titrate
BP Management:BP Management:Not Eligible for Thrombolytic Therapy 2Not Eligible for Thrombolytic Therapy 2

Nina T. Gentile, MD, FAAEM
• Systolic >185 or Diastolic >110Labetalol 10–20 mg IV over 1–2
min, may repeat x 1Nicardipine 5 mg/hr IV initial dose; increase 2.5 mg/hr Q 5 min (max 15 mg/hr)Nitropaste 1–2 inches
***If BP systolic>185 or diastolic>110, do not give r-TPA***
BP Management:BP Management:Pretreatment for Thrombolytic TherapyPretreatment for Thrombolytic Therapy

Nina T. Gentile, MD, FAAEM
• Diastolic >140: Nitroprusside
0.5 µg/kg/min IV initial dose and titrate
• Systolic 180-230 or Diastolic 105–140:
- Labetalol bolus then drip at 2-8 mg/min
- Nicardipine 5 mg/hr IV initial dose,
2.5 mg/hr Q 5 min (max15 mg/hr)
BP Management:BP Management:During & After Thrombolytic TherapyDuring & After Thrombolytic Therapy

Nina T. Gentile, MD, FAAEM
Induced HypertensionInduced Hypertension
• Phenylephrine or Norepinephrine can improve neurologic deficits
• IV NS, LR, or 10% hydroxyethyl starch 200/0.5 (HES) augments local perfusion to ischemic tissue
Rordorf, Stroke, 1997 Hillis, Cerebrovasc Dis, 2003
Aichner, 2003

Nina T. Gentile, MD, FAAEM
Returning to our CaseReturning to our Case
• BP remains ~220/120 mm Hg
• Anticipating IV t-PA or with the possibility of ICH….
…..give Labetalol (10 mg bolus IV ) or Cardene by IV infusion if available

The Nurse Wants to KnowThe Nurse Wants to Know
What about the Blood Sugar?
Do you want to hang fluids?
Give Insulin?
Nina T. Gentile, MD, FAAEM

Nina T. Gentile, MD, FAAEM
Hyperglycemia in StrokeHyperglycemia in Stroke
• Accounts for 25 to 50% of patients
• Associated with worsened outcome• increases cerebral edema
• hemorrhagic transformation of ischemic strokes
• increases mortality with BS > 130mg%

Nina T. Gentile, MD, FAAEM
Hyperglycemia after Stroke
<.0001Mortality
P
18 (7%)
High BS (>130 mg%)
n=259
6 (2%)
Normal BS (<130 mg%)
ICH <.000117 (7%)1 (2%)
<.0001Mortality 46 (52%)16 (15%)
Ischemic
Hemorrhagic
n=385
n=109 n=89

Nina T. Gentile, MD, FAAEM
Hyperglycemia after Stroke
GLYCEMIC CONTROL
<.00011 (1.3%)18 (7%)Mortality.0152 (64%)161 (62%)D/C Home
PControlNo control
n=81Ischemic n= 259
<.0001 Mortality 15 (43%)24 (65%)
Hemorrhagic n=37 n=35

HypercoagulabilityHypercoagulability
0
50
100
150
200
250
0 200 400 600Blood Glucose
Fa
cto
r V
IIa
Blood Glucose Level vs Factor VIIa
r2 =.82, p<.001

Nina T. Gentile, MD, FAAEM
HyperglycemiaHyperglycemia
• EUSI and AHA Recommendations:
- Treat hypoglycemia- Give Insulin for Blood Glucose >
300 mg%

Nina T. Gentile, MD, FAAEM
InsulinInsulin
NEJM

Nina T. Gentile, MD, FAAEM
Returning to our CaseReturning to our Case

Nina T. Gentile, MD, FAAEM
43 yo with ICH43 yo with ICH
• Patient given 50 gm Mannitol
• Emergently intubated and ventilated to maintain pCO2 of 32 mmHg
• Given with 8 mg midazolam and 10 mg vecuronium
• Nurse wants to know if you’ll need a bed or will you be transferring the patient

Nina T. Gentile, MD, FAAEM
Surgical Rx of ICH - 1Surgical Rx of ICH - 1
1. Large clots in the frontal, temporal or occipital regions with progressive clinical deterioration.

Nina T. Gentile, MD, FAAEM
Surgical Rx of ICH - 2Surgical Rx of ICH - 2
2. Deep basal ganglia clot in the non-dominant hemisphere with progressive deficit

Surgical Rx of ICH - 3Surgical Rx of ICH - 3
3. Acute cerebellar hematoma larger than 3cm.

Nina T. Gentile, MD, FAAEM
Nonsurgical Rx for ICHNonsurgical Rx for ICH
• Small bleeds or GCS >12
• No chance for recovery or GCS < 4

Nina T. Gentile, MD, FAAEM
Returning to our caseReturning to our case
• Undergoes craniotomy and evacuation of hemorrhage with ventriculostomy placement
ED Presentation 24o p ED Presentation

Nina T. Gentile, MD, FAAEM
43 yo s/p ICH Evacuation43 yo s/p ICH Evacuation
• Intermittently following commands with left arm, right-sided hemiparesis
• Discharged to extended care facility 24 days after admission
• Antihypertensive regimen• Clonidine• Minoxidil• Atenolol

Nina T. Gentile, MD, FAAEM
30-day Stroke Mortality30-day Stroke Mortality
22%36%10%1996-00
19%48% 10%1981-88
OverallHemorrhagicICH or SAH
IschemicLacunar or
Cortical
Period

Nina T. Gentile, MD, FAAEM
Disability Among Stroke SurvivorsDisability Among Stroke Survivors
Need Help caring for Themselves
Need Help Walking3120
71
01020304050607080
% Stroke Survivors
Impaired Vocational Capacity

Nina T. Gentile, MD, FAAEM
Stroke Patients’ Views Stroke Patients’ Views on Stroke Outcomeon Stroke Outcome
• Elderly stroke patients with disability vs age-matched controls
• Preferred death to severe disability• 69% of stroke patients• 82% of controls
• Over 1/3 preferred painless death to even minor disability
Clin Rehab 2000; 14:417-424

Nina T. Gentile, MD, FAAEM
Acute Stroke Care-Acute Stroke Care-It’s Not Just t-PAIt’s Not Just t-PA
• Aspirin should be avoided until after CT and the question of t-PA is answered
• Individualize BP management • Early ischemic changes on CT help with
decision-making• Heparin has no role (other than DVT
prophylaxis)• Intensify blood sugar management• Transfer: imaging, interventional neurorad, or
surgery

Stroke TeamStroke Team
Neuroradiology, Interventional
Neurology4 WEST4 WEST
Neurosurgery
EDED
Neuroradiology, Diagnostic
PHYSICAL MEDICINE and REHABILITATION
STAT LABSTAT LABNICUNICU
Neurovascular ResearchNeurovascular Research

Nina T. Gentile, MD, FAAEM
StrokeStroke

Questions?? Questions??
[email protected]@ferne.org
Nina Gentile, MDNina Gentile, MD
[email protected] 215 707 8402
formatted_gentile_stroke_aaem_2005.ppt 2/11/2005 10:31 PMNina T. Gentile, MD, FAAEM