a treatment planning study comparing volumetric arc...
TRANSCRIPT

Radiotherapy and Oncology 89 (2008) 180–191www.thegreenjournal.com
Cervix cancer radiotherapy
A treatment planning study comparing volumetric arcmodulation with RapidArc and fixed field IMRT for
cervix uteri radiotherapy
Luca Cozzia,b,*, Ketayun Ardeshir Dinshawc, Shyam Kishore Shrivastavac,Umesh Mahantshettyc, Reena Engineerc, Deepak Dattatray Deshpandec, S.V. Jamemac,
Eugenio Vanettia, Alessandro Clivioa, Giorgia Nicolinia, Antonella Fogliataa
aOncology Institute of Southern Switzerland, Medical Physics Unit, Bellinzona, Switzerland, bUniversity of Lausanne, Faculty ofMedicine, Lausanne, Switzerland, cDepartment of Radiation Oncology & Medical Physics, Tata Memorial Hospital, Mumbai, India
Abstract
Purpose: A treatment planning study was performed to evaluate the performance of the novel volumetric modulatedsingle arc radiotherapy on cervix uteri cancer patients. Conventional fixed field IMRT was used as benchmark.Methods and materials: CT datasets of eight patients were included in the study. Plans were optimised with the aim to
assess organs at risk and healthy tissue sparing while enforcing highly conformal target coverage. Planning objectives forPTV were: maximum significant dose lower than 52.5 Gy and minimum significant dose higher than 47.5 Gy. For organs atrisk, the median and maximum doses were constrained to be lower than 30 (rectum), 35 (bladder) and 25 Gy (smallbowel) and 47.5 Gy; additional objectives were set on various volume thresholds. Plans were evaluated on parametersderived from dose volume histograms and on NTCP estimates. Peripheral doses at 5, 10 and 15 cm from the PTV surfacewere recorded to assess the low-level dose bath. The MU and delivery time were scored to measure expected treatmentefficiency.Results: Both RapidArc and IMRT resulted in equivalent target coverage but RapidArc had an improved homogeneity
(D5%–D95% = 3.5 ± 0.6 Gy for RapidArc and 4.3 ± 0.8 Gy for IMRT) and conformity index (CI90% = 1.30 ± 0.06 for RapidArcand 1.41 ± 0.15 for IMRT). On rectum the mean dose was reduced by about 6 Gy (10 Gy for the rectum fraction notincluded in the PTV). Similar trends were observed for the various dose levels with reductions ranging from �3 to14.4 Gy. For the bladder, RapidArc allowed a reduction of mean dose ranging from �4 to 6 Gy and a reduction from �3 to9 Gy w.r.t. IMRT. Similar trends but with smaller absolute differences were observed for the small bowel and left andright femur. NTCP calculations on bladder and rectum confirmed the DVH data with a potential relative reduction rangingfrom 30 to 70% from IMRT to RapidArc. The healthy tissue was significantly less irradiated in the medium to high doseregions (from 20 to 30 Gy) and the integral dose reduction with RapidArc was about 12% compared to IMRT. Concerningperipheral dose, the relative difference between IMRT and RapidArc was of 9 ± 2%, 43 ± 11% and 36 ± 5% at 5, 10 and15 cm from the PTV surface, respectively. The MU/Gy from RapidArc was 245 ± 17 corresponding to an expected averagebeam on time of 73 ± 10 s per fractions of 2 Gy. IMRT plans presented higher values with an average of MU/Gy = 479 ± 63.Conclusion: RapidArc was investigated for cervix uteri cancer showing significant improvements in organs at risk and
healthy tissue sparing with uncompromised target coverage leading to better conformal avoidance of treatments w.r.t.conventional IMRT. This, in combination with the confirmed short delivery time, can lead to clinically significantadvances in the management of this highly aggressive cancer type. Clinical protocols are now advised to evaluateprospectively the potential benefit observed at the planning level.
�c 2008 Elsevier Ireland Ltd. All rights reserved. Radiotherapy and Oncology 89 (2008) 180–191.
Keywords: RapidArc; IMRT; Cervix uteri radiation therapy
Radiotherapy in most gynaecological malignancies is ofprimary interest and it is a standard component of definitiveand postoperative management of cervical and endometrialcancer [11,18,19,24]. In addition to the treatment of the
0167-8140/$ - see front matter �c 2008 Elsevier Ireland Ltd. All rights re
primary site, radiotherapy is often performed including pel-vic lymph nodes at various levels depending on stage. As aresult, gastrointestinal and genitourinary tracts are oftenhighly involved and could lead to acute and late toxicities
served. doi:10.1016/j.radonc.2008.06.013

L. Cozzi et al. / Radiotherapy and Oncology 89 (2008) 180–191 181
[11,33]. The challenge is therefore the usage of advancedtreatment techniques to enhance the degree of conformalavoidance of conventional conformal approaches.
Initial experience in the application of intensity modu-lated radiation therapy (IMRT) showed that for bowel, rec-tum and bladder, significant reduction of involvement athigh doses is achievable [2,12,13,17,20,27,30,34,41]. Georget al. [17] showed that the volume of organs at risk (OAR)irradiated at doses between 40 and 50 Gy (with a prescrip-tion of 50.4 Gy) was reduced by factors between 2 and 6with IMRT compared to conventional therapy. Portelanceet al. [30] investigating IMRT at planning level showed sim-ilar results reducing the volume of OARs irradiated at highdose levels by 3–10 times. Mundt et al. [27] and Roeskeet al. [34] investigated the benefit of IMRT and, with over40 patients treated with IMRT, no grade 3 toxicity was ob-served together with a decrease (more than 40%) in grade2 acute gastrointestinal toxicity.
Given these premises, a randomised phase II trial com-paring IMRT with conventional radiotherapy was activatedat Tata Memorial Hospital (TMH) in Mumbai for patients af-fected by stage IIB cervix carcinoma. The Cervix carcinomais the most common malignancy in Indian women and it isalso the leading cause of cancer mortality in India. Nearly85% of the patients present with advanced stage (FIGO II/III). The survival rates consolidated over decades in this geo-graphical area achieved a plateau of 30–55% at 5 years.Gastrointestinal and genitourinary toxicity is a concern.Grade III radiation cystitis and proctitis are in the range of3–15% with radiation alone and, in combination with che-motherapy toxicity is expected to increase (up to 35% gradeIII and grade IV) [18,24].
The aim of the present study was to investigate the po-tential clinical role of a novel treatment technique, Rapid-Arc (Varian Medical Systems, Palo Alto, CA), which isbased on volumetric intensity modulated single arc delivery.The intent is to offer improved conformal avoidance to thiscategory of patients.
RapidArc falls into the more general category of intensitymodulation therapy with arcs, or IMAT [6,10,14,25]. Amongthe pioneers, Yu’s group, starting the late 1990s clarifiedthe benefit of using multiple, coplanar or non coplanar mod-ulated arcs for most complex cases [39,40]. The Ghent groupapplied IMAT techniques with multiple non-coplanar beamsto pelvic treatments (rectum and whole abdominal-pelvicindications) [13,14], proving that IMAT offered equivalentor superior target coverage and highly improved sparing ofOARs compared to conventional conformal treatments.
RapidArc is a planning and delivery technique based on aninvestigation from K. Otto [28] and it aims to achieve sev-eral objectives at once: (i) improve OARs and healthy tissuesparing compared to other IMRT solutions; (ii) maintain orimprove the same degree of target coverage; (iii) reducesignificantly the treatment time (beam on time) perfraction.
The third objective has several corollaries. Faster treat-ments could have a clinical impact on single patients interms of comfort on couch, immobility and minimisationof internal organ’s displacement (e.g. bladder or rectumfilling changes over time). This could increase the dailytreatment quality and allows also more time for imaging
procedures within standard time slots. In addition, fastertreatments have an impact on the system throughput allow-ing the possibility to treat more patients per day, and toeventually reduce waiting list for selected groups ofpatients.
Materials and methodsPatient selection and planning objectives
CT data for a cohort of eight patients from the TMH cen-tre were selected for this comparative analysis. All patientswere affected by carcinoma of the cervix uteri to be treatedwith curative intent. For all patients, plans were designedon CT scans acquired with 5 mm slice thickness extendingthe scan from T11 to include the proximal third of the fe-mur’s diaphysis. The OAR considered were: rectum, blad-der, femoral heads and the small bowel. For rectum andbladder, two sets of OARs were defined being the entire or-gan or the fraction of organ not included in the PTV. Thehealthy tissue was defined as the patient’s volume coveredby the CT scan minus the PTV. PTV was defined adding 7–10 mm margins to CTV that included the cervix, uterus, par-ametrial tissues and the pelvic nodes including pre-sacral(no para-aortic nodes were included in this study). ThePTV mean volume was 1115 ± 136 cm3.
As for the TMH protocol and in other studies [38], doseprescription to the pelvis was set as 50 Gy in 2 Gy per frac-tions and plans were all normalised to the mean dose to thePTV to avoid any bias or rescaling effect in the comparison.The radiation treatment schedule included also a boost of21 Gy to be delivered in three weekly fractions with highdose rate brachytherapy (HDR). This was not included inthe study since it is not correlated to the evaluation ofthe differences between IMRT and RapidArc for the electivevolume irradiation.
Various planning objectives were imposed according tothe TMH protocol. For PTV plans aimed to achieve minimumdose >47.5 Gy and maximum dose <52.5 Gy (95–105% of theprescription). For rectum the maximum dose limit was47.5 Gy in combination with two complementary con-straints: D35% < 40 Gy and D50% < 30 Gy (Dx% is dose receivedby x% of the volume). Similarly for the bladder maximumdose was set to 47.5 Gy in combination with D40% < 40 Gyand D50% < 35 Gy. For the region containing the small bowel,maximum dose was limited to 47.5 Gy while complementaryconstraints were specified as D30% < 30 Gy and D50% < 25 Gy.
In all cases, planning objectives were transferred intonumerical dose–volume constraints used in the optimisa-tion phase and tailored to the specific patients characteris-tics. Priorities were adjusted during optimisation to achievethe best results for each patient.
Planning techniquesTwo isocentric techniques were compared in this study,
all designed on the Varian Eclipse treatment planning sys-tem (TPS) with 6 MV photon beams from a Varian Clinacequipped with a Millennium Multileaf Collimator (MLC) with120 leaves (this is characterised by a spatial resolution of5 mm at isocentre for the central 20 cm and of 10 mm in

182 Volumetric arc modulation for cervix uteri radiation therapy
the outer 2 · 10 cm, a maximum leaf speed of 2.5 cm/s anda leaf transmission of �1.8%). Plans for RapidArc were opti-mised selecting a maximum DR of 600 MU/min and a fixedDR of 300 MU/min was selected for IMRT.
The Anisotropic Analytical Algorithm (AAA) photon dosecalculation algorithm was used for all cases [5,15,23,33,37]. The dose calculation grid was set to 2.5 mm. All theplanning tools used for the present study were based onpre-clinical engineering versions available only for researchpurposes, version 8.2.16 in the Eclipse 8.2 environment.
Details for each planning method are as follows.
IMRTReference plans were computed selecting as benchmark
the ‘conventional’ intensity modulation approach with fixedgantry and intensity modulated beams delivering the doseby means of the sliding window approach. In Eclipse, theIMRT optimisation engine computes optimal fluence mapsfrom dose volume constraints derived from the generalplanning objectives [7–9,35,36]. Optimal fluence maps arethen converted by a leaf motion calculator into actual flu-ence maps which are deliverable using a multileaf collima-tor, for either a dynamic or a static method. In both casesthe same segmentation algorithm, the so-called ‘slidingwindow’ or ‘moving slit’, is applied. For the current studyonly the dynamic mode was selected. Plans were individu-ally optimised using five coplanar fields equally spaced.
RapidArc (RA)At a planning level, RapidArc consists of optimising a
dose distribution from dose–volume objectives. To achievethe desired level of modulation required, the optimiser isenabled to continuously vary the instantaneous dose rate(DR), MLC leaf positions, as well as the gantry rotationalspeed (GS, from a maximum of �5.5 �/s). To minimise thecontribution of tongue and groove effect during the arcrotation and to benefit from leaves trajectories non-copla-nar with respect to patient’s axis, the collimator rotationin RapidArc remains fixed to a value different from zero.In the present study the collimator was rotated to 45�.The entire gantry rotation is described in the optimisationprocess by a sequence of 177 control points, CP, i.e. oneevery �2�. The optimisation is based on the so-called Pro-gressive Resolution Optimisation (PRO) algorithm. WithPRO the total 360� arc is initially optimized considering 10beam angles. Thus the first resolution phase of the opitim-izer has an initial distribution of MLC shapes, with the doserate and gantry speed set at their respective maximum al-lowed values. The process is then divided in major phases(multi-resolution levels, MR) during each of them MLCshapes, DR and gantry speed are simultaneously optimisedfor a fixed number of iterations. At the end of each MRphase, the number of CPs is increased by a factor �2 andthe process repeated until the final number of 177 CPs isreached. Iterations in the optimisation loop inside a MR le-vel are ruled by means of a gradient back projection algo-rithm to minimise differences between current anddesired doses in the cost function, which is built on the basisof dose volume objectives defined by users. Variations ofMLC shapes, DR or gantry speed settings are randomly and
simultaneously performed in the search for each controlpoint. Seven random iterations (variations of MLC, DR andGS) are performed in parallel on a single control point be-fore a change is accepted. All control points in a MR levelare searched once before any is touched a second time.All this means there is an intrinsic stochastic componentin the process to allow variations in the search patterns aim-ing to avoid traps in local minima. In synthesis, to generatethe pattern of variable MU/� complementary to MLC shapesin creating the desired dynamic volumetric modulation, GSis kept as high as possible and reduced only when higherdose per degree is needed. Similarly, DR is reduced whenneeded to generate modulation with low dose per degree.Priority is given to DR variation over GS. During all phasesthe mechanical, electronic and dosimetric limits of the sys-tem are taken into account to prevent generation of illegalpatterns (namely: 0.5–5.54 �/s for GS, 0–600 for DR (ex-tended to 1000 for the Novalis TX linac model), 0.2–20 MU/� for the dose per degree and 0 to 3 cm/s for theMLC speed). Rational for the implementation of MR PRO isthat [28] the efficiency (speed vs. convergence) of the opti-misation is related to the number of CP used being fast (butnot converging) with low number of CP and slow (but con-verging) for high numbers. PRO utilises fewer control pointsto approach the convergent solution and then progressivelyincrements the number of CP to final improvements. Thedose distribution is computed during optimisation with afast Multi-Resolution Dose Calculation Algorithm (MRDC).When dose is calculated for a particular control point, theMLC motion and dose rate are converted into a temporaryfluence that models the linac head scattering, and theMLC leakage, rounded leaf ends, tongue and groove designas well as the leaf motion between neighbour controlpoints. MRDC is based on the convolution superposition prin-ciple and it uses 3D convolution scatter computation. Thescatter model is based on 3D superposition of Monte Carlosimulated point spread functions. MRDC calculates the scat-ter component using variable resolutions: finer close to thelocation of primary interactions, coarser at larger distances.
Both the optimisation and final dose calculation phaseswere performed for this study on a four core processor Dell490 workstation with 3 GB RAM and 3 GHz clock taking onaverage about 35 min each.
Evaluation toolsQuantitative evaluation of plans was performed by means
of standard dose–volume histogram (DVH).For PTV, the values of D98% and D2% (dose received by the
98% and 2% of the volume) were defined as metrics for min-imum and maximum doses and consequently reported. Tocomplement the appraisal of minimum dose, V95% (the vol-ume receiving at least 95% of the prescribed dose) was re-ported. The homogeneity of the treatment was expressedin terms of D5%–D95% (difference between the dose covering5% and 95% of the PTV). The degree of conformality of theplans was measured with a Conformity Index, CI90%, definedas the ratio between the patient volume receiving at least90% of the prescribed dose and the volume of the PTV.
For OARs, the analysis included the mean dose, the max-imum dose expressed as D2% and as D2cm3 and a set of appro-

L. Cozzi et al. / Radiotherapy and Oncology 89 (2008) 180–191 183
priate VX and DY values. For rectum and bladder, NormalTissue Complication Probability (NTCP) was computed usingthe relative seriality model of Kallmann [22] to ascertainthe expected incidence of complications. Parameters forvarious endpoints were derived from literature and reportedin Table 1. In the relative seriality model, s represents thedegree of seriality of the organ (1 is for an organ ideallyserial), c is the dose-response steepness index and TD50 isthe dose delivered to the whole organ to induce NTCP = 50%.Given the very low NTCP expected at 50 Gy with the OARsparing achievable with the RA and IMRT techniques, calcu-lations were repeated also for higher dose prescriptions (60and 70 Gy) assuming the same treatment plan quality.
For healthy tissue, the integral dose, ‘‘DoseInt’’ is de-fined as the integral of the absorbed dose extended to overall voxels excluding those within the target volume (DoseIntdimensions are Gy cm3). This was reported together withthe observed mean dose and some representative VxGyvalue.
In addition, to analyse the volumetric dose fall-off as afunction of the 3D distance from the target edge, the aver-age percentage dose (with respect to the prescription dose)measured on shells 1 mm thick at 5, 10 and 15 cm from thePTV was reported as a metric of the peripheral dose. Theseshells were obtained by expanding the PTV in three dimen-sions and cropping at patient’s surface. This method is feltto be more consistent to appraise the long distance dosebath in a multi field (or arc) treatment setup rather thenreporting dose estimates at nominal distances from fieldedges without a correlation to the PTV shape.
All data presented in the text, tables and figures referto the mean and standard deviation of the above-men-tioned parameters, averaged over the eight selectedcases. To visualise the global difference between tech-niques, average cumulative DVH for PTV, OARs andhealthy tissue, were built from the individual DVHs. Thesehistograms are obtained by averaging the correspondingvolumes over the whole patient’s cohort each dose bin(0.01 Gy in this case).
To appraise the difference between the techniques, thepaired, two-tails Student’s t-test was applied. Data wereconsidered statistically significant for p < 0.05.
ResultsDose distributions are shown for one example in Fig. 1 for
axial and coronal views. This figure allows visualisation of
Table 1Parameters used to compute NTCP with the relative seriality model
Organ Endpoint D
Rectuma Bleeding 8Rectumb Necrosis/stenosis 8Bladdera Contracture and volume loss 8Bladderb Contracture and volume loss 8Small bowela Obstruction perforation 5Small bowelb Obstruction perforation 6
Different datasets or endpoints have been labelled with ‘a’ and ‘b’.
the main characteristics of RapidArc compared to IMRT,with a systematic reduction of bladder and rectum involve-ment and a reduced dose bath. Similar results were ob-tained for the other patients and through the entireextension of the target volume.
Fig. 2 shows the average DVH for the PTV comparing in 2aRapidArc (solid lines) to IMRT (dashed lines) while Fig. 2b(RapidArc) and 2c (IMRT) show the average DVH and the cor-responding ±1 standard deviation uncertainty band to ap-praise the relative inter-patient variability, slightlyinferior for RapidArc.
Fig. 3 reports the average DVH computed for the variousOARs and for the healthy tissue comparing RapidArc (solidlines) to IMRT (dashed lines).
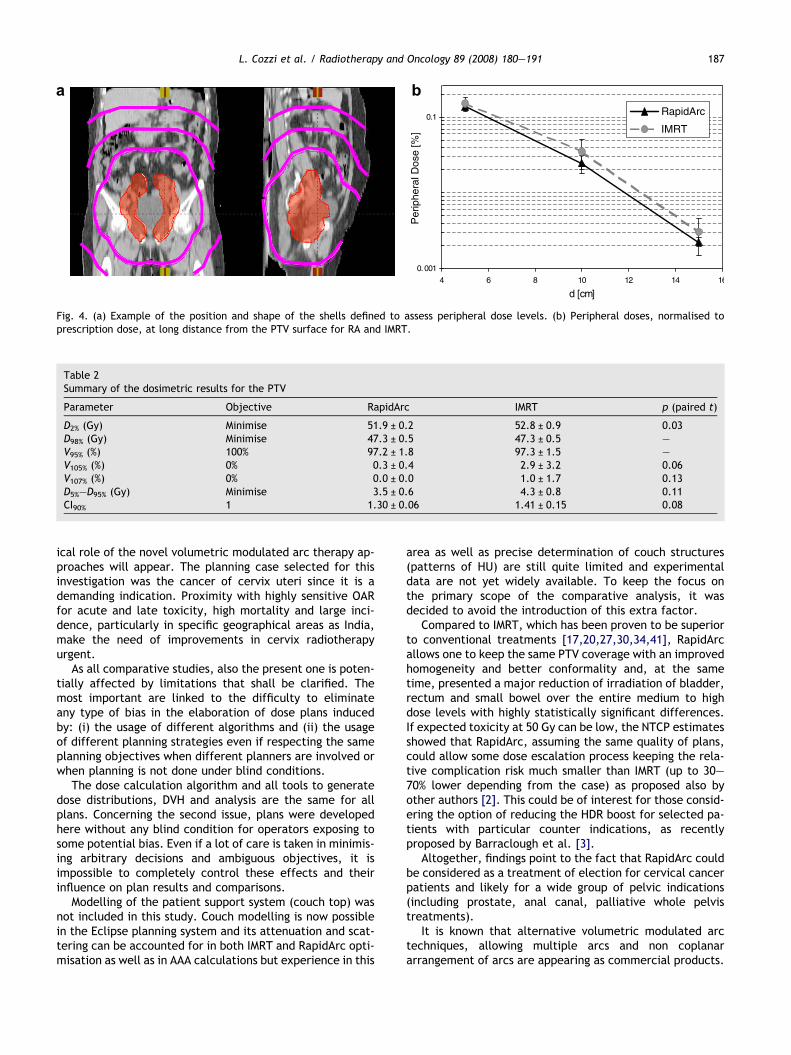
Fig. 4 reports the comparison of peripheral doses.Tables 2 and 3 report numerical findings. Averages are
over the eight investigated patients and errors indicated in-ter-patient variability at 1 standard deviation level.
Target coverage and dose homogeneityRapidArc showed a slightly improved target coverage
compared to IMRT in terms of D2% and D5%–D95% (in the firstcase statistically significant while the latter case with ptending to significance). No statistical difference was ob-served in terms of minimum dose. Measured homogeneityresulted in 7.0 ± 1.0% for RapidArc and 8.6 ± 1.6% for IMRT.RapidArc proved also better conformality with an averageCI90% reduction of �8% in the case of already highly confor-mal treatments (CI = 1.3 for RA).
Organs at riskResults from DVH analysis showed a systematic and
highly statistically significant reduction in OAR involve-ment with RA compared to IMRT. The only parameterwhere both techniques showed equivalent findings inall organs is D2%, the maximum significant dose. Thisis obvious since for all patients, bladder, rectum andbowel are in contact or overlap with PTV and thereforecorrelate their maximum doses to the minimum dose toPTV.
RectumThe mean dose was reduced by about 6–10 Gy depend-
ing if the entire organ or only the fraction not included inthe PTV is considered. Similar trends were observed forthe various Dx parameters with reductions ranging from�3 to 14.4 Gy (corresponding to relative better sparingfrom �6 to 42%). Relevant is the case of V40Gy representative
50 (Gy) c s Ref.
3.1 1.69 0.49 [32]0 2.2 1.5 [1,20]0 3 0.18 [1,20]0.3 3 1.3 [22]3.6 2.3 1.5 [1]2 2.1 0.14 [20]
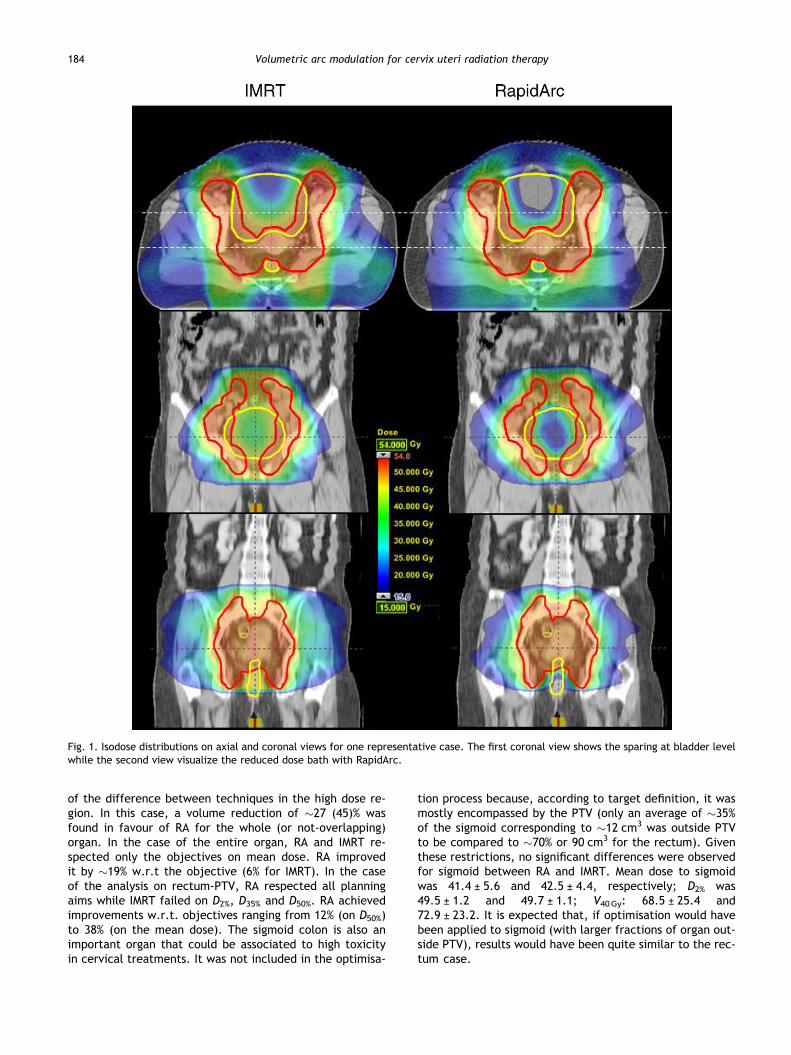
Fig. 1. Isodose distributions on axial and coronal views for one representative case. The first coronal view shows the sparing at bladder levelwhile the second view visualize the reduced dose bath with RapidArc.
184 Volumetric arc modulation for cervix uteri radiation therapy
of the difference between techniques in the high dose re-gion. In this case, a volume reduction of �27 (45)% wasfound in favour of RA for the whole (or not-overlapping)organ. In the case of the entire organ, RA and IMRT re-spected only the objectives on mean dose. RA improvedit by �19% w.r.t the objective (6% for IMRT). In the caseof the analysis on rectum-PTV, RA respected all planningaims while IMRT failed on D2%, D35% and D50%. RA achievedimprovements w.r.t. objectives ranging from 12% (on D50%)to 38% (on the mean dose). The sigmoid colon is also animportant organ that could be associated to high toxicityin cervical treatments. It was not included in the optimisa-
tion process because, according to target definition, it wasmostly encompassed by the PTV (only an average of �35%of the sigmoid corresponding to �12 cm3 was outside PTVto be compared to �70% or 90 cm3 for the rectum). Giventhese restrictions, no significant differences were observedfor sigmoid between RA and IMRT. Mean dose to sigmoidwas 41.4 ± 5.6 and 42.5 ± 4.4, respectively; D2% was49.5 ± 1.2 and 49.7 ± 1.1; V40Gy: 68.5 ± 25.4 and72.9 ± 23.2. It is expected that, if optimisation would havebeen applied to sigmoid (with larger fractions of organ out-side PTV), results would have been quite similar to the rec-tum case.
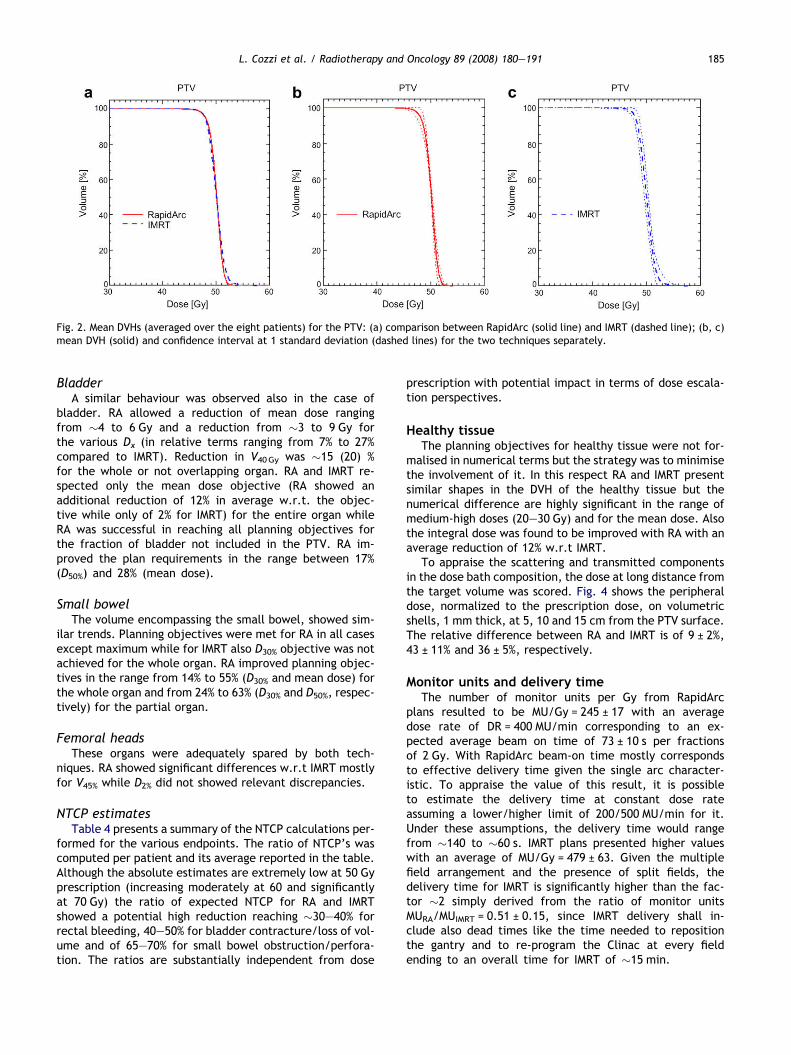
Fig. 2. Mean DVHs (averaged over the eight patients) for the PTV: (a) comparison between RapidArc (solid line) and IMRT (dashed line); (b, c)mean DVH (solid) and confidence interval at 1 standard deviation (dashed lines) for the two techniques separately.
L. Cozzi et al. / Radiotherapy and Oncology 89 (2008) 180–191 185
BladderA similar behaviour was observed also in the case of
bladder. RA allowed a reduction of mean dose rangingfrom �4 to 6 Gy and a reduction from �3 to 9 Gy forthe various Dx (in relative terms ranging from 7% to 27%compared to IMRT). Reduction in V40Gy was �15 (20) %for the whole or not overlapping organ. RA and IMRT re-spected only the mean dose objective (RA showed anadditional reduction of 12% in average w.r.t. the objec-tive while only of 2% for IMRT) for the entire organ whileRA was successful in reaching all planning objectives forthe fraction of bladder not included in the PTV. RA im-proved the plan requirements in the range between 17%(D50%) and 28% (mean dose).
Small bowelThe volume encompassing the small bowel, showed sim-
ilar trends. Planning objectives were met for RA in all casesexcept maximum while for IMRT also D30% objective was notachieved for the whole organ. RA improved planning objec-tives in the range from 14% to 55% (D30% and mean dose) forthe whole organ and from 24% to 63% (D30% and D50%, respec-tively) for the partial organ.
Femoral headsThese organs were adequately spared by both tech-
niques. RA showed significant differences w.r.t IMRT mostlyfor V45% while D2% did not showed relevant discrepancies.
NTCP estimatesTable 4 presents a summary of the NTCP calculations per-
formed for the various endpoints. The ratio of NTCP’s wascomputed per patient and its average reported in the table.Although the absolute estimates are extremely low at 50 Gyprescription (increasing moderately at 60 and significantlyat 70 Gy) the ratio of expected NTCP for RA and IMRTshowed a potential high reduction reaching �30–40% forrectal bleeding, 40–50% for bladder contracture/loss of vol-ume and of 65–70% for small bowel obstruction/perfora-tion. The ratios are substantially independent from dose
prescription with potential impact in terms of dose escala-tion perspectives.
Healthy tissueThe planning objectives for healthy tissue were not for-
malised in numerical terms but the strategy was to minimisethe involvement of it. In this respect RA and IMRT presentsimilar shapes in the DVH of the healthy tissue but thenumerical difference are highly significant in the range ofmedium-high doses (20–30 Gy) and for the mean dose. Alsothe integral dose was found to be improved with RA with anaverage reduction of 12% w.r.t IMRT.
To appraise the scattering and transmitted componentsin the dose bath composition, the dose at long distance fromthe target volume was scored. Fig. 4 shows the peripheraldose, normalized to the prescription dose, on volumetricshells, 1 mm thick, at 5, 10 and 15 cm from the PTV surface.The relative difference between RA and IMRT is of 9 ± 2%,43 ± 11% and 36 ± 5%, respectively.
Monitor units and delivery timeThe number of monitor units per Gy from RapidArc
plans resulted to be MU/Gy = 245 ± 17 with an averagedose rate of DR = 400 MU/min corresponding to an ex-pected average beam on time of 73 ± 10 s per fractionsof 2 Gy. With RapidArc beam-on time mostly correspondsto effective delivery time given the single arc character-istic. To appraise the value of this result, it is possibleto estimate the delivery time at constant dose rateassuming a lower/higher limit of 200/500 MU/min for it.Under these assumptions, the delivery time would rangefrom �140 to �60 s. IMRT plans presented higher valueswith an average of MU/Gy = 479 ± 63. Given the multiplefield arrangement and the presence of split fields, thedelivery time for IMRT is significantly higher than the fac-tor �2 simply derived from the ratio of monitor unitsMURA/MUIMRT = 0.51 ± 0.15, since IMRT delivery shall in-clude also dead times like the time needed to repositionthe gantry and to re-program the Clinac at every fieldending to an overall time for IMRT of �15 min.
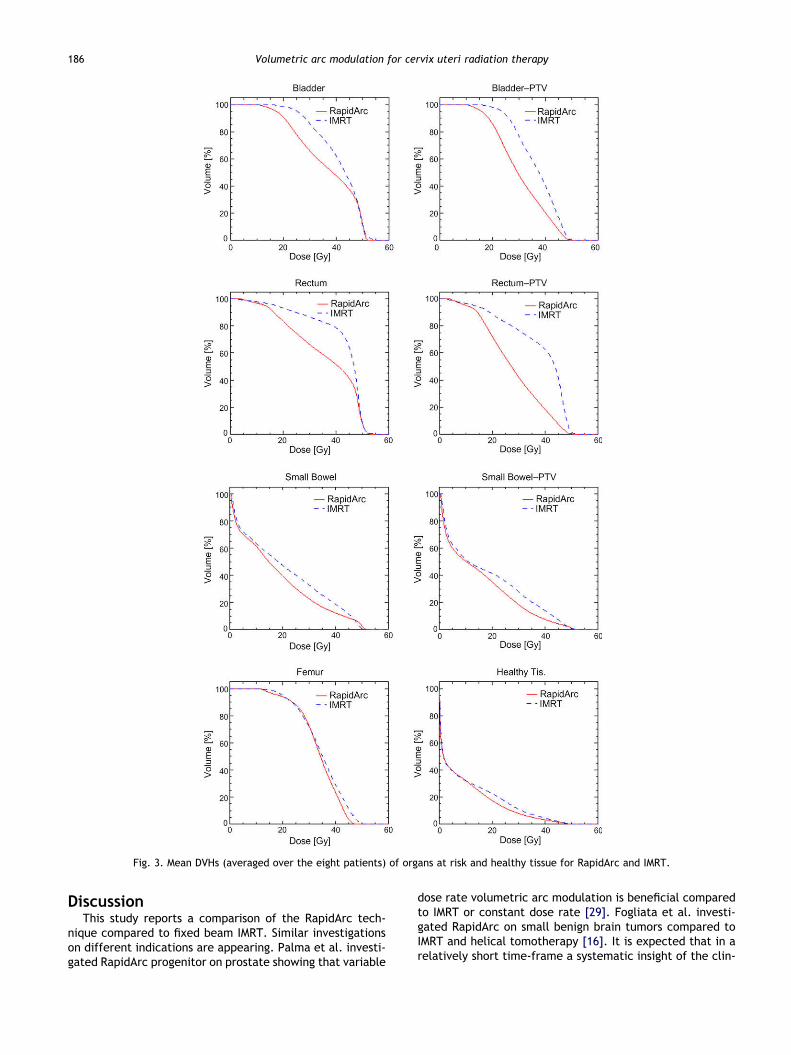
Fig. 3. Mean DVHs (averaged over the eight patients) of organs at risk and healthy tissue for RapidArc and IMRT.
186 Volumetric arc modulation for cervix uteri radiation therapy
DiscussionThis study reports a comparison of the RapidArc tech-
nique compared to fixed beam IMRT. Similar investigationson different indications are appearing. Palma et al. investi-gated RapidArc progenitor on prostate showing that variable
dose rate volumetric arc modulation is beneficial comparedto IMRT or constant dose rate [29]. Fogliata et al. investi-gated RapidArc on small benign brain tumors compared toIMRT and helical tomotherapy [16]. It is expected that in arelatively short time-frame a systematic insight of the clin-
0.001
0.1
4 6 8 10 12 14 16
d [cm]
Per
iphe
ral D
ose
[%]
RapidArc
IMRT
Fig. 4. (a) Example of the position and shape of the shells defined to assess peripheral dose levels. (b) Peripheral doses, normalised toprescription dose, at long distance from the PTV surface for RA and IMRT.
Table 2Summary of the dosimetric results for the PTV
Parameter Objective RapidArc IMRT p (paired t)
D2% (Gy) Minimise 51.9 ± 0.2 52.8 ± 0.9 0.03D98% (Gy) Minimise 47.3 ± 0.5 47.3 ± 0.5 –V95% (%) 100% 97.2 ± 1.8 97.3 ± 1.5 –V105% (%) 0% 0.3 ± 0.4 2.9 ± 3.2 0.06V107% (%) 0% 0.0 ± 0.0 1.0 ± 1.7 0.13D5%–D95% (Gy) Minimise 3.5 ± 0.6 4.3 ± 0.8 0.11CI90% 1 1.30 ± 0.06 1.41 ± 0.15 0.08
L. Cozzi et al. / Radiotherapy and Oncology 89 (2008) 180–191 187
ical role of the novel volumetric modulated arc therapy ap-proaches will appear. The planning case selected for thisinvestigation was the cancer of cervix uteri since it is ademanding indication. Proximity with highly sensitive OARfor acute and late toxicity, high mortality and large inci-dence, particularly in specific geographical areas as India,make the need of improvements in cervix radiotherapyurgent.
As all comparative studies, also the present one is poten-tially affected by limitations that shall be clarified. Themost important are linked to the difficulty to eliminateany type of bias in the elaboration of dose plans inducedby: (i) the usage of different algorithms and (ii) the usageof different planning strategies even if respecting the sameplanning objectives when different planners are involved orwhen planning is not done under blind conditions.
The dose calculation algorithm and all tools to generatedose distributions, DVH and analysis are the same for allplans. Concerning the second issue, plans were developedhere without any blind condition for operators exposing tosome potential bias. Even if a lot of care is taken in minimis-ing arbitrary decisions and ambiguous objectives, it isimpossible to completely control these effects and theirinfluence on plan results and comparisons.
Modelling of the patient support system (couch top) wasnot included in this study. Couch modelling is now possiblein the Eclipse planning system and its attenuation and scat-tering can be accounted for in both IMRT and RapidArc opti-misation as well as in AAA calculations but experience in this
area as well as precise determination of couch structures(patterns of HU) are still quite limited and experimentaldata are not yet widely available. To keep the focus onthe primary scope of the comparative analysis, it wasdecided to avoid the introduction of this extra factor.
Compared to IMRT, which has been proven to be superiorto conventional treatments [17,20,27,30,34,41], RapidArcallows one to keep the same PTV coverage with an improvedhomogeneity and better conformality and, at the sametime, presented a major reduction of irradiation of bladder,rectum and small bowel over the entire medium to highdose levels with highly statistically significant differences.If expected toxicity at 50 Gy can be low, the NTCP estimatesshowed that RapidArc, assuming the same quality of plans,could allow some dose escalation process keeping the rela-tive complication risk much smaller than IMRT (up to 30–70% lower depending from the case) as proposed also byother authors [2]. This could be of interest for those consid-ering the option of reducing the HDR boost for selected pa-tients with particular counter indications, as recentlyproposed by Barraclough et al. [3].
Altogether, findings point to the fact that RapidArc couldbe considered as a treatment of election for cervical cancerpatients and likely for a wide group of pelvic indications(including prostate, anal canal, palliative whole pelvistreatments).
It is known that alternative volumetric modulated arctechniques, allowing multiple arcs and non coplanararrangement of arcs are appearing as commercial products.
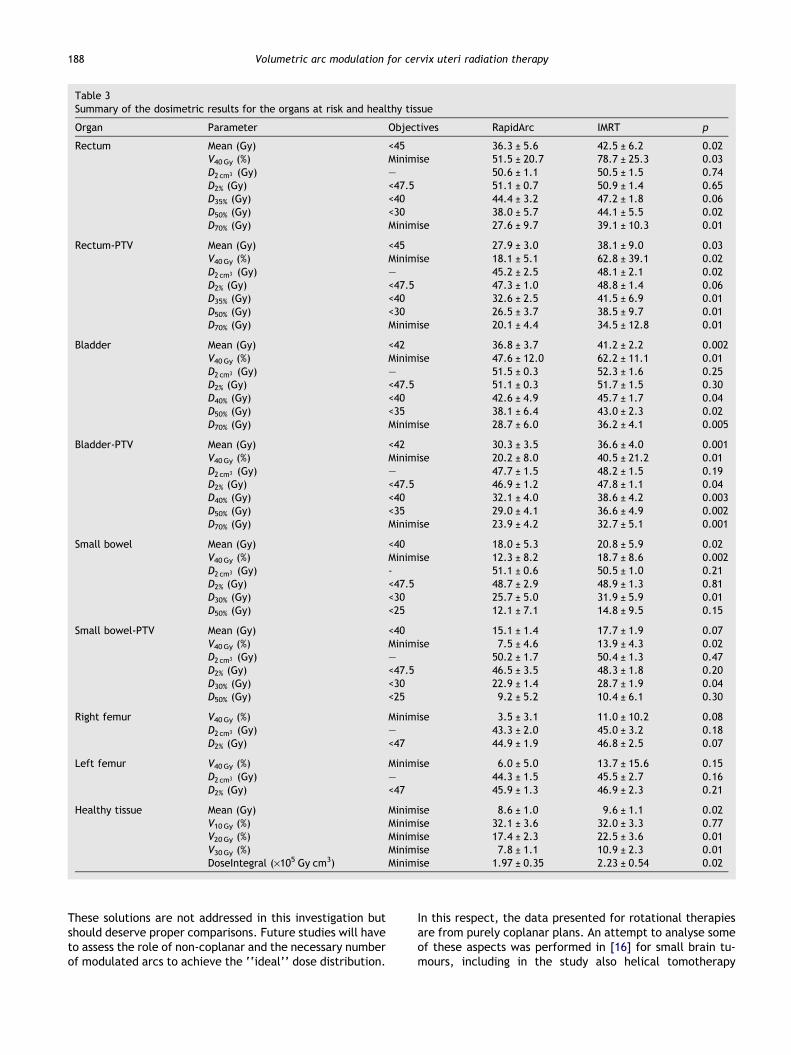
Table 3Summary of the dosimetric results for the organs at risk and healthy tissue
Organ Parameter Objectives RapidArc IMRT p
Rectum Mean (Gy) <45 36.3 ± 5.6 42.5 ± 6.2 0.02V40Gy (%) Minimise 51.5 ± 20.7 78.7 ± 25.3 0.03D2 cm3 (Gy) – 50.6 ± 1.1 50.5 ± 1.5 0.74D2% (Gy) <47.5 51.1 ± 0.7 50.9 ± 1.4 0.65D35% (Gy) <40 44.4 ± 3.2 47.2 ± 1.8 0.06D50% (Gy) <30 38.0 ± 5.7 44.1 ± 5.5 0.02D70% (Gy) Minimise 27.6 ± 9.7 39.1 ± 10.3 0.01
Rectum-PTV Mean (Gy) <45 27.9 ± 3.0 38.1 ± 9.0 0.03V40Gy (%) Minimise 18.1 ± 5.1 62.8 ± 39.1 0.02D2 cm3 (Gy) – 45.2 ± 2.5 48.1 ± 2.1 0.02D2% (Gy) <47.5 47.3 ± 1.0 48.8 ± 1.4 0.06D35% (Gy) <40 32.6 ± 2.5 41.5 ± 6.9 0.01D50% (Gy) <30 26.5 ± 3.7 38.5 ± 9.7 0.01D70% (Gy) Minimise 20.1 ± 4.4 34.5 ± 12.8 0.01
Bladder Mean (Gy) <42 36.8 ± 3.7 41.2 ± 2.2 0.002V40Gy (%) Minimise 47.6 ± 12.0 62.2 ± 11.1 0.01D2 cm3 (Gy) – 51.5 ± 0.3 52.3 ± 1.6 0.25D2% (Gy) <47.5 51.1 ± 0.3 51.7 ± 1.5 0.30D40% (Gy) <40 42.6 ± 4.9 45.7 ± 1.7 0.04D50% (Gy) <35 38.1 ± 6.4 43.0 ± 2.3 0.02D70% (Gy) Minimise 28.7 ± 6.0 36.2 ± 4.1 0.005
Bladder-PTV Mean (Gy) <42 30.3 ± 3.5 36.6 ± 4.0 0.001V40Gy (%) Minimise 20.2 ± 8.0 40.5 ± 21.2 0.01D2 cm3 (Gy) – 47.7 ± 1.5 48.2 ± 1.5 0.19D2% (Gy) <47.5 46.9 ± 1.2 47.8 ± 1.1 0.04D40% (Gy) <40 32.1 ± 4.0 38.6 ± 4.2 0.003D50% (Gy) <35 29.0 ± 4.1 36.6 ± 4.9 0.002D70% (Gy) Minimise 23.9 ± 4.2 32.7 ± 5.1 0.001
Small bowel Mean (Gy) <40 18.0 ± 5.3 20.8 ± 5.9 0.02V40Gy (%) Minimise 12.3 ± 8.2 18.7 ± 8.6 0.002D2 cm3 (Gy) - 51.1 ± 0.6 50.5 ± 1.0 0.21D2% (Gy) <47.5 48.7 ± 2.9 48.9 ± 1.3 0.81D30% (Gy) <30 25.7 ± 5.0 31.9 ± 5.9 0.01D50% (Gy) <25 12.1 ± 7.1 14.8 ± 9.5 0.15
Small bowel-PTV Mean (Gy) <40 15.1 ± 1.4 17.7 ± 1.9 0.07V40Gy (%) Minimise 7.5 ± 4.6 13.9 ± 4.3 0.02D2 cm3 (Gy) – 50.2 ± 1.7 50.4 ± 1.3 0.47D2% (Gy) <47.5 46.5 ± 3.5 48.3 ± 1.8 0.20D30% (Gy) <30 22.9 ± 1.4 28.7 ± 1.9 0.04D50% (Gy) <25 9.2 ± 5.2 10.4 ± 6.1 0.30
Right femur V40Gy (%) Minimise 3.5 ± 3.1 11.0 ± 10.2 0.08D2 cm3 (Gy) – 43.3 ± 2.0 45.0 ± 3.2 0.18D2% (Gy) <47 44.9 ± 1.9 46.8 ± 2.5 0.07
Left femur V40Gy (%) Minimise 6.0 ± 5.0 13.7 ± 15.6 0.15D2 cm3 (Gy) – 44.3 ± 1.5 45.5 ± 2.7 0.16D2% (Gy) <47 45.9 ± 1.3 46.9 ± 2.3 0.21
Healthy tissue Mean (Gy) Minimise 8.6 ± 1.0 9.6 ± 1.1 0.02V10Gy (%) Minimise 32.1 ± 3.6 32.0 ± 3.3 0.77V20Gy (%) Minimise 17.4 ± 2.3 22.5 ± 3.6 0.01V30Gy (%) Minimise 7.8 ± 1.1 10.9 ± 2.3 0.01DoseIntegral (·105 Gy cm3) Minimise 1.97 ± 0.35 2.23 ± 0.54 0.02
188 Volumetric arc modulation for cervix uteri radiation therapy
These solutions are not addressed in this investigation butshould deserve proper comparisons. Future studies will haveto assess the role of non-coplanar and the necessary numberof modulated arcs to achieve the ‘‘ideal’’ dose distribution.
In this respect, the data presented for rotational therapiesare from purely coplanar plans. An attempt to analyse someof these aspects was performed in [16] for small brain tu-mours, including in the study also helical tomotherapy
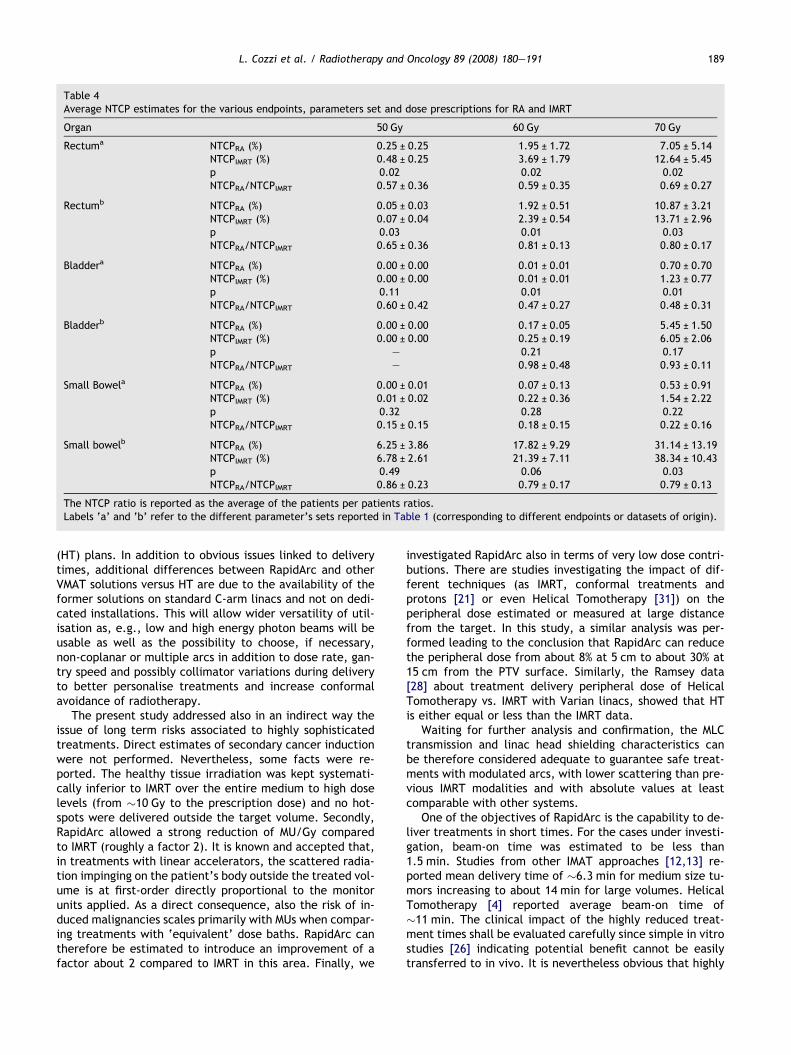
Table 4Average NTCP estimates for the various endpoints, parameters set and dose prescriptions for RA and IMRT
Organ 50 Gy 60 Gy 70 Gy
Rectuma NTCPRA (%) 0.25 ± 0.25 1.95 ± 1.72 7.05 ± 5.14NTCPIMRT (%) 0.48 ± 0.25 3.69 ± 1.79 12.64 ± 5.45p 0.02 0.02 0.02NTCPRA/NTCPIMRT 0.57 ± 0.36 0.59 ± 0.35 0.69 ± 0.27
Rectumb NTCPRA (%) 0.05 ± 0.03 1.92 ± 0.51 10.87 ± 3.21NTCPIMRT (%) 0.07 ± 0.04 2.39 ± 0.54 13.71 ± 2.96p 0.03 0.01 0.03NTCPRA/NTCPIMRT 0.65 ± 0.36 0.81 ± 0.13 0.80 ± 0.17
Bladdera NTCPRA (%) 0.00 ± 0.00 0.01 ± 0.01 0.70 ± 0.70NTCPIMRT (%) 0.00 ± 0.00 0.01 ± 0.01 1.23 ± 0.77p 0.11 0.01 0.01NTCPRA/NTCPIMRT 0.60 ± 0.42 0.47 ± 0.27 0.48 ± 0.31
Bladderb NTCPRA (%) 0.00 ± 0.00 0.17 ± 0.05 5.45 ± 1.50NTCPIMRT (%) 0.00 ± 0.00 0.25 ± 0.19 6.05 ± 2.06p – 0.21 0.17NTCPRA/NTCPIMRT – 0.98 ± 0.48 0.93 ± 0.11
Small Bowela NTCPRA (%) 0.00 ± 0.01 0.07 ± 0.13 0.53 ± 0.91NTCPIMRT (%) 0.01 ± 0.02 0.22 ± 0.36 1.54 ± 2.22p 0.32 0.28 0.22NTCPRA/NTCPIMRT 0.15 ± 0.15 0.18 ± 0.15 0.22 ± 0.16
Small bowelb NTCPRA (%) 6.25 ± 3.86 17.82 ± 9.29 31.14 ± 13.19NTCPIMRT (%) 6.78 ± 2.61 21.39 ± 7.11 38.34 ± 10.43p 0.49 0.06 0.03NTCPRA/NTCPIMRT 0.86 ± 0.23 0.79 ± 0.17 0.79 ± 0.13
The NTCP ratio is reported as the average of the patients per patients ratios.Labels ‘a’ and ‘b’ refer to the different parameter’s sets reported in Table 1 (corresponding to different endpoints or datasets of origin).
L. Cozzi et al. / Radiotherapy and Oncology 89 (2008) 180–191 189
(HT) plans. In addition to obvious issues linked to deliverytimes, additional differences between RapidArc and otherVMAT solutions versus HT are due to the availability of theformer solutions on standard C-arm linacs and not on dedi-cated installations. This will allow wider versatility of util-isation as, e.g., low and high energy photon beams will beusable as well as the possibility to choose, if necessary,non-coplanar or multiple arcs in addition to dose rate, gan-try speed and possibly collimator variations during deliveryto better personalise treatments and increase conformalavoidance of radiotherapy.
The present study addressed also in an indirect way theissue of long term risks associated to highly sophisticatedtreatments. Direct estimates of secondary cancer inductionwere not performed. Nevertheless, some facts were re-ported. The healthy tissue irradiation was kept systemati-cally inferior to IMRT over the entire medium to high doselevels (from �10 Gy to the prescription dose) and no hot-spots were delivered outside the target volume. Secondly,RapidArc allowed a strong reduction of MU/Gy comparedto IMRT (roughly a factor 2). It is known and accepted that,in treatments with linear accelerators, the scattered radia-tion impinging on the patient’s body outside the treated vol-ume is at first-order directly proportional to the monitorunits applied. As a direct consequence, also the risk of in-duced malignancies scales primarily with MUs when compar-ing treatments with ‘equivalent’ dose baths. RapidArc cantherefore be estimated to introduce an improvement of afactor about 2 compared to IMRT in this area. Finally, we
investigated RapidArc also in terms of very low dose contri-butions. There are studies investigating the impact of dif-ferent techniques (as IMRT, conformal treatments andprotons [21] or even Helical Tomotherapy [31]) on theperipheral dose estimated or measured at large distancefrom the target. In this study, a similar analysis was per-formed leading to the conclusion that RapidArc can reducethe peripheral dose from about 8% at 5 cm to about 30% at15 cm from the PTV surface. Similarly, the Ramsey data[28] about treatment delivery peripheral dose of HelicalTomotherapy vs. IMRT with Varian linacs, showed that HTis either equal or less than the IMRT data.
Waiting for further analysis and confirmation, the MLCtransmission and linac head shielding characteristics canbe therefore considered adequate to guarantee safe treat-ments with modulated arcs, with lower scattering than pre-vious IMRT modalities and with absolute values at leastcomparable with other systems.
One of the objectives of RapidArc is the capability to de-liver treatments in short times. For the cases under investi-gation, beam-on time was estimated to be less than1.5 min. Studies from other IMAT approaches [12,13] re-ported mean delivery time of �6.3 min for medium size tu-mors increasing to about 14 min for large volumes. HelicalTomotherapy [4] reported average beam-on time of�11 min. The clinical impact of the highly reduced treat-ment times shall be evaluated carefully since simple in vitrostudies [26] indicating potential benefit cannot be easilytransferred to in vivo. It is nevertheless obvious that highly

190 Volumetric arc modulation for cervix uteri radiation therapy
reduced beam on times and consequently effective treat-ment times will have a strong impact on the clinicalthroughput (e.g. waiting list reduction) and on the individ-ual patients management (improved comfort, reducedmovements and internal organs dynamics, increased spacefor image guidance on large scales) with potential signifi-cant synergies with the conformal avoidance degree of theRapidArc technique.
A final remark shall be devoted to experimental verifica-tion of RapidArc delivery accuracy compared to calculationestimates. These activities are mandatory before any clini-cal activation of any new technique and RapidArc has to beproperly verified. A dedicated analysis of this issue was be-yond the scope of this comparison but will be part of a ded-icated report from our group.
ConclusionsRapidArc was investigated for cervix uteri cancer and led
to highly significant improvements in OAR and healthy tissuesparing with uncompromised target coverage compared toconventional IMRT. This is equivalent to a highly improveddegree of conformal avoidance treatment. In addition,healthy tissue involvement, at short and long distancenearand far from the target and at both high and very low doselevels was improved with RapidArc compared to IMRT. Thepotential benefit of the better physical dose distribution iscombined with the shorter delivery time, which can haveimpact on both the biological and the logistical level. Clin-ical protocols are now advised to evaluate prospectively thepotential benefit observed at planning level.
DisclosureDr. L. Cozzi acts as Scientific Advisor to Varian Medical
Systems and as Head of Research and Technological Devel-opment to Oncology Institute of Southern Switzerland,Bellinzona.
AcknowledgementsThe study was conducted in strict cooperation with many per-
sons at Varian Medical Systems involved in the development of thisnovel technology. Among them we are particularly grateful for sup-port and assistance to Martin Sabel and Yves Archambault for plan-ning and to Jiri Bocanek for delivery issues. The Phase II randomisedtrial mentioned in the introduction is part of a Research Coopera-tion Agreement between TMH and Varian Medical Systems.
* Corresponding author. Cozzi Luca, Oncology Institute ofSouthern Switzerland, Radiation Oncology Department, MedicalPhysics Unit, 6504 Bellinzona, Switzerland. E-mail address: [email protected]
Received 22 April 2008; received in revised form 12 June 2008;accepted 19 June 2008; Available online 8 August 2008
References[1] Agren-Cronqvist AK. Quantification of the response of heter-
ogeneous tumours and organized normal tissues to fraction-ated radiotherapy. PhD thesis, Stockholm University,Department of Medical Radiation Physics Stockholm; 1995.
[2] Ahmed R, Kim R, Duan J, Meleth S, De Los Santos J, Fiveash J.IMRT dose escalation for positive para-aortic lymph nodes inpatients with locally advanced cancer while reducing dose tobone marrow and other organs at risk. Int J Radiat Oncol BiolPhys 2004;60:505–12.
[3] Barraclough L, Swindell R, Livsey J, Hunter R, Davidson S.External beam boost for cancer of the cervix uteri whenintracavitarz therapy cannot be performed. Int J Radiat OncolBiol Phys 2008;71:772–8.
[4] Bijdekerke P, Verellen D, Tournel K, Vinh-Hung V, Somers F,Biesman P, et al. TomoTherapy: implications on daily work-load and scheduling patients. Radiother Oncol2008;86:224–30.
[5] Bragg C, Windate K, Conway J. Clinical implications of theanisotropic analytical algorithm for IMRT treatment planningand verification. Radiother Oncol 2008;86:276–84.
[6] Cameron C. Sweeping-window arc therapy: an implementationof rotational IMRT with automatic beam-weight calculation.Phys Med Biol 2005;50:4317–36.
[7] Chui C, LoSasso T, Spirou S. Dose calculation for photon beamswith intensity modulation generated by dynamic jaw ormultileaf collimations. Med Phys 1994;21:1237–44.
[8] Chui C, Chan M, Yorke E, Spirou S, Ling C. Delivery of intensity-modulated radiation therapy with a conventional multileafcollimator: comparison of dynamic and segmental methods.Med Phys 2001;28:2441–9.
[9] Convery D, Rosenbloom M. The generation of intensity-mod-ulated fields for conformal radiotherapy by dynamic collima-tion. Phys Med Biol 1992;37:1359–74.
[10] Cotrutz C, Kappas C, Webb S. Intensity modulated arc therapy(IMAT) with centrally blocked rotational fields. Phys Med Biol2000;45:2185–206.
[11] Creutyberg C, Van Putten W, Koper P, et al. For the PORTC(Post Operative Radiation Therapy in Endometrial Carci-noma) Study Group. Surgery and postoperative radiotherapyversus surgery alone for patients with stage 1 endometrialcarcinoma. Multicentre randomized trial. Lancet2000;355:1404–11.
[12] Duthoy W, De Gersem W, Vergote K, Botenberf T, Derie C,Smeets P, et al. Clinical implementation of intensity modu-lated arc therapy (IMAT) for rectal cancer. Int J Radiat OncolBiol Phys 2004;60:794–806.
[13] Duthoy W, De Gersem W, Vergote K, Coghe M, Botenberf T, DeDeene Y, et al. Whole abdominal radiotherpay (WAPRT) usingintensity modulated arc therapy (IMAT): first clinical experi-ence. Int J Radiat Oncol Biol Phys 2003;57:1019–32.
[14] Earl M, Shepard D, Naqvi S, Li X, Zu CX. Inverse planning forintensity modulated arc therapy using direct aperture optimi-zation. Phys Med Biol 2003;21:1075–89.
[15] Fogliata A, Vanetti E, Albers D, et al. On the dosimetricbehaviour of photon dose calculation algorithms in thepresence of simple geometric heterogeneities: comparisonwith Monte Carlo calculations. Phys Med Biol2007;52:1363–85.
[16] Fogliata A, Clivio A, Nicolini G, Vanetti E, Cozzi L. Intensitymodulation with photons for benign intracranial tumours. Aplanning comparison of volumetric single arc, helical arc andfixed gantry techniques. Radiother Oncol 2008; doi:10.1016/j.radonc.2008.07.021.
[17] Georg P, Georg D, Hillbrand M, Kirisits C, Poetter R. Factorsinfluencing bowel sparing in intensity modulated whole pelvicradiotherapy for gynaecological malignancies. Radiother Oncol2006;80:19–26.
[18] Green J, Kirwan J, Tierney J, et al. Survival and recurrenceafter concomitant chemotherapy and radiotherapy for canceron the uterine cervix. A systematic review and meta analysis.Lancet 2001;358:781–6.
L. Cozzi et al. / Radiotherapy and Oncology 89 (2008) 180–191 191
[19] Grisby P. Update on radiation therapy for endometrial cancer.Oncology 2002;16:777–86.
[20] Guckenberger M, Baier K, Richter A, Vordermark D, FlentjeM. Dose Intensity Modulated Radiation Therapy (IMRT)prevent additional toxicity of treating the pelvic lymphnodes compared to treatment of the prostate only? RadiatOncol 2008;3:3.
[21] Hall EJ. Intensity modulated radiation therapy, protons andthe risk of second cancers. Int J Radiat Oncol Biol Phys2006;65:1–7.
[22] Kallmann P, Agren A, Brahme A. Tumour and normal tissueresponses to fractionated non-uniform dose delivery. Int JRadiat Biol 1992;62:249–62.
[23] Knoos T, Wieslander E, Cozzi L, et al. Comparison of dosecalculation algorithms for treatment planning in externalphoton beam therapy for clinical situations. Phys Med Biol2006;51:5785–807.
[24] Lukka H, Hirte H, Fyles A, et al. Concurrent cisplatin basedchemotherapy plus radiotherapy for cervical cancer. A metaanalysis. Clin Oncol 2002;14:203–12.
[25] MacKenzie MA, Robinson DM. Intensity modulated arc deliver-ies approximated by a large number of fixed gantry positionsliding window dynamic multileaf collimator fields. Med Phys2002;29:2359–65.
[26] Moiseenko V, Duzenli C, Durand R. In vitro study of cell survivalfollowing dynamic MLC intensity-modulated radiatioh therapydose delivery. Med Phys 2007;34:1514–20.
[27] Mundt A, Lujan A, Rotmensch J, Waggner S, Yamada D,Fleming G, et al. Intensity modulated whole pelvic radiother-apy in women with gynaecologic malignancies. Int J RadiatOncol Biol Phys 2002;52:1330–7.
[28] Otto K. Volumetric modulated arc therapy: IMRT in a singlearc. Med Phys 2008;35:310–7.
[29] Palma D, Vollans E, James K, Nakano S, Moiseenko V, ShafferR, et al. Volumetric modulated arc therapy for delivery ofprostate radiotherapy. Comparison with intensity modulatedradiotherapy and three-dimensional conformal radiotherapy.Int J Radiat Oncol Biol Phys 2008. e-pub.
[30] Portelance L, Chao C, Grisby P, Benner H, Low D. Intensitymodulated radiation therapy (IMRT) reduces small bowel,rectum and bladder doses in patients with cervical cancer
receiving pelvic and para-aortic irradiation. Int J Radiat OncolBiol Phys 2001;51:261–6.
[31] Ramsey C, Seibert R, Mahan S, Desai D, Chase D. Out of fielddosimetry measurements for a helical tomotherapy system. JAppl Clin Med Phys 2006:7.
[32] Rancati T, Fiorino C, Gagliardi G, et al. Fitting late rectalbleeding data using different NTCP models: results from anItalian multi-centric study (AIROPROS0101). Radiother Oncol2004;73:21–32.
[33] Roeske J, Mundt A, Halpen H, et al. Late rectal sequelaefollowing definitive radiation therapy for carcinoma of theuterine cervix. A dosimetric analysis. Int J Radiat Oncol BiolPhys 1997;37:351–8.
[34] Roeske J, Lujan A, Rotmensch J, Waggner S, Yamada D, MundtA. Intensity modulated whole pelvic radiation therapy inpatients with gynaecologic malignancies. Int J Radiat OncolBiol Phys 2000;48:1613–21.
[35] Spirou S, Chui C. Generation of arbitrary intensity profiles bydynamic jaws or multileaf collimators. Med Phys1994;21:1031–41.
[36] Spirou S, Chui C. A gradient inverse planning algorithm withdose–volume constrains. Med Phys 1998;25:321–33.
[37] Ulmer W, Pyyry J, Kaissl W. A 3D photon superposition/convolution algorithm and its foundation on results of MonteCarlo calculations. Phys Med Biol 2005;50:1767–90.
[38] Vrdoljak E, Prskalo T, Omrcen T, Situm K, Boraska T, Frleta I,et al. Concomitant chemobrachyradiotherapy owith ifosfa-mide and cisplatin followed by consolidation chemotherapy inlocally advanced squamous cell carcinoma of the uterine cerix.Results of a phase II study. Int J Radiat Oncol Biol Phys2005;61:824–9.
[39] Yu CX. Intensity-modulated arc therapy with dynamic multi-leaf collimation: an alternative to tomotherapy. Phys Med Biol1995;40:1435–49.
[40] Yu CX, Li XA, Ma L, et al. Clinical implementation of intensity-modulated arc therapy. Int J Radiat Oncol Biol Phys2002;53:453–63.
[41] Wong E, D’Souza D, Chen J, Lock M, Rodrigues G, Coad T,et al. Intensity modulated arc therapy for treatment of highrisk endometrial malignancies. Int J Radiat Oncol Biol Phys2005;61:830–41.
本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具