acute pain in the ambulatory setting - denver, colorado · acute pain in the ambulatory setting...
TRANSCRIPT

Acute Pain in the Ambulatory Setting
Tessa Mandler, M.D.
Assistant Professor
Disclosure
I do not have any financial or research affiliations with any product or pharmaceutical manufacturer displayed in this
presentation
2
Learning Objectives
• Understand consequences of poor pain control in the ambulatory setting
• Identify ways to improve pain control for outpatient surgeries
• Discuss the suitability of single shot peripheral nerve blocks versus continuous peripheral nerve catheters for ambulatory patients
• Discuss novel management strategies of outpatient peripheral nerve catheters in the setting of limited resources
3
Consequences of Poor Pain Control
Post-operative
Pain
Rescue Opioids
Sedation
PONV
↑PACU/HopsitalLOS
↓Satisfaction
↑Respiratory Cx
↑Cost
Unplanned/Prolonged admission
4Hines R, Barash PG, Watrous G , et al. “Complications occurring in the postanesthesia care unit: a survey.” Anesth Analg. 1992;74(4):503.Kehlet H, Dahl JB. Anesthesia, surgery and challenges in postoperative recovery. Lancet 2003;362:1921–8.
5
Marcario A. Anesth Analg. 1999 Sep;89(3):652-8.
6Macario A. Anesth Analg. 1999 May;88(5):1085-91.
Mandler, Tessa, MD Outpatient Issues: Acute Pain in the Ambulatory Setting
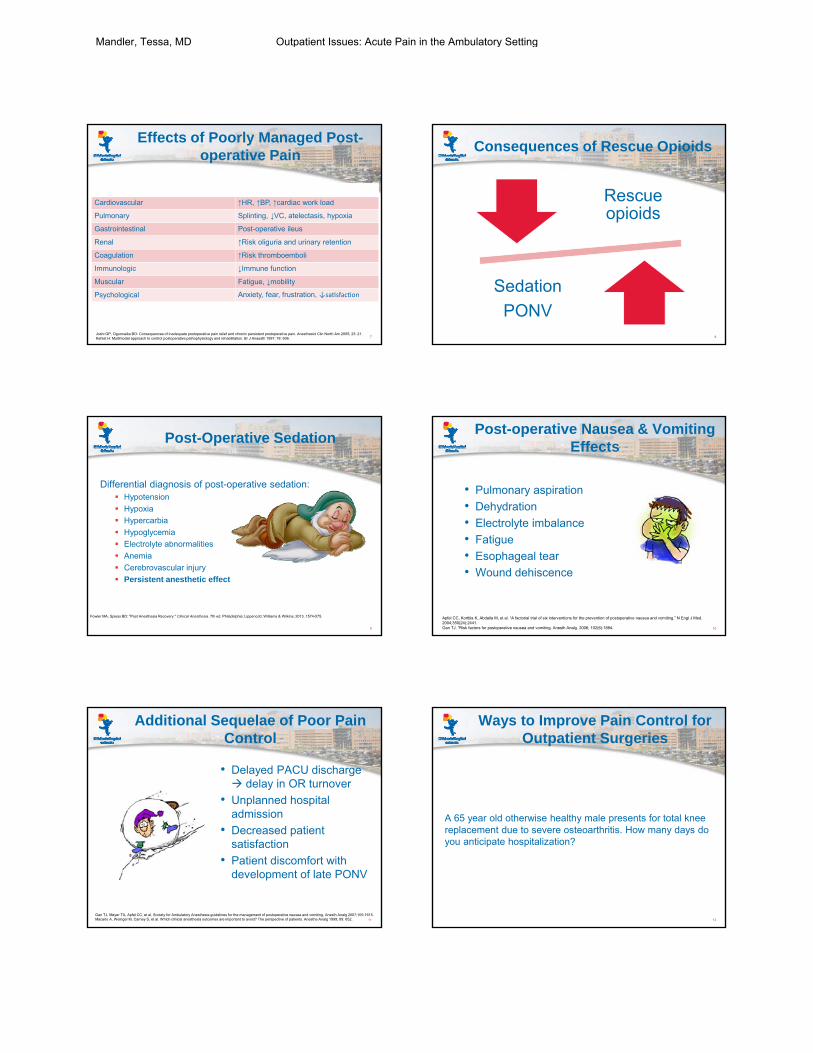
Effects of Poorly Managed Post-operative Pain
7
Cardiovascular ↑HR, ↑BP, ↑cardiac work load
Pulmonary Splinting, ↓VC, atelectasis, hypoxia
Gastrointestinal Post-operative ileus
Renal ↑Risk oliguria and urinary retention
Coagulation ↑Risk thromboemboli
Immunologic ↓Immune function
Muscular Fatigue, ↓mobility
Psychological Anxiety, fear, frustration, ↓sa sfac on
Joshi GP, Ogunnaike BO: Consequences of inadequate postoperative pain relief and chronic persistent postoperative pain. Anesthesiol Clin North Am 2005; 23: 21.Kehlet H: Multimodal approach to control postoperative pathophysiology and rehabilitation. Br J Anaesth 1997; 78: 606.
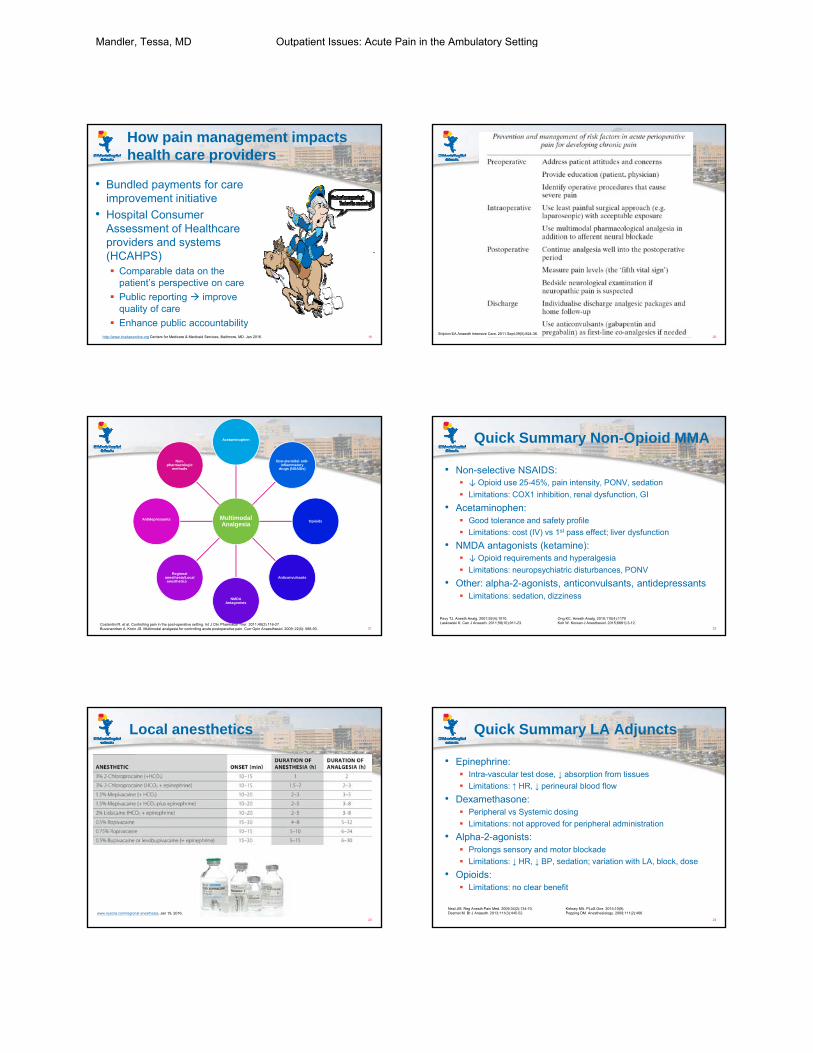
Consequences of Rescue Opioids
Rescue opioids
Sedation
PONV8
Post-Operative Sedation
Differential diagnosis of post-operative sedation: Hypotension
Hypoxia
Hypercarbia
Hypoglycemia
Electrolyte abnormalities
Anemia
Cerebrovascular injury
Persistent anesthetic effect
9
Fowler MA, Spiess BD: "Post Anesthesia Recovery." Clinical Anesthesia. 7th ed. Philadelphia: Lippencott, Williams & Wilkins, 2013. 1574-575.
Post-operative Nausea & Vomiting Effects
• Pulmonary aspiration
• Dehydration
• Electrolyte imbalance
• Fatigue
• Esophageal tear
• Wound dehiscence
10
Apfel CC, Korttila K, Abdalla M, et al. “A factorial trial of six interventions for the prevention of postoperative nausea and vomiting.” N Engl J Med. 2004;350(24):2441.Gan TJ. “Risk factors for postoperative nausea and vomiting. Anesth Analg. 2006; 102(6):1884.
Additional Sequelae of Poor Pain Control
• Delayed PACU discharge delay in OR turnover
• Unplanned hospital admission
• Decreased patient satisfaction
• Patient discomfort with development of late PONV
11
Gan TJ, Meyer TA, Apfel CC, et al. Society for Ambulatory Anesthesia guidelines for the management of postoperative nausea and vomiting. Anesth Analg 2007;105:1615.Macario A, Weinger M, Carney S, et al. Which clinical anesthesia outcomes are important to avoid? The perspective of patients. Anesthe Analg 1999; 89: 652.
Ways to Improve Pain Control for Outpatient Surgeries
A 65 year old otherwise healthy male presents for total knee replacement due to severe osteoarthritis. How many days do you anticipate hospitalization?
12
Mandler, Tessa, MD Outpatient Issues: Acute Pain in the Ambulatory Setting

13
• A 65 year old otherwise healthy male presents for total knee arthroplasty. The surgeon requests he go home the same day you therefore elect the following for his anesthetic plan:
a. Combined spinal epidural, femoral nerve catheter, ketorolac, acetaminophen, diazepam, fentanyl
b. Spinal, ketorolac, fentanyl, acetaminophen, pregabalin, diazepam
c. Spinal, ketorolac, acetaminophen, pregabalin, celecoxib
d. Combined spinal epidural, intraarticular block, ketorolac, acetaminophen
e. General anesthesia, paralytic, fentanyl, ketorolac
14
15Neurowiki, 2014 16
Chronic Pain affects us all
• Quality of life
• Psychological
• Social
• Socioeconomic
17
Page MG. J Pain Res. 2013; 6:167-80.
18
Park PW. Pain Pract. 2015 Oct 7.
Mandler, Tessa, MD Outpatient Issues: Acute Pain in the Ambulatory Setting
How pain management impacts health care providers
• Bundled payments for care improvement initiative
• Hospital Consumer Assessment of Healthcare providers and systems (HCAHPS) Comparable data on the
patient’s perspective on care
Public reporting improve quality of care
Enhance public accountability19http://www.hcahpsonline.org Centers for Medicare & Medicaid Services, Baltimore, MD. Jan 2016. 20
Shipton EA Anaesth Intensive Care. 2011 Sept;39(5):824-36.
Multimodal Analgesia
Acetaminophen
Non-steroidal anti-inflammatory
drugs (NSAIDs)
Opioids
Anticonvulsants
NMDA Antagonists
Regional anesthesia/Local anesthetics
Antidepressants
Non-pharmacologic
methods
21Costantini R, et al. Controlling pain in the post-operative setting. Int J Clin Pharmacol Ther. 2011;49(2):116-27.Buvanendran A, Kroin JS. Multimodal analgesia for controlling acute postoperative pain. Curr Opin Anaesthesiol. 2009; 22(5): 588-93.
Quick Summary Non-Opioid MMA
• Non-selective NSAIDS: ↓ Opioid use 25-45%, pain intensity, PONV, sedation
Limitations: COX1 inhibition, renal dysfunction, GI
• Acetaminophen: Good tolerance and safety profile
Limitations: cost (IV) vs 1st pass effect; liver dysfunction
• NMDA antagonists (ketamine): ↓ Opioid requirements and hyperalgesia
Limitations: neuropsychiatric disturbances, PONV
• Other: alpha-2-agonists, anticonvulsants, antidepressants Limitations: sedation, dizziness
22
Pavy TJ. Anesth Analg. 2001;92(4):1010. Ong KC. Anesth Analg. 2010;110(4):1170Laskowski K. Can J Anaesth. 2011;58(10):911-23. Koh W. Korean J Anesthesiol. 2015;6891):3-12.
Local anesthetics
23
www.nysora.com/regional-anesthesia, Jan 19, 2016.
Quick Summary LA Adjuncts
• Epinephrine: Intra-vascular test dose, ↓ absorption from tissues
Limitations: ↑ HR, ↓ perineural blood flow
• Dexamethasone: Peripheral vs Systemic dosing
Limitations: not approved for peripheral administration
• Alpha-2-agonists: Prolongs sensory and motor blockade
Limitations: ↓ HR, ↓ BP, sedation; variation with LA, block, dose
• Opioids: Limitations: no clear benefit
24
Neal JM. Reg Anesth Pain Med. 2009;34(2):134-70. Kirksey MA. PLoS One. 2015;10(9).Desmet M. Br J Anaesth. 2013;111(3):445-52. Popping DM. Anesthesiology. 2009;111(2):406.
Mandler, Tessa, MD Outpatient Issues: Acute Pain in the Ambulatory Setting

Bupivacaine liposome injectable suspension (Exparel)
• DepoFoam® slowly delivers bupivacaine ~72-96 hours analgesia
• Vial: 266 mg/20 ml 3% “free” bupivicaine
$285/each
Vial ≈ 300 mg Marcaine
25
How DepoFoam® works. Pacira Pharmaceuticals, Inc. website. http://www.pacira.com/depofoam-platform/how-it-works.php. Accessed January 20, 2016.
Bupivacaine liposome injectable suspension
• Indications: Wound infiltration to produce post-surgical anesthesia
• Safety: 21 clinical studies, >1300 patients Additive toxic effects with other local anesthetics
Most common adverse reactions (~10%): nausea, vomiting, constipation
1 ml Marcaine ≠ 1 ml bupivacaine liposome injectable solution
Maximum dose recommended is 266 mg
Caution with liver and/or renal impairment
26
Ilfeld BM. Anesth Pain Med. 2015;40(5):572-82
Bupivacaine liposome injectable suspension
27http://www.exparel.com/. Accessed January 20, 2016
Patient selection for ambulatory procedures/surgeries
28
Patient selection for regional anesthesia
Anyone and everyone!
29
Muhly WT. Local Reg Anesth. 2015 Nov 5; 8: 85-91.
Contraindications to Regional Anesthesia
Patient refusal
Infection at the site of needle/catheter placement
Coagulopathy
Allergy to local anesthetic
Pre-exiting peripheral neuropathy
Severe neurologic injury with precludes post-operative assessment for complications
30
Ecoffey C. Paediatr Anaesth. 2012;22(1):25-30.
Mandler, Tessa, MD Outpatient Issues: Acute Pain in the Ambulatory Setting

Caution! Appropriate candidate for ambulatory surgery?
• Chronic pain disorders
• Cardiac history
• Chronic lung disease
• OSA
• Craniofacial disorders
• Neuromuscular disorders
• Failure to thrive
• Morbid obesity
• Other: sickle cell disease, central hypoventilation syndromes, genetic/metabolic/storage disease, Down’s syndrome, pre-maturity
31
Marcus CL, Chapman D, Davidson WS, et al. Am Acad Ped, Pediatrics 2002; 109: 704-12.White PF. Anesth Analg 2012;114:1190-1215.
Single Shot Nerve Block
Pros:
• 12-24 hour analgesia
• Decreased opioid use
• Faster PACU discharge
• Cost effective
• Decreases stress response to surgery
• Decreases post-operative immunosuppression
Cons:
• Neuropraxia
• Hematoma
• Local anesthetic toxicity
• Infection
• Secondary injury
32
Sites BD. Reg Anesth Pain Med. 2012;37(5):478-82..Fredrickson MJ. Anaesthesia. 2009;64(8):836-44.
Peripheral Nerve Catheters
Pros:
• Decrease opioid use
• Decrease in adjuvant pain medication use
• Prolonged blockade
• ↑ patient satisfaction
Cons:
• Catheter malfunction
• Catheter site infection or bacteremia
• Increased technical difficulty and increased time
• Post-op catheter management
• “Expensive”33
Walker BJ. Br J Anaesth. 2015;115(3):457-62.Capdevila X. Anesthesiology. 2005;103(5):1035.
Cost of materials
Catheter: $475-850
Single shot block: $10-20
34
Novel management strategies of outpatient PNC’s
• Potential barriers to PNC’s: How are we going to
teach the families about the PNC without on site APS?
Who is going to order the pump and manage the catheter?
How will follow up be done?
35
• General information about catheter and medicine inside it
• How the local anesthetic is not like other pain medicines
• Risks of complications
• Care of a child with a PNC: Protect the limb
The pump is your friend
How to remove the catheter
Instructions when to call (i.e. infection, leakage, prolonged block effects, local anesthetic toxicity, etc.)
36
Mandler, Tessa, MD Outpatient Issues: Acute Pain in the Ambulatory Setting

Patient/Family Education sans APS
Face-to-face education Review highlights in the
handout
Use demo pain pump ball
Pen and paper exchange of contact information
37 38
Lessons learned in developing patient/family education materials
Communication
Consumer
APS
Education
39 40
Management of PNC
• RN’s connect pump in PACU
• APS follow up via phone +/- provider phone call
• Surgical team (i.e. post-op visits)
• Patient and his/her family
• Product representative41
Benefits Experienced
• Improved post-operative pain
• Decreased PACU length of stay
• Decreased number of unplanned admissions
• Decrease in unplanned hospital cost
42
Mandler, Tessa, MD Outpatient Issues: Acute Pain in the Ambulatory Setting

Patients that received Combined Block spent less time in the PACU
43
Fine tuning for the future
• Introduce anesthesia plan to patients pre-operatively to establish expectations and begin education on PNC’s
• Identify patient candidates for pre-operative block to ensure efficacy
• Continue to trial various combinations of the MMA wheel
44
45
Mandler, Tessa, MD Outpatient Issues: Acute Pain in the Ambulatory Setting