acute hiv in north carolina std clinics the north carolina stat project peter a. leone, md associate...
TRANSCRIPT

Acute HIV in North Carolina STD ClinicsThe North Carolina STAT Project
Peter A. Leone, MD
Associate Professor of Medicine
University of North Carolina
Medical Director,
NC HIV/STD Prevention and Care, NCDHHS

Acute HIV
• The window period between:
- Appearance of HIV in blood
- Host Antibody response
• Seroconversion defined as “confirmed” by + WB
• Time period (4-8 weeks) may narrow with newer generation ELISAs

Couthino et al., Bulletin of Mathematical Biology 2001

Diagnostic Testing Timeline
0 1 2 3 4 5 6 7 8 9 10
Symptoms
p24 AntigenHIV RNA
HIV ELISA
Weeks Since InfectionRecombinant peptide ELISA
Viral lysate ELISA Fiebig et al, AIDS 2003;17(13):1871-9

Rationale for Acute HIV Diagnosis
• Most Infectious period and Dx often missed• Individual Perspective
– Improve prognosis with acute treatment????– Early entry into care
• Public Health– Recognized previously missed infections– Avoid transmission to partners with risk reduction
• 10-100 fold increased transmission risk x 4-6 months• May be responsible for 30-50% of all transmission of HIV
- Identify Transmission networks for intervention

Pitfalls in AHI
• Diagnosis rarely pursued/rare event
• Majority of patients may be asymptomatic
• Signs and symptoms non-specific– few clues
• Laboratory testing must be directed
• Linkage to surveillance and PCRS in real time
Kahn JO, Walker BD, N Engl J Med1998;339: 33-39.

The North Carolina STAT Project

NC Approach to detection of AHI
• Screening of all HIV Ab negative or WB indeterminate Blood from public clinics for HIV RNA ( ~120,000 tests/year)
• Review of all community cases
- Ab neg., HIV RNA +
- Ab.+ with Hx neg. HIV Ab within 3 mo
- Ab + but with recent acute symptoms

Our approach to Screening for AHI Specimen pooling
• Advantages Reduced cost No change in specificity
Universal screening
• DisadvantagesRequires large testing volumeTrade off in sensitivityLogistics
Time to locating patient
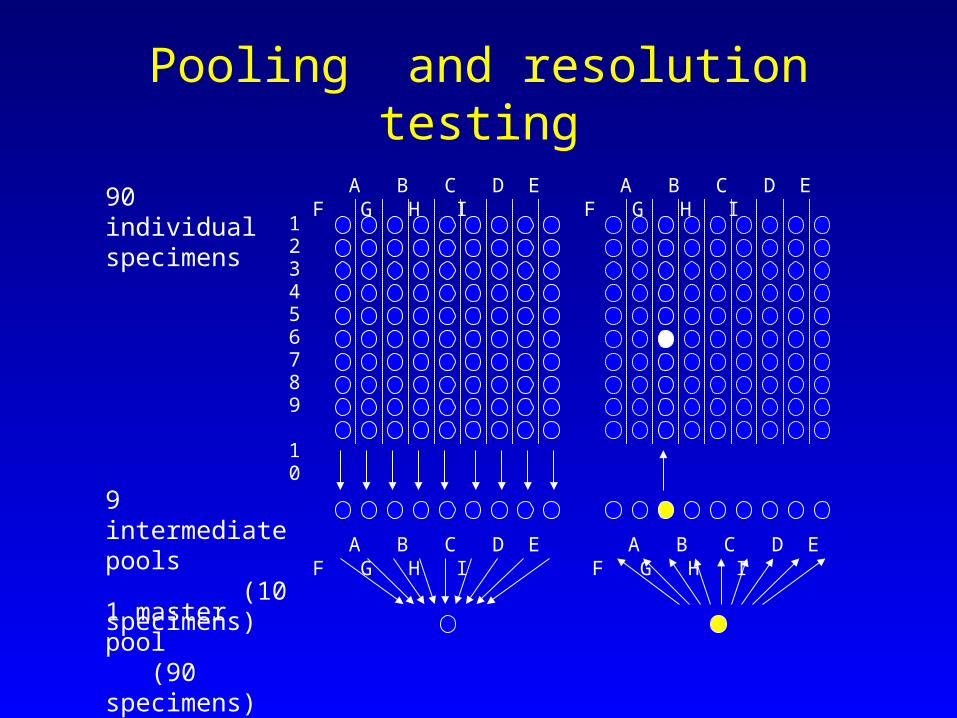
A B C D E F G H I
1 2 3 4 5 6 7 8 9 10
A B C D E F G H I
A B C D E F G H I A B C D E F G H I
90 individual specimens
9 intermediate pools (10 specimens)
1 master pool (90 specimens)
Pooling and resolution testing

NC STATAll Testing Sites
Nov.1, 2002- May 1,2005• Number screened: 287,760
• Number of Ab+: 1,379
• Number of AHI: 58
• AHI represents ~4.0% of all HIV infected

Testing Site Type
#Tests Ab+ AHI (%) Total AHI (%)
HIV CTS 18,299 400 12 (2.9) 21%
STD 117,804 526 27 (4.9) 48%
FP 47,476 28 -- --
Prenatal/OB 47,598 39 2 (4.9) 3%
Prison/Jail 7,158 57 4 (6.6) 7%
Other 37,073 320 13(3.9) 22%
Distribution of
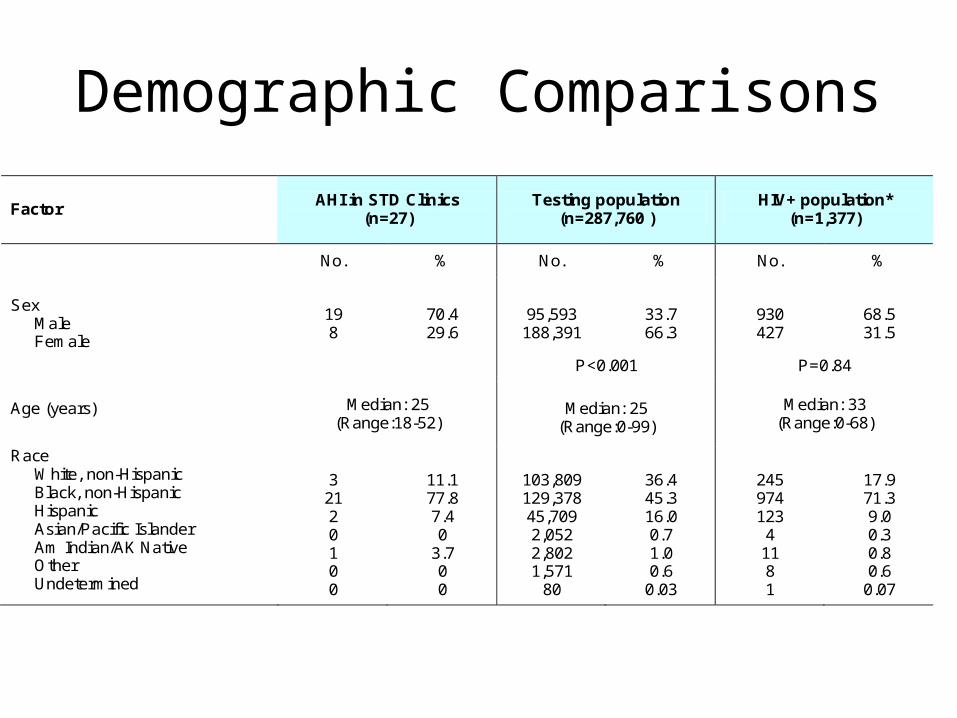
Demographic Comparisons
Factor AHI in STD Clinics
(n=27) Testing population
(n=287,760 ) HIV+ population*
(n=1,377)
No. % No. % No. %
Sex
Male Female
19 8
70.4 29.6
95,593 188,391
33.7 66.3
930 427
68.5 31.5
P<0.001 P=0.84
Age (years) Median: 25
(Range:18-52)
Median: 25
(Range:0-99) Median: 33
(Range:0-68)
Race White, non-Hispanic Black, non-Hispanic Hispanic Asian/Pacific Islander Am Indian/AK Native Other Undetermined
3 21 2 0 1 0 0
11.1 77.8 7.4 0
3.7 0 0
103,809 129,378 45,709 2,052 2,802 1,571
80
36.4 45.3 16.0 0.7 1.0 0.6
0.03
245 974 123 4 11 8 1
17.9 71.3 9.0 0.3 0.8 0.6
0.07
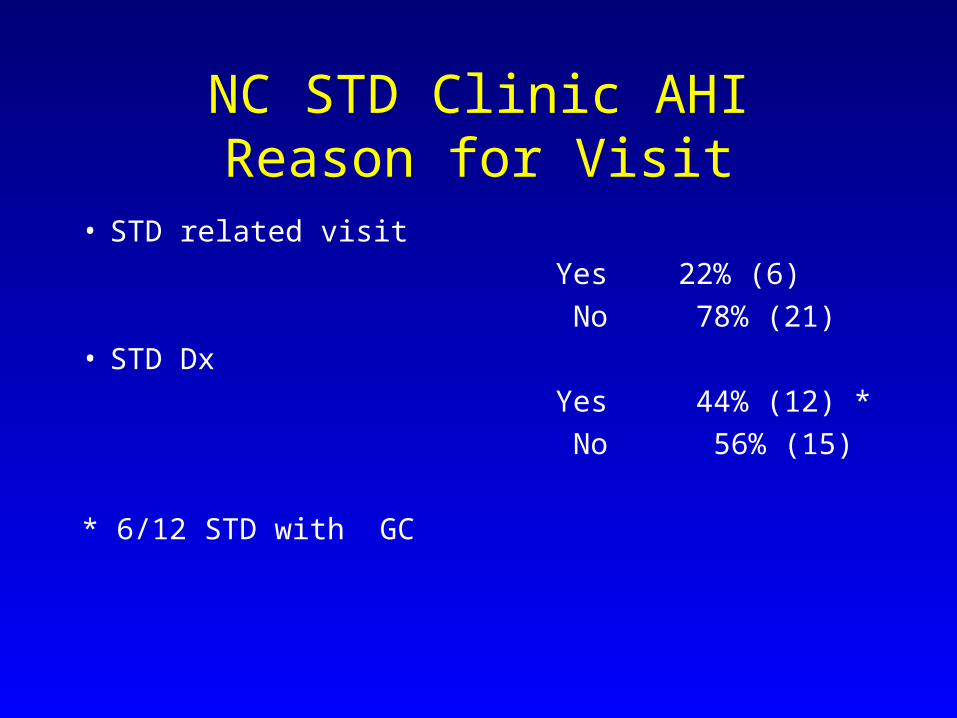
NC STD Clinic AHIReason for Visit
• STD related visit
Yes 22% (6)
No 78% (21)• STD Dx
Yes 44% (12) *
No 56% (15)
* 6/12 STD with GC

AHI and Symptoms
• 49-89% symptomatic (Schacker TW, et al., AIM 1996 125:257-64)
• SymptomsSchacker Kinloch-de Loes
NCSTDFever 93% 87% 48%Fatigue 93 26 37 Pharyngitis 70 48
30Headache 55 39 26Rash 15GI Symptoms 37
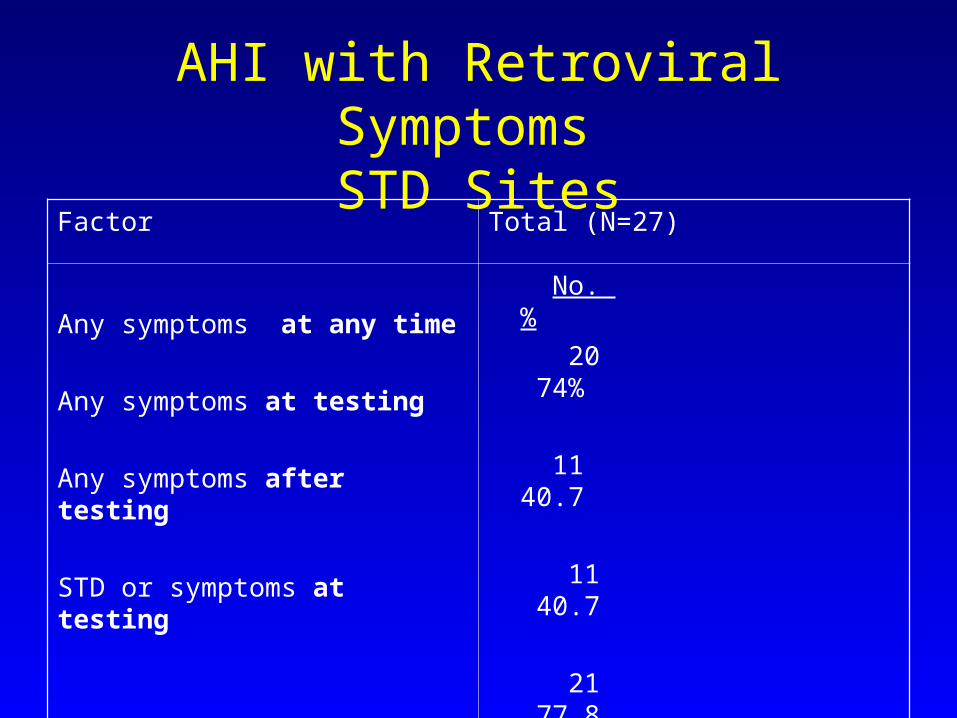
AHI with Retroviral Symptoms STD Sites
Factor Total (N=27)
Any symptoms at any time
Any symptoms at testing
Any symptoms after testing
STD or symptoms at testing
No. %
20 74%
11 40.7
11 40.7
21 77.8

Specific Symptoms at Time of Testing in STD Clinics
Symptoms Total (%)
Fever
Fatigue
GI Symptoms
Pharyngitis
Headache
Rash
Lymphadenopathy
6 (22%)
5 (18)
5 (18)
3 (11)
3 (11)
1 (4)
1(4)
Why Pursue AHI in STD Clinic Populations
• Entry point for high risk individuals
• High % of AHI in public health setting
• Overlap of incubation periods of classic STIs and HIV
• Already drawing blood for syphilis
• Opt out approach for HIV testing
Incorporating AHI Screening in STD clinics:
1. Screen all
2. Rapid Test “Plus”
-Rapid HIV tests can be offered with symptom screen
Problem: Which symptoms (fever?) over what time period (2-4 wks)?
Symptoms at best will detect 40%
- Targeted screening
based on risk ( i.e. MSM, anal/vaginal sex in past 2 weeks,etc )
based on site prevalence or type
3. Bottom line- rapid testing and AHI screening are not mutually exclusive -Need for further research to define symptom screen and develop predictive
models for AHI screening

Women with AHICase Age Race Testing Site Risk Factor
1 36 Black Nontraditional Injection Drug Use2 34 Amind STD Clinic Heterosexual3 44 Black STD Clinic Heterosexual4 29 White Prison Heterosexual5 35 Black STD Clinic Heterosexual6 41 Black STD Clinic Heterosexual7 21 Black STD Clinic Heterosexual8 48 Hispanic Nontraditional Heterosexual9 16 Black Prenatal/OB Heterosexual
10 28 Black STD Clinic Heterosexual11 25 Black HIV CTS Heterosexual12 18 Black STD Clinic Heterosexual13 21 Black STD Clinic Heterosexual14 22 Hispanic Prenatal/OB Heterosexual15 41 White Other Injection Drug Use16 32 Black HIV CTS Heterosexual
5/16 AHI women were pregnant at the time of testing. All were initiated on ART, received AZT at delivery, as did their infants. None of the infants were infected.
During this same frame, there were 6 HIV+ infants born in NC. 3/6 infants were born to women who retrospectively were found to have seroconverted after having undergone routine HIV testing earlier in pregnancy. This supports the use of a repeat testing strategy in pregnant women.

Pregnancy Conclusion
• STAT was effective in identifying 5 AHI pregnant women, resulting in prompt initiation of ART and, ultimately, preventing transmission of HIV to these at risk infants.
• Three of the 6 women who delivered HIV-infected infants during this same period seroconverted after undergoing HIV testing early in pregnancy. The strategy of AHI screening or repeat HIV testing is most likely highly cost effective due to the high risk and rate of vertical transmission in acutely infected pregnant women. A formal cost effectiveness analysis is in progress.
• Despite our overall low numbers of perinatal transmission, NC’s universal enhanced screening strategy has had an impact on the residual transmission of MTCT in our state.
Recommendations
• The residual cases of perinatal transmission may be reduced further if the following strategy were to be implemented domestically:
• Universal HIV testing of all pregnant women early in pregnancy. For all Ab(-) women, reflex testing with HIV RNA.
• For women who do have reflex RNA testing and are negative, repeat HIV Ab testing in the third trimester.
• All women who were Ab(-) RNA (-) early in pregnancy and did not have repeat testing in the third trimester, rapid testing with reflex HIV RNA at the time of delivery should be performed.
• All Ab(+) or Ab(-)RNA(+) pregnant women should be initiated on ART as soon as possible.
AcknowledgementsNC DHHSEvelyn FoustJ. Todd McPhersonLou TurnerLeslie WolfTodd VanhoyRhonda AshbyDel WilliamsSteve Beagle
North Carolina DIS
NIMH , NIDDK, HPTN, UNC Fogarty Center, UNC STD CRC, UNC CFAR
UNC-Chapel Hill Christopher PilcherSusan A. FiscusJoseph J. Eron, JrJoAnn KurucMyron S. CohenKris PattersonWilliam C. MillerTrang Q. NguyenSandi McCoy