abp practice performance improvement summit american board of radiology chicago, il august 19, 2006...
TRANSCRIPT

ABP
Practice Performance Improvement Summit
American Board of Radiology
Chicago, Il
August 19, 2006
Paul V. Miles MD
Vice President, Director of Quality Improvement
And Practice Assessment
American Board of Pediatrics
MOC Part IV: The Role of the ABP in Improving Quality of Care for Children
ABP
“I am sorry for you, young men (and women) of this generation. You will do great things. You will have great victories, and standing on our shoulders, you will see far, but you can never have our sensations. To have lived through a revolution, to have seen a new birth of science, a new dispensation of health, reorganized medical schools, remodeled hospitals, a new outlook for humanity, is not given to every generation.”
…Sir William Osler

ABP
Demands on Physicians for Quality of Care
Professional obligation
Maintenance of board certification
Career development
Maintenance of licensure
Credentialing
Malpractice
Pay for performance

ABP
The Program for Maintenance of Certification in Pediatrics™
PMCP-G™
Generalist Pediatricians
PMCP-S™
Pediatric Subspecialists

ABP
PMCP-GPMCP-G PMCP-SPMCP-S
Part One: Professional Standing
Part Two: Lifelong Learning
Part Three: Cognitive Expertise
Part Four: Performance in Practice
Valid license, no restrictions
ABP Knowledge self assessmentAAP PREP (ABP approved)ABP Decision Skills Assessment
Secure, proctored exam
ABP Knowledge self assessment via literature review AAP Neo Reviews (ABP approved)
A. Pediatric CAHPS Survey (and Peer Survey)
B. eQIPP or eQIPP-like modules or local QI effort
ABP: Maintenance of Certification
ABP
Part 1
Valid, unrestricted license – Maintenance of licensure (MOL)Pediatric patient survey (CAHPS) 2007Professionalism survey - future

ABP
Existing Available
ABP Knowledge self-assessment 2006
ABP Decision Skills 2006
AAP PREP (broad based general knowledge)
2006
Subspecialty modules (current best articles)
2006-10
Subspecialty prep programs (eg. Neoreviews)
2006-10
In Development
Patient Safety Self Assessment 2008
QI Self Assessment & QI Basics Module 2008
Part 2: Knowledge Self Assessment (Open book, low stakes, requires passing score)

ABP
ABP is considering requiring the secure exam every 10 years instead of every 7
years
Part 3

ABP
Part 4
Part 4 Practice Assessment & Improvement
Option A Option B Web based modules Participate in EstablishedSuch as eQIPP or ABMS Improvement ProjectPatient Safety Module (including attestation forms)
Complete QI Knowledge Self Assessmentor Stand Alone QI Module with Assessment
(Required with Option B)
Credit for Part IV MOC
Diplomate enrolls in MOCOn the ABP Web-site

ABP
Part 4Existing (Web based) Available
eQIPP modules (Asthma & ADHD)
2006
In Development – 4A Web based
ABMS Patient Safety Module 2007
eQIPP Nutrition & other modules
2007-10
Performance Improvement Modules (PIMs)
2007
In Development – 4B
Credit for ongoing projects 2007

ABP
MedicalKnowledge
QualityImprovementKnowledge
MeasurementImprovement
Re Measurement

ABP
eQIPP allows the learner to quickly assess their practice online.

ABP
A real-time data analysis allows the learner to begin to identify opportunities for improvement.

ABP
eQIPP offers an interactive learning environment. The program also includes practical, easy-to-use tools that can be implemented quickly into the office setting.

ABP
After completing the clinical content, the learner uses the Model for Improvement to identify opportunities for improvement in their practice.

ABP
Within each step, the learner will receive advice for identifying, prioritizing, refining, and launching new improvement cycles.

ABP
eQIPP subscribers have access to the modules for three years. You will be able to track your progress, and monitor your successes over time.
ABP
Additional eQIPP Modules
• Nutrition• Bright futures (well child care)• Six to ten additional common topics by
2009

ABP
ABMS Patient Safety Module
Accurate and Complete Medication List Safer Prescription and Medication Order Writing Accurate and Complete Allergy Information Hand Hygiene Correct Patient/Site/Procedure Critical Test Results Notification

ABP
Performance Improvement Modules (PIMs)
DiplomateRegisters &
ChoosesModule
DiplomateMeasures PracticeQuality
DiplomateChooses ChangePackage
DiplomateRe Measures
Quality
ClinicalData
SurveyData
Rapid Cycle Improvement
ChangePackage
1
ChangePackage
2
ChangePackage
3

ABP
Annotated Comparative Run Chart
0%10%20%30%40%50%60%70%80%90%
100%
Baseline Test #1 Test #2 Test #3 Test #4
Your Practice Comparison
AnnotationAnnotation
Annotation
Annotation
Annotation
Goal
Time

ABP
Part 4
Part 4 Practice Assessment & Improvement
Option A Option B Web based modules Participate in EstablishedSuch as eQIPP or ABMS Improvement ProjectPatient Safety Module (including attestation forms)
Complete QI Knowledge Self Assessmentor Stand Alone QI Module with Assessment
(Required with Option B)
Credit for Part IV MOC
Diplomate enrolls in MOCOn the ABP Web-site
ABP
Pass a QI Knowledge Self Assessment Exercise: an open book multiple choice question exam Part 2 (in development)Complete a valid QI project
Competence in Quality Improvement

ABP
ABP Standards for Part 4 B
Standards for Established Programs to receive ABP approval for Part 4Standards for meaningful participation by a diplomate in an Established Program

ABP
“Perfect Care”: composite measure of severity classified, identified management plan, and controller medications for patients with persistent asthmaCopyright © 2005 Cincinnati Children’s Hospital Medical Center; all rights
reserved
ImprovementCollaborative on
Reliability|q
PerformanceFeedback Reports
|q
P4PProgram
|q
qP4P
Deadline
zSelf -
ManagementCollaborative
Initiated
qWeb-based
RegistryLaunched
ProjectInception
|q
q"Perfect Care"
IncludingFlu Shot
Long Term Goal = 95%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Oct 0
3
Nov 0
3
Dec 0
3
Jan
04
Feb
04
Mar
04
Apr 0
4
May
04
Jun
04
Jul 0
4
Aug 0
4
Sep 0
4
Oct 0
4
Nov 0
4
Dec 0
4
Jan
05
Feb
05
Mar
05
Apr 0
5
May
05
Jun
05
Jul 0
5
Aug 0
5
Sep 0
5
Oct 0
5
Nov 0
5
OVPCA Network Practice 1 Practice 2 Practice 3 Practice 4 Practice 5 Practice 6
Cumulative % of Asthma Population with "Perfect Care": Network and Select Practices

ABP
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Oct 0
3
Nov 0
3
Dec 0
3
Jan 0
4
Feb 0
4
Mar 0
4
Apr 0
4
May 0
4
Jun 0
4
Jul 0
4
Aug 0
4
Sep 0
4
Oct 0
4
Nov 0
4
Dec 0
4
Jan 0
5
Feb 0
5
Mar 0
5
Apr 0
5
May 0
5
Jun 0
5
Jul 0
5
Aug 0
5
Sep 0
5
Oct 0
5
Commercially Insured Medicaid/Uninsured
Cumulative % of Asthma Population with "Perfect Care":Commercial vs. Medicaid/Uninsured
Copyright © 2005 Cincinnati Children’s Hospital Medical Center; all rights reserved
ABP
Subspecialty Care: What to do about small numbers?
Collaborative practice with standardization of careEnroll patients in multicenter studies with shared data to determine best practices

ABP
Acute Lymphoid Leukemia
0%10%20%30%40%50%
60%70%80%90%
100%
1960-63 70-73 74-76 77-79 80-82 83-90
Simone J., Lyons, J: J Clin Oncology 1998 Sep;16(9):2904-5
5 y
ear
surv
ival ra
te
ABP
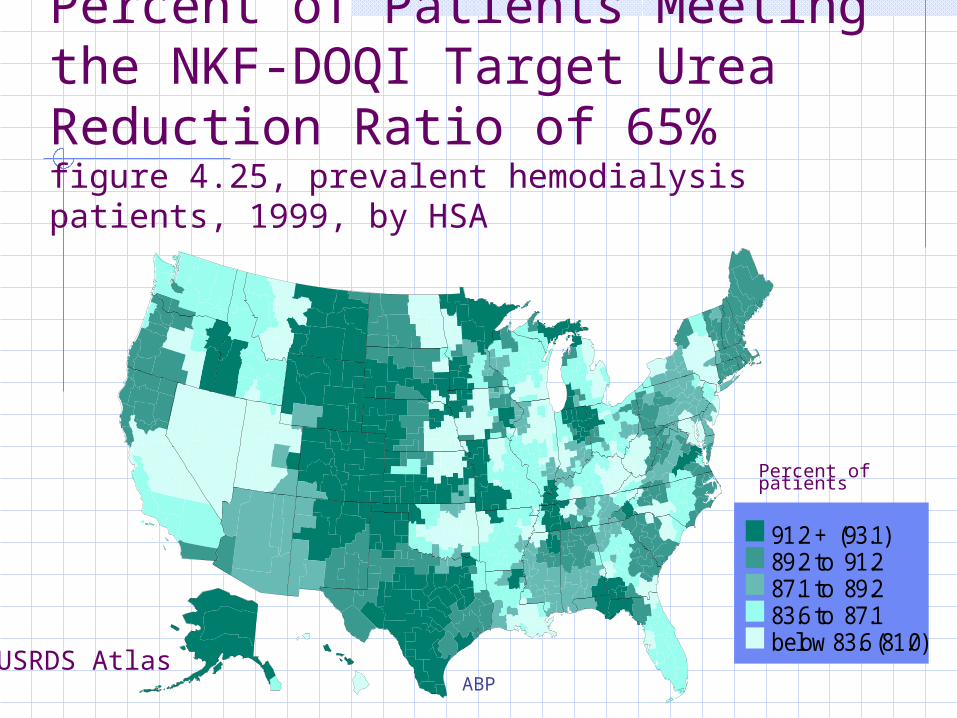
Percent of Patients Meeting the NKF-DOQI Target Urea Reduction Ratio of 65%figure 4.25, prevalent hemodialysis patients, 1999, by HSA
Percent of patients
91.2 + (93.1)89.2 to 91.287.1 to 89.283.6 to 87.1below 83.6 (81.0)
USRDS Atlas

ABP
Quality of Care (ESRD)
0
5
10
15
20
25
30
35
<50% 50-54% 55-59% 60-64% 65-69% 70-74% 75-79% 80+%
Urea Reduction Ratio (URR)
perc
ent
of p
atie
nts
Oct-Dec '93Oct-Dec '94Oct-Dec '95Oct-Dec '96Oct-Dec '97
Average URR1993: 62.7%1994: 63.8% 1995: 65.5%1996: 66.8%1997: 68.0%
* Sixteen Network areas participated in the first ESRD Core Indicators assessment (Oct-Dec 1993); all Networkareas participated in subsequent years.

ABP
Adequacy of Hemodialysis
Hemodialysis Dose by Race
4653
70 73 7685 87
3643
5463
69 7083 8462
0
20
40
60
80
100
1993
1994
1995
1996
1997
1998
1999
2000
Adequate
Hem
odia
lysi
s D
ose
, %
WhitesBlacks
Sehgal A, JAMA 2003;289:1996-1000

ABP
Initial Efforts in Subspecialty Care
PIBDnet – Inflammatory Bowel DiseaseCystic fibrosis - PulmonologyHigh risk newborns – NeonatologyCatheter Related Blood Stream Infections in PICU – Critical careNeonatal Congenital Heart Disease – Cardiology

ABP
Prevention of Catheter-related Blood Stream Infections
Marlene R. Miller, M.D., M.Sc.Christopher T. McKee, DOIvor Berkowitz, M.D.Claire Beers, R.N., M.S.N.
Johns Hopkins Children’s Center and Hospital Epidemiology and Infection Control

ABP
Subsequent BSI Outcomes
time period
Rate
of BSI per 1000 C
L Days
454137332925211713951
25
20
15
10
5
0
_X=3.99
UCL=15.19
LB=0
1 21
Rate of BSI per 1000 CL Days (reordered)
PRE POST

ABP
New Products and Programs that ABP has invested in
Part 2 General pediatric knowledge self
assessment Decision skills exercise Subspecialty specific (13
subspecialties) knowledge modules Quality Improvement knowledge self
assessment exam

ABP
Part 4 Web based modules
AAP eQIPP nutrition module Performance Improvement Modules Patient safety module
Practice based QI efforts Pediatric GI – inflammatory bowel disease database
and collaborative Critical care – catheter related blood stream infections Cardiology – Congenital heart disease project General pediatrics – RWJF funded Improving
Performance in Practice (IPIP) with internal medicine and family medicine
New Products and Programs that ABP has invested in

ABP
A collaboration of four major
national pediatric
organizations formed to
measurably improve
the quality of health care for
America’s children.
Alliance for Pediatric Quality

ABP
Timeline
Certificates expiring between 2003 and 2009 – Parts 1 and 3: Valid license and secure examCertificates expiring in 2010 and 2014 – all four Parts: One activity each in Parts 2 and 4