abortion policies in u.s. teaching hospitals
TRANSCRIPT

Dow
nloadedfrom
https://journals.lww.com
/greenjournalbyBhD
Mf5ePH
Kav1zEoum1tQ
fN4a+kJLhEZgbsIH
o4XMi0hC
ywCX1AW
nYQp/IlQ
rHD33D
9/FQ5Fz8kYutrkU
fO/NQXJavfw
8br52Oz8Fhq0jKkH
slPkFeADRw==
on06/08/2020
Downloadedfromhttps://journals.lww.com/greenjournalbyBhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD33D9/FQ5Fz8kYutrkUfO/NQXJavfw8br52Oz8Fhq0jKkHslPkFeADRw==on06/08/2020
Original Research
Abortion Policies in U.S. Teaching HospitalsFormal and Informal Parameters Beyond the Law
Varvara B. Zeldovich, MD, PhD, Corinne H. Rocca, PhD, MPH, Callie Langton, PhD, Uta Landy, PhD,Elizabeth S. Ly, MPH, and Lori R. Freedman, PhD
OBJECTIVE: To evaluate the prevalence and features of
policies regulating abortion in U.S. teaching hospitals.
METHODS: In this mixed-methods study, we con-
ducted a national survey of obstetrics and gynecology
teaching hospitals (2015–2016) and qualitative inter-
views (2014 and 2017) with directors at obstetrics
and gynecology residency programs. We asked partic-
ipants about hospital regulations on abortion and their
perceptions of the nature and enforcement of these
policies. Interview analysis was conducted with
a grounded theoretical approach and informed devel-
opment of the survey. The prevalence of policies was
described using survey data; differences in policy
structures by region were analyzed using a series of
logistic regression models.
RESULTS: Directors from 169 of 231 eligible training
programs responded to the survey (73%). Institutional
policies limited abortion beyond state law in 57% of
teaching hospitals, most commonly in the Midwest and
South (odds ratio [OR] 4.3, P,.01 for Midwest; OR 4.0,
P5.001 for South vs Northeast). Policies varied in form
(written and unwritten) and restricted abortion based on
the indication for the procedure and gestational age.
Nonmedically indicated, or “elective” procedures were
more commonly restricted (48% of sites reporting any
policy and 25% prohibiting these abortions altogether)
than medically indicated ones (28% of sites reporting
any policy.) Policies were created by those with institu-
tional power, including hospital leadership and obstetrics
and gynecology department chairs, and were perceived
to be motivated by personal beliefs and a desire to avoid
controversy. Rules were commonly enforced by medical
specialists, hospital ethics committees, and department
chairs. Qualitative data highlighted the convoluted nuan-
ces of these policies, which often put clinicians at odds
with their professional mandates.
DISCUSSION: Reportedly driven by broader institu-
tional interests, obstetrics and gynecology teaching
hospital policies often restricted abortion beyond
state law to the detriment of abortion access and
training opportunities. Vague or unwritten abortion
policies, although difficult to navigate, gave health
care providers some agency and flexibility over their
practices.
(Obstet Gynecol 2020;135:1296–305)
DOI: 10.1097/AOG.0000000000003876
Abortion is one of the most common medical pro-cedures in the United States, with one in four
women having an abortion in her lifetime.1 Studieshave repeatedly demonstrated the safety of abortionin both outpatient and hospital settings.2 Althoughmost abortions (95%) are performed in outpatientfacilities,1 hospital-based abortion is often the onlyoption for women with complex medical needs.3
U.S. federal law permits abortion until viabilityand allows states to narrow parameters within that. Inaddition, individual institutions have been reported torestrict abortion more narrowly than state law.4 These
From the Department of Family and Community Medicine, University ofCalifornia, San Francisco, San Francisco; Advancing New Standards inReproductive Health (ANSIRH) and the Bixby Center for Global ReproductiveHealth, Department of Obstetrics, Gynecology and Reproductive Sciences, Schoolof Medicine, University of California, San Francisco; and the University ofCalifornia, Berkeley, School of Public Health.
Supported by the Kenneth J. Ryan Residency Training Program in Abortion andFamily Planning.
Presented at the Society for Family Planning’s annual meeting, November 14–16, 2015, Chicago, Illinois, and at the Society for Family Planning’s annualmeeting, October 13–15, 2017, Atlanta, Georgia.
The authors thank the Kenneth J. Ryan Program for supporting this work andAriana Bennett for scientific review of the manuscript.
Each author has confirmed compliance with the journal’s requirements forauthorship.
Corresponding author: Lori R. Freedman, PhD, ANSIRH, Department ofObstetrics, Gynecology and Reproductive Sciences, UCSF, Oakland, CA; email:[email protected].
Financial DisclosureCallie Langton disclosed that she is currently employed at the Susan ThompsonBuffett Foundation. The other authors did not report any potential conflicts ofinterest.
© 2020 by the American College of Obstetricians and Gynecologists. Publishedby Wolters Kluwer Health, Inc. All rights reserved.ISSN: 0029-7844/20
© 2020 by the American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
1296 VOL. 135, NO. 6, JUNE 2020 OBSTETRICS & GYNECOLOGY

restrictions can decrease the availability of abortionand result in negative health outcomes for certainpatient populations.5
The Accreditation Council for Graduate MedicalEducation (ACGME) requires obstetrics and gynecol-ogy residency programs to provide access to abortiontraining,6 but research shows that many residentsgraduate with insufficient abortion procedural skills7
and seek additional training after residency.8 In fact,hospital policy is the most commonly reported restric-tion that interferes with obstetrics and gynecology res-ident abortion training.9
Given that teaching hospitals are critical sourcesof medically complex abortion care and the primarytraining grounds for physicians, understanding thecharacteristics of hospital-level abortion restrictionscan help to clarify how they affect patient care andclinician training. In this mixed-methods study, weconducted a national survey of obstetrics and gyne-cology teaching hospitals and interviews with trainingprogram directors to document the prevalence andnature of hospital regulation of abortion.
METHODS
The study was composed of two sets of qualitativeinterviews with a quantitative national survey con-ducted in between and was approved by the Univer-sity of California, San Francisco Institutional ReviewBoard (study number 12-11246, initially approved onJanuary 31, 2014). The first set of qualitative inter-views, conducted in 2014, explored obstetrics andgynecology residency and site director perceptions ofhospital abortion policies and approval processes.Results from these interviews informed the develop-ment of the national survey of U.S. obstetrics andgynecology residency training program directors,conducted 2015–2016, to understand the prevalenceof different policies and enforcement mechanisms. Asecond round of qualitative interviews was conductedin 2017 at the close of the national survey to balancethe sample by residency type and to confirm sufficientthematic saturation.
We recruited interviewees from a geographicallydiverse mix of obstetrics and gynecology residencyprograms around the country and purposively sam-pled from Kenneth J. Ryan Residency TrainingPrograms in Abortion and Family Planning. Weaimed to include at least three residencies in each ofthe four regions of the United States. A trainedresearch assistant sent emails to three to five programdirectors in each of the Southern, Midwestern, East-ern, and Western regions on a rolling basis to ask tointerview people most knowledgeable about their
hospital’s abortion policies and practices, until at leastthree were completed in each region. We selectedRyan programs because they have an explicit commit-ment to abortion training with the expectation thattheir faculty would be most willing to share theirthoughts on this sensitive topic and be willing to refercolleagues to participate. We focused on hospitalswith obstetrics and gynecology residencies, assumingthat a majority of residencies would likely have somesort of abortion service given the 1996 U.S. ACGMEabortion training mandate.6
In 2014, we conducted a first round of in-depth30–60-minute interviews with residency program di-rectors, abortion training site directors, or both, ateach responding institution. Interviews included eightopen-ended questions about hospital abortion prac-tice, policies, authorization, and enforcement, withseveral follow up questions to each asked only if theinformation was not volunteered spontaneously.Some examples were: “What abortion services doesyour hospital provide?”, “Are some abortions not al-lowed in your hospital? Which ones?”, “Do you everneed to get authorization to do an abortion proce-dure?”, and “What’s that process like?” Questionswere asked in the order most organic to the conver-sation in order to maximize rapport and allow thestory to unfold in the interviewee’s own words. Inter-views were conducted by L.R.F., a sociologist withextensive experience conducting qualitative inter-views with professionals in the field of obstetrics andgynecology.
Interviews were recorded and transcribed, andtranscriptions were uploaded into Atlas.ti, a qualitativedata management software program. Atlas.ti allowsqualitative researchers to view all transcripts and thenassign codes to segments of the texts, allowing for anorganized analysis. Codes represent behaviors orconcepts that give insight into the research question.Code output is then generated to group similar textsegments together so that interviewees’ experiencesand statements can be compared and contrasted.The software program does not conduct analysis butprovides a structure for researchers to analyze the datain a systematic way.
Two authors (V.B.Z. and L.R.F.) coded the tran-scripts together, developing consensus on codebookdefinitions through an iterative process of coding andreassessing jointly. The codebook definitions werefinalized after four transcripts and then appliedthroughout the rest. The analysis was conducted witha modified grounded theoretical approach that wasboth iterative and adaptive; we used insights fromearly interviews to inform subsequent survey
© 2020 by the American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
VOL. 135, NO. 6, JUNE 2020 Zeldovich et al Teaching Hospital Abortion Policies 1297

development (below) and further qualitative inquiry.In 2017, the second round of interviews was added totest whether the themes that arose remained salientover time and to include data from obstetrics andgynecology residencies without Ryan programs.These interviewees were drawn from a geographicallybalanced set of teaching programs with abortiontraining, referred by members of the professionalnetworks of one the coauthors (U.L.).
We sought to survey a residency program or sitedirector at all obstetrics and gynecology teachinghospitals about their institution’s abortion policies.Contact information for all ACGME-accreditedobstetrics and gynecology residency programs andprogram directors in the United States, excludingmilitary programs and those in Puerto Rico, wasdrawn from a publicly available ACGME database.An email introducing the study was sent to allresidency directors, noting its endorsement bythe President of the Association of Professors ofGynecology and Obstetrics. Three to seven dayslater, we emailed each residency director to for-mally invite them to participate. In order to ensurethe survey was completed by the person mostknowledgeable about abortion provision, we askedresidency directors to send us the contact informa-tion of the site director of the abortion training pro-gram if they themselves did not serve in this role.Emails were sent via secure Qualtrics system andlinked to an online consent form explaining thestudy purpose, risks, and benefits. Participantschecked a box indicating consent and continued tothe survey. The survey included modules aboutInstitutional Policy and Policy Enforcement, withfive to 14 multiple choice questions, some of whichallowed for open-ended responses. Skip patternswere preprogrammed into Qualtrics to ensure re-spondents flowed through the survey appropriately.After completing the survey, participants receiveda $25 gift card for remuneration. For prospectiveparticipants who did not respond to the survey invi-tation, we sent up to three additional emails. Papersurveys were sent to prospective participants whodid not respond electronically; the nine paper sur-veys returned were entered into the Qualtrics data-base by the data manager. Data were collected fromOctober 2015 to February 2016 and managedthrough secure Qualtrics databases.
Catholic affiliation of surveyed institutions wasqueried specifically, because extensive data docu-ment the significant effects of Catholic affiliation onprovision of abortion care and training at thesehospitals.10 Affiliation of sites was determined
through a national database of Catholic-affiliatedhospitals kept by MergerWatch, a nonprofit orga-nization that tracks the growth of religious healthcare.11
Survey items were developed based on the mostfrequently occurring themes from qualitative inter-views. For instance, given the high frequency withwhich qualitative participants said policies were basedon reasons for the abortion, we asked separately aboutpolicies affecting “nonmedically indicated” abortions(sometimes called “elective,” an abortion for reasonsother than maternal health, fetal health, rape, orincest) and “medically indicated” (reason of maternalor fetal health, rape, or incest). Although this demar-cation of abortion types has been critiqued for rein-forcing a problematic hierarchy of abortionlegitimacy,12 we chose to use these categories toreflect the language used by health care providersthemselves in the interviews and to most accuratelyquantify the policies in place.
Similarly, given the emphasis on the divisionbetween written and unwritten policies thatemerged from the qualitative interviews, we askedabout the existence of each. Written policies wereconsidered those formally codified, and unwrittenpolicies were rules set informally by hospital lead-ers. For enforcement of policies, we differentiatedbetween the need to get approval (a signature orverbal agreement from another party) and the needto notify someone (communication with anotherparty about a planned abortion, but not requiringa response to proceed.)
In order to define institutional policies thatrestricted abortion beyond state legal limitations,survey respondents were first queried about thegestational limits to which they were allowed toprovide abortion care based on state law, and allparticipants were able to answer. Subsequent ques-tions asked participants to specifically identify policiesthat restricted abortion provision further than theirstate’s law. All respondents were licensed physiciansand directors of an obstetrics and gynecology resi-dency training program that provides abortion care,thus we believe these physicians were knowledgeableof the legal boundaries of the care they provide andwere able to describe deviations from the state lawwithin their institutions.
We investigated differences in response rates byresidency site characteristics using a series oflogistic regression models. We described site andrespondent characteristics, as well as the types ofpolicies in place, and who makes and enforces thepolicies. We used logistic regression to investigate
© 2020 by the American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
1298 Zeldovich et al Teaching Hospital Abortion Policies OBSTETRICS & GYNECOLOGY
differences in policy structure by U.S. region. Thefew missing responses in the survey data (less than2% for any variable) were removed from thedenominator for the proportions presented. Allanalyses were conducted with Stata 15.
RESULTS
For the qualitative portion, 18 obstetrics and gynecol-ogy faculty members were interviewed from 15residency training programs throughout the UnitedStates. (four in the West, three Northeast, fiveMidwest, three South). The first round, consisting of13 interviews, were completed with faculty at 10 sites;round two included five additional interviews fromfaculty at five sites.
Of the 231 obstetrics and gynecology programscontacted, directors from 169 (73%) completed thesurvey. Respondents represented all four geographicregions (Table 1). Five percent represented Catholic-affiliated programs. Forty-three percent of respond-ents were residency program directors, and 57% werethe training directors at the particular site where mostabortions were performed. The average respondent’stenure at their site was 12.5 years.
The geography of responding sites were notsignificantly different from nonresponding sites. Re-sponding sites had a higher average number ofresidents (5.7) compared with nonresponding sites(4.4; P,.001). Non–Catholic-affiliated sites were morelikely to respond (76%) than Catholic-affiliated (42%;P,.01), although only 8% of target sites were Catho-lic-affiliated.
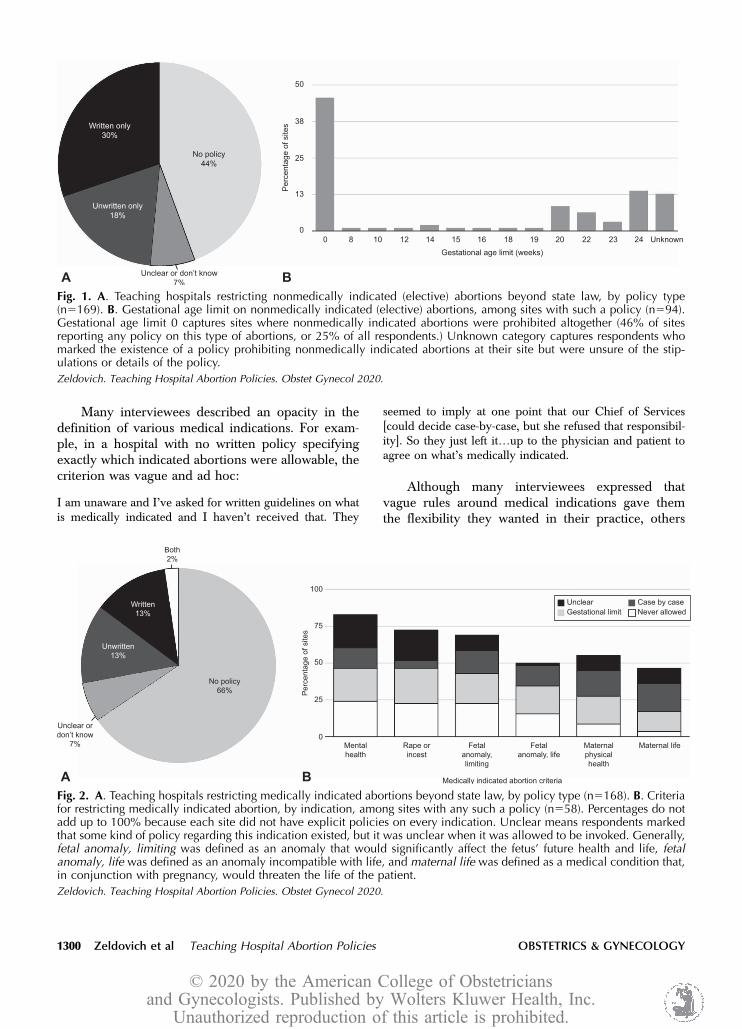
A majority of survey respondents (57%) reportedthat their training hospital had some sort of policythat restricted abortion provision beyond what isallowable under their state’s laws. Policies were es-tablished based on the reason given for the abortionand often divided into “nonmedically indicated” and“medically indicated” procedures. It was more com-mon for policies to restrict nonmedically indicatedabortions (48% of sites) than medically indicatedones (28%), and a quarter of institutions restrictedboth types beyond state law (Figs. 1A and 2A fortypes of policies.)
In the nearly half (48%) of institutions thatrestricted nonmedically indicated abortions, policieswere specified further: a quarter of all sites (25%)prohibited these types of abortions altogether, andmany restricted procedures to a specific gestationalage lower than that set by state law (Fig. 1B).
There were regional differences in hospital poli-cies limiting nonindicated abortion provision, but notfor indicated abortions. Teaching hospitals in the
Midwest (63%) and South (61%) were more likely tolimit nonindicated abortions beyond state law thanthose in the Northeast (28%) (odds ratio 4.3, P,.01 forMidwest; odds ratio 4.0, P5.001 for South). Forty-four percent of surveyed institutions in the West lim-ited nonindicated abortions. However, there were nosignificant differences in prevalence of policies limit-ing indicated abortions (34% Midwest, 28% South,21% Northeast, 33% West).
For medically indicated abortions, hospitalpolicies reflected a wide variety of required criteria,including maternal and fetal indications in a spec-trum of severity. Institutions delineated that someindications were never allowed, others were allow-able on a case-by-case basis, and some wererestricted to below a certain gestational age (Fig.2B.) Some respondents marked “unsure” or“unclear,” suggesting that some kind of policyregarding the indication existed, but it was unclearwhen and how it was to be invoked. Mental healthand rape or incest were the indications most com-monly limited by hospital policies, with fetal indi-cations following, and maternal indicationsrelatively less scrutinized (Fig. 2B).
Interviewees described a slew of nuanced rulessurrounding medical indications. For example, oneinterviewee explained that the only abortions allowedin her hospital for fetal indications were for lethalanomalies, “So trisomy 21, Down’s syndrome, wouldnot qualify. Trisomy 13 and 18 would.”
Table 1. National Survey of U.S. Obstetrics andGynecology Teaching Hospitals: Site andRespondent Characteristics (N5169)
Attribute Value
Geographic regionNortheast 53 (31)Midwest 35 (21)South 54 (32)West 27 (16)
Catholic affiliated 8 (5)Mean residency size* 5.762.3Respondent type
Residency director 72 (43)Primary abortion site director 97 (57)
Respondent genderFemale 112 (67)Male 54 (33)
Respondent years at site† 12.569.3
Data are n (%) or mean6SD.*Average reported number of residents enrolled in program per
year.†Average reported number of years survey respondent has worked
at the site (n5163).
© 2020 by the American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
VOL. 135, NO. 6, JUNE 2020 Zeldovich et al Teaching Hospital Abortion Policies 1299
Many interviewees described an opacity in thedefinition of various medical indications. For exam-ple, in a hospital with no written policy specifyingexactly which indicated abortions were allowable, thecriterion was vague and ad hoc:
I am unaware and I’ve asked for written guidelines on whatis medically indicated and I haven’t received that. They
seemed to imply at one point that our Chief of Services[could decide case-by-case, but she refused that responsibil-ity]. So they just left it.up to the physician and patient toagree on what’s medically indicated.
Although many interviewees expressed thatvague rules around medical indications gave themthe flexibility they wanted in their practice, others
Fig. 1. A. Teaching hospitals restricting nonmedically indicated (elective) abortions beyond state law, by policy type(n5169). B. Gestational age limit on nonmedically indicated (elective) abortions, among sites with such a policy (n594).Gestational age limit 0 captures sites where nonmedically indicated abortions were prohibited altogether (46% of sitesreporting any policy on this type of abortions, or 25% of all respondents.) Unknown category captures respondents whomarked the existence of a policy prohibiting nonmedically indicated abortions at their site but were unsure of the stip-ulations or details of the policy.
Zeldovich. Teaching Hospital Abortion Policies. Obstet Gynecol 2020.
Fig. 2. A. Teaching hospitals restricting medically indicated abortions beyond state law, by policy type (n5168). B. Criteriafor restricting medically indicated abortion, by indication, among sites with any such a policy (n558). Percentages do notadd up to 100% because each site did not have explicit policies on every indication. Unclear means respondents markedthat some kind of policy regarding this indication existed, but it was unclear when it was allowed to be invoked. Generally,fetal anomaly, limiting was defined as an anomaly that would significantly affect the fetus’ future health and life, fetalanomaly, life was defined as an anomaly incompatible with life, and maternal life was defined as a medical condition that,in conjunction with pregnancy, would threaten the life of the patient.
Zeldovich. Teaching Hospital Abortion Policies. Obstet Gynecol 2020.
© 2020 by the American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
1300 Zeldovich et al Teaching Hospital Abortion Policies OBSTETRICS & GYNECOLOGY

were critical of individual clinicians having the powerand responsibility of decision making, suggesting thatthe lack of definition allowed for overly subjective andhence biased decision making. For example, onephysician said,
We are basically telling patients that we take care of, “Wedon’t think your reason is good enough”.I struggled toexplain to students and residents how we make those deci-sions. Because it seems like it’s all based on our values andwhat we deem to be a worthy reason.
Although survey findings measured nationalprevalence of hospital abortion restrictions and crite-ria, qualitative interviews shed light on a range ofways that these abortion restrictions were understoodand operationalized by physicians.
Survey respondents were asked about whetherabortion policies at their institution were formallycodified in writing or unwritten. About a third (31%)of hospitals had written policies limiting abortion, andanother third (33%) had unwritten rules. Overall,restrictions on nonmedically indicated abortion weremore likely to be written (30%) than restrictions onmedically indicated ones (15%).
Unwritten rules were communicated verbally bycolleagues and could be opaque. One intervieweedescribed being told that nonmedically indicatedterminations were strictly forbidden by her institutionowing to a historical association with a Catholichospital and rumor of an abortion prohibition beingattached to the building bylaws (a national phenom-enon13). For years, she explained, the department fol-lowed this informal policy, until a new obstetrics andgynecology department chair, who was invested in“expanding our role in the community and havingan expanded capability to train residents,” questionedthe policy and thereafter began providing theseservices:
[The] new department chairman, who had a bit of a differentattitude and actually went to the greater hospital adminis-tration in his role as chair and said, you know, “What reallyis the institutional position on this?” And what he found outwas that the whole story, that there was some kind of bylawsagreement, you know, against doing elective termination ofpregnancy, was all a whole bunch of BS. It never existed inthe first place.
As with rules delineating permissible indicationsfor abortion, some respondents conveyed frustrationat the opacity that unwritten policies created. How-ever, others described how this lack of clarity gavethem flexibility, often in terms of gestational limits or
the nature of medical indication. For example,a respondent explained that she understood there tobe an exception to her abortion policy’s gestationallimit when the fetus could not survive.
Well the department has—I don’t know if it’s written or un-written—but an informal rule that.for lethal anomaliesbeyond 24 weeks I think there is some wiggle room in there;for nonlethal anomalies beyond that, there’s not.
Furthermore, interviewees explained that reluc-tance to formalize abortion policy in writing camefrom a desire to maintain this flexibility over practice,especially pertaining to cases at the locally acceptedmargins.
Nobody wants to talk about it, nobody wants to formalize it,you know, and nobody wants to kind of write any policies.It’s all sort of unspoken.the worry was that if you went tothe hospital and said we insist on a policy, that you’d geta policy that was very restrictive.
Thus, although survey data quantified prevalenceof formalization of policies in writing, qualitativeinterviews revealed that some physicians found lackof formalization to preserve their autonomy andability to provide abortion care for certain patientswith extenuating circumstances.
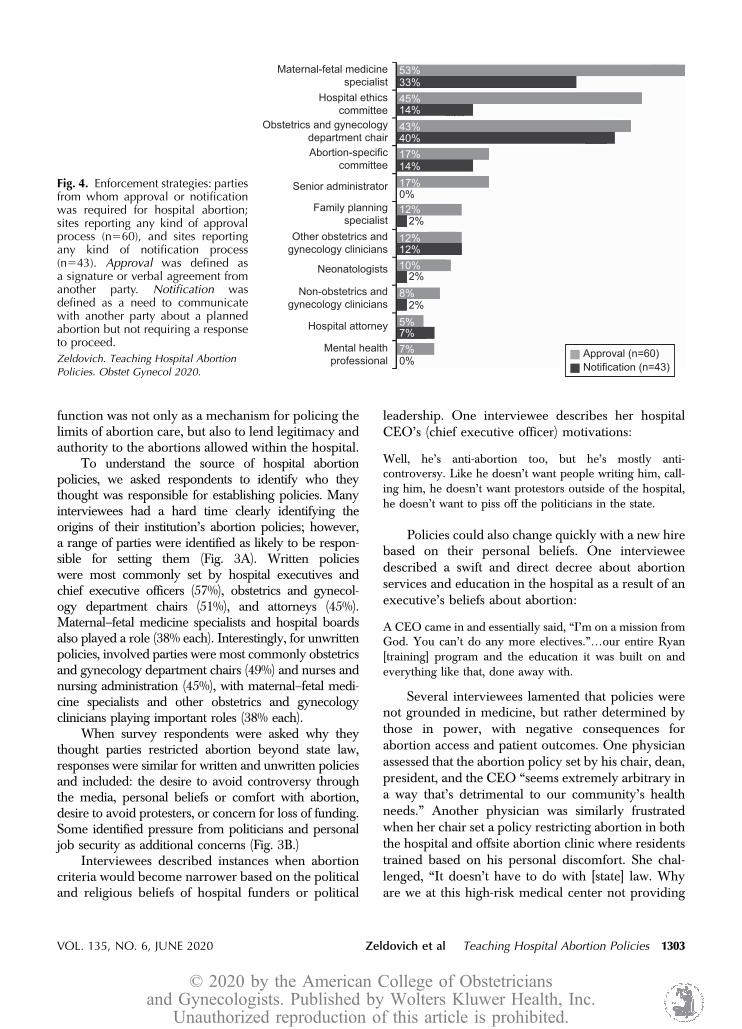
Just as institutional policies were variable, so wasthe enforcement of policies. Among hospitals withany type of abortion restriction, 57% required some-one’s approval to provide an abortion, and 34%required notifying someone, with others unclear onthe exact enforcement policy. The parties from whomactual approval was most commonly required werematernal–fetal medicine specialists (53%), hospitalethics committees (45%), and obstetrics and gynecol-ogy department chairs (43%) (Fig. 3). In contrast, forpolicies requiring notification, the parties most com-monly needing notification were obstetrics andgynecology department chairs (40%), maternal–fetalmedicine specialists (33%), and then hospital ethics(14%) or abortion-specific (14%) committees (Fig. 4).
In institutions where nonmedically indicatedterminations were allowed, interviewees soughtapproval for complex cases that were beyond thehospital’s gestational limit. On the other hand, formedically indicated procedures, physicians sometimesneeded to certify the medical necessity of the proce-dure using individual experts or a committee. Oneinterviewee described the complex process:
[I] can initiate it by going to the Chief of Service, [an] MFM[maternal–fetal medicine specialist], and what she will
© 2020 by the American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
VOL. 135, NO. 6, JUNE 2020 Zeldovich et al Teaching Hospital Abortion Policies 1301

normally do is get whoever else, like another MFM or if theperson has a cardiac problem, you know, a cardiologist ora cardio-thoracic surgeon to say that this is life-threatening.And then she will take that to the Chief of Staff for thehospital. And then if he has any questions, then we’ll con-vene the Ethics Committee to decide. But, if it’s straightfor-ward, he may just bypass everyone and say it can be done.
Although some interviewees felt that enforcementprocesses were convoluted or idiosyncratic, others feltapproval was helpful in legitimizing the procedure inthe eyes of others, and thus curbing opposition. They
described approval as somewhat of a formality used tosolidify support from hospital personnel and thecommunity at large:
Because of the potential for people catching wind of it andnot understanding.the direction was given to involve theEthics Committee. ’Cause then you’ve just, you know, dot-ted all the i’s and crossed the t’s.
In sum, survey findings showed approval pro-cesses were prevalent and commonly fell to leadershipand specialists. Interviews elucidated that their
Fig. 3. A. Etiology of hospital abor-tion policy: parties identified by sur-vey respondents to have had a rolein defining abortion policies at theirinstitutions, by policy type (writ-ten: n553 and unwritten: n555).B. Motivating factors for hospitalabortion policies: concepts per-ceived by survey respondents tomotivate abortion policies at theirinstitutions, by policy type (written:n553 and unwritten: n555). CEO,chief executive officer.
Zeldovich. Teaching Hospital AbortionPolicies. Obstet Gynecol 2020.
© 2020 by the American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
1302 Zeldovich et al Teaching Hospital Abortion Policies OBSTETRICS & GYNECOLOGY
function was not only as a mechanism for policing thelimits of abortion care, but also to lend legitimacy andauthority to the abortions allowed within the hospital.
To understand the source of hospital abortionpolicies, we asked respondents to identify who theythought was responsible for establishing policies. Manyinterviewees had a hard time clearly identifying theorigins of their institution’s abortion policies; however,a range of parties were identified as likely to be respon-sible for setting them (Fig. 3A). Written policieswere most commonly set by hospital executives andchief executive officers (57%), obstetrics and gynecol-ogy department chairs (51%), and attorneys (45%).Maternal–fetal medicine specialists and hospital boardsalso played a role (38% each). Interestingly, for unwrittenpolicies, involved parties were most commonly obstetricsand gynecology department chairs (49%) and nurses andnursing administration (45%), with maternal–fetal medi-cine specialists and other obstetrics and gynecologyclinicians playing important roles (38% each).
When survey respondents were asked why theythought parties restricted abortion beyond state law,responses were similar for written and unwritten policiesand included: the desire to avoid controversy throughthe media, personal beliefs or comfort with abortion,desire to avoid protesters, or concern for loss of funding.Some identified pressure from politicians and personaljob security as additional concerns (Fig. 3B.)
Interviewees described instances when abortioncriteria would become narrower based on the politicaland religious beliefs of hospital funders or political
leadership. One interviewee describes her hospitalCEO’s (chief executive officer) motivations:
Well, he’s anti-abortion too, but he’s mostly anti-controversy. Like he doesn’t want people writing him, call-ing him, he doesn’t want protestors outside of the hospital,he doesn’t want to piss off the politicians in the state.
Policies could also change quickly with a new hirebased on their personal beliefs. One intervieweedescribed a swift and direct decree about abortionservices and education in the hospital as a result of anexecutive’s beliefs about abortion:
A CEO came in and essentially said, “I’m on a mission fromGod. You can’t do any more electives.”.our entire Ryan[training] program and the education it was built on andeverything like that, done away with.
Several interviewees lamented that policies werenot grounded in medicine, but rather determined bythose in power, with negative consequences forabortion access and patient outcomes. One physicianassessed that the abortion policy set by his chair, dean,president, and the CEO “seems extremely arbitrary ina way that’s detrimental to our community’s healthneeds.” Another physician was similarly frustratedwhen her chair set a policy restricting abortion in boththe hospital and offsite abortion clinic where residentstrained based on his personal discomfort. She chal-lenged, “It doesn’t have to do with [state] law. Whyare we at this high-risk medical center not providing
Fig. 4. Enforcement strategies: partiesfrom whom approval or notificationwas required for hospital abortion;sites reporting any kind of approvalprocess (n560), and sites reportingany kind of notification process(n543). Approval was defined asa signature or verbal agreement fromanother party. Notification wasdefined as a need to communicatewith another party about a plannedabortion but not requiring a responseto proceed.
Zeldovich. Teaching Hospital AbortionPolicies. Obstet Gynecol 2020.
© 2020 by the American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
VOL. 135, NO. 6, JUNE 2020 Zeldovich et al Teaching Hospital Abortion Policies 1303

this service to women in need, you know? And inparticular, how is he able to dictate practice [whereresidents train offsite] where he doesn’t have any realauthority?”
Thus, survey findings quantified the perceivedorigins of abortion policies, and interviews fleshed outhow, in some specific instances, beliefs of particulardepartment or hospital leadership served to narrow orforeclose training and provision.
DISCUSSION
This mixed-methods study examined U.S. teachinghospitals’ policies for abortion practice. We found thatabortion policies existed in 57% of teaching hospitals,most prominently in the South and Midwest, andapproximately one-third were codified in writing. Poli-cies restricted nonmedically indicated abortions by ges-tational age and medically indicated procedures by theindividual indication. Qualitative data highlighted thenuances of policies, which were sometimes complex orconfusing. Rules were enforced primarily by maternal–fetal medicine specialists, obstetrics and gynecologydepartment chairs, and hospital ethics committees, es-tablished by individuals with institutional power, andperceived to be motivated by personal beliefs anda desire to avoid controversy. Interview respondentsreported that hospital leaders prioritized broad financialand political considerations when creating abortionpolicies which, in some cases, put physicians at oddswith their mission to train future health care providersaccording to ACGME standards for abortion.
Both survey respondents and interviewees re-ported that, in all their forms, hospital abortionpolicies perpetuated a system of value judgments onpatients’ reasons for seeking abortion. Intervieweesused the categories “medically indicated” and “non-medically indicated” or “elective” abortion to explaindifferential allowances, a dichotomy that masks thecomplex social and medical situations pregnant indi-viduals face, and perpetuates abortion stigma.12 Sur-vey respondents corroborated that even withinmedical indications, abortions for some indicationswere more heavily scrutinized than others. This strat-ification of legitimacy within teaching hospital abor-tion policies serves to reinforce abortion stigma forboth patients and medical trainees.14
One of the most notable themes in the data wasthe prominence and manifold effects of unclearabortion policies. Vague or unwritten policies,although difficult to navigate, gave health care pro-viders more agency and flexibility, especially incomplicated cases where patients did not fit theunderstood criteria for abortion in their hospitals.
On the other hand, formalized rules were perceived tolend protection to clinicians and the hospital fromopposing coworkers or community members whomay question the legitimacy of particular abortionprocedures.
Opaque policies were sometimes perpetuated bythe lore of an institution but could also be influencedby those responsible for their enforcement. Althoughthe theoretical goal of approval and enforcementmechanisms was to lend objectivity and support fora difficult clinical decision, interviewees perceivedthese strategies as protecting the hospital from polit-ical and financial—rather than medical, legal, or ethical—risk. In this way, hospital-level enforcement mecha-nisms resembled pre-Roe abortion committees.15
Many interviewees expressed discomfort with institu-tionally defined processes that adjudicated a legallyprivate medical decision. Overall, in hospitals withrestrictive abortion policies, power rested more subtlyin the flexibility of vague policies and the sway ofleaders tasked with enforcing them.
One limitation of the survey was the challenge ofcapturing the complexity of site-specific policies ina closed-ended format. We believe the qualitative dataserved as a counterbalance to that limitation, givinga sense of the nuance of policies. The survey responserate (73%) was good. Still, with greater representationof larger sites and those in the West and underrepre-sentation of Midwestern and religious institutions, ourfigures likely underestimated abortion restrictions.Finally, our findings may not be generalizable tononteaching U.S. hospitals. We suspect, based onqualitative work, that the average nonacademic U.S.hospital has more unyielding fiscal responsibilitiesand political motivations, and no ACGME mandateto have abortion services as part of training, likelyresulting in more abortion restrictions.16 The primarylimitation of the qualitative data was in its over-representation of sites with Ryan training programs(14/18), which explicitly train residents in abortion.Nevertheless, the four interviews with non-Ryan di-rectors yielded similar themes as those with Ryandirectors.
Patients presenting to hospitals for medical serv-ices reasonably expect to get legally protected care. Inreligiously affiliated hospitals, patients are oftenunaware how institutional policies curb their legalrights to abortion.17 It is likely that patients presentingto U.S. teaching hospitals with policies that restrictabortion access beyond state law are similarlyunaware of restrictions. Decreasing access to abortionhas been shown to create delays in care and poorpatient outcomes.1 Additionally, teaching hospital
© 2020 by the American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
1304 Zeldovich et al Teaching Hospital Abortion Policies OBSTETRICS & GYNECOLOGY

abortion policies present barriers to clinical trainingfor obstetrics and gynecology residents.9 Understand-ing the nature, etiology and arbiters of these policies isthe first step toward preserving hospital abortion asa vital resource for patients at the medical marginsand for the education of the next generation ofphysicians.18
REFERENCES1. Jones RK, Jerman J. Abortion incidence and service availability
in the United States, 2014. Perspect Sex Reprod Health 2017;49:17–27.
2. Raymond EG, Grossman D, Weaver MA, Toti S, Winikoff B.Mortality of induced abortion, other outpatient surgical proce-dures and common activities in the United States. Contracep-tion 2014;90:476–9.
3. O’Connell K, Jones HE, Lichtenberg ES, Paul M. Second-tri-mester surgical abortion practices: a survey of National Abor-tion Federation members. Contraception 2008;78:492–9.
4. Freedman L, Landy U, Darney P, Steinauer J. Obstacles to theintegration of abortion into obstetrics and gynecology practice.Perspect Sex Reprod Health 2010;42:146–51.
5. Jerman J, Frohwirth L, Kavanaugh ML, Blades N. Barriers toabortion care and their consequences for patients traveling forservices: qualitative findings from two states. Perspect Sex Re-prod Health 2017;49:95–102.
6. Review Committee for Obstetrics and Gynecology. Clarifica-tion of program requirement IV.A.6.d. Chicago, IL: Accredita-tion Council for Graduate Medical Education; 2012.
7. Steinauer JE, Turk JK, Pomerantz T, Simonson K, LearmanLA, Landy U. Abortion training in US obstetrics and gynecol-ogy residency programs. Am J Obstet Gynecol 2018;219:86.e1–6.
8. Guiahi M, Westhoff CL, Summers S, Kenton K. Training ata faith-based institution matters for obstetrics and gynecology
residents: results from a regional survey. J Grad Med Educ2013;5:244–51.
9. Turk JK, Landy U, Chien J, Steinauer JE. Sources of support forand resistance to abortion training in obstetrics and gynecologyresidency programs. Am J Obstet Gynecol 2019;221:156.e1–6.
10. Guiahi M, Hoover J, Swartz M, Teal S. Impact of Catholichospital affiliation during obstetrics and gynecology residencyon the provision of family planning. J Grad Med Educ 2017;9:440–6.
11. Uttley L KC, Hasbrouck P. Growth of Catholic hospitals andhealth systems: 2016 update of the Miscarriage of MedicineReport. New York, NY: MergerWatch; 2016.
12. Janiak E, Goldberg AB. Eliminating the phrase “elective abor-tion”: why language matters. Contraception 2016;93:89–92.
13. Sepper E. Zombie religious institutions. Northwestern Univer-sity Law Rev 2018;112:929–87.
14. Kimport K, Weitz TA, Freedman L. The stratified legitimacy ofabortions. J Health Soc Behav 2016;57:503–16.
15. Solinger R. “A complete disaster”: abortion and the politics ofhospital abortion committees, 1950–1970. Feminist Stud 1993;19:240–68.
16. Freedman L. Willing and unable: doctors’ constraints in abor-tion care. Nashville: Vanderbilt University Press; 2010;xi:186.
17. Guiahi M, Sheeder J, Teal S. Are women aware of religiousrestrictions on reproductive health at Catholic hospitals? A sur-vey of women’s expectations and preferences for family plan-ning care. Contraception 2014;90:429–34.
18. One Hundred Professors of Obstetrics and Gynecology. Astatement on abortion by 100 professors of obstetrics: 40 yearslater. Am J Obstet Gynecol 2013;209:193–9.
PEER REVIEW HISTORYReceived December 13, 2019. Received in revised form December14, 2020. Accepted January 23, 2020. Peer reviews are available athttp://links.lww.com/AOG/B851.
© 2020 by the American College of Obstetriciansand Gynecologists. Published by Wolters Kluwer Health, Inc.
Unauthorized reproduction of this article is prohibited.
VOL. 135, NO. 6, JUNE 2020 Zeldovich et al Teaching Hospital Abortion Policies 1305