aats skills course may 4, 2013webcast.aats.org/2013/files/saturday/20130504_101e_1330_14.00... ·...
TRANSCRIPT

AATS Skills Course
May 4, 2013
Thomas A. D’Amico MD
Professor and Vice Chair of Surgery
Chief Thoracic Surgery
Chief Medical Officer, Duke Cancer Institute

Thomas A. D’Amico MD Professor and Vice Chair of Surgery
Chief Thoracic Surgery Chief Medical Officer, Duke Cancer Institute
Thoracoscopic Lobectomy:
Mediastinal Lymph Node Dissection
AATS Skills Course
May 4, 2013

MLND: Thoracoscopic vs Open
Disclosure
• No conflicts related to this presentation

MLND: Thoracoscopic vs Open
Oncologic Outcomes
• Ability to achieve complete resection
• Survival and other oncologic surgical outcomes
• Immunologic competence
• Compliance with adjuvant therapy
• Mediastinal lymph node dissection

MLND: Thoracoscopic vs Open
Mediastinal Lymph Node Staging
• Important component of the assessment and
management of patients with NSCLC
• Although rigid standards regarding the conduct
and extensiveness of MLN staging do not exist,
current guidelines suggest that the assessment of a
minimum of three N2 nodes should be included,
in addition to the removal of regional N1 nodes

MLND: Thoracoscopic vs Open

MLND: Thoracoscopic vs Open

MLND: Thoracoscopic vs Open
Adoption of Thoracoscopic Lobectomy
• Several factors may explain the lack of complete
adoption
• Inadequate experience during training
• Concerns regarding oncologic effectiveness
• One specific concern relates to the ability of
thoracoscopic surgery to achieve adequate staging
of the mediastinum

MLND: Thoracoscopic vs Open
Mediastinal Lymph Node Dissection
• Several studies confirm equivalent lymph node
dissections
MLND: Thoracoscopic vs Open
Is complete systematic nodal dissection by
thoracoscopic surgery possible? Kondo et al JTCVS 1998; 116: 651-2
• 6 patients underwent VATS lobectomy with
MLND followed by thoracotomy
• # LN by VATS lobectomy was 27-48
• Remaining LN found in 2 patients at thoracotomy
• Weight of LN tissue resected by VATS was 5.0-
16.1 g
MLND: Thoracoscopic vs Open
Is complete systematic nodal dissection by
thoracoscopic surgery possible? Kondo et al JTCVS 1998; 116: 651-2
• In the 2 patients in whom remaining LN were
found at thoracotomy, the weight of the
additionally dissected tissue was 0.6 and 0.2 g
• The percentage of lymph nodes remaining was
3.5% and 2%, respectively
• Overall percentage of LN remaining after
systematic nodal dissection by VATS lobectomy
was 3.4% by #, and 1.5% by weight

MLND: Thoracoscopic vs Open
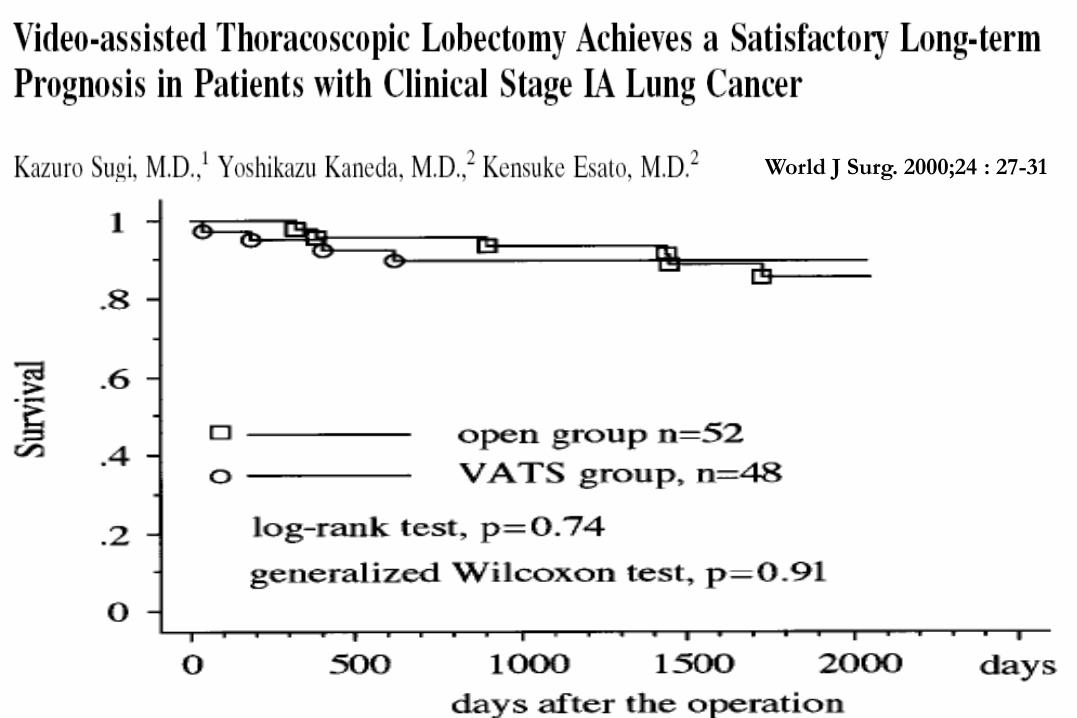
Sugi et al
• Randomized trial, with 100 consecutive patients
with clinical stage IA NSCLC
• Endpoints: nodal dissection and survival
World J Surg. 2000;24 : 27-31
MLND: Thoracoscopic vs Open Duke Thoracic
Oncology
Program
Sugi World J Surg. 2000;24 : 27-31

MLND: Thoracoscopic vs Open
Compared LN harvest in 350 patients with c-Stage I
NSCLC
• 191 thoracoscopic lobectomies and 159 open
lobectomies
Surgery. 2005;138:510-517.

MLND: Thoracoscopic vs Open
Watanabe et al Surgery. 2005;138:510-51

MLND: Thoracoscopic vs Open
Watanabe et al Surgery. 2005;138:510-517
Surgery. 2005;138:510-517.

MLND: Thoracoscopic vs Open
Is VATS a feasible approach for c-N0/p-N2
NSCLC? Watanabe A et al. Eur J Cardiothorac Surg 2008;33:812-818
• 770 patients who underwent lobectomy and
MLND by VATS or thoracotomy
• 69 patients were upstaged from cN0 to pN2
NSCLC
• The rate of LN upstaging was similar between the
two groups
• The 3-year and 5-year recurrence-free survivals
were similar

MLND: Thoracoscopic vs Open
Lymph Node Evaluation in VATS Lobectomy
Versus Lobectomy by Thoracotomy Denlinger C et al Ann Thorac Surg 2010;89:1730-1736
• Barnes Hospital, St. Louis: 79 VATS and 464 open lobectomy or segmentectomy
• No differences in N1 node sampling
• Fewer N2 nodes sampled with VATS vs thoracotomy (2.5 vs 3.3; p=0.004)
• Fewer station 7 lymph nodes with VATS vs thoracotomy (0.6 vs 1.2; p=0.002)
• Fewer total # nodes sampled with VATS vs thoracotomy (7.4 vs 8.9 p=0.029)
• No difference in 2-year survival: (81% vs 83%, p=0.4)

MLND: Thoracoscopic vs Open
Lymph Node Evaluation by Open or VATS Approaches in
11,500 Anatomic Lung Cancer Resections Boffa DJ, et al Ann Thorac Surg 2012;94:347-353
• STS database: lobe/segment resection 2001-11
• 11,531 (7,137 open, 4,394 VATS) c-stage I
• Upstaging: Open 14%, VATS 12% (p < 0.001)
• N0 to N1 higher in open (9% vs 7%; p < 0.001)
• N0 to N2 similar (5% open, 5% VATS; p = 0.52)
• 2,745 propensity-matched pairs, N0 to N1 lower
with VATS (7% vs 9%; p = 0.002)

MLND: Thoracoscopic vs Open
Prevalence of nodal upstaging (cN0 to pN1) by
participant use of VATS

MLND: Thoracoscopic vs Open
Nodal Upstaging is Lower after Thoracoscopic
Lobectomy Compared with Thoracotomy for
Clinical Stage-1 Lung Cancer: A Nationwide Study Licht P et al STS January 28, 2013
• Danish Lung Cancer Registry was 2007-11
• 1675 patients: lobectomy for clinical stage-1
• VATS: 751 patients (45%)
• # of LN stations not significantly different
• Nodal upstaging: 319 (19%) significantly more
frequent after thoracotomy in both N0 to N1
upstaging (14.0%vs. 8.3%, p<0.001) and in N0 to
N2 upstaging (10.9% vs. 3.6%, p<0.001)
MLND: Thoracoscopic vs Open
Open Lobectomy for Early Stage Lung Carcinoma
Achieves a Superior Lymph Node Dissection
Compared to Thoracoscopic Lobectomy Merritt RE et al STS January 28, 2013
• 130 pts lobectomy c-stage I-II NSCLC-54% open
• Mean # LN in open group was significantly
higher (15.4 vs. 9.8, p=0.002)
• Upstaging: Open 28.5% vs VATS 10% [p=0.02]
• Kaplan-Meier 3-year survival was similar
between the groups
MLND: Thoracoscopic vs Open
Hypothesis
There is no difference in the efficacy of
mediastinal lymph node assessment whether
lobectomy is performed with a Thoracoscopic
approach or with an Open approach
MLND: Thoracoscopic vs Open
Patients and Methods
• NCCN NSCLC Database: Web-based database
of patients who received primary treatment for
NSCLC since 2007 at 8 of the 21 NCCN
institutions
• Efficacy of MLN assessment analyzed in patients
who underwent lobectomy: VATS vs Open
Ann Thorac Surg 2011;92:226-232

MLND: Thoracoscopic vs Open
Patients and Methods
The # and location of all N1 and N2 lymph node
stations resected was analyzed by approach
1. The # of N2 LN stations resected
2. The % of patients with >3 MLN stations resected
3. The total # of lymph nodes (N1+N2)
4. The degree of upstaging and downstaging

MLND: Thoracoscopic vs Open
Results
• 2007 -2010: 4215 patients with NSCLC
• 851 pts underwent lobectomy for c-Stage I-III
• 388 evaluable pts underwent lobectomy:
199 Thoracoscopic and 189 Open
• There was no difference in age, sex, co-
morbidities, performance status, or histology

MLND: Thoracoscopic vs Open
# N2 Lymph Nodes: Open Vs VATS
Median Mean
Open 3 2.9
VATS 3 3.2 p=0.12
# of LN Stations
# o
f P
atie
nts

MLND: Thoracoscopic vs Open
At Least 3 N2 Lymph Node Stations
# N2
Stations
Open Thoracoscopic P value
N % N %
<3 77 42% 67 34% 0.12
>3 107 58% 130 66%

MLND: Thoracoscopic vs Open
Total Lymph Nodes (N1+N2): Open vs VATS
Median Mean
Open 4 4.4
VATS 4 4.8 p=0.06
# of LN Stations
# o
f P
atie
nts

MLND: Thoracoscopic vs Open
Upstaging Thoracoscopic Pathologic N: Up-Staging
Clinical N N0 N1 N2 Total
N0 152 11 4 171
N1 4 3 1 8
N2 4 0 10 14
Open Pathologic N: Up-Staging
Clinical N N0 N1 N2 Total
N0 122 10 11 145
N1 3 11 2 17
N2 4 2 17 23
9%
14%; P=.15

MLND: Thoracoscopic vs Open
Downstaging Thoracoscopic Pathologic N: Down-Staging
Clinical N N0 N1 N2 Total
N0 152 11 4 171
N1 4 3 1 8
N2 4 0 10 14
Open Pathologic N: Down-Staging
Clinical N N0 N1 N2 Total
N0 122 10 11 145
N1 3 11 2 17
N2 4 2 17 23
29%
26%; P=1.0

MLND: Thoracoscopic vs Open
Summary
• The majority of patients who underwent
lobectomy by either a Thoracoscopic or Open
approach had at least 3 MLN stations assessed
• There was no difference in
1. # of N2 LN stations resected
2. % of patients with >|3 MLN stations assessed
3. Total # of LN stations (N1 + N2) by approach
4. Degree of upstaging or downstaging

MLND: Thoracoscopic vs Open
• 21 comparative studies: 2 randomized
• Morbidity, mortality, recurrence, 5-year mortality
http://jco.ascopubs.org/cgi/doi/10.1200/JCO.2008.18.2733

MLND: Thoracoscopic vs Open
Systematic Review and Meta-Analysis of
Randomized and Nonrandomized Trials on Safety
and Efficacy of VATS Lobectomy
• VATS did not demonstrate any significant
difference in locoregional recurrence (P= 0.24)
• VATS associated with reduced systemic
recurrence rate (P=0.03) and an improved 5-year
mortality rate of VATS (P =0.04)

MLND: Thoracoscopic vs Open
All-Cause Mortality

MLND: Thoracoscopic vs Open
• Meta-analysis of 3 studies with propensity
matching
• Villamizar N, et al. J Thorac Cardiovasc Surg
2009; 138: 419
• Paul S, et al et al. J Thorac Cardiovasc Surg:
2010; 139: 366
• Ilonen IK et al. Acta Oncologic 2011; 50: 1126
Ann Cardiothorac Surg 2012: 1: 16-23

MLND: Thoracoscopic vs Open
Relative Risk of All Cause Mortality Un-matched
Matched

MLND: Thoracoscopic vs Open
Randomized Trial of MLNS vs MLND During
Pulmonary Resection for N0-1 NSCLC: Results of
the ACOSOG Z0030 trial Darling GE, et al. J Thorac Cardiovasc Surg. 2011;141:662-670
• 1,111 patients randomized intraoperatively after
MLNS performed (555 MLNS, 556 MLND)
• In the MLND group, only 20 patients (3.8%) were
found to have occult N2 disease
MLNS MLND P value
Deaths 214 (42.9%) 217 (41.3%) NS
Median Survival 8.1 years 8.5 years p=0.531
Time to recurrence 5.7 years 6.1 years p=0.655
MLND: Thoracoscopic vs Open
In Order To Avoid Complete MLND
1. T<3cm
2. Appropriate preoperative mediastinal lymph
node assess including EBUS or mediastinoscopy
3. Complete hilar dissection
4. Frozen section negative on all 10, 11, and N2
lymph nodes

MLND: Thoracoscopic vs Open
Summary
• There is no difference in the efficacy of MLN
assessment whether lobectomy is performed by
thoracoscopy or thoracotomy
• Concerns about the efficacy of MLN resection
should not limit the adoption of thoracoscopic
lobectomy
MLND: Thoracoscopic vs Open
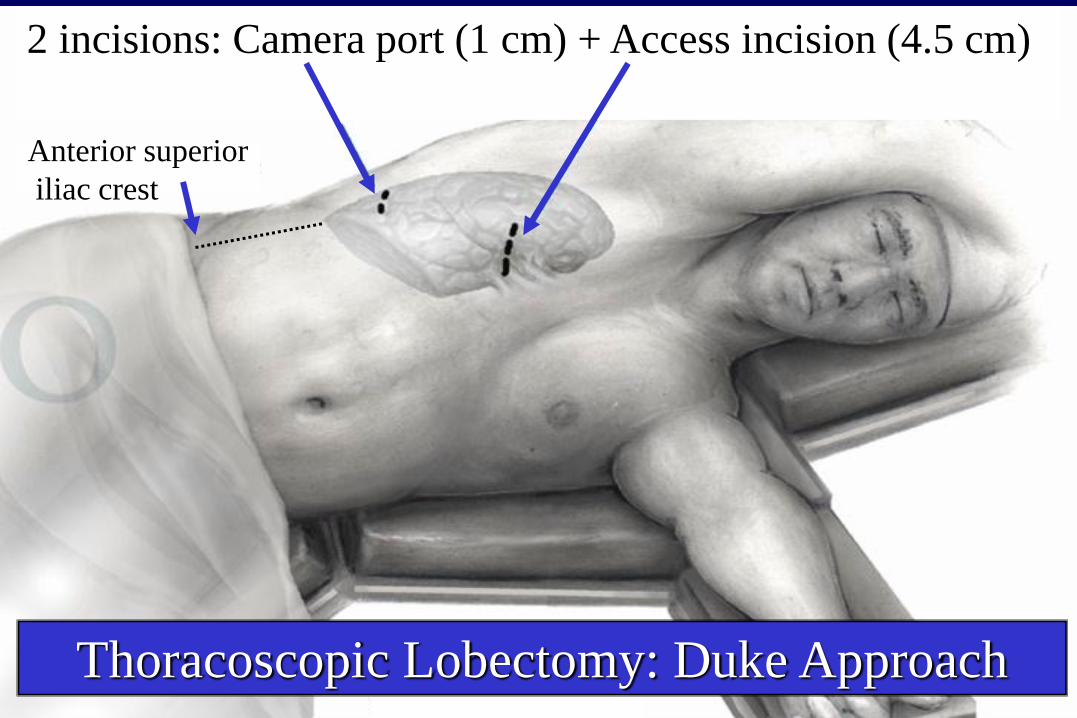
Duke Approach Anterior superior
iliac crest
Thoracoscopic Lobectomy: Duke Approach
2 incisions: Camera port (1 cm) + Access incision (4.5 cm)

MLND: Thoracoscopic vs Open
Duke Approach
Thoracoscopic Lobectomy: Duke Approach
2 incisions: Camera port (1 cm) + Access incision (4.5 cm)
Anterior superior
iliac crest

MLND: Thoracoscopic vs Open
Duke Approach
Thoracoscopic Lobectomy: Duke Approach
2 incisions: Camera port (1 cm) + Access incision (4.5 cm)
Anterior superior
iliac crest

MLND: Thoracoscopic vs Open
MLND: Thoracoscopic vs Open