acute respiratory distress syndrome (ards) update
TRANSCRIPT

Acute Respiratory Distress Syndrome (ARDS) Update
A ALAVI MD.
PROFESSOR OF RESPIATORY MEDICINE, GUMS

First description of ARDS • Clinical features 1st
described in 1967 by Ashbaugh:
1. severe dyspnea, 2. tachypnea, 3. refractory hypoxemia, 4. low lung compliance, 5. diffuse alveolar infiltrate
Lancet 1967; 2:319-323
ARDS remains a relatively common and lethal or disabling syndrome

• Introduction
• Epidemiology and outcomes
• Causes and risk factors
• Underlying biology
• Heterogeneity in ARDS
• ARDS due to COVID-19
• Diagnostic considerations
• Management

Introduction ARDS is the acute onset of hypoxaemia,
Bilateral pulmonary oedema due to excessive alveolocapillary permeability,
No single test to identify or exclude the diagnosis,
The Berlin definition: stages that estimate mortality risk,
The heterogeneity of ARDS: in causes, manifestations, and response to therapy,
challenges clinicians and scientists to provide impeccable supportive care and discover new therapies.
Ranieri VM, Rubenfeld GD, Thompson BT, et al. Acute respiratory distress syndrome: the Berlin definition. JAMA 2012; 307: 2526–33.
Calfee CS, Delucchi KL, Sinha P, et al. Acute respiratory distress syndrome subphenotypes and differential response to simvastatin: secondary analysis of a randomised controlled trial. Lancet Respir Med 2018; 6: 691–98.
Calfee CS, Delucchi K, Parsons PE, Thompson BT, Ware LB, Matthay MA. Subphenotypes in acute respiratory distress syndrome: latent class analysis of data from two randomised controlled trials. Lancet Respir Med 2014; 2: 611–20.

ARDS: Syndrome of Diffuse Pulmonary Edema
Results From Lung Injury
Edema Occurs From
Capillary Leak and not
Increased Hydrostatic
Pressure
Edema Fluid has a High
Protein Concentration
Similar to Plasma

Epidemiology and outcomes • ARDS is more common than initially believed. In 2016, a study of patients in 459 ICUs from 50 countries reported pts. that
fulfilled criteria for ARDS: 10% of ICU pts.
23% of mechanically ventilated pts.
Many patients with diffuse lung injury supported with high-flow nasal cannula (HFNC) do not meet the ARDS Berlin definition (which requires positive pressure ventilation), so the incidence of ARDS is probably even higher.
The COVID-19 pandemic has highlighted this limitation, as many patients are treated without mechanical ventilation.
Bellani G, Laffey JG, Pham T, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA 2016; 315: 788–800.
Gershengorn HB, Hu Y, Chen J-T, et al. The impact of high-flow nasal cannula use on patient mortality and the availability of mechanical ventilators in COVID-19. Ann Am Thorac Soc 2020; 18: 623–31.
Alqahtani JS, Mendes RG, Aldhahir A, et al. Global current practices of ventilatory support management in COVID-19 patients: an international survey. J Multidiscip

Epidemiology and outcomes
• Although the 2016 survey by Bellani was done during the winter viral season and included ARDS that resolved rapidly, the hospital mortality of 35–45% closely resembled that described by the large datasets used to validate the Berlin definition.
• Even patients whose ARDS resolved rapidly had a mortality rate of 31%.
Bellani G, Laffey JG, Pham T, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50
countries. JAMA 2016; 315: 788–800.
Villar J, Schultz MJ, Kacmarek RM. The LUNG SAFE: a biased presentation of the prevalence of ARDS! Crit Care 2016; 20: 108.
Madotto F, Pham T, Bellani G, et al. Resolved versus confirmed ARDS after 24 h: insights from the LUNG SAFE study. Intensive Care Med 2018; 44: 564–77.

Epidemiology and outcomes • Men might be slightly more likely to develop ARDS, Outcome is largely similar between sexes.
• Women—and patients of shorter stature—are less likely to receive lung protective ventilator tidal volumes. With severe persistent ARDS, women had higher mortality than men.
• Black patients might have a reduced risk of developing ARDS, Black and Hispanic patients with ARDS had a higher mortality in at least one
study, which seemed to be mediated by increased severity of illness. Lemos-Filho LB, Mikkelsen ME, Martin GS, et al. Sex, race, and the development of acute lung injury. Chest 2013; 143: 901–09.
Han S, Martin GS, Maloney JP, et al. Short women with severe sepsis-related acute lung injury receive lung protective ventilation less frequently: an observational cohort study. Crit Care 2011; 15: R262.
McNicholas BA, Madotto F, Pham T, et al. Demographics, management and outcome of females and males with acute respiratory distress syndrome in the LUNG SAFE prospective cohort study. Eur Respir J 2019; 54: 1900609.
Erickson SE, Shlipak MG, Martin GS, et al. Racial and ethnic disparities in mortality from acute lung injury. Crit Care Med 2009; 37: 1–6.

Epidemiology and outcomes • Causes of increase ARDS risk:
o Tobacco use, oAlcohol use, oHypoalbuminaemia, oChemotherapy within the previous 6 months, oAmbient air pollutant exposure,
• In some studies, patients with diabetes were less likely to develop ARDS.
Trillo-Alvarez C, Cartin-Ceba R, Kor DJ, et al. Acute lung injury prediction score: derivation and validation in a population-based sample. Eur Respir J 2011; 37: 604–09.
Calfee CS, Matthay MA, Kangelaris KN, et al. Cigarette smoke exposure and the acute respiratory distress syndrome. Crit Care Med 2015; 43: 1790–97.
Moss M, Burnham EL. Chronic alcohol abuse, acute respiratory distress syndrome, and multiple organ dysfunction. Crit Care Med 2003; 31 (suppl): S207–12.
Reilly JP, Zhao Z, Shashaty MGS, et al. Low to moderate air pollutant exposure and acute respiratory distress syndrome after severe trauma. Am J Respir Crit Care Med 2019; 199: 62–70.
Moss M, Guidot DM, Steinberg KP, et al. Diabetic patients have a decreased incidence of acute respiratory distress syndrome. Crit Care Med 2000; 28: 2187–92.
Boyle AJ, Madotto F, Laffey JG, et al. Identifying associations between diabetes and acute respiratory distress syndrome in patients with acute hypoxemic respiratory failure: an analysis of the LUNG SAFE database. Crit Care 2018; 22: 268.

Epidemiology and outcomes
• Mortality for ARDS remains sobering; Observational studies consistently report >30% hospital mortality,
one large trial of moderate to severe ARDS: 43% in-hospital mortality at 90 days.
The proportion of mortality attributable to the ARDS itself (as opposed to risk factors and comorbidities) has been challenging to determine, but was estimated for sepsis-associated ARDS at 27–37%.
The cause of death is more commonly sepsis and multiple organ failure (MOF) than respiratory failure.
Bellani G, Laffey JG, Pham T, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50
countries. JAMA 2016; 315: 788–800.
Moss M, Huang DT, Brower RG, et al. Early neuromuscular blockade in the acute respiratory distress syndrome. N Engl J Med 2019; 380: 1997–2008.
www.thelancet.com Vol 398 August 14, 2021 633 20 Auriemma CL, Zhuo H, Delucchi K, et al. Acute respiratory distress syndrome-attributable mortality in critically ill patients with sepsis. Intensive Care Med 2020; 46: 1222–31.
Stapleton RD, Wang BM, Hudson LD, Rubenfeld GD, Caldwell ES, Steinberg KP. Causes and timing of death in patients with ARDS. Chest 2005; 128: 525–32.

Epidemiology and outcomes
• Most ARDS survivors recover normal or near-normal pulmonary function, Many remain burdened by functional limitations related to: muscle weakness, deconditioning, psychological sequelae of severe illness.
• Cognitive impairment is also distressingly common, ~half of survivors at 2 years.
Herridge MS, Tansey CM, Matté A, et al. Functional disability 5 years after acute respiratory distress syndrome. N Engl J Med 2011; 364: 1293–304.
Cheung AM, Tansey CM, Tomlinson G, et al. Two-year outcomes, health care use, and costs of survivors of acute respiratory distress syndrome. Am J Respir Crit Care Med 2006; 174: 538–44.
Mikkelsen ME, Christie JD, Lanken PN, et al. The Adult Respiratory Distress Syndrome Cognitive Outcomes Study: long-term neuropsychological function in survivors of acute lung injury. Am J Respir Crit Care Med 2012; 185: 1307–15.
Hopkins RO, Weaver LK, Collingridge D, Parkinson RB, Chan KJ, Orme JF Jr. Two-year cognitive, emotional, and quality-of-life outcomes in acute respiratory distress syndrome. Am J Respir Crit Care Med 2005; 171: 340–47.

Causes and risk factors
• A clinical condition in the setting of various causes or risk factors, Identification the specific cause>a crucial therapeutic goal to improve outcomes.
• Genetic susceptibility to ARDS is suggested by: 1. the variability with which clinical risk factors predict ARDS development,
2. by the replicated association of numerous genetic variants with ARDS risk.
• The attributable risk of any singular genetic polymorphism to ARDS risk or outcome seems small.
Papazian L, Calfee CS, Chiumello D, et al. Diagnostic workup for ARDS patients. Intensive Care Med 2016; 42: 674–85.
Guillen-Guio B, Lorenzo-Salazar JM, Ma SF, et al. Sepsis-associated acute respiratory distress syndrome in individuals of European ancestry: a genome-wide association study. Lancet Respir Med 2020; 8: 258–66.
Reilly JP, Christie JD, Meyer NJ. Fifty years of research in ARDS. Genomic contributions and opportunities. Am J Respir Crit Care Med 2017; 196: 1113–21.

Causes and risk factors *Nuala J Meyer, Luciano Gattinoni, Carolyn S Calfee, Acute respiratory distress syndrome , Lancet 2021; 398: 622–37

Underlying biology
1. Endothelial permeability
2. Alveolar epithelial injury, permeability, and dysfunction
3. Dysregulated lung inflammation
4. Mechanical stress Normal Lung Tissue vs. ARDS

Inflammatory Alveolar Injury

Heterogeneity in ARDS
• ARDS is by definition a syndromic diagnosis rather than a distinct pathological entity; therefore, patients have great heterogeneity in their clinical, physiological, radiological, and biological phenotypes.
• This heterogeneity considered as a potential barrier to effective therapy.
• ARDS researchers and clinicians have lacked consensus on the usefulness of and optimal approach to further subdividing the syndrome.

Heterogeneity in ARDS: Clinically apparent subphenotypes differ physiologically and biologically, at least theoretically, and experimental data fit this model:
• Extrapulmonary ARDS (indirect) eg, non-pulmonary sepsis, should first affect endothelial permeability, leading to prevalent diffuse oedema.
• Pulmonary (direct) ARDS should first affect the alveolar epithelium. and patients have lower severity of illness, fewer organ failures, more evidence of lung epithelial injury and lower concentrations of plasma biomarkers of endothelial injury, compared with extrapulmonary lung injury.
However, after the first few days of ARDS, and indeed often in clinical practice, it is difficult to differentiate between pulmonary and extrapulmonary ARDS, and
evidence that these phenotypes should alter treatment is insufficient. Gattinoni L, Pelosi P, Suter PM, Pedoto A, Vercesi P, Lissoni A. Acute respiratory distress syndrome caused by pulmonary and extrapulmonary disease. Different syndromes?
Am J Respir Crit Care Med 1998; 158: 3–11.
Shaver CM, Bastarache JA. Clinical and biological heterogeneity in acute respiratory distress syndrome: direct versus indirect lung injury. Clin Chest Med 2014; 35: 639–53.
Calfee CS, Janz DR, Bernard GR, et al. Distinct molecular phenotypes of direct vs indirect ARDS in single-center and multicenter studies. Chest 2015; 147: 1539–48.
Luo L, Shaver CM, Zhao Z, et al. Clinical predictors of hospital mortality differ between direct and indirect ARDS. Chest 2017; 151: 755–63.

Heterogeneity in ARDS:
• Diffuse versus focal lung injury, • Higher inflammatory markers subphenotype (about 30% of patients),
o higher plasma concentrations of inflammatory cytokines, lower plasma concentrations of the coagulation factor protein C and bicarbonate, a higher prevalence of shock, and consistently worse clinical outcomes than patients with the subphenotype characterised by lower inflammatory markers.
o in secondary analyses of completed clinical trials, these two subphenotypes seemed to respond differently to PEEP, fluid management strategy, and simvastatin.
Constantin J-M, Jabaudon M, Lefrant J-Y, et al. Personalised mechanical ventilation tailored to lung morphology versus low positive end-expiratory pressure for patients with acute respiratory distress syndrome in France (the LIVE study): a multicentre, single-blind, randomised controlled trial. Lancet Respir Med 2019; 7: 870–80.
Calfee CS, Delucchi KL, Sinha P, et al. Acute respiratory distress syndrome subphenotypes and differential response to simvastatin: secondary analysis of a randomised controlled trial. Lancet Respir Med 2018; 6: 691–98.
Calfee CS, Delucchi K, Parsons PE, Thompson BT, Ware LB, Matthay MA. Subphenotypes in acute respiratory distress syndrome: latent class analysis of data from two randomised controlled trials. Lancet Respir Med 2014; 2: 611–20.
Famous KR, Delucchi K, Ware LB, et al. Acute respiratory distress syndrome subphenotypes respond differently to randomized fluid management strategy. Am J Respir Crit Care Med 2017; 195: 331–38.
Sinha P, Delucchi KL, Thompson BT, McAuley DF, Matthay MA, Calfee CS. Latent class analysis of ARDS subphenotypes: a secondary analysis of the statins for acutely injured lungs from sepsis (SAILS) study. Intensive Care Med 2018; 44: 1859–69.
Reilly JP, Calfee CS, Christie JD. Acute respiratory distress syndrome phenotypes. Semin Respir Crit Care Med 2019; 40: 19–30.
Heterogeneity in ARDS:
• Cluster analysis of plasma protein biomarker data identified two distinct ARDS subphenotypes: 1)reactive 2)uninflamed.
The reactive subphenotype had worse clinical outcomes and different expression of 29% of genes measured in whole blood using an array-based analysis.
How ARDS subphenotypes identified with these two different approaches correspond to each other, or to transcriptomic-based subphenotypes of sepsis, remains unknown.
• Prospective validation of subphenotype identification and differential treatment responses will be required before clinical care should be affected.
Bos LD, Schouten LR, van Vught LA, et al. Identification and validation of distinct biological phenotypes in patients with acute respiratory distress syndrome by cluster
analysis. Thorax 2017; 72: 876–83.
Bos LDJ, Scicluna BP, Ong DSY, Cremer O, van der Poll T, Schultz MJ. Understanding heterogeneity in biologic phenotypes of acute respiratory distress syndrome by leukocyte expression profiles. Am J Respir Crit Care Med 2019; 200: 42–50.
Davenport EE, Burnham KL, Radhakrishnan J, et al. Genomic landscape of the individual host response and outcomes in sepsis: a prospective cohort study. Lancet Respir Med 2016; 4: 259–71.

ARDS due to COVID-19
• Early reports highlighted unique features of COVID-19-associated ARDS, although subsequent data suggested that it shares many physiological aspects with classic ARDS, including heterogeneity.
• Similarly, early reports suggested a high prevalence of venous thrombosis and coagulopathy in COVID-19-associated ARDS.
• Gattinoni L, Coppola S, Cressoni M, Busana M, Rossi S, Chiumello D. COVID-19 does not lead to a “typical” acute respiratory distress syndrome. Am J Respir Crit
Care Med 2020; 201: 1299–300.
• Ziehr DR, Alladina J, Petri CR, et al. Respiratory pathophysiology of mechanically ventilated patients with COVID-19: a cohort study. Am J Respir Crit Care Med 2020; 201: 1560–64.
• Klok FA, Kruip MJHA, van der Meer NJM, et al. Confirmation of the high cumulative incidence of thrombotic complications in critically ill ICU patients with COVID-

Copyrights apply

Diagnostic considerations No single diagnostic test confirms or refutes
a diagnosis of ARDS.
ARDS is a syndrome rather than a specific pathologic entity and is currently identified by purely clinical criteria.(The Berlin definition).
Berlin definition provided more specific guidance on CXR patterns compared with previous definitions : consistent with ARDS— bilateral opacities
consistent with pulmonary oedema that can be patchy or asymmetric—
inconsistent with ARDS, including isolated pleural effusions, atelectasis, or tumours.

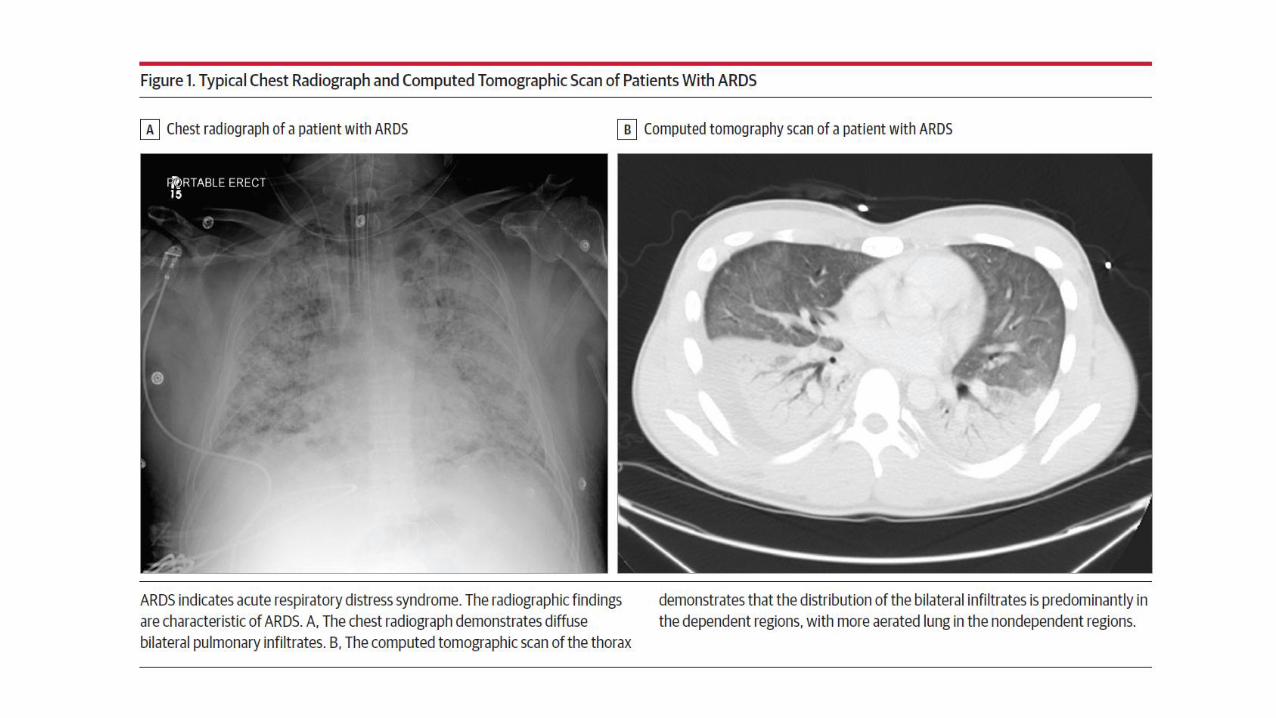
Diagnostic considerations: Imaging(CT Scan)
• CT can fulfil the radiographical ARDS criterion, replacing or adding to CXR, Can quantify lung oedema and potential recruitability of lung parenchyma. Can identify abnormalities that mimic ARDS on a CXR, including:
1. pleural effusions, 2. severe obesity with atelectasis, 3. nodules and masses, 4. interstitial lung disease.
• CT can be challenging: To obtain for severely hypoxaemic patients and those receiving high dose vasoactive
medications, CRRT, or other ICU interventions. Exposes patients to ionising radiation, which restricts its repeatability, Is expensive.


ARDS exudative and fibrotic phases

Diagnostic considerations: Imaging(US)
• Lung ultrasonography can identify alveolar flooding using bilateral B line patterns, defined as three or more discrete vertical lines arising from the
pleura in an intercostal space, representing hyperechoic reverberation artifacts.
• An alternative to CXR for resource-limited settings in the Kigali modification to the Berlin definition of ARDS.46
• US advantages is: 1. portable, 2. inexpensive, 3. free from radiation, 4. can be repeated as needed, 5. monitors lung recruitment & resolution of alveolar processes.
• US disadvantages: 1. B lines from hydrostatic pulmonary oedema are
indistinguishable from those in ARDS. Combining cardiac and lung US can suggest a cardiogenic process, although heart failure and ARDS can coexist.
2. Ultrasound can yield poor-quality images in the presence of extensive overlying soft tissue (as seen with obesity) or subcutaneous oedema.
Diagnostic considerations: Determining the inciting cause
• ARDS precipitants can be self-limited and do not have specific treatment, however it is essential to prompt recognition, and treatment of reversible insults such as: infection,
hypersensitivity,
autoinflammation.
• Clinical history provides crucial information about the duration of symptoms, an infectious prodrome or travel history, exposures, behaviours, or localising symptoms that might guide imaging or serological testing.
• Understanding the patient’s comorbidities is essential to consider risks for infectious and sterile (eg, blunt trauma, pancreatitis, postoperative) processes.

Diagnostic considerations: Determining the inciting cause
• The initial diagnostic approach focuses upon determining whether the patient has pneumonia or another infection.
1. Blood cultures: for all patients without an obvious sterile insult,
2. Obtain sputum, tracheal aspirate, or BAL samples if safe to do so. The value of bronchoscopy, with sensitivity only 58% in one prospective study, is likely to
be superior to sputum, especially for fungal causes (eg, Pneumocystis jirovecii), Legionella, or atypical pathogens (eg, Nocardia or Actinomyces bacteria).
Meduri GU, Reddy RC, Stanley T, El-Zeky F. Pneumonia in acute respiratory distress syndrome. A prospective evaluation of bilateral bronchoscopic sampling. Am J Respir Crit Care Med 1998; 158: 870–75.

Diagnostic considerations: Determining the inciting cause
BAL can also prompt consideration of: • Alternative diagnoses to ARDS using a differential cell count and fluid cytology to identify :
eosinophilic pneumonia, alveolar proteinosis, diffuse alveolar haemorrhage, suggest hypersensitivity pneumonitis.
• In EVALI, BAL detected vitamin E acetate in the majority of cases and never among healthy controls.
• BAL or nasopharyngeal swab with PCR can detect numerous viral pathogens, which might prompt: 1. pathogen-specific treatment 2. isolation precautions 3. reduce exposure to potentially unnecessary antibiotics.
Schwarz MI, Albert RK. “Imitators” of the ARDS: implications for diagnosis and treatment. Chest 2004; 125: 1530–35.
Blount BC, Karwowski MP, Shields PG, et al. Vitamin E acetate in bronchoalveolar-lavage fluid associated with EVALI. N Engl J Med 2020; 382: 697–705.
Siegel JD, Rhinehart E, Jackson M, et al. 2007 guideline for isolation precautions: preventing transmission of infectious agents in healthcare settings. Am J Infect Control 2007; 35: S65–164.
Beigel JH, Tomashek KM, Dodd LE, et al. Remdesivir for the treatment of COVID-19—preliminary report. Reply. N Engl J Med 2020; 383: 994.

Diagnostic considerations: Determining the inciting cause
• Open lung biopsy is not commonly done during ARDS because there are risks and a lack of useful information in most cases.
• Transbronchial biopsy through a flexible bronchoscope is possible but still poses risks of bleeding and PTX , and diagnostic yield might be only.
• Consideration for Bx increases as physicians question whether is an alternative to ARDS, particularly a disease that might be treatable.
Libby LJ, Gelbman BD, Altorki NK, Christos PJ, Libby DM. Surgical lung biopsy in adult respiratory distress syndrome: a meta-analysis. Ann Thorac Surg 2014; 98: 1254–60.
Bulpa PA, Dive AM, Mertens L, et al. Combined bronchoalveolar lavage and transbronchial lung biopsy: safety and yield in ventilated patients. Eur Respir J 2003; 21: 489–94.
Palakshappa JA, Meyer NJ. Which patients with ARDS benefit from lung biopsy? Chest 2015; 148: 1073–82.

Initial management
Standard ventilator management:
MV does not cure ARDS;
Allow time to recover from the disease that led to respiratory failure,
Providing adequate oxygenation and removing CO2 without inducing VILI or other side-effects.
*Nuala J Meyer, Luciano Gattinoni, Carolyn S Calfee, Acute respiratory distress syndrome , Lancet 2021; 398: 622–37

Initial management: Supportive care
• A fluid-conservative management strategy: In ARDS patients who either never or no longer require vasopressors, the Fluid
and Catheter Treatment Trial (FACTT) showed that a fluid-conservative management strategy increased the number of ventilator-free days as compared with a fluid-liberal strategy, without increasing AKI or need for dialysis.
In practice, a strategy of diuresis targeted at a net even to negative daily fluid balance is feasible and likely to recapitulate the benefits of the FACTT protocol.
• No specific caloric goal or supplementation were superior in large trials.
Wiedemann HP, Wheeler AP, Bernard GR, et al. Comparison of two fluid-management strategies in acute lung injury. N Engl J Med 2006; 354: 2564–75.
Calfee CS, Matthay MA. Non-ventilatory management of acute lung injury and the acute respiratory distress syndrome. Chest 2007; 131: 913–20.
Rice TW, Wheeler AP, Thompson BT, et al. Initial trophic vs full enteral feeding in patients with acute lung injury: the EDEN randomized trial. JAMA 2012; 307: 795–803.
Rice TW, Wheeler AP, Thompson BT, deBoisblanc BP, Steingrub J, Rock P. Enteral omega-3 fatty acid, gamma-linolenic acid, and antioxidant supplementation in acute lung injury. JAMA 2011; 306: 1574–81.

Initial management: Supportive care
• Management of pain, agitation or sedation, and delirium, along with immobility and sleep (PADIS), An important issue; sedation practices can strongly affect patient outcomes.
International critical care guidelines support a goal-directed approach to PADIS that seeks light sedation, and daily spontaneous breathing trials to test patients’ readiness to liberate from mechanical ventilation. For patients with ARDS, spontaneous breathing trials should not begin until patients
have reached an appropriately low threshold of support, typically with a FiO2 of 0·5 or less and PEEP less than or equal to 8 cm H2O.
Shehabi Y, Bellomo R, Reade MC, et al. Early intensive care sedation predicts long-term mortality in ventilated critically ill patients. Am J Respir Crit Care Med 2012; 186: 724–31.
Shehabi Y, Bellomo R, Kadiman S, et al. Sedation intensity in the first 48 hours of mechanical ventilation and 180-day mortality: a multinational prospective longitudinal cohort study. Crit Care Med 2018; 46: 850–59.
Devlin JW, Skrobik Y, Gélinas C, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med 2018; 46: 1532–48.
Girard TD, Alhazzani W, Kress JP, et al. An official American Thoracic Society/American College of Chest Physicians clinical practice guideline: liberation from mechanical ventilation in critically ill adults. Rehabilitation protocols, ventilator liberation protocols, and cuff leak tests. Am J Respir Crit Care Med 2017; 195: 120–33.
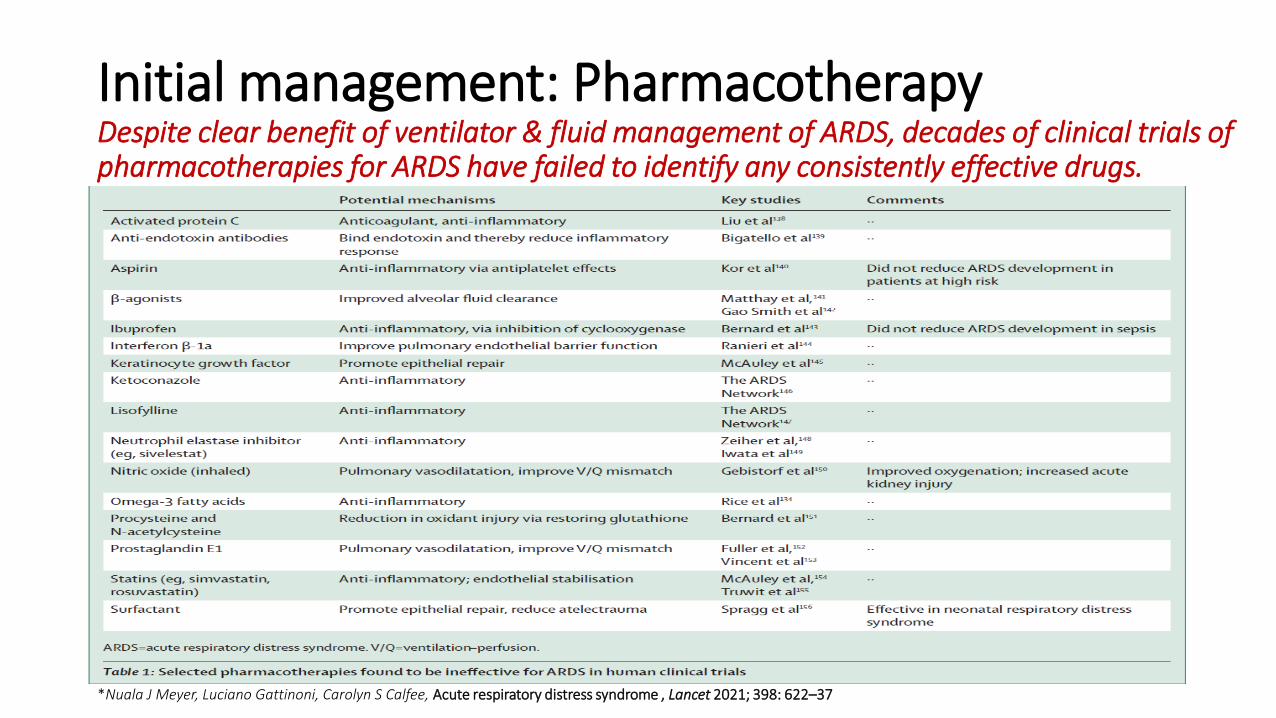
Initial management: Pharmacotherapy Despite clear benefit of ventilator & fluid management of ARDS, decades of clinical trials of pharmacotherapies for ARDS have failed to identify any consistently effective drugs.
*Nuala J Meyer, Luciano Gattinoni, Carolyn S Calfee, Acute respiratory distress syndrome , Lancet 2021; 398: 622–37

Initial management: Pharmacotherapy
• Most of the biological pathways thought to be dysregulated in ARDS have been targeted in clinical trials, including inflammation, epithelial injury, endothelial injury, and disordered coagulation, but no drugs targeting these pathways have proven consistently effective. Vitamin D,- interferon-β-1a,- Vitamin C ?+
Lewis SR, Pritchard MW, Thomas CM, Smith AF. Pharmacological agents for adults with acute respiratory distress syndrome. Cochrane Database Syst Rev 2019; 7:
CD004477.
Ginde AA, Brower RG, Caterino JM, et al. Early high-dose vitamin D₃ for critically ill, vitamin D-deficient patients. N Engl J Med 2019; 381: 2529–40.
Ranieri VM, Pettil نV, Karvonen MK, et al. Effect of intravenous interferon β-1a on death and days free from mechanical ventilation among patients with moderate to severe acute respiratory distress syndrome: a randomized clinical trial. JAMA 2020; 323: 725–33.
Fowler AA 3rd, Truwit JD, Hite RD, et al. Effect of vitamin C infusion on organ failure and biomarkers of inflammation and vascular injury in patients with sepsis and severe acute respiratory failure: the CITRIS-ALI randomized clinical trial. JAMA 2019; 322: 1261–70.
Mohammed BM, Fisher BJ, Kraskauskas D, et al. Vitamin C: a novel regulator of neutrophil extracellular trap formation. Nutrients 2013; 5: 3131–51.
Fowler AA 3rd, Syed AA, Knowlson S, et al. Phase I safety trial of intravenous ascorbic acid in patients with severe sepsis. J Transl Med 2014; 12: 32.
Fisher BJ, Seropian IM, Kraskauskas D, et al. Ascorbic acid attenuates lipopolysaccharide-induced acute lung injury. Crit Care Med 2011; 39: 1454–60.

Initial management: Pharmacotherapy
• Other potentially promising drugs in early phase clinical trials for ARDS: 1. allogeneic mesenchymal stromal cells,
2. carbon monoxide,
3. sevoflurane,
4. DNAse,
5. granulocyte-macrophage colony-stimulating factor.
Matthay MA, Calfee CS, Zhuo H, et al. Treatment with allogeneic mesenchymal stromal cells for moderate to severe acute respiratory distress syndrome (START study): a randomised phase 2a safety trial. Lancet Respir Med 2019; 7: 154–62.
Matthay MA, McAuley DF, Ware LB. Clinical trials in acute respiratory distress syndrome: challenges

Initial management: Rescue therapies • Adjunctive therapies for ARDS whose benefits have not been
conclusively shown for all patients but could show benefit in individualized circumstances.
• Include extracorporeal life support, alternative ventilator modalities or settings, or select pharmacotherapies.
• When we should consider? If despite maximal supportive therapy with optimal ventilator and fluid
management, patients with ARDS continue to worsen, with development of: 1. severe and refractory hypoxaemia, 2. hypercapnia or acidosis, 3. elevated plateau pressures, 4. a combination.
Fielding-Singh V, Matthay MA, Calfee CS. Beyond low tidal volume ventilation: treatment adjuncts for severe respiratory failure in acute respiratory distress syndrome. Crit Care Med 2018; 46: 1820–31.

Initial management: Rescue therapies *Nuala J Meyer, Luciano Gattinoni, Carolyn S Calfee, Acute respiratory distress syndrome , Lancet 2021; 398: 622–37

Initial management *Nuala J Meyer, Luciano Gattinoni, Carolyn S Calfee, Acute respiratory distress syndrome , Lancet 2021; 398: 622–37


THANK YOU FOR YOUR ATTENTION