acute kidney injury syndromes - nephrology2021.com
TRANSCRIPT

Acute Kidney Injury Syndromes
Alice M. Sheridan, MDDivision of Nephrology
Brigham and Women’s Hospital

Alice M. Sheridan, MD
• New York Medical College
• Medicine Residency @ BMC
• Nephrology Fellowship Fellowship @BMC
• Associate Professor of Medicine@ HMS
• Clinical focus: General nephrology
• Editorial Director of nephSAP

Disclosures
• I have no relevant financial disclosures

Objectives
• To define the common syndromes that underlie acute kidney injury (AKI)
• To describe the clinical presentation and prognosis of select syndromes

AKI definition
• A group of syndromes characterized by an acute decrease in glomerular filtration.
• The degree of reduction in glomerular filtration and/or urine output provide the sole criteria for diagnosis.
• Acute Dialysis Quality Initiative (2004) and revised by the AKI network (2007) and KDIGO (2012)

KDIGO
• - An increase in serum creatinine by > 0.3 mg/dL (>26.5 micromol/L) within 48 hours, or
• - An increase in serum creatinine to > 1.5 times baseline, which is known or presumed to have occurred within the past 7 days, or
• - Urine volume <0.5 mL/kg/hour for six hours.
• Acute Kidney Disease (AKD) was defined by KDIGO as a decline in glomerular filtration that persists for three months, and thus includes the AKI definition.

Pro…
• A common definition based on easily acquired data allows comparison of broad outcomes across populations.

Con…
• Functional classification tells us nothing about the underlying cause.
• Clinically• Estimates of prognosis are skewed toward ATN
• Research• Does not encourage development of precision cellular and genomic
therapeutics

There is room for both…
• A unifying diagnosis allow identification of clinically important outcomes.
• It is up to the clinician to identify when their patient departs from the norm…. (Proteinuria? Hematuria? Active sediment? )
What are the underlying syndromes
• Prerenal/acute tubular necrosis
• Hepatorenal
• Cardiorenal
• Rapidly progressive glomerulonephritis
• Acute interstitial nephritis
• Crystalopathies
• Obstruction
AKI-EPI Study
• Prerenal/acute tubular necrosis • Sepsis 41%• Hypovolemia 34%
• Hepatorenal 3.2%
• Cardiorenal • Cardiogenic shock 13%
• Rapidly progressive glomerulonephritis
• Acute interstitial nephritis• “Drug related” – 14%
• Crystalopathies
• Obstruction (1.4%)
Hoste et al, Intensive Care Medicine 2015 41: 1411
Case 1
• This patient presented to his primary care physician with nausea and vomiting and found to have creatinine of 6.1 mg/dL. Urinalysis showed 4+ heme
• Four days prior he had developed calf pain during hike). Took ibuprofen 200 mg during hike + 400 mg that evening. Urine turned dark after onset of pain.
• He has had multiple episodes exactly like this (10-12 over past ten years).

Case 1 continued
• The urine was noted to be red. After centrifugation, the sample remained red. Centrifuged plasma sample was yellow.

Case 1 continued
What is the most likely cause of his acute kidney injury?
A. Intermittently obstructing stone with gross hematuriaB. RhabdomyolysisC. Acute intermittent porphyriaD. Paroxysmal nocturnal hemoglobinuria

Case 1 continued
The best answer is
A. Intermittently obstructing stone with gross hematuriaB. RhabdomyolysisC. Acute intermittent porphyriaD. Paroxysmal nocturnal hemoglobinuria

Red urine, dip + for heme
Cause Urine dipstick heme
Sediment Supernatant
Hematuria ++ red clear
Myoglobinuria ++ normal Red/brown
Hemoglobinuria ++ normal Red/Brown
Porphyria -- Normal Red
Bosch et al, NEJM 2009: 361 p62
Gross hematuria clears upon centrifugation of urine. The urine supernatant remains RED in rhabdomyolysis, hemoglobinuria and porphyria

Plasma in hemolysis versus rhabdomyolysis
• Plasma supernatant may remain RED in hemolysis / hemoglobinuria due to hemoglobin’s large size compared to myoglobin (which is filtered and cleared).
• Creatinine phosphokinase >28,000

Causes of rhabdomyolysis
• Crush syndrome, limb compression• Strenuous exercise, seizures• Disorders of glycolysis, glycogenolysis, lipid metabolism• Infections (Influenza A and B, COVID), coxsackie-virus, HIV, EBV,
Strep, Staph,• Heat stroke, malignant hyperthermia, malignant neuroleptic
syndrome• Hypokalemia, hypophosphatemia, hypocalcemia, DKA• Drugs: fibrates, statins, alcohol, heroin, cocaine

Neuromuscular causes of rhabdomyolysis
• McArdle’s disease• Carnitine palmitoyle transferase deficiency• Muscular dystrophies (Becker, limb girdle) • Clinically evident ATN is uncommon• Chronic tubulointerstitial nephritis has been described in patients
with McArdle’s , and other myopathies
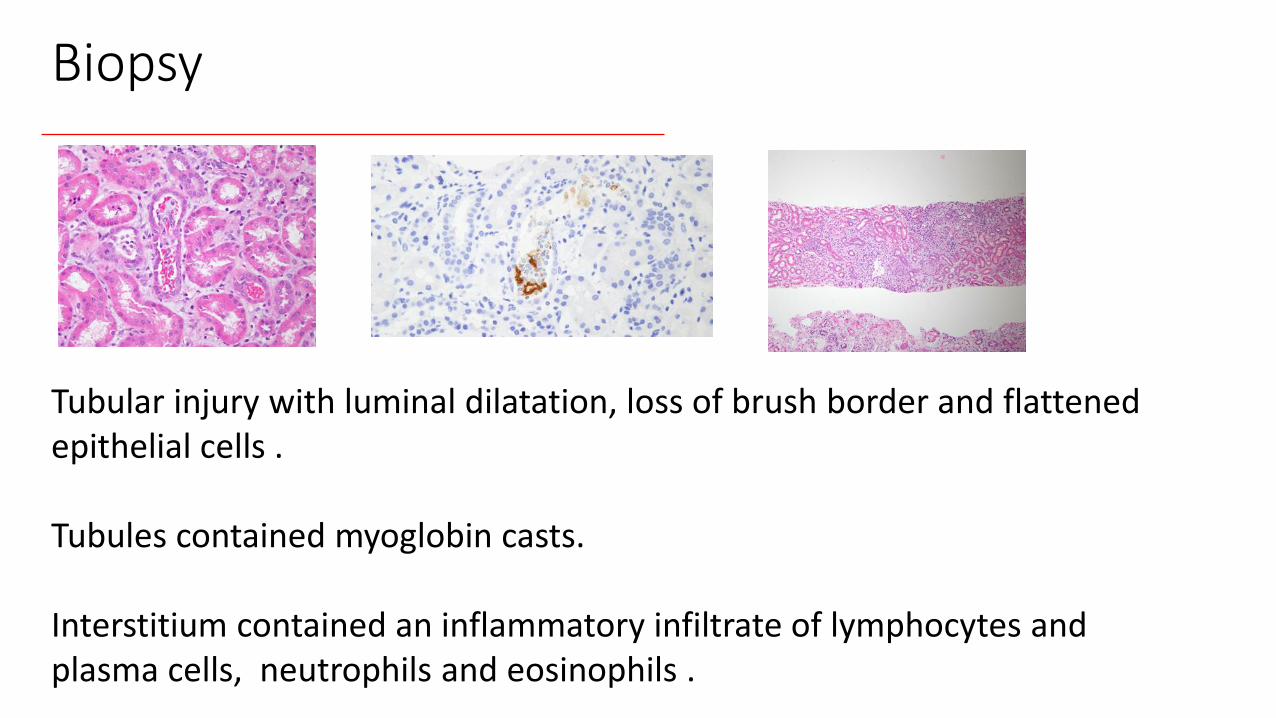
Biopsy
Tubular injury with luminal dilatation, loss of brush border and flattened epithelial cells .
Tubules contained myoglobin casts.
Interstitium contained an inflammatory infiltrate of lymphocytes and plasma cells, neutrophils and eosinophils .

Case 2
A 39 year old man is admitted to a New York City hospital with fevers chills, anosmia and dyspnea. He rules in for COVID. His creatinine is 2.3 mg/dL on admission and progresses to 4.5 mg/dL . He has hematuria and 4.5 grams proteinuria on 24 hour collection. All of the following statements are true EXCEPT:
A) AKI worsens his prognosisB) AKI increases his risk of end stage kidney diseaseC) The proteinuria is unlikely to be related to COVID and is most likely
due to prior lesionD) Prerenal AKI and ATN are the most likely causes of AKI in COVID
patients.
Case 2
A 39 year old man is admitted to a New York City hospital with fevers chills, anosmia and dyspnea. He rules in for COVID. His creatinine is 2.3 mg/dL on admission and progresses to 4.5 mg/dL . He has hematuria and 4.5 grams proteinuria on 24 hour collection. All of the following statements are true EXCEPT:
A) AKI worsens his prognosisB) AKI increases his risk of end stage kidney diseaseC) The proteinuria is unlikely to be related to COVID and is most likely
due to prior lesionD) Prerenal AKI and ATN are the most likely causes of AKI in COVID
patients.

AKI in COVID patients
• Incidence of AKI depends on population.
• Three NY cohorts, approximately 35 to 45 percent
• Multicenter US cohort, 21 % ICU admissions developed KRT-requiring AKI within 14 days.

AKI increases COVID mortality• From Wuhan, mortality was 62, 77 and 80 percent in patients with
AKI stages 1, 2 and 3 respectively. Cheng et al. CJASN 2020: 15; 1394.
• Multicenter US cohort, mortality was 60 % among ICU patients with KRT-requiring AKI. Gupta et al, JASN 2021: 32: 161
• NYC cohorts, mortality was 45 to 50 % among patients with AKI. Chan
et al. CJASN 2021; 32: 151; Ng et al, AJKD2021,: 77; 204
• After adjusting for severity , compared with COVID patients without AKI, mortality risk was higher for those with AKI without dialysis (hazard ratio 3.4) and with dialysis (hazard ratio 6.4). Ng et al, AJKD 2021,:
77; 204

AKI increases risk of ESRD
• Multicenter study among patients with KRT-requiring AKI, approximately 1/3 require dialysis by discharge and 1/5 were still on dialysis 2 months later. (Gupta S et a. JASN 2021: 32:161

Causes of AKI
• Pre-renal and ATN are most common causes of AKI • Numerous coincident glomerular lesions have been reported
• IgA• minimal change disease• Membranous • collapsing glomerulopathy
• High risk APOL1 genotype• Possibly related to g- interferon

Causes of AKI
• Pre-renal and ATN are most common causes of AKI • Numerous coincident glomerular lesions have been reported
• IgA• minimal change disease• Membranous • collapsing glomerulopathy
• High risk APOL1 genotype• Possibly related to g- interferon

Case-3
• 50 yarr old man referred for increased creatinine (1.1 1.48 mg/dL) noted over 3 months in setting of starting ACE inhibitor.
• ACE inhibitor stopped. Repeat creatinine stable at 1.40 to 1.50 mg/dL
• PMAH remarkable for new onset hypertension and osteoporosis

Case-3
• Urinalysis showed trace wbc on one occasion, sediment no casts, no crystals
• microalbumin/creatinine ratio normal• SPEP, light chains negative, total /ionized calcium normal• ANCA, ANA, dsDNA, anti-Ro/anti-La negative• C3,C4 normal
Case-3
Presentation is consistent with, though not diagnostic of A. Oxalate nephropathy
B. Acute interstitial nephritis
C. Post streptococcal glomerulonephritis
D. All of the above
E. A and B but not C

Case-3
Presentation is consistent with, though not diagnostic of A. Oxalate nephropathy
B. Acute interstitial nephritis
C. Post streptococcal glomerulonephritis
D. All of the above
E. A and B but not C
Biopsy
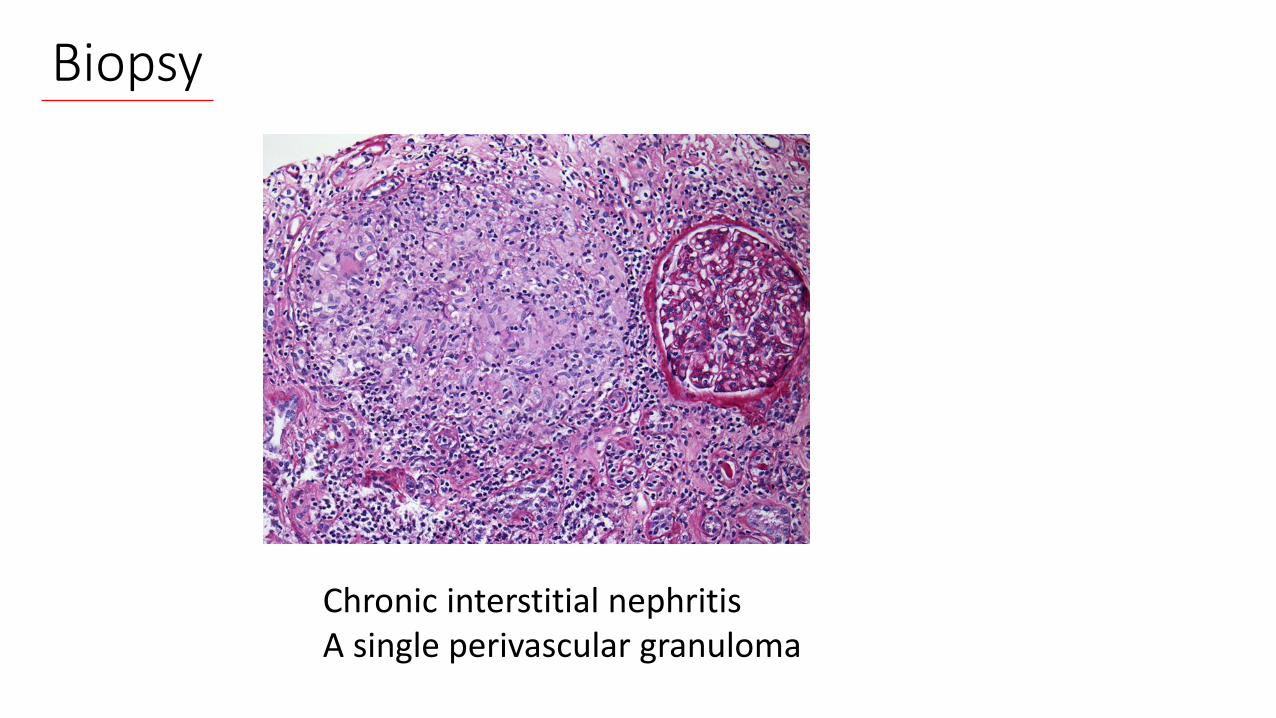
Chronic interstitial nephritisA single perivascular granuloma

Acute Interstitial Nephritis
• Common cause of unexplained AKI
• Drug related in >70 %
• Infections (legionella, leptospirosis, CMV, streptococcus)
• SLE
• Sjogren’s
• TINU (tubulointerstitial nephritis + uveitis) syndrome

Granulomatous Interstitial Nephritis
• Less common form of interstitial nephritis
• Drug related
• Infection - Mycobacterium, fungus (histoplasmosis, coccidiomycosis), bacteria, spirochetes, parasites.
• Tubulointerstitial nephritis and uveitis (TINU)
• Sarcoidosis
• Granulomatosis and polyangiitis (GPA)
Evaluation
• Drug review (NSAIDs, PPI, Antibiotics).
• ANCA, ACE, ANA, C3, C4, dsDNA
• Look for Infection - Mycobacterium, fungus (histoplasmosis, coccidiomycosis), bacteria, spirochetes, parasites.
• Sarcoid – Imaging (CXR, CT, bronchoscopy)
• Tubulointerstitial nephritis and uveitis (TINU)

Three syndromes
• Recurrent ATN
• COVID- AKI
• AIN

References- AKI
• KDIGO Clinical Practice Guideline for Acute Kidney Injury Kidney Int. 2012;2:1-141.
• Bellomo R, et al. Acute renal failure - definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004;8(4):R204-12.
• Mehta RL, et al. Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Crit Care. 2007;11(2):R31.
• Hoste EA, et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med. 2015;41(8):1411-23.

References- ATN• Melli G, et al. Rhabdomyolysis: an evaluation of 475 hospitalized
patients. Medicine (Baltimore). 2005 Nov;84(6):377-85.• Bosch X, et al. Rhabdomyolysis and acute kidney injury. N Engl J Med.
2009 Jul 2;361(1):62-72. doi: 10.1056/NEJMra0801327. Review. Erratum in: N Engl J Med. 2011 May 19;364(20):1982.
• McCarron DA, et al . Chronic tubulointerstitial nephritis caused by recurrent myoglobinur1a. Arch Int Med 1980:140:1106-7

References- COVID and AKICheng Y, et al: The Incidence, Risk Factors, and Prognosis of Acute Kidney Injury in Adult Patients with Coronavirus Disease 2019. Clin J Am Soc Nephrol CJASN 15: 1394–1402, 2020Hirsch JS, et al: AKI in Hospitalized Patients with COVID-19. J Am Soc Nephrol JASN 32: 151–160, 2021Chan L, et al: Characterization and clinical course of 1000 patients with coronavirus disease 2019 in New York: retrospective case series. BMJ 369: m1996, 2020Mohamed MMB, et al: Acute Kidney Injury Associated with Coronavirus Disease 2019 in Urban New Orleans. Kidney360 1: 614–622, 2020Gupta S, et al: AKI Treated with Renal Replacement Therapy in Critically Ill Patients with COVID-19. J Am Soc Nephrol JASN 32: 161–176, 2021Cheng Y, et al : Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int Friedman DJ: COVID-19 and APOL1: Understanding Disease Mechanisms through Clinical Observation. J Am Soc Nephrol 32: 1–2, 2021

References- AIN
• González E et al; Grupo Madrileño De Nefritis Intersticiales. Early steroid treatment improves the recovery of renal function in patients with drug-induced acute interstitial nephritis. Kidney Int. 2008 Apr;73(8):940-6.
• Clarkson MR et al. Acute interstitial nephritis: clinical features and response to corticosteroid therapy. Nephrol Dial Transplant. 2004 Nov;19(11):2778-83.
• Mahevas M at al. Renal Sarcoidosis. Clinical, Laboratory and Histologic Presentation and Outcome in 47 patients. Medicine 2009: 88; 98-106