abstract - eric - education resources information … · field test ii iii iv introduction 1 format...
TRANSCRIPT

ED 122 031
TITLE
INST I TUT ION
SPONS AGENCY
PUB LUCEGRANTNOTE
EDRS PRICEI DESCRIPTORS
DOCUMENT RESUME
EC 150.1
Screening and Assessment Tools: A Manual QiscussingAppropriate Tools for Use in the Home Setting.Ohio State Univ., Columbus. Herschel W. Nisonger
6Center.Health Resources Administration (DHHS/PHS), Bethesda,Md. Div. of Associated Health Professicins.802D12AH00135-0766p.
MF01/PC03 Plus Postage.!rDevelopmental Disabilities; *Evaluation Methods;Home Visits; Infants; *Screening Tests; *StudentEvaluation; Testing; goung Children
ABSTRACTThe manual describes seven tools for use in screening
ind :assessing the developmentally disabled infant and young child inthe home. Instruments are said to have met four criteria (easyadaptation to the home setting, minimum training required toadminister, speed of administration, and minimum equipment needed).Five categories of information are addressed for each instrument:basic information (title, authors, publication date, publisher,purpose, age, application, screening or astessment use, areasassessed, standardization, reliability, validity, and criteria for,refeArral); -admini.stration and scoring; time required foradministration; training required for administration andinterprtation; And advantages/disadvantages of the tool. Thefollowing instruments are analyzed: Denver Developmental ScreeningTest; Developmental Screeming Inventory; Nutrition/Feeding Screening;Early Intervention Developmental,Profile; Callier-Azuza Scale;Milani-Comparetti, Gidoni Developmental Chart; and Home Observationfor Measurement of the Environment. (CL)
**********************************************************************Reproductions supplied by EIW are the best that can be made
from the oriOnal document. * .
*****************************************t*****************************

ment do not nesesSar4 represent otfroal NIEPools or *new or opunons stated a, Itus docu
posa.on Of pont)/
U.S. DEPARTMENT OF EDUCATION
1'4 NATIONAL INSTITUTE OF EDUCATIONEOUCATIONAL RESOURCES INFORMATION
PrN CENTER (ERIC)
(:) .........trrnocuenent has been reptoduced Pswended horn the Pets On Of OlgaMOWOO
C\J ,1
MIP41 Joatur% Irwin been made to )(nom
C\i reproduchon wat7ty 4
Lw
.%
"PERMISSION TO REPRODUCE THISMATERIAL HAS BEEN GRANTED BY
TO THE EDUbATIONAL RESOURCESINFORMATION CENTER (ERIC)."
SCREENING AND ASSESSMENT TOOLS
A manual discussing appropriate toolsfor use in the home setting
by
The Family Centered Program en Intervention
Nisonger Centerfor
,r Mental Retardation and Developmental Disabilities
4-
The Ohio State UniversityColumbus, Ohio
1980
The Project was supported by Grant Number 2D12AH00135-07,awarded by the Division of Associated Health Professions,Public Health Service, Department of Health, Education and161fare. Its contents are polely the responsibility of the
(11
Family Centerad Program on Intervention Project.
\.
L\'1%

-TABLE OF CONTENTS
PREFACE
ACKNOWLEDGEMENTS
FIELD TEST
ii
iii
iv
INTRODUCTION 1
Format of Manual 3
Intended Audience 4
Learning Objectives 4
7
SCREENING TOOLS
Denver Developmental Screening Test (DDST) 11
Developmental Screening Inventory (DSI) 17 '
Nutiition/Feeding Screening 21
ASSESSMENT TOOLS 31
Early Intervention Developmental Profile 33
Callier-Azuza Scale 41
Milani-Comparetti, Giodoni Developmental ,Chart 47
Home Observation for Measurement of theEnvironment (HOME) 51
SCREENING AND ASSESSMENT TOOLS (Chart) 59
Gmwrii AND DEVELOPMENT BIBLIOGRAPHY 61
SCREENING AND ASSESSMENT BIBLIOGRAPHY 65
e
1.
PREFACE
' Family Centered Program on Intervention Project (FCPI)is.an outgrowth of Family Centered Practicum for Develop-mental Disabilities Project (FCP-DD) and, as such, hasadopted many of the philosophies FCP-DD acquired-during its
,f five years of working with and learning from families. FCPIwas funded by H.E.W., Division of Associated Health Profes-sions, to produce materials which will aid the student andprofessional in working with the family within the homesetting.
The professional is seen in a supportive role to parents,who are viewed as the primary caregivers in fostering the \growth and development Rf their children. The professionalassisks parents in beloming effective teachers of their de-velopmentally disabled child. It is in this climate that theprofessional shares hisreicpartise with the family.
Six'content areas were identified in order tg.producetraining materials which cover the broad range of skillsnecessary to the individual working with families,within thehome. These content areas are:
1. OBSERVATIONAL SKILLS2. SOCIAL-EMOTIONAL ASPECTS3. ENVIRONMENTAL FACTORS4. INTERPERSONAL COMMUNICATION AND
,RELA7ONSHIPS5. SCREENING AND ASSESSMENT6. ACTIVITIES 1N THE HOME
Five, categories of content are included within each area:generic knowledge, assesallent, levelopment opftreatment, im-planentation of treatment, and evaluation. The instructionalmaterials are presented in modular form to faciliatate pre-sentation in a variety of teaching settings.

ACKNOWLEDGBFTS
The staff of Family Centered Program on Interventionwishes to acknowledge the help of.many professionals whocontributed invaluable input ana time to the development ogthis manual. Grateful thanks is extended to Lynn Allen and.Debbie Arms who shared with us their knowledge of screeningarid assesSment tools: Thanks, also, to Betty Whittle. -Kozlowski and Katy Kram.for reviewing the Nutrition/FeedingScreening section. A special thanks is extended to BonnieRitchie, et al., authors of Maaual of Assessment Instrumentsfor the MR/DD Population, who allowed us to utilize much ofthg.ir information in the development of the evaluations.Acknowledgement is extended to the Nisonger Center for MentalRetardation-Developmental Disabilities for their continuingsupport and encouragement of all activities of the FamilyCentered-Program on Intervention.
PROJECT STAFF
Mariar F. Chase DirectorNancy L. Keyser/Patricia A. Eysser CoordinatorsWilliam H. Hurley Media SpecialistNancy W. Jones Training CoordinatorMarilyn S. Pramschufer CurOculum DeveloperFlorence H. Schermer
. Curriculum DeveloperRObin Milstead-O'Keeffe .1 EvaluatorAnn Carde.i. Secretary
iii

FIELD TEST
The manual, "Screening and Assessment Tools" has beenpilot tested and found to be a valuable learning tool forstudents and professionals interested in home-centered care.The manual will be field tested and data checked. related todhe quality of its effectiveness.
iv

1
SCREENINGLAND ASSESSMENT TOOLS
A manual discussing appropriate toolsfor use in the home setting
Introduction
Developmental screening and the assessment of the de-velopmentally disabled infant and youpg child is a necessaryand continuous'process. It is essential for those profes-sionals and students who work with children and their familiesin the home setting to be able to select and utilize thosescreening and assessment tools which are most suitable for thehnme setting. This manual contains a descriptive evaluationof seven tools which are either specifically designed for oreasily adapted to the home,setting.
There were four basic critpria which were used to deter=mine which tools should be included in the manual. The follow-ing defines tfiose four criteria:
. 1. The tool should be easily adapted to the home setting;
2. The tool shOUld not require extensive training to ad-minister. Individuals from a variety of relevantdisciplines should be able to administer it withlittle training. This is an especially important
!consideration since professionals and students in-: volved in home centered care often have a varietyof backgrounds and training;
3. Most tools included should take less than one-and-one-half hours to administer. This time factor approxi-mates the maximum time frame that one home visit mayrequire;
4. Tools were included which required only a minimum ofreadily available and easily transported equipmentand material-items. In most instances, the home visitcris responsible for transporting all equipment andmaterials required for the screening and/or assessment.

1
2
When evaluating the child in the home setting the pro-fessional should not overlook the subtle advantages that thehome setting offers. The presence of the parent(s) during anassessment done within the home il a most valual?le source ofinput, as they are obviously the experts on theiF own child'sbehavior. In addition, the 'home provides the most comfortablesetting for the young child. In his own territory, the childis more likely to exhibit typical behaviors which might be in-hibited'in an unfamiliar or more structured setting. Thus,
the person doing the assessment receives a more realistic pic-ture of the child's abilities and disabilities. It is alsopozsible for the,observant home visitor to discern relevantenvironmental factors found within the home which can contrib-ute to effective programming or which can be modified to facil-itate the child's development.
Ey'the title of this manual anplies, both screening andassessment tools are examined. It should be noted, at thistime, that there is a distinct difference between the two. Inorder to properly utilize the material presented in the manual,the difference should be clarified. Screening tools are "rela-tively short, of a surface natuve, and indicate the possibiliiyOf a variance in development." I Generally, administration ofd screening tool would be the first step in determining thestrong and weak areas in a child's development. When resultsfrom the screening tool indicate that the child has a delay in .
development, referral should be made to an appropriate disci-pline for follow-ug care. In addition, abnormal results on ascreening tool indicates the need for a more in-depth assess-ment of the child which, most probably, will be completed bythe most appropriate discipline. An assessment tool, by com-parison, ds "more lengthy, of an in-depth nature, and analyzesthe prohlems and makes differentiations not (based) on screen-ing results." 2 Results obtained from,an assessment Loolassist the professional to pinpoint more exactly the needs ofthe child so that proper treatment may be' initiatded with thechild and family.
Many of the screening and assessment toals described inthis manual were standardized on populations of children whodid not have developmental delays. It is therefore importantto remember that children with disabilities Wfio are tested mfall behind the established "norms" in some toola. However

3
it should be remembered that all children will follow a se-quence of development, i.e., they generally will progress in
1 a logical pattern from one skill to another. There re, It
; ray be very signifieant to follow tile manner in whi they
! acquire new skills.
This manual contains a smnpling of the most current testsin high use at the time of publication. Included are both
nonnative and criterian referenced tests. No attemPt,has beenmade to endorse one method over the other. It is more impor-ant.sto look at the purpose for testing rather than the scorinbmethod when selecting an appropriate tool for home use.
Format of Manual:
Within the evaluation of each tool information is organ-ized in the following ordell: (1) a face page including title, 4authors, date of publication, publisher, purpose, age, appli-cation, screening or assessment use, areas assessed, standardi-zation, reliability, validity, and criteria for referral, (2)
administration and scoring, (3) thne necessary for administra-
, tion, (4) *raining necessary by the home vis'itor to administeror interpret results, and (5) editorial comments on advantagesarid di-sadvantages of the individual tool. Much of this infor-mation is additionally available in a chart (p. 61) which canbe used as a quick reference for individuals who need to knowthe "vital statistics" of a certain tool. It may further assistthe professional to identify Uhich tool is appropriate for eachparticular child she is examining. It should be noted, however,that matedgas required for each tool are not listed Oith theevaluation nf the tool. Many of the tools required similarmaterials. Additionally, not all materials need to be utilized
each time the test is administered. The following is a generallist of materials which are required by various tools.
1
Red wool Round embroidery hoop
Raisins Aluminum cup
Rattle Child's picture\book
One-inch square blocks Large crayon and paper
Small bells' Small doll with bottle & chair
Tennis ball Tricycle
Pencil Toy Car
Push toy Sponge
44
. Note that all these materials arp readily available andeasily transported. /t is stressed thpt prior to administra-tion of the tool, the professional/has the responsibility toreview the section of the tool to4e utilized and discernwhich specific materials are requiked.
Intended Audience:
This manual was designed specifically for students andprofessionals who ars working with children and their familiesin the home setting. Unlike other instructionnl packages de-veloped by FCPI, this piece was intended to be used indepen-dently. It was not designed specifically for tise in a work-shop or classroom setting. gather, it was developed to beused as a reference manual which students and professionals
, could utilize when they want to obtain information about a%specific screening or assessment tool. The manual: discusses
the tools avaiable, but does not actually teach the'studentor professional how to administer the tool. It was decided
that the most effective manner ta learn to administer each toolwas to actually edminister it. COnsequently., information con- (tained within the manual should aid the home visitor to selectan appropriate tool for the child's needs.
It must be stressed that students and professionals workingin home-centered care with children must have a knowledge of"normal" growth and development before they will be able to doeffective screening and/pr assessment with any tool. The indi-
vidual should refer to tha bibliography on growth and develop-.
sment (p. 67) contained in alts manual for selezted readingsand references to either begin,to acquire or supplement thatessential knowledge.
Learning Objectives:
Learning objectives are intended to provide those whoutilize this manual with statements of:knowledge Aich theuser should have after successful utilizatiOn. Each learning
objective is followed by an Answer Key. Please note that these
, objectives begin with "5.1.1" because this manual representsthe fifth content area identified for production materialS (seepage ii).

4.
11-
5
5.1.1 list four ceiteria which should be considered whenselecting a scretning/as"sessment tool which is appro-priate for home use.
1, Adaptabilty to thq home2. Tool eastly administeah.by a variety of
disciplines3. Administration time under lk hours4. Equipment.and materials requirepfor administra-
awl readily available and easily transported.
5.1.2 Discuss the dlfferepce between a screening tool and anassessment,tool.
Scrtmningtooleare relatively short, of a surffce% nature, and indicate the possibility of a variance
in development. Generally, administration of ascreening tool woq.d.be the first step in deter-mining the strong and weak areas An a chil*sdevelopment.An assessment tool is "mere lengthy, of an indeptNnature, and analyzes .the problem and makes differ-ientiations not (based) on acreening results." 2Thus, the assessment tool, in.most sases, assiststhe professional to pinpoint more exactly the needsof the child so that work can begin with the famWin developirg a treatment program.
5.1.3 List At least two advantages to administering thescreening or assessmpnt tool in the home as opposed tothe clinic setting. a
1. Parents' presence - valuable input2.,In familAnr setting,. child mmre ltkely to
exhibit typical behaviors3.'Hare vtsitor clan observe relevant environ-
mdntal factors found in home which contributeto effectiye programming.
5.1.4 &plain the'rationale that the professional or studentmust have a knowledge of growth and.development priorto administering screening ard assessment tool; todevelopmentally disablcdchildran.
a
,
The professional most know the sentience ofnormal-divnlOpment and growth before he can telldeviatiobArom it.
5.14 List atleast two-tools which could effectively beutilized in the home setting to screen for delays in
'development. Discuss the age, purpose and areas* screened of each of the tOols.,
1. Denver Developmental SciPening TdatAge:.2 weeks to 6 yearsPurpose:,Used to detect developmontal delay
. among fnfanti and preschoolersAreas Screened: Personal/Social, Fine Motor/
Adaptive, Language, Gross Motor;N
2. Developrental Screening InventoryAge: 4 weeks to 36-monthsPurpose; Screening instrument for infant
behavior4reas Screened: Adaptive, Gross Motor, Fine
Motor, Lamguage,eersonal/Social
3. NCHS Growth GridsAge: Birth to 18 yearsPurpluse: Analyze growth patterns of a childAreas Screened: Height, Weight, Head Circum-
ference
5.1.6 List at least two tools Vhich could effectively beutilized in,the home,setting to assess the child's.developmental functioning level. Discuss the age,purpose, And areas screened of each of the tools.
1. Calller-Atuza Stale ir--Age: Generally birth to 4 years. Cognitive De-
velOpmental Subscale covers 0-231 years.Purpose; Designed specifically. to aid in
/ assessing deaftblind and multi-handi-
capped ciildren.Areas Screened: Motor Development, Perceptual
developtedat, Daily Living Skills, .
Cognitiom, Cmmmuhication and Language,
Socialization
NJ,
Aft
a
1 A.

4
7
2. Early Intervention Developmental Profitr-----Age: 0-36 monthsPurpose: Depicts developmental status of ex-
ceptional inTants in six areas of de-velopment
Areas: Perceptual/Fine Motor, Cognition,Language, Social/Emotional, Self-CareSkills, Gross Motor
3. Milani-Comparetti Gidoni Developmental ChartAge: Birth to 2 yearsPurpose: Designed to 'evaluate child's physical
development; can provide early evi-dence of neuromotor delay or deficitsin the child with mental retardationor Cerebral palsy.
Areas: Spontaneous Behavior, Evoked Responses
* * * * * * * *
References
1. Olion, LaDelle and Rodabaugh, Jeraldine. A Selected Listingof Instruments for Screening and Assessment. Bibliographyfor Preschool Children with Handicaps. The Head StartTechnical Assistance and Management System, Chicago, p. 2.
2. Ibid
I 3
0
SCREENING TOOLS 1

,
11 .
.
DENVER DEVELOPMENTAL SCREENING TEST (DDST)
W. Frankenburg and J.B. Dodds, 1467
Y

12
DENVER DEVELOPMENTAL SCREENING TEST (DDST)
W. Frankenburg and J.B. Dodds, 1967
41;6
Publisher: Ladoca Project and Publishing Foundation, Inc.East 51st Avenue and Lincoln Street
Denver, Colorado 80216
Purpose: This instrument may be used to detect developmentaldelay among infants and preschoolers
Applicpr
fo
be
old
2 weeks to 6 years
ation: This instrument was created for use by medicalofessionals as well as non-professional health workersr early identification of developmental delay. It may
used for all children who function below the 6-year-
level.
,Screening/Assessment: The test includes 105 tasks or iteils
whicheach a
are divided into four different areas. Skills 'n
rea are assessed by diiect observation or parentIt is assumed that they cover the basic areas
lopment and the specific skills normally acquired
ren. The four areas include:
report.of deveby chi/
1) Pa
a -2) Fito
j) Lanand
4) GrOss
ersonal/Social (self-care abilities andility tobrelate to others)ne-Motor Adaptive (use of'hands and abilitysolve non-verbal problems)guage (ability to hear, carry out commands
speak)Motor (ability to sit, walk and jump)/
Standardization: ThCaucasian chilyears. Of themale. All childnormalities werebreech deliveriesSubjects wmre sele
e test was.standardized on 1036 Denverdren between the ages of 2 weeks and 6.4total tested, 543 were Male and 493 fe-'ren with high risk of developmental ab-excluded (premature babies, twins,
, or those with gross physical defects).cted through private pediatricians,
'0

13
well baby clinics, schools, churches, and labor unionauxilaries. The distribution of,subjects was felt toreflect racioethnic and occupational group characteris-tics of the Denver population (according to the 1960census).
Reliability: Inter-rater reliabilities reported by Frankenburgand Dodds (1967) range from 0.66 - 0.95. Test-retestreliability ranges from 0.66 - 0.95.
Validity: A parallel study of the correlation Of DDST scoreswith the various developmental measures (Yale Develop-mental Schedule, Stanford-Binet, Cattell Infant.Intelli-
1 gence Scale, and Bayley Scales of Infant Development)yielded correlations between :74 and .97.
4
o
14
"The format of the Denver Developmental Screening Test wasdevised to present all the normative data for the total samplein a graphic manner so that the user can quickly compais anindividual child's performance with that of the children on
whom the items were standardized. Each item is repreaented by
a horizontal bar placed along an age continuum. Various points
on the bar represent the specific ages at which 25 percent, 50percent, 75 percent, and 90 percent of the sample of children
pass an item. The test form has each item arranged along thesame continuum in one of four categories: gross motdr, finemotor-adaptive, language, and personal-social."
The manual which accompanies the DDST explains the teitform, administration, and scoring of the test. It examines
each of the tasks and gives examples of how to assess thechild's ability to accomplish the task. gnitially, an age lineis drawn on the form which takes into account prematurity. This
age line will give reference on where to begin the test and how
to score it. rhe test should commence with items below the ageof the ,child and work up to his age (to the rig(t) until threefailures have been scored. Each item is scored with a "P" for
pass, "F" for failure, "R" for refusal or "N.0." for no oppor-tunity for the child to perform the item.
dIt is suggested that the test be initiated with the
Personal-Social section to familiarize the child with the tes-.ter (many Items may be passed by report from this section).It is recommended that the chird next be tested in the Fine-Motor Adaptive area so that by the time the Language area isadministered, the child will feel more at ease with the tester.It is best to give the Gross Motor section last so that thechild will not be too stimulated from the hoppj.ng, jumping,and/or throwing of the ball to complete the remaining aecticinS
of the exam.
, A "delay" is any item cfailed which is completely to the
left of the age line. Thus, an item_ is failed which 907 of the
rchildren normally pass at a younger age. Test results are ab-
normal if two sections have two or more delays, one section hastwo or gore delays and, in the same section, the age line does
not go through an ftem that is passed. The child should be re-
tested in one month. if the first test is abnormal.
1
ft&

15
The amount of time required to administer the DDST is 30minutes or less. The screening tool .... "is designed for useby people who have not had speselal training in psychologicaltesting." 2 It would be apptopriate for any professional whois working with children in any health care system. When de-lays are di,scovered, a more indepth assessment of the child'sfunctioning should be made. At such time, one of the follow-
* ing assessment tools, which is reviewed in this manual, maybe considered for use: The Callier-Azuza Scale, the EarlyIntetvention Developmental Profile and/or Home Observationfor Measurement of,the Environment.
The Denver Developmental Screening Test has the advantage .
of being inexansive, quick and easy to administer and shouldbe considered a practical, efficient and dependable devicefor use in screening children for delay. The manual whichaccom ipanies the tool is very valuable because it s
1
easy tounderstand and explicit with regard to scoring guidelines."The authors caution against using the DDST as a diagnostictool and recommend close observation of qualitative aspectsof test behavior in relation to motivation, dependency orhostility'between mother and child, examiner-child interaction,and maintenance of optimal and standard tesLing conditions." 3
References.,
1. Frankenburg, William, and Dodds, Josiah. "The DenverDevelopmental Screening Test." Journal of Pediatrics,Vol. 71, No. 2, August 1967, p. 183.
2. Frankenburg, William F., et aft. Denver DevelopmentalScreening Test Manual, 1970, Introduction page. -
3. Ritchie, Bonnie, et al. Manual of Assessment Tools forthe MR/DD Population, Nisonger Center on Mental Retardationand Developmental Disabilities, Columbus, Ohio, 1978, p. 15.
1.7
a
DEVELOPMENTAL SCREENING INVENTORY (DSI)
M. Knobloch, B. Pasmnanick, E. Sherard, 19540'
2 0
18
DEVELOPMENTAL SCREENING aNVhNTORY (DSI)
H. Knobloch, B. Pasamanick, E. Sherard, 195,4
Publisher: Division of Child DevelopmentDept. of Pediatrics and Dept. of Psychiatry
The Ohio State UniversityCollege of MedicineColumbus, Ohio 43210
Purpose: The Developmental Screening Inventory is designed asss
a screening instrument for infant behavior.
Aka: 4 weeks to 36 months
Application: "By asking some questions of,tAarents, observingthe.infant's behavior and recording this informationsystematically, an estimate of the level of function invarious areas off, behavior can be made which correlates
very highly with the maturity age assigned on the basis
.of a complete Gesell Developmental Neurologic Examinationfrom which the items are adapted." 11.
Screening/Assessment: The inventory is primarily a screening
iool. 1
Arnas Screened: The inOentory is administered to 20 different
age groupg'during the first 36 months. There are 4-week
divisions through-the age of 56 weeks. The areas screened
include:1) Adaptive 12) Gross Motor3) Fine Motor4) Language5) Personal/Social
Standardization: Standardization procedures are based on those
used for the Gesell Scale. The DSI had not, itself,
been standardized. .

s
ReliabilJity: No data available
Validity: No data available.
, * * * * * * *
Reference
19
1. Knoblach, H., Pasamanick, B. and Sherard, E. &DevelopmentalScreening Inventory, 1954, Columbus, Ohio, p. a.'
-
..
4
I

20
*
When using the Developmental Screening Inventory, thehome visit)r utilizes information gained through both obser-vation of the infant (recorded in "0" Observed Column) andthe history of the infant's behaviors as related by the par,-ents (recorded in "11" Column). In a variety of situations'ae,infant may perform a task routinely at home, but not beable to duplicate it when asked to by a professional. There-fore, it is significant that information the home visitor re-cordg may be the result of actual observation or history. Thehome visitor shoulil initiate the test at chronological age ofthe child (i.e., if a child is 15 months old, begin with the15 month block'of activities): If many of the answers arenegative, the lime visitor should drop back to a lower age,)level and work up to the child's chronological age. The homevisitor Fhould continue to ask questions at progressivelymore advanced ages until no more positives are obtained. It
is significant to note that an infant may be slow in one areaand nOrmal in the other. Consequently, administration couldconceivably span two or three designated time categories.
Observations should be recorded as (4) present, (-)absent, or (x) unknown,. In each of the areas of adaptive bp-havior, gross motor, fine motor, language, personal/socialmaturity levels (in weeks or months) hre assigned based ona clinical judgement of the age levels obtained from historyand observations. Finally, a diagnostic category is deter-mined, based on the age lel.els and will bee'either (a) abnormal:,
. () borderline, or (N) normal.
Administration of the inventory can be accomplished in 30minutes or less and does not require any special training inpsychological testing. It is a quick and useful instrument.for scvening problem areas in the.young child's development.The involvement of parents in obtaining data regarding thechild is viewed as a positive interaction for both the pro-fessiunal and the family workin8 in a home-centered care situ-ation. It is important to.note, however, that the DSI shouldnot be used as a diagnostic tool at any time. When delays arediscovered, a mure indepth assessment of the child should then
be dune: The reader is referred to the assessment tools re-viewed in the following section orthis manual.
9--

7
4
.17..
NITIIMON/FEEDING SCREENING
.
2.i
21
.7

earl'
22
,NUTRITION/FEEDING SCREENING
A complete nutritional and/or feeding assessment of achild is a complex and thne consuming undertaking. There are
many aspects of the child's feecting and nut,rition.al environ-
ment and status, however, that the professional may effectivelyscreen Whike in the home. If she knows how to look for prob-
lem areas, she may be able to detect where and when a completenutritional asseanent is warranted. The pralessional in thehome shipld inquire about and observe feeding sessions. By.,
watching interactions, Valuable informationAmay be obtained.Does the child have problems with sitting comfortably at meal
4 times or closing his mouth and chewing properly? Is he prop-
erly positioned for feeding? Does he eat foods which do notseem appropriate (i.e. large quantities of milk or pureed
foods at an older age)? These and other factOrs should all becues to the professional that the child may need screening ofhis nutritional status.
When the professional balieves that the child and familyrequire adiliti2nal help with feeding/nutrition, she should
, refer the family to a qualified dietitian or nutritionist whowill be able to help them with identified problem areas.
The number of'screening tools designed specificallY forchildren who have developmental disabilities is few. Conse-
quently, modifications of existing nutrition screening tools
, have been made by nutritionists for use with this population.is noteworthy that a nutritional screening took is being
developed at Nisonger Center for use with preschool-aged chil-
dren.) Al.though there may be various methods utilized in ob-taining information,regarding the child's feeding and nutri-tional status, the following is a list of important concernswhich the professional from any discipline should observe orquestion about while in the home:
1. Child's positioning during eating sessions and hisoral functioning
2. The child's self-feeding sk lls3. The manner in which the ch d adapts to various ter-
tures of food4. Information concerning special diets the child may
be following
71

0 s -
,
...
~
r-.
4
:..
S
,
a
-4. t..0'
io
or
23
s
-
5. Unusual eating or meiltime habits which the child has6. Problems the child experiences with elimination.7. Variety of foRds ihe child has in his diet8. The child's growth pattern
4 t,
*...
e
\
:
..
1
%
1
' I
. ti,

;"
2 4
NCHS GROWTH GRIDS
National Center for HeAkth-SZAtistics, 1976,
Publisher:Ross LaboratoriesColumba, Ohio 43216
Purpose: This instrument is used over a period of time to.analyze the growth patterns of a child.
Aga: Boys: Birth to 36,months (at one-month increments)2 to 18 years (at half-year increments)
Girls: Birth to 36 months (at one-month increments)-2'to 18 years (at half-year increments)
Application: Use of this tool for nutritional screening isbased upon the premise that if a child is consuming theproper amounts and types of nutrients, he will grow ata genetically predetermined rate. Thus, accurate periodic,measurmnents of the child are made and recorded,by theprofessional over a period of rime. The information ob-tained will Aid in the detettion of a child who is poten-tially "at risk" nutritionally.. b/r
Screenipg/Assessment: NCHS growth grids are used to analyzethe growth Pattern of an individual. Growth patterns ofan individual are affected by genetics and the individ-
ual's nutritional makeup. When growth rate is inappro-priate, the individual should be referred for an indepth
nutritional assessment.
Areas Screened: Areas screened include: height, weight, andhead circumference.'
AStandardization: Boys and Girls - birth to 24 months. Data
was collected from the Res2arch Institute concerning 867children who were followed longitudinally from birth.Not every child was measured at every age, but 700 to800 children were measured at birth, 1 month, 2 months,6 months, 9 months, 1 year, lk years, 2 years, 2k years,
and 3 years.Bays and Girls - 2 through 17. Information was obtainede
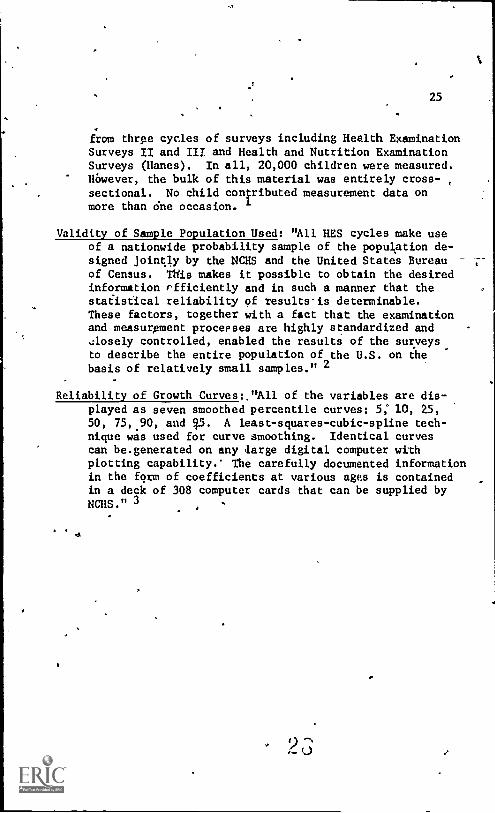
25
from three cycles of surveys including Health ExaminationSurveys II and II/ and Health and Nutrition ExaminationSurveys (Hanes). In all, 20,000 children were measured.However, the bulk of this material was entirely cross-sectional. No child co4ributed measurement data onmore than 6ne occasion.
Validity of Sample Population Used: "All HES cycles make useof a nationwide probability sample of the population de-signed jointly by the NCHS and the United States Bureauof Census. This makes it possible to obtain the desiredinformation rfficiently and in such a manner that thestaiistical reliability of results-is determinable.These factors, together with a fact that the examinationand measurpment processes are highly standardized and -
Aosely controlled, enabled the results of the surveysto describe the entire population of the U.S. on thebasis of relatively small samples." 2
2,
Reliability of Growth Curves:."All of the variables are dis-played as seven smoothed percentile curves: 5: 10, 25,50, 75, 90, and q5. A least-squares-cubic-spline tech-nique was used for curve smoothing. Identical curvescan be.generated on any large digital computer withplotting capability. The carefully documented informationin the form of coefficients at various ages is containedin a deck of 308 computer cards that can be supplied byNCHS." 3

26
Information obtained from accurate measurements is re-,corded op the growth grid. kength (in. or cm.), weight (Kg'.
or lb.) and head Circumference measurements (in. or cm.) areplotted on the vertical axis and age is plotted on the hori-zontal. Percentiles show the ag9 at which 5, 10, 25, 50, 75,90 and 95% Of the standardized population reach a specifiedheight, weight, or head eircumference. In addition, a specific ,
graph plots.length of the child (on the horizontal axis)against -weight (on vertical-axis).
The professional should attempt to obtain all previousgrowth mdasurements available from school, family, or medicalrecords. This information is then plotted on an NCHS growthgrid. Data should be interpreted according to the child'sindividual.growth pattern or curve. It is more signi.ficant
to monitor the direction of several plottings than an isolatedrecording.
Use of the NCHS growth grid will be helpful only in sofar as it reflects accurate information. Precise measurementsmust be obtained to provide accurate information. It is essen-tial that prpper equipment and techniques be utilized whenmeasurements are obtained. Equipment appropriate for use inthe clinical setting may not necessarily be equipment that isappropriate foe the home setting.
The following is 11°'.1ist of equipment used to obtain meas-urements which would be appropriate for use in the home setting:
1) Steel or plastic measuring tape (paper should neverbe used since it may stretch)
2) Headboard (when available) for use with childrenunder the age of three
3) Wooden block, squared at right angles or hard-bound book
4) Bathroom scale which has periodically been checkedfor accuracy.
5) Infant scale (when aVailable) for use with childrenUnder the weight of 30 lbs.
I. Obtaining Height or length Measurement
A. Children under age of 3, or those over the age of 3,who cannot stand erect must be measured for recumbantlength.

s
27
1. Headboard procedure. ,(A headboard is a measuringboard with rule screwed down on,one or both sides
and a rigid, moveable footboard.) The child lieson his back on the measuring board. One pefson
holds the crown of his head against the headboard.The other person holds both ankles with one handand places the child's heels firmly against thefootboard. The footboard is manipulated with theoeher hand,_ The measurer should be certain that"the.Child's iegs-are fully expended. The childshould be measured-twice to insure accuracy. 4
2. Procedure when heaTh ard is not'available. Thechild should be lying on a firm, flat surface withthe top of.his head.flat against the wall (selecta wall that does not have molding on the bottom).Take the child's ankles wip one hand and placethe child's heefs firmly against alflattUock orbook. Care should be given that the child isfully relaxed when the measurement is taken. If
'the knees are flexed there will be deviation inthe measurement. Next, lay the steel or plasttstape parallel to the child, placing the tip atthe head and measuring tn the heel of the foot,
-44or top of the block or book. (It bay be necessary-
to have a second person, perhaps Mother, assistin the process.) Measurements should be madetwice to insure accuracy.
B. Children three ydars,of age or older whoare able tostand erect should be measured standing up.
1To measuad the heighi-Of children a flexiblesteel )or pDestic measuring tape is attached to a door
frame or wall: A block which is squared at rightangleswith the leveler also is utilized. The child,shoes emoved,'stands on a horizontal bare floor in acomforiably erect position with heels, lower beck,shouldtrs or rear of heel touching against a verticalwall or door frame. The block is lowerej to make firmcontact with the scalp. Measurements are read to thenearest aM,- Measurements are made twice gor eachchild and should be within k cm. of eadh-other. Thechild iis.asked to step away from the wall after eachmeasur
7ment."-5
28
II. Measuring Weight
A. Children less thin 13.6 Kg (30 lbs.) should be measuredwith an infant scale. The scales_should_be -balancedprior to each use. All of the child's clothing is re-moved and the child is then placed on the scale andthe weights are recorded. Two weights should be ob:tained to insure accuracy. The scale shoufd be checkedperiodically tc insure their accuracy.
B. Children over 13.6 Kg (30 lbs.) may be weighed on a con-ventional bathroom scale. The professional must becertain that the scales are accurate. This may beaccomplished by checkfng them against a beam scale.The child should be instructed to remove all his clothesbut underpants. Two weights should be obtained to in-sure accuracy. (When a child wilb not stand on thescale, the professional or mother should weight them-pelves, record it, and then weigh the child with him-self. The first weight should then be subtracted fromthe second to equal the child's weight.)
III. Measuring Head Circumference
For this measurement, a flexible narrow steel or plastiitape (k" wide) should be used. "The tape is applied firmlyaround the head above the supraorbital ridges or the mostprominent part of the frontal bulge, anteriorly, and overthat part of the occiput which gives maximum frontal-occipital circumference. Measure in duplicate to thenearest cm." 6
WiEh practice, each professional who visits clients in thehome setting should be able to obtain accurate measurements.The actual time involved in taking the measurements, recordingthem, and plott:A& them on the graph should be under ten minutes.
3

29
References
1. Nutritional Disorders of Children: Screening, Prevention '
and Followup. U.S. Department of Health, Education and
Welfare, p. 18.2. P.V. Hamill, et al. "Physial Growth: National Center
for Health Statistics Percentiles." American Journal ofClinical Nutrition. Vol% 32, March 1979, p.°616.
3. Ibid, p. 617.4. Ekvall, Shirley. "Assessment of Nutritiodal Status." In
Palmer, Sushma and Ekvall. Tediatric Narition in Develop-mental Disorders. Charles C. Thomas, Springfield, Ill.,1978, p. 606.'
5. Ibid, p. 506.6. Ibid, p. 508.
a

ASSESSMENT TOOLS
o
-
33
31
,

l'A
f03
MNRLY INTERVENTION bEVELCPMENTAL PROFILE
33.
S. Rogers, D. D'Eugenio, S. Brown, C. Donovan, E. Lynch, 1977
3 4
,

34
EARLY INTERVENTION DEVELOPMENTAL PROFILE
S. Rogers, D. D'Eugenio, S. Brown, C. Donovan, E. Lynch, 1977
Publisher: University of MichiganPublication Distribution Service615 E. UniversityAnn Arbor, Michigan 48109
Purpose: The profile depicts the developmental status of in-
fants in six areas of development.
Lgs: 0-36 months
Application: This instrument was created for children withall types of handicaps who function below the 36-month
age level.
Screening/Assessment: This instrument can provide an in-depthpicture of a child's functioning in a variety of areasand should be considered an asaessment, rather than ageneral screening tool.
Areas Assessed: Perceptual/Fine Motor.DevelopmentCognitionLanguageSocial/Emotional DevelopmentSelf-Care Skills
'Gross Motor Development
Standardization: This profile has.not been standardized. The
authors assigned items, to specijic age ranges on thebasis af standardization norms of other well-known develop-mental instruments or original sources (i.e., Piaget).
Reliability: Inter-rater reliability was examined using a
tester-observer paradigm. The mean percent of agreementbetween the tester and the nine observers (all trainedraters) was 897.. Correlations between initial testscores after three and six months for 15 children was r
c. uniformly high (above .93).
3,5

35
Validity:che authors established concurrent validity bycorrelating each of the six scales with the Bayley Mental.and Motor Scales, Vineland, REEL, and clinical motorevaluations. Coefficients for all scales were generallyhigh. The-consistency of handicapped infants performanceacross all stales ranged from .59 among the language,self-care, and gross*motor scales to .95 between thecognition and socikl/eMotional scales.

36
The Early Intervention Developmental Profile is Volume 2of a three-volume set entitled Developmental Programming forInfants and Young Children. Volume 1, Assessment and Appli-cation, contains a detailed test item description and scoringprocedurps for each item listed in the profile.
"An item passed by the child is marked pith aP if the criteria are met. When therd is a questionas to whesther the child has fully met the criteriafor an item, a pass-fail (PF) should, be used to indr-cate the emergence of the skill measured by that par-ticular item. Clear failures are marked by an F. A
final scoring category, 0, is used to signify thatan item has been omitted by the evaluator *because ofintervening Variables which should be described inthe scoring box." 1
---
Volume I also contains information concerning the admini-stration of the instrument and actual program developmentbased upon results yielded by the piofile. The authors suggest
that a brief observation of the child's motor function precedeany actual administration, .of individual items on the profile.Ir motor abnormalities exist which may affect the child's per-formance on the profile, any necessarY relaxation and/or posit-ioning techniques can then be utilized to aid the-child. It
is recommended that the assebment begin with administrationof the perceptual/fine motor and cognition scales, since chil-dren appear to be particularly interested by the items ol these
scales.
"Since young children tire easily in a struc-tured situation, it is critical that the child'srange of functioning on each og the scales bequickly determined and that items within that rangeare adequately covered. This process is facilitatedby beginning with an open-ended activity which isscorable at several levels. The use of 1-inch coloredcubes is suggested for two reasons. First, they are
generally intere,ting to the child whose spontaneoushandling of the cubes often provides scorabla respon-ses. Second, because cube items exist at almost every
age level on the profile, the chiles highest levelof success on cube items will give the tester a guide

37
as to which.age ranges should be miploredVarious items should be administered using thesame toy as long as the child is interested, andmaterials should be chaqed in order to maintainthe child's attention." 4
The child may spontaneously vocalize throughout the asSess-ment. Therefore, the language scale should be administeredlater in the assessment and any vocalizations occurring earlierin the assessment Can be recorded as they occur. "Items fromthe social/emotional and selfrcare,scales can be administeredwhenever a break for either child or parent is needed duringthe assestment." 3 The gross motor scale is best administered,last besause children often become either quite active at thistime or upset and it may be difficult to reestablish the rapportneeded for further evaluation.
The program development section of Volume 1 describesseveral aspects and components of behavioral objectives and"discusses the development of objectives based on assessmentresults from the Early Intervention Developmental Profile." 4In addition, this section includes information concerningactivity planning for the individual child based on the de-veloped behavioral objective. Guidance on altering activitiesfor specific handicaps Es provided for those who may be assess-ing a population which includes severely damaged children.
Volume 2 is the Early Intervention Developmental Profile.It's contents include the 274 item profile of development inthe six previously identified areas, a list of necessary mater-
ials and a profile graph.
"The child's performance can be plotted on theprofile (graph) by marking the htghest number of con-sistently passed items in each of the six areas andthen connecting the marks. The resulting graph pro-
vides a visual representation of the child's relativestrengths, weaknesses, and general developmental level."5
Assessment with the Early Intervention Developnental Pro-file can be,accomplished within one-and-one-half hours. The
authors state that the profile should be administered by amultidisciplinary team or an experienced evaluator. It is felt
4

38
that with some time spent in eimiliarization with the tool,assessment can be done by an individual home visitor from avariety of disciplines. Several items contained in the gross
motor scale require that the evaluator have some knowledge ofearly reflexive development. However, the item descriptionscontained in Volume 1, Assessment and Application, clarify pro-cedures for administering and scoring those particular items.
The third volume of this set is entitled StimulationActivities and contains activities for young children whichprovide appropriate play and enrichment experiences. Volume 3
"is designed for use by professionals who are training parentsof,children withkevelopmental delay, chroeic illness, and de-fined mental., motor or sensory handicaps to become actively in-volved in their child's treatment program." 6 This model isparticUlarly applicable to the role in which the home visitorfunctions.
0
Stimulation Activities is a source of ideas for carrying'i
,opt the specific behavioral: objectives which have been devel-loped for an individual dhild and family. Each of the activitlesincluded pinpoints a specific area of development.(i.e., object
/
permanence) within each assessment area (i.e., cognition) and.1116 identifies a short term goal for the child who does theeactivity (i.e., child will lbok at the place where a movingobject has just disappeared). Beneath each of,the activitiesis a key which describes an adaptation of the activities dueto a child's handicap and the appropriate teaching,method forthe given short term goal.
.
Caution should be exercised when using the data yielded bythe profile. Profile data yield a general estimate of develop-mental level and therefore should not be used when diagnoses oraccurate (e.g. specific) devalblimental level is required.* Thisassessment, however, provides more detailed information aboutreflexive and cognitive development than most infant assess-ment tools.
The tool provides a natural progression from assessmentof the child to formulation of behavioral objectives to de-velopment of home activities. The professional or student wbo
administers the tool should be confident of his ability to
4.39
interpret results and subsequently plan proper activities.Consequentlyiyhen used appropriately, and by a qualifiedindividual, there may not be a need for referral to specificdiscipline& excePt at ttiC discretion of the evaluator.
The Early Intervention.Developmental Profile and thethree-voltraid set, Developmental Programming for InfantsfandYoung.Children, is an excellent resource for use by homevisitors. It is a comprehensive and easily understoqd pack-age whicb provides not only fdr an indepth assessment ofchildren with a variety of handicapping condiaons, but hasthe additional feature of provilling useful information con-
- cerning formulation of behavioral objectives and thedavelop-.ment of home activities. The activities are_designed to inrvotve the parents in the chilli's training and, as such, arewell suited to the programming goals of the professional in-
. volved in home-centerCd care.
* * * * * * * * *
References
-.4!1. Rbgers, D'Eugenio, D.B., Brown, S.L., Donovan,C.M.,
and Lynch, E.W. "Early Intervention DevelopMental Profile."In Developmental Progl:amming for Infants and Young Children,Vol. 2, ed: by Schafer anti Moersch. Anil Arbor: University
of Michigan PressK1977, p. 12. Rogers, S.J. andA'Eugenio:' D.B. "Assessment and App11.-
catiOn." In DevelimMental Programming or Infants andYoung Children, Vol. 2, ed. by Schafer and Moersch. Ann
Arbor: University of Michigan Press, 1977, p. 1.
3. Ibid.4. Ibid, p. 43.S. Rogers,-S.J., D'Eugenin, D.B., Brown, S.L., Donovan, C.M.,
and Lynch, E.W. "Early;Intervention.Developmental Profi/.64Z101,
In Develo mental Pro rammin Infants and Youn Children,
Vol..2, ed. by Schafer and Moersch. Alfh Arbor:, University
Of Michigan Press, 1977, p. 1. '
6. Brown, S.L. and Donovan, C.M. "Stimulation Activities."In Developmental ProgramMing for Infants and Young Children,Vol. 3, ed. by Schafer and Mearsch. Ann Arbor: University.
of Michigan Prels, 1977, p. t. .

,
r.,
_
-
..
t.
-
,
THE CALLIER-AZUZA SCALE (CAS),
R. Stillman, F Edition, 1977
..
! / ,

42
THE, CALLIER-A2UZA SCALE (CAS)
R.Stillman, F Edition, 1977
Publisher: Robert StillmanUniversity of TexasiDallas'Callier Center for Communication Disorderi1966 Inwood RoadDallas, TX 75235 .
Purpose: This instrument is a criterion-referenced developmentalscale which was designed specifically to aid in the assess-ment of deaf/blind and multi-handicapped Children.
Alle: Birth to 4 years of age; with the exception of the Cogni-tive Developmental Sfibscale, the sen-
soriMotor period (0-2k yrs.). S e items are includedup to nine years of age on several of the individual
.scales.
Application: This scale is a good developmental tool for usewith children for whom other methods of assessment are un-
, appropriate or inadequate due to the child's handicap.
Screening/Assess;nent: This instrument can provide an in-depthpicture of a child's functioning in a variety of areasand should be considered an assessment rather than ageneral screening tool.
Areas Assessed:- Motor Development: (Subscales) Postural Control, Loco-
motion, Fine Motor, Visual Motor- Perceptual Development: (Subsdales) Vision, Auditory,
Tactile- Daily Living Skills: (Subscales) Dressing, Personal Hy-
giene, Feeding, Toileting- Cognition, Communication and Language: (Subscales) Cog-
nition, RecePtive Language, Expressive Language,'
, Speech Development- Socialization: (Subscales) Socialization, Self-concept

43
Standardizatidn Approximate age equivalencies were obtainedfrom a variety of sources in the child developmentliterature,
Reliability: No data available.
yalidity: No data availakle.
4 :;
44
Administration of the Callier-Azuza Scale is based uponobservation of behaviors which typically occur within a class-room setting. To begin the assessment, a base step must beestablished for the child on an indivichil subscale. A child
has attained a specific step (base step) on a subscale if thebehaviors he exhibits are .
integrated components of the child's be-havior repertoire. The behaviors must be spontan-eously appearing and appropriately generalized. Achild has not attained a step,if the behaviors des-cribed are emerging, occur only infrequently, occur'only after prodding and coaxing, or occur only inspecific situations and are not generalized to otherappropriate situations." 1
In addition, the child should have exhitated the integratedbehaviors described in all preceding steps. The authurs notethat although svme early behaviors are expected to disappear, itwill be necessary for the home visitor to determine if the cur-rent behaviors are based on the integration of appropriate earlybehaviors and are not examples of splinter skills acquired bythe child. When the base step has been established, the child's
. behavior on later steps in the subscale should be observed.
The authors caution that the scale must be administeredby someone who is thoroughly familiar with the child's behaviorand recommend that a child be observed for at least two weeksbefore the assessment takes place. When the Callier-Azuza isused for home programs, the individual doing the assessment"must be certain that adequate opportality has been provided forthe observation of the child's typical spontaneously occurringbehaviors." 2
Due to the comprehensivenessof the tool, assessment of achild in all areas would be time consuming and might not beaccomplished in an hour-and-a-half. Although completion of theassessment within this time frame is possible, it is recommendd IPthat the home visitor clearly identify an approximate starting
\place within each subscale. It may also be necessary to sched-
\ule the assessment during more than one home visit. Although
\the Callier-Azuza Scale was designed for use by teachers within
\the classroom setting, it is f.'r that it can be administered
4,i
45
by home visitors representative of a variety oE disciplineswithout extensive training in its use.
The home visitor who sees primarily a population of youngchildren who are developmentally disabled will find this tool
valuable because it was designed for assessment use with deaf--blind and other severely and profoundly hanticapped children.
A useful feature of the Callier-Azuza Scale are certainitems which are starred and begfn with "May." "These items
may be omitted for a specific child only if the child cannotbe expected to exhibit ..he behavior because of a specificsensory or motor defic (e.g: totally blind, nonambulatory).It is the responsibil 4 of the observers to decide if attain-ment of specific starred items is appropriate for an indiVidualchild." 3 Pass/fail directions are vague in some'instances.The test relies strongly on the examiner to determine pass/failscoring and referral. Additional reflex testing might be nec-essary to supplement the Callier-Azuza.
The assessment is divided nicely into subscales that arevery important when dealing with a developmentally delayed
child. A wide range of developmental items are presented ineach section, thus allowing thorough evaluation of childrenwho may vary greatly in diffe:ent areas. In addition, the
criterion-referencing format of the Callier-Azuza Scale elemi-nates comparison of an individual child to the "norm" and in-stead, emphasizes the child's progress. It should be noted
that this tool is designed to be more comprehensive at lowerlevels than at upper levels. Since the scale is continually
undergoing revisions (the Cognitive Development subscale wAs
added in this current F edition), it is possible that addit-ional items (or subscales) will be added at the upper levels.
* * * * * * * * * *a4 References
1. Stillman, Robert; et al. "The Callier-Azuza Scale."The University of Texas at Dallas: Callier Center forCommunication Disorders, 1977, p. 5.
2. Ibid, p. 4.
3. Ibid, p. 5.

47
THE MILANI-COMPARETTI, GTIONI DEVELOPMENTAL CHART
A. Mi1ani-Campq'retti, E. A. Gidoni, 1967
1.

48
THE MILANI-COMPARETTI, GIDONI DgVELOPMENTAL CHART
A. Milani-Comparetti, E. A. Gidoni, 1967
Publisher: Refer to article:
Milani-Comparetti, A. and Gidoni, E.A. "RoutineDevelopmental Examination in Normal and RetardedChildren," Developmental Medicine and ChiidNeurology, Vol. 9, 1967.
Purpose: This developmental chart was designed to evaluate achild's physical development. It can provide earlyevidence of neuromotor delay or deficits in the childwith mental retardation or cerebral palsy.
Aga: Birth to 2 years.
Screening/Assessment: The chart should be considered a rapidscreening instrument which:can compliment other standar-dized tests of infant behavior.
Areas Screened:
- Spontaneous Behavior: Basic motor development whichincludes the child's ability to control his headand body and the child's capacity to actuallymove from one position to another.
- Evoked Responses: Child's responses to certain stimulusconditions imposed by the examiner for tne elici-tation of,reflexes.
Standardization:
Reliability:
Validity:
.1
There is no normative data available.The items on the chart have beenselected from Gesell, Bobath,Illingworth, and Prechtl, etc.

49
Administration of the Milani-Comparetti, Gidoni Develop-mental Chart should begin with observation of spontaneouspostures and motor behaviors. The results of this observationare recorded on the top half of the chart labeled "SpontaneousBehavior." Next, certain stimulus conditions are imposed forelicitation of reflexes and the child's responses are recordedon the bottom half of the chart, labeled "Evoked Responses.""Entries on the chart are made by writing the (child's) chrono-logical age in months beneath the functional lnding indicatedat the head of the columns."
.After recording the child's behavior in this manner, daeresults can then be read and the following patterns designatewhether the finding is normal or indicative of mental retar-
dation or motor dysfunction.
1. Vertical alfgnment of the annotations consistentwith the child's chronological age indiCatesnormalcy;
2. "Motor retardation of the type associated withmental deficiency usually appears as a homogenousshift towards the left - that is to say, themotor performance comes to correspond to a lowerchronological age but the vertical alignment isapproximately maintained;"
3. "A wider scattering of the findings is usually asign of a more severe or possibly a more specificmotor dysfunction, as seen in cerebral palsy." 2
The examination and recording procedure should take anexperienced observer approximately two to three minutes.Unless the individual possesses some occupational or physicaltherapy skills, however, it is likely that administration andscoring process will require a more extended period of time.
The Milani-Comparetti, Gidoni Developmental Chart is in-Lluded in this manual because it offers a graphic picture ofthe correlation between functional motor achievemeht and a
child's underlying reflex structure. Unless the home visEtor
has some background in neuru-developmental treatment, it is feltthat some difficulty may be encountered in administratiun and/or

50
interpretation of the results for programming purposes. If
consultation with individuals with this background and trainingis possible, the home visitor can find the chart a valuableinstrument for use with children.who have developmental disa-bilities.
A manual of testing procedures for the Milani-Comparetti,Cidoni Developmental Chart has been developed at the MeyerChildren's Rehabilitation Institute. The manual includes ex- 'tensive descriptions of positions in which to place the chijdand also some developmental information about when to expectcertain responses from the child. This precise information re-garding expectations facilitates appropriate reterral fortreatment. In addition, some minimal information concerningrecording responses is included. The authors of the manualalso recommend a 16-millimeter color training film (see bibli-ography) demonstrating procedures for administration which isavailable from either:
United Cerebral Palsy Associations, Inc.66 E. 34th StreetNew York, NY 10016
Or
Meyer Children's Rehabilitation InstituteUniversity of Nebraska Medical Center444 S. 44th StreetOmaha, NE 68131
* * * * * * * * * *
References
I. A. Milani-Comparetti and Cidoni, E.A. "Routine Develop-mental Examination in Normal and Retarded Children,"Developmental Medicine and Child's Neurology, Vol. 9,1967, p. 635.
2. Ibid.

-el
51.
ROME OBSERVATION FOR MEASUBEMENT OF THE ENVIRONMENT (liONE5
B. Caldwell, ).970
1
4
s
t

52.-.
HOME OBSERVATION FOR MEASUREMENT OF THE ENVIRONMENT,(HOME)
Bettye M: Caldwell, Robert H. Bradley and Staff,;1980
Publisher: Dr. Bettye M. CaldwellRobert H. BradleyCenter for Child DevelopmeRZ and EducationUniversity of Arkansas at Little Rock33rd and University AvenueLittle Rock, Arkansas 72204
Purposa: This inventory provides a frameWork for,systematicallyand objectively collecting information about, the charac-teristi9s of a young child's environment that might affectcognition and emotional development.
AyA: Infant Inventory (0-3 years)Preschool Inventory (3-6 years
4
Application: This tool can be used to assess any home or childcare envirqnment.
Areas Assessed:Infant Inventory
1. Emotional and verbal responsibility of.mother2. Avoidance of restitution or punishment3. Organization of-physical and temporal environment4. Provision of appropriate play materials5. Maternal involvement with child6. Opportunities for variety in daily stimulation
Preschool Inventory1. Stimulation through toys, games and reading materials2. Positive social responsiveness3. Physical 'environment: safe, cicau and con ducive to
development4. Pride, affection, warmth5. Stimulation of academic behavior6. Modeling,and encouragement of social maturity
f 7. Variety of stimulation8. Physical punishment
.1.

A
Standarization: Infant and Preschool InventoryHOME Inventory (0-3) assessments of 171 Little Rock fami-lies of infants and toddlers were used to calculate themean, standard deMation, and standard error measurementfor each of the HOME (3-3) subscales in the total HOME '
score (117 families for the Preschool). Home envirenmentof mile and female children differed very little.
53
a
Reliability: Infant InventoryThe total mean score increased over two points from the six-month assessment to the 12-month assessment, and another.point between the 12-month'and the 24-month assessment.Intraclass correlations computed determined the 03MEts 1
stability to be acceptable. Factor analysis performed onthe new 45-item Inventory was found to be similar to thatdone the 72-item Inventory.'
.--7 Preschool Inventory' Internal consistency estimate for the total scale was .93.
Stability was estimated utilizing data from 33-familieswhen dhildren were 3 yean and again at 41/2. These co-.
efficients range from r=.05 to r=.70 pointing to the'needfor continued assessments of th;- same household over aperiod of time.
Validity:,
Infant Inventory
Six, 12 and 24-month HOME data from 91 families were com-pared to six SES variables. Correlations remained con-sistent at a moderate level with a slight increase at the24-month period. Various levels of HONE scores.were also ,
compared with Bayley MDI, Stanford-Binet and ITP4_scores.These correlations appear to be moderate.
Preschool InventoryIn comparisons made between the HOME And five SES indices,the highest observed correlation (E=.65) was between ma-ternal education and the subscaie Toys, Games and ReadingMaterial. The rest-were negligible to modest. HOME scoresare found to be significantly related to IQ scores (.58)and SRA achievement test scores (E=.51 to r=.58).

54
The Home Observation for. Measurement of the Environmentis divided into two.separate inventories: an infant inventoryof home stimulation for children who are birth to three yearsof age and an inventory of home stimulation for preschdol,children who are three to six years of age.
The infant inventory consists of 45 items and the pre-school inventory lists a totaf of 55 items. The 55 item pre-school inventory reflects a recent revision of the inventorymade by the authors. They stress that reference be madd tothis 1980 preschool inventory as the "current' version ratherthan the 'final' version of the Inventory, as we are not likelyever to consider the development finished. Were we to do so,
our work might become 'static' rather than 'in process' - - -
and those who know the conceptualization behind the HOME knowthat we believe strongly in the value of process as opposedto status appraisal."' 1
All items from both HOME Inventories are indfvidually ex-plained in detail within the Administration and Scoring sec-tion of Home Observation for Measurement of the EnvironmentMonogynph (Caldwell, Bradley and Staff, 1980, available frompublisher's address on page 52). Scoring on the HOME is doneby placing a "yes" or "no" (based on observation and parentalresponse during the interview) in the appropriate box, whichfollows each item. When the, instrument is used clinically,interviewers can jot down brief notes on the form and notetheir general impressions during the visit. The authors pointout several facts concerning scoring which the home visitorshould keep in mind:
1. " .... all observation items refer to the contem-porary situatfon - - i.e., to conditions that pre-vail at the time of the visit. The Cale periodcovered by the interview items varies but is clearfrom the content of the item."
2. "The present form of the Inventory includes twosubscales which together cover the first six years
of life. Some items on each scale are more appro-priate for the younger half thee the older halfof this age range, or vice versa.

a*
5.5
3. "Inthose instances an attempt has beentoade to,give the item a certain amount of stretch byworking it so as to encompass characteristicactivities of both younger and older children.Change duiing the first few yeers of life is so 'dramatic that some such flexibility in the inter-pretation of items was essential." 2 -
the HOIIE Inventories provide space for recording sub.-scores (total "yes" or "no" items within each of the sub-scales) and a total score. A cover sheet provides space fortranscribing all raw scores for the subscales and then com-puting bbth a total raw scpreand a percentile band placement.
The interview can be accomplished in a home visit ofabout an hour's duration, and the visitor will find that_itcan easily be completed in the time span of one home visit.Concerning training of the individual using the HOME, theauthors state that !Asides being familiar with the items in.the inventor, the individdal Ulaking the home vi.sit should bea good interviewer. They further state that
".... a good interviewa? is.a persoh who can be at'.ease herself or himself in the situAtion, can putthe mother or caregiver at ease, can essily.adjustsubsequent questions to answers given by the mother,and can ask questions in such a"way'to avoid puttithe informant on the defensive and thereby to seconguess the interviewer as to what is the 'right' or7expectee response. (The) goal is to be object e
and accepting, as opposed to approving or disapprov-ing. This is essential if (the interviewer wants to)find out how this person feels and what she does withher child rather than what qfie may think (the inter-viewer) wants her to say." J
The authors do not specifically mention one type of pro-fessional training required of an individual before admini-qration of the HOME other than the preceding reference. Oneof the reasons for this,.perhapp; is the detailed informationprovided in the Administrati9 section of the Home Obsermationfor Measurement of the Environment Monograph. The informationcontained within this section can be extremely valuable to a
.

a
56\
\home visitor using the HOME because it cap provide answerts tomany questions. Content includes making arrangements fo the
;visit, conducting the interview, areas covered in xhe in er-view, wrap-up of the interview, exceptions to standard pro-cedures, scoring, and some miscellaneous questions and an-swers. Each of these content areas is dealt with specificallyand in dethil.
S.
Important to the professional using the HOME'is an under-standing of the basic rationale behind the tool and the usefor which it is intended. There is no intent on the part ofthe authors.to use the score on the HOME to identify "good"or "bad" parents or a "Pood" or "bad" home environment. Theauthors address the issue of possible cultural and SES biasin item selection by including the following in their mono-graph:
"Is this (e.g. administration of the HOME) anelitist procedure? It certalnly looks like one,
does it hot? One could say that the scale measuresnothing but money and wealth and that the,home ofthe poor child would definitely be penalized. To alarge extent, that istrue: however, it is not en-tirely true. For example, several factors have todo with toys and materials provided by the parents tohelp children learn and with whether the family pro-vides what we colloquially call "cultural" experiencesfor their children. There is no doubt that suchthings tend to be associated with higher family in-comes and with higher education. But higher incomeand higher parental education tend to be associatedwith favorable development in children and we couldnot have designed an effective inventory that ig-nored such things.
But we would like to stress again that everyattempt was made to include items that representstimulation and support but do not necessarily mean
meney, social status, or education. Thus, from thestandpoint of the Inventory, a trip to the grocerystore gets as much credit as a trip to an art museum,in that both are likely to be interesting, informa-tive, and stimulating to a young child.

57
Users of the Inventory are urged to rememberthis and not accuse the developers of the instru-ment of elitist tendencies which automatically dis-criminate against one group or another. Taken col-lectively the items in this Inventory are designedto reflect this elusj.ve condition that we refer toas a "quality'life" for children. Original itemselection.was based on a review of the literatureof research findings associated with favorable de-velopment in young children. Probably a quality
life for children requires considerable financialoutlay, and probably it also requires a certainlevel of consciousness-raising in parents aboutthe kinds of experiences which will favorably in-fluence the course of development of their chil-
dren. However, our intent was to.put together aset of items that described the quality of the homeenvironment available to a young child, not to offerany value judgment about whether these character-istics are good or bad for children (or familiesor for the total society). 4
In addition, it is critical that the parents be madeaware-J1E.this fact and that the true purpose of the assess-ment be understood by both the family and the individual using
the tool.
"As a teaching tool, however, the HOME serves
to foster more appropriate interpersonal interactionsbetween parents and children. It can help parents
feel more potent and confident about their parentalabilities to provide an environment that is'responsiveto their chi:id's individual needs, as well as their
own. Used properly, the Inventories can be valuablein reassuring parents about their unique capabilitiesto determine the child's readiness for new or differ-
entstimuli. , It can be a helpful guide in selecting
appropriate learning experiences that correspond with
the child's level of development. Used for the pur-
pose it was created, the HOME can focus on both the
child's changing needs, as well as the parents',re-sourcefulness ip meeting these ongoing needs."

It is suggested that the individual involved in home-centered care who uses the HOME with a given family be careful'about forming judgemental opinions about the home environmentbased on the results yielded by some of Lhe items on the HOME.For instance, it is quite possible that in a low-income familya child may notthave three or more books of his own (Infant
Inventory, Item 45). The home visitor should avoid using thisinformation in a negative manner, but sho-ld approach it in aconstructive, positive way. For example, the parent can begiven suggestions about inexpensive home-made books which canprovide excellent stimulation for a young child.
It is iurther essential that visitors using the HOME beaware that one assessment in the home is not sufficient to de-
termine adequacy of the environment. This tool will be used
must appropriately in,conjunction with other developmental
assessment tools.
"By using the inventories on a serial basis,changes in the environment can be observed in a
systematic and reliable manner. Parents can beoffered valuable feedback on a more objective, con-crete basis and can be assisted in seeing the changesthey were able Lo implement. Changes in the child'sdevelopment can be documented as well." 6
No criteria for referral to other agencies or disciplines
is described in the manual. Referral to other resources must
be at the discrimination of the professioral administering
the tool.
* * *\* * * * * * * *
References
1. Bradley, Robert H., and Caldwell, Bettye M. Home Obser-
vat-Lin for Measurement of the Environment Monograph,Preface, Center for Child Development and Education,College of Education, University of Arkansas at Little,Rock, Arkansas, 72204, no date listed (received April,
1980).
2. Ibid, pp. 98-99.

59
3. Ibid, p. 89.4. Ibid, p. 98.5. Erickson, Mardene L. Assessment and Management of.. Developmental Changes in Children. St. Louis: C.V.
Mosby, 1976, pp. 134-35.6. Ibid, p. 135.

AREAS
SCREENING AND ASSESSMENT
TOOLS -
i
u.w.a.
4
g...'iI
!r.
I
.
.0)
a>
Iii
8
a
Mr..,
,
iZ...4
°
1
;:
ko
isg
I .
3
i:.:I:
i::Ig
*8
.0
1r.lii.
. 4IXtiiig
0:I-144
0::I
5,4
I.
o
V
. . . .
i1
a°
.I:i.
a .
"1i1
tf=I
aa
3f: I
*
4!t
SCREENING TOOLS
_
Denver Developm antalScreening Test
2 wk
'°6Yr
30min
X X r X Yee Yes Yes
Develop mental ScreeningInventory
4 vit
t°m,36
30
ain X X X X X No No No
H ORS Growth Grid0.1e
yr10
X Yes
ASSESSMENT TOOLS
CallierAsums Scale* 0to
4yr
**X X X X X X X No No No
Early InterventionDevelopmental profile
0 rc36
mo
30
min X X X
.
X X X No Yes Yes
Hom e Observation fur Honours-eent of the Environment
0.33. 6
Yr
I
hr X Yee $Ye
Milani ComparettiCiduni Developmental
0.2
yr
5
min X X No No No
*Cognitive Developmental Subsea (0.2 yre ); other individual mca es Included to 9 yrhh Adminl Lon of Cellist Azusa Scale say require more than iJ hour.
C".1 r

63
GROWTH AND DEVELOPMENT BIBLIOGRAPHY
Articles and Books:
Ambron, Sueann,Robinson. Child Development. San Francisco:Rinehart Press, 1975.
Ames, Louise Bates and Ilg, Frances L. Your Three Year Old.New York: Delacorte Press, 1976.
Anderson, Linnea, et al. "Nutrition for Children and Youth.'Nutrition in Nursing. Linnea Anderson, et al.,Philadelphia: J. B. Lippincott Co., 1972, pp. 153-63.
Brazleton, T. Berry. Infants and Mothers: Difference inDevelopment. New York: Dell Publishing Co., Inc. 1972.
Toddlers and Parents: A Declaration ofIndependence. New York: Dell Publishing Co., Inc:, 1975.
Breckenridge, Marian E. and Murphy, Margaret Nesbitt. .Growthand Development of the Young Child. Philadelphia: W. B.Saunders Co., 1969.
Breckenridge, Marian E. and Vincent, E. Lee. Child Development.Philadelphia: W. B. Saunders, 1965.
Caplan, Frank. The First Twelve Months of Life. Princeton,N.J.: Grosset and Dunlap, 1974.
Caplan, Frank. The Second Twelve Months of Life. Princeton,N.J.: Grossc.tt and Dunlap, 1977.
Church, Joseph (ed.) Three Babies: Biographies of CognitiveDevelopment. New York: Random House, 1966.
Cohen, Stewart. Social and Personality Development in Child-hood. New York: MacMillan Publishing Co., Inc., 1976.

64
Connor, Francis P., Williamson, G. Gordon and Supp, John M.(eds.) Program Guide for Infants and Toddlers withNeuromotor and Other Developmental Disabilities. NewYork: Teachers College Press: Teachers College, ColumbiaUniversity, 1978.
Crace, Dixie, "Background of Developmental Milestones inFeeding," in Feeding the Handicapped Child. (ed.) MaryAnn Harvey Smith. Memphis: Child Development Center,University of Tennessee, Center for Health Services,(no date).
Fiorentino, Mary. Moroi'. and Abnormal Development: TheInfluence of Primative Reflexes on Motor Development.Springfield, Ill.: Charles C. Thomas, 1972.
Fraiberg, Selma H. The Magic Years. New York: CharlesScribner's Sons, 1959.
Gardner, D. Bruce. Development in Early Childhood. New York:Harper and Row, 1964.
Gesell, Arnold, et al. The First Five Years of Life. NewYork: Harper and Brothers, 1940.
Gordon, Ira J. The Infant Experience. Columbus, Ohio:Charles E..Merrill Publishing Cp., 1975.
Hellmuth, Jerome (ed.)Infant. New York:
Illingworth, R.S. TheChild: Normal andWilkens Co., 1972.
Lamb, Michael C. (ed.).
Development. New
Exceptional Infant: Vol. I The NormalBrunner/Mazel, Inc., 1967.
Development of the Infant and YoungAbnormal. Baltimore: The William and
The Role of the Father in ChildYork: John Wiley and Sons, 1976.
Malansky, E. "Survey of Infant Feeding Practices." Am. J.Public Health, 64, 1974, pp. 780-85.
McWilliams, Margaret. Nutrition for the Growing Years. 2ndEd. New York: John Wiley and Sons, Inc., 1975, pp. 1-25.

65
Munsinger, Harry. Fundamentals of Child Development. NewYork: Holt, Rinehart and Winston, 1971.
Nesser, Edith G. The Roots of Self-Confidence. Chicago,
Ill.: Science Research Associates, Inc. (259 Erie St.,60611). (no date)
Owen, G.M. et al. "A Study of Nutritional Status of Pre-school Children in thg United States, 1968-1970."Pediatrics, 53, April 1974 Suppl., pp. 597-646.
Palmer, Sushma and Ekvall, Shirley. Pediatric Nutrition inDevelopmental Disorders. Springfield, Ill.: Charles C.Thomas, 1978.
Pipes, Peggy. Nutrition in Infancy and Childhood. S. Louis:C.V. Mosby Co., 1977.
S1fhiefelbusch, Richard L. and Lloyd, Lyle L. (eds.) Language
Perspectives - Acquisition, Retardation and Idtervention.Baltimore: University Park Press, 1974.
Sheridan, Mary D. Children's Developmental Progress. NewYork: Humanities Press, Inc., 1960.
Stone, L. Joseph and Church, Joseph. Childhood and Adolescence.Third Edition. New York: Random Rouse, 1973.
rizard, Barbara and Harvey, David (eds.) Biology of Play.Clinics in Developmental Medicine, No. 62. Philadelphia:
J.B. Lippencott Co., 1977.
Travers, John F. The Growing Child: Introduction to Child
Developmmnt. New York: John Wiley and Sons, 1977.
Wallace, Helen M. "Nutrition and Handicapped Children."Journal of the American Dietetic Association, Vol. 61,1972, pp. 127-33.
Wursten, Helmut. "on the Relevancy of Piaget Theory toOccupational Therapy," American Journal of Occu ationalTherapy, Vol. 28, No. 4 (April '74), pp. 213-16.

4
66
Non-Print Material
"Beyond Survival." (slide/tape)Part I: "Normal Progression of Feeding."Part TT:: "The Feeding Experience."PartYTII: "Problems of Oral Mechanisms and Remedial
Suggestions."Omaha: C. Louis Meyer, Children's Rehab. Institute,University of Nebraska Medical Center.
"Child Development and Child Health." (Five film strips andaudio cassettes) Parents' Magazine Films, Inc.
"Development of the Child: Cognition." (color film)Harper and Row.
"Development of the Child: Cross-Cultural Approach toCognition." (color film) Harper and Row.
"Development of the Child: Infancy." (color film) Harperand Row.
"Development of the Child: Language." (color film) Harperand Row.
"Everyday Problems of Young Children." (Five film strips andaudio cassettes) Parents' Magazine Films, Inc.
"Play and Self Expression." (Five filmstrips and audio cas-. settes) Parents' Magazine Films, Inc.
"The First 18 Months: From Infant to Toddler." (Five film-strips and audiocassettes) Parents' Magazine Films, Inc.
"Tim: His Sensori-Motor Development." (color film) Harperand Row.
"Wrhat Do I See When I See Me?: Emotional and Social Growth inChildren." Set 4: "I See Love - Parent/Chfld Relation-ships." (Five filmstrips and audio cassettes) Parents'Magazine Films, Inc.

67
SCREENING/ASSESSMENT BIBLIOGRAPHY
Articles and Books:
Bardwell, Ann, Krieg, Fred J. and Olion, LaDelle. KnowinRthe Chtld with Special Needs: A Primer. (A Publicationof the Head Start Technical AsSistance and ManagementSystem. Available from Head Start, Office of Child De-velopment, Region V, 300 S. Wacher Dr., Chicago, Ill.
60606.) 1973.
Barnard, Kathryn E. and Powell, Marcene L. Teaching the Men-tally Retarded Child! A Family Care Approach. St. Louis:C. V. Mosby Co., 1972, pp. 44-82.
Bradley, R. H. and Caldwell, Bettye M. "Screening the Environ-ment" American Journal Orthopsychiatry, 48 (1), Jan. 1978,pp. 114-130.
Christakis, G. "Nutritional Assessment in Health Programs."American Journal of Public Health, Vol. 63 supp., Nov.1973, pp. 1-52.
Currie, Catherine. "Evaluation Function of MR Children Throughthe Use of Toys and Play Activities." American Journal ofOssupational Therapy., XXIII, 1, 1969, pp. 35-43.
Egan, Illingworth, and MacKeith. Developmental Screening 0-5Years. London: Spastics International Medical Publicationin Association with William Herneman Medical Books, Ltd.,1971.
Ekvall, Shirley. "Assessment of Nutritional Status." PediatricNutrition in Developmental Disorders. Eds. Sushma Palmerand Shirley Ekvall. Springfield, IL: Charles C. Thomas,1978, pp.
Erickson, Marcene. Assessment and Management of DevelopmentalChanges in Children. St. Louis: C. V. Mosby Co., 1976.
Frankenburg, William and Dodds, Josiah. "The Denver Develop-mental Screening Test." Journal of Pediatrics, Vol. 71,
No. 2, August 1967, pp. 181-91.
61,t

68
Johnston, Robert B. and Magrab, Phyllis R. DevelopmentalDisorders: Assessment, Treatment, Education. Baltimore:University Park Press, 1976.
Krajicek, Marilyn J. and Tearney, Alice I. (Eds.). Detectionof Developuentall Problems in Children. Baltimore:University Park1Press, 1977, pp. 1-5, 31-45.
"Nutrition and Feeding of Children with Developmental Delaysand Related Problems." Ed. Pipes, P. Nutrition inInfancy and Childhood. C. V. Mosby Co., 1977, pp. 170-84.
\
Nutritional Disorders of Children. Prevention, Screening andFollow-Up. U. S. Dept. of HEW.- DREW Public No. (HSA)77-5104, Reprinted, 1977.
Olion, LaDelle and Rodabaugh, Jeroldine. A Selected Listing,of Instruments for Screening and Assessment. (A Publi-cation of the Head Start Technical Assistance and ganage-ment System. Available from Head Start, Office of ChildDevelopment, Region V, 300 S. Wacher Dr., Chicago, Ill.60606.) (no date)
O'Neil, Sally M. "Behavior Management of Feeding." Nutritionin Infancy and Childhood. Ed. Peggy Pipes. St. Louis:C. V. Mosby, 1977, pp. 170-184.
Pipes, Peggy. "Assessing Food and Nutrient Intake." Asiess-ment and Management of Developmental Changes in Children.Ed. Marcene Erickson. St. Louis: C. V. Mosby Co., 1976,pp. 137-151.
Rindenour, Nina and Johnson, Isabel. Same Special Problems or%Cnildren Aged 2-5 Years. New York: Child Study Ass. ofAmerica, Inc. (9 E. 89th St., 10028), 1969.
Ritchie, Bonnie, et.al., Manual of Assessment Instruments forthe MR/DD Population. Columbus, Ohio: Nisonger Centeron Mental Retardation and Developmultal Disabilities,The Ohio State University, 1978.
Robert,Christopher. "Evaluation of Deviation in FeedingAbilities." Feeding the Handicapped Child. Ed. Mary AnnHarvey Smith. Memphis: Child Development Center, Univ.of Tennessee, Center for Health Services, (no date).
6t;

69
Screening and Assessment of Young Children at Developmental
Risk. The President's Committee on Mental Retardation.Washington, D. C.: HEW Pub: No. (OS) 73-90, March, }.973.
Smith, Mary Ann Harvey, Ed. Feeding the Handicapped Child'.
Memphis: Child Development Center, University of Tennessee,
Center for Health Services, (no date).
Guides for Nutritional Assessment of the Mentally
Retarded and Developmentally Disabled. MempHis:
Child Development Center, University of Tennessee,,
Center for Health Services, 1976.
Thorpe, Helen S. and Werner, Emery E. "Developmental Screening
of Preschool Children: A Critical Review of Inventories
Used in Health and Education Programs." Pediatrics, Vol.
53, No. 3, March 1974, pp. 362-369.
Non-Print Media:
"MCRI-*Milani-ComparLtti fest" (color film), Meyer Children's
Rehabilitation Institute, University of Nebraska Medical
Center.
.4"