a randomized trial comparing peak expiratory flow versus symptom self-management plans for children...
TRANSCRIPT

PEDIATRIC ASTHMA, ALLERGY & IMMUNOLOGYVolume 17, Number 3, 2004© Mary Ann Liebert, Inc.
A Randomized Trial Comparing Peak Expiratory FlowVersus Symptom Self-Management Plans for Children
with Persistent Asthma*
K.L. LETZ, N.D.,1,2 A.R. SCHLIE, B.A.,2 and W.L. SMITS, M.D.2
ABSTRACT
The aim of this study was to investigate the utility of peak flow meter based asthma actionplans versus symptom based asthma action plans in children 6–12 years old diagnosed withpersistent asthma. Fifty children diagnosed with mild to severe persistent asthma were ran-domly selected to receive a peak flow meter-based asthma action plan or a symptom-basedasthma action plan. Participants were followed for 3 months to evaluate the number of timesthe asthma action plan was used, the steps taken, the number of systemic corticosteroidbursts received, the number of acute care visits, and the number of telephone calls made tothe health-care provider. The data were analyzed and compared between the two equal-sizedaction plan groups. The two treatment groups did not differ in terms of their need for ur-gent treatment or for admissions to a hospital for asthma in the 3-month study period. Groupswere also similar regarding the need for systemic corticosteroid treatment for asthma ex-acerbations. Subjects in the symptom group utilized the action plan step an average of 0.75times, whereas subjects in the peak flow meter group averaged 0.25 times. The symptomgroup averaged 0.42 phone calls per patient to the clinic during the 3-month period, whereasthe peak flow group averaged 0.75 calls per patient. Although all asthmatic children andtheir parents should receive an asthma action plan, there appear to be no clear advantagesfor a peak flow meter-based action plan versus one that is symptom based.
INTRODUCTION
ASTHMA REMAINS THE MOST COMMON chronic disease of childhood, affecting nearly six million children.1
Asthma hospitalization rates have been the highest among children,1 and the number of both diagnosedand hospitalized continues to rise. Childhood asthma is also one of the leading causes of school absence2
and one of the top five diagnoses seen by the primary care practitioner in the office setting. Currently, theNational Institutes of Health3 defines asthma as “a chronic inflammatory disorder of the airways in whichmany cells and cellular elements play a role, in particular, mast cells, eosinophils, T lymphocytes, neu-trophils, and epithelial cells.” More concisely, asthma is a chronic inflammatory process of the airwaysleading to bronchoconstriction and decreased air exchange.
177
1Department of Graduate Nursing, Online Faculty, University of Phoenix, Phoenix, AZ 85040.2The Allergy & Asthma Center, Fort Wayne, IN 46804.*This project was partially funded by a grant from the American Academy of Nurse Practitioners.
5255_e08_p177-190 10/7/04 1:13 PM Page 177

The increasing problem of childhood asthma can not be fully understood, but possible causes may in-clude a rise in indoor and outdoor allergens, or perhaps, as a result of under treatment of asthma both bypatients and health-care providers. New guidelines emphasize the early recognition and aggressive treat-ment of asthma to control irreversible lung damage potentially through airway remodeling and decrease themorbidity and mortality of asthma.3 Asthma is a serious disease and can be fatal even in patients with mildasthma.4 Asthma is frequently characterized by its episodic symptoms and exacerbations. As a result, mon-itoring such events is critical in the care of an asthmatic patient with the intent of early detection and day-to-day control of chronic persistent asthma.
The best way to assess and monitor asthma in primary care has yet to be resolved; however, it is criti-cal due to the vast burden the illness has caused. The National Heart, Lung, & Blood Institute5 recom-mendations for the home management of asthma exacerbations include: (1) following a written asthma ac-tion plan with information of what to do at home, when to call a provider, and when to seek urgent care;(2) use of peak flow meters for children 5 years and older to assess the severity of an exacerbation as wellas to monitor response to therapy; (3) initiation of bronchodilators; (4) initiation of oral corticosteroids foran incomplete bronchodilator response; and (5) communication with the child’s health-care provider aboutmajor changes in symptoms or peak flow readings.
Background and significance
Studies have shown that estimates of the degree of airflow obstruction, by asthma patients as well asphysicians, are incorrect greater than 50% of the time.6 The inaccurate perception of the degree of airwayobstruction may be responsible for the morbidity and mortality of asthma related to delays in seeking med-ical attention and poor adherence with treatment regimens leading to under-treatment of the disease.7 Sev-eral studies have revealed that persons with a history of life-threatening events related to an asthma exac-erbation or persons identified with more severe obstructive disease, and thus at greater risk for asthmamorbidity, have a poor perception of the degree of airway obstruction8 and are more likely to fail to per-ceive changes in airway tone.9
Pulmonary function testing, or spirometry, has been advocated to give the clinician and patient an ob-jective measurement of airflow obstruction in persons with asthma to better classify the severity of theirdisease and amount of airway obstruction occurring. Spirometry can be attempted in persons greater than4 years of age to obtain sound readings.3 The most frequently used spirometry indicators to measure asthmainvolvement and degree of airway obstruction are forced expiratory volume in 1 second (FEV1) and peakexpiratory flow rate (PEFR). FEV1 can be defined as the maximal amount of vital capacity expressed in 1second of time. PEFR is the largest amount of expiratory flow achieved with a maximally forced effort.Subsequently, it should be noted that both FEV1 and PEFR measurements are dependent upon the effort ofthe individual patient; therefore, the PEFR may appear normal while the forced expiratory flow at 25–75%of vital capacity (FEF25–75%) is reduced. Airway obstruction is indicated by reductions in both of these read-ings when compared to predicted values. It should also be noted that reduction of FEV1 and PEFR from apatient’s “personal best” is also a valid indicator of increased airway obstruction. Reversible airway ob-struction noted when there is significant improvement (�15%) in these readings after bronchodilator useor a significant decrease (�20%) in readings after methacholine or exercise challenge is indicative of asthma.
Most asthma experts favor the use of FEV1 as the standard for functional assessment of airway obstruc-tion due to less intrasubject variability and better reflection of overall airway caliber than PEFR. The cor-relation between FEV1 and PEFR is not always sound, with variation of up to 30% that could result in un-recognized airway obstruction.10,11 Portable, low-cost devices to measure FEV1 remain largely unavailable,with only one company producing a small unit in the $25 range, hence the widespread use of peak flowmeters. Peak flow meters are portable plastic devices that allow patients and clinicians to measure PEFRwithout substantial time involvement or training (Figure 1). PEFR measurements using peak flow metersare easily obtained by the patient. Peak flow meters also require limited instruction and education on theiruse and no practitioner involvement. Peak flow meter use among children, however, requires direct obser-vation, intense training, and involvement of parents and/or caregivers.
Peak flow readings have become the most frequently employed tool for measuring lung function in thepatient with asthma both at home and often in the office setting. The cost of spirometers, time involvement,
LETZ ET AL.
178
5255_e08_p177-190 10/7/04 1:13 PM Page 178

and clinician’s inability to interpret their results hinder their usage in many primary-care practices. Researchstudies with new medications and medication delivery devices have often used the changes in peak flowreadings to justify the efficacy of such treatments and devices. All the recent published guidelines recom-mend daily peak flow readings to be performed on selected groups of patients.3,5,12,13 Experts believe thatthe use of peak flow meters enables a patient to recognize changes in lung function before symptoms de-velop and thus enables the patient and practitioner to make changes in the treatment plan sooner. The di-agnosis of asthma should be established objectively with the use of spirometry devices either in the hospi-tal setting or in health providers’ offices capable of performing such tests. Peak flow meters are designedand recommended for use in monitoring the severity of asthma only and not for use as a diagnostic tool.3
ASTHMA MANAGEMENT PLANS
179
FIG. 1. Symptom Asthma Action Plan.
5255_e08_p177-190 10/7/04 1:13 PM Page 179

Asthma management in children is unique because children are often poor perceivers of their asthmaseverity and they are less likely to communicate their difficulties. Thus, it becomes even more importantto obtain an objective measurement of their lung function. Peak flow meters may be the answer to take the“guess work” out of estimating the stability of their asthma. These inexpensive hand-held peak flow de-vices are widely available to clinicians and patients. Is it feasible to expect children to use peak flow me-ters at home on a consistent basis with the proper technique and maximum effort? Studies investigating thevalue of peak flow use in the adult population have not established these devices as reliable indicators ofairway obstruction and have barely touched on other important aspects of their use, including adherence,reliability of documented results, and the quality of different peak flow meter devices.
Literature review
It is well known that poor adherence with asthma medications is widespread, with even the most con-servative estimates recording adherence14,15 at only about 50%. Researchers have found appreciable dis-crepancies between self-reported and objective measures of medication adherence when adherence wasrecorded electronically.16,17 Medication adherence represents only a part of the patient’s role in the man-agement of asthma, but gives at least a thumbnail picture of the obstacles in managing asthma. Adherencedefined by Haynes18 is the extent to which a person’s behavior—in terms of taking medications, followinga recommended diet, or executing lifestyle changes—coincides with medical health-care advice. Multiplestrategies have been suggested to help patients comply with prescribed treatment regimens, including pa-tient education about the disease entity and its recommended treatment, jointly developing treatment goalswith the patient, frequent follow-up by health-care providers to monitor adherence, simplification of thetreatment program, and teaching self-management and providing the patient with tools for self-manage-ment. Significant progress in the development and assessment of asthma self-management programs hasbeen made in the past decade as asthma has become nearly epidemic. The goal of asthma self-managementis two-fold: to teach patients to assume more responsibility for managing their disorder and to identify andtreat exacerbations early, thus avoiding unnecessary acute care visits. Self-management programs allow pa-tient and provider to establish a partnership for controlling asthma.
Most self-management programs developed for patients with asthma allow decision-making and actionto occur without provider involvement. To assist patients in making such decisions, the “asthma action plan”has been developed as a framework for patients to follow. Asthma action plans are usually based on a “traf-fic light” approach based on peak flow meter readings or symptoms. The colors of the stoplight representsteps to be taken by the asthma patient. The color green represents stable asthma and suggests that usualdaily treatment be followed, including avoidance of triggers and administration of preventative medicationssuch as inhaled steroids. The color yellow represents the second stage of the asthma action plan and thebeginning of an asthma exacerbation. The second step, or “yellow zone” as it is often called, recommendsdoubling the daily dosage of inhaled steroid and every 4-hour usage of a bronchodilator for 2 days. Thecolor red or “red zone” represents the last step of the asthma action plan and a full-fledged asthma exac-erbation. The last step recommends that the patient present to the emergency department, call their health-care provider, or, in some cases, start a burst of oral corticosteroids at home.
Theoretically, the use of peak flow meters in the home environment makes good sense, and thus explainsthe probable reason for such strong recommendations by most asthma management guidelines. Peak flowmeasurement would allow the patient to detect asymptomatic deterioration in lung function, the responseto self-initiated therapy, and the need to seek medical intervention.12 A comprehensive review of literaturerelated to peak flow use does not demonstrate its usefulness, however, due to documented poor adherence,lack of evidence to support the accuracy of such devices in reflecting airway inflammation, lack of demon-strated benefit of peak expiratory flow (PEF) plans over symptom-driven plans, and lack of studies show-ing a decrease in mortality with PEFR monitoring.
Purpose
Despite the overwhelming expert recommendations for the use of peak flow meters at home, there is lim-ited clinical support for the benefits or usefulness in doing so. There have been a limited number of ran-
LETZ ET AL.
180
5255_e08_p177-190 10/7/04 1:13 PM Page 180

domized studies specifically addressing the usefulness of peak flow meters. The purpose of this study is tocompare peak expiratory flow versus symptom self-management plans for children with persistent asthma.A small number of studies have investigated the use of peak flow meters in asthmatic children both in thehome and office setting. More research is needed to define the utility of peak flow meter usage among thepediatric population, especially in the home environment, because this is now being strongly encouragedby many experts and insurance agencies.
Research questions/hypothesis
The objective of this study was to determine if children and parents use asthma action plans based onPEFR readings more than action plans based on symptoms, and whether there are differences in the num-ber of acute exacerbations and number of visits to health-care providers between the two groups. The pri-mary hypothesis of this study is that children and parents using symptom-based asthma action plans willbe more likely to implement medication adjustments without practitioner support than children and parentsfollowing a PEFR-based plan. Subsequently, the secondary hypothesis is that there will be no differencesin acute exacerbations, visits, or phone calls between those patients utilizing PEFR and those using actionplans.
METHODS
Setting population
The setting of this study is an allergy, asthma, and immunology clinic that cares for a mixed populationof children and adults who live in a Midwest suburban town and the surrounding area. The majority of thepopulation served consists of Caucasian, middle class, privately insured persons. Common diagnoses in-clude allergic rhinitis, asthma, urticaria, atopic dermatitis, beta-cell immune deficiencies, chronic sinusitis,headaches, and food allergies. Approximately 200 new patients are seen each month. A large majority ofpatients (65%) are referred to the clinic by family physicians and practitioners in the surrounding area. Manyreferrals (30%) also come from the current patient population, as well as patients who are referred by me-dia devices such as newspaper ads, telephone books, insurance handbooks, health fairs, and/or the WorldWide Web.
Design
A quasi-experimental prospective design was used to guide this study. The study is quasi-experimentalin the sense that patients from a general population of pediatric asthmatics were randomly assigned to ei-ther the PEFR group or the symptom plan group in the absence of a control group. The study is also prospec-tive in nature because the patients in both groups have been identified and followed up on over time; also, the outcome measures examined did not occur prior to the initiation of the study. This design waschosen due to its practicality, feasibility, and methodological sophistication. The use of the quasi-experi-mental design allows the researcher to introduce some research controls with little disruption of the naturalsetting.19
Population
The target population consisted of children between the ages of 6–12 years of age seen in an allergy andasthma clinic and having been diagnosed with mild to severe persistent asthma. This age group was cho-sen to increase likelihood of correct peak flow technique in a population requiring significant parental over-sight. Peak flow meter use can be attempted in ages 4 years and greater; however, technique improvesgreatly in ages greater than 6 years.20 Diagnosis of asthma was made on the basis of patient history, ex-amination, and pre/post-bronchodilator pulmonary function testing. Persistent asthma was defined as sub-jects experiencing symptoms at least two times per week, FEV1 � 80% predicted, and FEV1 or PEF vari-ability of 12% or greater.
ASTHMA MANAGEMENT PLANS
181
5255_e08_p177-190 10/7/04 1:13 PM Page 181

Recruitment and informed consent
Participants were recruited from new patients returning for a follow up visit within a 2-week time inter-val. All subjects had an initial consultation with an allergist and received a new diagnosis of chronic per-sistent asthma and were initiated on a daily-inhaled corticosteroid regimen. The 2-week follow up ap-pointment was scheduled with a nurse practitioner that consecutively recruited the children during this visit.Children and parents enrolled in the study signed assent/consent forms after an explanation of the proce-dure and the principal investigator provided requirements of the study. Participants were randomly assignedto receive one of two asthma action plans based on the last digit of their medical record number as assignedby computer upon initial data entry by office staff. Subjects with a medical record number ending in anodd number received a PEF asthma action plan, whereas those with a medical record number ending in aneven number received a symptom-based asthma action plan. Internal review board approval was obtainedfrom the clinic where the study was performed and Rush University, Chicago. The benefit:risk ratio wasassessed for this study, indicating minimal risk and important benefits.
Procedures
All participants were provided an individual asthma education session by 1 of 16 full-time registerednurses at the clinic during the recruitment visit. Education was consistent with the standard of care pro-vided on a usual and customary basis at the clinic. The educational session included a review of the phys-iology of asthma, asthma triggers, inhaler device instruction and return demonstration, medication types,purpose, and side effects; use of the steps in the asthma action plan; recognition of asthma exacerbations,and emergency and routine contact information. The role of medication to control asthma was emphasized,and all participants were given the general information that the dosage of medication may need to be ad-justed with changes in asthma severity. Subjects’ use of inhalers were checked and corrected if necessary.All participants were also assessed by spirometry before and after bronchodilator use during this enrollmentvisit and at the 3-month follow-up visit. The total visit time averaged 68 minutes among all groups, withapproximately 30 minutes devoted to the educational session.
Group 1: Symptom-based plan
Asthma action plan materials included information about the clinic and the providers, contact informa-tion, informational pages regarding the nature of asthma and asthma triggers including avoidance mecha-nisms, and the action plan portion of the plan. The action plan portion (Figure 1) of each plan comprisedthree steps, including baseline therapy with inhaled corticosteroid (green zone), a step-up level of therapyin which the dose of inhaled steroid was doubled and �2 agonists are used every 4 hours (yellow zone),and a third level where the patient or parent is instructed to call the office or present to the emergency room(red zone).
The instructions for the symptom-based plan listed common symptoms of asthma including persistentcough, symptoms of a common cold, and dyspnea as indications for initiating the yellow zone. The redzone was initiated if relief following bronchodilator lasted less than 2 hours, if the patient became short ofbreath doing normal daily activities, if there was uncontrolled coughing, or if breathing made it difficultfor the patient to speak.
Group 2: Peak flow-based plan
Participants allocated to the peak-flow-based plan were given a peak flow meter (Personal Best®,Respironics, Cedar Grove, NJ, supplied by the clinic) (Figure 2). Instructions on its use and recording ofdata were given by a registered nurse as well as provided in written form and included in their asthma ac-tion plan materials. Instruction included demonstration by the registered nurse with at least three returndemonstrations by the patient to assure proper technique. The individualized action plan included peak flowmeasurements that were estimated from the patient’s measured and predicted peak expiratory flows. Peakflow readings at or below which each step should be initiated were written into each subject’s action plan.The yellow zone was recommended when peak expiratory flow was less than 80% but greater than 60% of
LETZ ET AL.
182
5255_e08_p177-190 10/7/04 1:13 PM Page 182

the patient’s estimated best reading. Initiation of the red zone was advised when peak expiratory flow wasat or less than 60% of the estimated best expiratory flow. The published recommendations for the percent-ages in each zone vary among guidelines and it is unclear which is best considering limited research on thesubject.21–24 Participants in this study were asked to do three consecutive peak flow readings daily andrecord the best of the three in a provided written diary. The best reading was the one used to determinewhich zone of the asthma action plan the patient was in (Figure 3).
Follow up
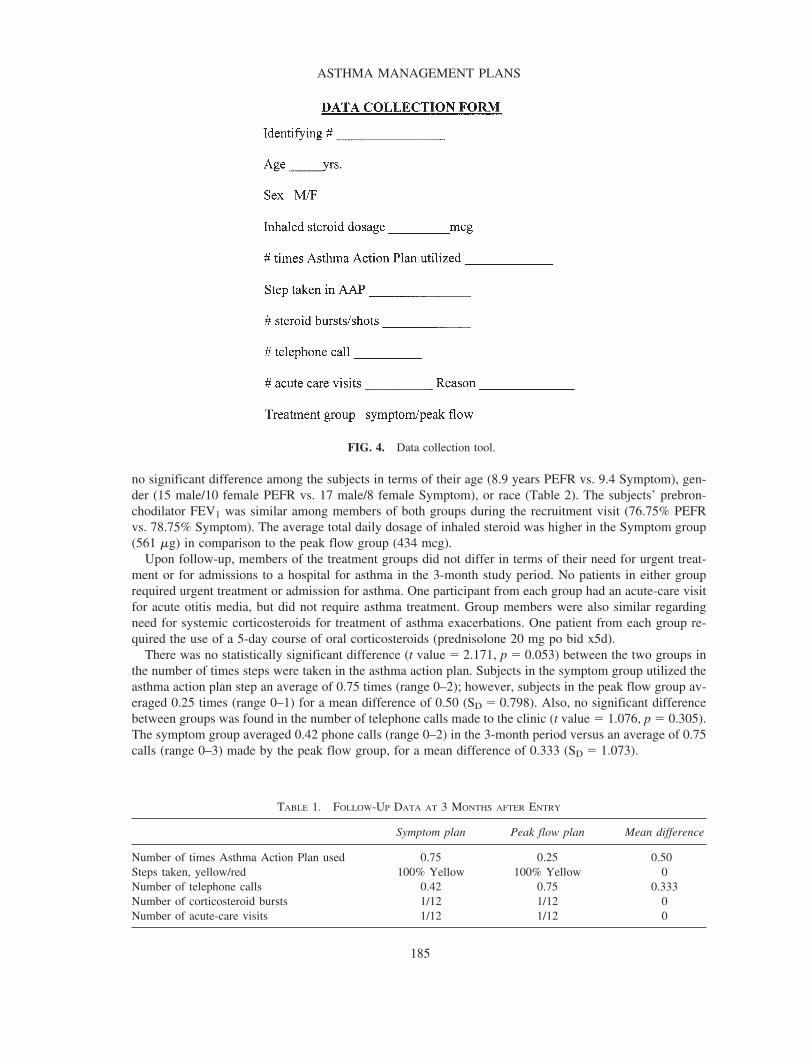
Participants returned to the clinic for follow up 3 months following enrollment in the study. Questionswere asked of parents in both groups by the registered nurse or principal investigator at the follow-up ap-pointment. Data were also collected from the participant’s problem log included in the action plan and fromtelephone calls made by the participants to the clinic in the interim period, as recorded in the triage systemof an electronic medical record. Data was recorded on a Data Collection Form (Figure 4). The questionsincluded:
ASTHMA MANAGEMENT PLANS
183
FIG. 2. Peak flow meter (with peak flow diary).
5255_e08_p177-190 10/7/04 1:13 PM Page 183

• How many times did you initiate the asthma action plan?• What step of the asthma action plan was taken?• How many phone calls were made to the clinic?• How many oral or injectable steroids were given between visits?• How many sick visits were made to the clinic, primary care physician, or urgent/emergency care center?
Urgent treatment was defined as treatment sought to provide relief of asthma symptoms.
Analysis
Comparisons were made among the two intervention groups. Data were analyzed by one-tailed paired t-test to increase the statistical power, with p � 0.05 considered significant. MYSTAT® (Systat Software Inc.,Point Richmond, CA) statistical software was utilized. The paired t-test was chosen due to the comparisonof two groups, small group size, quasi-experimental design, and to decrease chance differences that wouldoccur to a greater degree when measured independently.25 Analyzed and compared data included the num-ber of times the action plan was utilized, the steps taken in the plan, the number of telephone calls made,the number of corticosteroid bursts, and the number of acute-care visits (Table 1). Demographic data in-cluding age, sex, race, daily-inhaled steroid dose, and lung function measures (FEV1) were collected viathe medical chart during follow-up visits and compared between groups.
RESULTS
A total of 51 pediatric subjects who had recently received a diagnosis of mild to severe persistent asthmawere enrolled in the study. One subject was withdrawn from the study’s peak expiratory flow group whenhe/she failed to show for the 3-month follow-up visit. In total, the remaining 50 subjects included 25 whowere allocated to receive a symptom-based plan and 25 who received a peak flow-based plan. There was
LETZ ET AL.
184
FIG. 3. Peak Flow Asthma Action Plan.
5255_e08_p177-190 10/7/04 1:13 PM Page 184
no significant difference among the subjects in terms of their age (8.9 years PEFR vs. 9.4 Symptom), gen-der (15 male/10 female PEFR vs. 17 male/8 female Symptom), or race (Table 2). The subjects’ prebron-chodilator FEV1 was similar among members of both groups during the recruitment visit (76.75% PEFRvs. 78.75% Symptom). The average total daily dosage of inhaled steroid was higher in the Symptom group(561 �g) in comparison to the peak flow group (434 mcg).
Upon follow-up, members of the treatment groups did not differ in terms of their need for urgent treat-ment or for admissions to a hospital for asthma in the 3-month study period. No patients in either grouprequired urgent treatment or admission for asthma. One participant from each group had an acute-care visitfor acute otitis media, but did not require asthma treatment. Group members were also similar regardingneed for systemic corticosteroids for treatment of asthma exacerbations. One patient from each group re-quired the use of a 5-day course of oral corticosteroids (prednisolone 20 mg po bid x5d).
There was no statistically significant difference (t value � 2.171, p � 0.053) between the two groups inthe number of times steps were taken in the asthma action plan. Subjects in the symptom group utilized theasthma action plan step an average of 0.75 times (range 0–2); however, subjects in the peak flow group av-eraged 0.25 times (range 0–1) for a mean difference of 0.50 (SD � 0.798). Also, no significant differencebetween groups was found in the number of telephone calls made to the clinic (t value � 1.076, p � 0.305).The symptom group averaged 0.42 phone calls (range 0–2) in the 3-month period versus an average of 0.75calls (range 0–3) made by the peak flow group, for a mean difference of 0.333 (SD � 1.073).
ASTHMA MANAGEMENT PLANS
185
FIG. 4. Data collection tool.
TABLE 1. FOLLOW-UP DATA AT 3 MONTHS AFTER ENTRY
Symptom plan Peak flow plan Mean difference
Number of times Asthma Action Plan used 0.75 0.25 0.500Steps taken, yellow/red 100% Yellow 100% Yellow 0Number of telephone calls 0.42 0.75 0.333Number of corticosteroid bursts 1/12 1/12 0Number of acute-care visits 1/12 1/12 0
5255_e08_p177-190 10/7/04 1:13 PM Page 185

DISCUSSION
Findings
Statistical differences between the two groups were not found in the number of times the action plans wereemployed and the number of telephone calls made by participants. There is no indication whether the in-creased use of the asthma action plan by the symptom group was beneficial or not. One could argue that theincreased utilization may have thwarted potential asthma exacerbations, but one could also dispute that thisgroup had unnecessary increases in their medications. In the case of asthma, early treatment is the best strat-egy for the management of asthma exacerbations.20 Most asthma experts would agree that it is better to over-treat a potential exacerbation than not to treat it at all. The expert guidelines recommend that patients at allseverity levels monitor symptoms to recognized early signs of deterioration.20 Recognizing symptoms indi-cating inadequate control is of the utmost importance so that the need for additional therapy is met.
Although the purpose of this study was to determine differences in the use of asthma action plans, it isworth noting that the symptom group had made less phone calls to the clinic or other health professionalsfor questions or suggestions regarding their asthma. Typical telephone calls in both groups included ques-tions regarding over-the-counter medication use, symptoms, medication dosage, and side effects of med-ications. It is interesting to note that patients in the peak flow group were placed in the yellow zone of theaction plan upon calling a triage nurse at the clinic with symptoms suggestive of an early exacerbation ofasthma (i.e., mild cough, runny nose, fatigue). This may be an indication that participants in the peak flowgroup may not have been utilizing their action plans at a time when they should have been. The peak flowgroup did not have an increased number of acute-care visits or steroid bursts to support this notion. Al-though not all exacerbations will result in the need for an acute-care visit or treatment with an oral steroidburst, most exacerbations should result in a reduced peak flow meter reading.
This study yielded findings similar to the other studies examined in relation to the minute differences be-tween symptom and peak flow-based plans. The number of acute-care visits and required corticosteroidbursts were similar between the groups in the majority of the comparison studies. This study did examinevariables not studied in the other research endeavors, including the utilization of the action plans and num-ber of telephone calls made by participants in each group. These variables were not found to have statisti-cal differences between the two groups; however, a higher utilization rate among the symptom-based plangroup and a higher telephone call ratio among the participants in the peak flow group was noted.
Our practice has not made drastic changes since the conclusion of this study. It has been our standard togive symptom-based action plans to our patients with all classes of asthma. Peak flow meters and plans aregiven on occasion when patients are identified as poor perceivers of their asthma (indicated by frequentemergency room visits), when the patient and/or parent(s) request the device, or when the patient/parent(s)display a high level of motivation toward the utilization of the devices, such as from previous experience.Important elements of early asthma exacerbation treatment include a written action plan, recognition ofearly signs of worsening asthma, prompt communication between patient and clinician, removal or with-drawal of precipitants, and appropriate intensification.3 The written asthma action plan based on symptomshas been shown to assist in accomplishing these elements and may do so to a greater degree than the peak-flow-based plan in children with persistent asthma.
LETZ ET AL.
186
TABLE 2. DEMOGRAPHICS OF THE 24 SUBJECTS WHO COMPLETED STUDY
Symptom plan Peak flow plan
Age (years) 9.4 8.9Gender (male/female) 17/8 15/10Race 25 Caucasian 25 CaucasianAverage inhaled steroid dose 561 �g 434 �gFEV1 % of predicted 78.75 76.75prebronchodilator
5255_e08_p177-190 10/7/04 1:13 PM Page 186

Implications for practice and research
The implementation of asthma action plans based on peak flow readings has been widely advocated forthe home management of persistent asthma. It can be suggested after this study and literature review of theresearch currently available that PEFR monitoring via peak flow meters used in the home environment amongpediatric patients be suggested for use only among those patients who have been identified as poor per-ceivers of their asthma and among patients and parents who have demonstrated strong adherence in the pastand are committed to the use of such devices. The use of peak flow meters among children with mild-to-moderate asthma and who have not had a past life-threatening event is unrealistic and without significantevidence of benefit at present time. Less expensive portable spirometers which measure FEV1 are now be-coming available and may offer a way to monitor FEV1 at home in the future. Management of the child di-agnosed with asthma should most importantly focus on continued frequent follow-up visits, with the prac-titioner assessing airway obstruction via spirometry, monitoring patient adherence with the treatment regimen,continuing patient and family education, and assessing medication effectiveness and potential side effects.
Concordance between PEFR and other asthma severity markers can be poor. Findings26 suggest the useof peak flow monitor could either underestimate or overestimate FEV1 changes and result in over- or un-der-treatment of the patient. Regular monitoring of PEF could assist in the early detection of an asthma ex-acerbation, especially in those patients demonstrated to be poor assessors of airflow obstruction. However,to be effective, there would need to be a strong motivation on the part of the patient and parents and in-tense adherence. Because adherence involves both parents and children, there is an increased likelihood ofcommunication problems with health-care providers.27 Persons with poor perception of airflow limitationcould possibly be identified by the use of inhalation challenge testing. Patients with marked decrease inFEV1 with methacholine or histamine challenge testing and who do not develop significant symptoms couldbe thought of as poor perceivers. Children who require frequent emergency department visits, hospital ad-missions, and prednisone bursts may also be defined as those who may have a poor perception of theirasthma severity. Unfortunately, it has been demonstrated that those who are most likely to benefit from reg-ular peak flow meter use are the least likely to comply with such a management plan.28
Barriers to peak flow monitoring as identified by pediatricians include time, training, follow-up, patientadherence, and cost, which relate to lack of agreement, lack of self-efficacy, and lack of outcome ex-pectancy.29 Patients also need to be instructed as to which PEF value to record and how to interpret the re-sults. One problem is that during an exacerbation PEFR values are often taken soon after bronchodilatortherapy, which may skew the results upward, indicating better than actual control. Additional teaching isrequired with peak flow utilization, especially in the pediatric population. We also know that adherencewith asthma therapy usually declines as the number of drugs prescribed increases.30,31
There is a question of whether the addition of a peak flow meter may decrease adherence as well, sincethis does increase the daily regimen. Nearly every study examined regarding the use of inhaled medicationsin a clinical population has reported that as many as 50% of patients employ poor technique.32–36 Althoughproper technique of peak flow use has not been examined, the technique for metered dose inhaler is gen-erally described as easier than that for a peak flow meter device.
Because of the growing reliance on home monitoring and self-management of chronic asthma, accurateand reliable information about adherence to treatment is needed. Electronic-based spirometry devices arenow becoming available for use in the home environment. The ability to transmit data via the Internet canhave a tremendous value by giving the patient some level of autonomy, yet not leaving all the decisionmaking to them. Adherence with inhaled medications has been found to be poor in children with asthmadespite them knowing that an electronic inhaler counted the number of times the device was activated,30
and this may be the case with this sort of device. An electronic device will at least make the level of ad-herence known and not hidden from view to the health-care provider. The issue of how much autonomypatients and parents want in decision making with asthma management is an important factor that shouldbe addressed. Determining the degree of decision making a person prefers and the degree of self-efficacyone has can provide the health-care provider with useful information. An individual action plan or self-management plan could then be catered to the specific patient. Assessment tools are yet to be available forgathering this data, but may be a worthwhile endeavor.
ASTHMA MANAGEMENT PLANS
187
5255_e08_p177-190 10/7/04 1:13 PM Page 187

Until further information is available, it is important that published national guidelines be followed inthe assessment and management of pediatric asthma. The use of action plans in general has shown benefitand certainly no disadvantage in pediatric asthma patients. The benefit of using symptom versus peak flow-based plans has yet to be truly determined, but no major advantages exist for using a peak flow meter. Fur-ther inquiries of research may include whether the use of peak flow meters in the home environment in-creases or decreases asthma medication adherence, the use of assessment tools to measure self-efficacy anddecision-making characteristics of pediatric asthma patients, and the effect it has on asthma management.
All asthmatic children and their parents should receive an asthma action plan, whether based on PEFRmonitoring or symptoms. Asthma action plans consist of written protocols to follow when PEFR decreasesor when asthma symptoms arise. Most asthma action plans instruct the patient to increase dosages of in-haled corticosteroids (which are now the mainstay of treatment for chronic asthmatics) and may also rec-ommend use of a quick-fix inhaler or treatments such as pirbuterol or albuterol every 4 hours. A compre-hensive education plan should be in place for children and their parents when the diagnosis of asthma isgiven and during follow-up visits. Spirometers should be available in the office of every primary careprovider who cares for children with moderate to severe asthma to both diagnose and monitor asthma andairway obstruction.20
Supervision of a child’s treatment program by parents is essential and should be reinforced by providersat every visit. Interventions to increase patient involvement in the decision-making process of disease man-agement lead to better outcomes for a number of chronic illnesses37,38 and should also be considered whenmanaging a child with asthma.
Referral to a specialist is recommended when a life-threatening event has occurred, the patient is notmeeting the goals of asthma therapy, signs and symptoms are atypical, other conditions complicate the di-agnosis, additional testing is needed, patients under the age of 3 with moderate-to-severe asthma, patientswho require continuous oral corticosteroids, and patients who require additional education.20 The special-ist’s office may offer a more comprehensive educational program and patient instruction as well as have agreater number of resources available for pediatric asthmatics and their caregivers. The specialist will bemore familiar and comfortable with the utilization of multiple medications that may be necessary to con-trol severe asthma and may suggest further options such as immunotherapy. A specialist may also providea wider array of studies for evaluation of the etiology of the child’s asthma.
Project limitations
The limitations of this study include small sample size and short study duration. A larger-scale study iscertainly warranted and may be worthwhile to include a control group for comparison.
SUMMARY
In mild and moderate asthma, symptom-based plans seem to be as effective as PEFR monitoring, espe-cially considering identified poor adherence with the devices and frequent falsification of records. Adher-ence to a self-management plan is enhanced when the plan is simplified as much as possible.20 The addi-tional routine peak flow monitoring does nothing to simplify the self-management plan.
Sole reliance on PEFR monitoring alone is never warranted. Subjective symptoms should always be con-sidered in the evaluation and management of asthma and should often include nocturnal symptoms, fre-quency of �2 agonist use, sputum production, and exercise tolerance. PEFR monitoring via peak flow me-ters, when used, should be a part of a comprehensive education and management plan. Regardless of thetype of monitoring used, patients and parents should be given a written action plan and be instructed on itsuse.20 Merely providing written action plans will not necessarily assist patients to initiate changes in med-ication during exacerbations unless the question of whether this will be done without consultation with aclinician has also been specifically discussed and negotiated, rather than left unstated or implied. Writtenaction plans need to be personalized to each patient. Easy access to a clinician is also essential for the ap-propriate care of the asthmatic patient.
LETZ ET AL.
188
5255_e08_p177-190 10/7/04 1:13 PM Page 188
REFERENCES
1. United States Center for Disease Control and Prevention. Surveillance for Asthma. MMWR. 1998; 47:1–28.
2. Weinberger, M. Asthma management: guidelines for the primary care physician. Medscape Respiratory Care, 1999.(Available online at http//www.medscape.com/medscape/r).
3. National Asthma Education and Prevention Program. Expert Panel Report II. Guidelines for the Diagnosis andManagement of Asthma. Publication 97-4051. Bethesda, MD: National Institutes of Health; 1997.
4. Robertson CF, Rubinfield AR, Bowes G. Pediatric asthma deaths in Victoria: the mild are at risk. Pediatr Pulmonol1992; 13:95–100.
5. National Heart, Lung, and Blood Institute (NHLBI). National Asthma Education Program. Expert Panel Report:Guidelines for the Diagnosis and Management of Asthma. J Allergy Clin Immunol. 1991; 88:425–534.
6. Cote J, Cartier A, Malo JL, Rouleau M, Boulet LP. Adherence with peak expiratory flow monitoring in home man-agement of asthma. Chest 1998; 113:968–972.
7. Li JTC, O’Connell E. Clinical evaluation of asthma. Ann Allergy Asthma Immunol 1996; 76:1–14.
8. Kickuchi Y, Okabe S, Tamura G, et al. Chemosensitivity and perception of dyspnea in patients with a history ofnear-fatal asthma. N Engl J Med 1994; 330:1329–1334.
9. Apter A, Affleck G, Reisine S, et al. Perception of airway obstruction in asthma: sequential daily analyses of symp-toms, peak expiratory flow rate, and mood. J Allergy Clin Immunol 1997; 99:605–612.
10. Berube D, Cartier A, L’archeveque J, et al. Comparison of peak expiratory flow rate and FEV1 in assessing bron-chomotor tone after challenges with occupational sensitizers. Chest 1991; 99:831–836.
11. Gautrin D, D’Aquino LC, Gagnon G, Malo JL, Cartier A. Comparison between peak expiratory flow rates (PEFR)and FEV1 in the monitoring of asthmatic subjects at an outpatient clinic. Chest 1994; 106:1419–1426.
12. National Heart, Lung, and Blood Institute. Guidelines for the diagnosis and management of asthma: expert panelreport. Clinical Practice Guidelines. Publication 92-3091. Bethesda, MD: National Institutes of Health, 1991.
13. British Thoracic Society (BTS). 1993. Guidelines on the management of asthma. Thorax 1993; 48(suppl):1–24.
14. Weinstein AG. Clinical management strategies to maintain drug adherence in asthmatic children. Ann AllergyAsthma Immunol 1995; 74:304–310.
15. Creer T. Medication Adherence and Childhood Asthma. In NA Krasnegor, L Epstein, SB Johnson, SJ Yaffe, eds.Developmental aspects of health adherence behavior. Hillsdale, NJ: Lawrence Erlbaum Associates, 1993, pp.303–333.
16. Coutts JA, Gibson NA, Paton JY. Measuring adherence with inhaled medication in asthma. Arch Dis Child 1992;67:332–333.
17. Zora J, Lutz C, Tinkelman D. Assessment of adherence in children using inhaled beta adrenergic agonists. AnnAllergy 1989; 62:406–409.
18. Haynes R. Adherence in healthcare. Baltimore, MD: Johns Hopkins University Press, 1979.
19. Burns N, Grove S. The practice of nursing research: conduct, critique, and utilization, 3rd ed. Philadelphia: W.B.Saunders, 1997.
20. National Asthma Education and Prevention Program. Expert panel report II. Guidelines for the diagnosis and man-agement of asthma. Publication 97-4051. Bethesda, MD: National Institutes of Health, 1997.
21. Clough J, Sly P. Association between lower respiratory tract symptoms and falls in peak expiratory flow in chil-dren. Eur Respir J 1995; 8:718–722.
22. Woolcock A, Yan K, Salome C. Effect of therapy on bronchial hyperresponsiveness in the long-term managementof asthma. Clin Allergy 1988; 18:165–176.
23. Beasley R, Cushley M, Holgate S. A self-management plan in the treatment of adult asthma. Thorax 1989; 44:200–204.
24. Clark N, Evans D, Mellins R. Patient use of peak flow monitoring. Am Rev Respir Dis 1992; 145:722–725.
25. Munro B, Page E. 1993. Statistical methods for health care research, 2nd ed. Philadelphia: Lippinicott, 1993.
ASTHMA MANAGEMENT PLANS
189
5255_e08_p177-190 10/7/04 1:13 PM Page 189

26. Gautrin D, D’Aquino LC, Gagnon G, Malo JL, Cartier A. Comparison between peak expiratory flow rates (PEFR)and FEV1 in the monitoring of asthmatic subjects at an outpatient clinic. Chest 1994; 106:1419–1426.
27. Creer T. Medication adherence in chronically ill children. Tijdschr Kindergeneeskd 1998; 66:141–145.
28. Turner M, Grump G, Contrearas R, Fitzgerald M. The challenge of delivering asthma education to a high riskgroup. Am J Respir Crit Care Med 1994; 149:251.
29. Leickly F. Barriers pediatricians face when using asthma guidelines. Pediatrics 2001; 108:551.
30. Coutts JA, Gibson NA, Paton JY. Measuring adherence with inhaled medication in asthma. Arch Dis Child 1992;67:332–333.
31. Tashkin D. Multiple dose regimens: impact on adherence. Chest 1995; 107(suppl):176–182.
32. Rand CS, Wise RA. Adherence with asthma therapy in the management of asthma: review and clinical guidelines.In SJ Szefler, DYM Leung, eds. Severe asthma: pathogenesis and clinical management. New York: Marcel Dekker,1996, pp. 434–464.
33. Baciewicz A, Kyllonen K. Aerosol inhaler technique in children with asthma. Am J Hosp Pharm 1989; 46:2510–2511.
34. Pederson S. Ensuring adherence in children. Eur Respir J 1992; 5:143–145.
35. DeBlaquiere P, Christensen D, Carter W, Martin T. Use and misuse of metered-dose inhalers by patients withchronic lung disease. Am Rev Respir Dis 1989; 140:910–916.
36. Crompton G. The adult patient’s difficulty with inhalers. Lung 1990; 168:658–662.
37. Kaplan S, Greenfield S, Dukes K, et al. Effect of joint physician-patient training program on health outcomes andinterpersonal care. Clin Res 1993; 41:541A.
38. Greenfield S, Kaplan S, Ware J, et al. Patients’ participation in medical care. J Gen Intern Med 1988; 3:448–457.
Address reprint requests to:Kevin Letz, N.D.
The Allergy & Asthma Center7230 Engle Road, Suite 300
Fort Wayne, IN 46804
E-mail: [email protected]
LETZ ET AL.
190
5255_e08_p177-190 10/7/04 1:13 PM Page 190