a study to assess the knowledge of staff nurses on …
TRANSCRIPT

i
“A STUDY TO ASSESS THE KNOWLEDGE OF STAFF NURSES
ON NEEDLE STICK INJURY IN SELECTED HOSPITALS AT
BANGALORE WITH A VIEW TO DEVELOP INFORMATIONAL
BOOKLET”
BY
MR. JAGADEESHA D S
Dissertation Submitted to the
Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore
In partial fulfillment of the requirements for the degree of
MASTER OF SCIENCE
In
MEDICAL SURGICAL NURSING
Under the guidance of
ASSO. PROF. MRS. MANJU THOMAS
HOD
DEPARTMENT OF MEDICAL SURGICAL NURSING
SRI LAKSHMI COLLEGE OF NURSING
BANGALORE.
2018

ii
Rajiv Gandhi University of Health Sciences, Karnataka, Bangalore.
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation/thesis entitled “A Study To
Assess The Knowledge Of Staff Nurses On Needle Stick Injury In Selected Hospitals At
Bangalore With A View To Develop Informational Booklet” is a bonafide and genuine
research work carried out by me under the guidance of Asso. Prof. MRS. MANJU
THOMAS, Head of Department, Department of Medical Surgical Nursing, Sri
Lakshmi College of Nursing, Sunkadakatte, Bangalore.
Date: Signature by candidate
Place: Bangalore
MR. JAGADEESHA D S

v
COPYRIGHT
DECLARATION BY THE CANDIDATE
I hereby declare that the Rajiv Gandhi University of Health Sciences,
Karnataka shall have the rights to preserve, use and disseminate this dissertation /
thesis in print or electronic format for academic / research purpose.
Date: Signature of the Candidate
Place: Bangalore
MR. JAGADEESHA D S
© Rajiv Gandhi University of Health Sciences, Karnataka

x
RESEARCH ABSTRACT
Name : Mr. JAGADEESHA D S
Guide : MRS. MANJU THOMAS
Subject : Dissertation submitted in partial fulfillment of the
requirements of the degree of Master of Science in Nursing to Rajiv Gandhi
University of Health Sciences, Bangalore, Karnataka, 2018.
Statement of the problem : “A Study To Assess The Knowledge Of Staff Nurses On
Needle Stick Injury In Selected Hospitals At Bangalore With A View To Develop
Informational Booklet”.
OBJECTIVES OF THE STUDY
1. To assess the knowledge of staff nurses on needle stick injury.
2. To develop an informational booklet on needle stick injury.
3. To associate knowledge of staff nurses on needle stick injury with selected
demographic variables
HYPOTHESIS
H1 - There will be inadequate knowledge regarding needle stick injury staff nurses.
H2 -There will be significant association between knowledge and selected
demographical variables.
RESEARCH DESIGN:
The research design is Non-experimental
RESEARCH APPROACH:
Descriptive survey approach was adopted for the study.
SETTING OF THE STUDY
The setting of the study is selected hospitals, Bangalore, Karnataka

xi
POPULATION
TARGET POPULATION:
The target population of this study is the staff nurses in Bangalore, Karnataka
ACCESSIBLE POPULATION:
The accessible population of this study is the staff nurses in selected hospitals,
Bangalore, Karnataka.
SAMPLE
Sample for the study will be staff nurses who are fulfilling the inclusion criteria
SAMPLE SIZE
For this study a sample of 100 staff nurses will be considered.
SAMPLING TECHNIQUE
Random sampling technique will be adopted to select the sample
SAMPLING CRITERIA:
INCLUSION CRITERIA FOR SAMPLING
The study includes who staff nurses who are:
Registered staff nurses
willing to participate in the study
present on the day of sampling
EXCLUSION CRITERIA FOR SAMPLING
The study excludes staff nurses who are:
not willing to participate in the study
those who are absent on that day
TOOL
The tool used for the collection of data was self-administered questionnaire. It
consisted of three sections.
xii
Sections -1
Socio demographic variables consists of 08 items such age, sex, religion, residence,
Educational qualification, experience, previous classes and Area of working.
Sections -2
The structured Questionnaire on knowledge related to needle stick injury and it
consists of 30 items
The content validity of the tool was ascertained by submitting it to 7 experts. With
certain modifications and rearrangements as suggested by the subject experts, the
second draft of the tool was finalized.
MAIN STUDY:
The main study data collection was done from 20st of May, 2018 to 21
th of June, 2018.
The total sample of main study consisted of 100 staff nurses. Data was collected using
structured questionnaire to assess the knowledge of staff nurses. Each data collection
session last for about 30-40 minutes and it took 20-30 days to complete the study
DATA COLLECTION METHOD:
A formal written permission was obtained from Medical Superintendent of
Srilakshmi Multi Specialty Hospital and Ashraya hospital, Bangalore. The data was
collected from 20st of May, 2018 to 21
th of June, 2018 from staff nurses who fulfilled
sample inclusion criteria. Before conducting the study oral-consent was taken from
them by explaining the purpose of the study.
DATA ANALYSIS:
The data was analyzed on the basis of objective and hypothesis of the study.
The obtained data was analyzed by descriptive and inferential statistics and
interpreted in terms of objectives and hypothesis of the study. The level of
significance was set at 0.01 and 0.05 level of significance.

xiii
MAJOR FINDINGS OF THE STUDY:
Section I
Distribution of participants according to their demographic variables.
Based on the age: 71% were distributed in the 20-30 years, 17% were distributed in
the 31-40 years and 12% were distributed in the 41 years and above.
Based on the sex: 51% were female and 49 % were male.
Based on the religion: 71% were distributed in Hindu, 19% were distributed in
Muslim and 10% were distributed in the Christian.
Based on the residence 39% were distributed in the urban and 61% were distributed
in rural.
Based on the Educational qualification: 71% were distributed in B.Sc. N, 19% were
distributed in GNM and 10% were distributed in the M.Sc.N.
Based on the experience, 64% were distributed <1 years, 18 % were distributed 1-3
years, 18 % were distributed in >3 years
Based on the whether attended any previous classes regarding needle stick
injury: 60% were distributed in No and 40% were distributed in Yes.
Based on the Area of working 36% were in the Ward, 27 % were from the
Causality, 19 % were from the ICU, 7% were in Dialysis, 11% of them in OPD
Section II (Knowledge score)
Knowledge level of the participants regarding the needle sticks injury
The mean knowledge score obtained by staff nurses was 11.13, mean
percentage was 49.76, and standard deviation 3.12

xiv
Section III
Association of knowledge score of participants with selected demographic
variables.
The chi-square value shows that there is no significance association between
age, sex, residence area, religion, area of work and level of knowledge with socio
demographic variable.(P > 0.05)
The experience, qualification and previous classes show the significant
association the level of knowledge.

1
IINNTTRROODDUUCCTTIIOONN

2
1. INTRODUCTION
“CARING FOR THOSE WHO CARE”
“A safe injection is one that does not harm the recipient, does not
expose the provider to any avoidable risk, and does not result in any waste that is
dangerous to the community.”1
Each day thousands of health worker around the world, suffer accidental
occupational exposures during the course of their role of caring for patients. These
injuries can result in a variety of serious and distressing consequence ranging from
extreme anxiety to chronic illness and premature death. The health care workforce, 35
million people worldwide, represents 12% of the working population. The
misconception exists that health care industry is without hazards, but in fact blood
borne exposures encountered can be career and life-ending.2
A needle stick injury is a percutaneous piercing wound typically set by a
needle point, but possibly also by other sharp instruments or objects. Commonly
encountered by people handling needles in the medical setting, such injuries are an
occupational hazard in the medical community. These events are of concern because
of the risk to transmit blood-borne diseases through the passage of the hepatitis B
virus (HBV), the hepatitis C virus (HCV), and the Human Immunodeficiency Virus
(HIV), the virus which causes AIDS. Despite their seriousness as a medical event,
needle stick injuries have been neglected: most go unreported needle sticks have
been recognized as occupational hazards.3
Needle stick injuries are a common event in the healthcare environment. When
drawing blood, administering an intramuscular or intravenous drug, or performing
other procedures involving sharps, the needle can slip and injure the healthcare
worker. This sets the stage to transmit viruses from the source person to the recipient.

3
These injuries also commonly occur during needle recapping and as a result of failure
to place used needles in approved sharps containers. During surgery, a surgical needle
may inadvertently penetrate the glove and skin of the surgeon or assistant. Generally
needle stick injuries cause only minor bleeding or visible trauma, however, even in the
absence of bleeding the risk of viral infection remains. Scalpel injuries tend to be
larger than a needle stick. In turn, a needle stick injury may also pose a risk for a
patient if the injured health professional carries HBV, HCV or HIV. Needle stick
injuries are not limited to the medical community. Any environment where sharps are
encountered poses a risk. Needle stick injuries may occur not only with freshly
contaminated sharps, but also, after some time, with needles that carry dry blood.
While the infectiousness of HIV and HCV decrease within a couple of hours, HBV
remains stable during desiccation and infectious for more than a week.3
While needle stick injuries have the potential of transferring bacteria, protozoa,
viruses and prions, from a practical point the transmission of the hepatitis B and
hepatitis C viruses and the Human Immunodeficiency Virus (HIV) is important. The
specific risk of a single injury depends on a number of factors when the patients
harbor the virus of concern. Injuries with a hollow-bore needle, deep penetration,
visible blood on the needle, a needle that was located in a deep artery or vein, or with
blood from terminally ill patients are known to increase the risk for HIV infection.3
The incidence of NSI is considerably higher than current estimates, due to gross
under-reporting (often less than 50%)2,3. In USA 6,00,000 to 10,00,000 receive NSI
from conventional needles and sharps every year, while in UK it is 1,00,000
HCWs/year4. In India, authentic data on NSI are scarce. It is known that around 3-6
billion injections are given per year, of which 2/3rd injections are unsafe (62.9%) and
the use of glass syringe is constantly associated with higher degree of

4
unsafety5.Direct and indirect costs6-8. The average percutaneous transmission rates
for hepatitis B (HBV) and C (HCV) are 33.3 (6-33%) and 3.3 per cent (1-10%),
respectively, while the seroconversion risk for HIV is 0.31 per cent9. Although HBV
exposures pose the highest risk for infection, it has an effective vaccine and post
exposure prophylaxis (PEP) for HCWs which can dramatically reduce the risk. This is
not so for HCV and HIV. Therefore, prevention is the only recourse for these.
Preventing NSI is an essential part of any blood borne pathogen prevention
programme in the work place. Every healthcare facility should have an infection
control programme in place through a working hospital infection control committee.
The present study addresses the important issue of NSI and aims at determining the
occurrence of NSI among different categories of HCWs, the various factors
responsible, the circumstances under which these occur and explores the availability
and possibilities of measures to prevent these through improvement in knowledge,
attitude and practice. The study also aims at assessing the awareness levels among
various categories of HCWs, on issues like NSI policy, segregation of sharps at
source and the use and availability of safety devices to prevent NSI.4
Every day while caring for patients, nurses are at risk to exposure to blood
borne pathogens. These exposures, while preventable, are often accepted as being a
part of the job. In the United States, needle stick injuries have begun to decrease from
an estimated one million exposures per year in 1996 to 385,000per year in 2000. This
decline has resulted from the protections afforded by the Occupational Safety and
Health Administration’s (OSHA) Blood borne Pathogens Standard. Reasons for the
success in decreasing needle stick and sharps injuries may be attributed to the
elimination of needle recapping and the use of safer needle devices, sharps collection
boxes, gloves and personal protective gear, and universal precautions.7

5
To prevent needle stick injuries an effective exposure control program
should have a responsible person assigned to head the program and a committee that
includes representatives from frontline patient care providers to evaluate the hazards,
injury data and make recommendations for prevention. The committee should assure
appropriate follow up and post exposure prophylaxis as determined by the nature of
the injury and source patient. The most effective means of preventing the transmission
of blood borne pathogens is to prevent exposure to needle stick injuries. The primary
prevention of needle stick injuries is achieved through the elimination of unnecessary
injections and needles. The implementation of education, universal precautions,
elimination of needle recapping and use of sharp containers have reduced needle stick
injuries by 80%.8
While the vast majority of needle sticks injuries occur when the source-person
does not carry the HBV, HCV, and HIV and thus do not carry a risk of infection, these
events nevertheless cause stress and anxiety and signal a breakdown in protocol and
prevention. Preventive steps can be taken at several levels and include reduction or
elimination of use of sharps as much as possible, engineering controls (i.e. needles
with safety devices), administrative controls including training and provision of
adequate resources, and work practice controls; the latter may include using
instruments (not fingers) to grasp needles, load scalpels, and avoiding hand-to-hand
passing of sharp instruments. After a needle stick injury, certain procedures must be
followed to minimize the risk of infection for the recipient. The affected area should
be rinsed and washed thoroughly with soap. 5
Nurses are the largest work force of the health care industry.There are more
than 1 million licensed nurses currently working all over the world2. India produces
over 2,50,000 doctors annually in the modern system of medicine and a similar
6
number of nurses and para-professionals. Accidental needle-stick exposure poses the
greatest hazard to health care workers.6
Every year, hundreds of thousands of health care workers are exposed to
deadly viruses such as hepatitis and the Human Immunodeficiency Virus (HIV) as a
result of needle stick and sharps injuries.These preventable injuries expose workers to
over 20 different blood borne pathogens (CDC, 1998a) and result in an estimated
1,000 infections per year. The most common being hepatitis B, hepatitis C and HIV
(International Health Care Worker Safety Center, 1998). In November 2002, the
World Health Report published data demonstrating that 2.5 % of HIV cases among
health care workers and 40% of hepatitis B and C cases among health care workers
worldwide are the result of occupational exposure (WHO, 2002).7
In developing countries, where the prevalence of HIV-infected patients is
the highest in the world, the number of needle stick injuries is also highest. African
health care workers suffer on average two to four needle stick injuries per year and
over half of the hospitalized patients in South Africa are HIV positive (Prüss-Üstün et
al., 2003). In some regions of Africa and Asia close to half of all hepatitis B and C
infections among health care workers are attributable to contaminated sharps. In some
areas of the Eastern Mediterranean region over two-thirds of hepatitis B and C
infections in health care workers are attributable to contaminated sharps. Over two-
thirds of all hepatitis B in Central and South American are the result of occupational
exposure (Prüss-Üstün et al.).7
Every day while caring for patients, nurses are at risk to exposure to blood
borne pathogens. These exposures, while preventable, are often accepted as being a
part of the job. In the United States, needle stick injuries have begun to decrease from
an estimated one million exposures per year in 1996 to 385,000per year in 2000. This

7
decline has resulted from the protections afforded by the Occupational Safety and
Health Administration’s (OSHA) Blood borne Pathogens Standard. Reasons for the
success in decreasing needle stick and sharps injuries may be attributed to the
elimination of needle recapping and the use of safer needle devices, sharps collection
boxes, gloves and personal protective gear, and universal precautions.7
To prevent needle stick injuries an effective exposure control program
should have a responsible person assigned to head the program and a committee that
includes representatives from frontline patient care providers to evaluate the hazards,
injury data and make recommendations for prevention. The committee should assure
appropriate follow up and post exposure prophylaxis as determined by the nature of
the injury and source patient. The most effective means of preventing the transmission
of blood borne pathogens is to prevent exposure to needle stick injuries. The primary
prevention of needle stick injuries is achieved through the elimination of unnecessary
injections and needles. The implementation of education, universal precautions,
elimination of needle recapping and use of sharp containers have reduced needle stick
injuries by 80%.8
To prevent the needle stick accidents, there is comprehensive program which
includes; employee training, controlled work practice, implementing engineering
control, surveillance programs, safe recapping procedures, effective disposal systems.
As nurses are the largest work force of the health care industry and at high risk to
incur needle stick injuries, it is important to have adequate knowledge about hazards,
prevalence and controlling measures of needle stick injury.9

8
NEED FOR THE STUDY
“Reject your sense of injury and the injury itself disappears”
-Marcus Aurelious
Needle stick injuries are a common event in the health care environment.
Needle stick injuries, being accidental self-inoculation, are seldom reported or where
reportable are usually under reported. One study found that needle-stick injuries
represented one third of all work-related accidents and two-thirds of work-related
injuries to nursing staff.10
An investigation estimates the rates of injuries on a global level to affect about
3.5 million individuals. Needle-sticks are virtually undocumented in developing
countries, but probably equal or exceed those in the industrial world. In the absence of
statistics from India, statistics from United States provide some insight into the
occupational risk. American health workers suffer 800,000 to 1 million needle-sticks
annually, not including the vast number that goes unreported. There are more than
100,000 needle-stick injuries in UK hospitals each year.11
A Health Protection Agency (HPA) report regarding healthcare workers,
released in 2012, stated that:[2]
Between 2002 and 2011, 4,381 significant occupational exposures were reported
(increasing from 276 in 2002 to 541 in 2011).
Between 2008 and 2011, there were five HCV hospital-acquired transmissions
from patients to healthcare workers following percutaneous exposure injuries; three
reported from England and two in Scotland.
Even though percutaneous injuries remain the most commonly reported
occupational exposures in the healthcare setting, they have decreased over time as a
percentage of all exposures (from 79% in 2002 to 67% in 2011), whilst

9
mucocutaneous exposures have shown an increase (from 21% in 2002 to 29% in
2011).
The percentage of healthcare workers reporting percutaneous exposures that
involved an HCV-infected source patient declined from 38% in 2002 to 32% in
2011.
Between 2002 and 2011 most occupational exposures occurred in the nursing
profession. In 2011, medical and dental professions reported a similar number of
occupational exposures as nursing professionals. Exposures in the medical and
dental professions increased by 131% (from 100 to 231) between 2002 and 2011.
72 significant occupational exposures reported between 2002 and 2011 involved
ancillary staff. The majority of these exposures were due to non-compliance with
standard infection control precautions for the handling and safe disposal of clinical
waste.
The total number of HCV seroconversions in healthcare workers reported between
1997 and 2011 is 20; 17 cases reported in England and 3 in Scotland.
The last case of an HIV seroconversion in an occupationally exposed healthcare
worker was reported in 1999.
Prevention of sharps injuries; NHS Employers
Eye of the Needle 2012; Health Protection Agency (archived content)
The average estimated seroconversion risks from reports are:[1]
0.3% for percutaneous exposure to HIV-infected blood.
0.1% for mucocutaneous exposure to HIV-infected blood.
0.5-1.8% for percutaneous exposure to HCV-infected blood with detectable RNA
30% for percutaneous exposure of a non-immune individual to an HBeAg positive
source.

10
The Ontario Hospital Association/Ontario Medical Association (2012) estimate that
after an injury in workplace situations from a needle contaminated with hepatitis B
virus, there is a 6 to 30% chance that an exposed person will be infected. In a similar
situation with HIV, there is about a 0.3% chance of infection, and there is about a 2%
chance of infection for hepatitis C.
Note also that because the hepatitis B virus may survive on environmental
surfaces for more than a week, indirect exposure can occur via contaminated
inanimate objects. Injuries have transmitted many other diseases involving viruses,
bacteria, fungi, and other microorganisms to health care workers, laboratory
researchers, and veterinarian staff.12
Needle stick injuries are among the most important occupational injuries for the
nurses. Ebrahami H and Khosrari A (2007) conducted a study to determine the
incidence of needle stick injuries in population of nurses in Shabroud Imam Hossein
hospital Iran. The case incidence of needle stick injury was 63.6%. The causal devices
in 105 cases (92.1%) were hollow borne needles and the main cause of percutaneous
injuries with hollow borne needle were recapping (32.4%); and manipulating needles
in pats (18.1%). The majority (51.8%) of injuries occurred after use and before
disposal of the objects.13
Training the staff and developing good sharps management plans can ensure
safety from sharps. A standing order procedure should be formulated regarding sharp
injuries in all health institutions. Since needle stick injuries were highest in waste
handlers and nurses (33%), it underscores the need to provide compulsory, education
to health care workers, with respect to needle stick injuries. Health care workers
should made aware of hazards and preventive measures against needle stick injuries.14

11

12
2. OBJECTIVES
This chapter deals with the statement of the problem, objectives of the study,
operational definition, assumptions, hypothesis, and delimitation of the study and
conceptual frame work, which provides a frame of reference.
STATEMENT OF THE PROBLEM:-
“A Study To Assess The Knowledge Of Staff Nurses On Needle Stick Injury In
Selected Hospitals At Bangalore With A View To Develop Informational Booklet”.
OBJECTIVES OF THE STUDY
1. To assess the knowledge of staff nurses on needle stick injury.
2. To develop an informational booklet on needle stick injury.
3. To associate knowledge of staff nurses on needle stick injury with selected
demographic variables
HYPOTHESIS
H1 -There will be inadequate knowledge regarding needle stick injury staff nurses.
H2 - There will be significant association between knowledge and selected
demographical variables.
VARIABLE UNDER STUDY
DEPENDENT VARIABLE
Knowledge of staff nurses regarding effects of needle stick injury
EXTRANEOUS VARIABLE
Socio demographic variables: age, sex, religion, residence, Educational
qualification, experience, previous classes and Area of working.

13
OPERATIONAL DEFINITIONS
Assess: In this study it refers to the organized systematic and continuous
process of collecting information regarding effect of needle stick injury among
staff nurses
Staff nurses: It refers to the nurses registered from any state nursing council
and practicing in selected hospitals, Bangalore.
Informational booklet: Self learning information furnished in simple and
illustrated way prepared in English regarding the needle stick injury to
improve the knowledge of staff nurses.
Needle stick injury: A needle stick injury is a percutaneous piercing wound
typically set by a needle point, but possibly also by other sharp instruments or
objects.
ASSUMPTIONS
The present study assumes that Staff nurses will have minimal knowledge on needle
stick injuries
DELIMITATIONS
This study is limited to staff nurses working in selected hospitals, Bangalore,
Karnataka

18
REVIEW OF LITERATURE
19
3. REVIEW OF LITERATURE
A review of literature enables one to get an insight into the various
aspects of the problem under study. It covers promising methodological tools, throws
light on ways to improve the efficiency of data collection and suggests how to
increase effectiveness of data analysis and interpretation. Review of literature is
therefore an essential step in the development of the research project.
The sources to obtain information on the topic were books, journals, abstracts,
Medline, unpublished dissertations and internet. For the purpose of logical sequence,
the chapter is divided into sections.
The literature reviewed has been presented under the following categories:
Studies related to Needle Stick Injuries.
Studies related to knowledge on Needle Stick Injuries among Staff Nurses.
Studies related to effects of Needle Stick Injuries.
Studies related to Needle Stick Injuries.
Fredrich M, Nsuduga and Maritta S. Jalkkola (2005)Conducted a study on needle
stick injuries among nurses in sub-saharan Africa. The study revealed that 57% of the
nurses and midwifes had experienced at least on needle stick injury in the last year.
Only 18% had not experience any such injury in their entire career. The rate of needle
stick injury was 4.2 individually per year. The study concluded that strongest
predictor for needle stick injury was lack of training.15
Elmiyeh B, Whitaker S, James MJ, Chahal CAA, Galea A, Alshafi K (2004)
conducted a study regarding needle stick injuries in the National Health Service. A
confidential questionnaire was posted to 300 health professional in clinical work (175
nurses and 125 doctors) at the Lister hospital, Stevenage, U.K. 57% of the

20
respondents had sustained one or more needle stick injuries in their careers and
doctors were less likely to report injuries than nurses.16
Syed F. Shah, Abdulbari, Berner, Suad Al Kaabi, Abdul Latif Al Khal, Soji
Samson (2001)Conducted a study to characterize the epidemiology of needle stick
injuries of health care workers working at Hamad medical corporation Doha. A
survey was carried out among health care workers. 1022 workers responded to the
questionnaire on needle stick injuries with a response rate of 80.2%. Out of this, 214
studied subjects (20.9%) were victims of needle stick injuries. The highest incidence
of episodes of needle stick injuries occurred in the area of specialty such as 25
workers in medicine (13.1%), 20 in laboratory (9.3%) and 19 in emergency (5.9%),
followed by 17 in pediatric (7.9%).17
Rober t C (2001) conducted a study to find out factors responsible for needle stick
injuries to nurses. The study showed that 5-25% of the 346 nurses had needle stick
injury. 22 (63%) reported injury involving needle stick containing blood and nurses
who were working with poor work climate and lower staffing levels had more risk
factors for needle stick injuries.18
M. Varma, G. Mehta (2000) Conducted a study on needle sticks in medical
students in India. A questionnaire survey of 100 third year medical students in India
and they were asked about observation of safety precautions during invasive
procedures. Injuries occurred at some time in 65 students. The most common injury
was associated with drawing blood with a needle and syringe occurring at about 1.5
injuries per student per month.19
A retrospective study was conducted to assess the risk of needle stick injury
among nurses caring for patients with diabetes in 381 different hospitals throughout
the United States. The study was based on responses to an internet-based survey.

21
Result revealed that of 400 nurses who responded, 313 (78.3%) reported experiencing
at least one needle stick injury. The study found that nearly 80% of nurses experience
needle stick injuries caring for patients with diabetes.20
A survey was conducted on epidemiology of needle stick injuries among health
care workers working in Buraidah Central Hospital in Buraidah, Saudi Arabia. The
data was collected by a retrospective survey of all self-reported documents related to
needle stick injuries. Result revealed that of the total 73 injuries reported, nurses were
involved in 66% of instances, physicians in 19%, technicians in 10% and non-clinical
support staff in 5.5%.The study emphasized the importance of awareness, training and
education of health care workers for reporting and prevention of needle stick
injuries.21
A study was conducted on risk of needle stick injuries among healthcare workers
of L.T.M. Medical College and General Hospital, Sion over a period of one year. The
data collected was based on self-reported incidence of needle stick injuries and other
exposures to patient’s blood and body fluids. Result revealed that a total of 38 cases
were reported and no sero-conversion in any of the reported accidental injury cases.
This data emphasized that needle stick injuries present the single greatest risk to
medical personnel and the importance of increased awareness and training is in
universal safety precautions for prevention of nosocomial infections.22
A study was conducted on the prevalence of needle stick injuries among medical,
dental, nursing and midwifery students at Shiraz University of Medical Sciences, Iran.
A self- administered questionnaire was used to collect data. The results revealed that
out of 688 students responded, 71.1% of the students had needle stick injuries and
82% of the injuries were not reported. The study concluded that needle stick injuries
and non-reporting of needle stick injuries were highly prevalent in these students.23

22
Husoyam conducted a study on needle stick injury and reportingroutines in
Norwegian shows that health care workers transmission of blood-borne agents
through percutaneous exposure. Reporting of sharps injuries is essential for
instigation of adequate post-exposure prophylaxis and follow-up. We aimed at
providing an account of number of sharps injuries reported by type of health care
worker and the reporting systems used for injuries that have an inherent risk of
transmitting blood-borne agents. On average, 210 sharps injuries are reported
annually at Hauk eland University Hospital. In addition analyses of hepatitis and HIV
linked to 159 sharps injuries that had not been reported otherwise, were requested
annually. 51 % of sharps injuries were reported by nurses, 10 % by laboratory
workers, 6 % by doctors and 33 % by others.24
Rajis conducted a study on Guideline 'Needle stick injuries' risk assessment and
post-exposure management in practice in Bithoven. The objective of the national
guideline 'Needle stick injuries' is to make the assessment of needle stick injuries
more structured and uniform. The injury is classified as high risk or low risk
according to the volume of blood transmitted. For high-risk injuries measures to
prevent hepatitis B, hepatitis C and HIV infection have to be considered, whereas for
low-risk injuries only measures to prevent hepatitis B. The need for post-exposure
prophylaxis is determined by the victim's immunity to hepatitis B and the presence of
hepatitis B virus, hepatitis C virus or HIV in the source person. Post-exposure
prophylaxis against hepatitis B consists primarily of hepatitis B vaccination; hepatitis
B immunoglobulin is added in the case of a high-risk injury with a hepatitis B positive
source or a source belonging to a risk group for hepatitis B. In high-risk injuries the
victim is tested for hepatitis C and HIV transmission (except in case of a seronegative

23
source). Antiretroviral post exposure prophylaxis is advised for high-risk injuries with
a HIV seropositive source or a source belonging .25
Von Over Beck J Wess conducted a study on ” Needle stick accidents procedures
following potentially infectious exposure in medical personnel in Bern
(Germany)shows that exposure of blood carries with a definite risk for the health care
worker of infection by various blood borne pathogens, especially the hepatitis B,
hepatitis C, and human immunodeficiency virus. The risk of transmission from
exposure to HIV is lower than that associated with exposure to HBV and HCV.
Should HIV infection occur, however, the outcome is likely to be fatal. Although
general infection control precautions, safer use of needles, gloves, and other
procedures may substantially reduce the incidence of occupational exposures; they
cannot eliminate the risk completely. The post-exposure management is discussed.
Neither the efficacy nor the safety of AZT (zidovudine) for use as a chemo
prophylactic agent following occupational exposures to HIV has been established.
Nevertheless in selected cases it can be proposed to health care workers.26
A study conducted at selected hospitals in New Zealand. The aim of the study was
to determine frequency of needle stick injury. The response rate of health care
workers was 82%. An incidence rate of 22 needle stick injuries in 100 health care
workers per month period was found. For practice nurses it was 17 in 100 per months
period. Precautionary measures were not being followed by most individuals. Needle
stick injury is a substantial problem in practice nurse to a serious risk of infection
from blood borne transmissible agents.27
A study was carried out in three hospitals of Karachi. Total of 222 health care
providers in which 52 were nurses participated in the study. Approximately 60% of
health care providers had experienced needle stick injury at least once during their

24
service. The most frequency source of injury occurred while recapping the syringe.
None of the health care provider had adequate knowledge regarding immediate
measures following in needle stick injury.28
Studies related to knowledge on Needle Stick Injuries among Staff Nurses.
A study was conducted to assess the knowledge, attitude and practices regarding
needle stick injuries among 70 nurses and paramedical staff from different
departments of 100-bedded armed force’s hospital, Sharourah. Data collection was
carried out using a standardized questionnaire. The results revealed that 21% and 30%
of the healthcare workers, respectively, were unaware of the fact that AIDS and
Hepatitis C can be transmitted by needle stick injury. A total of 74% had a history of
needle stick injury and only 4% reported the injuries. The survey concluded that
knowledge of healthcare workers about the risks associated with needle stick injuries
and use of preventive measures is inadequate.29
A study was conducted to assess the knowledge, attitude and practices on needle
stick injuries among 70 nurses and paramedical staffs from different departments of
Kathmandu Medical College and Teaching Hospital. A 15-item questionnaire was
administered for analysis. Result revealed that 4% and 61% of healthcare workers,
respectively, were unaware of the fact that hepatitis B and hepatitis C can be
transmitted by needle stick injuries. 74% had a history of needle stick injuries and
only 21% reported the injuries. Only 23% were in the habit of using gloves for
phlebotomy procedures all the time.79% were of the impression that needle should be
recapped after use. Only 66% were aware of universal precaution guidelines. The
study concluded that knowledge of health care workers about the risk associated with
needle stick injuries and use of preventive measures is inadequate.30
25
A study was conducted to assess the knowledge, attitude and practices of
healthcare workers regarding needle stick injuries among 29 doctors and 51 registered
nurses at Aga Khan University hospital. A structured pretested questionnaire was
administered. Results revealed that about 45% reported having a needle stick injury in
the past. The most common reason identified was stress or being overburdened
followed by careless attitude. Two-third of the participants was familiar with the
prevention protocols. The study concluded that despite knowing the risk frequency of
needle stick injury, higher and mandatory reporting, proper follow-up and constant
reinforcement are recommended to reduce the rate of nosocomial transmission to
healthcare workers.31
A cross sectional study conducted in southern England to know the knowledge
and attitude of health care workers including staff nurses regarding glove techniques
and precautions followed in needle stick injury at a teaching hospital. The result
showed knowledge could be improved in relation to standard precautions to be taken
to avoid needle stick injury. Respondents had negative attitude towards use of gloves.
Interventions could be aimed at staff education and training.32
A study conducted at a hospital in Britain to know the attitude of health care
workers including nurses. The study revealed some general and psychological factors
contributing to low reporting attitude of personals regarding needle stick injury.
Continued training of staff, a sympathetic attitude and clarification of some general
issues might improve reporting of needle stick injury.33
Study conducted to know knowledge and nurses attitude regarding
gloving practice and risk factors of needle stick injury at a metropolitan hospital,
Taiwan. 210 nurses included in study, in which all nurses use, gloves because fear of
contracting HIV. The knowledge of nurses was deficit regarding risk factors of needle

26
stick injury. Continuous education program may alleviate these nurses attitude and
concerns regarding risk factors of needle stick injury.34
Knowledge concerning needle stick injury Most of the students had knowledge
about the diseases transmitted by contaminated sharp objects. In a study by Norsayani
MY et al, most of the student acquired knowledge of blood borne disease mainly from
the lectures 98.3%, books 90.8% through informally 81.6%. Almost all of the
participants (n = 250, 93%) identified blood as the most infectious body fluid that can
transmit infections through occupational exposure. 35 In the study by Deisenhammer
S et al, general, students’ knowledge about the transmission risks of HIV, hepatitis B
and C through a needle stick injury with a contaminated needle
Most of the students had knowledge about the diseases transmitted by
contaminated sharp objects. In a study by Norsayani MY et al, most of the student
acquired knowledge of blood borne disease mainly from the lectures 98.3%, books
90.8% through informally 81.6%. Almost all of the participants (n = 250, 93%)
identified blood as the most infectious body fluid that can transmit infections through
occupational exposure. 35 In the study by Deisenhammer S et al, general, students’
knowledge about the transmission risks of HIV, hepatitis B and C through a needle
stick injury with a contaminated needle was poor. A study by Saleem T et al, more
than 85% students from each class were aware of the possibility of acquisition of
Hepatitis B, Hepatitis C and HIV from needle stick injuries. Only 16.4% 3rd year
students, 29.5% 4th year students and 36.2% final year students knew the full details
of needle stick injury prevention protocols. Curriculum was cited as an important
source of information regarding needle stick injuries. 19The percentage of students
who acquired knowledge of universal precaution was 70.3%10 and in a study by
Kulkarni et al ,the knowledge of the study participants was high regarding standard

27
precautions, as 70.5% (n = 189) of the participants were able to identify all of the
components35
.
A similar study on health science students in northern china reported that the
students displayed a general lack of knowledge of occupational exposure standards.22
the transmission risk of HIV was rated correctly by only 9% of a first year as compare
to 45% of the fifth year students. Similar results were found for hepatitis B and C.
Overall, the students tended to overestimate the transmission risks. Author
International Journal of Collaborative Research on Internal Medicine & Public
Health.35
Studies related to effects of Needle Stick Injuries.
A quasi- experimental study was conducted to assess the impact of structured
training on prevention of occupational exposure to blood-borne pathogens on
knowledge, behaviour and incidence of medical sharp injuries among 106 student
nurses in Changsha, People’s Republic of China. The 106 students taken for the study
were divided into two classes, one class served as experimental group while the other
served as a control group. Students in the experimental group participated in
structured training interventions. Results revealed that the group that received the
structured training scored significantly higher than the standard education group on
both knowledge and behavior.36
A study was conducted to assess the effectiveness of a training program on
reducing needle stick injuries/sharp object injuries among soon graduate vocational
nursing school students in Southern Taiwan. The study method consisted of a lecture
to the students after the internship training and a self-study brochure for them to
study. This study used the pre-test questionnaires completed by the students and the
post-test questionnaires completed by 107 graduates after work experience as licensed

28
nurses. The results revealed that, the incidence of needle stick injuries / sharp injuries
decreased significantly from 50.5% pre-test to 25.2% post-test, and the report rate
increased from 37.0% to 55.6%, respectively. In conclusion, this intervention
significantly reduced the incidence of needle stick injuries/sharp injuries and
increased the report rate of such events.37
A study was conducted to assess the knowledge and existing practices of staff
nurses regarding needle stick injuries and to evaluate the guidelines developed for the
prevention and management of needle stick injuries in a selected government hospital
of Delhi. The study revealed that 70% of the staff nurses had sustained needle stick
injuries. There was lack of awareness among staff nurses regarding prevention and
management of needle stick injuries. Among the nurses who sustained needle stick
injuries, the majority (71%) did not report it. The developed guidelines regarding,
prevention and management of needle stick injuries was found to be effective in
enhancing the knowledge and improving the practice of staff nurses. The study
concluded that it is useful to the British nurses to be able to compare their experience
of needle stick injuries with that of nurses in Delhi. 38
A study was conducted to assess the impact of introduction of sharp containers
and education programmes on the pattern of needle stick injuries in a tertiary care
centre in India. Introduction of large sharp containers, accompanied by an intensive
education programme was used as the study method. Details of documented injuries
were analysed using the epi-info software for a selected period of time. Result
revealed that a total of 347 injuries occurred mainly due to improper disposal of
needles, recapping and carelessness during use. After the education programme the
percentage of injuries attributed to disposal fell from 69.2% to 38.5%.A further

29
decrease was noted after the additional introduction of small sharp containers. The
study concluded that relatively simple intervention decreased the number of injuries.39

30

31
FIG:-2 SCHEMATIC PRESENTATION OF RESEARCH STUDY/DESIGN.
Population = staff nurses
Sample= 100 staff nurses
Target population = staff nurses
Accessible population = Staff nurses working in selected hospital, Bangalore
Sampling technique = Random sampling technique
Tool = 1. Structured questionnaire to assess the knowledge
Data analysis
Findings
Development of information booklet
Distribution of
sample
characteristics in
frequency and
percentage of the
staff nurses
Chi-square test to
associate the socio
demographic
variable with
knowledge

32
4. RESEARCH METHODOLOGY
Research methodology designed to develop or refine procedure for obtaining
organizing and analyzing data. Research methods are the steps, procedure and the
strategies for gathering and analyzing the data in a research investigation.
This chapter deals with the methodological approach adopted to evaluate the
knowledge of staff nurses on needle stick injury
Research methodology organized all the components of the study deals with
the type of research approach used, the setting of the study, the population, sampling
technique, sample selection, the inclusion and exclusion criteria, the development of
the tool, collection of data, pilot study, procedure of data collection and plan for data
analysis.
RESEARCH APPROACH:
Research approach is the basic procedure for the research enquiry. The research
approach helps the researchers to determine what data to collect and how to analyze
it. It also suggests possible conclusions to be drawn from the data. A descriptive
survey approach was considered as the most appropriate and adopted for assess the
knowledge on needle stick injury among staff nurses working in Srilakshmi Multi
Specialty Hospital and Ashraya hospital, Bangalore.
RESEARCH DESIGN:
The research design refers to the researcher’s overall plan for obtaining
answers to the research question or for testing the hypothesis. Research design helps
the researcher in selection of subjects, identification of variables, their manipulation
and control. The research design adopted for this study was Non experimental
descriptive design.

33
SETTING OF THE STUDY
The study was conducted in selected hospital (Srilakshmi Multi Specialty
Hospital and Ashraya hospital, Bangalore, Karnataka). The settings were chosen
based in terms of availability of samples and feasibility for conducting study
VARIABLES UNDER STUDY
Variable is “an attribute of a person or object that to varies, that is taken on
different values”
Dependent Variable
Knowledge of staff nurses regarding effects of needle stick injury
Extraneous Variable
Age, sex, religion, residence, Educational qualification, experience, previous
classes and Area of working.
POPULATION
The population refers to the aggregate or totality of all the objects, subject or
members that conform to a set of specification
The target population of this study is the staff nurses in Bangalore, Karnataka
The accessible population of this study is the staff nurses in selected hospitals,
Bangalore, Karnataka.
SAMPLE
Sample consists of the subset of the population selected to participate in research
study. Sampling refers to the process of selecting the portion of population, which
represents the entire population.
Sample for the study will be staff nurses who are fulfilling the inclusion criteria
SAMPLING TECHNIQUE:
Random sampling technique will be adopted to select the sample
34
SAMPLING CRITERIA:
INCLUSION CRITERIA FOR SAMPLING
The study includes who staff nurses who are:
Registered staff nurses
willing to participate in the study
present on the day of sampling
EXCLUSION CRITERIA FOR SAMPLING
The study excludes staff nurses who are:
not willing to participate in the study
those who are absent on that day
DATA COLLECTION TOOL
Selection and Development of the Tool
The data collection technique is through self-administered structured
questionnaire. It was prepared to assess knowledge of staff nurses regarding needle
stick injury. Based on the research problem and objective of the study the following
steps were under taken to select and develop the data collection tool.
DESCRIPTION OF THE TOOL
Data collection is the gathering of information needed to research problem.
The tool was constructed after an extensive review of literature, discussion with the
experts and investigator’s personal experience.
The tool consists of 2 sections:
Sections -1
Socio demographic variables consists of 08 items such age, sex, religion, residence,
Educational qualification, experience, previous classes and Area of working.

35
Sections -2
The structured Questionnaire on knowledge related to needle stick injury and
it consists of 30 items
Development of Criteria Rating Scale
Criteria rating scale for validation of tool was developed,
Part-I – comprised of demographical data
Part-II – self-administered questionnaire on needle stick injury which had
very relevant, relevant, needs modification, not relevant and remarks of experts.
CONTENT VALIDATION OF THE TOOL:-
Content validity refers to the degree to which an instrument measures what it
is intended to measure.
The prepared instrument along with the objectives, blue print and criteria
check list was submitted to 7 experts comprising of experts in the field of Medical
Surgical Nursing (4), Statistician (1) and Medical personals (2) for establishing the
content validity. The tool was modified as per suggestions of the experts and the final
tool was constructed.
Pre testing the Tool:
Pretesting of self-administered questionnaire was done to check the clarity of the
items, their feasibility and practicability. Pretest was done in Srilakshmi Multi
Specialty Hospital, Bangalore. It was administered to 10 staff nurses. The sample
chosen were similar in characteristics to those of the population under study.
It was found it took 40 minutes to complete the tool and it was found that the items
were simple to comprehend.

36
The first of the tool consisted of 35 items on knowledge. Based on the suggestions
given by experts, modifications, and rearrangements of few items were done, and few
items were not found appropriate by item analysis, so they were deleted.
Thus the second draft of the prepared tool consisted of 30 items on knowledge
RELIABILITY OF THE TOOL
Reliability of the research instrument was defined as the extent to which the
instrument yields the same results in repeated measures. It was then concerned with
the consistency, accuracy, precision, stability, equivalence and homogeneity.
The tool after validation was subjected to test for its reliability. The self-
instructed questionnaire was tested for reliability by administering it to 10 staff nurses
of Srilakshmi Multi Specialty Hospital, Bangalore. The reliability was established by
split half method. The internal consistency was assessed by using split half technique
with raw score method and deviation method and Spearman’s Brown Prophecy
formula.
Spearman’s Brown Prophecy formula for reliability
r1
= 2r / 1+r
r = the correlation, coefficient, computed on the split haves
r1
= the estimated reliability of the entire test.
For computing the coefficient of correlation, the formulae used were:
Raw score method:
∑
Deviation method: ∑
√∑

37
The reliability obtained for tool was r = 0.88 which was considered to reliable
and adequate.
PREPARING INFORMATION BOOKLET
Preparing of first draft of information booklet was done according to review of
literature. Modification was done after the expert validation. The final draft of
information booklet was prepared containing adequate information on needle stick
injury.
PILOT STUDY
“Pilot study is a small scale version or a trial run, done in preparation for a major
study”.
The pilot study is a small preliminary investigation of the same general
character as in major study.
It is conducted in selected hospital (Srilakshmi Multi Specialty Hospital)
Bangalore and the pilot study data was collected from 4-04-2018 to 10-04-2018. 10
staff nurses are selected by Random sampling technique after obtaining permission
from the concerned authority. Verbal consent was obtained from staff nurses and
assured regarding confidentiality of the information.
Knowledge about needle stick injury was assessed by using self-administered
questionnaire on selected aspects. The time taken for the completion of the tool was in
between 30-40 min.
The pilot study result shows that the study is necessary on the selected sample
in the selected setting
Problems faced during pilot study:
- It consumed more time to collect the data from the staff nurses in ICU.

38
- Some questions that had been framed were found to be slightly difficult to be
understand by the participants and they were modified so that they were easy for
them to understand.
Procedure for data collection:
“Data collection is the gathering of information needed to address a research
problem.”
The main study data collection was done from 20st of May 2018 to 21
th of
June 2018. The total sample of main study consisted of 100 staff nurses. Data was
collected from the sample by administering structured questionnaire after obtaining
consent from the participants. Each session of data collection last for about 30-40
minutes and it took 25-30 days to complete the study.
Plan for data analysis:
The data collected from the participants was planned to be analyzed on the
basis of the objectives of the study using descriptive and inferential statistics.
Organize the data in master data sheet.
Demographic variables are to be analyzed in terms of frequency and percentage.
Knowledge score on needle stick injury is to be presented in the form of mean,
median and standard deviation.
X2 (Chi-Square) is used to determine the association between the knowledge and
selected demographic variables among staff nurses regarding on needle stick
injury.

39

40
5. RESULTS
Analysis is a process of organizing and synthesizing the data in such a
way that the research questions may be answered and hypothesis tested. Analysis of
data is processed by which quantitative information is reduced, summarized,
organized, interpreted and communicated in a meaningful way
This chapter deals with the analysis and interpretation of the data collected
from 100 staff nurses of Srilakshmi Multi Specialty Hospital and Ashraya hospital to
find out the knowledge. The result was computed descriptive and inferential statistics
based on the objective of the study. The results were computed using descriptive and
inferential statistics based on following objectives of the study
Objectives of the Study:
1. To assess the knowledge of staff nurses on needle stick injury.
2. To develop an informational booklet on needle stick injury.
3. To associate knowledge of staff nurses on needle stick injury with selected
demographic variables
Research Hypothesis:
H1 -There will be inadequate knowledge regarding needle stick injury staff nurses.
H2 - There will be significant association between knowledge and selected
demographical variables.
ORGANIZATION AND PRESENTATION OF DATA
The data collected was organized and presented under the following sections
a) Section –A :Description of sample characteristics
b) Section –B: Findings related to knowledge scores of participants.
c) Section –C: Association between knowledge scores and selected demographic
variables.

41
Section A
Table- 1 – Distribution of Staff Nurses according to demographic variables by
frequency and percentage N=100
Socio demographic variables Frequency Percentage
1.Age in years
a. 20-30yrs 71 71%
b. 31-40 yrs 17 17%
c. 41 yrs and above 12 12%
2.Sex
a. Male 49 49%
b. Female 51 51%
3. Educational qualification
a. B.Sc.N 71 71%
b. GNM 19 19%
c. M.Sc. N 10 10%
4. Religion:
a) Christian 71 71%
b) Hindu 19 19%
c) Muslim 10 10%
5. Residence belongs to
a) Urban 39 39%
b) Rural 61 61%
6. Experience
a) < 1 years 64 64%
b) 1-3 years 18 18%
c) >3 years 18 18%
42
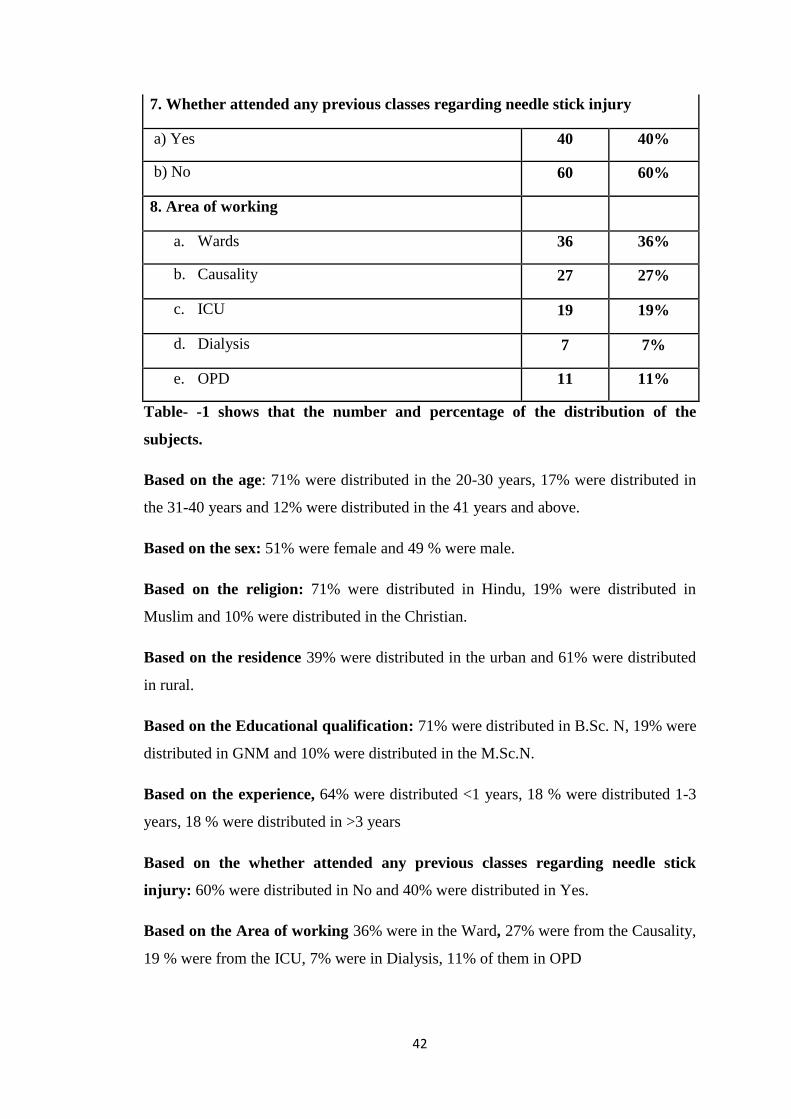
7. Whether attended any previous classes regarding needle stick injury
a) Yes 40 40%
b) No 60 60%
8. Area of working
a. Wards 36 36%
b. Causality 27 27%
c. ICU 19 19%
d. Dialysis 7 7%
e. OPD 11 11%
Table- -1 shows that the number and percentage of the distribution of the
subjects.
Based on the age: 71% were distributed in the 20-30 years, 17% were distributed in
the 31-40 years and 12% were distributed in the 41 years and above.
Based on the sex: 51% were female and 49 % were male.
Based on the religion: 71% were distributed in Hindu, 19% were distributed in
Muslim and 10% were distributed in the Christian.
Based on the residence 39% were distributed in the urban and 61% were distributed
in rural.
Based on the Educational qualification: 71% were distributed in B.Sc. N, 19% were
distributed in GNM and 10% were distributed in the M.Sc.N.
Based on the experience, 64% were distributed <1 years, 18 % were distributed 1-3
years, 18 % were distributed in >3 years
Based on the whether attended any previous classes regarding needle stick
injury: 60% were distributed in No and 40% were distributed in Yes.
Based on the Area of working 36% were in the Ward, 27% were from the Causality,
19 % were from the ICU, 7% were in Dialysis, 11% of them in OPD

43
Figure (3) Bar Diagram showing the distribution of the age among Staff
Nurses
Based on the age: 71% were distributed in the 20-30 years, 17% were distributed in
the 31-40 years and 12% were distributed in the 41 years and above.
Figure (4) Pie Diagram showing the distribution of sex among the Staff Nurses.
Based on the sex, 51% were female and 49 % were male.
0
10
20
30
40
50
60
70
80
20-30yrs 31-40 yrs 41 yrs and above
Male 49%
Female 51%
DISTRIBUTION OF SEX

44
Figure (5) Bar Diagram showing the distribution of the religion
Based on the religion: 71% were distributed in Christian, 19% were distributed in
Hindu and 10% were distributed in the Muslim.
Figure (6) Bar Diagram showing the distribution of residence
Based on the residence 39% were distributed in the urban and 61% were distributed
in rural.
0 10 20 30 40 50 60 70 80
Christian
Hindu
Muslim
Urban Rural
39
61
DISTRIBUTION OF RESIDENCE

45
Figure (7) Doughnut Diagram showing the Educational Qualification
Based on the Educational qualification: 71% were distributed in B.Sc. N, 19% were
distributed in GNM and 10% were distributed in the M.Sc.N.
Figure (8) Pie Diagram showing the distribution of experience among Staff
Nurses.
Based on the experience, 64% were distributed < 1 years, 18 % were distributed 1-3
years, 18 % were distributed in >3 years
Qualification
B.Sc.N
GNM
M.Sc. N
Experience
<1 years
1-3 years
>3 years

46
Figure (9) Bar diagram showing the distribution previous classes regarding
needle stick injury among Staff Nurses.
Based on the previous classes regarding needle stick injury: 60% were distributed
in No and 40% were distributed in Yes.
Figure (10) Pie Diagram showing the distribution of the Area of working among
Staff Nurses.
Based on the Area of working 36% were in the Ward, 27 % were from the
Causality, 19 % were from the ICU, 7% were in Dialysis, 11% of them in OPD
0
10
20
30
40
50
60
Yes No
36
27
19
7
11
Area of working
Wards
Causality
ICU
Dialysis
OPD

47
SECTION –B
Table- 2: Frequency and percentage distribution of knowledge of Staff Nurses
KNOWLEDGE LEVEL Score
N %
INADEQUATE( < 50 % ) 64 64%
MODERATE ( 51 - 75 % ) 36 36%
ADEQUATE ( >75 % ) 00 00%
TOTAL 100 100%
Table 2: Depicts Percentage and frequency distribution of knowledge of Staff Nurses
With regard to knowledge scores of Staff Nurses on importance of needle stick
injury, majority of the Staff Nurses 64% had inadequate knowledge, 36% of them had
moderate knowledge and none of them had adequate knowledge.
Figure 11: Percentage distribution of knowledge of Staff Nurses
0
10
20
30
40
50
60
70
INADEQUATE( <50 % )
MODERATE ( 51 -75 % )
ADEQUATE ( >75% )

48
Table-3
Distribution of overall knowledge scores of staff nurses on Needle
stick injury
The above table represents that overall mean knowledge score of staff nurses
regarding Needle stick injury is 11.13.
Sl. no.
No. of items
Max Score
Mean
SD
Mean%
1 30 30 11.13 3.12
49.76

49
SECTION 3
Table- -4 Chi square test associate the selected Socio demographic
Variables with the level of knowledge on Needle stick injury
N=100
Socio demographic variables Inadequate
knowledge
Moderate
Knowledge
Chi-square
value
1.Age in years
χ2 = 6.01
P> 0.05
NS
a. 20-30yrs 51 19
b. 31-40 yrs 10 7
c. 41 yrs and above 13 0
2.Sex χ2 =0.114
P>0.05
NS
a. Male 37 12
b. Female 37 14
3. Educational qualification
χ2 = 0.35
p <0.05
S*
a. B.Sc. N 58 13
b. GNM 12 7
c. M.Sc. N 4 6
4. Religion:
χ2 =1.4
p> 0.05
NS
a) Christian 45 19
b) Hindu 14 4
c) Muslim 15 3
5. Residence belongs to χ2 =0.756
P>0.05
NS
a) Urban 27 12
b) Rural 47 14
6. Experience
χ2 = 0.35
p <0.05
S*
a) <1 years 58 13
b) 1-3 years 12 7
c) >3 years 4 6

50
7. Whether attended any previous classes regarding needle
stick injury χ
2 =0.554
P<0.05
S*
a) Yes 28 12
b) No 46 14
8. Area of working
χ2 =6.22
P>0.05
NS
a) Wards 28 8
b) Causality 19 8
c) ICU 17 2
d) Dialysis 4 3
e) OPD 6 5
S* -Significance P < 0.05 NS – No Significance P > 0.05
Table- 4 shows that the association between knowledge and socio demographic
variable
Based on the third objectives, the chi square test used to associate the level of
knowledge and selected socio demographic variables such as age, sex,
residence, educational qualification, previous classes, experience, religion,
area of working.
The chi-square value shows that there is no significance association between
age, sex, residence area, religion, area of work and level of knowledge with
socio demographic variable.(P > 0.05)
The experience, qualification and previous classes show the significant
association the level of knowledge.

51
DISCUSSION

52
6. DISCUSSION
Needle stick injuries are a hazard for people who work with hypodermic
syringes and other needle equipment. These injuries can occur at any time when
people use, disassemble, or dispose of needles. When not disposed of properly,
needles can become concealed in linen or garbage and injure other workers who
encounter them unexpectedly. As a nurse, it is essential to have adequate knowledge
regarding the needle stick injury, as it can spread so many diseases.
The present study is to assess knowledge regarding needle stick injury among staff
nurses of selected hospital (Srilakshmi Multi Specialty Hospital and Ashraya hospital)
Bangalore.
The findings were discussed under following sections.
1. To assess the knowledge regarding needle stick injury among nurses.
2. To determine the association between knowledge of staff nurses with the
selected demographic variables.
3. To develop an informational booklet on needle stick injury.
1. Knowledge scores of participants on needle stick injury
The mean knowledge score obtained by staff nurses was 11.13; mean
percentage was 49.76, and standard deviation 3.12
The knowledge scores of Staff Nurses on importance of needle stick injury,
majority of the Staff Nurses 64% had inadequate knowledge, 36% of them had
moderate knowledge and none of them had adequate knowledge.
This study is supported by the study, carried out in three hospitals of Karachi.
Total of 222 health care providers in which 52 were nurses participated in the study.

53
Approximately 60% of health care providers had experienced needle stick injury at
least once during their service. The most frequency source of injury occurred while
recapping the syringe. None of the health care provider had adequate knowledge
regarding immediate measures following in needle stick injury.
2. To determine the association between knowledge of staff nurses with the
selected demographic variables.
Distribution of demographic characteristics of staff nurses.
Based on the age: 71% were distributed in the 20-30 years, 17% were distributed in
the 31-40 years and 12% were distributed in the 41 years and above.
Based on the sex: 51% were female and 49 % were male.
Based on the religion: 71% were distributed in Hindu, 19% were distributed in
Muslim and 10% were distributed in the Christian.
Based on the residence 39% were distributed in the urban and 61% were distributed
in rural.
Based on the Educational qualification: 71 % were distributed in B.Sc. N, 19%
were distributed in GNM and 10% were distributed in the M.Sc.N.
Based on the experience, 64% were distributed <1 years, 18 % were distributed 1-3
years, 18 % were distributed in >3 years
Based on the whether attended any previous classes regarding needle stick
injury: 60% were distributed in No and 40% were distributed in Yes.
Based on the Area of working 36% were in the Ward, 27% were from the Causality,
19 % were from the ICU, 7% were in Dialysis, 11% of them in OPD
54
Association of knowledge score with selected demographic variable.
The chi-square value shows that there is no significance association between
age, sex, residence area, and religion, area of work and level of knowledge with socio
demographic variable. (P > 0.05)
There is a significant association between the knowledge and demographic
variables like experience (χ2 = 0.35), qualification (χ2 = 0.35) and previous classes
(χ2=0.554).
This study is supported by the quasi- experimental study, conducted to assess
the impact of structured training on prevention of occupational exposure to blood-
borne pathogens on knowledge, behaviour and incidence of medical sharp injuries
among 106 student nurses in Changsha, People’s Republic of China. The 106 students
taken for the study were divided into two classes, one class served as experimental
group while the other served as a control group. Students in the experimental group
participated in structured training interventions. Results revealed that the group that
received the structured training scored significantly higher than the standard education
group on both knowledge and behaviour.
This study is supported by the survey, conducted on epidemiology of needle stick
injuries among health care workers working in Buraidah Central Hospital in Buraidah,
Saudi Arabia. The data was collected by a retrospective survey of all self-reported
documents related to needle stick injuries. Result revealed that of the total 73 injuries
reported, nurses were involved in 66% of instances, physicians in 19%, technicians in
10% and non-clinical support staff in 5.5%.The study emphasized the importance of
awareness, training and education of health care workers for reporting and prevention
of needle stick injuries.

55
This study is supported by the study, conducted on risk of needle stick injuries
among healthcare workers of L.T.M. Medical College and General Hospital, Sion
over a period of one year. The data collected was based on self-reported incidence of
needle stick injuries and other exposures to patient’s blood and body fluids. Result
revealed that a total of 38 cases were reported and no sero-conversion in any of the
reported accidental injury cases. This data emphasized that needle stick injuries
present the single greatest risk to medical personnel and the importance of increased
awareness and training is in universal safety precautions for prevention of nosocomial
infections.

56

57
CONCLUSION
Many studies state the importance of proper knowledge of staff nurses
regarding needle stick injury. The study helps the nurses to aware about the effects
and precautions for needle stick injury
The findings shows that only 36% of staff nurses have moderate knowledge
regarding needle stick injury and the aim is to increase the knowledge by providing
informational booklet
Nursing implication:
The finding of this study has brought out certain facts that have far-reaching
implications for nursing, particularly in the areas of practice, education,
administration and research.
Nursing Practice:
Safe practices during procedures are vital for the patient as well as health
workers. The findings of the study can be utilized by practicing nurse in alleviating
the needle stick and sharp injuries.
Nursing education
Nurses with higher education and up to date knowledge can provide cost
effective and quality patient care. Nurse educators need to include various aspects of
needle stick injury and precautions in the curriculum of basic nursing education as a
part of practical and should encourage their students to practice the same in the
clinical setting.
Nursing Administration:
Today there is an increasing demand for quality care. Nurse administrators are
in a key position to prepare policies and its execution of quality nursing care based on
research findings. In- service education should be organized periodically to upgrade

58
the knowledge and skills of health care professionals in regarding needle stick
injuries.
Nursing Research:
Nursing researchers should be aware of the new trends and existing health care
system. Emphasis should be laid on research in the areas of quality care. The findings
of the research need to be disseminated through publications so that the utilization of
such research findings could be encouraged.
Limitations
The study is limited to staff nurses working in selected hospitals (Srilakshmi
Multi Specialty Hospital and Ashraya hospital) at Bangalore
Assessment of knowledge based on responses of the participants to items
included in the questionnaire.
Recommendations:
On the basis of the findings of the study the following recommendations
have been made:
The study can be replicated in different hospital
Experimental study can be conducted with structured learning programme on
knowledge and practice.
Follow up study can be conducted to evaluate effectiveness of VAT.
A comparative study can be conducted between government and private
hospitals.
Summary
The investigator felt satisfaction and fulfillment for having undertaken the
present study. The result of the present study shows that there is a great need for the
health personnel to implement appropriate practice in preventing needle stick injury.

59

60
8. SUMMARY
This chapter presents the summary of the study, its discussion, conclusion, its
nursing implications and recommendations.
The main objective of the study was to assess the knowledge among staff nurses
regarding needle stick injury at selected hospitals, Bangalore.
OBJECTIVES OF THE STUDY:
1. To assess the knowledge of staff nurses on needle stick injury.
2. To develop an informational booklet on needle stick injury.
3. To associate knowledge of staff nurses on needle stick injury with selected
demographic variables
HYPOTHESIS:
H1 - There will be inadequate knowledge regarding needle stick injury staff nurses.
H2 - There will be significant association between knowledge and selected
demographical variables.
CONCEPTUAL FRAMEWORK:
The conceptual frame work for this study was based on Imogene KING’s
goal attainment theory to assessing the knowledge regarding the needle stick injury.
The review of related research and non-research literature helped the investigator to
develop the conceptual frame work, structured interview schedule and to plan for data
analysis.
The study was conducted at Srilakshmi Multi Specialty Hospital and Ashraya
hospital, Bangalore from 20st of May 2018 to 21
th of June 2018, adopted descriptive

61
survey approach with random sampling technique. Sample of the study consisted of
100 staff nurses.
The tool used for the collection of data was structured interview schedule. It
consisted of following sections:
Sections -1
Socio demographic variables consists of 08 items such age, sex, religion, residence,
Educational qualification, experience, previous classes and Area of working.
Sections -2
The structured Questionnaire on knowledge related to needle stick injury and
it consists of 30 items
The steps involved in the development of instruments were preparation of
their print, construction of items, content validity, pre-testing, reliability, conducting
pilot study and preparation of the final copy of the tool.
After obtaining the formal permission from Srilakshmi Multi Specialty
Hospital and Ashraya hospital, Bangalore and taking consent from the subjects, the
validated tool was used to collect data from staff nurses for 50-55 minutes.
Then the collected data were analyzed using descriptive and inferential
statistics and interpreted in terms of objective and hypothesis of the study. The level
of significance was set at 0.01 & 0.05 level of significance.
On the basis of the obtained knowledge score score an information booklet
was prepared on needle stick injury and was validated by subject experts.

62
MAJOR FINDINGS OF THE STUDY:
Section I
Distribution of participants according to their demographic variables.
Based on the age: 71 %were distributed in the 20-30 years, 17% were distributed in
the 31-40 years and 12% were distributed in the 41 years and above.
Based on the sex: 51% were female and 49 % were male.
Based on the religion: 71 % were distributed in Hindu, 19% were distributed in
Muslim and 10% were distributed in the Christian.
Based on the residence 39% were distributed in the urban and 61% were distributed
in rural.
Based on the Educational qualification: 71 % were distributed in B.Sc. N, 19%
were distributed in GNM and 10% were distributed in the M.Sc.N.
Based on the experience, 64% were distributed <1 years, 18 % were distributed 1-3
years, 18 % were distributed in >3 years
Based on the whether attended any previous classes regarding needle stick
injury: 60% were distributed in No and 40% were distributed in Yes.
Based on the Area of working 36% were in the Ward, 27 % were from the
Causality, 19 % were from the ICU, 7% were in Dialysis, 11% of them in OPD
Section II (Knowledge score)
Knowledge level of the participants regarding the needle stick injury
With regard to knowledge scores of Staff Nurses on importance of needle stick injury,
majority of the Staff Nurses 64% had inadequate knowledge, 36% of them had
moderate knowledge and none of them had adequate knowledge

63
Section III
Association of knowledge score of participants with selected demographic
variables.
The chi-square value shows that there is no significance association between
age, sex, residence area, religion, area of work and level of knowledge with
socio demographic variable.(P > 0.05)
The experience, qualification and previous classes show the significant
association with level of knowledge

64

65
9. BIBLIOGRAPHY
1. Rajasekaran M, Sivagnanam G, Ravindran C, “Injection practices in southern part
of India”, Public Health 2003 May; 117(3):208-13
2. Susan Q, Wilburn BSN,MPH, Gerry Eijkemans MD, “Preventing needle stick
injuries among health care workers”, International Journal of Occupational and
Environmental Health 2004; 10:451-456
3. SumathiMualidhar, Prashanth Kumar Singh,R.K.Jain,MeenakshiMalhotra and
ManjuBala.
4. Indian J Med Res 131,March 2010,pp no 406
5. Prüss-Üstün A, Rapiti E, Hutin Y. Estimation of the global burden of disease
attributable to contaminated sharps injuries among health-care workers. Am .J Ind
.Med 2005; 48: 482–90. @www.google.com
6. Cone JE, Hagadone K, Boyd A. The epidemiology of sharp injuries in the
epidemic of healthcare worker injury. Journal of epidemiology 1999 3:6-7
7. Susan Q. Wilburn, MPH, RN
8. Susan Q, Wilburn BSN,MPH, Gerry Eijkemans MD, “Preventing needle stick
injuries among health care workers”, International Journal of Occupational and
Environmental Health 2004; 10:451-456
9. Purnima Gupta, “Needle stick injury- consequences and prevention.”, Health Care
Management 2006 June
10. McCormick RD, Maki DG. Epidemiology of needle sticks injuries in hospital
personnel. American Journal of Medicine. 1981; 70:928-932.
11. Pruss-Ustun A, Rapiti E, Hutin Y. Estimation of the global burden of disease
attributable to contaminated sharp injuries among health care workers. Am J Ind
Med 2005;48:482-90.

66
12. © Copyright 1997-2017 Canadian Centre for Occupational Health & Safety
13. Ebrahami H. Khosravi A. needle stick injuries among nurses, J.R. Health sciences,
vol. 7, No.2 (2007), pp. 56-62.
14. Rishi Buli, Parveen Sharma. Needle stick injuries in health care providers. The
nursing journal of India, Nov-2008, pp. 251-254.
15. .Nsuduga, Fredrich M, Maritta S. Jalkkola. Tropical medicine and international
health, volume 10, 2005, pp. 773-777.
16. Elmiyeh B, Whitaker S, Tames MT, Chahal CAA, Galea A, Alshafi K, Journal of
the royal society of medicine, volume 97, No. 7, pp. 326-372, 2004.
17. Syed F. Shah, Abdul Bari, Bener, Suad Al Kaabi, Abdul Latif Al Khal,
SofiSamson : Science direct –safety sciences, volume 44, issue 5, June 2006, pp.
387-394.
18. Robert C. Improving the knowledge of trained nurses, Department of public
health medicine, North Wales, health authority, Mold.
19. Varma M, Mehta G. Journal of the Indian medical association, 2000, vol. 95, pp.
436-438.
20. Lee JM 1,.Botteman MF 1, Nicklasson L 2, Cobden D 2, Pashos CL. Needle stick
injury in acute care nurses caring for patients with diabetes melitus: A
Retrospective Study. Current Medical Research and Opinion 2005;21(5):741-47.
21. Jahan S. Epidemiology of needle stick injuries among health care workers in a
secondary care hospital in Saudi Arabia. Ann Saudi Med 2005 May-Jun;
25(3):233-8.
22. Rele M, Mathur M, Turbadkar D. Risk of needlestick injuries in healthcare
workers- A report. Indian J Med Microbiol 2002 Oct-Dec;20(4):206-7.

67
23. Askarian M, Malekmakan L. The prevalence of needle stick injuries in medical,
dental, nursing and midwifery students at the university teaching hospitals of
Shiraz, Iran. Indian J Med Sci 2006 jun;60(6):227-32.
24. Husoyam,mindeT,KnudenH,Tidsskr No Laegeforen,.Needle stick injury
routines.2010 April:130(7),Nowerign. www .pubmed. gov. in
25. RujisWH,Timen .A Guidelines of needle stick injuries risk assessment and post
exposure management in practices Ned TijdschrGeneeskd. 2008 Sep 6;
152(36):1967-71. Review. Dutch. PMID: 18807333.www.pubmed.gov
26. Von OverbeckJ,Wess D Furrer HNeedle stick accident procedure following
potentially infectious exposure in medical personelIn
Geneva.www.pubmed.gov.in
27. Lum D, Meyer-Rochow G, Neveldson GB, Siriwardena M, Turner P, Firth H,
“Needle stick injuries in country general practice.”, Newzealand Medical Journal
1997; 110(1041): 122-5
28. Rio de Janeiro, “Frequency of needle stick injuries and its knowledge among
health care providers in public hospitals of Karachi.”, International AIDS Society
2005 July 24-27
29. Alam M. Knowledge, attitude and practices among healthcare workers on needle
stick injuries. Ann Saudi Med. 2002;22(5-6).
30. Gurubhacharya DL, Mahura KC, Karki DB. Knowledge attitude and practices
among health care workers on needle-stick injuries. Kathmandu univ Med J
2003;1(2):91-4.
31. Zafer A, Aslam N, Nasir N, Meraj R, Mehraj V. Knowledge , attitudes and
practices of health care workers regarding needle stick injuries at a tertiary care
hospital in Pakistan. J Pak Med Assoc 2008;58(2):57-60.
68
32. A Flores, DJ Pevalin, “Health care workers knowledge and attitude to glove use.”,
British Journal of Infection Control 2006(7): 18-22
33. D Debnath, “Improving reporting of sharp injuries.”, Hospital Medicine 2000
Dec, (61): 852-854
34. Juan, Chi-wen MD, Siebers, Chia-Ju RN BS, Chang, Yu-Jun Bcom, “The
attitudes, concerns, gloving practices and knowledge of nurses.”, International
Journal of Nursing Practice 2004; 10(1): 32-38
35. International Journal of Collaborative Research on Internal Medicine & Public
Health Vol. 6 No. 5 (2014)
36. Wang H, Fannie K, He G, Burgess J, Williams AB, A training for prevention of
occupational exposure to blood borne pathogens: Impact on knowledge, behavior
and incidence of needle stick injuries among student nurses in Changsha, Peoples
Republic of China. J AdvNurs 2003 Jan;41(2):187-94
37. Ya-Hui-Yang, Saou-HsingLiou, Chiou-Jong Chen, Chun-Yuh Yang, Chao-Ling
Wang,Chiu-Ying Chen and Trong-Nengwu. The Effectiveness of a Training
Program on reducing needle stick injuries / Sharp object injuries among soon
graduate vocational nursing school students in southern Taiwan. Journal of
Occupational Health 2007;49(5)424-9.
38. Simon LP. Prevention and management of needle stick injury in Delhi. Br J Nurs
2009 Feb 26- Mar11;18(4):252-6.
39. Richard VS, Kenneth J, Ramaprabha P, Kirupakaran H, Chandy GM. Impact of
introduction of sharp containers and of educational programmes on the pattern of
needle stick injuries in a tertiary care centre in India. J Hosp Infect 2001
Feb;47(2):163-5.

70
ANNEXURES- A 1
LETTER REQUESTING PERMISSION TO CONDUCT A PILOT STUDY.
From,
Mr. JAGADEESHA D S
II Year M.Sc. Nursing.
Sri Lakshmi College of nursing.
Bangalore – 91.
To
………………………………
………………………………
………………………………
Forwarded through Principal,
Sri Lakshmi College of nursing.
Bangalore
Respected Madam/ Sir,
SUB: LETTER FOR SEEKING PERMISSION TO CONDUCT MAIN STUDY IN
YOUR HOSPITAL.
I Mr. JAGADEESHA D S, Second year student of M.Sc. Nursing (MSN) at Sri
Lakshmi College of nursing, Bangalore. I have selected the following topic for my Research
Project to be submitted to Rajiv Gandhi University of Health sciences, Bangalore, Karnataka
in partial fulfillment of Master of Science in Nursing Programme.
TITLE OF THE TOPIC:
“A Study To Assess The Knowledge Of Staff Nurses On Needle Stick
Injury In Selected Hospitals At Bangalore With A View To Develop
Informational Booklet.”
I am in need of your permission and esteemed help as I intend to conduct a study to
assess the knowledge of staff nurses on needle stick injury in selected hospitals at Bangalore
with a view to develop information booklet. I am herewith request you to kindly grant
permission and inform the concerned authorities to extend the necessary facilities for me in
your hospital to enable my work on the proposed study personally.
Thanking you in anticipation
Date:
Place: Bangalore Yours faithfully,
[JAGADEESHA D S]

71
ANNEXURES- A 2

72
ANNEXURES- B 1
LETTER REQUESTING PERMISSION TO CONDUCT A MAIN STUDY.
From,
Mr. JAGADEESHA D S
II Year M.Sc. Nursing.
Sri Lakshmi College of nursing.
Bangalore – 91.
To
………………………………
………………………………
………………………………
Forwarded through Principal,
Sri Lakshmi College of nursing.
Bangalore
Respected Madam/ Sir,
SUB: LETTER FOR SEEKING PERMISSION TO CONDUCT MAIN STUDY IN
YOUR HOSPITAL.
I Mr. JAGADEESHA D S, Second year student of M.Sc. Nursing (MSN) at Sri
Lakshmi College of nursing, Bangalore. I have selected the following topic for my Research
Project to be submitted to Rajiv Gandhi University of Health sciences, Bangalore, Karnataka
in partial fulfillment of Master of Science in Nursing Programme.
TITLE OF THE TOPIC:
“A Study To Assess The Knowledge Of Staff Nurses On Needle Stick
Injury In Selected Hospitals At Bangalore With A View To Develop
Informational Booklet.”
I am in need of your permission and esteemed help as I intend to conduct a study to
assess the knowledge of staff nurses on needle stick injury in selected hospitals at Bangalore
with a view to develop information booklet. I am herewith request you to kindly grant
permission and inform the concerned authorities to extend the necessary facilities for me in
your hospital to enable my work on the proposed study personally.
Thanking you in anticipation
Date:
Place: Bangalore yours faithfully,
[JAGADEESHA D S]

73
ANNEXURES- B 2

74
ANNEXURES- B 3

75
ANNEXURE – C
LETTER TO HOD REQUESTING PERMISSION TO CONDUCT STUDY
From,
Mr. MR. JAGADEESHA D S
II year M.Sc. Nursing.
Sri Lakshmi College of Nursing.
TO,
The Head of the department
Department of Medical Surgical nursing
Sri Lakshmi College of Nursing.
Bangalore,
Respected sir/Madam
Sub: Permission to conduct research at Department of Medical Surgical nursing,
SriLakshmi College of Nursing, Bangalore.
With reference to above subject, I would like to bring to your kind notice that,
I Mr. JAGADEESHA D S, II year M.Sc. Nursing student of Sri Lakshmi College of
Nursing, Bangalore, has to submit a Dissertation in my specialty of Medical Surgical
nursing to the Rajiv Gandhi University of Health Sciences as a partial fulfillment of
my requirement. My subject of Dissertation is
“A Study To Assess The Knowledge Of Staff Nurses On Needle Stick
Injury In Selected Hospitals At Bangalore With A View To Develop
Informational Booklet..”
Thanking yours faithfully
Date Yours faithfully
Place: Bangalore.
MR. JAGADEESHA D S

76
ANNEXURE – D
LETTER SEEKING PERMISSION FOR VALIDATION OF THE TOOL
From,
Mr. JAGADEESHA D S
2nd
year M.Sc. Nursing
Sri Lakshmi College of nursing, Bangalore.
To,
..............................................
...................................................
Forwarded through principal
Sri Lakshmi College of nursing
SUB; Request for acceptance to validate the research tool
Respected madam/sir,
I am a post graduate student (medical and surgical nursing) of Sri Lakshmi
College of nursing, Bangalore. I have selected below mentioned topic for research project to
be submitted to Rajiv Gandhi University of health science, Bangalore as a partial fulfilment of
M.Sc. nursing programme.
TOPIC: “A Study to Assess the Knowledge of Staff Nurses On Needle Stick
Injury in Selected Hospitals at Bangalore with a View to Develop Informational
Booklet”
With regards to this may I kindly request you to validate my research to structured interview
schedule for its appropriateness and relevancy. I am enclosing the tools along with objectives
of study for your reference
I would be highly obliged and remain thankful for your great help if you could validate the
tool as early as possible
Thanking you, Yours faithfully
(JAGADEESHA D S)
Enclosure
Reply letter
Envelop

77
ANNEXURE – E
LETTER SEEKING EXPERT’S OPINION AND SUGGESTIONS FOR
CONTENT VALIDITY OR RESEARCH TOOL
From,
Mr. JAGADEESHA D S
2nd
year M.Sc. Nursing
Sri Lakshmi College of nursing, Bangalore.
To,
..............................................
...................................................
Forwarded through principal
Sri lakshmi College of nursing
SUB; Request for opinion and suggestions of experts for establishing content validity of
research tool.
Respected madam/sir,
I am a post graduate student (medical and surgical nursing) of Sri Lakshmi
College of nursing, Bangalore. I have selected below mentioned topic for research project to
be submitted to Rajiv Gandhi University of health science, Bangalore as a partial fulfilment of
M.Sc. nursing programme.
TOPIC: “A Study to Assess the Knowledge of Staff Nurses On Needle Stick
Injury in Selected Hospitals at Bangalore with a View to Develop Informational
Booklet”
With regards to this may I kindly request you to validate my research to structured interview
schedule for its appropriateness and relevancy. I am enclosing the tools along with objectives
of study for your reference
I would be highly obliged and remain thankful for your great help if you could validate the
tool as early as possible
Thanking you, Yours faithfully
(JAGADEESHA D S)
Enclosure
Objectives and hypothesis.
Tools.
Content validity certificate.

78
ANNEXURE- F
CRITERION RATING SCALE FOR VALIDATING THE STRUCTURED
QUESTIONNAIRE ON KNOWLEDGE RELATED TO NEEDLE STICK
INJURY
Respected Madam / Sir,
Kindly go through the content and place tick mark () against
questionnaire in the following columns ranging from very relevant to not relevant,
when found to be not relevant and needs modification kindly give your opinion in the
remarks column.
SL
NO
Item Very
Relevant
Relevant Needs
Modification
Not
Relevant
Remarks
Part -1
Demographic
variables
1
2
3
4
5
6
7
8
79
SL
NO
Item Very
Relevant
Relevant Needs
Modification
Not
Relevant
Remarks
Part 2
Knowledge questionnaire
regarding needle stick
injury
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21

80
22
23
24
25
26
27
28
29
30
SUGGESTIONS:
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
__________________
SIGNATURE OF THE VALIDATOR

81
ANNEXURE-G
CONTENT VALIDITY CERTIFICATE
I hereby certify that I have validated the tool of Mr. JAGADEESHA D S,
M.Sc. Nursing student who is undertaking a study on “A Study To Assess The
Knowledge Of Staff Nurses On Needle Stick Injury In Selected Hospitals At Bangalore
With A View To Develop Informational Booklet.”
Name:
Designation:
Place:
Date:
Signature of the expert
82

83

84

85

86

87

88
ANNEXURE H
CERTIFICATE OF ANALYSIS OF DATA
This is to certify that dissertation done by Mr. JAGADEESHA D S,
2nd
year M.Sc. student of Sri Lakshmi College of Nursing on “A Study to Assess the
Knowledge of Staff Nurses on Needle Stick Injury in Selected Hospitals at
Bangalore with a View to Develop Informational Booklet”. The data analysis for the
study is done by me.
SEAL & SIGNATURE
89


INFORMATION BOOKLET ON
NEEDLE STICK INJURIES
PREPARED BY
MR. JAGADEESHA. D S
II M.Sc. NURSING, (MSN.)
SRILAKSHMI COLLEGE OF NURSING,
SUNKADAKATTE, BANGALORE-91.

NEEDLE STICK INJURIES
Needle stick injuries are wounds caused by needles that accidentally puncture the
skin.Needle stick injuries are a hazard for people who work with hypodermic syringes and other
needle equipment. These injuries can occur at any time when people use, disassemble, or dispose
of needles. When not disposed of properly, needles can become concealed in linen or garbage
and injure other workers who encounter them unexpectedly.
Sharps
"Sharps" include needles, as well as items such
as scalpels, lancets, razor blade, scissors, metal wire,
retractors, clamps, pins, staples, cutters, and glass
items. Essentially, any object that is able to cut the
skin can be considered a "sharp".
Hazards of needle stick and sharps injuries
These injuries transmit infectious diseases, especially
blood-borne viruses. More than 20 pathogens have
been reportedly transmitted from needle sticks.
Concern includes the
Human Immunodeficiency Virus (HIV) which leads
to AIDS (Acquired Immune Deficiency Syndrome),
Hepatitis B,
Hepatitis C.
Injuries have transmitted many other diseases involving viruses, bacteria, fungi, and other
microorganisms to health care workers, laboratory researchers, and veterinarian staff. The
diseases include:
Blastomycosis.
Brucellosis.
Cryptococcosis.
Diphtheria.
Cutaneous gonorrhea.
Herpes.
Malaria.
Mycobacteriosis.
Mycoplasma caviae.
Rocky Mountain spotted fever.
Sporotrichosis.
Staphylococcus aureus.
Streptococcus pyogenes.
Syphilis.
Toxoplasmosis.
Tuberculosis.
Injuries can occur at every stage of their use, disassembly, or disposal. Equipment designs,
nature of the procedure, condition of work, staff experience, recapping, and disposal have all
been mentioned as factors that influence these occurrences.
Activities with potential for needlestick injuries
Home healthcare workers can be at risk for needle sticking or
sharps injuries when they:
• Handle needles that must be taken apart or manipulated after use.
• Dispose of needles attached to tubing.
• Manipulate the needle in the client.
• Recap a needle.
• Use needles or glass equipment to transfer body fluid between
containers.
• Fail to dispose of used needles in puncture-resistant sharps
containers.
• Lack proper workstations for procedures using sharps.
• Work quickly.
• Bump into a needle, a sharp, or another worker while either person
is holding a sharp.
Specific features make certain devices more dangerous.
• Devices with hollow bore needles.
• Needle devices that need to be taken apart or manipulated by the health care worker like
blood drawing devices that need to be detached after use.
• Syringes that retain an exposed needle after use.
• Needles that are attached to tubing like butterflies that can be difficult to place in sharps
disposal containers.

Prevention of needle sticks and sharps injuries
Preventing injuries is the most effective way to protect workers.
A comprehensive sharps injury prevention program would include:
Recommended guidelines.
Improved equipment design.
Effective disposal systems.
Employee training.
Safe recapping procedures, where necessary.
Surveillance programs.
Preventing injuries from sharps and needle sticks is considered a part of the "routine
practices" used by healthcare workers.Workerswho use sharps require education and training as
part of a sharps injury prevention program. Workers should be educated in how to protect
themselves during use and to protect others who may encounter the device during or after
procedures.
PHAC recommends that:
Needles should not be recapped. Used items should be placed immediately in a
designated puncture-resistant container that is easily accessible at the point-of-care.
Healthcare workers should cover open skin areas or lesions on hands and arms with a dry
dressing at all times. Hand hygiene is still essential, so consultation is necessary if the
dressing interferes with this procedure.
Eyes, nose, and mouth should be protected if splashes with blood or body fluids are
anticipated.
First-aid should be immediate if there has been exposure to blood or body fluids. Report
to employer. Follow the employer's procedure for further testing.
First-aid will include:
o Thoroughly rinsing the injury site with running water, and gently cleaning with soap
and water if possible.
o Eyes, nose, or mouth should be flushed with running water.
o Non-intact skin should be rinsed thoroughly.

Steps to take following a needle stick:
If you experienced a sharps injury during your work, immediately follow these steps:
Wash wound with soap and water
Flush out mouth, nose, or skin with water
Irrigate eyes with water, saline, or sterile irrigants
Report the incident to your supervisor
Immediately seek medical treatment at the nearest ER or treatment facility.
Follow-Up:
Get confidential follow-up, post-exposure testing at six weeks, three months, and six
months, and depending on the risk, at one year.
Receive monitoring and follow-up of PEP.
Take precautions (especially by practicing safe sex) to prevent exposing others until
follow-up testing is complete.
Don’t be afraid to seek additional information or a referral to an infectious disease
specialist if you have any questions. Also, consider counseling—a needlestick injury
can be traumatic, regardless of the outcome.
Safer needle device
A safer needle device has built-in safety controls to
reduce needle stick injuries before, during, or after
use and to make needle sticks less likely.

Important Principles
PHAC refers to the CDC "Workbook for designing, implementing and evaluating a
sharps injury prevention program" as an example of a program. This workbook uses a hierarchy
of control approach, including:
Elimination - find ways to eliminate or reduce needle use during procedures, medication
delivery, and specimen collection
Engineering controls - remove or isolate the hazard by using sharps disposal containers or other
devices that have an integrated injury prevention feature. Safety devices must be chosen with
care as no one device or strategy will work in every situation.
Work-practice controls - Steps that can be taken to reduce injuries include using instruments to
grasps needles or load/unload scalpels, avoiding hand-to-hand passage of sharps, separating
sharps from other waste, not carry garbage or linen bags close to the body, etc.
Personal Protective Equipment (PPE) - PPE should be used as the last control approach, where
appropriate.
Vaccination– all staff should consider appropriate vaccination in particular hepatitis B
vaccination where there is a risk of exposure to blood or body fluids.
Employer’s responsibility in the workplace:
Implement the use of engineering controls to reduce needlestick injuries.
Avoid the use of needles when there are other safe alternatives.
Implement use of devices with safety features.
Set priorities and strategies for needle stick injury prevention by examining local and
national information about risk factors.
Ensure proper training of employees on the safe use and disposal of needles.
Modify work practices that have an increased risk of a needle stick injury.
Promote safety awareness in the work environment.
Establish procedures for and encourage the reporting of all needle stick and other sharps-
related injuries.
Evaluate the effectiveness of prevention efforts and provide feedback on performance.

Employee’s responsibility in the workplace:
Avoid recapping needles.
Before beginning any procedure using needles, plan for
safe handling and proper disposal.
Help your employer select and evaluate devices with safety
features.
Use devices with safety features.
Dispose of used needles in appropriate sharps disposal
containers.
Inform your employer of hazards from needles that you
observe at work.
Participate in blood borne pathogen training and follow
recommended infection prevention practices, including
hepatitis B vaccination
Remind employers that they are required by law to
evaluate and purchase safety devices
Make sure that you receive training on any new safety
devices
Place a sharps disposal container close to the procedure
area.
Limit interruptions during procedures
Explain the procedure to patients to gain their cooperation
and avoid potential movement during the procedure
Ask for assistance with patients that might be
uncooperative, such as children
Avoid overfilling sharps disposal containers
Care for yourself
Get a hepatitis B vaccination; this should be provided at no
cost by your employer
Report all needle stick and other injuries

Most needle stick injuries can be prevented with the use of safety devices, which in conjunction
with worker education and training and work practice controls
Training
All staff will receive annual training in:
• The risks associated with blood and body fluid
exposures.
• The correct use of medical devices
incorporating sharps protection mechanisms.
• The importance of immunization and how to
access Occupational Health services
• The reporting, response and monitoring
procedures and their importance.
Disposal of used sharps
An effective system for disposing of used
needles and sharps is crucial to preventing injuries.
Have disposal containers readily available. Workers
should place needles in wide-mouth, puncture-proof
containers. Locate disposal containers specifically
where needles and sharps are used to make safe
disposal possible. Replace the containers before they
are completely filled - sharps containers should be
removed and replaced when they are three quarters full.
Make sure they are sealed, collected, and disposed of in
accordance with local regulations for biomedical waste.
All staff should report every incident in which they
find needles or sharps left at the bedside or thrown into
the regular garbage.

Sharps disposal container height should be:
• Standing workstation: 52 to 56
inches above the standing surface of the
user.
• Seated workstation: 38 to 42 inches above
the floor on which the chair rests
• Sharps containers must be easily accessible
to employees and located as close as
feasible to the immediate area
where sharps are used (e.g., patient care
areas). In areas, such as correctional
facilities and psychiatric units, there may be
difficulty placing sharps containers in the
immediate use area.
• Sharps Containers should be disposed when
the bucket is 3/4 full, rather than waiting to
be completely filled. Most of the
time, sharps containers will have a clear lid
so one can monitor the fill levels.
All the following can be put in a sharps
container,
• Needles.
• Scalpels.
• Broken glass.
• Broken capillary tubes.
• Exposed ends of dental wires.
• Cardio-catheter wires.
• Disposable suture sets and biopsy forceps.
• Electro cautery devices (tips only)
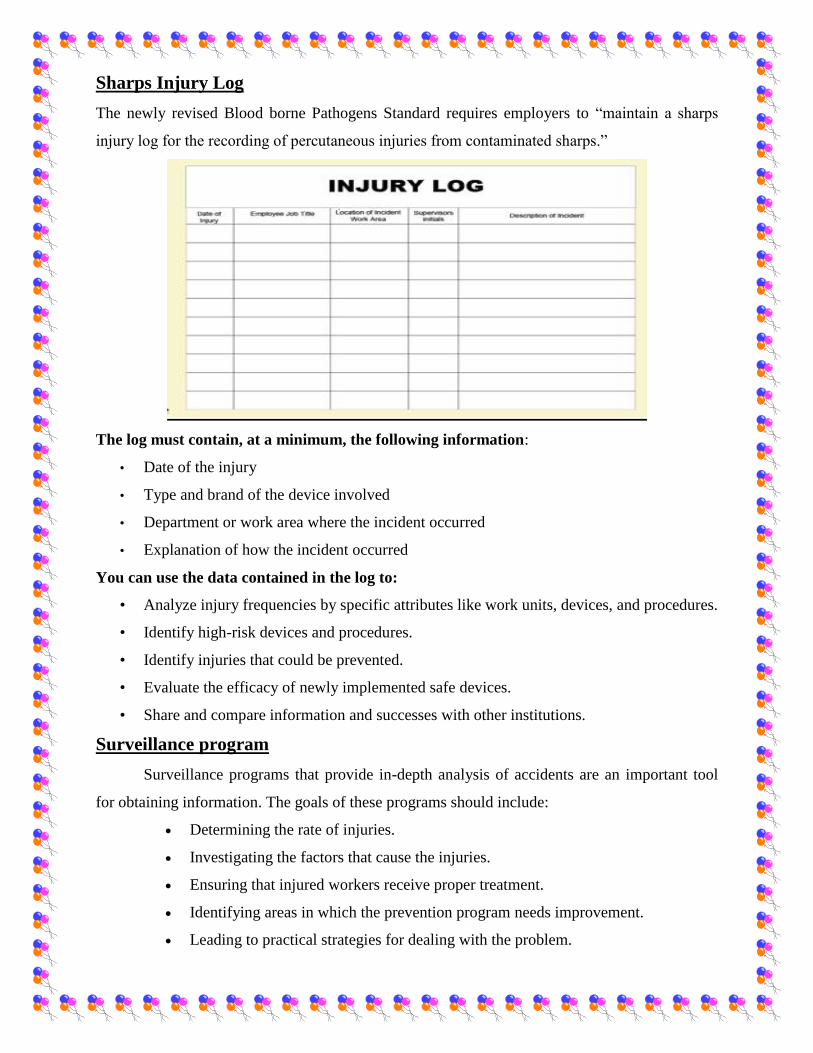
Sharps Injury Log
The newly revised Blood borne Pathogens Standard requires employers to “maintain a sharps
injury log for the recording of percutaneous injuries from contaminated sharps.”
The log must contain, at a minimum, the following information:
• Date of the injury
• Type and brand of the device involved
• Department or work area where the incident occurred
• Explanation of how the incident occurred
You can use the data contained in the log to:
• Analyze injury frequencies by specific attributes like work units, devices, and procedures.
• Identify high-risk devices and procedures.
• Identify injuries that could be prevented.
• Evaluate the efficacy of newly implemented safe devices.
• Share and compare information and successes with other institutions.
Surveillance program
Surveillance programs that provide in-depth analysis of accidents are an important tool
for obtaining information. The goals of these programs should include:
Determining the rate of injuries.
Investigating the factors that cause the injuries.
Ensuring that injured workers receive proper treatment.
Identifying areas in which the prevention program needs improvement.
Leading to practical strategies for dealing with the problem.

xv
TABLE OF CONTENT
SL. NO. CONTENT PAGE NO.
1. Introduction 01
2. Objectives 11
3. Review of literature 18
4. Methodology 30
5. Results 39
6. Discussion 51
7. Conclusion 55
8. Summary 58
9. Bibliography 63
10. Annexure 68

69
ANNEXURES

70
ANNEXURES- A 1
LETTER REQUESTING PERMISSION TO CONDUCT A PILOT STUDY.
From,
Mr. JAGADEESHA D S
II Year M.Sc. Nursing.
Sri Lakshmi College of nursing.
Bangalore – 91.
To
………………………………
………………………………
………………………………
Forwarded through Principal,
Sri Lakshmi College of nursing.
Bangalore
Respected Madam/ Sir,
SUB: LETTER FOR SEEKING PERMISSION TO CONDUCT MAIN STUDY IN
YOUR HOSPITAL.
I Mr. JAGADEESHA D S, Second year student of M.Sc. Nursing (MSN) at Sri
Lakshmi College of nursing, Bangalore. I have selected the following topic for my Research
Project to be submitted to Rajiv Gandhi University of Health sciences, Bangalore, Karnataka
in partial fulfillment of Master of Science in Nursing Programme.
TITLE OF THE TOPIC:
“A Study To Assess The Knowledge Of Staff Nurses On Needle Stick
Injury In Selected Hospitals At Bangalore With A View To Develop
Informational Booklet.”
I am in need of your permission and esteemed help as I intend to conduct a study to
assess the knowledge of staff nurses on needle stick injury in selected hospitals at Bangalore
with a view to develop information booklet. I am herewith request you to kindly grant
permission and inform the concerned authorities to extend the necessary facilities for me in
your hospital to enable my work on the proposed study personally.
Thanking you in anticipation
Date:
Place: Bangalore Yours faithfully,
[JAGADEESHA D S]

71
ANNEXURES- A 2

72
ANNEXURES- B 1
LETTER REQUESTING PERMISSION TO CONDUCT A MAIN STUDY.
From,
Mr. JAGADEESHA D S
II Year M.Sc. Nursing.
Sri Lakshmi College of nursing.
Bangalore – 91.
To
………………………………
………………………………
………………………………
Forwarded through Principal,
Sri Lakshmi College of nursing.
Bangalore
Respected Madam/ Sir,
SUB: LETTER FOR SEEKING PERMISSION TO CONDUCT MAIN STUDY IN
YOUR HOSPITAL.
I Mr. JAGADEESHA D S, Second year student of M.Sc. Nursing (MSN) at Sri
Lakshmi College of nursing, Bangalore. I have selected the following topic for my Research
Project to be submitted to Rajiv Gandhi University of Health sciences, Bangalore, Karnataka
in partial fulfillment of Master of Science in Nursing Programme.
TITLE OF THE TOPIC:
“A Study To Assess The Knowledge Of Staff Nurses On Needle Stick
Injury In Selected Hospitals At Bangalore With A View To Develop
Informational Booklet.”
I am in need of your permission and esteemed help as I intend to conduct a study to
assess the knowledge of staff nurses on needle stick injury in selected hospitals at Bangalore
with a view to develop information booklet. I am herewith request you to kindly grant
permission and inform the concerned authorities to extend the necessary facilities for me in
your hospital to enable my work on the proposed study personally.
Thanking you in anticipation
Date:
Place: Bangalore yours faithfully,
[JAGADEESHA D S]

73
ANNEXURES- B 2

74
ANNEXURES- B 3

75
ANNEXURE – C
LETTER TO HOD REQUESTING PERMISSION TO CONDUCT STUDY
From,
Mr. MR. JAGADEESHA D S
II year M.Sc. Nursing.
Sri Lakshmi College of Nursing.
TO,
The Head of the department
Department of Medical Surgical nursing
Sri Lakshmi College of Nursing.
Bangalore,
Respected sir/Madam
Sub: Permission to conduct research at Department of Medical Surgical nursing,
SriLakshmi College of Nursing, Bangalore.
With reference to above subject, I would like to bring to your kind notice that,
I Mr. JAGADEESHA D S, II year M.Sc. Nursing student of Sri Lakshmi College of
Nursing, Bangalore, has to submit a Dissertation in my specialty of Medical Surgical
nursing to the Rajiv Gandhi University of Health Sciences as a partial fulfillment of
my requirement. My subject of Dissertation is
“A Study To Assess The Knowledge Of Staff Nurses On Needle Stick
Injury In Selected Hospitals At Bangalore With A View To Develop
Informational Booklet..”
Thanking yours faithfully
Date Yours faithfully
Place: Bangalore.
MR. JAGADEESHA D S

76
ANNEXURE – D
LETTER SEEKING PERMISSION FOR VALIDATION OF THE TOOL
From,
Mr. JAGADEESHA D S
2nd
year M.Sc. Nursing
Sri Lakshmi College of nursing, Bangalore.
To,
..............................................
...................................................
Forwarded through principal
Sri Lakshmi College of nursing
SUB; Request for acceptance to validate the research tool
Respected madam/sir,
I am a post graduate student (medical and surgical nursing) of Sri Lakshmi
College of nursing, Bangalore. I have selected below mentioned topic for research project to
be submitted to Rajiv Gandhi University of health science, Bangalore as a partial fulfilment of
M.Sc. nursing programme.
TOPIC: “A Study to Assess the Knowledge of Staff Nurses On Needle Stick
Injury in Selected Hospitals at Bangalore with a View to Develop Informational
Booklet”
With regards to this may I kindly request you to validate my research to structured interview
schedule for its appropriateness and relevancy. I am enclosing the tools along with objectives
of study for your reference
I would be highly obliged and remain thankful for your great help if you could validate the
tool as early as possible
Thanking you, Yours faithfully
(JAGADEESHA D S)
Enclosure
Reply letter
Envelop

77
ANNEXURE – E
LETTER SEEKING EXPERT’S OPINION AND SUGGESTIONS FOR
CONTENT VALIDITY OR RESEARCH TOOL
From,
Mr. JAGADEESHA D S
2nd
year M.Sc. Nursing
Sri Lakshmi College of nursing, Bangalore.
To,
..............................................
...................................................
Forwarded through principal
Sri lakshmi College of nursing
SUB; Request for opinion and suggestions of experts for establishing content validity of
research tool.
Respected madam/sir,
I am a post graduate student (medical and surgical nursing) of Sri Lakshmi
College of nursing, Bangalore. I have selected below mentioned topic for research project to
be submitted to Rajiv Gandhi University of health science, Bangalore as a partial fulfilment of
M.Sc. nursing programme.
TOPIC: “A Study to Assess the Knowledge of Staff Nurses On Needle Stick
Injury in Selected Hospitals at Bangalore with a View to Develop Informational
Booklet”
With regards to this may I kindly request you to validate my research to structured interview
schedule for its appropriateness and relevancy. I am enclosing the tools along with objectives
of study for your reference
I would be highly obliged and remain thankful for your great help if you could validate the
tool as early as possible
Thanking you, Yours faithfully
(JAGADEESHA D S)
Enclosure
Objectives and hypothesis.
Tools.
Content validity certificate.

78
ANNEXURE- F
CRITERION RATING SCALE FOR VALIDATING THE STRUCTURED
QUESTIONNAIRE ON KNOWLEDGE RELATED TO NEEDLE STICK
INJURY
Respected Madam / Sir,
Kindly go through the content and place tick mark () against
questionnaire in the following columns ranging from very relevant to not relevant,
when found to be not relevant and needs modification kindly give your opinion in the
remarks column.
SL
NO
Item Very
Relevant
Relevant Needs
Modification
Not
Relevant
Remarks
Part -1
Demographic
variables
1
2
3
4
5
6
7
8

79
SL
NO
Item Very
Relevant
Relevant Needs
Modification
Not
Relevant
Remarks
Part 2
Knowledge questionnaire
regarding needle stick
injury
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21

80
22
23
24
25
26
27
28
29
30
SUGGESTIONS:
_____________________________________________________________________
_____________________________________________________________________
_____________________________________________________________________
__________________
SIGNATURE OF THE VALIDATOR

81
ANNEXURE-G
CONTENT VALIDITY CERTIFICATE
I hereby certify that I have validated the tool of Mr. JAGADEESHA D S,
M.Sc. Nursing student who is undertaking a study on “A Study To Assess The
Knowledge Of Staff Nurses On Needle Stick Injury In Selected Hospitals At Bangalore
With A View To Develop Informational Booklet.”
Name:
Designation:
Place:
Date:
Signature of the expert

82

83

84

85
86

87

88
ANNEXURE H
CERTIFICATE OF ANALYSIS OF DATA
This is to certify that dissertation done by Mr. JAGADEESHA D S,
2nd
year M.Sc. student of Sri Lakshmi College of Nursing on “A Study to Assess the
Knowledge of Staff Nurses on Needle Stick Injury in Selected Hospitals at
Bangalore with a View to Develop Informational Booklet”. The data analysis for the
study is done by me.
SEAL & SIGNATURE
89

90
ANNEXURE I
STRUCTURED QUESTIONNAIRE
THE TOOL CONSISTS OF THREE PARTS:
Part 1: Demographic variables
Part 2: Questionnaire on knowledge related to Needle stick injury
PART-1: DEMOGRAPHIC PERFORMA.
Instruction; - Dear participants please read the questionnaire carefully and put a tick
mark () in the appropriate places provided.
Date: Participant No.
1. Age in years:
a) 20-30. ( )
b) 31-40. ( )
c) 41-above. ( )
2. Sex:
a) Male. ( )
b) Female. ( )
3. Educational Qualification.
a) B.Sc. Nursing) ( )
b) GNM. ( )
c) M.Sc. Nursing ( )
4. Religion:
a) Christian ( )
b) Hindu ( )
c) Muslim ( )

91
5. Residence belongs to
a) Urban ( )
b) Rural ( )
6. Experience
a) <1 years ( )
b) 1-3 years ( )
c) >3 years ( )
7. Whether attended any previous classes regarding needle stick injury
a) Yes ( )
b) No ( )
8. Area of working
a) Wards ( )
b) Causality ( )
c) ICU ( )
d) Dialysis ( )
e) OPD ( )

92
PART-2
KNOWLEDGE ASSESSSMENT OF STAFF NURSES
REGARDING NEEDLE STICK INJURY.
Instruction: Please read every statement carefully and select one which is most suitable
to you.
GENERAL INFORMATION
1. What is needle stick injury?
a) IV injection. ( )
b) Accidental injury by the health worker ( )
c) Needle injury to the patient ( )
d) Invasive procedure ( )
2. What are sharps?
a) Needles, scalpels and lancets ( )
b) Razor blade and scissors ( )
c) Clamps, pins and staples ( )
d) All the above ( )
3. Expand HBV?
a) Hepatitis B Virus ( )
b) Hepatitis B Vaccine ( )
c) Hemoglobin V ( )
d) None of these ( )
4. Expand AIDS?
a) Acquired Infection Disease Syndrome ( )
b) Acquired Immune Deficiency Syndrome ( )
c) All India Drug Services. ( )
d) None of these ( )
5. Needle stick injuries and exposure of mucous membranes of unintact skin to
blood may lead to which disease?
a) AIDS/ hepatitis B ( )
b) Common cold or flu ( )
c) Skin Cancer ( )
d) Dermatitis ( )

93
6. Highest risky injury is from:
a) Blood filled hollow bore needles. ( )
b) Blades ( )
c) Plain needles ( )
d) Suture needles ( )
7. HIV transfers in health workers at a ratio?
a) 1: 3000 ( )
b) 1: 300 ( )
c) 3: 100 ( )
d) 2: 100 ( )
8. Name the Blood borne Pathogens that medical staff and health personnel are
most commonly exposed to:
a) HIV ( )
b) Hepatitis B ( )
c) Hepatitis C ( )
d) All the Above ( )
9. Which of the following is not a factor that influence the occurrences of needle
stick injury
a) Equipment design ( )
b) Nature of the procedure ( )
c) Staff experience ( )
d) Manufactures of the equipment ( )
10. Needle stick Injuries can occur at which stage of use?
a) During injection/procedure ( )
b) While assembling or disassembling ( )
c) During Disposal ( )
d) Every stage of use ( )
11. Expand PPE
a) Private Protective Equipment ( )
b) Personal Protective Equipment ( )
c) Purified Protein Element ( )
d) Patient Protective Equipment ( )

94
12. What personal protective equipment (barriers) need to be worn to protect the
Mucous membranes of the face against splash with blood/ body fluids?
a) Mask ( )
b) Goggles ( )
c) Both a and b ( )
d) None of these. ( )
13. Whom should you tell if you see needles without a safety device?
a) Charge Nurse ( )
b) Co-Worker ( )
c) Supervisor or Safety Officer ( )
d) Patient ( )
14. First-aid for needle stick injury will include:
a) Thoroughly rinsing the injury site with running water ( )
b) Bandage the site ( )
c) Wipe the blood ( )
d) None of these ( )
15. As part of sharps injury prevention, workers who use sharps require
a) Medicine ( )
b) Education and training ( )
c) High salary ( )
d) Promotion ( )
16. Needle stick accidents may be avoided by:
a) Safer devices and techniques ( )
b) Gloves ( )
c) Mask ( )
d) Gown ( )
17. What is the maximum capacity for a sharp container?
a) 100% ( )
b) 75% ( )
c) 90% ( )
d) 80% ( )

95
18. TO whom we should report after a needle stick accident?
a) Patient ( )
b) Doctors ( )
c) Supervisor ( )
d) Owner of hospital ( )
19. Sharp containers should be ______ to _______ inches from the floor at a
standing workstation
a) 50- 55 inches ( )
b) 52- 56 inches ( )
c) 56- 60 inches ( )
d) 60- 65 inches ( )
20. Sharp containers should be ______ to _______ inches from the floor at a
sitting workstation
a) 44- 48 inches ( )
b) 38- 42 inches ( )
c) 32-36 inches ( )
d) 48-52 inches ( )
21. Where should a sharps container be located?
a) Close to Patient bed ( )
b) Close to Patient care area ( )
c) Close to Doctors room ( )
d) Close to Nurse’s station ( )
22. What percentage of needle stick injury can be prevented with the use of safer
needle devices?
a) 100 % ( )
b) 90 % ( )
c) 80 % ( )
d) 70 % ( )
23. When did the Needle stick Safety and Prevention Act introduced?
a) 2000 ( )
b) 1953 ( )
c) 2001 ( )
d) 2005 ( )

96
24. When did the Needle stick Safety and Prevention Act come into effect?
a) 2000 ( )
b) 1953 ( )
c) 2001 ( )
d) 2005 ( )
25. According to Public Health Agency of Canada’s Recommendation after the
procedure the needles,
a) Should be recapped carefully ( )
b) Should be thrown in dust bin ( )
c) Should not be recapped ( )
d) Should be reused ( )
26. How should sharps be disposed of?
a) In disposal containers ( )
b) Can be reused ( )
c) In open area ( )
d) In garbage ( )
27. Which of the following is not the part of surveillance program?
a) Determining the rate of injuries ( )
b) Providing proper care for the patient ( )
c) Investigating the factors that cause the injuries. ( )
d) Ensuring that injured workers receive proper treatment. ( )
28. What's a safer needle device?
a) It can save the patient ( )
b) It may not be painful ( )
c) It has built-in safety controls ( )
d) Needles can be hold safely. ( )
29. Who all are responsible for preventing needle stick injury in a Hospital?
a) Employers and employees ( )
b) Patient and relatives ( )
c) Manufacturing companies ( )
d) Law ( )
97
30. The nurse should report:
a) All needle stick injuries ( )
b) Sharps-related injuries ( )
c) Blood splashes ( )
d) All the above. ( )

98
ANNEXURE - J
LIST OF EXPERTS
1. Mrs. Bhagyalakshmi .R
Principal,
Srilakshmi College of nursing
Bangalore.
2. Mrs. Manju Thomas
Asso.Professor
Medical and Surgical Nursing,
Srilakshmi College of nursing
Bangalore.
3. Mr. Melbin Michael Arackal
Asso.Professor
Medical and Surgical Nursing
Shantidhama College Of Nursing
Bangalore.
4. Mrs. Viji C
Professor
Medical and Surgical Nursing
Brite College Of Nursing
Bangalore

99
5. Mrs. Vanamathi T
Professor
Medical and Surgical Nursing
Gayathri College Of Nursing
Bangalore
6. Dr. M. L. Giridhar
Medical Director
Sri Lakshmi Multi Specialty Hospital
Bangalore.
7. Mr. D. Elakkuana Bhaskar Raj
Dept.Of Biostatistics

100
ANNEXURE - K
STATISTICAL FORMULAS
1) Spearman’s Brown Prophecy formula for reliability
2 r
r¹ =
1+ r
r- The correlation coefficient computed on the split halves
r- The estimated reliability of the entire test
For computing coefficient of correlation:
Raw score method:
r = ∑ x y – x y
n
S1 .S2
Deviation method:
r = ∑ x y
∑ x2.∑ y
2
2) Descriptive statistics
Mean X = ∑ x
n

101
Standard deviation = ∑ x2 - (∑ x)
2
n
n-1
3) Inferential statistics
Chi square χ² = ∑ (O-E) 2
E

102
ANNEXURE - L
CERTIFICATE FOR ENGLISH EDITING
This is to certify that the tool prepared by JAGADEESHA D S,
II year M. Sc. nursing student of Sri Lakshmi College of Nursing for his study “A
Study to Assess the Knowledge of Staff Nurses On Needle Stick Injury in
Selected Hospitals at Bangalore with a View to Develop Informational Booklet”
is translated and edited for appropriateness by me.
Seal and Signature