acute assessment and managemen - med.unc.edu · acute assessment and managemen . when a concussion...
TRANSCRIPT

This reference sheet on the assessment and management of concussion is adapted from the article Sports Concussion by Jeffrey S Kutcher MD MPH Christopher C Giza MD and Anthony G Alessi MD MMM FAAN in the December 2010 issue of Continuum Lifelong Learning in Neurologyreg (Traumatic Brain Injury Vol 16 No6) Additional input was provided by Jeffrey S Kutcher MD MPH and Christopher C Giza MD lead authors of the update to the American Academy of Neurology (AAN) guideline (Neurologyreg 199748581-585) regarding management of sports concussion
The information provided in this reference sheet is not evidence based The updated gUideline (in press) may present evidence that contradicts the information presented here
Concussion is a brain injury caused by biomechanical forces and generally characterized by the rapid onset of a set of neurologic symptoms or cognitive impairment The injury is typically self-limited and resolves spontaneously Concussion commonly arises from sports injuries which account for between 16 and 38 million concussions annually in the United States Nearly nine percent of all US high school sports injuries involve concussions A small percentage of concussions can be ser ious leading to prolonged symptom course significant morbidity or even death (For more information on sports concussion and traumatic brain injury refer to the December 2010 issue of Continuum Lifelong Learning in NeurologyregJ
Increasing media coverage and government regulation of concussion management have boosted public awareness of this preva lent and potentiall y serious condition Clinicians thus are advised to learn about their states laws concerning concussion management Visit wwwaancomgoaboutsectionssports for information on concussion laws by state
Current Clinical Trends The 1997 guideline provides a grading system for acute concussion symptoms However subsequent research suggests that this grading system does not predict long-term symptom occurrence or outcomes Rather it is important to treat concussion on a case-by-case basis taking into account the unique circumstances of the affected indi vidual and the injury event Thus clinicians should consider their clinical experience to be more va luable than a written protocol in their decision making A multidisCiplinary panel is currently updating the 1997 guideline and examining the best available evidence for concussion management
The assessment of concussion is a complex process However assessing concuss ion in athletes poses particular challenges Because many sports involve physical impact the source of head injury in athletes is not always clear In addition accuracy of reporting varies more for athletes than for others In the general population patients typically report concussion accurately or overstate symptoms However athletes (or their coaches teammates or families) tend to underreport concussion symptoms Sometimes concussion symptoms are downplayed so that the injured athlete may return to the game quickly In other cases the athlete is not aware of being concussed because signs and symptoms can be delayed for up to several days
Clinical Presentation The signs and symptoms of concussion often begin immediately after or within minutes of the injury These may worsen over minutes and even hours In some cases symptoms may not appear until the affected person undergoes significant physical or mental exertion See Table 1 for common signs and symptoms of concussion
Table 1 Common Signs and Symptoms of ConclIssion Signs Amnesia regarding events prior to or after injury -
Behavior or personal it) change Confabulation Delayed verbal and motor responses Disequilibrium Disorientation Emotiona l labi lity Loss of consciollsness Slurredincoherent speech
r-Symptoms
Vacant stare Blurryv isiondouble vision Confusion
1-shyDizziness
Txcessive drowsiness sleee difficulty Feelin haz Jsgtgg~ r~ggy Headache Inability to focus concentrate Nallsea andor vomiting Not feeling right Photophobiaphonophobia
Adapted from Kutcher JS Giza CC Alessi AG Sports concussion Continuum Lifelong Learning Neurol 201016(6) 45 Copyright copy 2010 American Academy of Neurology All rights reserved
Acute Assessment and Managemen When a concussion is suspected the injured athletes safety is of paramount concern The athlete should be removed from play and assessed carefully for airway breathing and circulation problems (the concussion ABCs) The possibility for cervical spine injury and the need for emergency medical intervention also should be determined These steps are recommended regardless of whether the athlete is able to walk on his or her own The person should not return to play until evaluated by a clinician or other certified medical professional experienced in concussion management
If a concussion is diagnosed the athlete should be removed from participation for the rest of the day It is essential to document the time and cause of the injury and any presenting signs and symptoms The athlete should be monitored for the next three to four hours for signs the condition is worsening He or she should be advised not to return to play until having been reeva luated over a period of days
After diagnosis symptom management becomes the focus The injured athlete should be directed to manage physica l and mental exertion carefully and to avoid exacerbating activities Pain medications such as acetaminophen can be taken immediately after the injury later when hemorrhage has mostly been ruled out antiinflammatory medications (eg ibuprofen) may be introduced The clinician should identify and treat any alternative or aggravating diagnoses including migraine medication overuse and rebound headache In addition the
-----
clinician should advise general supportive ca re such as maintaining oral intake and sleep ing liberally Psychological counse ling with the aim of cognit ive restructuring also is encouraged This may invo lve educating the athlete and famil y about the nature of the injury It also may include reassuring them about both the prognosis and one of the few interventions proven to reduce the likelihood of developing chronic post-concussion syndrome
Return-to-Play Decision Making Before returning the athlete to participation it is essential that the clinician be reasonably certain that the physiologic effects of the injury have subs ided Any preinju ry objective data if available shou ld be examined Several tools are available as aids In addition to a comprehensive neurologic history and examination assessment tool s to consider include the Sport Concussion Assessment Too l 2 Balance Error Scoring System standardized symptom checklists reaction time testing and neuropsychological testing Regardless of the too ls used it is important to remember that no tool be used as the sole determinant in decision making Rather tools optimally should be used in the context of a comprehensive concussion management program
The clinician should ensure the following before returning the ath lete to play
bull Performance on objective testing is normal
bull Symptoms are absent even wi thout medication use
bull Examination is normal patient is asymptomatic at rest and on exertion
The return to physica l activity should occur in a gradual well-defined manner w ith activity levels escalated in a stepwise fashion The final level should mimic game conditions as much as possible w ithout ri sk of further head injury It also is suggested that return-to-play guidelines be more conservati ve in younger athletes w ith concussion
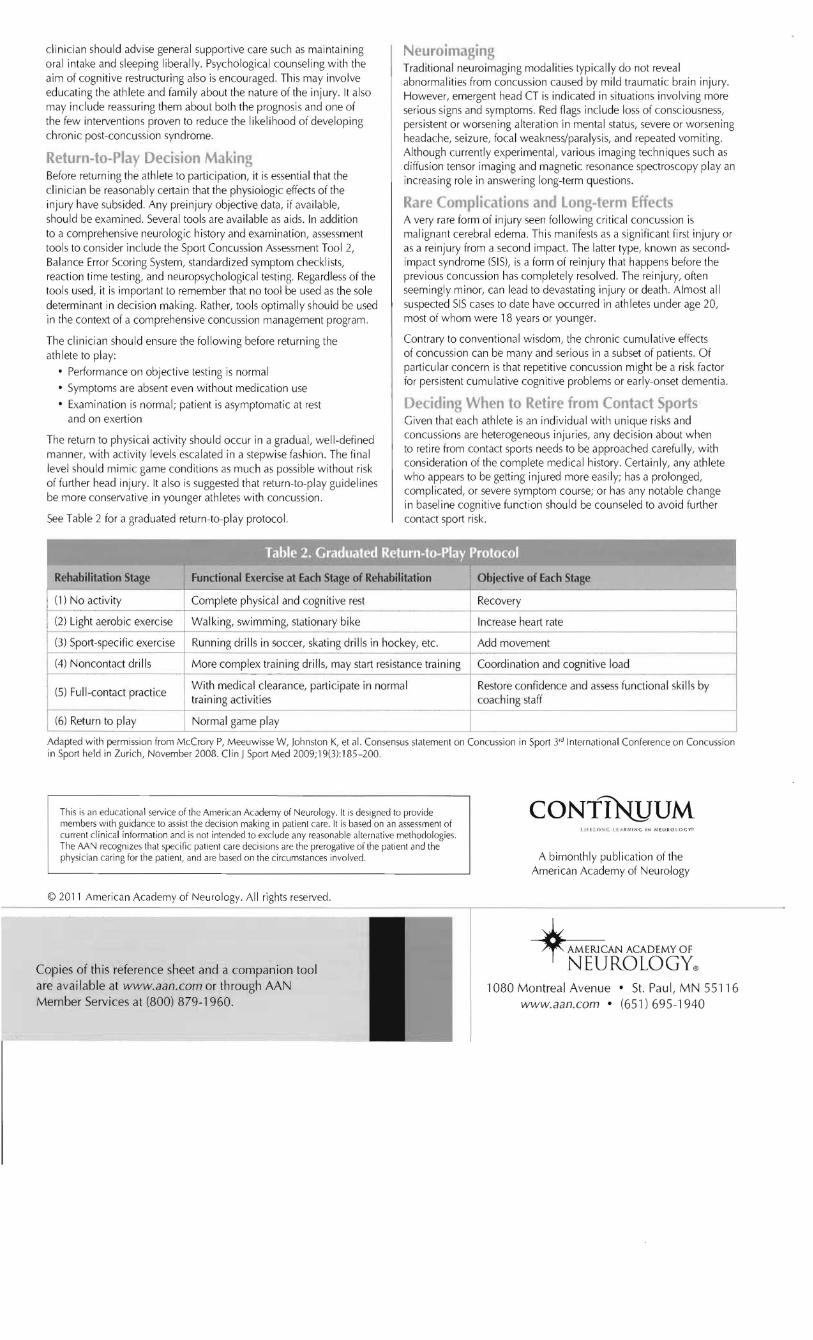
See Table 2 for a graduated return-to-play protocol
Neuroimaging Traditional neuroimaging modalities typica lly do not reveal abnormalities from concussion caused by mild traumatic brain injury However emergent head CT is indica ted in situat ions involving more serious signs and symptoms Red flags include loss of consc iousness persistent or worsening alteration in mental status severe or worsening headache seizure focal weaknessparalysis and repeated vomiting Although currently experimental various imaging techniques such as diffusion tensor imaging and magnetic resonance spectroscopy play an increasing role in answering long-term quest ions
Rare Complications and long-term Effects A very rare form of injury seen following critical concu ss ion is malignant cerebral edema This manifests as a significant first injury or as a reinjury from a second impact The latter type known as secondshyimpact syndrome (SIS) is a form of reinjury that happens before the previous concussion has completely resolved The reinjury often seemingly minor can lead to devastating injury or death Almost all suspected SIS cases to date have occurred in athletes under age 20 most of whom were 18 years or younger
Contrary to conventional wisdom the chronic cumu lative effects of concussion can be many and serious in a subset of patients Of part icular concern is that repetitive concussion might be a ri sk factor for persistent cumulative cognitive problems or early-onset dementia
Deciding When to Retire from Contact Sports Given that each athlete is an indiv idual w ith unique ri sks and concussions are heterogeneous injuries any decision about when to ret ire from contact sports needs to be approached ca refully with consideration of the complete medical history Certainl y any athlete who appears to be getting injured more easil y has a prolonged complicated or severe symptom course or has any notable change in basel ine cognitive function should be counseled to avoid further contact sport risk
- -bull f bull - ----~
Rehabilitation Stage Functional Exercise at Each Stage of Rehabilitation Objective of Each Stage
(I) No activity Complete physical and cognitive rest Recovery
(2) Light aerobic exercise Walking swimming stationary bike Increase heart rate ~------------------+------------ ------------------------+----------------------------------------i
(3) Sport-spec ific exercise Running drills in soccer skating drills in hockey etc Add movement ~------------------+-----~---
(4) Noncontact drills More complex training drills may start resistance training Coordination and cognitive load r-------------------+--shy
With medical clearance parti cipate in normal Restore confidence and assess functional ski ll s by (5) Fu II-contact practice
training activities coaching staff
(6) Return to play Normal game play
Adapted w ith permission from McCrory P Meeuw isse W Johnston K et al Consensus statement on Concussion in Sport 3 InternJti onal Conference on Concussion in Sport held in Zurich November 2008 Clin J Sport Med 200919(3) 185-200
This is an educational seNice of the American Academy of Neurology It is designed to provide members with gu idance to assist the decision making in patient care It is based on an assessment of current clin ical information and is not intended to exclude any reasonable altern ative methodologies The AAN recognizes that specific patient care decisions are the prerogative of the patient and the physician ca ring for the patient and are based on the circumstances involved
CONT1NJJUM t ll f (~I r I r R ~IN G I N NElJRO lQ c yG
A bimonthly publi cat ion of the American Academy of Neurology
copy 2011 American Academy of Neurology All rights rese rved ----- ----------------------------------------shy
Copies of this reference sheet and a companion tool are available at wwwaancom or through AAN Member Services at (800) 879-1960
~CANACADEMYOf NEUROLOGYreg
1080 Montreal Avenue bull St Paul MN 55116 wwwaancom bull (651)695-1940
-----
clinician should advise general supportive ca re such as maintaining oral intake and sleep ing liberally Psychological counse ling with the aim of cognit ive restructuring also is encouraged This may invo lve educating the athlete and famil y about the nature of the injury It also may include reassuring them about both the prognosis and one of the few interventions proven to reduce the likelihood of developing chronic post-concussion syndrome
Return-to-Play Decision Making Before returning the athlete to participation it is essential that the clinician be reasonably certain that the physiologic effects of the injury have subs ided Any preinju ry objective data if available shou ld be examined Several tools are available as aids In addition to a comprehensive neurologic history and examination assessment tool s to consider include the Sport Concussion Assessment Too l 2 Balance Error Scoring System standardized symptom checklists reaction time testing and neuropsychological testing Regardless of the too ls used it is important to remember that no tool be used as the sole determinant in decision making Rather tools optimally should be used in the context of a comprehensive concussion management program
The clinician should ensure the following before returning the ath lete to play
bull Performance on objective testing is normal
bull Symptoms are absent even wi thout medication use
bull Examination is normal patient is asymptomatic at rest and on exertion
The return to physica l activity should occur in a gradual well-defined manner w ith activity levels escalated in a stepwise fashion The final level should mimic game conditions as much as possible w ithout ri sk of further head injury It also is suggested that return-to-play guidelines be more conservati ve in younger athletes w ith concussion
See Table 2 for a graduated return-to-play protocol
Neuroimaging Traditional neuroimaging modalities typica lly do not reveal abnormalities from concussion caused by mild traumatic brain injury However emergent head CT is indica ted in situat ions involving more serious signs and symptoms Red flags include loss of consc iousness persistent or worsening alteration in mental status severe or worsening headache seizure focal weaknessparalysis and repeated vomiting Although currently experimental various imaging techniques such as diffusion tensor imaging and magnetic resonance spectroscopy play an increasing role in answering long-term quest ions
Rare Complications and long-term Effects A very rare form of injury seen following critical concu ss ion is malignant cerebral edema This manifests as a significant first injury or as a reinjury from a second impact The latter type known as secondshyimpact syndrome (SIS) is a form of reinjury that happens before the previous concussion has completely resolved The reinjury often seemingly minor can lead to devastating injury or death Almost all suspected SIS cases to date have occurred in athletes under age 20 most of whom were 18 years or younger
Contrary to conventional wisdom the chronic cumu lative effects of concussion can be many and serious in a subset of patients Of part icular concern is that repetitive concussion might be a ri sk factor for persistent cumulative cognitive problems or early-onset dementia
Deciding When to Retire from Contact Sports Given that each athlete is an indiv idual w ith unique ri sks and concussions are heterogeneous injuries any decision about when to ret ire from contact sports needs to be approached ca refully with consideration of the complete medical history Certainl y any athlete who appears to be getting injured more easil y has a prolonged complicated or severe symptom course or has any notable change in basel ine cognitive function should be counseled to avoid further contact sport risk
- -bull f bull - ----~
Rehabilitation Stage Functional Exercise at Each Stage of Rehabilitation Objective of Each Stage
(I) No activity Complete physical and cognitive rest Recovery
(2) Light aerobic exercise Walking swimming stationary bike Increase heart rate ~------------------+------------ ------------------------+----------------------------------------i
(3) Sport-spec ific exercise Running drills in soccer skating drills in hockey etc Add movement ~------------------+-----~---
(4) Noncontact drills More complex training drills may start resistance training Coordination and cognitive load r-------------------+--shy
With medical clearance parti cipate in normal Restore confidence and assess functional ski ll s by (5) Fu II-contact practice
training activities coaching staff
(6) Return to play Normal game play
Adapted w ith permission from McCrory P Meeuw isse W Johnston K et al Consensus statement on Concussion in Sport 3 InternJti onal Conference on Concussion in Sport held in Zurich November 2008 Clin J Sport Med 200919(3) 185-200
This is an educational seNice of the American Academy of Neurology It is designed to provide members with gu idance to assist the decision making in patient care It is based on an assessment of current clin ical information and is not intended to exclude any reasonable altern ative methodologies The AAN recognizes that specific patient care decisions are the prerogative of the patient and the physician ca ring for the patient and are based on the circumstances involved
CONT1NJJUM t ll f (~I r I r R ~IN G I N NElJRO lQ c yG
A bimonthly publi cat ion of the American Academy of Neurology
copy 2011 American Academy of Neurology All rights rese rved ----- ----------------------------------------shy
Copies of this reference sheet and a companion tool are available at wwwaancom or through AAN Member Services at (800) 879-1960
~CANACADEMYOf NEUROLOGYreg
1080 Montreal Avenue bull St Paul MN 55116 wwwaancom bull (651)695-1940