a study to assess the challenges faced in labour …
TRANSCRIPT
i
A STUDY TO ASSESS THE CHALLENGES FACED
IN LABOUR WARD AT NAROK DISTRICT
HOSPITAL.
BY
SHEILA C. SAWE
(BMS/7060/62/DF)
A RESEARCH REPORT SUBMITTED TO FACULTY OF CLINICAL
MEDICINE AND DENTISRY IN PARTIAL FULLFILMENT OF THE
REQUIREMENT
FOR THE AWARD OF BACHELOR’S DEGREE IN MEDICINE AND
BACHELORS OF SURGERY OF KAMPALA INTERNATIONAL
UNIVERSITY
DECEMBER 2013.

ii
DECLARATION I declare that this report is my original work based on facts and figures collected in Narok
District Hospital.
NAME: Sheila C. Sawe
SIGNATURE: ……………………….. DATE……………………..
SUPERVISOR SIGNATURE DATE
PROF. BEGUMYA YOVAN ………………… ………………
iii
ACKNOWLEDGMENT
I acknowledge the staff at Narok District Hospital, in particular the Medical Superintendent for
allowing me to carry out this research and staff in the obstetric wards participating in carrying
out of this study.
I acknowledge my supervisor, Prof. Begumya (Department of Physiology), for his guidance and
assistance in the preparation of this report.
I acknowledge the members of the Narok District Health Management Team for their invaluable
assistance during the carrying out of this research.
Lastly, I acknowledge the guardians interviewed for their contribution to this research.

iv
DEDICATION
I dedicate this report to my dear mother and to the mothers of Narok.

v
LIST OF ABBREVIATIONS
DHMT - District Health Management Team
DMOH – District Medical officer of Health
COBES - Community Based Education and Service
MCH – Maternal and Child Health
MCH/FP – Maternal and Child Health/ Family Planning
NGO – Non Governmental Organizations’
POPC – Pediatric Out-Patient Clinic
SOPC – Surgical Out-Patient Clinic
MOPC – Medical Out-Patient Clinic
GOPC – Gynecology Out-Patient Clinic
FGM Female Genital Mutilation
HMB Health Management Board
HIV/ AIDS Human Immuno-Deficiency Virus/ Acquired Immuno-Deficiency Syndrome
GOK Government of Kenya
PMTCT Prevention of Mother To Child Transmission
MTRH Moi Teaching and Referral Hospital
KNH Kenyatta National Hospital

vi
Contents
DECLARATION .......................................................................................................................................... ii
ACKNOWLEDGMENT .............................................................................................................................. iii
DEDICATION ............................................................................................................................................. iv
LIST OF ABBREVIATIONS ....................................................................................................................... v
ABSTRACT ................................................................................................................................................ vii
CHAPTER ONE ........................................................................................................................................... 8
1.1 Background information ..................................................................................................................... 8
1.2 Study objectives ................................................................................................................................ 10
Broad objective ................................................................................................................................... 10
Specific objectives .............................................................................................................................. 10
1.3 Justification for the study .................................................................................................................. 10
CHAPTER TWO ........................................................................................................................................ 11
2.0 LITERATURE REVIEW ................................................................................................................. 11
Introduction. ............................................................................................................................................ 11
CHAPTER THREE .................................................................................................................................... 13
3.0 METHODOLOGY ........................................................................................................................... 13
CHAPTER FOUR ....................................................................................................................................... 14
4.0 FINDINGS ........................................................................................................................................ 14
APPENDIX I .............................................................................................................................................. 25
APPENDIX II ............................................................................................................................................. 29
1.1 map of the DISTRICT: SHOWING the health services and facilities in the district .................... 29

vii
ABSTRACT
Title:
Assess challenges faced in the labour ward at Narok District Hospital
Broad objective:
To determine challenges faced in the labour ward at Narok District Hospital.
Methodology:
A cross sectional study was done at Narok District hospital on staff and women attended to in
labour ward. Convenience sampling patients was used with a sample size of 75, data collected
using interviewer administered questionnaires, entered and analyzed on Microsoft excel and
presented as tables, pie charts and graphs.
Findings
Average age of respondents was 24 years, majority (56%)of respondents were of the Maasai
community. All care providers (12) used a partograph for each delivery and all respondents said
that partographs were readily available in labour ward. Few healthcare providers (33%) checked
all vitals according to standard protocol. 33% of those who didn’t attributed this to lack of
instruments, and 33% to being overwhelmed by number of patients.
All healthcare providers managed labour using a partograph and (83%) performed active labour.
A number of care providers (41%) did not feel motivated to work in labour ward, (34%) felt
overworked and 25% contented. Each respondent attended to an average of 8 patients per day.
Many healthcare providers (89%) said language barrier hindered service delivery and all stated
culture and traditional practices of women in Narok district hindered services delivery in labour
ward.Majority (68%) attributed it to FGM, (42%) to gender inequality.
Only (33%) of health care providers felt there were adequate supplies in labour ward. Majority
(67%) said laboratory results were available on time.
Majority of patient (54%) respondents were Primigravidae. Of the multiparous respondents,
(58%) had had home delivery using traditional birth attendants.
Respondents took an average of 3.6hrs to deliver after arriving at the hospital
Majority of respondents rated services at the labour ward as Affordable.
Many patient respondents (65%) rated service offered as Good and 35% thought it was
Excellent.
Conclusion
i. Patients in labour ward are young adults with an age average of 24years.
ii. Staff in labour ward are not motivated and feel overworked.
iii. There is inconsistency in availability of supplies in labour ward.
iv. Culture and traditional practices in Narok hinder optimum service delivery in labour
ward.
8
CHAPTER ONE
1.0 Study Introduction
Maternal mortality is a major health problem in Kenya. Most recent estimates by Kenya
Demographics Health Survey 2003 are 414 maternal deaths per 100,000 live births.
Deteriorating public health service and the HIV/AIDS epidemic are contributing factors.
Kenyan women face a 1 in 20 lifetime risk of maternal death, which is the leading cause
(27%) among women of childbearing age in Kenya. There are five major causes of maternal
death: hemorrhage, infection, hypertensive disease in pregnancy, unsafe abortion and
obstructed labour. Many of these deaths could be averted if women had access to essential
obstetric care when they need it.
This research aims at assessing the challenges faced in the labour ward at Narok district
hospital.
1.1 Background information
Narok District hospital is located in Narok North district, Narok County. It was founded in
1969. Narok district covers an area of 15087.8 square kilometers and has an approximate
population of 365,750 people. It’s bordered by Bomet District, Nakuru District, Kajiado
District, and Transmara District.
The district hospital attends to approximately 400,000 people some of who are from the
neighboring districts.
The district hospital has an outpatient department in which several clinics are run. They
include the Dental clinic, Eye clinic, POPC, SOPC, MOPC, GOPC, the mother and
child/family planning clinic (MCH/FP) and the diabetic clinic. The hospital also has an
inpatient department with a capacity of 155 beds with surgical, medical, paediatric,
gynaecology and maternity wards.

9
There are a number of health facilities in the district. They are summarized below.
Table 1 number of facilities in the district
GOK
NGO No. Health_ Facility_ Name
No. Health_ Facility_ Name
Agency
1
Narok District
Hospital
D.
Hos
1
Ereto Project H/C CCF
/Comm.
2 Olokurto H/C
2 Siyapei Disp. AIC
3 Enabel bel H/C
3 Enoosupukia Disp. Catholic
4 Nairagie Enkare H/c
4 Olenkasurai Disp. Mission
5 Ololpironito H/C
5 Olendeem Disp. ACK
6 Sakutiek H/C
6 Nturumeti Disp. ACK
7 G K Prison Disp.
7 Oloropil Disp. Catholic
8 Nkareta Disp.
8 Olasiti Disp. AIC
9 Naisoya Disp.
9 Olokirikirai Disp. Catholic
10 oletukat Disp.
10 fauntain medical services Disp. Mission
11 Ewaso Ngiro Disp.
11 Nairasirasa Disp. Mission
12 enteyani Disp.
12 Olooltoto
13 Olpusimoru Disp.
13 PCEA Nairasirasa
14 Olchorro Disp. 15 Entol tol Disp. 16 Kojonga Disp. 17 Mosiro Disp. 18 Enaibor Ajijik Disp. 19 Ongata naado Disp. 20 Ilaiser Disp. 21 Ntulele Disp.
The top ten diseases in the district according to the health records are
1. Malaria
2. Diarrhea
3. Pneumonia
4. Dehydration
5. Anaemia
6. Tuberculosis
7. Typhoid
8. HIV/AIDS
9. Diabetes mellitus
10. Meningitis

10
1.2 Study objectives
Broad objective
To determine challenges faced in the labour ward at Narok District Hospital.
Specific objectives
1. To assess practices of staff in labour ward at Narok District Hospital.
2. To assess the availability and reliability of equipment in labour ward at Narok
District Hospital
3. To assess the influence of gender inequality and traditional practices and beliefs on
procedures in labour ward at Narok District Hospital.
1.3 Justification for the study
In Kenya bearing children is still considered as a primary purpose of marriage. While there
are 10 maternal deaths per 100,000 live births in developed countries, in Kenya the ratio is
alarmingly high at 488 per 100,000 live births as of 2010 an increase from 414 per 100,000
in 2003.
25years after the launch of Kenya Safe Motherhood Program, maternal and neonatal
mortality ratio remain high. It currently stands at 488 per 100,000 a mere drop compared to
657 per 100,000 live births in 1987. Several factors have played a role in the poor health
indicators. The major factors are HIV/AIDS pandemic, shortage of trained nursed and
midwives, inadequate resources in the hospitals and gender inequality and traditional
practices.
11
CHAPTER TWO
2.0 LITERATURE REVIEW
Introduction.
Labour is the culmination of a human pregnancy or gestation period with the birth of one or
more newborn infants from a woman's uterus. It is a process that requires careful monitoring
of both the mother and the fetus due to their vulnerability at the time. An efficient, well-
staffed and equipped labour ward plays a key role in achieving this goal.
Hemorrhage, sepsis, hypertension disorders of pregnancy, obstructed labour, complications
of induced labour are the top five killers. [1]
The global dimension.
A comparison of labour and birth outcomes in Jordan with WHO guidelines found: the rates
of a number of labour and birth practices were inappropriately high, and differed from WHO
guidelines and evidence-based recommendations. [2]
Majority of hospitals do not have written policies or standard birth procedures and lack
mechanisms for evaluation. Generally, minimal prenatal information is given to women.
The reported configuration of professional care during labour and delivery is favorable to
high quality care. 31 hospitals set an i.v. drip to all women and some use continuous fetal
monitoring method. Nearly all hospitals give intra-muscular anesthesia whereas epidurals
are used less frequently. [3]
About 63% of births were attended by a skilled attendant: from 47% in Africa to 88% in
Latin America/Caribbean. In 16 of 23 countries with data, less than 50% of the
recommended levels of emergency obstetric care had been fulfilled. Countries with maternal
mortality ratios of 750+ per 100,000 live births shared problems of high fertility and
unplanned pregnancies, poor health infrastructure with limited resources and low
availability of health personnel. [4]
The African dimension.
In a study on the challenges facing nurse-midwives in working towards Safe Motherhood in
Malawi, it was noted that public hospitals were running with critical shortage of medical
supplies and equipment. This could have contributed to considerable delays in provision of
care and poor quality care, unnecessary deaths from emergencies and frustration of nurse-
midwives. Sometimes an attendant had to leave to go to another ward in search of supplies.
There was also a shortage of nurse-midwives leading to a high client to nurse-midwife ratio,
this contributed to poor quality of care.
Gender inequality also played a big role; there were some delays in seeking maternity care
due to the fact that women couldn’t make independent decisions to seek care when sick.
Majority of women were not economically empowered and this put them in a situation
whereby they could not do much to improve their wellbeing. [5]

12
A study in Burkina Faso on quality of antenatal care and obstetrical coverage in rural
Burkina Faso Health facilities were poorly equipped, and the availability of qualified staff
remained low (mean total score for the provision of care was 22.9 +/- 4.2, ranging from 14
to 33. [6]
A study on how a midwife can change attitudes showed The midwife employs the services
of a good interpreter and gives Somali women the information they require to plan a
delivery. All but one of the women had undergone female genital mutilation, and the
midwife urged the women to become de-infibulated early in the pregnancy. The midwife
also used this opportunity to discuss the health problems that follow female genital
mutilation in an effort to dissuade the couple from having any female children subjected to
this practice. Most of her clients reported their intention to keep their daughters intact.
[7]
In evaluation on the affordability of labour ward services in district hospitals a study done in
South Africa concluded that the Unit costs of inpatient days in district hospitals for
maternity patients was more than double the average unit cost for medical patients. [8]
In East Africa, Using practical quality improvement approaches and tools in reproductive
health services resulted in high-quality care, including management and supervision, safety,
and information and client--provider interactions. For example, maternity ward staff learned
how to pass on to their clients’ information about clients' rights and family planning
methods through posters, pamphlets, sample contraceptives, and health talks. However
Quality Improvement requires considerable staff development and capacity building at all
levels. [9]
The Kenyan perspective.
In a report by Kenyan Ministry of Health titled Safe Motherhood Demonstration Project
Western Province 2004, Provider knowledge and experience was to seen to improve over
the project period. More providers used partographs to manage labour and improved
management of complications. More providers monitored labour more effectively and
referred earlier. Fewer women gave birth after more than 12 hours of labour. Significantly
more women delivered with Skilled Attendance at home. Health care providers were more
knowledgeable about obstetric problems and had more experience to manage them.
Management and organizational issues had improved including an improvement in systems
for procurement of equipment, drugs and supplies. Fewer women had to bring in drugs and
supplies during labour. More health facilities were now using guidelines and protocols. [10]

13
CHAPTER THREE
3.0 METHODOLOGY
Study area
The study area was Narok District Hospital.
Study setting
Labour ward.
Study design
Cross sectional study.
Study population
Doctors, clinicians and nurses in labour ward.
Women attended to in labour ward at Narok District Hospital.
Sampling technique
Purposive sampling was used.
Data collection
Data was collected using interviewer administered questionnaires and observational check
list
Data analysis and presentation
Microsoft excel was used to generate percentages from findings entered for easy
comparison, and drawing of conclusions. Qualitative data was analyzed intelligently then
organized and presented as thematic issues in narrative form. Pie charts were used for
presenting quantitative data.
Inclusion criteria
Medical staff working in labour ward at Narok District Hospital
Women attended to in labour ward .
Limitation of the study
Time was limited.
Ethical considerations
Obtaining informed consent from the participants.
Observing confidentiality by not disclosing the names of the participants who took
part in the study.
Information obtained from the participants was treated with confidentiality.
Consent was sought from the hospital administration to carry out the study.

14
CHAPTER FOUR
4.0 FINDINGS
4.1Demographic data
Average age of respondents was 24 years
Table 1 Average age of patient respondents.
AVERAGE AGE 24YEARS
Majority (56%)of respondents were of the Maasai community.
Fig 1 Bar graph showing the community of patients interviewed (n=34)
0
2
4
6
8
10
12
14
16
18
20
COMMUNITIES

15
4.2 Management of patients in labour ward
All care providers n=12 (100%) used a partograph for each delivery.
All (100%) respondents said that partographs were readily available in labour ward.
Few healthcare providers (33%) checked all vitals according to standard protocol.
Fig 1 Bar graph showing care providers who checked all vitals according to
Protocol (n=12)
n=4 (33%) of those who didn’t check all vitals attributed this to lack of instruments, and
33% to being overwhelmed by number of patients.
Fig 2 Factors for not checking all vitals according to protocol (n=12)
LACK OF INSTRUMENTS
OVER-WHELMED BY
PATIENTS
FACTORS FOR NOT CHECKING ALL VITALS
0% 10% 20% 30% 40% 50% 60% 70%
CHECKED ALL VITALS
ALL VITALS NOT CHECKED
VITALS

16
All (100%) healthcare providers managed labour using a partograph.
Majority of healthcare providers (83%) performed active labour.
Fig 3 Pie Chart showing type of labour management used (n=12)
41% of care providers did not feel motivated to work in labour ward.
A few (34%) felt overworked.
Each respondent attended to an average of 8 patients per day.
Fig 4 Bar Gragh showing attitude of healthcare providers (n=12)
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
NOT MOTIVATED OVER WORKED CONTENTED
41%
34%
25%
ACTIVE LABOUR83%
CONSERVATIVE LABOUR
17%
LABOUR MANAGEMENT

17
Many healthcare providers (89%) said language barrier hindered service delivery
TABLE 2 Influence of language in service delivery in labour ward
LANGUAGE BARRIER HEALTHCARE PROVIDERS
HINDERED SERVICE DELIVERY 10
NO LANGUAGE BARRIER 2
All healthcare providers 100% said culture and traditional practices of women in Narok
district in labour ward hindered services delivery.
Majority (68%) attributed it to FGM, (32%) to gender inequality.
Fig 5 Pie Chart showing influence of culture and traditions in service delivery (n=12).
68%
32%
INFLUENCE OF CULTURE AND TRADITION
FGM
GENDER INEQUALITY

18
Table 3 Check List showing equipment and supplies available in labour ward
Equipment and Supplies Check/Remarks
Delivery beds 3
Number of delivery sets, vaginal specula, tear repair sets 1
Fridge, vaccine carrier with ice packs -N
Adult scale 1
Infant scale 1
BP machine 1
Stethoscope -N
Fetoscopes- Doppler 3
Thermometers -N
Suction machine 1
Resusitation tray -N
Vacuum extractor and set -N
Spotlight 3
Oxygen concentrator 1
Heater for neonates 1
Guidelines for management of obsteric complications,
PMTCT
-N
Drugs: Oxytocin, Magnesium Sulphate
Y
Antibiotics: Gentamicin, Pen G Y
Analgesics: Ibuprofen, Diclofenac Y
Antihypertensive drugs; e.g Hydralazine Y
Sutures and Local Anaesthesia -N
Disinfectant, 3 buckets, Skin didinfection of mothers Y
Autoclave -N
Long glaves Y
Referal system in place? Where? Kijabe
Mission Hosp, MTRH,
KNH

19
Only (33%) of health care providers felt there were adequate supplies in labour ward.
Fig 6 Pie Chart showing timely availability of laboratory results for labour ward.
(n=12)
Majority (67%) said laboratory results were available on time.
Fig 7 Pie Chart showing timely availability of laboratory results for labour ward.
(n=12)
33%
67%
SUPPLIES IN LABOUR WARD
ADEQUATE SUPPLIES INADEQUATE SUPPLIES
67%
33%
LABORATORY RESULTS
AVAILABLE ON TIME
DELAYED
20
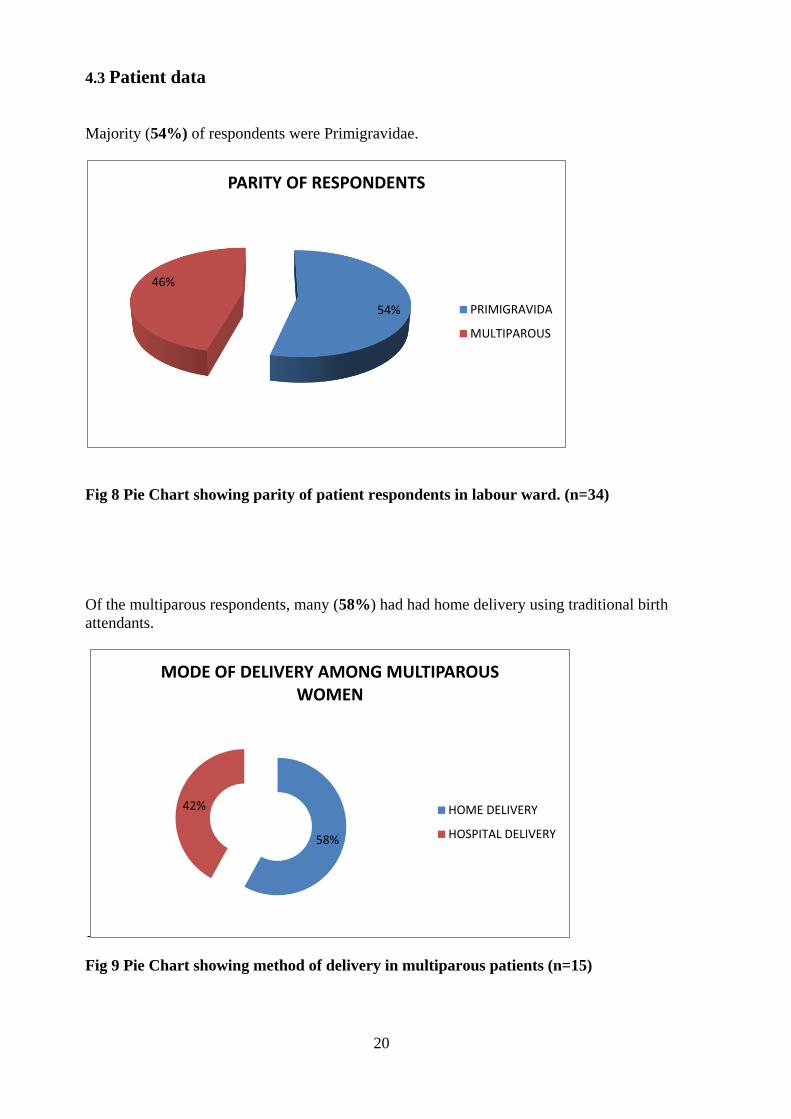
4.3 Patient data
Majority (54%) of respondents were Primigravidae.
Fig 8 Pie Chart showing parity of patient respondents in labour ward. (n=34)
Of the multiparous respondents, many (58%) had had home delivery using traditional birth
attendants.
Fig 9 Pie Chart showing method of delivery in multiparous patients (n=15)
54%
46%
PARITY OF RESPONDENTS
PRIMIGRAVIDA
MULTIPAROUS
58%
42%
MODE OF DELIVERY AMONG MULTIPAROUS WOMEN
HOME DELIVERY
HOSPITAL DELIVERY

21
Respondents took an average of 3.6hrs to deliver after arriving at the hospital
Fig 10 Graph showing average number of hours to delivery after arriving at the
hospital (n=34)
Majority of respondents rated services at the labour ward as Affordable.
Table 4 Cost of labour ward services
COST CHEAP AFFORDABLE EXPENSIVE
PATIENTS 0 29 5
Many respondents (65%) rated service offered as Good and 35% thought it was Excellent.
Table 5 Quality of services in labour ward
QUALITY POOR AVERAGE GOOD EXCELLENT
PATIENTS 0 0 22 12
0
1
2
3
4
5
6
7
8
9
0 5 10 15 20 25 30 35 40
(HR
) TO
DEL
IVER
Y O
NC
E IN
HO
SPIT
AL
PATIENTS

22
CHAPTER FIVE
5.0 DISCUSSION
Majority of respondents were in their youth,24 years and were of the Maasai community.
This could be attributed to; Culture and society. Maasai girls are subjected to early
marriages and lack of girl child education [4]
Partographs are widely used to manage labour. This can be attributed to government policy
on protocal adherence, Nurses, doctors and clinicians are well versed with its use and
availability of partographs.[10]
Respondents took an average of 3.6hrs to deliver after arriving at the hospital. This agreed
with a report by Kenyan Ministry of Health titled Safe Motherhood Demonstration Project
Western Province 2004, which found that in: Intrapartum Care: Significantly more providers
are using partograph to manage labour and improved Management of complications. Fewer
women gave birth after more than 12 hours of labour. [10,12]
However few health care providers checked all vitals according to standard protocol citing
lack of instruments such as blood pressure machine, thermometers. [5,6]
Negligence by healthcare providers also played part. This agreed with a study that found
that; the rates of a number of labour and birth practices were inappropriately high, and
differed from WHO guidelines and evidence-based recommendations. [2]
Healthcare providers did not feel motivated to work in labour ward and felt overworked. [5]
Poor enumeration and lack of consistent availability of supplies to facilitate their work were
contributuing factors. There was lack of consistency of supplies in labour ward. This was as
a result of lack of prioritization in funding labour ward by the hospital and sharing of
equipment between different departments leading to inconviniences. [6,9]
Language barrier was a problem in labour ward. Less than half could communicate in both
Kiswahili and English.majority of respondents only apprehended mother-tongue. Maasai
language is widely spoken in Narok and there was lack of adequate formal education. [7]
Home delivery by traditional birth attendants is still widely practiced.[4] There was
availability of trained traditional birth attendants in the villages, influence of traditional
beliefs and practices and inaccessibility of health facility due to poor road
infrastructure.Language barrier hindered service delivery in labour ward. This led to
inaccurate patient history.[3]
Culture and traditional practices in Narok district in labour ward also hindered services
delivery. Consent could only be given by the patients’ husband and Female Genital
Mutilation led to prolonged labour due to altered physiology of delivery. [5,7]
Majority of respondents rated services at the labour ward as Affordable. This was in contrast
to a study done in South African district hospitals. [8]

23
CHAPTER SIX
6.0 CONCLUSION
1. Patients in labour ward are young adults with an age average of 24years.
2. Staff in labour ward are not motivated and feel overworked.
3. There is inconsistency in availability of supplies in labour ward leading to service
delivery inconveniences.
4. Culture and traditional practices in Narok hinder optimum service delivery in labour
ward.
7.0 RECOMMENDATIONS
To Ministry of Medical Services
1. Better pay for Nurses and clinicians
2. Post more doctors, nurses and clinicians to District Hospitals
3. Adequately fund budgets of District Hospitals
To Narok District Hospital
1. Allocate more funds to labour ward for consistent availability of supplies
2. Avail equipments to every department to avoid inconveniences of sharing
To Narok District Community leaders
1. Hold forums to empower women
2. Educate the public on adverse effects of female genital mutilation
3. Encourage women to deliver in hospitals

24
REFERENCES
1. Trends in mortality rate: 1990 to 2008 .Estimates developed by World Health
Organization, UNICEF, UNFPA and The World Bank (2010)
2. Khresheh R, Homer C, Barclays L: A comparison of labour and birth outcomes in
Jordan with W.H.O guidelines. Midwifery,2009 Dec, 25(6)
3. Khayat R, Campbell O: Hospital practices in maternity wards in Lebanon. Health Policy
Plan, 2000 Sep;15(3):
4. Shah IH, Say L (2007). Maternal mortality and maternity care from 1990 to 2005:
uneven but important gains. Reprod Health Matters Nov; 15(30):17-27.
5. M. Hami (2005). The Challenges Facing nurse-midwives in working towards Safe
Motherhood in Malawi. Malawi Medical Journal17 (4): 125-127
6. Nikiema L. (2010). Quality of antenatal care and obstetrical coverage in rural Burkina
Faso. J Health Popul Nutr Feb; 28(1):67-75.
7. Nybro L (1998) How a midwife can change attitudes. Entre Nous Cph Den. Spring
;(38):7.
8. Olukoga A (2007). Unit costs of inpatient days in district hospitals in South Africa.
Singapore Med J. Feb;48(2):143-7.
9. Dohlie MB, Mielke E, Mumba FK, Wambwa GE, Rukonge A, Mongo W et al. Using
practical quality improvement approaches and tools in reproductive health services in
East Africa. Jt Comm J Qual Improv. 1999 Nov;25(11):574-87.
10. Wilson Liambila et al (2004). Kenya Ministry of Health: Safe Motherhood
Demonstration Project Western Province, 2004.
11. Routines in facility-based maternity care. BJOG, 2005 Sep; 112(9):1270-6
12. Spiby H, Green JM et al (2012). Early labour services: Changes, triggers, monitoring
and evaluation. Midwifery. Jul 26.
25
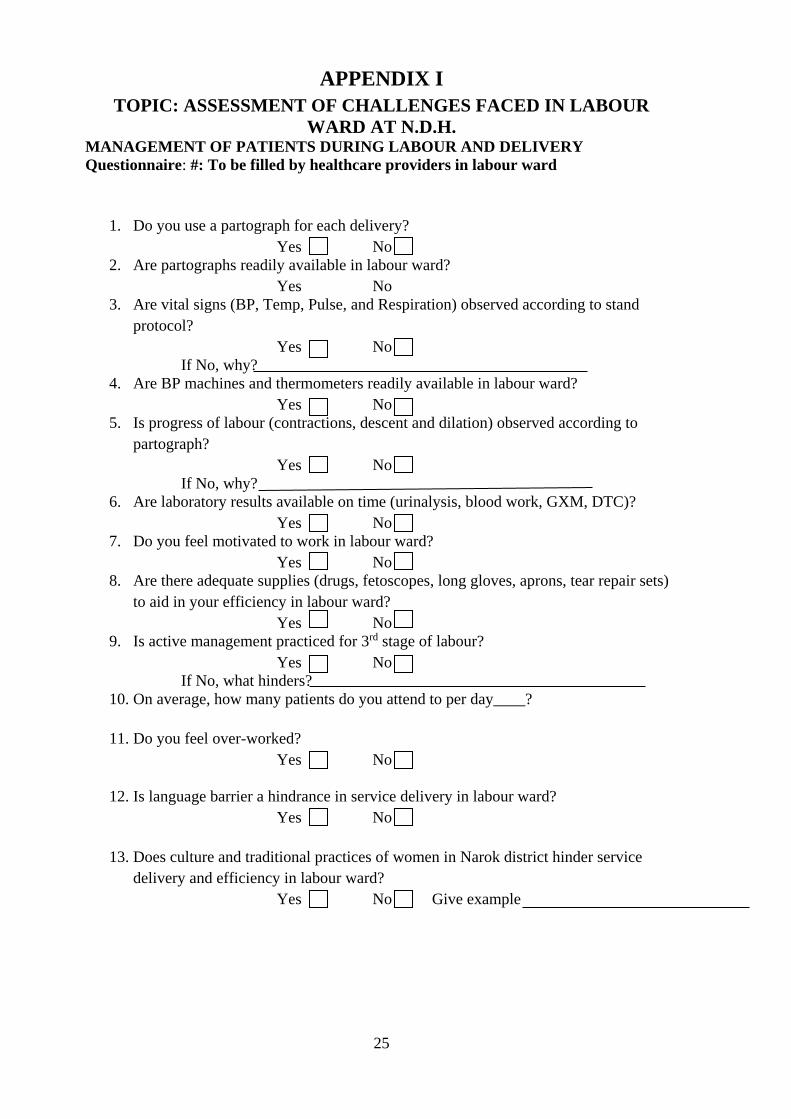
APPENDIX I
TOPIC: ASSESSMENT OF CHALLENGES FACED IN LABOUR
WARD AT N.D.H. MANAGEMENT OF PATIENTS DURING LABOUR AND DELIVERY
Questionnaire: #: To be filled by healthcare providers in labour ward
1. Do you use a partograph for each delivery?
Yes No
2. Are partographs readily available in labour ward?
Yes No
3. Are vital signs (BP, Temp, Pulse, and Respiration) observed according to stand
protocol?
Yes No
If No, why?
4. Are BP machines and thermometers readily available in labour ward?
Yes No
5. Is progress of labour (contractions, descent and dilation) observed according to
partograph?
Yes No
If No, why?
6. Are laboratory results available on time (urinalysis, blood work, GXM, DTC)?
Yes No
7. Do you feel motivated to work in labour ward?
Yes No
8. Are there adequate supplies (drugs, fetoscopes, long gloves, aprons, tear repair sets)
to aid in your efficiency in labour ward?
Yes No
9. Is active management practiced for 3rd stage of labour?
Yes No
If No, what hinders?
10. On average, how many patients do you attend to per day____?
11. Do you feel over-worked?
Yes No
12. Is language barrier a hindrance in service delivery in labour ward?
Yes No
13. Does culture and traditional practices of women in Narok district hinder service
delivery and efficiency in labour ward?
Yes No Give example

26
TOPIC: ASSESSMENT OF CHALLENGES FACED IN THE LABOUR
WARD AT NAROK DISTRICT HOSPITAL. Questionnaire: #: To be filled by patients in labour ward
PATIENTS SATISFACTION DURING LABOUR AND DELIVERY
Correspondent:
1. Name? Age? Address
2. What is your mother tongue?
3. Are you well versed in Kiswahili or English or both?
Kisw. Eng. Both
4. Is this your first delivery?
Yes No
Have you previously delivered at home?
Yes NO
If yes, what reason?
5. Did you face any challenges getting to hospital?
Yes No
If yes, state?
6. Once in maternity approximately how long did it take you before delivering___?
7. Were you able to access adequate pharmacological pain relief during labour?
Yes No
8. How do you rate services in labour ward: a) Expensive
b) Affordable
c) Cheap
9. How would you rate services rendered in labour ward: a) Excellent
b) Good
c) Fair
d) Poor
27
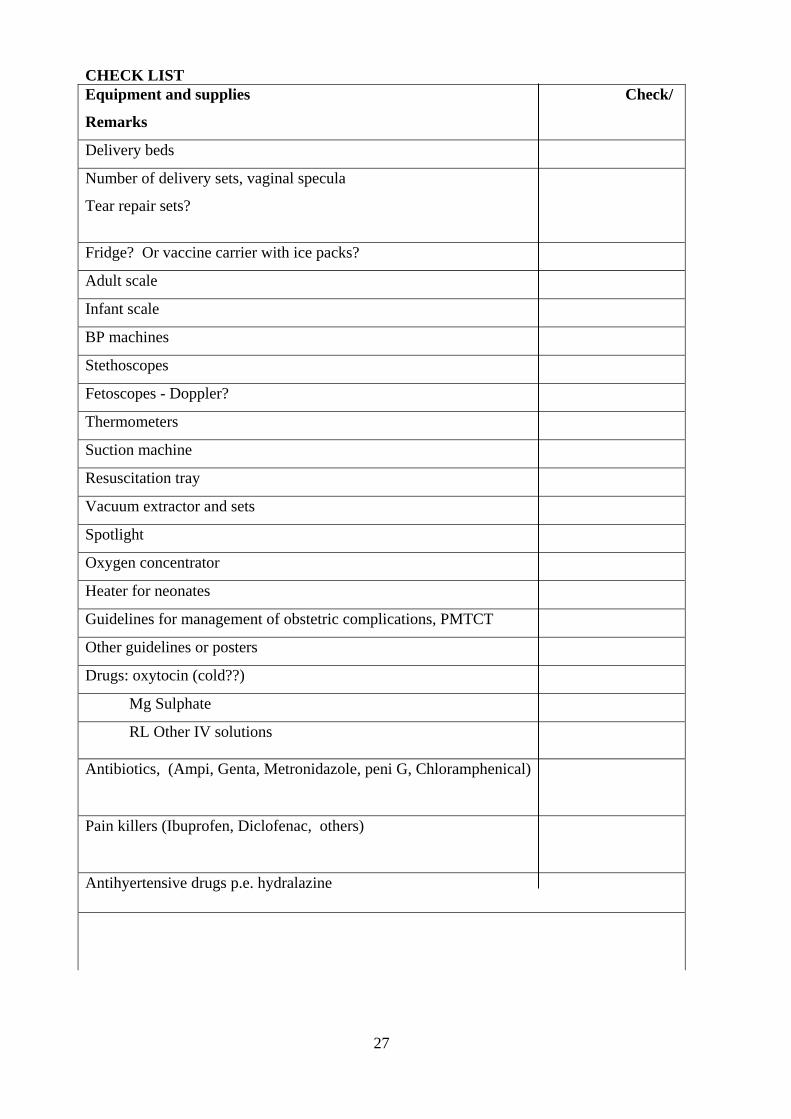
CHECK LIST
Equipment and supplies Check/
Remarks
Delivery beds
Number of delivery sets, vaginal specula
Tear repair sets?
Fridge? Or vaccine carrier with ice packs?
Adult scale
Infant scale
BP machines
Stethoscopes
Fetoscopes - Doppler?
Thermometers
Suction machine
Resuscitation tray
Vacuum extractor and sets
Spotlight
Oxygen concentrator
Heater for neonates
Guidelines for management of obstetric complications, PMTCT
Other guidelines or posters
Drugs: oxytocin (cold??)
Mg Sulphate
RL Other IV solutions
Antibiotics, (Ampi, Genta, Metronidazole, peni G, Chloramphenical)
Pain killers (Ibuprofen, Diclofenac, others)
Antihyertensive drugs p.e. hydralazine

28
Cleaning materials and disinfectant available Chlorine, 3 buckets
Skin disinfection of mothers?
Autoclave
Stove for boiling
Protective wear available? long gloves
Referral system in place?
How many? Why and where?

29
APPENDIX II
1.1 map of the DISTRICT: SHOWING the health services and facilities in the district

1