acute stroke imaging - university of california, · pdf fileacute stroke imaging. ... •...
TRANSCRIPT

Acute Stroke Imaging
Radoslav Raychev, MD
UCI Stroke Center
Goals: • Determine stroke subtype • Understand mechanism • Institute treatment

Acute Stroke Facts • Leading cause of disability • 4rd leading cause of death in USA • 2nd leading cause of death worldwide • >5 million stroke survivors • $40 to $50 billion per year in the US • 1 in 6 Americans will be affected • 90% of those who survive will have deficits • 30% of strokes can be reversed • 80 % of strokes can be prevented
UCI Stroke Center
Stroke: Definition
Permanent injury to the brain or spinal cord of vascular origin (reduced blood flow or bleeding into or around the brain or spinal cord)
Stroke imaging objectives
• Brain tissue • Brain vessels
UCI Stroke Center


Brain Tissue Imaging - Non Contrast Head CT
ISCHEMIC
UCI Stroke Center
Stroke Suspected
HEMORRHAGIC

Hemorrhagic stroke imaging
• Non-traumatic Intracerebral hemorrhage (ICH) = Intraparenchymal hemorrhage » 70% of intracranial hemorrhage
• Subarachnoid hemorrhage » 30% of intracranial hemorrhage
UCI Stroke Center

Head CT
• Advantages: » Quick » Best for bony anatomy » Excellent for blood » Widely available
• Disadvantages: » Radiation » Limited detail
UCI Stroke Center

MRI for ICH
UCI Stroke Center
Large draining vein
AVM nidus
Blood – dark on GRE weighted sequence

Gradient Echo Imaging – best for blood
UCI Stroke Center
GRE: Multiple microbleeds, not visible on other sequences
FLAIR

UCI Stroke Center

Traumatic ICH » Epidural » Subdural » Intraprenchymal » Subarachnoid
• Mostly in the convexities
UCI Stroke Center

UCI Stroke Center
All Traumatic hemorrhages at once

Intraparenchymal Hemorrhage
• Cortical (lobar) • Deep (basal ganglia)
UCI Stroke Center

Basal ganglia hemorrhage
UCI Stroke Center

Basal ganglia = small vessel rupture usually due to chronic HTN
UCI Stroke Center

Lobar hemorrhage - multiple etiologies
UCI Stroke Center

Lobar hemorrhage = r/o vascular lesion
UCI Stroke Center
VASCULAR LESIONS CAUSING ICH • AVM • DURAL AV FISTULA • CAVERNOUS MALFORMATION • VENOUS SINUS THROMBOSIS • ANEURYSM
• Mycotic • Blister • Dissecting
• VASCULITIS
VASCULAR IMAGING
CTA • Advantages
» Great spacial resolution • Aneurysms • Dissections • Stenosis
» Quick » Readily available
• Disadvantages » Radiation » Contrast
UCI Stroke Center
MRA • Advantages
» No contrast » No radiation » Special sequencing for arterial wall
• Dissection • Intraluminal clot
• Disadvantages » Less optimal spacial resolution » Prolonged acquisition » Motion artifact » Contraindicated in some implants

UCI Stroke Center
CTA MRA
Good for LARGE lesions

UCI Stroke Center
Patient with posterior fossa ICH

UCI Stroke Center
CTA - negative

Angiogram
• The “gold standard” vascular imaging • Most detailed • Dynamic • Invasive (0.5% risk of stroke) • Therapeutic
» The most advanced way to treat stroke
UCI Stroke Center

UCI Stroke Center
AVM
Tiny residual post embolization
Complete treatment with surgical resection

Vascular lesions requiring catheter angiogram
• AVM • Dural AV Fistula • Small (mycotic and “blister”) aneurysms
Vasculitis
UCI Stroke Center

Dural AV Fistula
UCI Stroke Center
• 15 % of all cerebral vascular malformation » Direct high-flow communication between dural veins and
arteries » No intervening nidus (as opposed to AVM)
• Often missed on CTA or MRA • Leading to hemorrhage due to high venous pressure • Completely curable endovascularly
Artery
Vein

Patient with ICH and SAH
UCI Stroke Center
CTA – negative

Cervical Dural AV fistula
Microcatheter in the fistula
No residual fistula after embolization with Onyx
Aneurysmal subarachnoid hemorrhage - facts
UCI Stroke Center
• 10-15% of patients die before reaching the hospital • 30-60% in-hospital mortality
• Lower at facilities with Interventional Neuroradiology Johnston S et al. Stroke. Jan 2000
• 80 % of survivors will have deficits • Better outcome with dedicated Neuro ICU team
Samuels et al, Neurocritcal Care 2001

Common location of cerebral aneurysms surrounding the circle of Willis.
•Meyers P M et al. Stroke 2009;40:e366-e379
• Copyright © American Heart Association
A, Middle cerebral (proximal to bifurcation, bifurcation, distal to bifurcation); (B) carotid terminus; (C) anterior choroidal; (D) superior hypophyseal; (E) anterior communicating (proximal to communicating artery, at communicating artery); (F) posterior communicating; (G) ophthalmic; (H) basilar artery (terminus, trunk); (I) superior cerebellar; (J) V4 segment, vertebral; (K) posterior inferior cerebellar; (L) pericallosal artery.

Aneurysmal subarachnoid hemorrhage - imaging
UCI Stroke Center
Blood is mostly in the cisterns and fissures, often accompanied by • Intraventricular Hemorrhage (IVH) • Hydrocephalus • Cerebral edema • Intraparechymal hemorrhage (IPH)
• Frontal lobe (A-comm) • Temporal lobe (MCA)
SAH FIISHER GRADING SCALE
UCI Stroke Center
1 - No hemorrhage evident. 2 - SAH < 1mm thick 3 - SAH > 1mm thick 4 - SAH of any thickness with intra-ventricular hemorrhage (IVH) or parenchymal extension

ACA SAH pattern
UCI Stroke Center
Blood in the interhemispheric fissure
Hematoma in the corpus callosum
IVH with hydrocephalus

Pericallosal Artery Aneurysm
UCI Stroke Center
CTA

UCI Stroke Center
ANGIO with coiling
Vasospasm after SAH
• Diagnostic » TCD – great screening and diagnostic tool » CTA or MRA – may be used for confirmation of
suspected vasospasm • Diagnostic and therapeutic
» Angiogram
UCI Stroke Center

Vasospasm after SAH
UCI Stroke Center

Vasospasm after SAH
UCI Stroke Center

Ischemic Stroke Imaging
UCI Stroke Center

The Ischemic Penumbra
Core Infarct
Ischemic Penumbra:
zone of salvageable tissue surrounding
core infarct
UCI Stroke Center

In a typical acute ischemic stroke, every minute the brain loses
• 1.9 million neurons • 14 billion synapses • 7.5 miles myelinated fibers -- Saver, Stroke 2006
UCI Stroke Center

Strategies in Acute Ischemic Stroke Therapy
• Proven » Recanalization » Supportive Care » Early Implementation of Secondary Prevention
• Experimental » Neuroprotection » Reperfusion via Collateral Enhancement
UCI Stroke Center

NINDS tPA Stroke Trials 1 and 2
tPA tPA Placebo Placebo
Excellent Recovery (mRS 0-1) Death
Hemorrhage p < .001
UCI Stroke Center

UCI Stroke Center
• Absolute imaging contraindication for IV TPA: »Evidence of intracranial hemorrhage
• In the first 3 hours virtually every patient has potentially salvageable tissue

Impact of Acute Ischemic Stroke Treatments
NNT Benefit per 100 pts TPA 1-3h 3 32 Thrombectomy (ICA/M1) 5 20 TPA 3-4.5h 6 16 IA Lytics 7 14 Stroke Unit 10 10 Aspirin 77 1 UCI Stroke Center

Ticking Clock Tissue Clock
UCI Stroke Center

Bioenergetic Compromise
Hemodynamic Compromise
Occlusions or Stenoses
DWI PWI MRA
Tissue Status Perfusion Status Vessel Status
CBV CT PCT CTA
Multimodal CT
Multimodal MRI
UCI Stroke Center

Non – contrast head CT
UCI Stroke Center
Hyperdense vessel
No Evidence of early ischemic changes in the territory

Early ischemic changes
UCI Stroke Center
• Effacement of the sulci • Obscuration between the gray/white matter junction

Completed infarct – frank hypodensity
UCI Stroke Center

CT Perfusion Imaging
UCI Stroke Center
Cerebral blood volume - for core Time to peak - for tissue at risk
Mismatch (penumbra) = Core / Tissue at risk
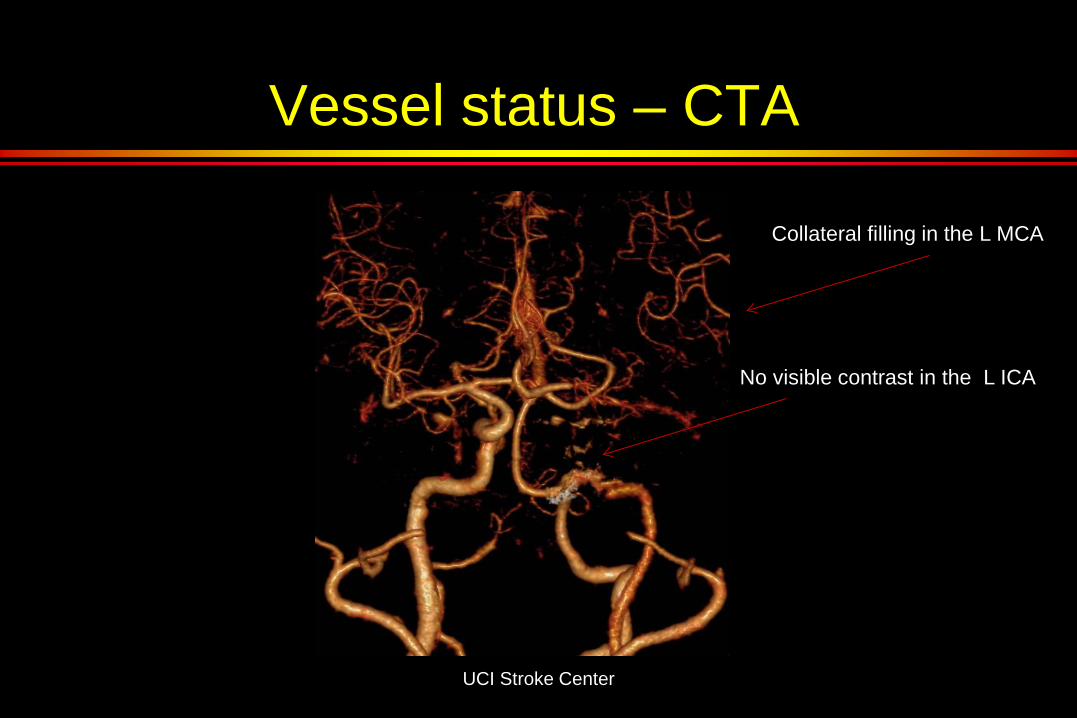
Vessel status – CTA
UCI Stroke Center
No visible contrast in the L ICA
Collateral filling in the L MCA

MRI – best for acute stroke
UCI Stroke Center
Diffusion weighted imaging (DWI) • Bright area = completed infarction • Identifies infarcted tissue within minutes of onset • The “gold standard” for visualization of core

DWI: Very tiny area of completed infarction GRE: No hemorrhage
Multimodal MRI
FLAIR: L ICA hyperintensity
PERFUSION: Large area of tissue at risk MRA: No flow in the L ICA

UCI Stroke Center
FLAIR or T2 • best for subacute and old strokes
DWI FLAIR

MRI for acute stroke
UCI Stroke Center
• Advantages: Most accurate evaluation of stroke size and location Detailed brain tissue evaluation
• Potential pitfalls: Time consuming Cost Contraindicated for some patients

Case # 1
• 65 y/o male with acute global aphasia and right sided hemiplegia (NIHSS 20)
• Presented to ED within 1 hour of onset • On full dose anticoagulation (contraindication
for IV TPA)
UCI Stroke Center

UCI Stroke Center
Hyperdense L MCA No early ischemic changes
UCI Stroke Center
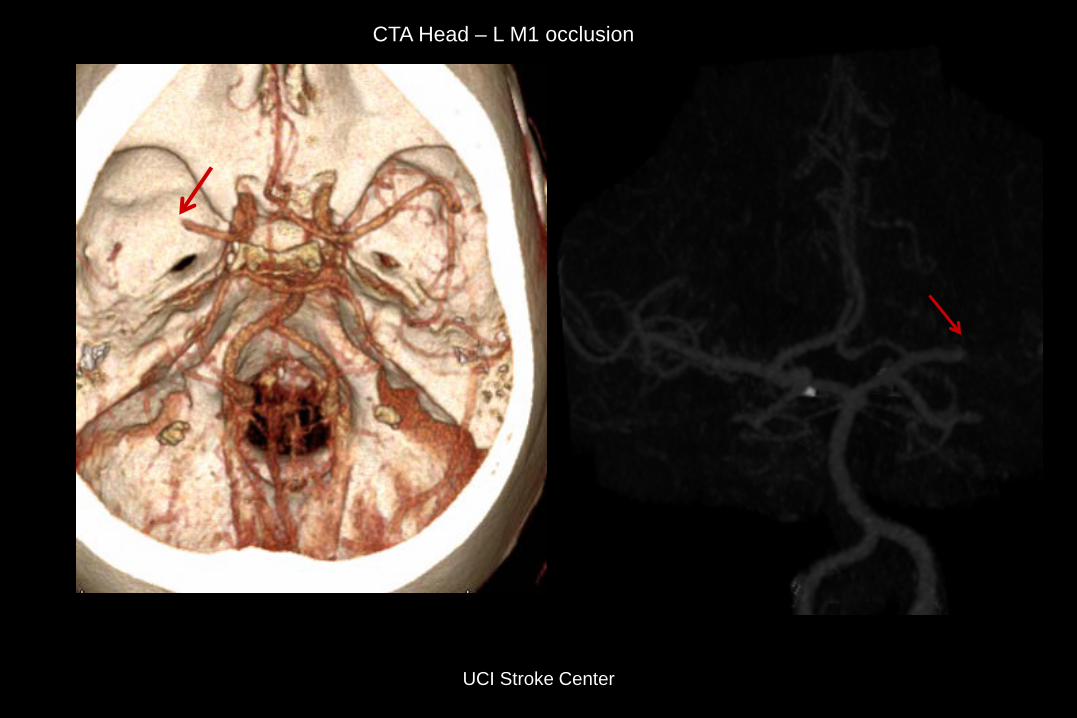
CTA Head – L M1 occlusion

UCI Stroke Center
CTA Neck: - Severe R ICA stensosis - Complete L ICA occlusion


UCI Stroke Center
Tiny channel within the occluded L ICA
• Catheter passed through the channel in the L ICA terminus • Injection through the catheter confirmed L MCA occlusion

UCI Stroke Center
Complete reperfusion after one pass with the Solitaire Device
UCI Stroke Center
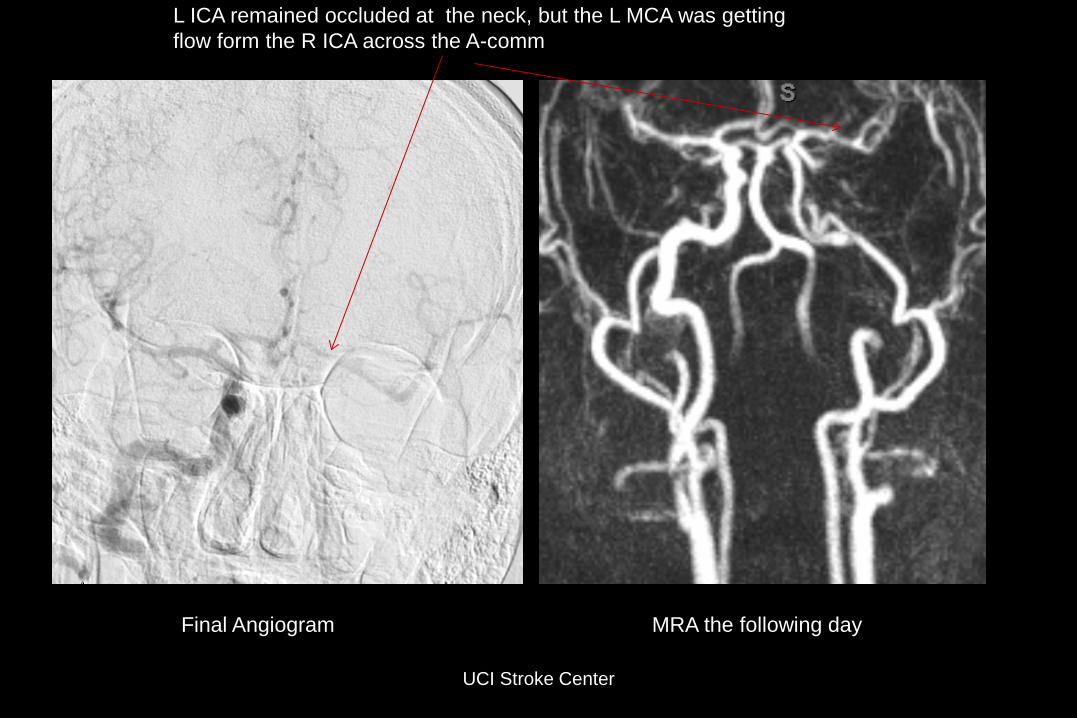
L ICA remained occluded at the neck, but the L MCA was getting flow form the R ICA across the A-comm
Final Angiogram MRA the following day

Patient was walking and talking in full sentences within 24h (NIHSS = 2)
UCI Stroke Center
DWI sequence: Small area of infarcted tissue in the L frontal operculum

R ICA stenosis
Ulcerated plaque causing 80% stenosis

Successful CEA 2 weeks later

Case 2
• 50 y/o male with acute aphasia and R hemiplegia (NIHSS 22)
• Witnessed onset at work • 911 called • EMS transported the patient to primary stroke
center within 15 min (Riverside county)
UCI Stroke Center

Non – contrast head CT
UCI Stroke Center

• Patient received IV TPA • No improvement noted • Transferred to UCI • Arrived at UCI 4.5 hours after onset • Repeat exam showed persistent global
aphasia and R sided hemiplegia – NIHSS 22
UCI Stroke Center

UCI Stroke Center
Occluded L ICA Large Mismatch

• INR suite » within 60 minutes of CT completion
UCI Stroke Center

Solitaire FR
UCI Stroke Center

UCI Stroke Center

Follow up
• Substantial improvement within 24 hours: » Patient is moving the right side against gravity,
comprehends and utters simple words = NIHSS 10
UCI Stroke Center
UCI Stroke Center
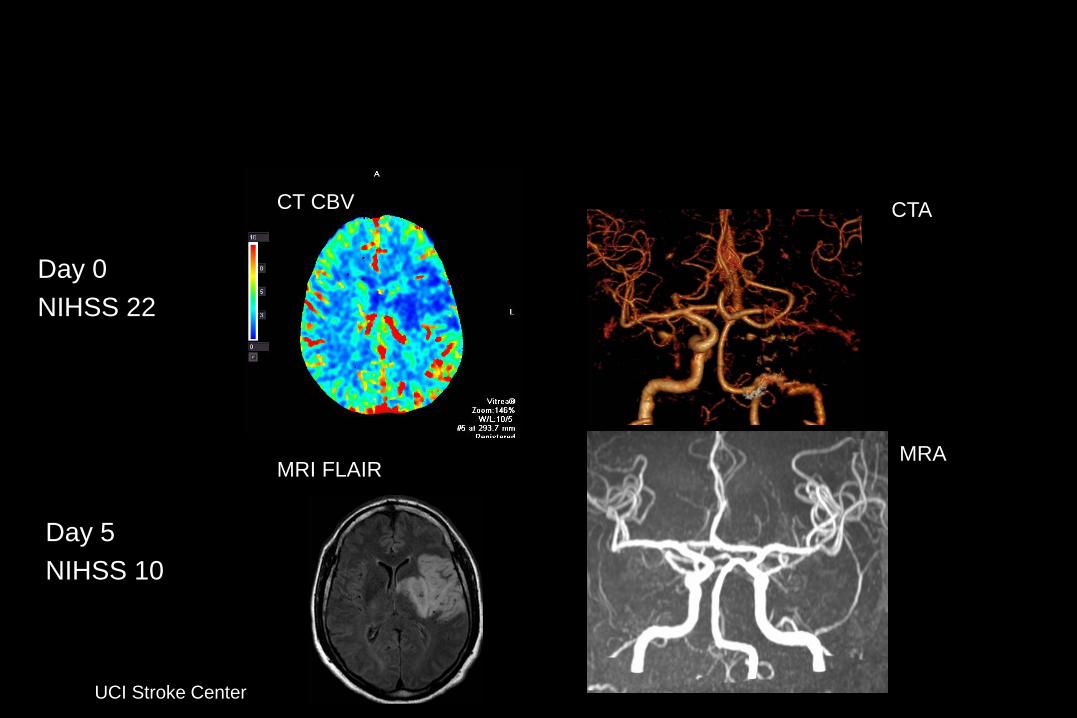
Day 0 NIHSS 22
Day 5 NIHSS 10
CT CBV
MRI FLAIR
CTA
MRA
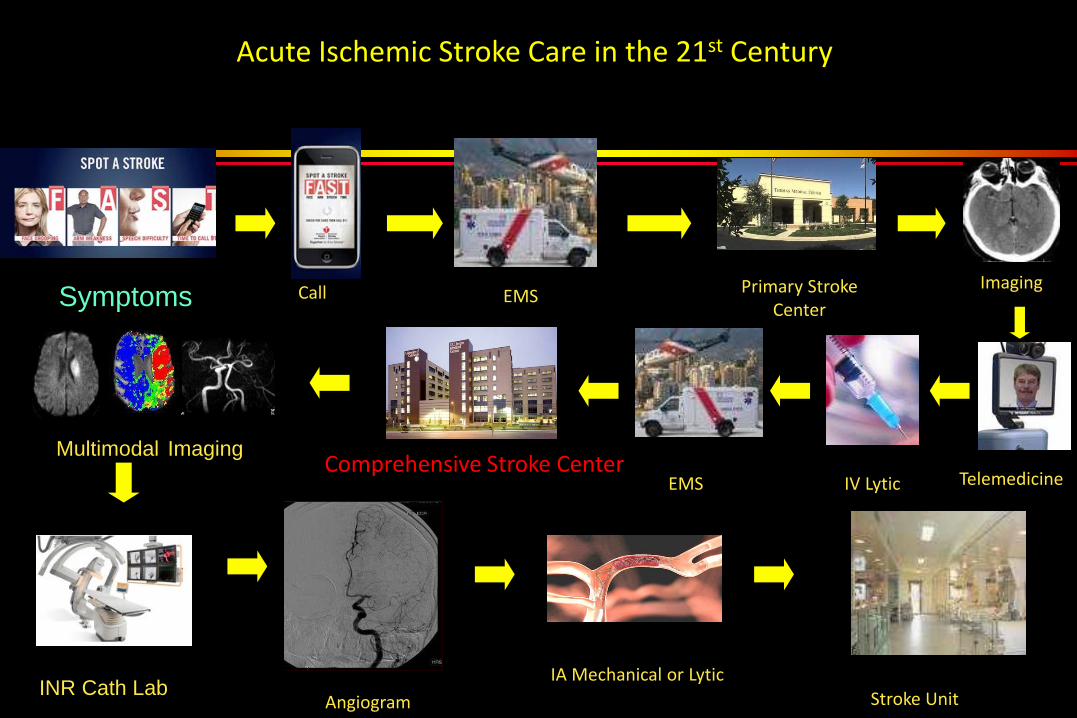
Acute Ischemic Stroke Care in the 21st Century
Symptoms Primary Stroke Center
EMS Call
Comprehensive Stroke Center EMS IV Lytic
IA Mechanical or Lytic Angiogram Stroke Unit
Multimodal Imaging
Imaging
Telemedicine
INR Cath Lab