a s rhinitis t o f o d eczema allergies (immune-mediated ... · tissue damage progresses with...
TRANSCRIPT

Adve
rse
reac
tions
to fo
od
Allergies(immune-mediated)
Rhinitis
Eczema
Asthma
Coeliac disease
Intolerances(non-immune)
Irritable bowel
Lactose intolerance
Phenylketonuria

DefinitionImmune response to dietary gluten Damage to proximal small intestine epithelium Malabsorption featuresResponds to gluten-free diet
Other NamesCoeliac sprueGluten-sensitive enteropathy

Prevalence0.5 to 1% among those of White European ancestry Most commonly 30-60y with peaks in infancy and in 50s
Abadie, V. et al., 2011

Morbidity

Patient perceptions Whitaker, J.K.H., et al., 2009
Complaint % reporting
Reduced enjoyment of food 68%
Food costs >£10 per week extra 46%
Food costs a problem 21%
Doing enjoyable things less often 54%
Regret not being diagnosed earlier 66%

MortalityMainly in undiagnosed and untreated Most mortality from malignancies Long-term survival when properly treated

€ -
€ 0.50
€ 1.00
€ 1.50
€ 2.00
€ 2.50
Bread Cereal Spagetti Flour Bakingpowder
Grocery prices (€ per 100g)
RegularGluten-free
Data: Coeliac Society of Ireland

£-
£100
£200
£300
£400
£500
Consultations Prescriptions
Annual healthcare costs to patient
ControlsCoeliac patients
Data: Violata, M. et al., 2012
PathogenesisImmune-mediated reaction to gluten in intestineMost people have no problem with glutenThus disease attributable mainly to host factors

Digestion, IngestionGluten is ingested in cereal grains (wheat, rye, barley).Gluten is digested by intestinal enzymes to amino acids andpeptides.A peptide, gliadin, remains, which cannot be degraded byregular enzymesGliadin is instead deamidated (has an amide group removed)by tissue transglutaminase (tTG).


APC Presentation, T cell responseDeamidated gliadin interacts with HLA DQ2 or HLA DQ8on antigen presenting cells (APCs).Deamidated gliadin is presented to CD4 T cells.CD4 T cells produce cytokines (such as IFNγ) which causetissue damage.


B cell responseT cells also elicit a B cell response.B cells produce the antibodies:
Anti-tissue transglutaminase (anti-tTG)Anti-deamidated gliadinAnti-endomysial antibody (anti-EMA)


IL-15, intraepithelial lymphocytesGliadin also induces IL-15 production from enterocytes.IL-15 activates and upregulates intraepithelial CD8lymphocytes.


MIC-A, NKG2DVarious stressors causes MIC-A to be expressed onenterocytes. Intraepithelial lymphocytes receive MIC-A via NKG2D in acytotoxic interaction, killing enterocytes.


ProgressionTissue damage progresses with villous atrophy and loss ofsurface area.Damage allows increased movement of gliadin across theepithelium, amplifying disease.An increased rate of mitosis is seen with reducedenterocyte differentiation and function.Tissue damage, loss of surface area, and reduced functionresult in malabsorption.


Clinical featuresMany atypicalpresentations, often anincidental finding
Presentations mostcommonly 30-60y, butany agePeaks in infancy and 50s
No gender difference, but2-3x more womendetected
menstrual blood losspotentiates anaemia
<10 10-20 20-30 30-40 40-50 50-60 60-70 70-80 80-90
Age at diagnosis (illustrative data)
Female Male

Disease associationsImmune diseases andatopy:
Diabetes mellitus type 1ThyroiditisSjögren syndrome
Other diseases:EpilepsyIgA nephropathyDown syndromeTurner syndrome

Symptoms

Malabsorption-related symptomsManifestation Malabsorbed nutrient
Steatorrhoea Fats
Diarrhoea Fats, carbohydrates
Manifestation Deficiency
Weight loss, wasting Fats, proteins, carbs
Anaemia Iron, vit B12, folic acid
Paraesthesia, tetany Calcium, vit D
Osteoporosis, arthritis Calcium, vit D
Bleeding, bruising Vit K
Oedema Protein
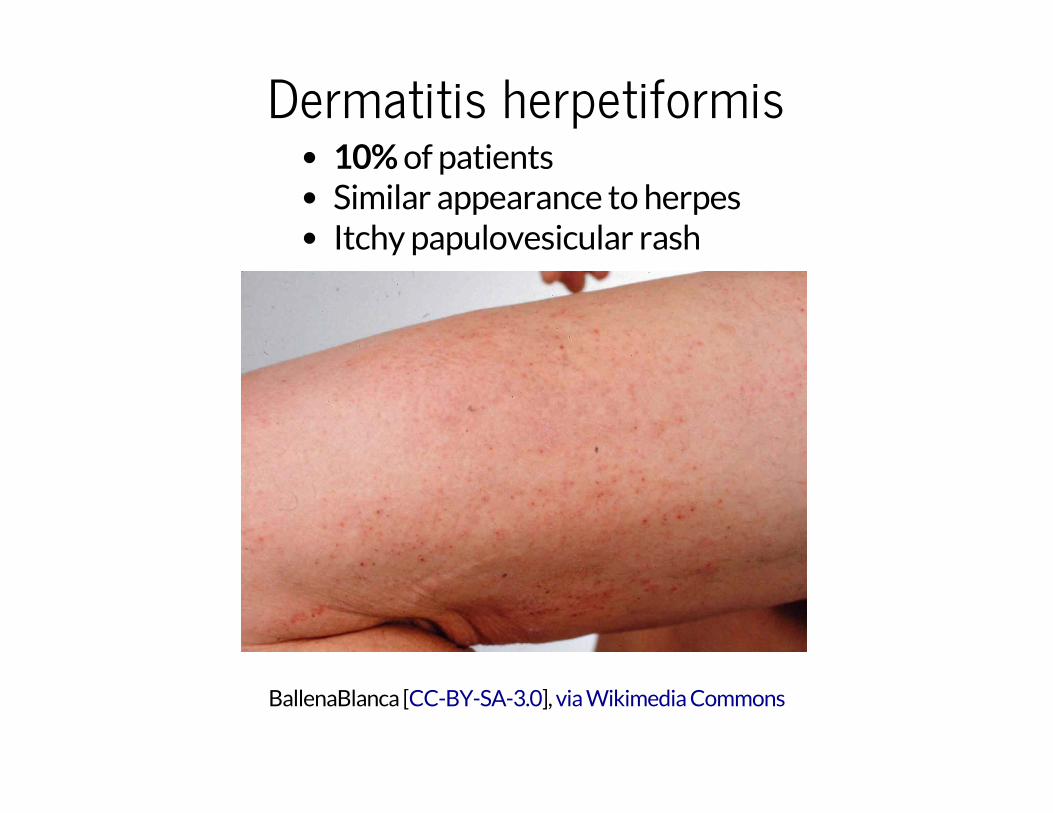
Dermatitis herpetiformis10% of patientsSimilar appearance to herpesItchy papulovesicular rash
BallenaBlanca [ ], CC-BY-SA-3.0 via Wikimedia Commons

PaediatricClassical:
6-24 monthsIrritabilityAbdominal distension, diarrhoeaAnorexia, weight loss, failure to thriveMuscle wasting
Non-classical:Older agesAbdominal pain, nausea, vomitingBloating, constipation

SignsFew and non-specific
Anaemiatachycardiapallor
Bruising (vit K deficiency)Hyperactive bowel soundsNeurological signsOedema (severe cases)

HLA DQ2, HLA DQ895% of patients have at least oneaccounts for 50% of genetic component
Abadie, V. et al., 2011

Other risk factorsOther immune system polymorphisms:
e.g. IL-2, IL-21
Other ill-defined genetic components:10-15% of 1st degree relatives (may be clinically silent)70% monozygotic twin concordance
Breast feeding and gluten introduction ages significantInfant rotavirus infection

SerologyConduct non-invasive serology before biopsyAlso for dietary compliance monitoring2.5% of coeliac patients have IgA deficiency
Verify normal levelsInvestigate IgG if IgA deficient
IgA anti-tTG + sensitive
IgA or IgG anti-demanidated gliadin
+ sensitive
Anti-EMA ++ specific, - sensitive
HLA DQ2/DQ8 cannot confirmdiagnosishelps exclude diagnosisif negative

BiopsySmall bowel endoscopicbiopsy'Gold standard', but notalways necessary in clear-cutcases with serologyNot specific, other causes,need serology also
Histology:Sub-total villous atrophyIncrease in lamina propria,lymphocytes, plasma cells,mast cells and eosinophils

Acute complicationsMostly rareAnecdotal intestinal obstructions and perforations
Coeliac crisis acute, fulminant worsening of symptomsoften with a gluten challengehypoproteinaemia, oedemasevere diarrhoeadehydration, electrolyte imbalancemetabolic acidosishospitalisation, fluid replacement, corticosteroids

Chronic complicationsRefractory coeliac disease (RCD)
improvement with diet, then loss of responseincreased complications (malignancy), poor prognosis
Malignancy riskEnteropathy-assoc. T cell lymphomaSmall intestinal adenocarcinoma

Chronic complicationsUlcerative jejunitisAnaemiaFemale infertilityOsteoporosis (even when on strict diet)Malnutrition, cachexiaParaesthesia, ataxia, muscle weaknessSplenic atrophy
need pneumococcal vaccinations

TreatedInitial supplementation of mineral and vitamin body stores
Gluten-free dietImprovement in symptoms within days/weeksImprovement in morphology after monthsLong-term survival, unrelated mortalityChallenging and costly to maintain
Long-term risk of small intestinal and oesophageal malignancy

UntreatedPoor compliance relatively common
Elaboration of malabsorption featuresSevere diarrhoea
dehydration, electrolyte imbalancesOsteoporosisMalignancyNeurological, psychiatric complications
Childrengrowth retardationshort stature
Pregnancymiscarriagecongenital malformations