a phlebolith in the anterior portion of the masseter …mj-med-u-tokai.com/pdf/370106.pdfh. kato et...
TRANSCRIPT

Tokai J Exp Clin Med., Vol. 37, No. 1, pp. 25-29, 2012
―25―
INTRODUCTION
The pathological calcification of soft tissues occurs when calcium and other mineral salts are deposited in a tissue or passage. Dystrophic calcification occasion-ally occurs in degenerating and dead tissues, while metastatic calcification is the result of an excess of calcium salts in the circulating blood [1, 2].
The buccal soft tissues rarely contain lesions that include calcifications. Phleboliths associated with vas-cular lesions are the most frequent [3, 4]. However, the differential diagnosis includes sialolithiasis, traumatic myositis ossificans, calcified acne lesions, neoplasms, and calcified lymph nodes, including tuberculosis [5-9]. Plain x-rays show the typical appearance of the calci-fied bodies and may help to differentiate these entities. Computed tomography (CT), magnetic resonance im-aging (MRI), and ultrasonography are also useful for differentiating these lesions.
We report a patient with a small mass that con-tained a calcified body in the anterior portion of the masseter muscle. The mass was resected and evaluated histologically, confirming the diagnosis of a phlebolith. We also discuss the differential diagnosis of buccal soft tissue masses with calcification and suggest that the immunolocalization of CD31 at capillaries in the mass may help to diagnose as a phlebolith.
CASE REPORT
A 17-year-old girl was referred to the Department of Oral and Maxillofacial Surgery, National Hospital Organization Shizuoka Medical Center, with a small, painless, movable, hard nodule in the right buccal submucosa. It was first noticed incidentally when the patient touched her cheek 1 month earlier. The size had not changed during the month. Her past and fam-ily histories were unremarkable.
There was no facial asymmetry, restriction of mouth opening, swelling of the right cheek, or associated lymph node enlargement. A soybean-sized, round nod-ule was palpable under the buccal skin and mucosa. The skin and mucosa covering the lesion appeared normal. The mass was located far from Stensen’s duct. There was no history of trauma, dental problems, al-lergy, or other medical problems.
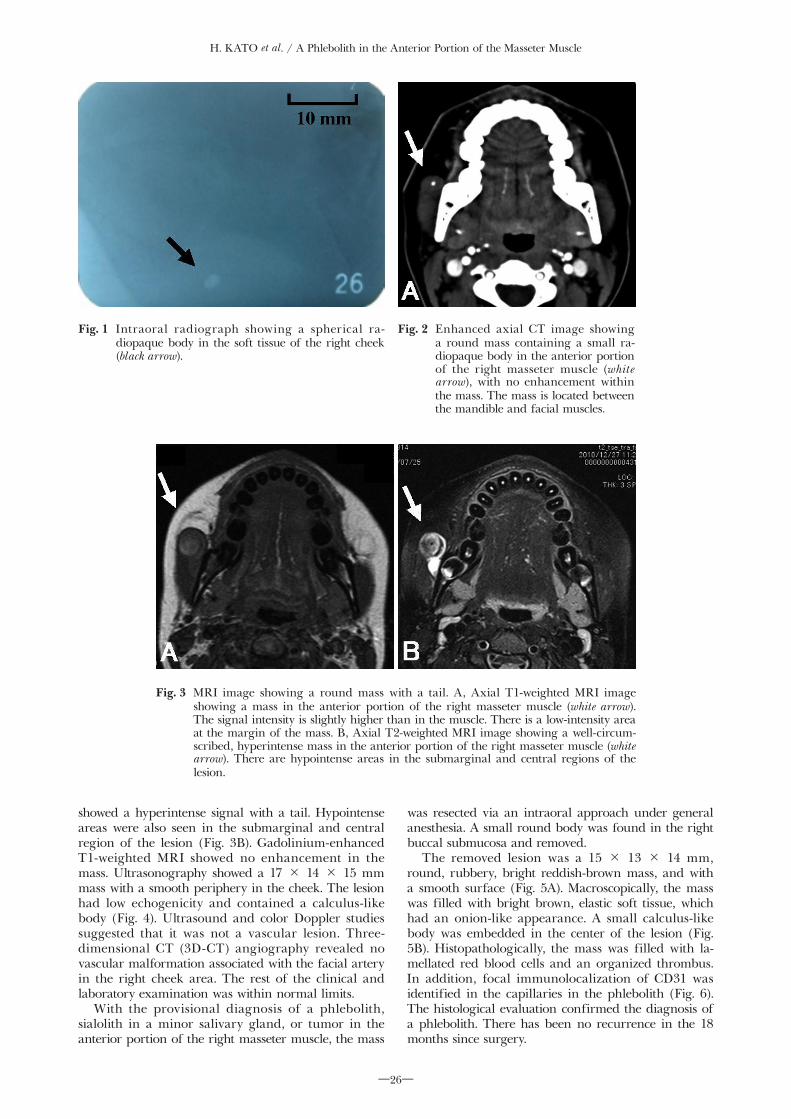
Intraoral radiographs revealed a radiopaque, mil-liary body in the soft tissue of the right cheek (Fig. 1). CT showed a round mass containing a small radiopaque body in the anterior portion of the right masseter muscle. The lesion was located between the mandible and facial muscles. There was no enhance-ment within the mass (Fig. 2). T1-weighted MRI revealed a well-circumscribed, round mass with a tail in the anterior portion of the right masseter muscle. The signal had a slightly greater intensity than the surrounding muscle, but there was a low-intensity area at the margin of the mass (Fig. 3A). T2-weighted MRI
A Phlebolith in the Anterior Portion of the Masseter Muscle
Hisashi KATO*1, Yoshihide OTA*1, Masashi SASAKI*2, Toshihiro ARAI*1, Yasutomo SEKIDO*3 and Keiichi TSUKINOKI*4
*1Department of Oral and Maxillofacial Surgery, Tokai University School of Medicine *2Department of Oral and Maxillofacial Surgery, National Hospital Organization
Shizuoka Medical Center *3Department of Pathology, Tokai University School of Medicine
*4Department of Diagnostic Science Division of Pathology, Kanagawa Dental College
(Received January 12, 2012; Accepted February 20, 2012)
The differential diagnosis of a buccal soft tissue mass containing calcified bodies includes a phlebolith as-sociated with a vascular lesion, such as a hemangioma with a calcified intravascular thrombus, and diseases such as sialolithiasis, traumatic myositis ossificans, calcified acne lesion, neoplasm, and calcified lymph nodes, including tuberculosis. The appearance of the calcified bodies on plain radiographs may help to dif-ferentiate these entities. Computed tomography, magnetic resonance imaging, and ultrasonography are also useful for differentiating the soft tissue lesions.We report a 17-year-old girl with a small mass containing a calcified body in the anterior portion of the masseter muscle. The mass was resected surgically and evaluated histologically, confirming the diagnosis of phlebolith. We also discuss the differential diagnosis of a buccal soft tissue mass containing calcifications and suggest that the immunolocalization of CD31 at capillaries in the mass may help to diagnose as a phlebo-lith.
Key words: phlebolith, calcified body, buccal soft tissue mass, intravascular thrombus,hemangioma
Hisashi KATO, Department of Oral and Maxillofacial Surgery Tokai University School of Medicine, 143 Shimokasuya, Isehara, Kanagawa 259-1193, JapanTel: +81-463-93-1121 Fax: +81-463-95-7567 Email: [email protected]
H. KATO et al. / A Phlebolith in the Anterior Portion of the Masseter Muscle
―26―
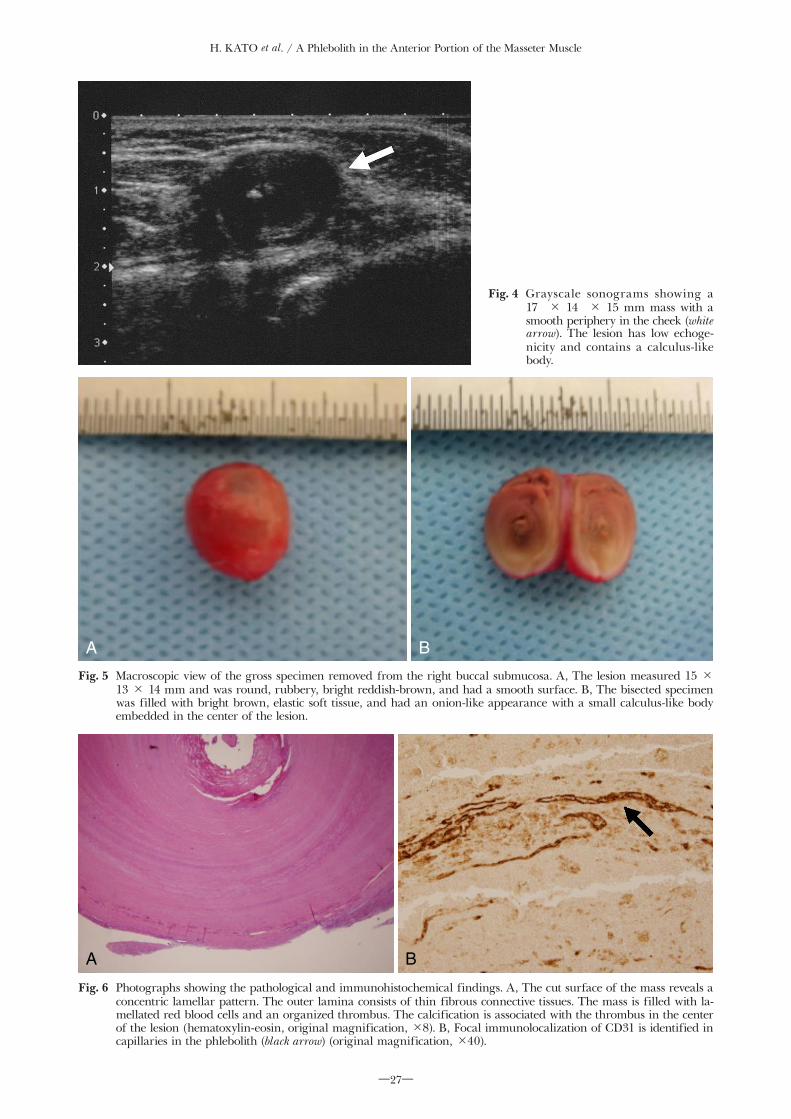
showed a hyperintense signal with a tail. Hypointense areas were also seen in the submarginal and central region of the lesion (Fig. 3B). Gadolinium-enhanced T1-weighted MRI showed no enhancement in the mass. Ultrasonography showed a 17 × 14 × 15 mm mass with a smooth periphery in the cheek. The lesion had low echogenicity and contained a calculus-like body (Fig. 4). Ultrasound and color Doppler studies suggested that it was not a vascular lesion. Three-dimensional CT (3D-CT) angiography revealed no vascular malformation associated with the facial artery in the right cheek area. The rest of the clinical and laboratory examination was within normal limits.
With the provisional diagnosis of a phlebolith, sialolith in a minor salivary gland, or tumor in the anterior portion of the right masseter muscle, the mass
was resected via an intraoral approach under general anesthesia. A small round body was found in the right buccal submucosa and removed.
The removed lesion was a 15 × 13 × 14 mm, round, rubbery, bright reddish-brown mass, and with a smooth surface (Fig. 5A). Macroscopically, the mass was filled with bright brown, elastic soft tissue, which had an onion-like appearance. A small calculus-like body was embedded in the center of the lesion (Fig. 5B). Histopathologically, the mass was filled with la-mellated red blood cells and an organized thrombus. In addition, focal immunolocalization of CD31 was identified in the capillaries in the phlebolith (Fig. 6). The histological evaluation confirmed the diagnosis of a phlebolith. There has been no recurrence in the 18 months since surgery.
Fig. 1 Intraoral radiograph showing a spherical ra-diopaque body in the soft tissue of the right cheek (black arrow).
Fig. 2 Enhanced axial CT image showing a round mass containing a small ra-diopaque body in the anterior portion of the right masseter muscle (white arrow), with no enhancement within the mass. The mass is located between the mandible and facial muscles.
Fig. 3 MRI image showing a round mass with a tail. A, Axial T1-weighted MRI image showing a mass in the anterior portion of the right masseter muscle (white arrow). The signal intensity is slightly higher than in the muscle. There is a low-intensity area at the margin of the mass. B, Axial T2-weighted MRI image showing a well-circum-scribed, hyperintense mass in the anterior portion of the right masseter muscle (white arrow). There are hypointense areas in the submarginal and central regions of the lesion.
H. KATO et al. / A Phlebolith in the Anterior Portion of the Masseter Muscle
―27―
Fig. 4 Grayscale sonograms showing a 17 × 14 × 15 mm mass with a smooth periphery in the cheek (white arrow). The lesion has low echoge-nicity and contains a calculus-like body.
Fig. 6 Photographs showing the pathological and immunohistochemical findings. A, The cut surface of the mass reveals a concentric lamellar pattern. The outer lamina consists of thin fibrous connective tissues. The mass is filled with la-mellated red blood cells and an organized thrombus. The calcification is associated with the thrombus in the center of the lesion (hematoxylin-eosin, original magnification, ×8). B, Focal immunolocalization of CD31 is identified in capillaries in the phlebolith (black arrow) (original magnification, ×40).
Fig. 5 Macroscopic view of the gross specimen removed from the right buccal submucosa. A, The lesion measured 15 × 13 × 14 mm and was round, rubbery, bright reddish-brown, and had a smooth surface. B, The bisected specimen was filled with bright brown, elastic soft tissue, and had an onion-like appearance with a small calculus-like body embedded in the center of the lesion.
A B
A B

H. KATO et al. / A Phlebolith in the Anterior Portion of the Masseter Muscle
―28―
DISCUSSION
When evaluating a buccal soft tissue mass with a calculus-like body, phleboliths associated with vascular lesions are the most frequent. However, the mass must be differentiated from sialolithiasis, traumatic myositis ossificans, calcified acne lesions, neoplasms, and calci-fied lymph nodes including tuberculosis [5-9].
Calcified acne lesions are easily ruled out based on the clinical findings because they are superficial lesions [3]. The appearance of calcified bodies on plain radio-graphs may help to differentiate other entities. A phle-bolith is usually laminated, with a radiopaque center, although the center is sometimes radiolucent; a small phlebolith is uniformly radiopaque [3]. Moreover, there are often multiple phleboliths when associated with a hemangioma. By contrast, traumatic myositis ossifi-cans, which is associated with trauma and occasionally occurs in the masseter muscle, has a feathery pattern along the muscle fibers or a striated linear morphology [3]. The lymphadenopathy associated with tuberculosis forms a cauliflower-shaped pattern in a chain [10]. In our case, the plain radiograph showed a round, uniformly radiopaque lesion. Therefore, these two lat-ter diseases could also be ruled out. A sialolith in the buccal region can occur in the parotid duct and gland or in a minor salivary gland. In our case, the calcified body was not associated with the parotid gland, as it was located far from Stensen’s duct. Although sialoliths in the minor salivary glands are rare, they frequently appear in the buccal mucosa. Perhaps masticatory trauma to the buccal mucosa has some bearing on the increased incidence of sialoliths in this area [6].
The pathogenesis of phleboliths is thought to involve an organized thrombus produced when the peripheral blood flow slows [3, 4]. The thrombus calcifies, form-ing the core of the phlebolith. Then, the fibrinous component undergoes secondary calcification and becomes attached. Repetition of this process causes enlargement of the phlebolith [11]. Therefore, most phleboliths are found along with vascular anomalies such as a hemangioma. However, there are rare cases that do not involve vascular anomalies. Although our case was not associated with a vascular anomaly, the mass was filled with lamellated red blood cells, and the focal immunolocalization of CD31, which is found on endothelial cells, was identified in the capillaries [12]. The immunohistochemical finding of CD31 may be evidence of a phlebolith.
Vascular anomalies usually include two separate clinical and histopathological entities: hemangiomas and vascular malformations [13]. Hemangiomas are the most common benign soft tissue tumors of child-hood [13]. In the maxillofacial area, intramuscular hemangiomas most frequently occur in the masseter muscle [14]. Approximately 40% of venous malforma-tions, which are the most common vascular malfor-mation, are located in the head and neck region [13, 15, 16]. In addition, there occasionally is masticatory trauma to the buccal mucosa, leading to thrombus for-mation [15]. Therefore, phleboliths are most frequently found in the buccal region. Although there was no history of trauma in our case, there might have been unidentified masticatory trauma to the buccal mucosa.
Diagnostic imaging modalities such as CT, MRI, and ultrasonography have significantly increased the accuracy of the preoperative diagnosis of patients with such lesions [11]. Vascular lesions are characteristi-cally much brighter on T2-weighted images than T1-weighted images due to the increased free water pres-ent within stagnant blood in the vessels. Ultrasound and color Doppler studies can also suggest a vascular lesion [16]. In our case, the lesion was characteristically much brighter on T2-weighted MRI images and there was no enhancement or blood flow within the mass. In the preoperative assessment, CT, MRI, and ultrasonog-raphy accurately showed that the mass did not involve vascular anomalies and contained a calculus-like body.
When evaluating a buccal soft-tissue mass with a calculus-like body, the lesion should initially be considered a phlebolith in patient who are in the first or second decade of life. In addition, a detailed interview of the history of the illness, such as injury and masticatory trauma to the buccal mucosa, may help to differentiate several entities. Plain x-rays may also help with the diagnosis because of the typical appearance of the calcified bodies and CT, MRI, and ultrasonography are more useful for making an ac-curate diagnosis. Moreover, the immunolocalization of CD31 to capillaries in the mass may help to diagnose as a phlebolith when the mass does not accompany a vascular anomaly.
REFERENCES1) Scarpelli DG, Chiga M, Kissane JM, editors. Cell injury and
errors of metabolism. Saint Louis: Mosby, 1977: 90-147.2) Sencimen M, Gulses A, Ogretir O, Gunhan O, Ozkaynak O,
Okcu KM. Dystrophic calcifications arising in the masseter muscle: a case report. Quintessence Int 2010; 41: 295-7.
3) O’Riordan B. Phleboliths and salivary calculi. Br J Oral Surg 1974; 12: 119-31.
4) Raymond AK, Batsakis JG. Angiolithiasis and sialolithiasis in the head and neck. Ann Otol Rhinol Laryngol 1992; 101: 455-7.
5) Wussow GC. Myositis ossificans of the buccinator muscle. Oral Surg Oral Med Oral Pathol 1968; 26: 615-8.
6) Bahn SL, Tabachnick TT. Sialolithiasis of minor salivary glands. Oral Surg Oral Med Oral Pathol 1971; 32: 371-7.
7) Stewart JG, MacMahon H, Vyborny CJ, Pollak ER. Dystrophic calcification in carcinoma of the lung: demonstration by CT. AJR Am J Roentgenol 1987; 148: 29-30.
8) Torres-Lagares D, Barranco-Piedra S, Serrera-Figallo MA, Hita-Iglesias P, Martínez-Sahuquillo-Márquez A, Gutiérrez-Pérez JL. Parotid sialolithiasis in Stensen’s duct. Med Oral Patol Oral Cir Bucal 2006; 11: E80-4.
9) Keberle M, Robinson S. Physiologic and pathologic calcifications and ossifications in the face and neck. Eur Radiol 2007; 17: 2103-11.
10) Katz JO, Langlais RP, Underhill TE, Kimura K. Localization of paraoral soft tissue calcifications: the known object rule. Oral Surg Oral Med Oral Pathol 1989; 67: 459-63.
11) Kanaya H, Saito Y, Gama N, Konno W, Hirabayashi H, Haruna S. Intramuscular hemangioma of masseter muscle with promi-nent formation of phleboliths: a case report.Auris Nasus Larynx 2008; 35: 587-91.
12) Parums DV, Cordell JL, Micklem K, Heryet AR, Gatter KC, Mason DY. JC70: a new monoclonal antibody that detects vascu-lar endothelium associated antigen on routinely processed tissue sections. J Clin Pathol 1990; 43: 752-7.
13) Mulliken JB, Fishman SJ, Burrows PE. Vascular anomalies. Curr Probl Surg 2000; 37: 517-84.
14) Rossiter JL, Hendrix RA, Tom LW, Potsic WP. Intramuscular hemangioma of the head and neck. Otolaryngol Head Neck Surg 1993; 108: 18-26.

H. KATO et al. / A Phlebolith in the Anterior Portion of the Masseter Muscle
―29―
15) Scolozzi P, Laurent F, Lombardi T, Richter M. Intraoral venous malformation presenting with multiple phleboliths. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003; 96: 197-200.
16) Rai P, Setia S, Kalra N, Upreti L. Intramuscular vascular mal-
formation of the masseter muscle presenting with turkey wattle sign. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006; 102: 618.