abstract of thesis entitled - hku nursing · abstract of thesis entitled “an evidence-based...
TRANSCRIPT

i
Abstract of thesis entitled
“An evidence-based protocol of home-based intervention to reduce readmission rate in
heart failure patients”
Submitted by
Cheung Shuk Man
for the degree of Master of Nursing
at The University of Hong Kong
In July 2016
Heart failure (HF) is a major chronic disease in the society. It brings great burden to the
healthcare system and also to the individuals. During hospitalization, HF patients receive care
from different parties. However, when they are discharged, monitoring is discontinued.
Adherence to treatment regimen is not guaranteed. Due to poor compliance to the treatment
regimen, HF patients are readmitted to hospitals. A home-based intervention is therefore
proposed to be an innovation to promote the continuity of care from hospital to home in order
to reduce the hospital readmission rate.
A systematic literature review about home-based intervention for HF patients was done.
8 randomised controlled trials (RCTs) were selected and critically appraised. Evidence had
shown that home-based intervention carried out by nurses would have a positive effect on the
reduction in the hospital readmission rate, the improvement of patients’ quality of life (QoL)
and the reduction in healthcare cost when compared with usual care.
An evidence-based protocol based on the best available evidence with quality
recommendations was established. A communication plan, a pilot study and a cost-benefit ratio
were made to assess the transferability, feasibility and implementation potential of the home-

ii
based intervention. An evaluation plan was also developed to evaluate the effectiveness of the
intervention.
With the inclusion of the home-based intervention the current management of HF
patients, it is expected that there will be favorable impacts on both the healthcare system and
individuals.

iii
An evidence-based protocol of home-based intervention to reduce readmission rate in
heart failure patients
By
Cheung Shuk Man
BNurs (HKU)
A dissertation submitted in partial fulfilment of the requirements for
the degree of Master of Nursing
at the University of Hong Kong
July 2016
iv
Declaration
I declare that this dissertation represents my own words, except where due acknowledgement
is made, and that it has not been previously included in a thesis, dissertation or report submitted
to this University or to any other institution for a degree, diploma or other qualifications.
Signed: ____________________________
Cheung Shuk Man

v
Acknowledgements
I would like to take this opportunity to express my gratitude to my supervisor, Ms.
Rebecca Poon, for her insightful supervision and guidance in this dissertation. Ms. Poon also
gave me encouragement throughout the study of the master program.
I would also like to express my sincere appreciation to the lecturers for their education
in the master program.
Last but not least, I would like to thank my dearest family members and friends who
always take care of me and support me throughout the study of the master program.

vi
Table of contents
Abstract………………………………………………………………………………………ⅰ
Declaration…………….……………………………………………………………………..ⅳ
Acknowledgements…………………………………………………………………………..ⅴ
Table of contents……………………………………………………………………………..ⅵ
List of Appendices……………………………………………………………………………ⅷ
Abbreviation……………………………………………………..………………....………..ⅸ
Chapter 1: Introduction
1.1 Background………………………………………………….…………………………….1
1.2 Significance ……………………………………………………………………………….2
1.3 Affirming need…………………………………………………………………………….3
1.4 Research question………………………………………………………………………….6
1.5 Objectives………………………………………………………………………………….6
Chapter 2: Critical appraisal
2.1 Search and appraisal strategies…………………………………………………………….8
2.2 Results……………………………………………………………………………………10
2.3 Summary and synthesis…………………………………………………………………..16
2.4 Conclusion………………………………………………………………………………..19
Chapter 3: Implementation Potential
3.1 Target setting……………………………………………………………………………..21
3.2 Target participants………………………………………………………………………..21

vii
3.3 Transferability……………………………………………………………………………21
3.4 Feasibility………………………………………………………………………………...23
3.5 Cost and Benefit ratio…………………………………………………………………….26
3.6 Evidence-based Practice Guideline………………………………………………………28
Chapter 4: Implementation Plan
4.1 Communication Plan……………………………………………………………………..30
4.2 Pilot study ………………………………………………………………………………..32
4.3 Evaluation Plan…………………………………………………………………………..33
4.4 Basis for implementation………………………………………………………………...37
4.5 Conclusion……………………………………………………………………………….38
References…………………………………………………………………………………...39
Appendices…………………………………………………………………………………..44

viii
List of Appendices
Appendix 1 Heart failure classification………………………………………………………44
Appendix 2 PRISMA 2009 Flow Diagram…………………………………………………..45
Appendix 3 Flowchart………………………………………………………………………..46
Appendix 4 Table of evidence……………………………………………………………….47
Appendix 5 Level of evidence……………………………………………………………….61
Appendix 6 Critical appraisal SIGN checklist…………………………………………....….62
Appendix 7 Potential cost………………………………………………………….………...78
Appendix 8 Grades of recommendations………………………………………………….....79
Appendix 9 Evidence-based practice guideline…………………………………….………..80
Appendix 10 Timeline of the pilot study…………………………………………………….85
Appendix 11 Questionnaire for healthcare providers for assessing the satisfaction level about
the home-based intervention…………………………………………………..86
Appendix 12 Audit form- Home-based intervention for heart failure patients……….……...87
Appendix 13 Questionnaire for patients for assessing the satisfaction level about the home-
based intervention……………………………………………………………..88
Appendix 14 Minnesota Living with Heart Failure (MLHF) questionnaire…………….…...89
Appendix 15 Interview questions for assessing patients’ knowledge………………….…….90

ix
Abbreviations
ACC American College of Cardiology
ACEI Angiotensin Converting Enzyme inhibitors
AED Accident and Emergency Department
AHA American Heart Association
APN Advanced practiced nurse
ARBs Angiotensin 2 Receptor Blockers
CABG Coronary artery bypass graft surgery
CAD Coronary artery disease
COS Chief of Service
CVD Cardiovascular disease
DOM Department Operation Manager
EHFScBs European Heart Failure Self Care Behaviour Scale
HA Hospital Authority
HCPs Healthcare providers
HF Heart failure
ICD Implantable Cardioverter Defibrillator
LVEF Left ventricular ejection fraction
MLHF Minnesota Living with Heart Failure
NYHA New York Heart Association
PND Paroxysmal nocturnal dyspnea
QoL Quality of life
RCTs Randomised controlled trials
SIGN Scottish Intercollegiate Guidelines Network
1
Chapter 1
Introduction
1.1 Background
1.1.1 Definition, causes and classification of heart failure
Heart failure (HF) is a chronic disease and is the common final stage of many heart
diseases (Bui, Horwich & Fonarow, 2011). Ventricular dysfunction, degenerative valve disease
and idiopathic dilated cardiomyopathy are some common heart diseases that lead to HF
(McMurray & Pfeffer, 2005). According to International Classification of Disease- 10th Edition
(2016), HF is characterized as the inability of the heart to pump an adequate amount of blood
to meet the metabolic requirements of different organ systems and/or to do so only at an
increased filling pressure.
According to American Heart Association (2015), the most common cause of HF is
coronary artery disease (CAD). It accounts for 60-75% of HF in developed countries (Nasif &
Alahmad, 2015). CAD is caused by the narrowing of arteries due to the buildup of fatty deposits
called plaque, which affects the supply of blood to the heart (American Heart Association,
2015). Hypertension is another leading cause of HF because of its high prevalence (Mosterd &
Hoes, 2007 as cited in Heidenreich et al., 2013). Besides, diabetes mellitus increases the risk
of HF by around 2 times in men and up to 5 times in women (Ingelsson, Sundstrom, Arnlov,
Zethelius & Lind, 2005; Kannel, 2000 as cited in Heidenreich et al., 2013). Moreover, smoking
solely leads to an increased risk of developing HF by 47% (Hoffman, Pasty & Kronmal, 1994
as cited in Bui et al., 2011). In addition, obesity with BMI >/= 30kg/m2 doubles the risk of HF
(Bibbins-Domingo et al., 2009; Chen et al., 1999; Kenchaiah et al., 2002 as cited in Bui et al.,
2011).
There are two systems for classifying different stages of HF (Nasif & Alahmad, 2015),
namely the New York Heart Association (NYHA) classification and American College of

2
Cardiology/ American Heart Association (ACC/AHA) Stages. NYHA classification focuses
on patients’ functional capacity whereas ACC/AHA Stages concentrate on the progressive
nature of HF. Their outlines are shown in Appendix 1.
1.1.2 Epidemiology of HF
In the world, there are more than 20 million people affected by HF (Nasif & Alahmad,
2015).
In Hong Kong, a retrospective study was conducted in 1997 to analyze the epidemiology
of HF in 11 emergency departments of hospitals under the Hospital Authority (HA) (Hung,
Cheung, Ip & Fung, 2000). This study showed that the prevalence of HF for patients aged 55-
64 and 65-74 were 1.3 and 4.4 per 1000 men, respectively, and 0.9 and 3.9 per 1000 women,
respectively. In addition, the annual incidence rate was 0.7 per 1000 persons, which increased
with age. Besides, it revealed that the overall mortality rate was 32%, which also increased
with age. A recent data from the Centre for Health Protection (2015) showed that heart disease
was the third most common cause of death in Hong Kong in 2013. It accounted for 13.4% of
all the deaths in 2013. There were 74534 in-patient discharges and deaths because of heart
disease in all public and private hospitals in 2013. Among the cases, about 25% (18590 cases)
was due to HF.
With the aging population in Hong Kong and the fact that incidence and mortality rates
of HF increase with age, more people are at the risk of developing and suffering from HF.
1.2 Significance
1.2.1 Impacts - to patients
In the early stage of HF, shortness of breath with exertion is a common symptom. As the
disease progresses, dyspnea emerges when patients are at rest. Later on, difficulty in breathing
is associated with the recumbent position, which is called orthopnea. Patients may also develop
paroxysmal nocturnal dyspnea (PND), which refers to the sudden onset of severe shortness of

3
breath at night. PND will awaken patients from their sleep (Nasif & Alahmad, 2015). Moreover,
peripheral edema, weight gain and confusion can also happen in HF patients (American Heart
Association, 2015).
In addition, HF increases patients’ mortality rate (Centre for Health Protection, 2015) and
hospital readmission rate (Aguado et al., 2010).
1.2.2 Impacts - to the health care system
HF places a heavy and growing burden on the health care system.
Hospitalization
In Hong Kong, there were 4589 new cases and 1614 old cases of HF that required
hospitalization in 1997 (Hung et al., 2000). There was a 10% annual increase in hospital
admissions due to HF from 1998 to 2003 (Sanderson, 2004). In 2015, the admission record of
an acute medical ward in a public hospital revealed that the monthly admission rate of HF cases
was about 5%.
Cost
Handling HF cases incurs 1-2% of the total health care expenditure in developed countries
(Bui et al., 2011). This includes the cost of health care services, medications and cost of taking
sick leave.
1.3 Affirming need
1.3.1 Current management
In local public hospital medical units, the current management of HF is mainly by
pharmacological therapy. The usual first line drugs for treating patients with HF are
Angiotensin Converting Enzyme inhibitors (ACEI), Angiotensin 2 Receptor Blockers (ARBs),
beta blockers, aldosterone antagonists and diuretics (Nasif & Alahmad, 2015).
Invasive procedures, such as the implantation of Implantable Cardioverter Defibrillator
(ICD), are used in patients who remain symptomatic, despite an optimal medical therapy.
4
Besides medication, dietary and lifestyle changes are essential and recommended to all
patients with HF. Such changes include smoking cessation, dietary restriction on sodium,
abstinence from alcohol consumption, daily weight monitoring and routine modest aerobic
exercise.
1.3.2 Deficiency
In Hong Kong, when patients are hospitalized due to HF, pharmacological therapy is
usually the initial treatment for the disease. In addition to medications prescribed by medical
officers, the amount of fluid is restricted in HF patients so as to reduce the workload of the
heart. Their body weight is measured regularly (e.g. on daily basis or on alternate days) to
monitor the amount of fluid that build ups in the body. Dietitian is also referred for adjusting
patients’ diet and amount of sodium intake. All of the data are closely monitored by nurses
with appropriate chartings because they are responsible for offering round-the-clock care to
patients and most familiar with patients’ conditions.
However, when HF patients are discharged, monitoring by nurses is discontinued at home.
They only receive outpatient follow-up by cardiologists or general practitioners, which is
already one or several months after their discharge. Without any professional supervision at
home, it is not guaranteed that the HF patients will follow the recommendations taught in
hospitals appropriately. Poor compliance with treatment is the primary cause of hospital
readmission (Aguado et al., 2010). It is estimated that up to 50% of the readmissions were
potentially avoidable (Aguado et al., 2010).
According to a presentation in HA Convention (2012), a program called ‘Heart to Heart
Program’ was conducted in 2011-2012 by the North District Hospital in Hong Kong. This
program aimed at providing continuous care for HF patients in the community by adopting a
multidisciplinary approach of home visits, telephone contacts and making referrals by nurses
to various disciplines like physiotherapists, dietitians and occupational therapists. This

5
program showed positive outcomes on shortening the length of hospitalization and reduction
in the number of hospital readmissions.
Despite the positive outcomes of the ‘Heart to Heart Program’, the cost of the program
was huge as the involvement of different parties would be needed. Nurses are probably the
most suitable persons to take care of patients and can be a health educator to provide health
education on diet and exercise. Most importantly, there is a lack of an established evidence-
based protocol for monitoring patients’ conditions and providing care for patients after they
are discharged from hospitals.
Owing to deficiency in the continuity of care for HF patients after they are discharged,
there is an affirming need to develop an evidence-based protocol to ensure standardization so
that the home-based intervention can also be implemented.
1.3.3 Intervention- Home-based intervention
Home-based intervention for HF patients consists of home visits and telephone follow-
ups conducted by nurses. Patients only stay in their most familiar environment, i.e. their home
(Tsuchihashi-Makaya et al., 2013).
During home visits, patients and nurses meet directly. This face-to-face interaction
helps to build a ‘therapeutic alliance’ between them (Tsuchihashi-Makaya et al., 2013). On one
hand, nurses can have a better understanding of the difficulties patients may face at home when
carrying out any health-related behavior (Riegel et al., 2009 as cited in de Souza et al., 2014).
They can also identify the precipitating factors in patients’ own environment that are likely to
result in the deterioration of patients’ health (Stewart, Marley & Horowitz, 1999). On the other
hand, patients can develop a better insight of the importance of their therapy and how they can
achieve the therapeutic goals in an easier way (de Souza et al., 2014).
6
Telephone follow-ups can promote the continuity of the treatment regimen because
nurses can continue to monitor patients’ health conditions and patients can raise their questions
about the therapeutic treatment.
With this home-based intervention, HF patients are more likely to acquire better
knowledge of their own disease and to adhere to the recommended treatment regimen. Hospital
readmissions could also be reduced (Morcillo et al., 2009; Tsuchihashi-Makaya et al., 2013;
Sisk et al., 2006; Stewart et al., 1999; Stewart, Vandenbroek, Pearson & Horwitz, 1999).
However, there is no systematic review for home-based intervention for HF patients.
In view of such inadequacy, a systematic review is therefore needed for the development of an
evidence-based protocol about home-based intervention for HF patients. With the protocol,
nurses will be able to continue monitoring and providing care for patients after they are
discharged from hospitals.
1.4 Research question
How effective is home-based intervention in reducing the readmission rate of adult HF
patients?
1.5 Objectives
1. To critically appraise the selected literature and extract related data.
2. To investigate the effectiveness of home-based intervention in reducing the
readmission rate of HF patients.
3. To develop an evidence-based protocol for the implementation of home-based
intervention.
4. To assess the implementation potential of home-based intervention for HF patients
when they are discharged from hospitals in acute medical settings in Hong Kong.
7
5. To establish an implementation plan to evaluate the effectiveness of home-based
intervention after its implementation.

8
Chapter 2
Critical appraisal
2.1 Search and appraisal strategies
2.1.1 Inclusion and Exclusion criteria
The literature should include the study of adult patients aged 18 or above and they are
admitted to hospitals because of HF. The studies should be randomized controlled trials (RCTs)
and compare home-based intervention with usual care that patients would receive outpatient
follow-up from cardiologists or general practitioners but no extra follow-up (neither home
visits nor telephone follow-up) by nurses. Readmission rate should be the primary or secondary
outcome in the studies.
Studies targeting at pediatric patients were excluded. Qualitative studies, unpublished
studies and non-empirical research papers like news and letters were also excluded. Further
exclusion was made if the study interventions focused on multidisciplinary intervention or
specialized nurse clinics.
2.1.2 Search strategies
Three electronic databases were used to conduct a systematic search for identifying
relevant literature. The databases were PubMed, CINAHL Plus (EBSCohost) and Cochrane
Library. The keywords used included “heart failure”, “home-based intervention”, “home-based
education”, “home-based counseling”, “home-based caring”, “nurse-led”, “readmission rate”,
“resource use”, “hospitalization”, “hospital utilization”, “hospital use” and “hospital
readmission”. No time and language restrictions were applied to the systematic search. Manual
search by screening the reference lists of eligible literature was done for additional relevant
literature. Details of the search history and results are shown in PRISMA (Appendix 2) and in
a flowchart (Appendix 3).

9
2.1.3 Data extraction
Data was extracted from all the selected literature and organized in tables of evidence.
Every table of evidence included design, study quality, sample characteristics, intervention,
control, length of follow up, outcomes and effect size. Details of the tables of evidence are
shown in Appendix 4.
2.1.4 Appraisal strategies
The methodology checklist for RCTs by Scottish Intercollegiate Guidelines Network
(SIGN, 2015) was used for the critical appraisal of the selected literature. The checklist has
two sessions. The first session is used for addressing issues related to internal validity of the
study. The second session is used for making an overall assessment of the study. The quality
of the study is reflected by a set of symbol. “++” indicates that the study is of high quality with
little or no risk of bias; “+” means that the study is of acceptable quality with some flaws and
risks of bias; “-” suggests that the study is of low quality with significant flaws related to key
aspects of the study design; and “0” expresses that the study is unacceptable and it has to be
rejected.
The level of evidence in each piece of literature was determined according to the SIGN
(SIGN, 2008) (Appendix 5). According to SIGN (2008), RCTs, meta-analyses, and systematic
review of RCTs belong to level 1. As all the selected literature in the present review is RCTs,
it belongs to level 1.
Details of the critical appraisal of the selected literature are shown in Appendix 6.

10
2.2 Results
2.2.1 Search results
As shown in the PRISMA (Appendix 2), a systematic search was conducted from 15th
September 2015 to 26th September 2015 and a total of 239 articles were retrieved from PubMed,
CINAL Plus (EBSCohost) and Cochrane Library, and 6 additional articles were located
manually among the reference lists of the eligible articles. After the removal of duplicated
articles, 132 articles remained. By reviewing the titles and abstracts of the 132 articles, 37 of
them remained. After examing the full text of the remaining 37 potential articles, 9 were
selected. However, 2 articles came from the same study that the lengths of outcome measure
were different- 6 months and 18 months respectively. The one with 6 months as its length of
outcome measure was not recruited because it was only an intermittent study (Stewart, Pearson
& Horwitz, 1998), but it was still used as reference in order to provide more information when
analyzing the quality of the other article. Therefore, 8 full-text articles were finally selected for
this review.
2.2.2 Summary of data (Table of evidence)
Study type
The 8 articles were all RCTs. They were published between 1998 and 2014 (Brotos et
al., 2009; de Souza et al., 2014; Krumholz et al., 2002; Morcillo et al., 2005; Sisk et al., 2006;
Stewart et al., 1999; Stewart et al., 1999; Tsuchihashi-Makaya et al., 2013).
Patient characteristics
The sample size of the selected studies ranged from 70 (Brotos et al., 2009) to 406
(Krumholz et al., 2002). The mean age of the participants was between 59.4 years old (Sisk et
al., 2006) and 77.7 years old (Brotos et al., 2009). The participants were all diagnosed with HF
with different NYHA classes and were recruited in hospitals before they were discharged. The

11
mean ejection fraction of the participants was between 29.6% (de Souza et al., 2014) and 47.4%
(Tsuchihashi-Makaya et al., 2013). One study did not state the ejection fraction of the
participants (Sisk et al., 2006). And one study stated that the ejection fraction of its participants
ranged from <30% to >50% (Brotons et al., 2009).
Intervention
All the studies included nurse-initiated home visits combined with telephone follow-
ups as intervention after the patients were discharged from hospitals except one study (Morcillo
et al., 2009), in which only home visits were conducted.
The intervention in the selected studies had different components.
In one study (Brotons et al., 2009), HF patients were given a booklet with information
about the disease, and its pharmacological and non-pharmacological treatments before they
were discharged. Another study declared that patients were visited by nurses and counseled
about the treatment regimen before they were discharged (Stewart et al., 1999).
For the home visits, in five studies, nurses assessed patients’ health status, adherence
to the medication and lifestyle habits (Brotons et al., 2009; de Souza et al., 2014; Morcillo et
al., 2009; Stewart et al., 1999; Tsuchihashi-Makaya et al., 2013). In two studies, education
about the disease and its symptoms was given by nurses (Brotons et al., 2009; Sisk et al, 2006).
In two studies, nurses performed physical examinations of patients (Morcillo et al., 2009;
Stewart et al., 1999). In three studies, caregivers or family members were involved by receiving
counseling and instructions given by nurses (Brotons et al., 2009; Morcillo et al., 2009; Stewart
et al., 1999). In one study, nurses used a teaching booklet based on the five sequential care
domains for chronic illnesses to provide care during home visit (Krumholz et al., 2002). One

12
study included a pharmacist during home visits (Stewart et al., 1999). The pharmacist assessed
patients’ knowledge of medication while the nurse detected patients’ clinical status.
Single home visits were conducted in four studies (Krumholz et al., 2002; Morcillo et
al., 2009; Sisk et al., 2006; Stewart et al., 1999). The time of initial visits lied between 1 week
(Stewart et al., 1999) and 1 month after patients’ discharge (Brotons et al., 2009). Three studies
stated the duration of a home visit, which ranged from around 60 minutes (de Souza et al.,
2014) to 2 hours (Morcillo et al., 2009; Stewart et al., 1999).
Four studies included telephone follow-ups in the interventions for monitoring patients’
disease progress and the symptoms of their disease (Brotons et al., 2009; Sisk et al., 2006;
Stewart et al., 1999; Tsuchihashi-Makaya et al., 2013). In four studies, telephone follow-ups
were used for reinforcing the recommended lifestyle changes, exercise and prescribed
medications (de Souza et al., 2014; Krumholz et al., 2002; Sisk et al., 2006; Stewart et al.,
1999). Only one study stated the duration of the telephone follow-up, which was around 10
minutes each time (de Souza et al., 2014).
In six studies, nurses would consult primary physicians or cardiologists in case the
patients showed deterioration in their health status or when there was a need for modifying the
current treatment (Brotos et al., 2009; de Souza et al., 2014; Sisk et al., 2006; Stewart et al.,
1999; Stewart et al., 1999; Tsuchihashi-Makaya et al., 2013).
Control group
All the selected studies had control groups for making comparison. The control groups
were under usual care with the standard routine follow-up by cardiologists or physical
practitioners. They did not receive any home visits or telephone follow-ups conducted by
nurses.

13
Length of follow-ups
The length of follow-ups of the studies ranged from 6 months (de Souza et al., 2014;
Morcillo et al., 2005; Stewart et al., 1999) to 18 months (Stewart et al., 1999). In one study, it
also measured the quality of life (QoL) of the participants in the 2nd, 6th and 12th months
respectively (Tsuchihashi-Makaya et al., 2013).
Outcome measures
All the selected studies included hospitalization and/or all cause deaths as their outcome
measures. Four studies measured the health care cost as one of the outcomes (Krumholz et al.,
2002; Morcillo et al., 2009; Stewart et al., 1999; Stewart et al., 1999). The number of days of
hospitalization was measured in three studies (Krumholz et al., 2002; Stewart et al., 1999;
Stewart et al., 1999). Three studies counted the attendances to hospital emergency departments
(de Souza et al., 2014; Sisk et al., 2006; Stewart et al., 1999). QoL was compared in three
studies (Brotons et al., 2009; Stewart et al., 1999; Tsuchihashi-Makaya et al., 2013). de Souza
et al. (2014) also measured the level of HF knowledge and self-care. Brotons et al. (2009)
assessed patients’ adherence to therapy and satisfaction of the information they had received.
In addition, Morcillo et al. (2009) measured patients’ perception of health.
2.2.3 Summary of appraisal results
All the selected articles addressed an appropriate and clearly focused question with all
the elements in PICO presented in the text. These articles clearly stated how home-based
intervention could reduce readmission and mortality rate, and improve health outcomes.
For the randomization method, four studies used computer programs to generate the
allocation list (Brotos et al., 2009; de Souza et al., 2014; Sisk et al., 2006; Stewart et al., 1999).
Morcillo et al. (2005) used a random number table for randomization. One study initiated

14
randomization through telephone calls (Stewart et al., 1999). In two studies, randomization was
mentioned but the method was not specified (Krumholz et al., 2002; Tsuchihashi-Makaya et
al., 2013).
For the concealment method, computerized allocation was used in three studies (Brotos
et al., 2009; de Souza et al., 2014; Stewart et al., 1999). In one study, sealed and opaque
envelopes were used (Sisk et al., 2006). No concealment method was reported in the remaining
studies (Krumholz et al., 2002; Morcillo et al., 2005; Tsuchihashi-Makaya et al., 2013; Stewart
et al., 1999).
For the blinding method, interviewers or intervention nurses or assessors were blinded
to patients’ intervention allocation in six studies (Brotos et al., 2009; de Souza et al., 2014;
Krumholz et al., 2002; Morcillo et al., 2005; Sisk et al., 2006; Stewart et al., 1999). In two
studies, the presence of blinding was not clear (Tsuchihashi-Makaya et al., 2013; Stewart et al.,
1999).
The baseline characteristics of the treatment and control groups in all the selected
studies were similar with no significant differences.
The outcome measures were clearly stated in all the studies. Five studies used hospital’s
record system to measure inpatient and outpatient activities (de Souza et al., 2014; Krumholz
et al., 2002; Stewart et al., 1999; Stewart et al., 1999; Tsuchihashi-Makaya et al., 2013). One
study also acquired the inpatient and outpatient activities from next-of-kin (Krumholz et al.,
2002). Three studies measured the number of deaths by receiving the information from local
Birth, Deaths and Marriage Registry (Sisk et al., 2006; Stewart et al., 1999; Stewart et al., 1999).
Sisk et al. (2006) used reports from patients’ families for measuring the number of deaths. For
calculating the healthcare cost, three studies obtained data finance departments in hospitals
(Krumholz et al., 2002; Stewart et al., 1999; Stewart et al., 1999). For the measurement of

15
QoL, three studies used Minnesota living with Heart Failure (MLHF) questionnaire (Brotons
et al., 2009; Sisk et al., 2006; Stewart et al., 1999); two studies used SF-36 (Morcillo et al.,
2009; Stewart et al., 1999); and one study used SF-12 (Sisk et al., 2006). MLHF is a valid tool
in assessing the QoL related to HF (Middel et al., 2001); SF-36 is a widely used generic
measure for measuring physical and mental health (Brazier et al., 1992); SF-12 is a subset of
SF-36, which also measures physical and mental health (Brazier & Roberts, 2004).
Tsuchihashi-Makaya et al. (2013) measured depression level, anxiety level and QoL by
conducting interviews. de Souza et al. (2014) used a validated 14-item questionnaire to
measure patients’ HF knowledge and the European Heart Failure Self Care Behaviour Scale
(EHFScBS) for the measurement of patients’ self-care skills. EHFScBS is proved to be a
reliable measurement tool for measuring self-care behavior (Vellone et al., 2014). For the
measurement of adherence to the pharmacological treatment, Brotos et al. (2009) used
Morisky-Green questionnaire, which is a widely used and validated self-reported medication-
taking behavior scale (Brotos et al., 2009).
The dropout rate in the selected studies ranged from 0% (Krumholz et al., 2002; Sisk
et al., 2006; Stewart et al., 1999) to 6% (Stewart et al., 1999). The dropout rate smaller than
20% is regarded as acceptable (SIGN, 2008). Except in one study (Morcillo et al., 2005), the
dropout rate for the assessment of impact on perceived health was 27.14%. Such an
unacceptable dropout rate was due to the inability to respond by telephone, patients’ death or
patients’ refusal to answer.
Intention to treat analysis was performed in six studies (Brotos et al., 2009; de Souza et
al., 2014; Krumholz et al., 2002; Sisk et al., 2006; Stewartet et al., 1999; Stewart et al., 1999).
It was not mentioned in the other two studies (Morcillo et al., 2005; Tsuchihashi-Makaya et al.,
2013).
16
Four studies were conducted in one site only (Krumholz et al., 2002; Morcillo et al.,
2005; Stewart et al., 1999; Stewart et al., 1999). The other four studies were conducted in multi-
center but no site specific data was given (Brotos et al., 2009; de Souza et al., 2014; Sisk et al.,
2006; Tsuchihashi-Makaya et al., 2013).
In summary, four studies have high methodological (++) (Brotos et al., 2009; de Souza
et al., 2014; Sisk et al., 2006; Stewart et al., 1999). These studies have fulfilled the major
criteria in the SIGN checklist. Two studies covered most of the criteria and were rated as
acceptable (+) (Morcillo et al., 2005; Stewart et al., 1999). Their randomization methods were
not good enough and no concealment method was reported. The two studies without their
randomization method reported were rated as low quality (-) (Krumholz et al., 2002;
Tsuchihashi-Makaya et al., 2013).
2.3 Summary and Synthesis
2.3.1 Summary of the conclusions
Healthcare use
Home-based intervention showed positive effect on and statistical significance to the
reduction of hospital readmission rate when compared with the usual care group in five out of
the eight selected studies (Morcillo et al., 2009; Tsuchihashi-Makaya et al., 2013; Sisk et al.,
2006; Stewart et al., 1999; Stewart et al., 1999). Despite not showing statistical significance to
the reduction of hospital readmissions, three studies showed positive effect on lowering the
number of readmissions (Brotons et al., 2009; de Souza et al., 2014; Krumholz et al., 2002).
These three studies also revealed statistical significance to the reduction of the combined
clinical outcomes, i.e. heart-failure-related emergency department visits, hospital readmission
or death.
17
Four studies measured the attendance to emergency departments. Three of them showed
statistical significance to the reduction of the number of emergency department visits (Morcillo
et al., 2009; Sisk et al., 2006; Stewart et al., 1999). However, one of them showed insignificant
results (de Souza et al., 2014).
Two studies evaluated the days of hospitalization and both of them showed statistical
significance that home-based intervention could reduce the length of hospitalization (Stewart
et al., 1999; Stewart et al., 1999).
Home-based intervention showed inconclusive results in the reduction of the number of
deaths. Three studies showed statistical significance (Krumholz et al., 2002; Morcillo et al.,
2009; Stewart et al., 1999) while three studies showed statistical insignificance (Brotons et al.,
2009; de Souza et al., 2014; Tsuchihashi-Makaya et al., 2013).
Health-related QoL
Four studies evaluated the effect of home-based intervention on patients’ QoL. Three
of them evaluated patients’ QoL by MLHF and showed positive effect and statistical
significance that home-based intervention could improve patients’ QoL (Brotons et al., 2009;
Sisk et al., 2006; Stewart et al., 1999). One study showed that home-based intervention could
improve patients’ QoL mentally but not physically (Tsuchihashi-Makaya et al., 2013).
Healthcare cost
Four studies measured healthcare cost as one of their outcomes. Among them, three
showed that home-based intervention could significantly reduce healthcare cost (Krumholz et
al., 2002; Morcillo et al., 2009; Stewart et al., 1998). One of them showed that there was no
statistical significance in reducing healthcare cost (Stewart et al., 1999).
18
2.3.2 Synthesis of results
Evidence from the reviewed literature supports the proposed innovation to reduce the
readmission rate HF adult patients.
Home-based intervention for adult patients with HF
Seven out of the eight selected studies included both home visits and telephone follow-
ups conducted by nurses as their home-based intervention. Only one study used home visits
conducted by nurses alone as its intervention.
Target group and setting
All of the reviewed studies included adult patients who were admitted to hospital due
to HF. The participants ranged from class 1 to class 4 according to the NYHA. Therefore, the
target group of the proposed intervention is adult patients admitted to hospital with any severity
of HF. They are recruited in the local acute medical unit of a public hospital before they are
discharged.
Home visit
Single home visits were conducted in four studies, which showed both statistical
significance and positive effect in reducing hospital readmission rate. Regular home visits
were conducted in three studies but only one of them expressed both statistical significance
and positive effect on reducing the hospital readmission rate. The other two studies only
demonstrated a positive effect on lowering hospital readmissions. This implies that a single
home visit done by nurses has a beneficial effect. In most selected studies, home visits took
place between 7 to 14 days after the patient was discharged. The duration of each home visit

19
was around 1 to 2 hours, which could be more flexible as nurses can adjust it according to the
real situation they encountered during their home visit.
The contents of home visit varied between studies. The key component is an assessment
of patients’ clinical health status and their adherence to the treatment advised. Counseling and
education about the disease, symptoms and the recommended treatment regimen are given to
both patients and their family members or caregivers for improving their knowledge. A
physical examination performed by nurses can provide more information about patients’ health
status.
Telephone follow-ups
The methodology of conducting telephone follow-ups also varied between studies. On
average, telephone follow-ups were conducted at an interval of 15 days. The duration of each
telephone follow-up was so flexible that nurses could adjust the time according to the condition
of patients. The key components include an assessment of patients’ progress and the
reinforcement on the importance of adherence to treatment regimen.
Consultation
Consultation sessions were available in five of the selected studies. Nurses can contact
patients’ primary physicians or cardiologists when the patients require medical review.
2.4 Conclusion
HF is a chronic disease. Its management should be extended from hospital to patients’
homes. Evidence from the reviewed literature showed that there is a beneficial effect on HF
adult patients by implementing home-based intervention which consists of a single home visit
together and telephone follow-ups with proper consultation conducted by nurses. The hospital
20
readmission rate, emergency department attendances, the length of hospitalization and the
healthcare cost can be reduced. Moreover, patients’ QoL can also be improved. Therefore, this
intervention should be proposed in the current management of HF adult patients in the local
acute medical unit of a public hospital.

21
Chapter 3
Implementation Potential
3.1 Target setting
The proposed home-based intervention will be implemented in an acute medical ward
of a public hospital in Hong Kong. The acute medical ward admits patients from the Accident
and Emergency Department (AED) with various medical problems including HF. According
to the admission record in October 2015 of the target setting, there are around 300 all
emergency admissions every month.
3.2 Target participants
The target participants of the home-based intervention are adult patients who are
admitted to the targeted medical ward with the primary or secondary diagnosis as HF. The HF
patients are of different degrees of severity. By general observation, the mean age of the
patients is 70 years old and the mean ejection fraction of their hearts is around 30% to 45%.
According to the admission record in October 2015 of the target setting, about 5% of the
emergency admission cases are diagnosed as HF every month. That means around 15 patients
(180 patients annually) are admitted to the target setting due to HF monthly.
3.3 Transferability
3.3.1 Setting and audience
In order to assess the transferability of the innovation, a comparison of the setting and
participants between the reviewed literature and the proposed setting is made.
From the reviewed literature, the setting was acute hospitals. The participants were
recruited in hospitals before they were discharged. They were all adults with a mean age
between 59.4 years old and 77.7 years old. They were admitted to hospital due to HF with
different stages classified under the NYHA. The mean ejection fraction of their hearts was
between 29.6% and 47.4%.

22
From the above information, the setting and patients’ characteristics between the
reviewed literatures and the proposed setting were comparable. This ensures a high
transferability of the innovation into the target setting.
3.3.2 Philosophy of care
The target setting is an acute medical ward of a public hospital under HA. According
to HA (2006), its vision is to help patients to avoid the need of spending time in hospitals and
being readmitted, and to stay healthy in the community. Its mission is to empower patients to
regain their health and stay healthy by providing them with support. One of its values is to
provide the best-possible people-centred services with a caring heart by two-way
communication for understanding and meeting patients’ needs.
The objectives of the proposed intervention are identical to the vision, mission and
value of HA. The proposed intervention aims at reducing the hospital readmission rate of adult
patients with HF. The intervention provides information about the disease and stresses the
importance of adherence to the treatment regimen to the target audience. This can empower
the patients to make effort for their own health because patients themselves play a crucial role
in the management of a chronic illness (Sisk et al., 2006). The innovation, which includes home
visit and telephone follow-ups conducted by nurses, is based on the best available evidence to
provide care for HF patients. Its goal is to serve patients in a holistic way to meet both the
physical and psychological needs. The face-to-face interaction during home visits and
telephone follow-ups are two-way communication tools. These tools help the patients to
identify, explore and analyze the problems they encountered when following the treatment
regimen.
All the objectives of the proposed intervention are consistent with the vision, mission and
value of HA. This further enhances the transferability of the innovation into the target setting.

23
3.3.3 Number of patients to be benefited
From the admission record in October 2015 of the target setting, there are around 300
emergency admissions every month. Among these 300 patients, 5% of them are diagnosed as
HF. Therefore, there are about 180 HF patients admitted to the target medical ward annually.
This implies that around 180 HF patients would benefit from the home-based intervention
annually.
3.3.4 Length of implementation and evaluation
A total of 18 months will be required for the implementation and evaluation of the
intervention. For the 18-month period, a month will be spent on staff training and the
preparation of equipment, 5 months on conducting a pilot study and refining the protocol, 6
months on implementing the home-based intervention, and 6 months as the follow-up period
and the evaluation of the entire home-based intervention protocol.
3.4 Feasibility
The feasibility of the intervention is evaluated through three aspects: organization, nurse
and resources.
3.4.1 Organization
Organizational support is an essential element for the success of a new intervention.
The target hospital supports evidence-based practice. An Evidence-Based Practice
committee was established in 2011. The Journal Club, which was founded in 2013, holds
meetings three times a year. The members of the committee come from different disciplines,
such as nurses, physiotherapists and occupation therapists. They share literature on the same
topic and develop guidelines together based on the latest available evidence for improving the
current practice. A program of the early removal of Foley catheter was one of the guidelines
developed in March 2015 by this committee and implemented in different departments.

24
As the innovation is based on the best available evidence, it has a very high potential to
gain organizational support.
3.4.2 Nurse
Autonomy
In the target setting, the ward manager supports evidence-based practice. She always
encourages and provides opportunities for her subordinates to attend different courses. Then
she will gather the latest information from her subordinates and put into current practice
wherever appropriate. She shows great support to new changes if they are beneficial to patients
or the staff. For example, the target ward was the first medical ward to implement a new
program called ‘Safe Mobilization of Fragile Patient’ in August 2015. The program aims at
reducing the number of accidents by using some noticing cards to increase the alertness of the
staff when transferring patients. With the support from ward manager, the autonomy and
freedom for nurses to implement new intervention is greater.
In the home-based intervention, nurses may need to consult patients’ primary physicians
if the patient requires medical review. In this part, cooperation with physicians is required.
Potential barriers may appear. Meetings will be held for getting their support.
Interference
The innovation will not interfere the current staff function. The ward nurses are only
required to stick a gum label of the HF patient in a designated file when the patient is discharged,
which facilitates the tracing of the patient. This action only takes 10 seconds at most. Therefore,
it would not interfere the daily routine of the ward and nurses.
For the home visits and telephone follow-ups, a total of four nurses are required, which
will not interfere the current staff function as they only need to utilize the overlapping time
between A shift and P shift, i.e. from 1 pm to 4 pm every day. Only 1 to 2 staff are needed to
conduct home visits or telephone follow-ups each time. The ward routine will not be disturbed.
25
Availability of manpower and training
The intervention includes home visits and telephone follow-ups. I will be responsible for
home visits. An additional nurse will also be trained by me to conduct home visits. The training
session for home visits will last 2 hours. I will coach two nurses to conduct telephone follow-
ups in a 1-hour training session. The trainees should have at least three years of working
experience in a medical unit. The rank of the trainees can be advanced practice nurses,
registered nurses or enrolled nurses in the target setting. The overlapping hours between A shift
and P shift will be utilized for conducting home visits and telephone follow-ups, i.e. between
1pm and 4pm. During this period, A shift nurses usually help with the routine such as
medication administration, turning of patients and admitting patients; while P shift nurses
usually study kardex and do bedside cares for patients. Normally, there are four A shift nurses
to complete the routine duties. As only 1 to 2 A shift nurses are required to conduct home visits
or telephone follow-ups, the manpower is readily available. A home visit will take around 2
hours for each patient, and a telephone follow-up will take around 15 minutes for each patient.
Attitude
The attitude of nurses towards the intervention is another important issue that has to be
considered when implementing a new intervention as nurses are the ones who facilitate the
implementation of the intervention.
Extra work is added to nurses’ daily work. Work allocation among nurses changes. For
example, they have to stick a gum label of HF patients to a file to facilitate the tracing of
discharged HF patients. This requires some time and nurses have to remember to do this. As
mentioned before, the overlapping time between A shift and P shift will be spent on conducting
home visits and telephone follow-ups. This will affect the manpower for routine duties. Their
work schedule is tight already. As a result, it may be difficult to ask them to do extra work
despite the fact that it takes only little time and effort. Their motivation for adapting to such a

26
change may be low. Hence, a briefing session for the frontline staff about the intervention will
be held for getting their support.
3.4.3 Resources
Availability of resources
Paper for sticking the gum label of HF patients and a file for keeping the paper are readily
available. Telephone for the telephone follow-ups are also readily available in the target setting.
Availability of measuring tool
The admission rate due to HF will be used for evaluating the success of the intervention.
The admission record is kept in the target setting’s admission book, which is readily available.
With the above items readily available in the target setting, the feasibility of implementing
the innovation is enhanced.
3.5 Cost and benefit ratio
3.5.1 Benefits
The benefits of the innovation can be observed from three aspects: the health care
system, patients and nurses.
Health care system
Home-based intervention helps with the reduction in hospital readmission due to HF
(Morcillo et al., 2009; Tsuchihashi-Makaya et al., 2013; Sisk et al., 2006; Stewart et al., 1999;
Stewart et al., 1999). The number of emergency department visits due to HF can also be
reduced (Morcillo et al., 2009; Sisk et al., 2006; Stewart et al., 1999). Furthermore, the length
of hospital stay can be reduced (Stewart et al., 1999; Stewart et al., 1999). Moreover, the
number of deaths due to HF can be reduced (Krumholz et al., 2002; Morcillo et al., 2009;
Stewart et al., 1999).
27
With the reduction of healthcare use brought about by the implementation of home-
based intervention, healthcare cost can be significantly reduced (Krumholz et al., 2002;
Morcillo et al., 2009; Stewart et al., 1998).
Patients
By implementing home-based intervention, patients can continue to receive
professional care from nurses in their most familiar environment, i.e. their homes. With
reduced admission to hospital and length of hospitalization, patients’ QoL can be improved
(Brotons et al., 2009; Sisk et al., 2006; Stewart et al., 1999).
Nurses
The bed occupancy of the target setting is usually over 100% according to the record of
the daily ward occupancy in 2015. A nurse usually takes care of 10 to 12 patients during A
shift or P shift, and up to 25 patients during the night shift. In comparison, the mandatory nurse-
to-patient ratio in acute care hospitals in California is 1:4 (Upenicks, Kotlerman, Akhavan,
Esser & Ngo, 2007). With the unreasonable nurse-to-patient ratio in the target setting, the
workload of a nurse is very high. Their mealtime may be reduced. Overtime work may also be
needed. They are exhausted both physically and mentally after a day of work. By implementing
the intervention, the admissions due to HF can be reduced by around 15% (Morcillo et al.,
2009; Tsuchihashi-Makaya et al., 2013; Sisk et al., 2006; Stewart et al., 1999; Stewart et al.,
1999). This implies that there will be fewer patients in the ward. As a result, nurses’ workload
may be reduced.
In addition, the innovation is constructed as a result of doing literature review and
deploying the best available evidence. This provides a chance for nurses to appreciate high
quality studies and gain more knowledge of evidence-based practice.

28
3.5.2 Risk of avoiding the innovation
Hong Kong has a rapid aging population. According to the Population Census (2011), the
average annual growth rate of the number of older persons was 4.8% over the past 50 years. In
addition, the incidence rate of HF increases with age (Hung et al., 2000). The demand for
healthcare services by HF patients will become greater. If the innovation is not implemented,
the burden to the healthcare system will be heavier.
3.5.3 Potential cost
The required materials for the innovation, which include paper, files and telephones,
are all readily available. The estimated annual material cost will be HK$60.
The major manpower for the intervention is nurses. Nurses are involved in the training
session, home visits and telephone follow-ups. By using the median hourly wage for a
registered nurse, the estimated annual manpower cost will be HK$91,400.
Therefore, the total annual cost for the intervention will be HK$91,460. As mentioned
before, there are about 180 HF patients annually. That means the potential cost for each HF
patient will be around HK$508.
The details about the potential cost of the intervention are listed in Appendix 7.
Analysis
It is assumed that a HF patient is admitted to hospital and stay for one day only.
According to the report by HA annual planning 2015-16 (Hospital Authority, 2015), the daily
in-patient fee for a patient who is admitted to a general ward is HK$4,910. By comparing the
potential cost of the intervention and the actual daily in-patient fee, approximately about
HK$4,402 will be saved in taking care of one HF patient.
3.6 Evidence-Based Practice Guideline
The development of the evidence-based practice protocol is based on the results
synthesized from the reviewed literature and after the assessment of the implementation

29
potential. The protocol is used as a simple tool by nurses working in the medical unit for the
management of HF patients. Each recommendation in the protocol is graded with reference to
the grading system of the SIGN (SIGN, 2008). The grading system of the SIGN is shown in
Appendix 8. The details of the protocol are shown in Appendix 9.

30
Chapter 4
Implementation Plan
4.1 Communication Plan
Potential stakeholders are identified for implementing the innovation. They include the
Chief of Service (COS) and the Department Operation Manager (DOM) of the Department of
Medicine, one cardiac specialist, the ward manager, three physicians and all frontline nurses
of the target setting.
A top-down approach will be used in the communication plan. Approval and support will
firstly be gained from the managerial level, then the executive level and finally the frontline
level.
Various communication activities will be conducted to gain support and get opinions from
the stakeholders.
4.1.1 Communication activities
For the managerial level
Gaining approval from the managerial level is the first step in the implementation of the
innovation. The COS and the DOM of the Department of Medicine are the two most powerful
policymakers in the proposed setting. They are responsible for decision making, approving
guidelines and allocating resources. In order to gain their approval, an oral presentation will be
arranged to present the significance, evidence, implementation potential, cost-benefit ratio,
timeline, protocol and pilot test of the innovation to them. A written proposal including the
details of the innovation will also be submitted.
For the executive level
Gaining support and getting opinions from the executive level is the second step in the
implementation phase. The cardiac specialist is an expert at the management of HF. With his
opinions, the protocol of the innovation will be more comprehensive. The ward manager of the
31
target setting is in charge of the ward. She is responsible for allocating resources and assisting
with the implementation of new protocols in the ward. In order to gain the support and get
opinions from the cardiac specialist and the ward manager, meetings will be arranged. During
the meetings, the significance, evidence, implementation potential, cost-benefit ratio and
timeline of the innovation will be discussed.
For the frontline staff
The final step of the implementation process is gaining support from the frontline staff.
The frontline staff is the users of the innovation. It includes the nurses and physicians who are
working in the target setting. Nurses are included because some of them are responsible for
conducting home visits and telephone follow-ups with eligible patients, and all of them are
required to stick a gum label of HF patients to a designated file when they are discharged.
Physicians are included because when their opinions are needed for medical review. Briefing
sessions will be given to the frontline staff for increasing their awareness of the importance of
the issue, allowing them to understand the advantages of the innovation, and getting their
opinions about the workflow of the innovation.
4.1.2 Communication team
A communication team will be set up to monitor the implementation process. The team
will be composed of the proposer of the innovation, a cardiac specialist, the ward manager and
an advanced practice nurse (APN) of the target setting. The proposer will be responsible for
training the nurses for the home visits and telephone follow-ups. The cardiac specialist will
provide assistance in and opinions about home visits and telephone follow-ups of the
innovation. The ward manager will be responsible for monitoring the progress and the outcome
of the innovation. The APN will collect feedback from different parties. Meetings will be held
within the communication team every 2 weeks. During the meetings, team members will share
their information and modifications of the protocol will be made.

32
4.2 Pilot study
A pilot study will be conducted to explore the feasibility of the proposed innovation. It
will last 5 months. Opinions from different parties will be collected during the pilot study. The
protocol will be refined after the pilot study.
The training session and the briefing session will be conducted in Week 1. Eligible
patients will be recruited from Week 2 to Week 5. Home visit and telephone follow-ups will
be conducted from Week 6 to Week 17. The pilot study will be evaluated between Week 18
and Week 19. The proposed protocol will be refined in Week 20. A diagram for the timeline
of the pilot study is shown in Appendix 10.
4.2.1 Training session
The proposed intervention will include home visits and telephone follow-ups. A 2-hour
training session on conducting home visits will be held by the proposer to train a nurse in the
target setting. A 1-hour training session on conducting telephone follow-ups will be held by
the proposer to train two nurses in the target setting. The trainee should have at least three years
of working experience in a medical unit. As the training sessions are taught by the proposer,
this can ensure the standardization of the services to be offered.
4.2.2 Briefing session
A 15- to 30-minute briefing session will be held for the frontline staff by the
communication team. It will be held every day for 1 week so that every frontline staff member
can join it. The session will introduce the significance of the issue, evidence and cost-benefit
ratio of the innovation. The workflow and the responsibilities of different parties will also be
explained. A simple Question and Answer session will be included to answer any enquiries.
4.2.3 Recruitment of patients
Patients for the pilot study will be recruited under the inclusion and exclusion criteria
that will be stated in chapter 4.3.3. The recruitment period will last 4 weeks. It is expected that

33
around 15 patients will be recruited under convenience sampling in 4 weeks according to
previous admission record in the target setting.
4.2.4 Evaluation of the pilot study
Through evaluation, problems arisen during the pilot study can be identified.
Refinements of the proposed protocol can then be made. The feasibility of the proposed
innovation can also be verified. The evaluation will be conducted by the communication team
for 2 weeks. The following aspects will be considered.
The first aspect is the cost. The ward manager will calculate the material and non-
material costs of the pilot study. The total cost of the full-scale study can then be estimated and
a budget plan can be worked out.
The second aspect is the feedback from frontline staff. The APN will conduct a discussion
session with them. Misunderstanding of the innovation can be clarified. Opinions about the
workflow can be collected. Problems encountered can be resolved during the discussion. A
questionnaire (Appendix 11) will be distributed to the frontline staff for evaluating their
satisfaction level with the innovation. Moreover, the APN will have an audit to monitor the
compliance of nursing staff. The audit form is shown in Appendix 12.
4.2.5 Refinement of the proposed protocol
Based on the evaluation results in the pilot study, refinement of the proposed protocol
will be made by the communication team. This will last 1 week.
4.3 Evaluation plan
An evaluation plan is developed for assessing the outcomes of the innovation. By
assessing the outcomes, the effectiveness of the innovation can be examined.

34
4.3.1 Outcomes of the innovation
Patients
The objective of the innovation is to reduce the hospital readmission rate of HF patients,
which is the primary outcome of the innovation. It is measured and evaluated by using the data
from the admission record book in the target setting.
Besides the hospitalization rate, the reduction in the AED visiting rate can also help to
evaluate the effectiveness of the innovation. The AED visiting rate is measured by using
electronic medical records.
From the reviewed literature, patients’ QoL might be potentially improved by the
innovation. It will also be assessed in this innovation. It is measured by MLHF questionnaire
with a scale of 0 to 5 in each question, which means ‘no impairment’ to ‘very much
impairment’. It is a valid and reliable tool in measuring health-related QoL in HF patients (Ho,
Clochesy, Madigan & Liu, 2007). The MLHF questionnaire is shown in Appendix 14.
Patients’ satisfaction level towards the innovation and their knowledge of HF are also
considered and will be assessed through interviews during telephone follow-ups.
Healthcare providers (HCPs)
The satisfaction level of HCPs towards the innovation will affect the sustainability and
effectiveness of the innovation. Therefore, a questionnaire will be distributed to collect their
opinions about the innovation. Focus group interviews will also be arranged for discussing the
issues related to the innovation.
The compliance of the HCPs is another factor that will affect the sustainability of the
innovation. Regular audits will be done every month.
The healthcare system
The material and non-material costs for implementing the innovation are the major
concerns of the healthcare system. Data from the hospital finance department will be used.
35
4.3.2 Timeline for evaluation
Based on the effect size and length of follow-up from the reviewed studies, the
innovation will take effect in about 6 months. Therefore, all the outcomes will be measured
within 6 months after the implementation of the innovation.
4.3.3 Nature of clients
The inclusion and exclusion criteria are based on the reviewed literature. Eligible patients
are adult patients aged 18 or above and admitted to hospital with the primary or secondary
diagnosis as HF and of different degrees of severity. Patients having communication barriers,
being unable to participate in telephone follow-ups or having cognitive deficit are excluded
from the innovation.
4.3.4 Sample size calculation
A same group pretest-posttest design will be used to compare the readmission rate before
and after the innovation is adopted. The statistical method used is a two-tailed paired t-test.
The sample size calculation is based on the reviewed studies and the pilot study. By using an
online software called G*Power, with a 5% scientific significance level, a power of 0.80 and a
calculated effect size of 0.41, a sample size of 48 subjects is needed. With reference to the
average dropout rate of 8.25% in the reviewed studies (Brotos et al., 2009; de Souza et at.,
2014; Morcillo et al., 2005; Stewart et al., 1999; Tsuchihashi-Makaya et al., 2013), an addition
of 12 subjects is required for covering the dropout rate. Therefore, the total sample size will be
60. According to the admission record of the target setting in Oct 2015, the number of HF
patients admitted is 15 every month. Therefore, a 4-month period is needed for recruiting the
required sample size.
4.3.5 Data analysis
Different outcomes are collected and analyzed by different methods.

36
Outcomes of patients
The healthcare utilization rate will be evaluated in the 6th month. The healthcare
utilization rate during the 6 months before the intervention will be traced through electronic
medical records and used as the baseline. After the intervention is implemented for 6 months,
the rate will be measured again for comparison. The mean group differences between the
changes from the baseline will be evaluated by paired t-test.
Patients’ QoL will be evaluated in the 6th month by calculating the scores in the MLHF
questionnaire. Before the start of the intervention, the participants are required to complete the
questionnaire as the baseline information. After the intervention is implemented for 6 months,
they will complete the questionnaire again for making comparison. The mean group differences
between the changes from the baseline will be evaluated by paired t-test.
Patients’ knowledge will be evaluated by conducting telephone interviews in the 6th
month. A validated questionnaire developed from the Coronary Artery Disease Education
Questionnaire will be used (Bonin et al., 2014). The questionnaire is shown in Appendix 15.
The number of correct answers will be counted and analyzed by descriptive statistics. Patients’
satisfaction level will also be evaluated in the 6th month during an interview by using a
questionnaire with a 5-point likert scale (Appendix 13). The total score of their responses will
be analyzed by descriptive statistics. An open-ended question is included for getting more
information.
Outcomes of HCPs
The satisfaction level of HCPs will be evaluated in the 6th month by using a 5-point
likert scale questionnaire (Appendix 11). The scores calculated from the questionnaire will be
analyzed by descriptive statistics. There is an open-ended question for getting more comments.
A focus group interview will be held in the 3rd month. It will be tape-recorded and transcribed

37
for qualitative analysis. The group will include three nurses and three physicians, and will focus
on discussing the workflow of the intervention and their problems throughout the intervention.
The compliance level of nurses will be evaluated by descriptive statistics by doing
regular audits every month for 6 months. The audit form is shown in Appendix 12.
Outcomes of the healthcare system
The material and non-material costs of the intervention will be calculated in the 6th
month. A cost-benefit analysis will be performed.
4.4 Basis for implementation
The primary outcome of the intervention is the reduction in hospital readmission rate
of HF patients. From the reviewed studies, its reduction rate ranged from 5.2% to 85%
(Morcillo et al., 2009; Sisk et al., 2006; Stewart et al., 1999; Steward et al., 1999, Tsuchihashi-
Makaya et al., 2013). If there is a reduction of at least 5.2% after 6 months, the innovation will
be considered to be effective.
The AED visiting rate is evaluated. Its reduction rate ranged from 5.7% to 112% in the
reviewed studies (Morcillo et al., 2009; Sisk et al., 2006). If there is a reduction of at least 5.7%
in 6 months, the innovation will be considered to be effective.
An improvement in patients’ QoL indicates the success of the innovation. It is measured
by MLHF questionnaire. A lower score indicates less harmful effect of HF on patients’ QoL
(Ho et al., 2007). Three reviewed studies showed there was a reduction in MLHF scores, which
ranged from 7 to 19 (Brotons et al., 2009; Sisk et al., 2006; Steward et al., 1999). A reduction
of at least 7 in the scores reflects that the innovation is effective.
An improvement in patients’ knowledge also indicates the success of the innovation. It
is assessed by a validated questionnaire. If the patient can answer 50% of the questions
correctly, it implies that he has an acceptable level of knowledge (Bonin et al., 2014). Therefore,

38
if more than 80% of the patients can answer 50% of the questions correctly, the innovation will
be considered to be effective.
Satisfaction levels of both patients and HCPs are important indicators of the
effectiveness of the innovation. They are evaluated by calculating the scores in the satisfaction
questionnaires. The innovation will be considered to be effective if the mean score is 3 among
80% of the respondents or more.
For the compliance level of nurses, the innovation will be considered to be effective if
the rate is 70%. The percentage is set at a moderate level because the innovation is new to the
frontline staff.
For the healthcare cost, with the consensus reached in the communication team, the
innovation will be considered to be effective if there is a 20% reduction in the cost annually.
4.5 Conclusion
With the fact that Hong Kong has an aging population and the incidence of HF increases
with age, more people are suffering from HF. When HF patients are discharged from hospitals,
no one can monitor their conditions or guarantee that they will follow the treatment regimen at
home.
A translational research was done to formulate an evidence-based protocol on home-
based intervention for HF patients. 8 studies were critically appraised and evidence showed
that home-based intervention could reduce hospital readmission rate. Besides, home-based
intervention for HF patients could also improve patients’ QoL and reduce healthcare cost.
With numerous favorable outcomes, home-based intervention is recommended and
should be incorporated into current management of HF patients in local medical units in public
hospitals.

39
References
Aguado, O., Morcillo, C., Delàs, J., Rennie, M., Bechich, S., Schembari, A., Fernández, F. &
Rosell, F. (2010). Long-term implications of a single home-based educational
intervention in patients with heart failure. Heart Lung, 39(6), S14-22.
American Heart Association (2015). What is Heart Failure? Retrieved Oct 30, 2015
from
http://www.heart.org/idc/groups/heartpublic/@wcm/@hcm/documents/downloadable/uc
m_300315.pdf
Bonin, C.D., Santos, R.Z., Ghisi, G.L., Vieira, A.M., Amboni, R. & Benetti, M (2014).
Construction and Validation of a questionnaire about heart failure patients’
knowledge of their disease. Arq Bras Cardiol, 102(4), 364-373.
Brazier, J.E., Hraper, R., Jones, N.M., O’Cathain, A., Thomas, K.J., Usherwood, T. &
Westlake, L. (1992). BMJ, 305(6864), 160-164.
Brazier, J.E. & Roberts, J. (2004). The estimation of a preference-based measure of health
from the SF-12. Medical Care, 42(9), 851-859.
Brotos, C., Falces, C., Alegre, J., Ballarin, E., Casanovas, J., Catà, T., Martinez, M.,
Moral, I., Ortíz, J., Pérez, E., Rayó, E., Recio, J., Roig, E. & Vidal, X. (2009).
Randomized Clinical Trial of the Effectiveness of a Home-Based Intervention in
Patients With Heart Failure: The IC-DOM Study. Rev Esp Cardial, 62(4), 400-408.
Bui, A.L., Horwich, T.B. & Fonarow, G.C. (2011). Epidemiology and risk profile of
heart failure. Nat Rev Cardiol, 8(1), 30-41.
Centre for Health Protection (2015). Heart Diseases. Retrieved Oct 30, 2015 from
http://www.chp.gov.hk/en/content/9/25/57.html

40
de Souza, E.N., Rohde, L.E., Ruschel, K.B., Mussi, C.M., Beck-da-Silva, L., Biolo, A.,
Clausell, N. & Rabelo-Silva, E.R. (2014). A nurse-based strategy reduces heart failure
morbidity in patients admitted for acute decompensated heart failure in Brazil: the
HELEN- clinical trial. European Journal of Heart Failure, 16(9), 1002-1008.
Heidenreich, P.A., Albert, N.M., Allen, L.A., Bluemke, D.A., Butler, J., Fonarow, G.C., et al.
(2013). Forecasting the impact of heart failure in the United States: a policy statement
from the American Heart Association. Circ Heart Fail, 6(3), 606-619.
Ho, C.C., Clochesy, J.M., Madigan, E. & Liu, C.C. (2007). Psychometric evaluation of the
Chinese Version of the Minnesota Living with Heart Failure Questionnaire. Nursing
Research, 56(6), 441-448.
Hospital Authority Convention (2012). Heart to Heart Program: From hospital to
community. Retrieved on February 11, 2016 from
www.ha.org.hk/haconvention/hac2012/proceedings/downloads/SPS5.6.pdf
Hospital Authority (2015). Hospital Authority Annual Planning 2015-16. Retrieved on
February 11th, 2016 from http://www.ha.org.hk/upload/publication_13/298.pdf
Hospital Authority (2016). Vision, Mission and Values. Retrieved on February 11th, 2016
from
http://www.ha.org.hk/visitor/ha_visitor_index.asp?Content_ID=10009&Lang=ENG&
Dmension=100&Parent_ID=10004#
Hospital Authority Convention (2012). Heart to Heart Program: From hospital to
community. Retrieved on February 11, 2016 from
www.ha.org.hk/haconvention/hac2012/proceedings/downloads/SPS5.6.pdf
Hung, Y.T., Cheung, N.T., Ip, S. & Fung, H. (2000). Epidemiology of heart failure in
Hong Kong, 1997. Hong Kong Med J, 6(2), 159-162.
41
ICD-10 (2016). ICD-10-CD Diagnosis Codes. Retrieved on February 11, 2016 form
www.icd10data.com/ICD10CM/Codes/100-199/130-152/150-
Krumholz, H.M., Amatruda, J., Smith, G.L., Mattera, J.A., Roumanis, S.A., Radfora,
M.J., Crombie, P. & Vaccarino, V. (2002). Randomized Trail of an Education and
Support Intervention to Prevent Readmission of Patients With Heart Failure.
Journal of the American College of Cardiology, 39(1), 83-89.
McMurray, J.J. & Pfeffer, M.A. (2005). Heart Failure. Lancet, 365(9474), 1877-1889.
Middel, B., Bouma, J., de Jongste, M., van Sonderen, E., Niemeijer, M.G., Crijns, H. & van
den Heuvel, W. (2001) Psychometric properties of the Minnesota Living with Heart
Failure Questionnaire (MLHF-Q). Clinical Rehabilitation, 15(5), 489-500.
Moher, D., Liberati, A., Tetzlaff, J., Altman, D.G., The PRISMA group (2009). Preferred
Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA
Statement. PLoS Med 6(6): e1000097. doi:10.1371/journal.pmed1000097
Morcillo, C., Valderas, J.M., Aguado, O., Delás, J., Sort, D., Pujadas, R. & Rosell, F.
(2005). Evaluation of a Home-Based Intervention in Heart Failure Patients. Results of
a Randomized Study. REV Esp Cardial, 58(6), 618-625.
Nasif, M. & Alahmad, A. (2015). Public Health and Specific Diseases: Congestive Heart
Failure. Public Health Management & Policy (12th ed.): Case Western Reserve
University.
Population Census (2011). Thematic Report: Older Persons. Census and Statistics
Department, Hong Kong Special Administrative Region. Retrieved on February 11th,
2016 from http://www.census2011.gov.hk/pdf/older-persons.pdf
Sanderson, J.E. (2004). Heart failure- a growing epidemic in Asia. Hong Kong Med J,
10(2), 76.

42
Scottish Intercollegiate Guidelines Network, (2008). SIGN50: A guideline developer’s
handbook. Retrieved Nov 7, 2015 from
http://www.sign.ac.uk/guidelines/fulltext/50/annexoldb.html
Scottish Intercollegiate Guidelines Network, (2015). Critical appraisal: Notes and
checklists. Retrieved Nov 7, 2015 from
http://www.sign.ac.uk/methodology/checklists.html
Sisk, J.E., Hebert, P.L., Horowitz, C.R., McLaughlin, M.A., Wang, J.J. & Chassin, M.R.
(2006). Effects of Nurse Management on the Quality of Heart Failure Care in
Minority Communities. Annals of Internal Medicine, 145(4), 273-283.
Stewart, S., Marley, J.E. & Horowitz, J. D. (1999). Effects of a multidisciplinary, home-
based intervention on planned readmissions and survival among patients with chronic
congestive heart failure: a randomized controlled study. Lancet, 354(9184), 1077-
1083.
Stewart, S., Pearson, S. & Horwitz, J.D. (1998). Effects of a Home-Based Intervention
Among Patients With Congestive Heart Failure Discharges From Acute Hospital
Care. Archives of Internal Medicine, 158(10), 1067-1072.
Stewart, S., Vandenbroek, A.J., Pearson, S. & Horwitz, J.D. (1999). Prolonged Beneficial
Effects of a Home-Based Intervention on Unplanned Readmissions and Mortality
Among Patients With Congestive Heart Failure. Archives ofInternal Medicine,
159(3), 257-261.
Tsuchihashi-Makaya, M., Matsuo, H., Kakinoki, S., Takechi, S., Kinugawa, S. & Tsutsui, H.
(2013). Home-Based Disease Management Program to Improve Psychological Status
in Patients With Heart Failure in Japan. Circulation Journal, 77(4), 926-933.
43
Upenieks, V.V., Kotlerman, J., Akhavan, J., Esser, J. & Ngo, M.J. (2007). Assessing nursing
staffing rates: variability in workload intensity. Policy, Politics & Nursing Practice,
8(1), 7-19.
Vellone, E., Jaarsma, T., Stromberg, A., Fida, R., Arestedt, K., Rocco, G., Cocchieri, A. &
Alvaro, R. (2014). The European Heart Failure Self-care Behaviour Scale: new
insights into factorial structure, reliability, precision and scoring procedure. Patient
Education and Counseling, 94(1), 97-102.
44
Appendix 1
Heart Failure classification
NYHA Classes of heart failure:
Class 1- no limitation during ordinary activity
Class 2- slight limitation by SOB and/or fatigue during moderate exertion or stress
Class 3- symptoms with minimal exertion that interfere with normal daily activity
Class 4- inability to carry out any physical activity without SOB, which may be present
even at rest
ACC/AHA Stages of heart failure:
Stage A- high risk for heart failure, without structural heart disease or symptoms
Stage B- heart disease with asymptomatic left ventricular dysfunction
Stage C- prior or current symptoms of heart failure
Stage D- refractory end stage heart failure
(Nasif & Alahmad, 2015)

45
Appendix 2
PRISMA 2009 Flow Diagram
(Moher, Liberati, Tetzlaff & Altman, 2009)
Records identified through PubMed
(n = 166 )
Scre
enin
g In
clu
ded
El
igib
ility
Id
enti
fica
tio
n
Additional records identified through
other sources (n = 6 )
Records after duplicates removed (n = 132 )
Records screened (n = 37 )
Records excluded (n = 95 )
Full-text articles assessed for eligibility
(n = 9)
Full-text articles excluded Reason:
inappropriate study types, inappropriate study interventions,
inappropriate outcome
measurements (n = 28)
Studies included in qualitative synthesis
(n = 8 )
Records identified through CINAHL Plus (EBSCohost)
(n = 1 )
Records identified through Cochrane
Library (n = 72 )

46
Appendix 3
Flowchart
PubMed CINAHL Plus
(EBSCohost)
Cochrane
Library
By keyword search:
1.heart failure
2. home-based intervention OR home-based education OR home-based
counseling OR home-based caring OR nurse-led
3. readmission rate OR resource use OR hospitalization OR hospital utilization
OR hospital use OR hospital readmission
PubMed
166 articles
Reviewed by titles
33 articles
Reviewed by abstracts
1 article
18 articles
1 article
Reviewed by full papers
12 articles
9 articles
24 articles
1 article
7 articles
Total number of articles for review after elimination of duplication: 12 articles
CINAHL Plus
(EBSCohost)
1 article
Cochrane
Library
72 articles
RCT: 8 articles
Manual search
Manual search
6 articles
6 articles
6 articles
6 articles
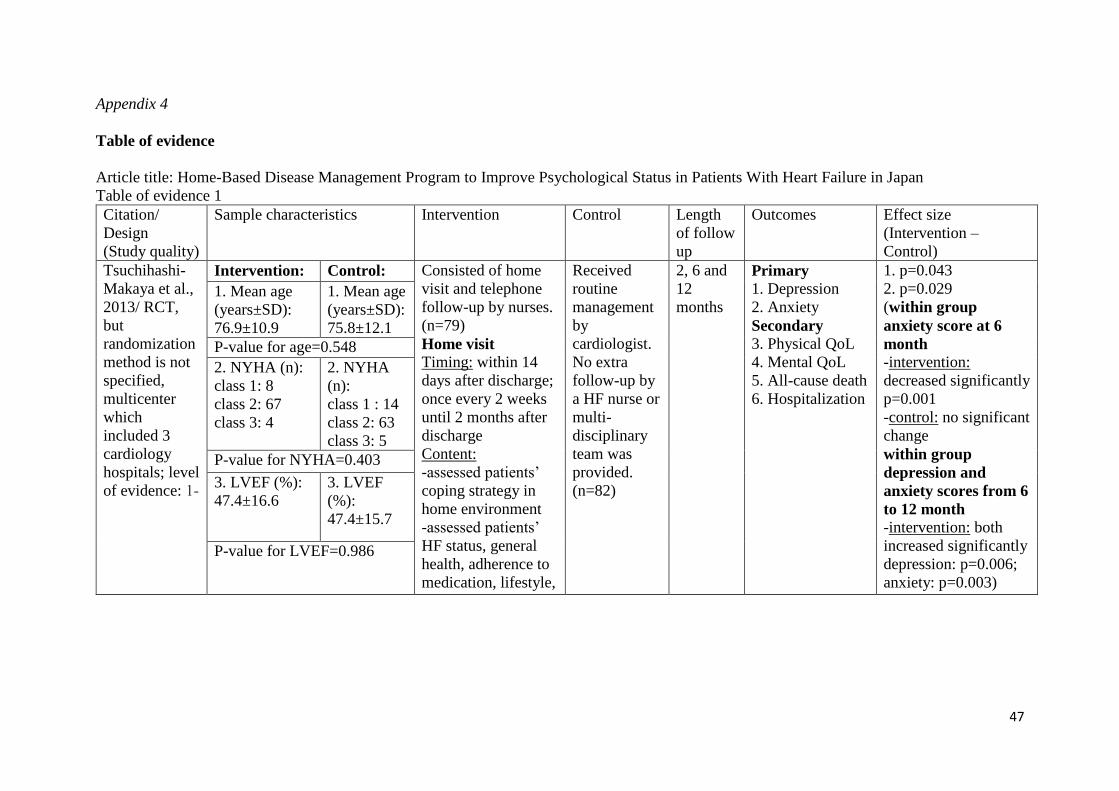
47
Appendix 4
Table of evidence
Article title: Home-Based Disease Management Program to Improve Psychological Status in Patients With Heart Failure in Japan
Table of evidence 1
Citation/
Design
(Study quality)
Sample characteristics Intervention Control Length
of follow
up
Outcomes Effect size
(Intervention –
Control)
Tsuchihashi-
Makaya et al.,
2013/ RCT,
but
randomization
method is not
specified,
multicenter
which
included 3
cardiology
hospitals; level
of evidence: 1-
Intervention: Control: Consisted of home
visit and telephone
follow-up by nurses.
(n=79)
Home visit
Timing: within 14
days after discharge;
once every 2 weeks
until 2 months after
discharge
Content:
-assessed patients’
coping strategy in
home environment
-assessed patients’
HF status, general
health, adherence to
medication, lifestyle,
Received
routine
management
by
cardiologist.
No extra
follow-up by
a HF nurse or
multi-
disciplinary
team was
provided.
(n=82)
2, 6 and
12
months
Primary
1. Depression
2. Anxiety
Secondary
3. Physical QoL
4. Mental QoL
5. All-cause death
6. Hospitalization
1. p=0.043
2. p=0.029
(within group
anxiety score at 6
month -intervention:
decreased significantly
p=0.001
-control: no significant
change
within group
depression and
anxiety scores from 6
to 12 month
-intervention: both
increased significantly
depression: p=0.006;
anxiety: p=0.003)
1. Mean age
(years±SD):
76.9±10.9
1. Mean age
(years±SD):
75.8±12.1
P-value for age=0.548
2. NYHA (n):
class 1: 8
class 2: 67
class 3: 4
2. NYHA
(n):
class 1 : 14
class 2: 63
class 3: 5
P-value for NYHA=0.403
3. LVEF (%):
47.4±16.6
3. LVEF
(%):
47.4±15.7
P-value for LVEF=0.986

48
4. Medical
history with
atrial
fibrillation: 34
4. Medical
history with
atrial
fibrillation:
51
daily activity and
social support needs
Telephone follow-
up
Timing: monthly
until 6 months after
discharge at the
conclusion of home
visit
Content:
-monitored HF
symptoms, general
heath and
requirement for
other health and
social support
Consultation
-consulted a
multidisciplinary
team (cardiologist,
dietitian, pharmacist
and social worker)
during the
intervention period
to optimize the
advice given to each
patient.
3. p=0.359
(within group
-intervention:
p<0.001 at 2 month;
p<0.001 at 6 month;
p<0.001 at 12 month
-control:
p=0.001 at 2 month;
p=0.041 at 6 month;
p=0.037 at 12 month)
4. p=0.046
(within group
-intervention:
p=0.001 at 2 month;
p<0.001 at 6 month;
p=0.003 at 12 month
-control: unchanged)
5. 0%, p=0.967
6. -14%, p=0.037
P-value for medical history
with atrial fibrillation=0.030
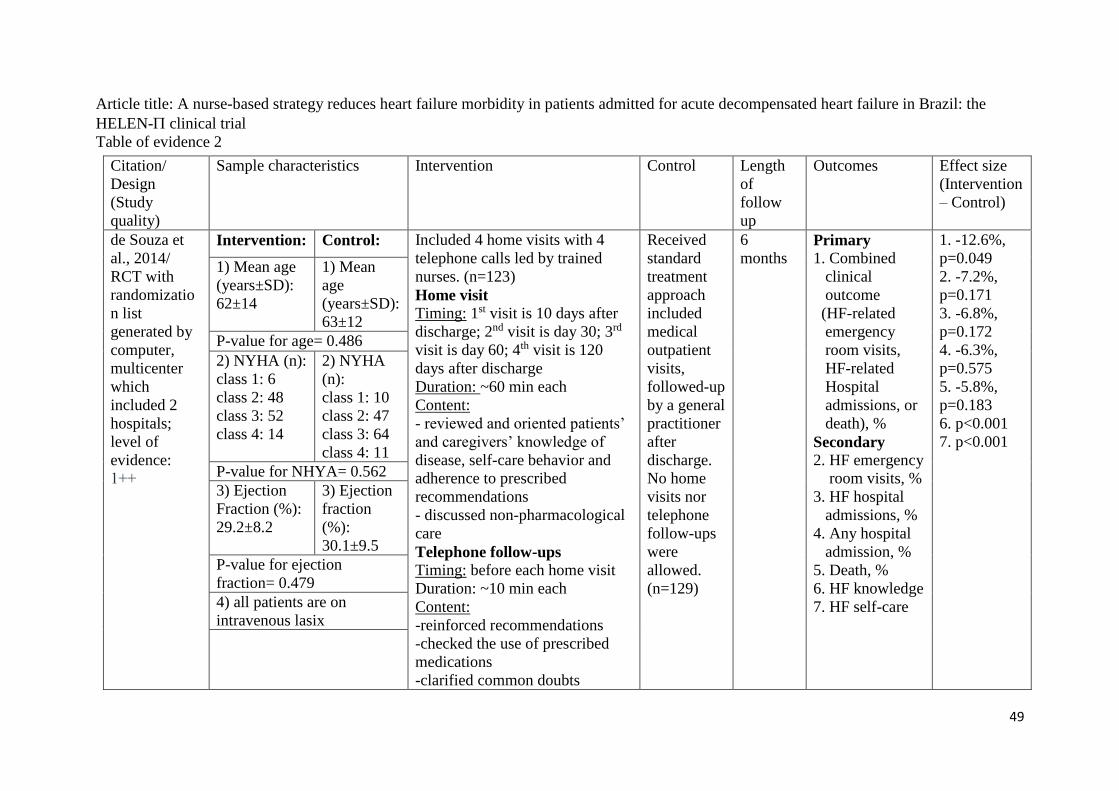
49
Article title: A nurse-based strategy reduces heart failure morbidity in patients admitted for acute decompensated heart failure in Brazil: the
HELEN- clinical trial
Table of evidence 2
Citation/
Design
(Study
quality)
Sample characteristics Intervention Control Length
of
follow
up
Outcomes Effect size
(Intervention
– Control)
de Souza et
al., 2014/
RCT with
randomizatio
n list
generated by
computer,
multicenter
which
included 2
hospitals;
level of
evidence:
1++
Intervention: Control: Included 4 home visits with 4
telephone calls led by trained
nurses. (n=123)
Home visit
Timing: 1st visit is 10 days after
discharge; 2nd visit is day 30; 3rd
visit is day 60; 4th visit is 120
days after discharge
Duration: ~60 min each
Content:
- reviewed and oriented patients’
and caregivers’ knowledge of
disease, self-care behavior and
adherence to prescribed
recommendations
- discussed non-pharmacological
care
Telephone follow-ups
Timing: before each home visit
Duration: ~10 min each
Content:
-reinforced recommendations
-checked the use of prescribed
medications
-clarified common doubts
Received
standard
treatment
approach
included
medical
outpatient
visits,
followed-up
by a general
practitioner
after
discharge.
No home
visits nor
telephone
follow-ups
were
allowed.
(n=129)
6
months Primary
1. Combined
clinical
outcome
(HF-related
emergency
room visits,
HF-related
Hospital
admissions, or
death), %
Secondary
2. HF emergency
room visits, %
3. HF hospital
admissions, %
4. Any hospital
admission, %
5. Death, %
6. HF knowledge
7. HF self-care
1. -12.6%,
p=0.049
2. -7.2%,
p=0.171
3. -6.8%,
p=0.172
4. -6.3%,
p=0.575
5. -5.8%,
p=0.183
6. p<0.001
7. p<0.001
1) Mean age
(years±SD):
62±14
1) Mean
age
(years±SD):
63±12
P-value for age= 0.486
2) NYHA (n):
class 1: 6
class 2: 48
class 3: 52
class 4: 14
2) NYHA
(n):
class 1: 10
class 2: 47
class 3: 64
class 4: 11
P-value for NHYA= 0.562
3) Ejection
Fraction (%):
29.2±8.2
3) Ejection
fraction
(%):
30.1±9.5
P-value for ejection
fraction= 0.479
4) all patients are on
intravenous lasix

50
-reminded patients about the date
of next home visit

51
Article title: Randomized Clinical Trial of the Effectiveness of a Home-Based Intervention in Patients With Heart Failure: The IC-DOM Study
Table of evidence 3
Citation/
Design (Study
quality)
Sample characteristics Intervention Control Length
of follow
up
Outcomes Effect size
(Intervention –
Control)
Brotons et al.,
2009/ RCT
with
randomization
list generated
by computer,
multicenter
which
included 4
hospitals; level
of evidence:
1++
Intervention: Control: Included home visits and
telephone follow-ups
conducted by nurses. And
before discharged, patients
received information about
their disease,
pharmacological and non-
pharmacological
treatments prescribed,
including a booklet
containing information on
heart failure. (n=144)
Home visits
Timing: monthly for entire
year
Content:
-educated about the
disease, symptoms
-assessed adherence to
medication and lifestyle
-reviewed medical history
-checked functional status
and vital signs
Referred to
family
physician or
cardiologist
and a visit
was
scheduled
for 1 year
after
discharge.
(n=139)
12
months Primary
1. Combination
of all-cause
death and
hospital
readmissions
due to
worsening of
HF, %
Secondary
2. cardio-
vascular death,
%
3.hospital
readmission due
to cardio-
vascular disease,
mean number
4. QoL, mean
MLHF scores
5. adherence to
therapy, %
6. satisfaction
1. -12.6%,
p=0.043
2. -1.3%, non-
significant
difference
3. -0.29, non-
significant
difference
4. -12.54,
p<0.001
5. 10.6%,
p=0.057
6. p<0.001
1. Mean age
(years±SD):
76.6±7.5
1. Mean age
(years±SD):
76±8.9
2. NYHA (n):
class 1: 3
class 2: 8
class 3: 62
class 4: 68
unknown: 3
2. NYHA (n):
class 1: 2
class 2: 12
class 3: 48
class 4: 75
unknown: 2
3: LVEF (%):
<30%: 14
30-39%: 24
40-49%: 21
>50%: 40
3. LVEF (%):
<30%: 18
30-39%: 18
40-49%: 21
>50%: 43
4. Comorbidity
with COPD
(numbers): 49
4. Comorbidity
with COPD
(numbers): 28
P-value for comorbidity with
COPD=0.01

52
Telephone follow-ups
Timing: every 15 days
Content:
-evaluated patients’
clinical status
Consultation
-contacted patient’s family
physician or cardiologist
when it is necessary to
start a new treatment or
modify the existing one
(MLWHF: higher scores indicate impaired QoL, negative changes indicate improvement)

53
Article title: Evaluation of a Home-Based Intervention in Heart Failure Patients. Results of a Randomized Study
Table of evidence 4
Citation/
Design (Study
quality)
Sample characteristics Intervention Control Length
of follow
up
Outcomes Effect size
(Intervention –
Control)
Morcillo et
al., 2009/
RCT with
randomization
list generated
by using a
random
number table,
single center;
level of
evidence: 1+
Intervention: Control: Included a single nurse’s
home visit. (n=34)
Home visit
Timing: within the first
month after discharge
Duration: ~2 hour
Content:
-investigated patients’
habits
-established the priority of
behavior susceptible to
modification
-applied an education plan
-instructed patient and
caregivers about the
disease and essential
points regarding self-
management
-complied a short log of
current symptoms
-performed a
cardiovascular physical
examination
Received
conventional
care and had
outpatient
follow-up as
scheduled
by attending
physicians.
Did not
receive a
nurse’s visit.
(n=36)
6 months Primary
1. use of health
service (number
of
hospitalizations
for HF and visit
to emergency
room for HF), %
Secondary
2. patient’s
perception of
health, SF-36
scores
3.economic cost,
€
4. mortality, %
(this outcome
was not included
as an outcome
measure in the
study design)
1. p<0.001
(hospitalization for
HF: -85%,
p<0.001; visit to
emergency room
for HF: -112%,
p<0.001)
2. p<0.01
(within group
intervention:
-physical health
13.2, p<0.01
-mental health
16.4, p<0.01;
control:
-physical health
-0.99, p=0.712
-mental health
-6.29, p=0.120)
3. -€1190.90, p<0.001
4. -24.68%, p<0.05
1. Mean age
(years±SD):
79.1±5.5
1. Mean
age
(years±SD):
76.3±6.2
P-value for age=0.052
2. NYHA (n):
class 2: 9
class 3: 18
class 4: 7
2. NYHA
(n):
class 2: 18
class 3:6
class 4: 12
P-value for NYHA= 0.06
3. mean
LVEF
(%±SD):
35.4±6.8
3. mean
LVEF
(%±SD):
34.3±6.4
P-value for LVEF=0.498
(SF-36: lower scores indicate impaired QoL, positive changes indicate improvement)
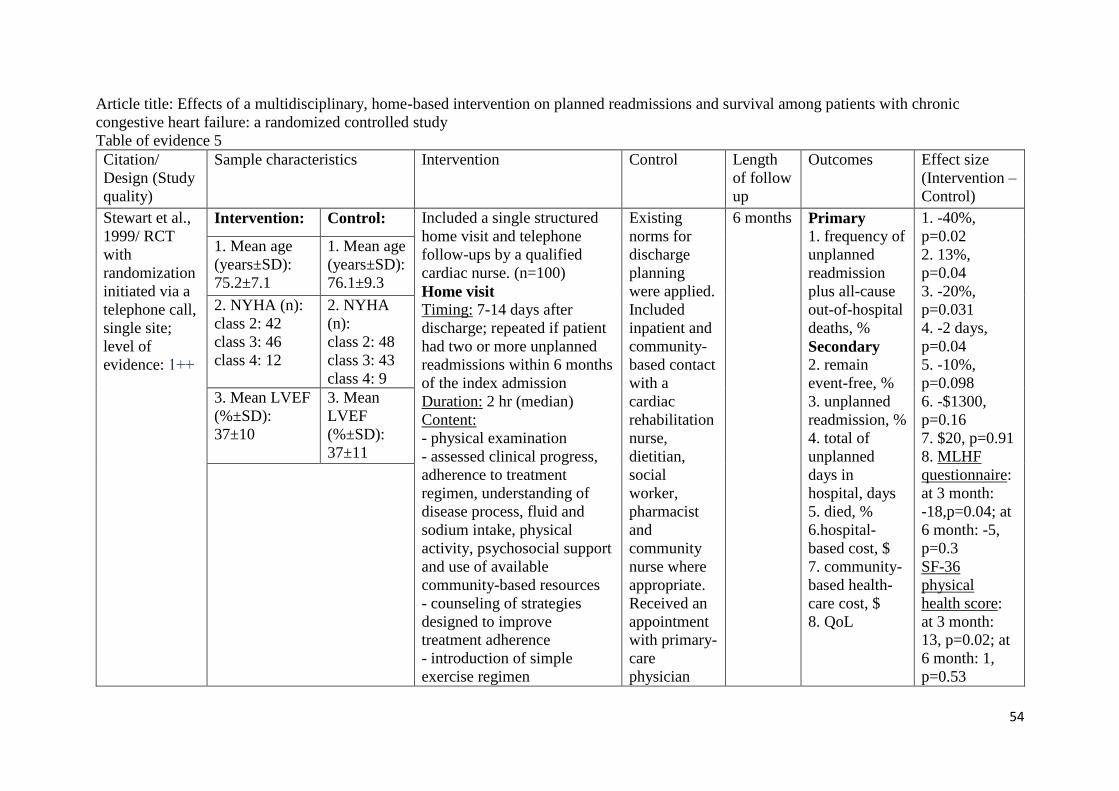
54
Article title: Effects of a multidisciplinary, home-based intervention on planned readmissions and survival among patients with chronic
congestive heart failure: a randomized controlled study
Table of evidence 5
Citation/
Design (Study
quality)
Sample characteristics Intervention Control Length
of follow
up
Outcomes Effect size
(Intervention –
Control)
Stewart et al.,
1999/ RCT
with
randomization
initiated via a
telephone call,
single site;
level of
evidence: 1++
Intervention: Control: Included a single structured
home visit and telephone
follow-ups by a qualified
cardiac nurse. (n=100)
Home visit
Timing: 7-14 days after
discharge; repeated if patient
had two or more unplanned
readmissions within 6 months
of the index admission
Duration: 2 hr (median)
Content:
- physical examination
- assessed clinical progress,
adherence to treatment
regimen, understanding of
disease process, fluid and
sodium intake, physical
activity, psychosocial support
and use of available
community-based resources
- counseling of strategies
designed to improve
treatment adherence
- introduction of simple
exercise regimen
Existing
norms for
discharge
planning
were applied.
Included
inpatient and
community-
based contact
with a
cardiac
rehabilitation
nurse,
dietitian,
social
worker,
pharmacist
and
community
nurse where
appropriate.
Received an
appointment
with primary-
care
physician
6 months Primary
1. frequency of
unplanned
readmission
plus all-cause
out-of-hospital
deaths, %
Secondary
2. remain
event-free, %
3. unplanned
readmission, %
4. total of
unplanned
days in
hospital, days
5. died, %
6.hospital-
based cost, $
7. community-
based health-
care cost, $
8. QoL
1. -40%,
p=0.02
2. 13%,
p=0.04
3. -20%,
p=0.031
4. -2 days,
p=0.04
5. -10%,
p=0.098
6. -$1300,
p=0.16
7. $20, p=0.91
8. MLHF
questionnaire:
at 3 month:
-18,p=0.04; at
6 month: -5,
p=0.3
SF-36
physical
health score:
at 3 month:
13, p=0.02; at
6 month: 1,
p=0.53
1. Mean age
(years±SD):
75.2±7.1
1. Mean age
(years±SD):
76.1±9.3
2. NYHA (n):
class 2: 42
class 3: 46
class 4: 12
2. NYHA
(n):
class 2: 48
class 3: 43
class 4: 9
3. Mean LVEF
(%±SD):
37±10
3. Mean
LVEF
(%±SD):
37±11
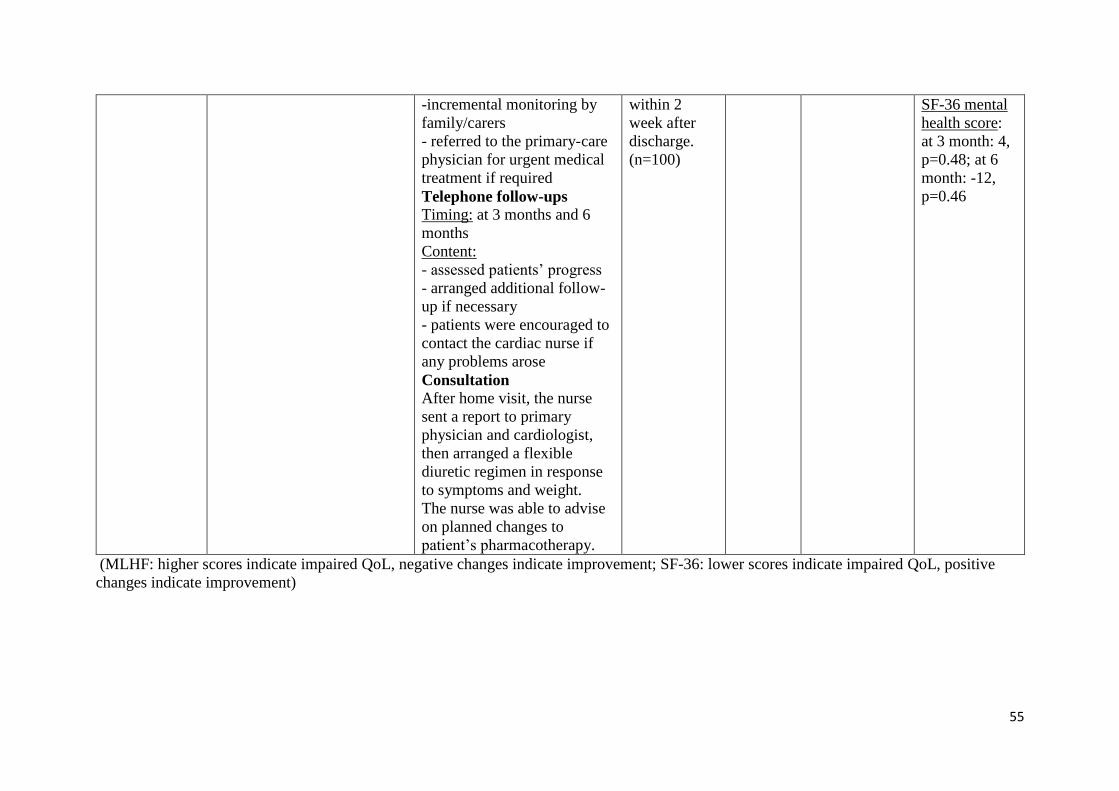
55
-incremental monitoring by
family/carers
- referred to the primary-care
physician for urgent medical
treatment if required
Telephone follow-ups
Timing: at 3 months and 6
months
Content:
- assessed patients’ progress
- arranged additional follow-
up if necessary
- patients were encouraged to
contact the cardiac nurse if
any problems arose
Consultation
After home visit, the nurse
sent a report to primary
physician and cardiologist,
then arranged a flexible
diuretic regimen in response
to symptoms and weight.
The nurse was able to advise
on planned changes to
patient’s pharmacotherapy.
within 2
week after
discharge.
(n=100)
SF-36 mental
health score:
at 3 month: 4,
p=0.48; at 6
month: -12,
p=0.46
(MLHF: higher scores indicate impaired QoL, negative changes indicate improvement; SF-36: lower scores indicate impaired QoL, positive
changes indicate improvement)

56
Article title: Effects of Nurse Management on the Quality of Heart Failure Care in Minority Communities
Table of evidence 6
Citation/
Design (Study
quality)
Sample characteristics Intervention Control Length
of follow
up
Outcomes Effect size
(Intervention
– Control)
Sisk et al.,
2006/ RCT
with
randomization
list generated
by using
computer,
multicenter
which
included 4
hospitals; level
of evidence:
1++
Intervention: Control: Consisted a single initial
visit at patients’ usual
practice setting and follow-
up phone calls conducted by
trained nurses. (n=203)
Initial visit
Content:
-counselling
-stressed the relationship
among sodium intake, fluid
buildup and symptoms
Telephone calls
Timing: scheduled regularly
Content:
-assessed patients’ feeling
and symptoms
-reinforced the importance
of medication adherence,
smoking cessation and low-
sodium
Consultation
-contacted clinicians to
discuss specific medications
-arranged any prescription
changes and examinations
Received
federal
consumer
guidelines for
managing
systolic
dysfunction
but no other
intervention.
(n=203)
12
months Primary
1. all-cause
hospitalization-
persons
hospitalized, %
2. mean change in
SF-12 physical
component scores
3. mean change in
MLHF scores
Secondary
4. hospitalizations
for HF- persons
hospitalized, %
5. AED visit-
persons with an
AED visit, %
1. -7.1%
2. 3.1
3. -7.0
4. -5.2%
5. -5.7%
1. Mean age
(years±SD):
59.6±13.8
1. Mean age
(years±SD):
59.3±13.7
2. NYHA class
(%):
class 1: 17.7
class 2: 24.6
class 3: 16.3
class: 41.4
2. NYHA
class (%):
class 1: 19.2
class 2: 20.2
class 3: 11.8
class 4: 48.8
(MLHF: higher scores indicate impaired QoL, negative changes indicate improvement)
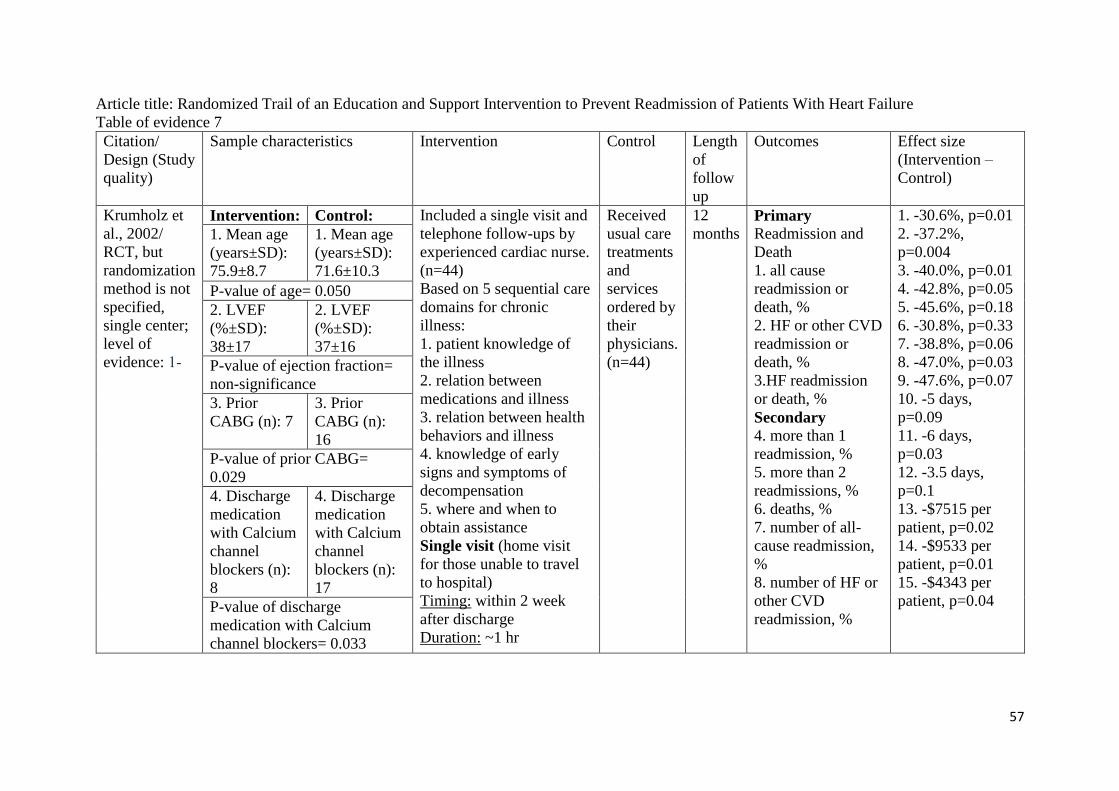
57
Article title: Randomized Trail of an Education and Support Intervention to Prevent Readmission of Patients With Heart Failure
Table of evidence 7
Citation/
Design (Study
quality)
Sample characteristics Intervention Control Length
of
follow
up
Outcomes Effect size
(Intervention –
Control)
Krumholz et
al., 2002/
RCT, but
randomization
method is not
specified,
single center;
level of
evidence: 1-
Intervention: Control: Included a single visit and
telephone follow-ups by
experienced cardiac nurse.
(n=44)
Based on 5 sequential care
domains for chronic
illness:
1. patient knowledge of
the illness
2. relation between
medications and illness
3. relation between health
behaviors and illness
4. knowledge of early
signs and symptoms of
decompensation
5. where and when to
obtain assistance
Single visit (home visit
for those unable to travel
to hospital)
Timing: within 2 week
after discharge
Duration: ~1 hr
Received
usual care
treatments
and
services
ordered by
their
physicians.
(n=44)
12
months Primary
Readmission and
Death
1. all cause
readmission or
death, %
2. HF or other CVD
readmission or
death, %
3.HF readmission
or death, %
Secondary
4. more than 1
readmission, %
5. more than 2
readmissions, %
6. deaths, %
7. number of all-
cause readmission,
%
8. number of HF or
other CVD
readmission, %
1. -30.6%, p=0.01
2. -37.2%,
p=0.004
3. -40.0%, p=0.01
4. -42.8%, p=0.05
5. -45.6%, p=0.18
6. -30.8%, p=0.33
7. -38.8%, p=0.06
8. -47.0%, p=0.03
9. -47.6%, p=0.07
10. -5 days,
p=0.09
11. -6 days,
p=0.03
12. -3.5 days,
p=0.1
13. -$7515 per
patient, p=0.02
14. -$9533 per
patient, p=0.01
15. -$4343 per
patient, p=0.04
1. Mean age
(years±SD):
75.9±8.7
1. Mean age
(years±SD):
71.6±10.3
P-value of age= 0.050
2. LVEF
(%±SD):
38±17
2. LVEF
(%±SD):
37±16
P-value of ejection fraction=
non-significance
3. Prior
CABG (n): 7
3. Prior
CABG (n):
16
P-value of prior CABG=
0.029
4. Discharge
medication
with Calcium
channel
blockers (n):
8
4. Discharge
medication
with Calcium
channel
blockers (n):
17
P-value of discharge
medication with Calcium
channel blockers= 0.033

58
Content:
-used a teaching booklet
for education
Telephone calls
Timing: weekly for 4
weeks then biweekly for 8
weeks then monthly for a
total intervention period of
1 year
Content:
-reinforced care domains
9. number of HF
readmission, %
10. hospital days in
all-cause
readmission, days
11. hospital days in
HF or CVD
readmission, days
12. hospital days in
HF readmission,
days
13. cost of care in
all-cause
readmission, $
14. cost of care in
HF or other CVD
readmission, $
15. cost of care in
HF readmission, $
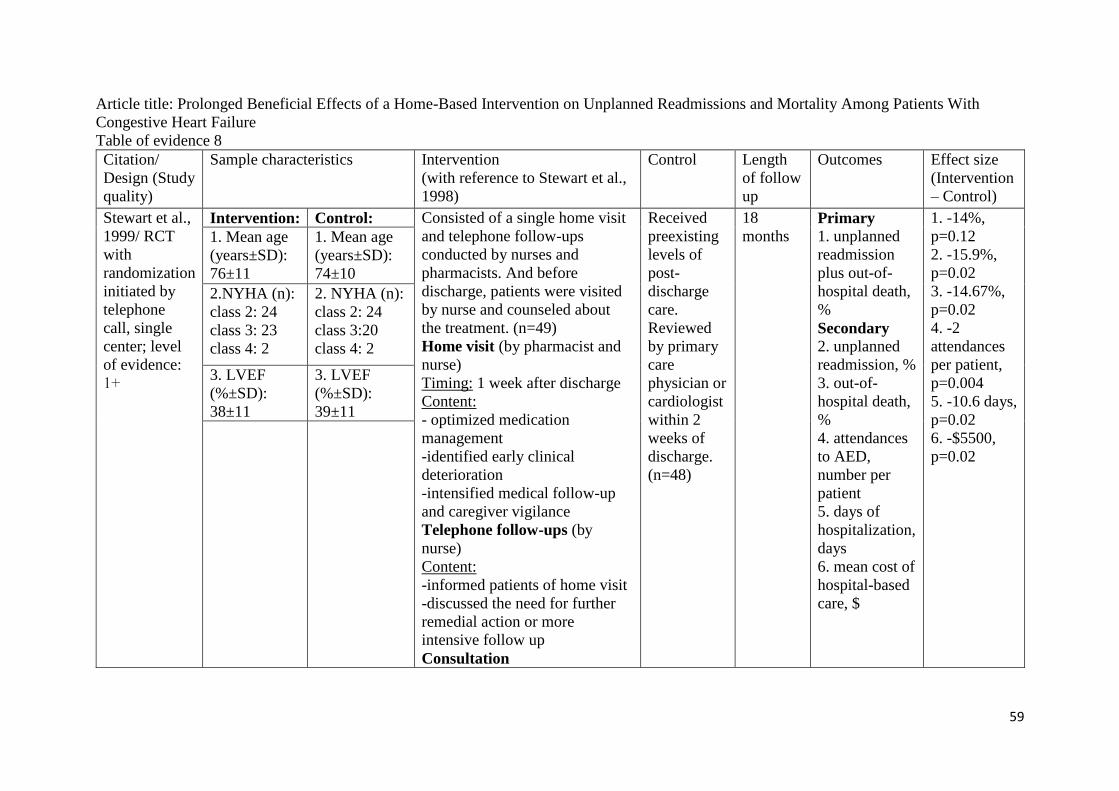
59
Article title: Prolonged Beneficial Effects of a Home-Based Intervention on Unplanned Readmissions and Mortality Among Patients With
Congestive Heart Failure
Table of evidence 8
Citation/
Design (Study
quality)
Sample characteristics Intervention
(with reference to Stewart et al.,
1998)
Control Length
of follow
up
Outcomes Effect size
(Intervention
– Control)
Stewart et al.,
1999/ RCT
with
randomization
initiated by
telephone
call, single
center; level
of evidence:
1+
Intervention: Control: Consisted of a single home visit
and telephone follow-ups
conducted by nurses and
pharmacists. And before
discharge, patients were visited
by nurse and counseled about
the treatment. (n=49)
Home visit (by pharmacist and
nurse)
Timing: 1 week after discharge
Content:
- optimized medication
management
-identified early clinical
deterioration
-intensified medical follow-up
and caregiver vigilance
Telephone follow-ups (by
nurse)
Content:
-informed patients of home visit
-discussed the need for further
remedial action or more
intensive follow up
Consultation
Received
preexisting
levels of
post-
discharge
care.
Reviewed
by primary
care
physician or
cardiologist
within 2
weeks of
discharge.
(n=48)
18
months Primary
1. unplanned
readmission
plus out-of-
hospital death,
%
Secondary
2. unplanned
readmission, %
3. out-of-
hospital death,
%
4. attendances
to AED,
number per
patient
5. days of
hospitalization,
days
6. mean cost of
hospital-based
care, $
1. -14%,
p=0.12
2. -15.9%,
p=0.02
3. -14.67%,
p=0.02
4. -2
attendances
per patient,
p=0.004
5. -10.6 days,
p=0.02
6. -$5500,
p=0.02
1. Mean age
(years±SD):
76±11
1. Mean age
(years±SD):
74±10
2.NYHA (n):
class 2: 24
class 3: 23
class 4: 2
2. NYHA (n):
class 2: 24
class 3:20
class 4: 2
3. LVEF
(%±SD):
38±11
3. LVEF
(%±SD):
39±11

60
-referred to primary care
physician for those requiring
medical review

61
Appendix 5
Levels of evidence
Scottish Intercollegiate Guidelines Network (SIGN) Grading System 1999-2012
1++ High quality meta-analyses, systematic reviews of RCTs, or RCTs with a very low
risk of bias
1+ Well-conducted meta-analyses, systematic reviews, or RCTs with a low risk of bias
1- Meta-analyses, systematic reviews, or RCTs with a high risk of bias
2++ High quality systematic reviews of case control or cohort or studies High quality
case control or cohort studies with a very low risk of confounding or bias and a high
probability that the relationship is causal
2+ Well-conducted case control or cohort studies with a low risk of confounding or bias
and a moderate probability that the relationship is causal
2- Case control or cohort studies with a high risk of confounding or bias and a
significant risk that the relationship is not causal
3 Non-analytic studies, e.g. case reports, case series
4 Expert opinion
(SIGN, 2008)
.

62
Appendix 6
Critical appraisal SIGN checklist
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
1. Tsuchihashi-Makaya, M., Matsuo, H., Kakinoki, S., Takechi, S., Kinugawa, S. & Tsutsui, H. (2013).
Home-Based Disease Management Program to Improve Psychological Status in Patients With Heart Failure
in Japan. Circulation Journal, 77(4), 926-933.
Guideline topic: An Evidence-Based Home-Based
Intervention to Reduce Hospital Readmission Rate in
Patients with Heart Failure
Key Question No: Reviewer:
Cheung Shuk Man
Before completing this checklist, consider:
1. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the study design algorithm available from SIGN and make sure you have the correct checklist. If it is a controlled clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be rated higher than 1+
2. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist. Yes
Reason for rejection: 1. Paper not relevant to key question 2. Other reason (please specify):
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
P: patients with HF in Japan; I: home-based disease management program;
O: improve psychological status
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised.
Randomisation is mentioned but method is not specified.
Yes
Can’t say
No
1.3 An adequate concealment method is used.
No concealment method is reported.
Yes
Can’t say
No
1.4 The design keeps subjects and investigators ‘blind’ about treatment allocation.
The presence of blinding is not clear.
Yes
Can’t say
No
1.5 The treatment and control groups are similar at the start of the trial.
p=0.247
Yes
Can’t say □
No
1.6 The only difference between groups is the treatment under investigation.
The only difference is that the intervention group has home visits and
telephone follow-ups.
Yes
Can’t say
No

63
1.7 All relevant outcomes are measured in a standard, valid and reliable way.
Depression, anxiety and QoL are collected directly or by phone interview.
Prognostic data is based on medical records or telephone.
Yes
Can’t say
No
1.8 What percentage of the individuals or clusters recruited into each treatment arm of the study dropped out before the study was completed?
Total number of participants
who dropped out from the
study =7
The dropout rate
=7/168*100% =4.17%
which is acceptable.
1.9 All the subjects are analysed in the groups to which they were randomly allocated (often referred to as intention to treat analysis).
ITT is not mentioned.
Yes
Can’t say
No
Does not apply
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
No site specific data is given.
Yes
Can’t say
No
Does not apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++)
Acceptable (+)
Low quality (-)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the study intervention?
No
The sample size’s calculation is not mentioned.
Randomization and concealment methods are not
included. ITT is also not mentioned.
Therefore, there is a high risk of bias, and overall
effect might be greatly affected.
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline?
No
The study was conducted in 3 hospitals specializing in
cardiovascular treatment. Therefore, the results are
applicable to the patient group targeted by this
guideline.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question and mention any areas of uncertainty raised above.
The author concluded that a home-based disease management intervention improved depression and anxiety
level in HF patients. It also reduced the rate of hospitalization for HF patients.
However, the author did not present the methodology clearly. This greatly reduced the confidence of the study
results. This literature should not be considered in designing the evidence-based guideline.

64
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
2. de Souza, E.N., Rohde, L.E., Ruschel, K.B., Mussi, C.M., Beck-da-Silva, L., Biolo, A., Clausell, N. &
Rabelo-Silva, E.R. (2014). A nurse-based strategy reduces heart failure morbidity in patients admitted for
acute decompensated heart failure in Brazil: the HELEN- clinical trial. European Journal of Heart Failure,
16(9), 1002-1008.
Guideline topic: An Evidence-Based Home-Based
Intervention to Reduce Hospital Readmission Rate in
Patients with Heart Failure
Key Question No: Reviewer:
Cheung Shuk Man
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
P: patients admitted for acute decompensated HF in Brazil; I: nurse-based
strategy; O: reduce HF morbidity
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised.
Simple sequence randomization is used and the assignment list is
generated electronically.
Yes
Can’t say
No
1.3 An adequate concealment method is used.
Computerised allocation is used. A health care professional who is not a
member of the research group is responsible for the patient allocation list.
Yes
Can’t say
No
1.4 The design keeps subjects and investigators ‘blind’ about treatment allocation.
The intervention nurses are blinded to the patients’ allocation group.
Yes
Can’t say
No
1.5 The treatment and control groups are similar at the start of the trial.
p>0.05
Yes
Can’t say □
No
1.6 The only difference between groups is the treatment under investigation.
The only difference is that the intervention group has home visits and
telephone follow-ups.
Yes
Can’t say
No
1.7 All relevant outcomes are measured in a standard, valid and reliable way.
The primary outcome is based on the final 6-month visit and a review of
electronic records. When electronic records are not available, validation is
based on clinical discharge notes. HF knowledge is measured by a 14-item
questionnaire which is validated. Self-care skills are measured by
EHFScBS which is validated.
Yes
Can’t say
No
1.8 What percentage of the individuals or clusters recruited into each treatment arm of the study dropped out before the study was completed?
Total number of participants
who dropped out from the
study =9
The dropout rate
=9/252*100% =3.57%
which is acceptable.

65
1.9 All the subjects are analysed in the groups to which they were randomly allocated (often referred to as intention to treat analysis).
ITT is mentioned.
Yes
Can’t say
No
Does not apply
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
No site-specific data is given.
Yes
Can’t say
No
Does not apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++)
Acceptable (+)
Low quality (-)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the study intervention?
Yes
The sample size is adequate and its calculation is
mentioned with statistical power 90%. The
randomization and concealment methods are good. The
dropout rate is low.
As the methodology of the study is good, so it is
certain that the overall effect is due to the study
intervention.
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline?
Yes
The results are applicable to the patient group targeted
by this guideline.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question and mention any areas of uncertainty raised above.
The authors concluded that home-based intervention based on home visits and phone calls conducted by nurses
had meaningful reduction of HF morbidity, promoted a significant increase in HF knowledge and self-care
actions.
The study matched the topic of interest. The methodology used minimized the bias. Therefore, it is certain that
home-based intervention could reduce HF morbidity, hospital readmission, emergency room visits or all-cause
deaths.
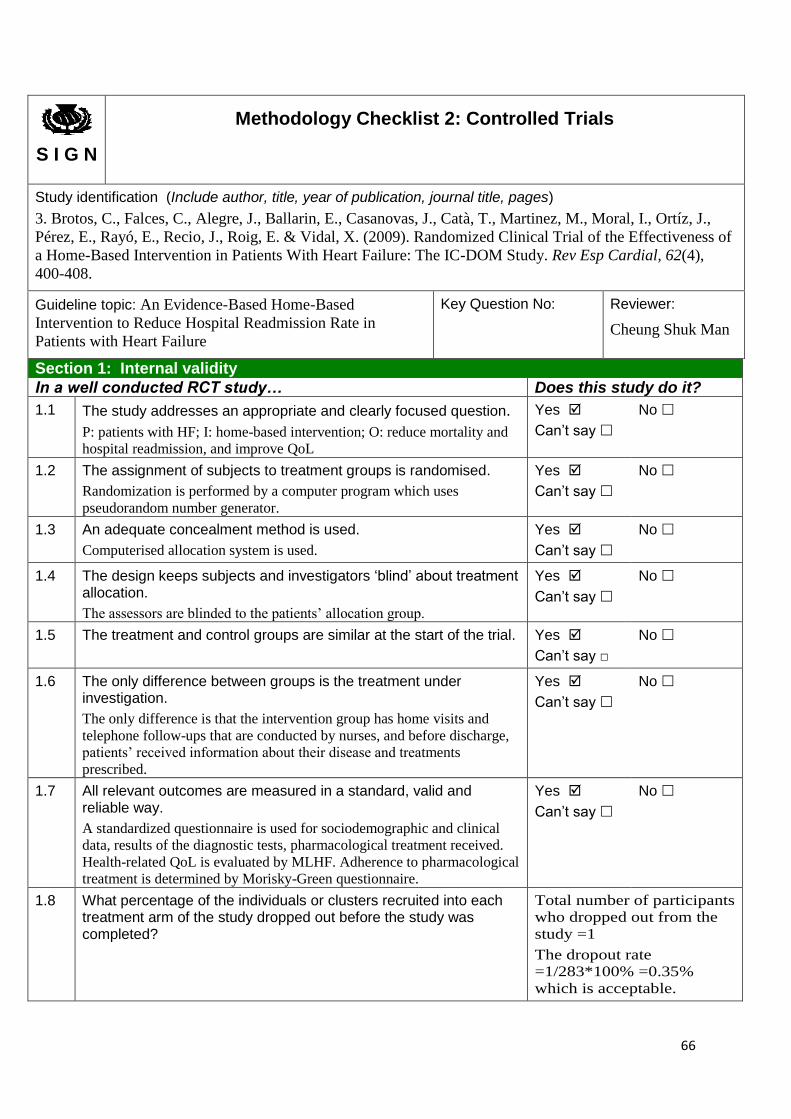
66
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
3. Brotos, C., Falces, C., Alegre, J., Ballarin, E., Casanovas, J., Catà, T., Martinez, M., Moral, I., Ortíz, J.,
Pérez, E., Rayó, E., Recio, J., Roig, E. & Vidal, X. (2009). Randomized Clinical Trial of the Effectiveness of
a Home-Based Intervention in Patients With Heart Failure: The IC-DOM Study. Rev Esp Cardial, 62(4),
400-408.
Guideline topic: An Evidence-Based Home-Based
Intervention to Reduce Hospital Readmission Rate in
Patients with Heart Failure
Key Question No: Reviewer:
Cheung Shuk Man
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
P: patients with HF; I: home-based intervention; O: reduce mortality and
hospital readmission, and improve QoL
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised.
Randomization is performed by a computer program which uses
pseudorandom number generator.
Yes
Can’t say
No
1.3 An adequate concealment method is used.
Computerised allocation system is used.
Yes
Can’t say
No
1.4 The design keeps subjects and investigators ‘blind’ about treatment allocation.
The assessors are blinded to the patients’ allocation group.
Yes
Can’t say
No
1.5 The treatment and control groups are similar at the start of the trial.
Yes
Can’t say □
No
1.6 The only difference between groups is the treatment under investigation.
The only difference is that the intervention group has home visits and
telephone follow-ups that are conducted by nurses, and before discharge,
patients’ received information about their disease and treatments
prescribed.
Yes
Can’t say
No
1.7 All relevant outcomes are measured in a standard, valid and reliable way.
A standardized questionnaire is used for sociodemographic and clinical
data, results of the diagnostic tests, pharmacological treatment received.
Health-related QoL is evaluated by MLHF. Adherence to pharmacological
treatment is determined by Morisky-Green questionnaire.
Yes
Can’t say
No
1.8 What percentage of the individuals or clusters recruited into each treatment arm of the study dropped out before the study was completed?
Total number of participants
who dropped out from the
study =1
The dropout rate
=1/283*100% =0.35%
which is acceptable.

67
1.9 All the subjects are analysed in the groups to which they were randomly allocated (often referred to as intention to treat analysis).
ITT is mentioned.
Yes
Can’t say
No
Does not apply
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
No site specific data is given.
Yes
Can’t say
No
Does not apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++)
Acceptable (+)
Low quality (-)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the study intervention?
Yes
Sample size calculation is mentioned with statistical
power of 80%. And the sample size is adequate.
Randomization and concealment method is good. The
drop-out rate is low. ITT is mentioned.
With rigor methodology, it is certain that the overall
effect is due to the study intervention.
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline?
Yes
The results are applicable to the patient group targeted
by this guideline.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question and mention any areas of uncertainty raised above.
The authors concluded that home-based intervention conducted by trained nursing professionals was effective
in reducing overall mortality and hospital readmissions for HF. It could also improve QoL, adherence to
therapy and satisfaction with the care received.
The study matched the topic of interest. The rigor methodology used minimized the bias. Therefore, it is
certain that home-based intervention could reduce overall mortality and hospital readmissions for HF.

68
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
4. Morcillo, C., Valderas, J.M., Aguado, O., Delás, J., Sort, D., Pujadas, R. & Rosell, F. (2005). Evaluation of
a Home-Based Intervention in Heart Failure Patients. Results of a Randomized Study. REV Esp Cardial,
58(6), 618-625.
Guideline topic: An Evidence-Based Home-Based
Intervention to Reduce Hospital Readmission Rate in
Patients with Heart Failure
Key Question No: Reviewer:
Cheung Shuk Man
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
P: HF patients; I: home-based intervention; O: readmission rate,
emergency department visits, healthcare costs
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised.
Randomization is performed by using a random number table, which is
not very good method.
Yes
Can’t say
No
1.3 An adequate concealment method is used.
No concealment method is reported.
Yes
Can’t say
No
1.4 The design keeps subjects and investigators ‘blind’ about treatment allocation.
The physicians implicated in assessment and follow up have no
knowledge of the assigned group.
Yes
Can’t say
No
1.5 The treatment and control groups are similar at the start of the trial.
p>0.05 for sociodemographic variables, comorbidity, function and
cardiological variables.
Yes
Can’t say □
No
1.6 The only difference between groups is the treatment under investigation.
The only difference is that the intervention group has a single home visit
by nurse.
Yes
Can’t say
No
1.7 All relevant outcomes are measured in a standard, valid and reliable way.
Patients’ perceived health is assessed by the use of SF-36 health
questionnaire (version 1.4).
Can’t say
No
1.8 What percentage of the individuals or clusters recruited into each treatment arm of the study dropped out before the study was completed?
Patients drop out in the assessment of impact on perceived health because
of inability to respond to the questionnaire by telephone, death of the
patients and refused to answer.
In the assessment of impact
on perceived health, number
of participants who dropped
out=19
The dropout rate
=19/70*100% =27.14%
which is not acceptable.
1.9 All the subjects are analysed in the groups to which they were randomly allocated (often referred to as intention to treat analysis).
ITT is not mentioned.
Yes
Can’t say
No
Does not apply

69
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
There is only one site.
Yes
Can’t say
No
Does not apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++)
Acceptable (+)
Low quality (-)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the study intervention?
Yes
It is a randomised controlled study. All analyses are
performed using the statistical significance level
considered for calculation of sample size (α=0.05).
Blinding was performed.
The methodology is acceptable. Therefore, it is certain
that the overall effect is due to the intervention.
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline?
Yes
The results are applicable to the patient group targeted
by this guideline.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question and mention any areas of uncertainty raised above.
The authors concluded that single home visit with no subsequent visits or monitoring by telephone follow-ups
could reduce the mean number of hospitalization and emergency room visits and reduce in costs and
improvement in patient perceived health.
However, the sample size was small and it was only conducted in a single site. This reduced the confidence of
the study results.
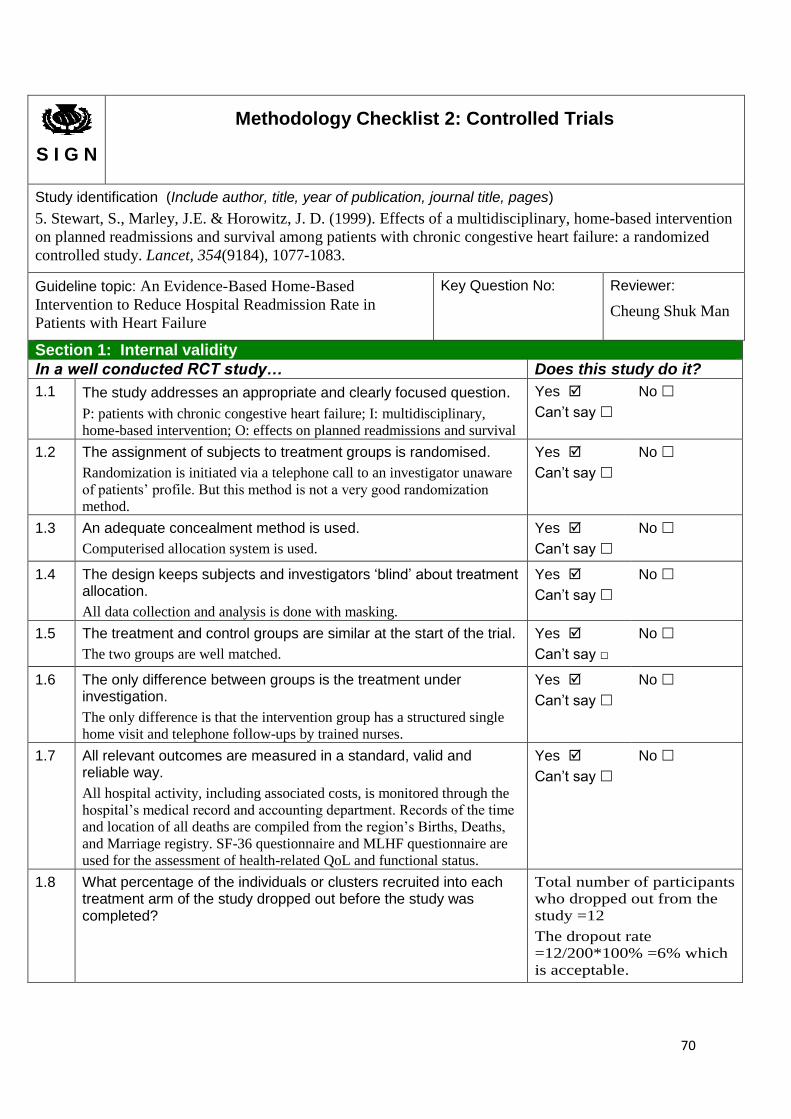
70
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
5. Stewart, S., Marley, J.E. & Horowitz, J. D. (1999). Effects of a multidisciplinary, home-based intervention
on planned readmissions and survival among patients with chronic congestive heart failure: a randomized
controlled study. Lancet, 354(9184), 1077-1083.
Guideline topic: An Evidence-Based Home-Based
Intervention to Reduce Hospital Readmission Rate in
Patients with Heart Failure
Key Question No: Reviewer:
Cheung Shuk Man
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
P: patients with chronic congestive heart failure; I: multidisciplinary,
home-based intervention; O: effects on planned readmissions and survival
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised.
Randomization is initiated via a telephone call to an investigator unaware
of patients’ profile. But this method is not a very good randomization
method.
Yes
Can’t say
No
1.3 An adequate concealment method is used.
Computerised allocation system is used.
Yes
Can’t say
No
1.4 The design keeps subjects and investigators ‘blind’ about treatment allocation.
All data collection and analysis is done with masking.
Yes
Can’t say
No
1.5 The treatment and control groups are similar at the start of the trial.
The two groups are well matched.
Yes
Can’t say □
No
1.6 The only difference between groups is the treatment under investigation.
The only difference is that the intervention group has a structured single
home visit and telephone follow-ups by trained nurses.
Yes
Can’t say
No
1.7 All relevant outcomes are measured in a standard, valid and reliable way.
All hospital activity, including associated costs, is monitored through the
hospital’s medical record and accounting department. Records of the time
and location of all deaths are compiled from the region’s Births, Deaths,
and Marriage registry. SF-36 questionnaire and MLHF questionnaire are
used for the assessment of health-related QoL and functional status.
Yes
Can’t say
No
1.8 What percentage of the individuals or clusters recruited into each treatment arm of the study dropped out before the study was completed?
Total number of participants
who dropped out from the
study =12
The dropout rate
=12/200*100% =6% which
is acceptable.

71
1.9 All the subjects are analysed in the groups to which they were randomly allocated (often referred to as intention to treat analysis).
All analyses are done by ITT.
Yes
Can’t say
No
Does not apply
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
There is only one site.
Yes
Can’t say
No
Does not apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++)
Acceptable (+)
Low quality (-)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the study intervention?
Yes
The sample size calculation is mentioned and the
sample size is adequate. Randomisation, concealment,
masking and ITT are used in the study.
With rigor methodology, it is certain that the overall
effect is due to the study intervention.
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline?
Yes
The results are applicable to the patient group targeted
by this guideline.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question and mention any areas of uncertainty raised above.
The authors concluded that home-based intervention was inexpensive. It improved the efficacy of
pharmacotherapy in limiting readmission to hospital and death in HF patients.
The methodology used is rigor. It minimized the bias. The sample is adequate. All these increased the
confidence of the study results.
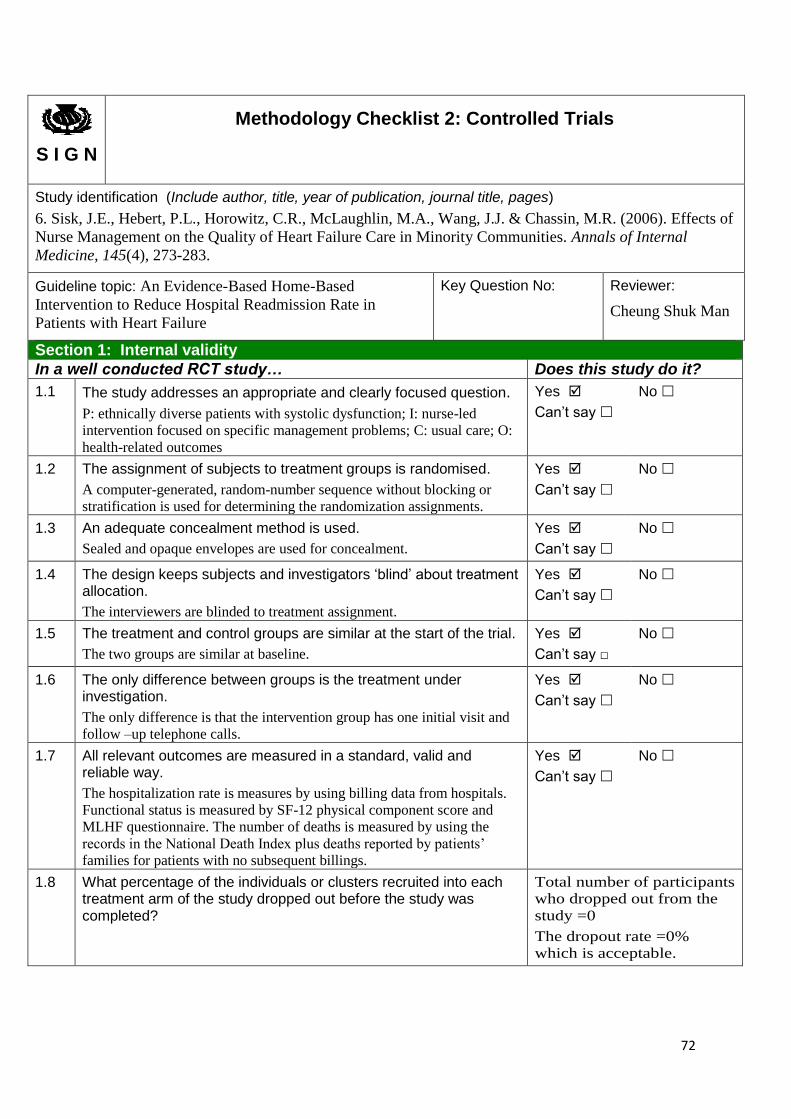
72
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
6. Sisk, J.E., Hebert, P.L., Horowitz, C.R., McLaughlin, M.A., Wang, J.J. & Chassin, M.R. (2006). Effects of
Nurse Management on the Quality of Heart Failure Care in Minority Communities. Annals of Internal
Medicine, 145(4), 273-283.
Guideline topic: An Evidence-Based Home-Based
Intervention to Reduce Hospital Readmission Rate in
Patients with Heart Failure
Key Question No: Reviewer:
Cheung Shuk Man
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
P: ethnically diverse patients with systolic dysfunction; I: nurse-led
intervention focused on specific management problems; C: usual care; O:
health-related outcomes
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised.
A computer-generated, random-number sequence without blocking or
stratification is used for determining the randomization assignments.
Yes
Can’t say
No
1.3 An adequate concealment method is used.
Sealed and opaque envelopes are used for concealment.
Yes
Can’t say
No
1.4 The design keeps subjects and investigators ‘blind’ about treatment allocation.
The interviewers are blinded to treatment assignment.
Yes
Can’t say
No
1.5 The treatment and control groups are similar at the start of the trial.
The two groups are similar at baseline.
Yes
Can’t say □
No
1.6 The only difference between groups is the treatment under investigation.
The only difference is that the intervention group has one initial visit and
follow –up telephone calls.
Yes
Can’t say
No
1.7 All relevant outcomes are measured in a standard, valid and reliable way.
The hospitalization rate is measures by using billing data from hospitals.
Functional status is measured by SF-12 physical component score and
MLHF questionnaire. The number of deaths is measured by using the
records in the National Death Index plus deaths reported by patients’
families for patients with no subsequent billings.
Yes
Can’t say
No
1.8 What percentage of the individuals or clusters recruited into each treatment arm of the study dropped out before the study was completed?
Total number of participants
who dropped out from the
study =0
The dropout rate =0%
which is acceptable.

73
1.9 All the subjects are analysed in the groups to which they were randomly allocated (often referred to as intention to treat analysis).
ITT is mentioned.
Yes
Can’t say
No
Does not apply
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
No site-specific data is given.
Yes
Can’t say
No
Does not apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++)
Acceptable (+)
Low quality (-)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the study intervention?
Yes
Sample size calculation is mentioned with level of
significance 5% and statistical power 80% noted. The
randomization and concealment methods are good. ITT
is used and no participants dropped out from the study.
Therefore, it is certain that the overall effect is due to
the study intervention.
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline?
Yes
The results are applicable to the patient group targeted
by this guideline.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question and mention any areas of uncertainty raised above.
The authors concluded that a nurse management strategy could reduce the rate of hospitalization and improve
patients’ functioning. The diversity of the hospitals, practices and patients enhanced the generalizability of the
results.
The study is conducted at multicenter. The sample size is adequate. Also, the methodology is rigor. All these
increase the certainty and confidence of using the results of the study.
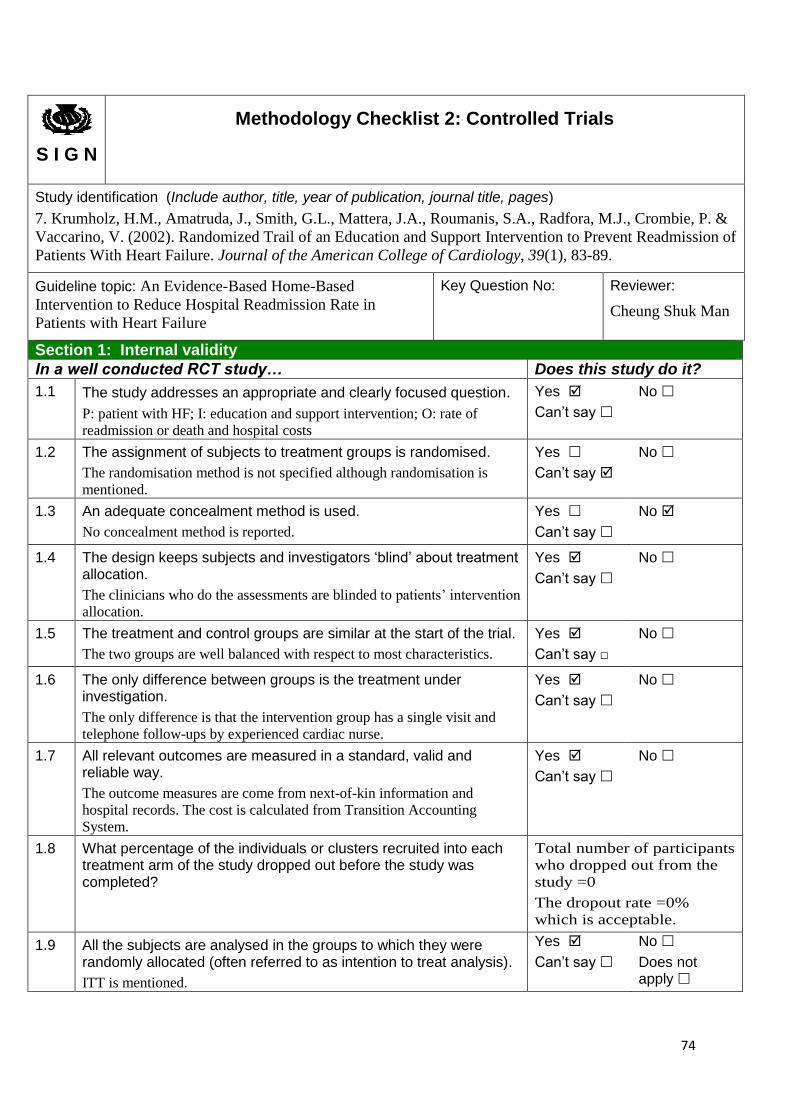
74
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
7. Krumholz, H.M., Amatruda, J., Smith, G.L., Mattera, J.A., Roumanis, S.A., Radfora, M.J., Crombie, P. &
Vaccarino, V. (2002). Randomized Trail of an Education and Support Intervention to Prevent Readmission of
Patients With Heart Failure. Journal of the American College of Cardiology, 39(1), 83-89.
Guideline topic: An Evidence-Based Home-Based
Intervention to Reduce Hospital Readmission Rate in
Patients with Heart Failure
Key Question No: Reviewer:
Cheung Shuk Man
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
P: patient with HF; I: education and support intervention; O: rate of
readmission or death and hospital costs
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised.
The randomisation method is not specified although randomisation is
mentioned.
Yes
Can’t say
No
1.3 An adequate concealment method is used.
No concealment method is reported.
Yes
Can’t say
No
1.4 The design keeps subjects and investigators ‘blind’ about treatment allocation.
The clinicians who do the assessments are blinded to patients’ intervention
allocation.
Yes
Can’t say
No
1.5 The treatment and control groups are similar at the start of the trial.
The two groups are well balanced with respect to most characteristics.
Yes
Can’t say □
No
1.6 The only difference between groups is the treatment under investigation.
The only difference is that the intervention group has a single visit and
telephone follow-ups by experienced cardiac nurse.
Yes
Can’t say
No
1.7 All relevant outcomes are measured in a standard, valid and reliable way.
The outcome measures are come from next-of-kin information and
hospital records. The cost is calculated from Transition Accounting
System.
Yes
Can’t say
No
1.8 What percentage of the individuals or clusters recruited into each treatment arm of the study dropped out before the study was completed?
Total number of participants
who dropped out from the
study =0
The dropout rate =0%
which is acceptable.
1.9 All the subjects are analysed in the groups to which they were randomly allocated (often referred to as intention to treat analysis).
ITT is mentioned.
Yes
Can’t say
No
Does not apply

75
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
There is only one site.
Yes
Can’t say
No
Does not apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++)
Acceptable (+)
Low quality (-)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the study intervention?
Yes
Sample size calculation is not mentioned and the
sample size is not adequate. Randomization and
concealment methods are not clearly stated. However,
The study has blinding. ITT is mentioned and zero
drop-out rate is noted.
The methodology is acceptable. So, it is certain that the
overall effect is due to the study intervention.
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline?
Yes
The results are applicable to the patient group targeted
by this guideline.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question and mention any areas of uncertainty raised above.
The authors concluded that education and support could reduce poor outcomes and cost of health care.
However, the study is single center. The sample size is small. These reduce the confidence of the study results.
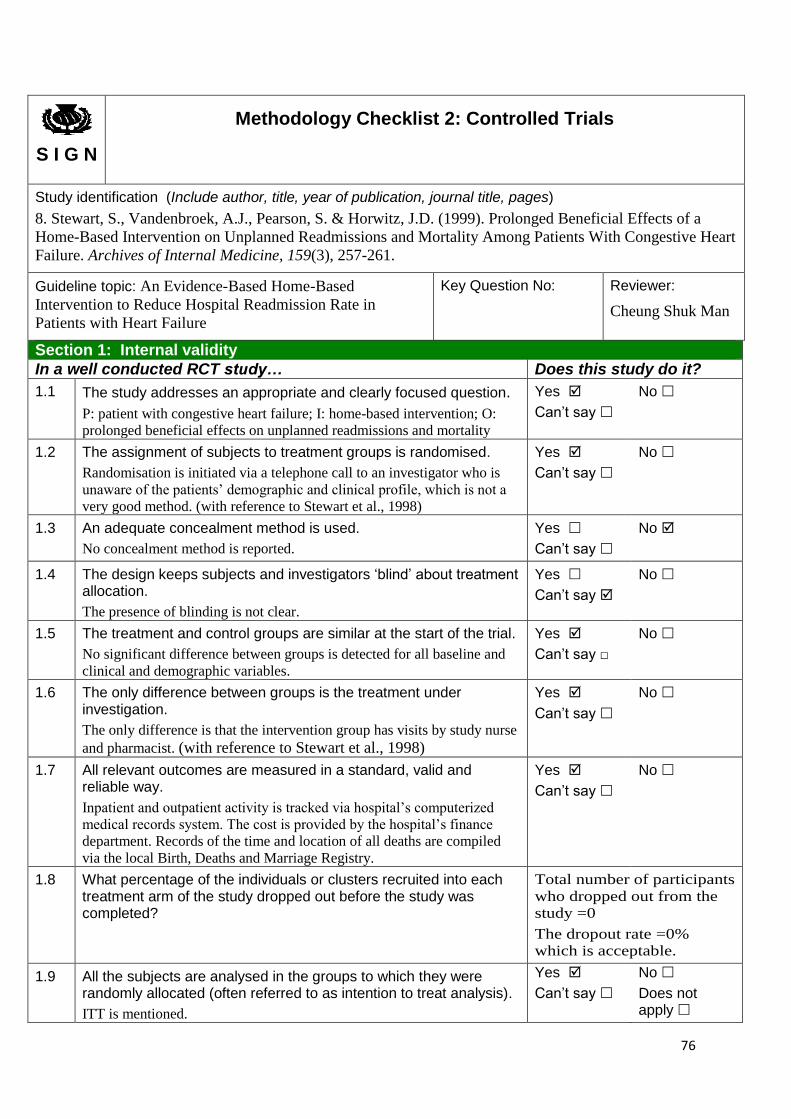
76
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
8. Stewart, S., Vandenbroek, A.J., Pearson, S. & Horwitz, J.D. (1999). Prolonged Beneficial Effects of a
Home-Based Intervention on Unplanned Readmissions and Mortality Among Patients With Congestive Heart
Failure. Archives of Internal Medicine, 159(3), 257-261.
Guideline topic: An Evidence-Based Home-Based
Intervention to Reduce Hospital Readmission Rate in
Patients with Heart Failure
Key Question No: Reviewer:
Cheung Shuk Man
Section 1: Internal validity
In a well conducted RCT study… Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
P: patient with congestive heart failure; I: home-based intervention; O:
prolonged beneficial effects on unplanned readmissions and mortality
Yes
Can’t say
No
1.2 The assignment of subjects to treatment groups is randomised.
Randomisation is initiated via a telephone call to an investigator who is
unaware of the patients’ demographic and clinical profile, which is not a
very good method. (with reference to Stewart et al., 1998)
Yes
Can’t say
No
1.3 An adequate concealment method is used.
No concealment method is reported.
Yes
Can’t say
No
1.4 The design keeps subjects and investigators ‘blind’ about treatment allocation.
The presence of blinding is not clear.
Yes
Can’t say
No
1.5 The treatment and control groups are similar at the start of the trial.
No significant difference between groups is detected for all baseline and
clinical and demographic variables.
Yes
Can’t say □
No
1.6 The only difference between groups is the treatment under investigation.
The only difference is that the intervention group has visits by study nurse
and pharmacist. (with reference to Stewart et al., 1998)
Yes
Can’t say
No
1.7 All relevant outcomes are measured in a standard, valid and reliable way.
Inpatient and outpatient activity is tracked via hospital’s computerized
medical records system. The cost is provided by the hospital’s finance
department. Records of the time and location of all deaths are compiled
via the local Birth, Deaths and Marriage Registry.
Yes
Can’t say
No
1.8 What percentage of the individuals or clusters recruited into each treatment arm of the study dropped out before the study was completed?
Total number of participants
who dropped out from the
study =0
The dropout rate =0%
which is acceptable.
1.9 All the subjects are analysed in the groups to which they were randomly allocated (often referred to as intention to treat analysis).
ITT is mentioned.
Yes
Can’t say
No
Does not apply

77
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
There is only one site.
Yes
Can’t say
No
Does not apply
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++)
Acceptable (+)
Low quality (-)
Unacceptable – reject 0
2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, are you certain that the overall effect is due to the study intervention?
Yes
Randomization method and ITT are mentioned in the
study. The study takes 2% for the level of significance
and it has zero drop-out rate. These enhanced the
certainty that the overall effect of the study id due to
the intervention.
2.3 Are the results of this study directly applicable to the patient group targeted by this guideline?
Yes
The results are applicable to the patient group targeted
by this guideline.
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of the study, and the extent to which it answers your question and mention any areas of uncertainty raised above.
The authors concluded that the results of the extended follow up demonstrated continued benefit in regard to
the primary end point of frequency of unplanned readmissions plus out-of-hospital deaths.
The sample size is small and its calculation is not mentioned. Also, the study is conducted in a single site.
However, the length of follow up is long.

78
Appendix 7
Potential cost
Assuming there are 180 HF patients and the median hourly paid for a registered nurse is
HK$200.
Manpower Amount of time Estimated
cost (HK$)
Training session for
home visit
1 nurse trainer,
1 nurse trainee
2 hours 2 x 2 x 200
=800
Training session for
telephone follow-
ups
1 nurse trainer,
2 nurse trainees
1 hour 3 x 1 x 200
=600
Home visit 1 nurse 2 hours for each patient
Total =180 patients x 2 hours
=360 hours
360 x 200
=72,000
Telephone follow-
ups
2 nurses 15 minutes for each patient, each
patient receives 2 telephone
follow-ups
Total =180 patients x15 minutes x
2
= 5400 minutes =90 hours
90 x 200
=18,000
Total cost for manpower annually 91,400
Total cost for the innovation annually = HK$ (60+91,400) =HK$91,460
The cost for each HF patient will be = HK$(91,460/180) ≈HK$508
Resources Amount Estimated
cost (HK$)
Paper 1 fold (500 sheets) 30
File 1 30
Total cost for resources annually 60

79
Appendix 8
Grades of recommendations
The Scottish Intercollegiate Guidelines Network (SIGN) Grading System
A At least one meta-analysis, systematic review, or RCT rated as 1++, and directly
applicable to the target population; or
A body of evidence consisting principally of studies rated as 1+, directly
applicable to the target population, and demonstrating overall consistency of
results
B A body of evidence including studies rated as 2++, directly applicable to the
target population, and demonstrating overall consistency of results; or
Extrapolated evidence from studies rated as 1++ or 1+
C A body of evidence including studies rated as 2+, directly applicable to the
target population and demonstrating overall consistency of results; or
Extrapolated evidence from studies rated as 2++
D Evidence level 3 or 4; or
Extrapolated evidence from studies rated as 2+
(SIGN, 2008)

80
Appendix 9
Evidence-based practice guideline
Title:
An evidence-based practice protocol of home-based intervention for heart failure (HF) patients
Clinical issue:
With the aging population in Hong Kong and the fact that incidence and mortality rate
of HF increase with age, more people are at risk of developing and suffering from HF.
When HF patients are hospitalized, their conditions are monitored by nurses. However,
when they are discharged, monitoring by nurses is discontinued. No one will guarantee that
they will follow the instructions that were taught in hospitals. Poor compliance to treatment
regimen leads to readmission. Therefore, in order to reduce HF patients’ readmission rate, there
is a need for developing an evidence-based protocol for monitoring their condition and
providing care for them after they are discharged.
Aim:
1. To provide evidence-based recommendations for nurses in the management of HF patients.
2. To standardize nursing care for the discharged HF patients.
Objectives:
1. To implement home-based intervention for HF patients.
2. To reduce readmission rate in HF patients.
Guideline users:
For nurses who are working in medical units under Hospital Authority.
Target participants:
Adult patients who are admitted to the targeted medical ward with the primary or secondary
diagnosis as HF.
81
Recommendations
Recommendation 1
A home-based intervention should be implemented for HF patients when they are
discharged. (Grade A)
Evidence:
Home-based intervention showed both positive effect and statistical significance in the
reduction of hospital readmission rate when compared with the usual care group (Sisk et al.,
2006; Stewart et al., 1999) (1++); (Morcillo et al., 2009; Stewart et al., 1999) (1+);
(Tsuchihashi-Makaya et al., 2013) (1-).
Recommendation 2
The home-based intervention should include both home visits and telephone follow-ups.
(Grade A)
Evidence:
Among the five studies that showed both positive effect and statistical significance in
the reduction of hospital readmission rate, four of them included both home visits and
telephone follow-ups as their intervention (Sisk et al., 2006; Stewart et al., 1999) (1++);
(Stewart et al., 1999) (1+); (Tsuchihashi-Makaya et al., 2013) (1-).
Recommendation 3 – home visit
Recommendation 3.1
A 2-hour single home visit should be conducted within 7 to 14 days after the HF patient
is discharged. (Grade A)
Evidence:
A single home visit will be appropriate for the intervention (Sisk et al., 2006;) (1++);

82
(Morcillo et al., 2009; Stewart et al., 1999) (1+). It has to be conducted between Day 7 to Day
14 after the patient is discharged (Stewart et al., 1999) (1++); (Stewart et al., 1999) (1+);
(Tsuchihashi-Makaya et al., 2013) (1-). This can help to detect any early decompensation
(Morcillo et al., 2009) (1+). And the duration is within 2 hours (Stewart et al., 1999) (1++);
(Morcillo et al., 2009) (1+).
Recommendation 3.2
The home visit should include the following elements:
-assessment on patients’ health status and adherence to the treatment regimen
-education about the disease and symptoms
-physical examination
-involvement of caregivers
(Grade A)
Evidence:
During home visit, the nurse has to assess patients’ health status and their adherence to
the recommendations (Stewart et al., 1999) (1++); (Morcillo et al., 2009) (1+); (Tsuchihashi-
Makaya et al., 2013) (1-). The nurse has to educate the patients about the disease and its signs
and symptoms (Sisk et al., 2006) (1++). A physical examination has to be conducted during
home visit for assessing patients’ physical condition (Stewart et al., 1999) (1++); (Morcillo et
al., 2009) (1+). Caregivers may also be included during the home visit (Stewart et al., 1999)
(1++); (Morcillo et al., 2009; Stewart et al., 1999) (1+).
Recommendation 4 – telephone follow-ups
Recommendation 4.1
Telephone follow-ups should be conducted every 3 month. (Grade A)
Evidence:
83
The telephone follow-ups for the intervention have to be conducted at the 3rd month
and the 6th month after the patient is discharged (Stewart et al., 1999) (1++).
Recommendation 4.2
The contents of telephone follow-ups should include the following:
-monitoring patients’ progress and symptoms
-reinforcing the adherence on recommendations
(Grade A)
Evidence:
Monitoring patients’ progress was one of the contents in the telephone follow-ups in
the reviewed studies (Sisk et al., 2006; Stewart et al., 1999) (1++); (Tsuchihashi-Makaya et al.,
2013) (1-). Reinforcement on the adherence to treatment regimen has to be given during
telephone follow-ups (Sisk et al., 2006) (1++); (Stewart et al., 1999) (1+).
Recommendation 4.3
Patients should be encouraged to contact the nurse if any problem arose. (Grade A)
Evidence:
Patients can contact their nurses if they have encountered problems (Stewart et al., 1999)
(1++).
Recommendation 5
Primary physician or cardiologist should be consulted when the patient requires medical
review. (Grade A)
Evidence:
It is recommended that nurses have to contact patients’ primary physician or
cardiologist if there is a need for a new treatment or modifying the existing one (Sisk et al.,
2006; Stewart et al., 1999) (1++); (Stewart et al., 1999) (1+); (Tsuchihashi-Makaya et al., 2013)

84
(1-).
Recommendation 6
The total length of follow-up should be 6 months. (Grade A)
Evidence:
The studies that used 6 months as their length of follow up showed greater effect size
(Stewart et al., 1999) (1++); (Morcillo et al., 2009) (1+).

85
Appendix 10
Timeline of the pilot study
Week number 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Training and briefing session ✔
Recruitment of patients ✔ ✔ ✔ ✔
Intervention ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔ ✔
Evaluation ✔ ✔
Refinement of protocol ✔
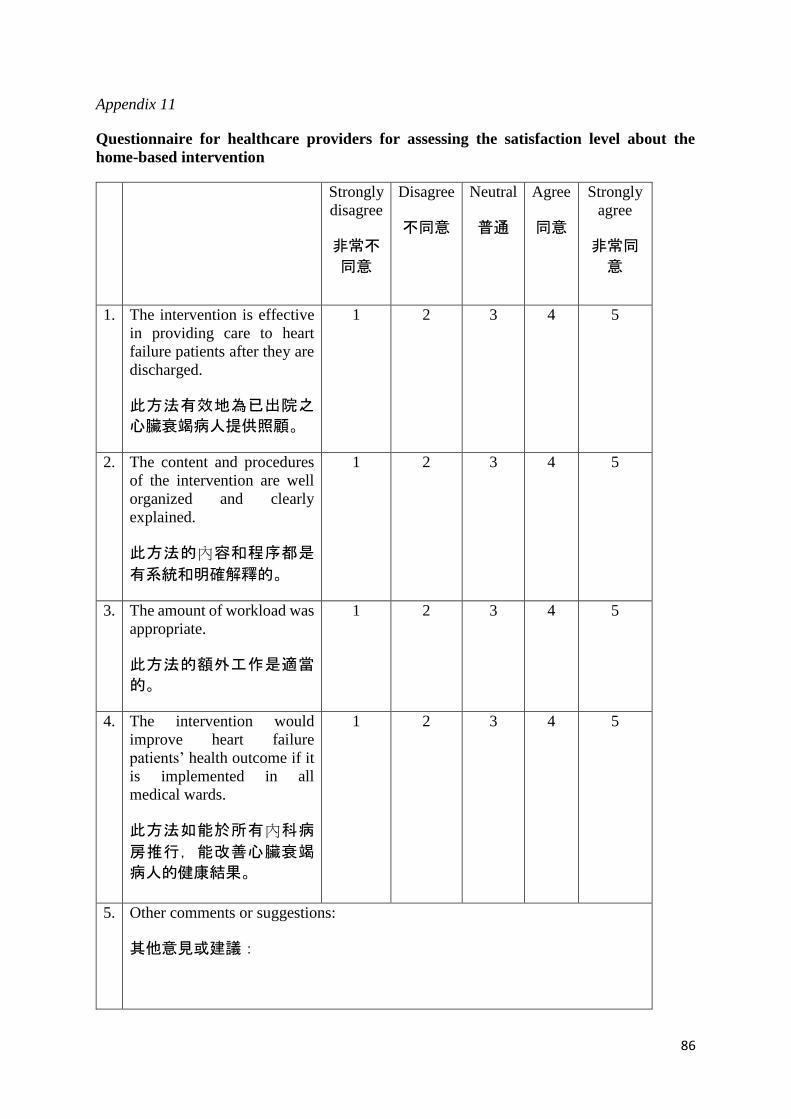
86
Appendix 11
Questionnaire for healthcare providers for assessing the satisfaction level about the
home-based intervention
Strongly
disagree
非常不
同意
Disagree
不同意
Neutral
普通
Agree
同意
Strongly
agree
非常同
意
1. The intervention is effective
in providing care to heart
failure patients after they are
discharged.
此方法有效地為已出院之
心臟衰竭病人提供照顧。
1 2 3 4 5
2. The content and procedures
of the intervention are well
organized and clearly
explained.
此方法的內容和程序都是
有系統和明確解釋的。
1 2 3 4 5
3. The amount of workload was
appropriate.
此方法的額外工作是適當
的。
1 2 3 4 5
4. The intervention would
improve heart failure
patients’ health outcome if it
is implemented in all
medical wards.
此方法如能於所有內科病
房推行,能改善心臟衰竭
病人的健康結果。
1 2 3 4 5
5. Other comments or suggestions:
其他意見或建議:
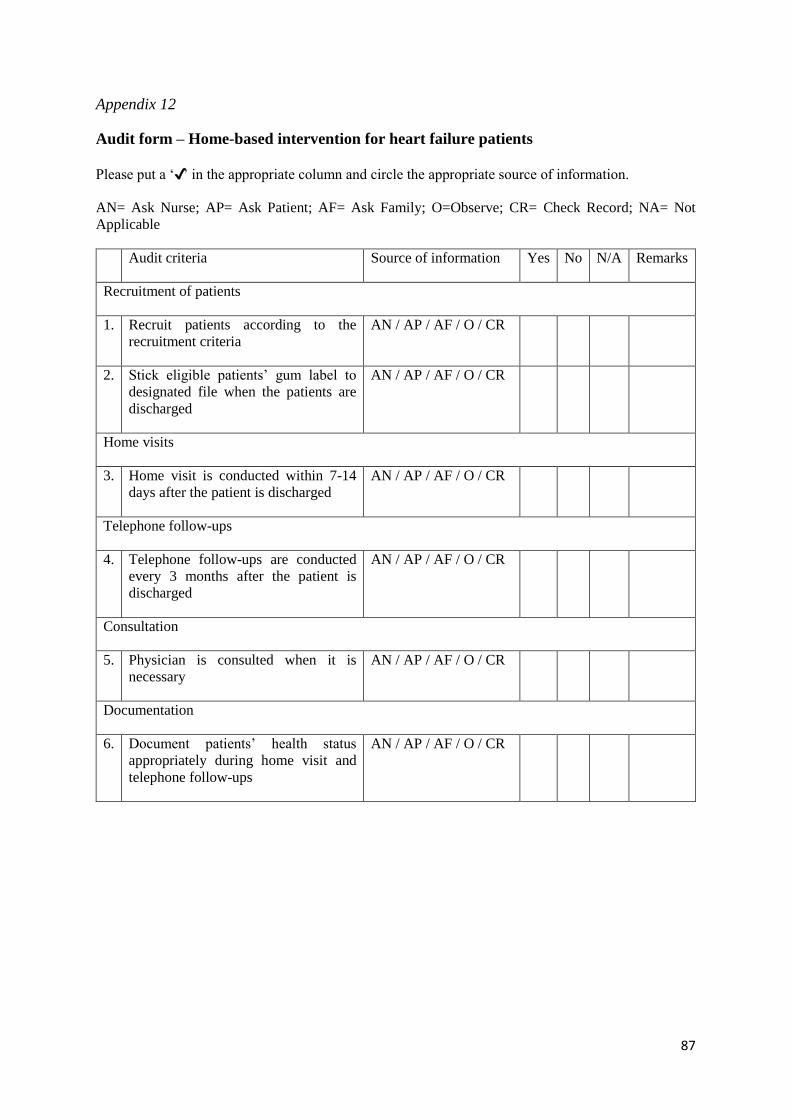
87
Appendix 12
Audit form – Home-based intervention for heart failure patients
Please put a ‘✔’ in the appropriate column and circle the appropriate source of information.
AN= Ask Nurse; AP= Ask Patient; AF= Ask Family; O=Observe; CR= Check Record; NA= Not
Applicable
Audit criteria Source of information Yes No N/A Remarks
Recruitment of patients
1. Recruit patients according to the
recruitment criteria
AN / AP / AF / O / CR
2. Stick eligible patients’ gum label to
designated file when the patients are
discharged
AN / AP / AF / O / CR
Home visits
3. Home visit is conducted within 7-14
days after the patient is discharged
AN / AP / AF / O / CR
Telephone follow-ups
4. Telephone follow-ups are conducted
every 3 months after the patient is
discharged
AN / AP / AF / O / CR
Consultation
5. Physician is consulted when it is
necessary
AN / AP / AF / O / CR
Documentation
6. Document patients’ health status
appropriately during home visit and
telephone follow-ups
AN / AP / AF / O / CR

88
Appendix 13
Questionnaire for patients for assessing the satisfaction level about the home-based
intervention
Strongly
disagree
非常不
同意
Disagree
不同意
Neutral
普通
Agree
同意
Strongly
agree
非常同意
1. The content of home visit and
telephone follow-ups is easy to
understand.
家居探訪和電話聯系的內容都
是容易明白的。
1 2 3 4 5
2. The length of time of home visit
and telephone follow-ups is
appropriate.
家居探訪和電話聯系的時間長
度是適當的。
1 2 3 4 5
3. The intervention could meet your
needs.
此方法能滿足您的需求。
1 2 3 4 5
4. The intervention could help to
improve your health outcomes.
此方法能改善您的健康結果。
1 2 3 4 5
5. Other comments or suggestions:
其他意見或建議:
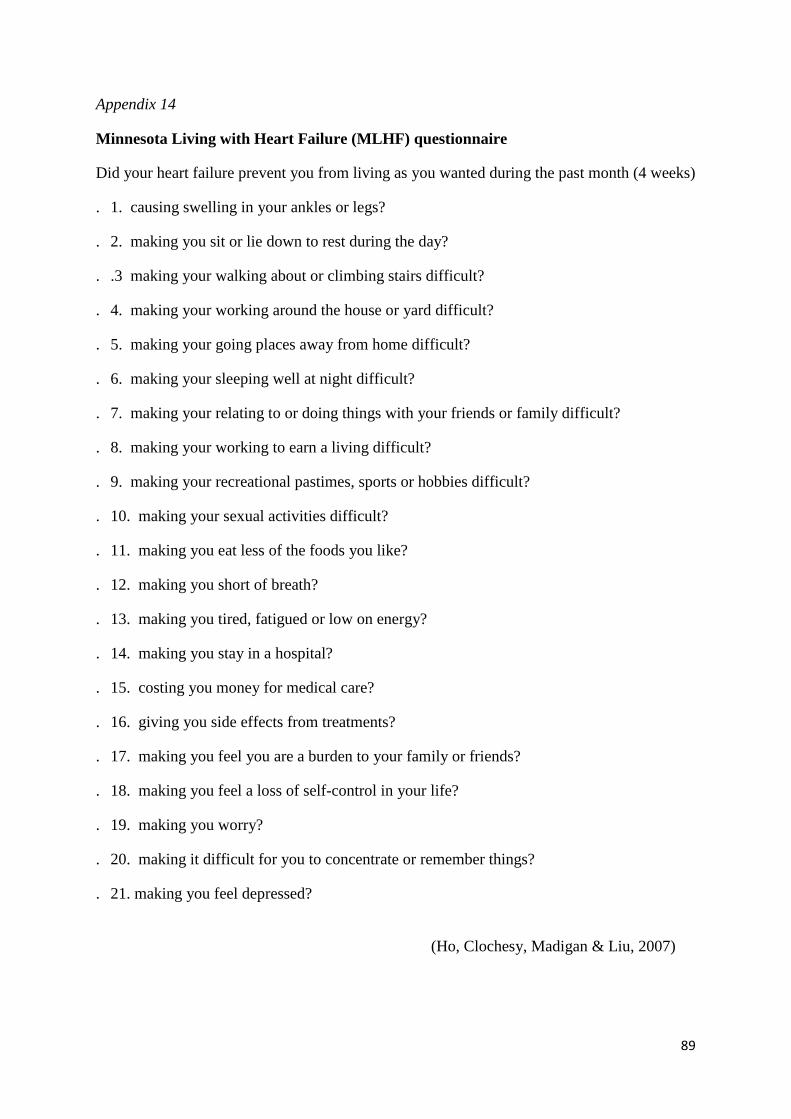
89
Appendix 14
Minnesota Living with Heart Failure (MLHF) questionnaire
Did your heart failure prevent you from living as you wanted during the past month (4 weeks)
. 1. causing swelling in your ankles or legs?
. 2. making you sit or lie down to rest during the day?
. .3 making your walking about or climbing stairs difficult?
. 4. making your working around the house or yard difficult?
. 5. making your going places away from home difficult?
. 6. making your sleeping well at night difficult?
. 7. making your relating to or doing things with your friends or family difficult?
. 8. making your working to earn a living difficult?
. 9. making your recreational pastimes, sports or hobbies difficult?
. 10. making your sexual activities difficult?
. 11. making you eat less of the foods you like?
. 12. making you short of breath?
. 13. making you tired, fatigued or low on energy?
. 14. making you stay in a hospital?
. 15. costing you money for medical care?
. 16. giving you side effects from treatments?
. 17. making you feel you are a burden to your family or friends?
. 18. making you feel a loss of self-control in your life?
. 19. making you worry?
. 20. making it difficult for you to concentrate or remember things?
. 21. making you feel depressed?
(Ho, Clochesy, Madigan & Liu, 2007)
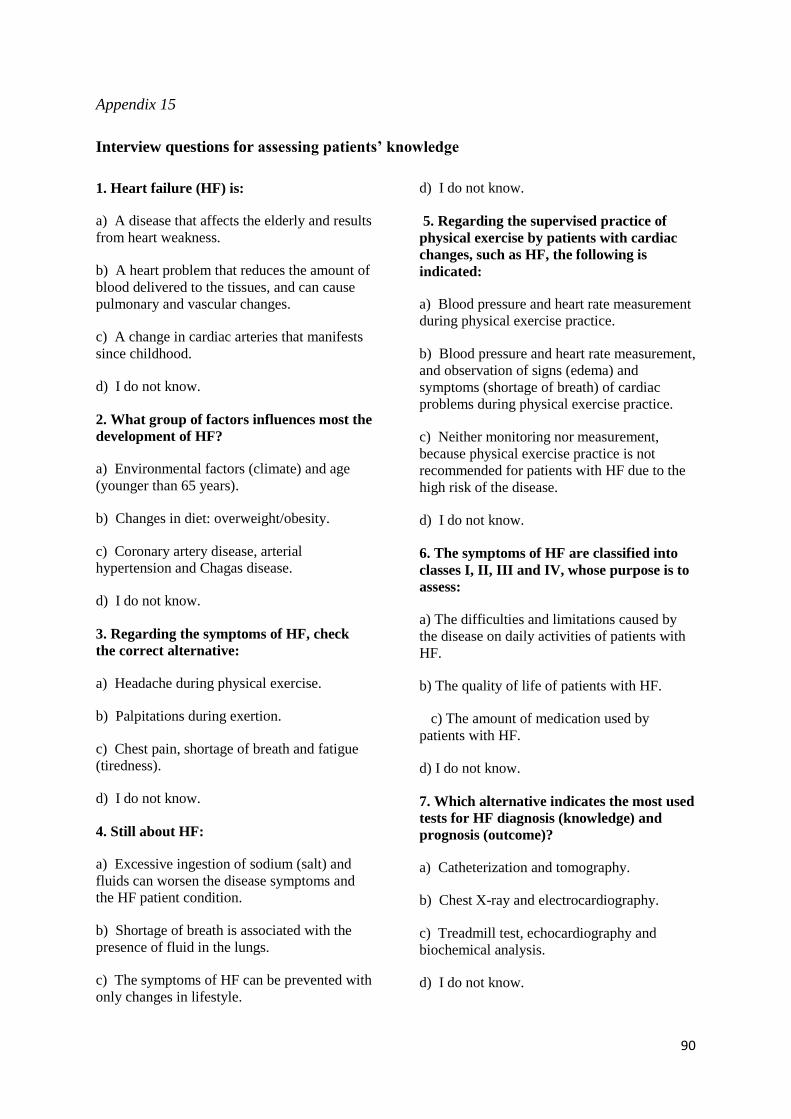
90
Appendix 15
Interview questions for assessing patients’ knowledge
1. Heart failure (HF) is:
a) A disease that affects the elderly and results
from heart weakness.
b) A heart problem that reduces the amount of
blood delivered to the tissues, and can cause
pulmonary and vascular changes.
c) A change in cardiac arteries that manifests
since childhood.
d) I do not know.
2. What group of factors influences most the
development of HF?
a) Environmental factors (climate) and age
(younger than 65 years).
b) Changes in diet: overweight/obesity.
c) Coronary artery disease, arterial
hypertension and Chagas disease.
d) I do not know.
3. Regarding the symptoms of HF, check
the correct alternative:
a) Headache during physical exercise.
b) Palpitations during exertion.
c) Chest pain, shortage of breath and fatigue
(tiredness).
d) I do not know.
4. Still about HF:
a) Excessive ingestion of sodium (salt) and
fluids can worsen the disease symptoms and
the HF patient condition.
b) Shortage of breath is associated with the
presence of fluid in the lungs.
c) The symptoms of HF can be prevented with
only changes in lifestyle.
d) I do not know.
5. Regarding the supervised practice of
physical exercise by patients with cardiac
changes, such as HF, the following is
indicated:
a) Blood pressure and heart rate measurement
during physical exercise practice.
b) Blood pressure and heart rate measurement,
and observation of signs (edema) and
symptoms (shortage of breath) of cardiac
problems during physical exercise practice.
c) Neither monitoring nor measurement,
because physical exercise practice is not
recommended for patients with HF due to the
high risk of the disease.
d) I do not know.
6. The symptoms of HF are classified into
classes I, II, III and IV, whose purpose is to
assess:
a) The difficulties and limitations caused by
the disease on daily activities of patients with
HF.
b) The quality of life of patients with HF.
c) The amount of medication used by
patients with HF.
d) I do not know.
7. Which alternative indicates the most used
tests for HF diagnosis (knowledge) and
prognosis (outcome)?
a) Catheterization and tomography.
b) Chest X-ray and electrocardiography.
c) Treadmill test, echocardiography and
biochemical analysis.
d) I do not know.
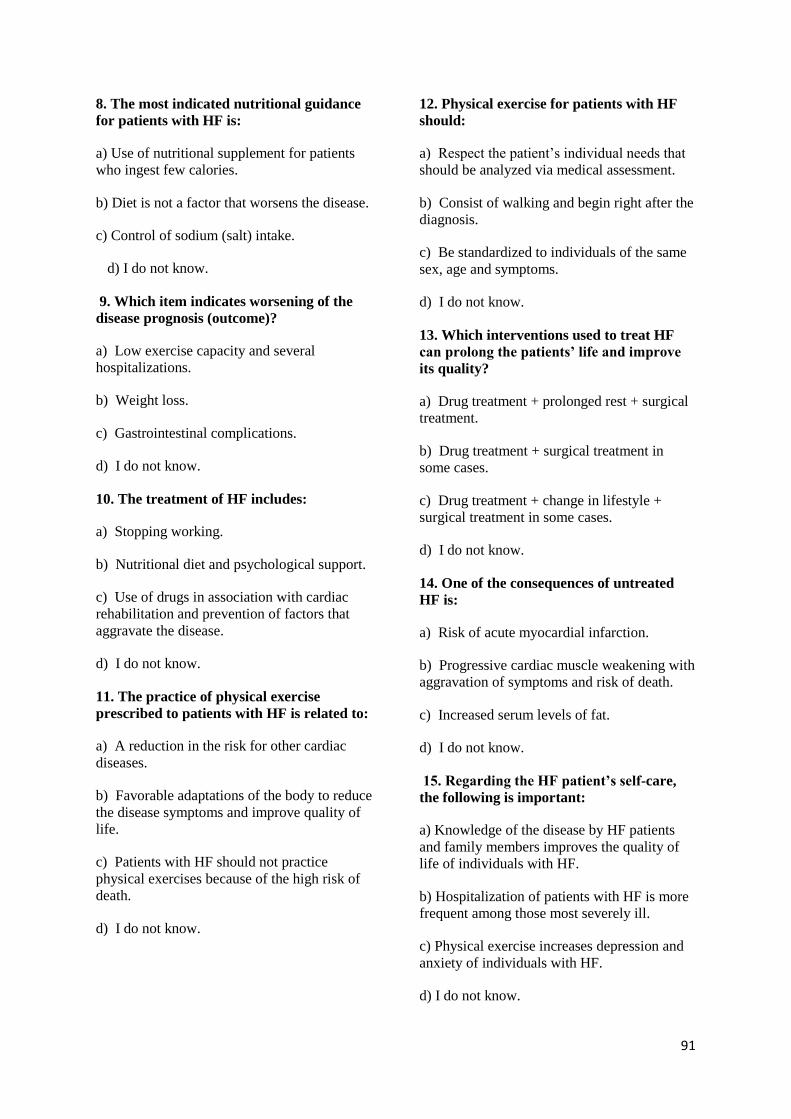
91
8. The most indicated nutritional guidance
for patients with HF is:
a) Use of nutritional supplement for patients
who ingest few calories.
b) Diet is not a factor that worsens the disease.
c) Control of sodium (salt) intake.
d) I do not know.
9. Which item indicates worsening of the
disease prognosis (outcome)?
a) Low exercise capacity and several
hospitalizations.
b) Weight loss.
c) Gastrointestinal complications.
d) I do not know.
10. The treatment of HF includes:
a) Stopping working.
b) Nutritional diet and psychological support.
c) Use of drugs in association with cardiac
rehabilitation and prevention of factors that
aggravate the disease.
d) I do not know.
11. The practice of physical exercise
prescribed to patients with HF is related to:
a) A reduction in the risk for other cardiac
diseases.
b) Favorable adaptations of the body to reduce
the disease symptoms and improve quality of
life.
c) Patients with HF should not practice
physical exercises because of the high risk of
death.
d) I do not know.
12. Physical exercise for patients with HF
should:
a) Respect the patient’s individual needs that
should be analyzed via medical assessment.
b) Consist of walking and begin right after the
diagnosis.
c) Be standardized to individuals of the same
sex, age and symptoms.
d) I do not know.
13. Which interventions used to treat HF
can prolong the patients’ life and improve
its quality?
a) Drug treatment + prolonged rest + surgical
treatment.
b) Drug treatment + surgical treatment in
some cases.
c) Drug treatment + change in lifestyle +
surgical treatment in some cases.
d) I do not know.
14. One of the consequences of untreated
HF is:
a) Risk of acute myocardial infarction.
b) Progressive cardiac muscle weakening with
aggravation of symptoms and risk of death.
c) Increased serum levels of fat.
d) I do not know.
15. Regarding the HF patient’s self-care,
the following is important:
a) Knowledge of the disease by HF patients
and family members improves the quality of
life of individuals with HF.
b) Hospitalization of patients with HF is more
frequent among those most severely ill.
c) Physical exercise increases depression and
anxiety of individuals with HF.
d) I do not know.

92
16. The recommendation of physical
exercise for patients with HF should
include:
a) Aerobic exercise (walking) associated with
resistance exercise (muscle strengthening), in
addition to stretching.
b) Stretching exercise associated with
flexibility exercise.
c) Localized exercise for weight reduction.
d) I do not know.
17. What are the possible side effects of
drugs used to treat HF?
a) Arterial hypotension (decrease in blood
pressure) and sexual dysfunction.
b) Cough and dehydration.
c) Dermatitis (skin disease) and intestinal
disorders.
d) I do not know.
18. What should someone with HF know?
a) Individuals with HF have depression, and
psychological support is recommended.
b) Knowing about the disease helps people to
identify HF signs and symptoms.
c) Follow-up and treatment of non-cardiac
diseases, such as diabetes, are not important to
the health of HF patients.
d) I do not know.
19. What drugs can be used in the
treatment of HF?
a) Diuretics (furosemide, lasix and
hydrochlorothiazide).
b) Angiotesin-converting enzyme inhibitors
(ACEI), suh as captopril and enalapril; beta-
blockers (carvedilol, propranolol, atenolol,
selozok and nebivolol); diuretics (furosemide,
lasix and hydrochlorothiazide).
c) Nitrates (isordil and monocordil).
d) I do not know
(Bonin et al., 2014)

93