acute management of pediatric sports related trauma
TRANSCRIPT

Acute Management of Pediatric
Sports Related Trauma
Jonathan R. Schiller, M.D.
Assistant Professor Department of Orthopaedics
Director Adolescent and Young Adult Hip Program
The Warren Alpert Medical School of Brown University
Hasbro Children’s Hospital and Rhode Island Hospital
November 15, 2012

Faculty Disclosures
Jonathan R. Schiller, MD
Has the following financial interest to disclose:
• Depuy-Mitek Division of Hip Arthroscopy -
Educational Consultant
• Clinical Decision Support Program -
Contributor

Not covered in this talk…

Outline - Orthopaedic Injuries
• Limb injuries
• Spine injuries

Limb Injuries
• Fractures
• Dislocations
• Soft tissue injuries

Fractures
• Fractures
– Mild or limb threatening
– Establish amount of displacement
VS

Fractures
• Open vs. closed
• Sometimes may be subtle
• Even small pinholes in the skin constitute an open
fracture
• “better to overcall”

Fractures
• Neurovascular exam
– Capillary refill, pulse
– Sensation
– Motor
• Compartment syndrome

Compartment syndrome
• Muscle in limbs
enclosed in fascial
compartments
• Swelling may
dramatically increase
pressure, leading to
myonecrosis

Compartment syndrome
• Sensory changes and pain with passive stretch
• Loss of pulse - END STAGE EVENT

Fracture Management
• Open or closed
– If open, cover with
sterile bandage
– Do not replace bone
under skin
• Neurovascular status
– If pulseless, gentle
traction to align the
extremity may restore
blood flow

Fractures
• Immobilize joint above and below and
transport

Dislocations

Dislocations
• Open or closed
• Neurovascular
structures
• Compartment syndrome

Dislocations
• Differentiate from fracture
• No crepitus, gross deformity usually a clue
• Care is the same as for fracture
– Evaluate
– Immobilize
– Transport

Dislocation
• Knee dislocation - vascular compromise – 5-30%
– Rapid evaluation – ABI, arteriogram
• Suspected dislocations - spontaneously reduce
– Immobilized and referred

Soft tissue injury
• Ligamentous disruption common
• Growing children, growth plate weak link and must be evaluated in the presence of a “torn ligament”
• Immobilization, as well as a thorough neurovascular exam are performed
• “Significant” injuries (i.e. can’t weight bear) should go to the ER for evaluation


Spine Injuries

Thoracic/Lumbar Fractures
• Fortunately, rare in the acute setting
• Can be seen occasionally in contact sports
• Evaluation for associated injuries extremely
important
– Liver/spleen
– Pulmonary/cardiac contusion

Cervical Spine

Epidemiology: Football
INCIDENCE
National FB Head & Neck
Injury Registry (1971-5)
• Cervical Fx-dis : 259 (4.1/100,000)
• Quadriplegia : 99 (1.6/100,000)
Development of Modern Helmet
• Improved head protection
• Altered playing technique
• * Increased Risk C-spine Injury

Epidemiology: Football
INCIDENCE
NCAA Rules Committee (1976)
• Banned head-first contact
Progressive decrease in rate of SCI
over next decade
– Injury Rate 1985 - 2000 = stable
• 0.45/100,000 : high school
• 1.40/100,000 : college

Epidemiology: Hockey
INCIDENCE
Rare before 1980 ; increase past 20 yrs
– CANADIAN SURVEY 1966-93 (Tator )
Spine Fracture-Dislocation
– 241 total ; 16.8/yr (1982-93)
– 90% in Cervical region
Spinal Cord Injury
– Permanent SCI : 108
– Complete lesion : 52
– Deaths : 8
Epidemiology: Hockey
CATASTROPHIC CERVICAL TRAUMA
American FOOTBALL : higher total # per year
Canadian HOCKEY : annual incidence 3 X greater
U.S. High School Data – Annual Incidence
Football : 0.68/100,000
Hockey : 2.56/100,000
Epidemiology: Hockey
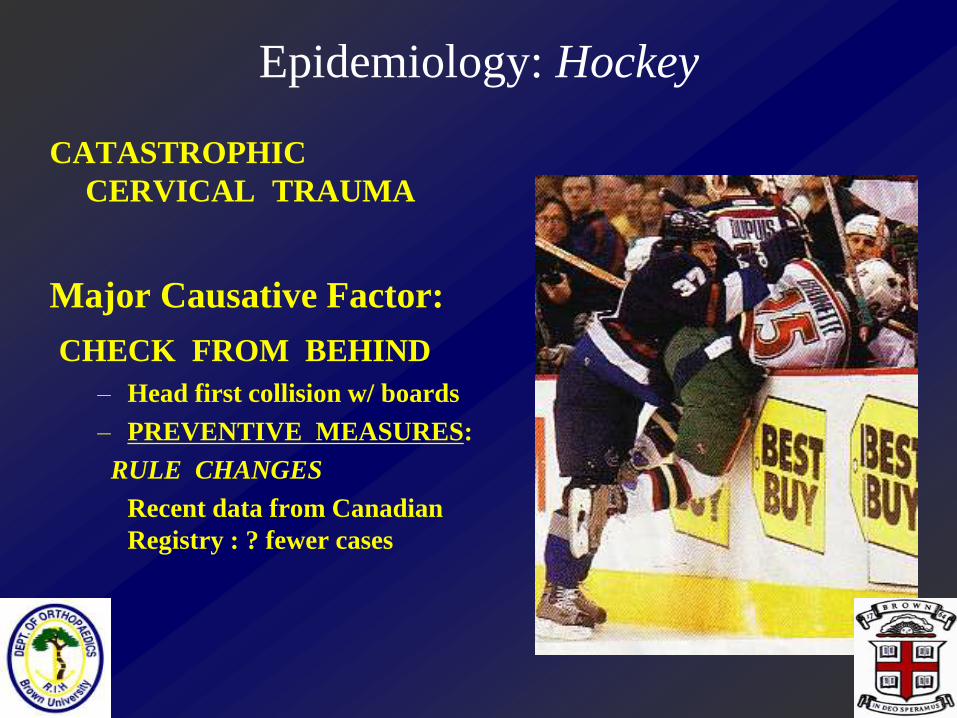
CATASTROPHIC
CERVICAL TRAUMA
Major Causative Factor:
CHECK FROM BEHIND
– Head first collision w/ boards
– PREVENTIVE MEASURES:
RULE CHANGES
Recent data from Canadian
Registry : ? fewer cases

Clinical Anatomy
SPINAL CANAL
Shape of a “funnel”
Cross-sectional area
occupied by cord
• < 50% at C1
• 75% from C4-C7
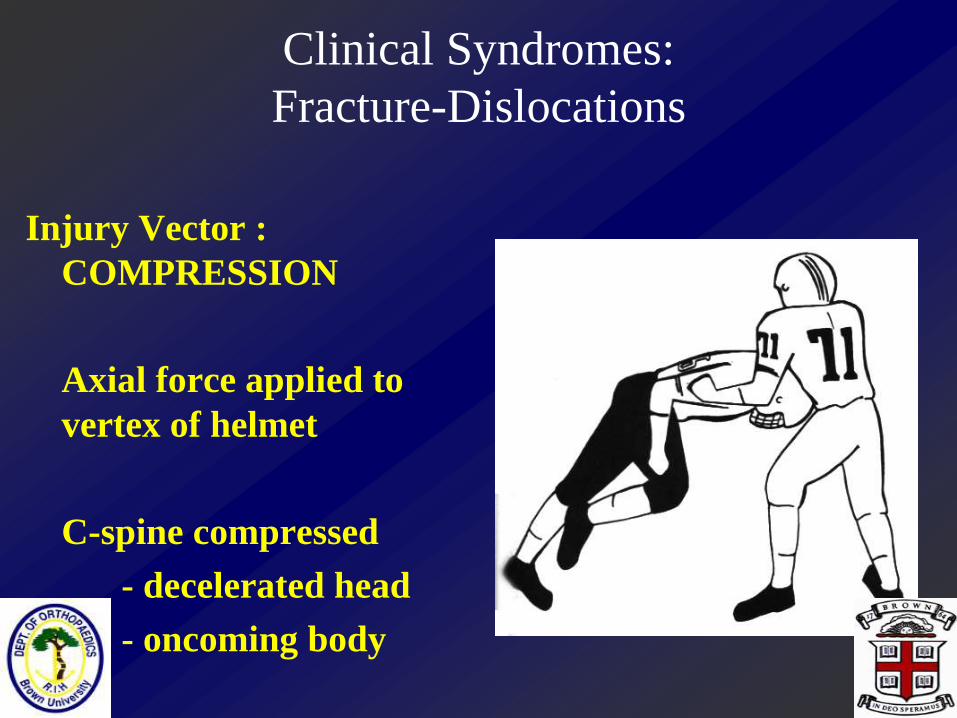
Clinical Syndromes:
Fracture-Dislocations
Injury Vector :
COMPRESSION
Axial force applied to
vertex of helmet
C-spine compressed
- decelerated head
- oncoming body

Clinical Syndromes:
Fracture-Dislocations
Injury Vector :
COMPRESSION
Cadaveric Studies
– C-spine
• straight
• colinear w/ axial load
– Response to compression:
BUCKLING

Clinical Syndromes:
Fracture-Dislocations
Fracture Pattern:
Compressive-Flexion
Highly unstable
Often assoc. w/ SCI

Cervical Spine
• Persisent neck pain
warrants evaluation
• Any neurologic
symptoms need to be
taken seriously
• Transport to ER if
unsure for eval
• Assume the spine is
UNstable

Spine injury-evaluation

ON-SITE EVALUATION & MANAGEMENT
Primary Survey
OBJECTIVES
– Assess for life-threatening conditions
– Prevent further injury
SEQUENCE OF TRAUMA CARE :
Airway (+ c-spine protection)
Breathing and ventilation
Circulation
Disability / neurologic status
Exposure

PRIMARY SURVEY
Normal Mental Status & Cardiorespiratory Status
Athlete awake & communicative
– r/o compromise of ABC
SECONDARY SURVEY
Neurologic exam
Suspect Catastrophic Neck Injury
• Findings referable to cord damage
• Serious neck pain
• Focal spinal TTP
• Restricted cervical ROM

PRIMARY SURVEY
Altered Mental Status
Depressed LOC
• Assume C-spine Injury!!!
– Manual immobilization
– Remove facemask

PRIMARY SURVEY
Cardiopulmonary Compromise
OBJECTIVES
• Identify hypoxia
• Intervene => proper ventilation
• Avoid injury spine/n. elements
Assume catastrophic neck injury
PROTECT CERVICAL SPINE
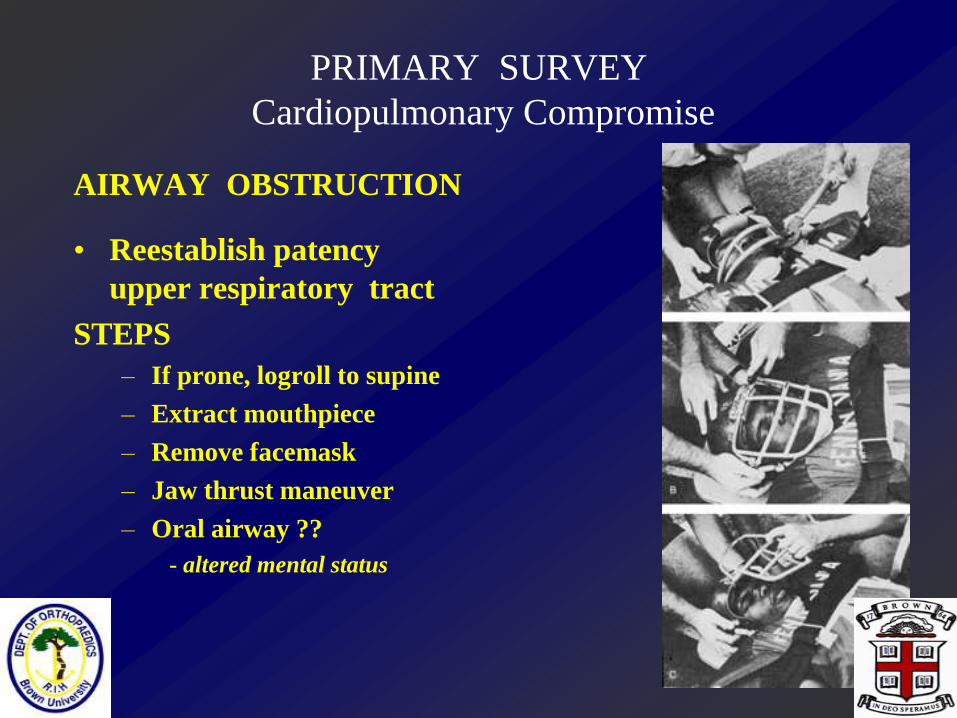
PRIMARY SURVEY
Cardiopulmonary Compromise
AIRWAY OBSTRUCTION
• Reestablish patency
upper respiratory tract
STEPS
– If prone, logroll to supine
– Extract mouthpiece
– Remove facemask
– Jaw thrust maneuver
– Oral airway ??
- altered mental status

PRIMARY SURVEY
PULSE EVALUATION
Decreased amplitude + bradycardia
– Neurogenic shock ; cervical SCI
Rapid & thready w/ normal rhythmn
– Hypovolemic shock (? splenic injury)
Irregular rhythmn
– Cardiac dysfunction
Absent central pulses
– Need for CPR

IMMOBILIZATION & TRANSPORT
Secondary Survey complete
Log roll to backboard
Immobilize C-spine
– HELMET & SHOULDER PADS
IN PLACE
*n.b. basic science data

Spinal Injury
• Transport to emergency department for
emergency care
• Steroid protocol
• +/- surgery

Herniated Discs in Children
• Less commonly seen than in the adult
population
• Can be seen with exertion (i.e. weightlifting)
• Male slightly greater than female
• Early degenerative changes often seen on MRI
in these patients
• Patients may be predisposed :
– Congenitally narrow canal
– familial cases of HNP
• In the growing child, ring apophysis fracture
(RAF) must also be considered
• Pop in back during heavy lifting is classic

Ring Apophysis Fracture

HNP/RAF
• Usually below spinal cord level, so pathology
is of the individual nerve root
• Large central herniations can compress the
cauda equina, leading to bowel and bladder
dysfunction
• Evaluation should include sensory and motor,
as well as specific question regarding perianal
sensation

• Conservative treatment
• Surgery refractory symptoms

MRI
16 year old powerlifter…


Summary
• More and more children
each year are involved in
sports
• Recognition of the need to
prevent injuries has helped
lower the risk
• Potentially catastrophic
injuries can occur and
require prompt recognition
and treatment

Summary
• Cooperation between all
members of the health
care team is essential