a review of colonic volvulus - · pdf filea review of colonic volvulus a ... sigmoid colon...
TRANSCRIPT

PRACTICAL GASTROENTEROLOGY • SEPTEMBER 200942
A Review of Colonic Volvulus
A68-year-old man presented to the emergencydepartment with abdominal pain. His pain had beenpresent for one day. His last bowel movement was
three days ago and he had passed no flatus in 24 hours.He had a history of chronic constipation, diabetes melli-tus, hypertension, and bipolar disorder. He had undergonean appendectomy and cholecystectomy several years ago.On physical exam, the patient had a temperature of100.2°F. His abdomen was distended, tympanitic, andtender to palpation in all quadrants. Rectal exam was neg-ative for stool, blood, or palpable mass. WBC count was11,000 per cubic millimeter and lactate level was normal.Abdominal x-ray demonstrated a distended and ahaustralsigmoid colon with a maximal diameter of 14 cm sug-gestive of a sigmoid volvulus (Figure 1). Urgent flexiblesigmoidoscopy was performed in the emergency depart-ment. A spiral area of colonic mucosa was visualized 20cm from the anal verge. The scope was advanced withgentle pressure and a sudden expulsion of gas andstraightening of the colon was achieved consistent withvolvulus detorsion. The sigmoid mucosa appeared viablewith no evidence of necrosis. A rectal tube was placed,and a sigmoidectomy was performed on the fifth hospitalday. The patient had an uneventful hospital course andwas discharged on the tenth hospital day.
COLONIC VOLVULUS—INTRODUCTION AND EPIDEMIOLOGYColonic volvulus (Latin, volvere, to roll or turn) is theaxial twisting of the colon on its vascular pedicle. The
result is partial or complete obstruction of the bowellumen with a variable degree of perfusion impairment.The sigmoid colon and cecum are the most frequent sitesof colonic volvulus, accounting for about 75% and 22%of all cases (1). Rare sites of colonic volvulus include thetransverse colon (2%) and the splenic flexure (<1%). Arare variant of sigmoid volvulus is an ileosigmoid knot,which occurs when the ileum encircles the sigmoidcolon leading to a sigmoid torsion and potential strangu-lation (2). Although the term cecal volvulus is ingrainedin the literature, true volvulus of the cecum rarely occurs.The condition is more accurately referred to as cecocolicvolvulus consisting of an axial rotation of the terminalileum, cecum, and ascending colon with concomitanttwisting of the associated mesentery. A less common but
A CASE REPORT
Adam Spiegel, D.O., Gastroenterology Fellow, Divisionof Gastroenterology and Hepatobiliary Disease, NewYork Medical College, Valhalla, NY. Tarun Chugh,M.D,, Internal Medicine Resident, Department of Inter-nal Medicine, New York Medical College, Valhalla, NY.Edward Lebovics, M.D.,Professor of Clinic Medicine,Division of Gastroenterology and Hepatobiliary Dis-ease, New York Medical College, Valhalla, NY.
by Adam Spiegel, Tarun Chugh, Edward Lebovics
Figure 1. Abdominal radiograph demonstrating a sigmoid volvulus
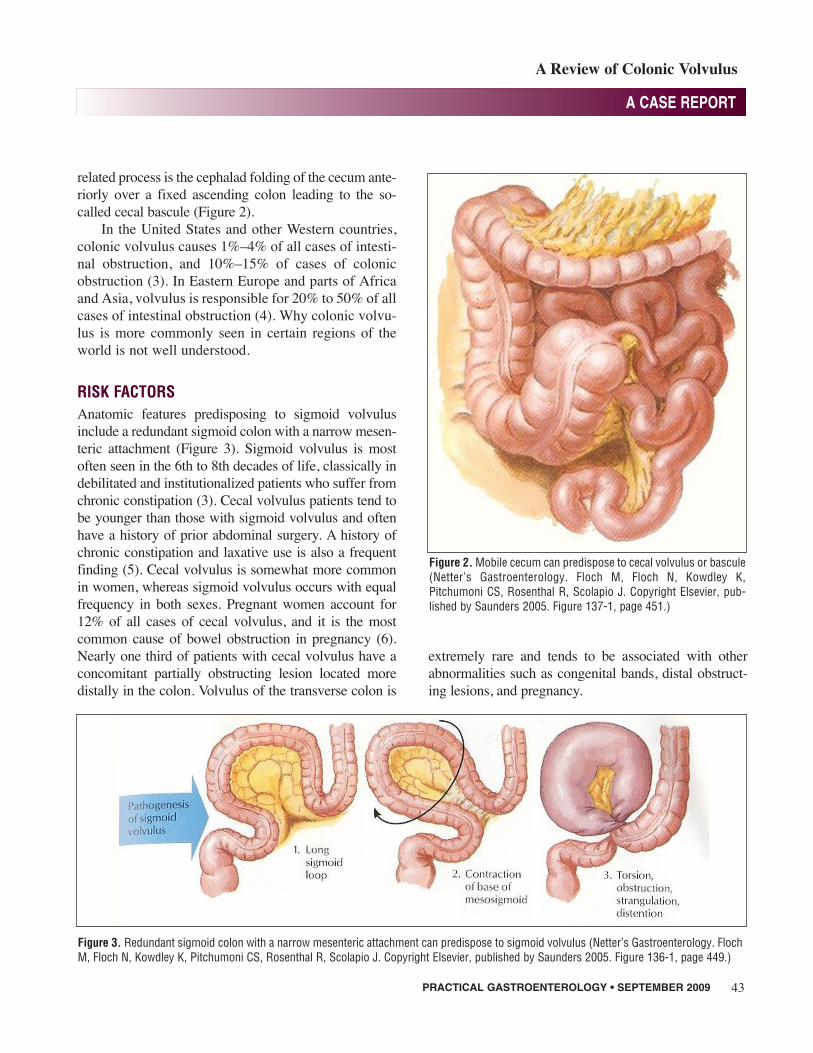
related process is the cephalad folding of the cecum ante-riorly over a fixed ascending colon leading to the so-called cecal bascule (Figure 2).
In the United States and other Western countries,colonic volvulus causes 1%–4% of all cases of intesti-nal obstruction, and 10%–15% of cases of colonicobstruction (3). In Eastern Europe and parts of Africaand Asia, volvulus is responsible for 20% to 50% of allcases of intestinal obstruction (4). Why colonic volvu-lus is more commonly seen in certain regions of theworld is not well understood.
RISK FACTORSAnatomic features predisposing to sigmoid volvulusinclude a redundant sigmoid colon with a narrow mesen-teric attachment (Figure 3). Sigmoid volvulus is mostoften seen in the 6th to 8th decades of life, classically indebilitated and institutionalized patients who suffer fromchronic constipation (3). Cecal volvulus patients tend tobe younger than those with sigmoid volvulus and oftenhave a history of prior abdominal surgery. A history ofchronic constipation and laxative use is also a frequentfinding (5). Cecal volvulus is somewhat more commonin women, whereas sigmoid volvulus occurs with equalfrequency in both sexes. Pregnant women account for12% of all cases of cecal volvulus, and it is the mostcommon cause of bowel obstruction in pregnancy (6).Nearly one third of patients with cecal volvulus have aconcomitant partially obstructing lesion located moredistally in the colon. Volvulus of the transverse colon is
extremely rare and tends to be associated with otherabnormalities such as congenital bands, distal obstruct-ing lesions, and pregnancy.
PRACTICAL GASTROENTEROLOGY • SEPTEMBER 2009 43
A CASE REPORT
A Review of Colonic Volvulus
Figure 2. Mobile cecum can predispose to cecal volvulus or bascule(Netter’s Gastroenterology. Floch M, Floch N, Kowdley K, Pitchumoni CS, Rosenthal R, Scolapio J. Copyright Elsevier, pub-lished by Saunders 2005. Figure 137-1, page 451.)
Figure 3. Redundant sigmoid colon with a narrow mesenteric attachment can predispose to sigmoid volvulus (Netter’s Gastroenterology. FlochM, Floch N, Kowdley K, Pitchumoni CS, Rosenthal R, Scolapio J. Copyright Elsevier, published by Saunders 2005. Figure 136-1, page 449.)

PRACTICAL GASTROENTEROLOGY • SEPTEMBER 200944
A CASE REPORT
A Review of Colonic Volvulus
CLINICAL MANIFESTATIONSThe majority of patients with colonic volvulus presentwith abdominal pain, nausea, vomiting, obstipation,and a diffusely distended abdomen. The pain is usuallyconstant with a superimposed colicky component.Cecal bascule manifests clinically with intermittentbouts of abdominal pain due to isolated cecal obstruc-tion with subsequent spontaneous relief as the cecumunfolds back into normal position. Manifestations ofcolonic volvulus may not be as apparent in elderlypatients or in those with neurologic disease (7). Fever,peritonitis, sepsis, and/or leukocytosis should raise thesuspicion of intestinal gangrene.
DIAGNOSISThe diagnosis of colonic volvulus can be made withabdominal radiographs alone in as many as 85% ofcases. Sigmoid volvulus classically appears as amarkedly distended ahaustral sigmoid loop (i.e., “bentinner-tube” appearance), the apex of which is oftendirected toward the patient’s right shoulder (8) (Figure
1). In equivocal cases of sigmoid volvulus, a water sol-uble contrast enema may be helpful by demonstratinga point of torsion (i.e., a spiral pattern or “birds beaksign”) (Figure 4).
Classic radiologic features of cecal volvulusinclude a massively dilated cecum located in the epi-gastrium or left upper quadrant (Figure 5), a coffee-bean appearance of the distended cecum (“coffee-beansign”) (Figure 6), and a single long air-fluid level onupright films (1) (Figure 7). A CT scan may demon-strate a whirl pattern, secondary to dilation of thecolon around its mesentery (9).
MANAGEMENTThe initial management of patients with colonic volvulusincludes restoration of intravascular volume, correctionof electrolyte abnormalities, nasogastric suction, analge-sia, and consideration of broad spectrum intravenousantibiotics. Urgent endoscopic decompression should beperformed for sigmoid volvulus without evidence of
(continued on page 46)
Figure 4. Point of torsion due to sigmoidvolvulus highlighted by contrast enema(Sleisenger and Fordtran’s Gastrointestinaland Liver Disease: Pathophysiology, Diagno-sis, Management. Feldman M, Friedman LS,Brandt LJ Editors. Publisher: Saunders; 8thedition, July 21, 2006. Figure 116-17, page2670)
Figure 5. Dilated cecum in a cecal volvulus(Sleisenger and Fordtran’s Gastrointestinaland Liver Disease: Pathophysiology, Diag-nosis, Management. Feldman M, FriedmanLS, Brandt LJ Editors. Publisher: Saunders;8th edition, July 21, 2006. Figure 116-16,page 2669)
Figure 6. “Coffee-bean sign” in a cecalvolvulus http://www.radpod.org/2007/07/03/caecal-volvulus-2/. Perret RS, KunbergerLE: Case 4: Cecal volvulus. Am J Roentgenol,1998 Sep; 171(3): 855, 859, 860.

PRACTICAL GASTROENTEROLOGY • SEPTEMBER 200946
A CASE REPORT
A Review of Colonic Volvulus
intestinal gangrene. Two large series reported successfulproctoscopic decompression of sigmoid volvulus in 83%and 93% of patients (10,11). In addition to restoringcolonic perfusion, sigmoidoscopy also provides anassessment of colonic mucosal viability. Completecolonoscopy should be avoided in the emergent settingsecondary to the risk of perforation of the distended andunprepped bowel (12). If endoscopic detorsion of thevolvulus cannot be accomplished, urgent laparotomywith sigmoid resection is required. Endoscopic reductionof a sigmoid volvulus is associated with a recurrence rateof 25% to 50%, which can occur hours to weeks afterdetorsion (13). Placement of a soft rectal tube after detor-sion can reduce the potential for early recurrence (14).Subsequent recurrence is prevented via elective sigmoidresection with either primary colorectal anastomosis, orin medically compromised patients, end colostomy.Recurrence with this approach is around 3% to 6% (14).Case reports of percutaneous endoscopic sigmoidopexyto prevent recurrence in poor surgical candidates have
shown positive results (15). Colonoscopy prior to elec-tive sigmoid resection is important to exclude an associ-ated neoplasm.
Colonoscopy has been utilized in case reports tosuccessfully reduce a cecal volvulus; however, there issubstantial risk of perforating the thin and oftenischemic cecum (12). Hence, the mainstay of cecalvolvulus treatment is operative. Management optionsinclude cecopexy, cecostomy, and colonic resection.Right colectomy with primary ileo-transverse anasto-mosis effectively prevents recurrence and is the proce-dure of choice for most surgeons (1).
The overall mortality rate for patients with colonicvolvulus is about 8% to 14% (1). The major predictorof death is the presence of gangrenous bowel (3). Afterdiagnosing a colonic volvulus, the primary goals oftreatment are to urgently prevent the development of bowel ischemia, and to prevent volvulus recurrenceby ultimately correcting the underlying anatomicabnormality. n
References1. Ballantyne GH, Brandner MD, Beart Jr RW, et al. Volvulus of the
colon: incidence and mortality. Ann Surg, 1985; 202:83.2. VerSteeg KR, Whitehead WA. Ileosigmoid knot. Arch Surg,
1980;115:761.3. Grossmann EM, Longo WE, Stratton MD, et al. Sigmoid volvu-
lus in Department of Veterans Affairs Medical Centers. DisColon Rectum, 2000;43:414-418.
4. Udezue NO. Sigmoid volvulus in Kaduna, Nigeria. Dis ColonRectum, 1990;33:647.
5. Haskin PH, Teplick SK, Teplick JG, et al. Volvulus of the cecumand right colon. JAMA, 1981;245:2433.
6. John H, Gyr T, Giudici G, et al. Cecal volvulus in pregnancy.Case report and review of literature. Arch Gynecol Obstet,1996;258:161.
7. Avots-Avotins KV, Waugh DE. Colon volvulus and the geriatricpatient. Surg Clin North Am, 1982;62:249.
8. Agrez M, Cameron D. Radiology of sigmoid volvulus. Dis ColonRectum, 1981; 24:510.
9. Catalano O. Computed tomographic appearance of sigmoidvolvulus. Abdom Imag, 1996;21:314.
10. Grossmann EM, Longo WE, Stratton MD, et al. Sigmoid volvu-lus in Department of Veterans Affairs Medical Centers. DisColon Rectum, 2000; 43:414.
11. Arnold GJ, Nance FC. Volvulus of the sigmoid colon. Ann Surg,1973;177:527.
12. Brothers TE, Strodel WE, Eckhauser F. Endoscopy in colonicvolvulus. Ann Surg, 1987; 206:1.
13. Bak MP, Boley SJ. Volvulus in elderly patients. Am J Surg,1986;151:71-75.
14. Ballantyne GH. Review of sigmoid volvulus: history and resultsof treatment. Dis Colon Rectum, 1982; 25:494.
15. Pinedo G, Kirberg A. Percutaneous Endoscopic Sigmoidopexy inSigmoid Volvulus with T-Fasteners. Dis Colon Rectum,2001;44:1867-1870.
(continued from page 44)
Figure 7. Single long air-fluid level in a cecal volvulus (Sleisengerand Fordtran’s Gastrointestinal and Liver Disease: Pathophysiology,Diagnosis, Management. Feldman M, Friedman LS, Brandt LJ Editors. Publisher: Saunders; 8th edition, July 21, 2006. Figure116-16, page 2669