a simple technique for removal of recurring granular dystrophy in corneal grafts
TRANSCRIPT
A SIMPLE TECHNIQUE FOR REMOVAL O F RECURRING GRANULAR DYSTROPHY IN CORNEAL GRAFTS
S T E V E N L. L E M P E R T , M.D., MARK S. JENKINS, M.D., B R U C E L. JOHNSON, M.D., AND STUART I. B R O W N , M.D.
Pittsburgh, Pennsylvania
Three studies describing the light and electron microscopic appearance of seven regraft specimens have focused on recurrences of granular corneal dystrophy in grafted corneas.1'2'3 In one of the specimens, the recurrence appeared throughout the stroma. The recurrence of the dystrophy in the other six specimens was localized in an avascular fibrous tissue between the epithelium and Bowman's layer. We describe herein a quick, simple technique for the excision of the anterior opaque layer of tissue recurring in granular dystrophy in otherwise transparent corneal transplants.
SUBIECTS AND METHODS
In 1968, a 54-year-old man and his 15-year-old son each related a similar history of a slowly progressing decrease in visual acuity beginning at approximately 3 years of age. The left eye of the father had been destroyed in a concentration camp during World War II. The father's right eye had a visual acuity of finger counting at one foot, whereas the son had 6/30 (20/100) in each eye. The corneas of both patients had diffuse anterior stromal opacifications that did not involve the periphery and were characteristic of granular dystrophy. During that year, 7.5-mm partial-penetrating corneal transplants were performed on the right eye of the father and both eyes of the son. The grafts remained transparent, and the corrected visual acuities were 6/18 (20/60)
From the Department of Ophthalmology, University of Pittsburgh School of Medicine, and Eye and Ear Hospital', Pittsburgh, Pennsylvania.
Reprint requests to Stuart I. Brown, M.D., Department of Ophthalmology, Eye and Ear Hospital, 230 Lothrop Street, Pittsburgh, PA 15213.
in the father's eye and 6/12 (20/40) in each of the son's eyes. Light and electron microscopic examination of the corneas excised at surgery corroborated the clinical diagnosis.4
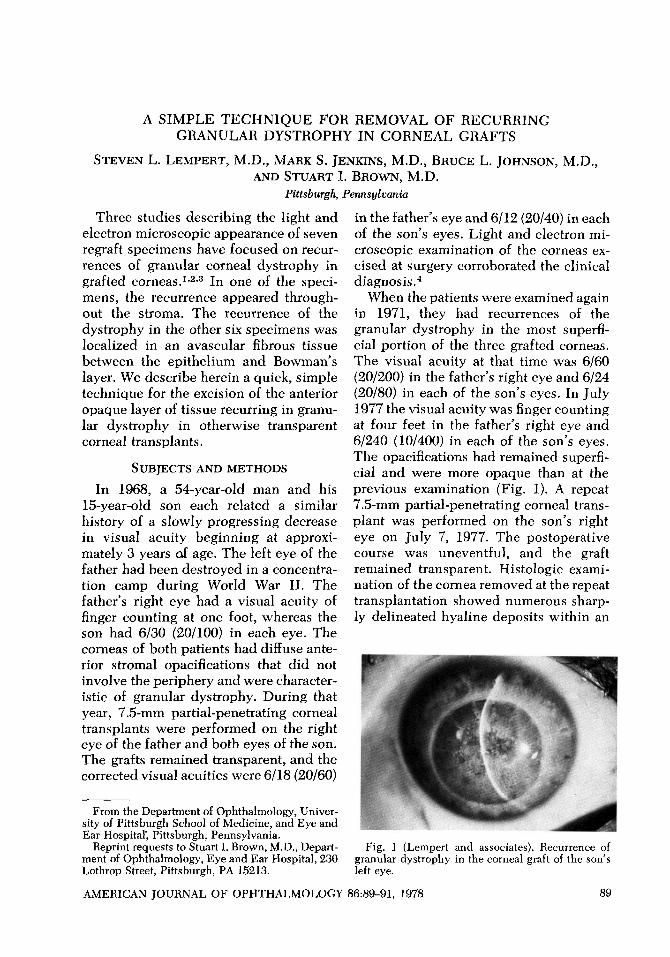
When the patients were examined again in 1971, they had recurrences of the granular dystrophy in the most superficial portion of the three grafted corneas. The visual acuity at that time was 6/60 (20/200) in the father's right eye and 6/24 (20/80) in each of the son's eyes. In July 1977 the visual acuity was finger counting at four feet in the father's right eye and 6/240 (10/400) in each of the son's eyes. The opacifications had remained superficial and were more opaque than at the previous examination (Fig. 1). A repeat 7.5-mm partial-penetrating corneal transplant was performed on the son's right eye on July 7, 1977. The postoperative course was uneventful, and the graft remained transparent. Histologic examination of the cornea removed at the repeat transplantation showed numerous sharply delineated hyaline deposits within an
Fig. 1 (Lempert and associates). Recurrence of granular dystrophy in the corneal graft of the son's left eye.
AMERICAN JOURNAL OF OPHTHALMOLOGY 86:89-91, 1978 89
90 AMERICAN JOURNAL OF OPHTHALMOLOGY JULY, 1978
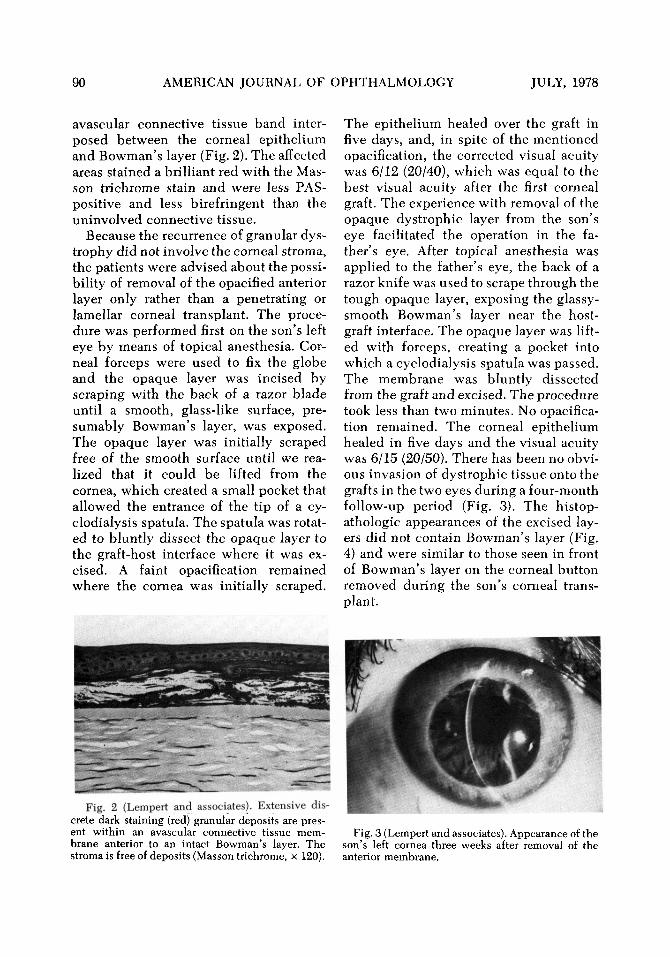
avascular connective tissue band interposed between the corneal epithelium and Bowman's layer (Fig. 2). The affected areas stained a brilliant red with the Mas-son trichrome stain and were less PAS-positive and less birefringent than the uninvolved connective tissue.
Because the recurrence of granular dystrophy did not involve the corneal stroma, the patients were advised about the possibility of removal of the opacified anterior layer only rather than a penetrating or lamellar corneal transplant. The procedure was performed first on the son's left eye by means of topical anesthesia. Corneal forceps were used to fix the globe and the opaque layer was incised by scraping with the back of a razor blade until a smooth, glass-like surface, presumably Bowman's layer, was exposed. The opaque layer was initially scraped free of the smooth surface until we realized that it could be lifted from the cornea, which created a small pocket that allowed the entrance of the tip of a cy-clodialysis spatula. The spatula was rotated to bluntly dissect the opaque layer to the graft-host interface where it was excised. A faint opacification remained where the cornea was initially scraped.
Fig. 2 (Lempert and associates). Extensive discrete dark staining (red) granular deposits are present within an avascular connective tissue membrane anterior to an intact Bowman's layer. The stroma is free of deposits (Masson trichrome, x 120).
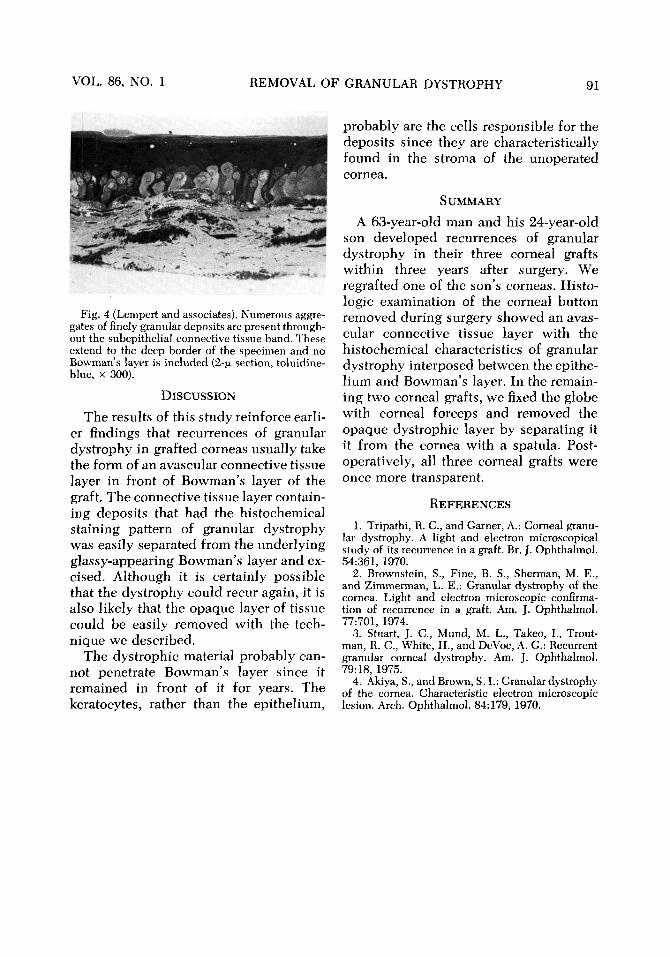
The epithelium healed over the graft in five days, and, in spite of the mentioned opacification, the corrected visual acuity was 6/12 (20/40), which was equal to the best visual acuity after the first corneal graft. The experience with removal of the opaque dystrophic layer from the son's eye facilitated the operation in the father's eye. After topical anesthesia was applied to the father's eye, the back of a razor knife was used to scrape through the tough opaque layer, exposing the glassy-smooth Bowman's layer near the host-graft interface. The opaque layer was lifted with forceps, creating a pocket into which a cyclodialysis spatula was passed. The membrane was bluntly dissected from the graft and excised. The procedure took less than two minutes. No opacification remained. The corneal epithelium healed in five days and the visual acuity was 6/15 (20/50). There has been no obvious invasion of dystrophic tissue onto the grafts in the two eyes during a four-month follow-up period (Fig. 3). The histop-athologic appearances of the excised layers did not contain Bowman's layer (Fig. 4) and were similar to those seen in front of Bowman's layer on the corneal button removed during the son's corneal transplant.
Fig. 3 (Lempert and associates). Appearance of the son's left cornea three weeks after removal of the anterior membrane.
VOL. 86, NO. 1 REMOVAL OF GRANULAR DYSTROPHY 91
Fig. 4 (Lempert and associates). Numerous aggregates of finely granular deposits are present throughout the subepithelial connective tissue band. These extend to the deep border of the specimen and no Bowman's layer is included (2-u. section, toluidine-blue, x 300).
DISCUSSION
The results of this study reinforce earlier findings that recurrences of granular dystrophy in grafted corneas usually take the form of an avascular connective tissue layer in front of Bowman's layer of the graft. The connective tissue layer containing deposits that had the histochemical staining pattern of granular dystrophy was easily separated from the underlying glassy-appearing Bowman's layer and excised. Although it is certainly possible that the dystrophy could recur again, it is also likely that the opaque layer of tissue could be easily removed with the technique we described.
The dystrophic material probably cannot penetrate Bowman's layer since it remained in front of it for years. The keratocytes, rather than the epithelium,
probably are the cells responsible for the deposits since they are characteristically found in the stroma of the unoperated cornea.
SUMMARY
A 63-year-old man and his 24-year-old son developed recurrences of granular dystrophy in their three corneal grafts within three years after surgery. We regrafted one of the son's corneas. Histo-logic examination of the corneal button removed during surgery showed an avascular connective tissue layer with the histochemical characteristics of granular dystrophy interposed between the epithelium and Bowman's layer. In the remaining two corneal grafts, we fixed the globe with corneal forceps and removed the opaque dystrophic layer by separating it it from the cornea with a spatula. Post-operatively, all three corneal grafts were once more transparent.
REFERENCES 1. Tripathi, R. C , and Garner, A.: Corneal granu
lar dystrophy. A light and electron microscopical study of its recurrence in a graft. Br. J. Ophthalmol. 54:361, 1970.
2. Brownstein, S., Fine, B. S., Sherman, M. E., and Zimmerman, L. E.: Granular dystrophy of the cornea. Light and electron microscopic confirmation of recurrence in a graft. Am. J. Ophthalmol. 77:701, 1974.
3. Stuart, J. C , Mund, M. L., Takeo, I., Trout-man, R. C., White, H., and DeVoe, A. G.: Recurrent granular corneal dystrophy. Am. J. Ophthalmol. 79:18, 1975.
4. Akiya, S., and Brown, S. I.: Granular dystrophy of the cornea. Characteristic electron microscopic lesion. Arch. Ophthalmol. 84:179, 1970.