a goal orientated pilates program to improve strength in ... · a goal orientated pilates program...
TRANSCRIPT

A goal orientated Pilates Program to improve strength in the hip joint following Total
Hip Arthroplasty- A case report
Lisa-Mari De Villiers
October 2nd, 2017
2016 Vancouver

Abstract
Osteoarthritis (OA) is degenerative joint disease involving the cartilage and surrounding
structures. OA of the hips and knees cause the greatest burden to the population as pain
and stiffness in these joints may cause disfunction and may require surgical intervention.
One in 4 people may develop symptomatic hip osteoarthritis in his or her lifetime. The total
number of replacement surgeries are increasing while the average age of candidates
receiving surgery are decreasing, especially in younger and more active individuals who
want to stay active and maintain good, pain free range of motion (ROM) of their joints. By
the year 2030 it is estimated that more than 4 million people would receive replacement
surgery annually.
In South Africa, the costs of private care and medical aids are rising and there is a
demanding need for earlier functional recovery post total hip replacement (THR) surgery
by a younger population. Consequently, there is an increased need for cost effective
outpatient intervention, specifically exercise programs as an alternative or as a
supplementary to rehabilitation. It would make sense to say that younger clients would
benefit from a more aggressive approach to post operative rehabilitation as they have
more functional demands and have higher implant life expectancy. The goal of
rehabilitation for these younger patients in the long-term is to maintain a good functional
hip for as long as possible without having to undergo revision surgery.
In this case report a goal orientated pilates based exercise program was used to improve
hip control in a 48 year old female patient 6 weeks post total hip arthroplasty surgery.
Taking hip replacement precautions into consideration, a 6 weeks exercise program was
compiled after assessing the patient’s ability to perform simple functional strength tests as
�2

� well as performing some basic fundamental pilates exercises. The necessary adaptations 3
and modifications were made to protect the joint and to ensure gradual strengthening to
improve hip control especially during Gait.
After 6 weeks of Pilates training and a thorough re-assessment it was found that there was
an improvement in the performance of the functional tests, as well as an improvement in
the quality of movement when performing the pilates exercises. Functionally there was an
overall improvement in Gait, demonstrating better hip control and balance.
The aim of this study is to prove that a goal orientated pilates program could be useful in
improving and addressing weakness in the hip joint complex and improve overall
functional ability of the hip joint following hip replacement surgery.
Table of Contents
1. Introduction
2. Anatomy of the hip joint and THR
3. Client History
4. Physiotherapy Assessment
5. Therapeutic Approach and Goal setting
6. Conditioning Program
7. Results
8. Conclusion
9. References
�4
1. Introduction
OA of the hips and knees could be described as the greatest burden to society mainly due
to the rising costs of health care. Pain and stiffness in these weight baring joints often lead
to significant disability requiring surgical intervention.
Arthroplasty for the management of hip OA is increasing in frequency. It has been shown
to to improve pain, disability, function, physical activity and quality of life (QOL). There has
been a shift from hip replacements for the crippled elderly mainly to an increasing younger
generation presenting with OA, wanting to improve their QOL as well as wanting to
continue physically demanding activities. Improvements in the prosthetic design also
contributes to an increased demand for surgery. Candidates for THR’s require a more
complex management strategy in terms of rehabilitation. They have higher functional and
physical demands.
Because most individuals receiving THR surgery have had pain and dysfunctional walking
patterns for a period of time before the operation, it is evident that there would also be
significant weakness of surrounding muscles of the hip joint even after surgery. A strong
emphasis is placed on strengthening the muscles around the hip for better hip control and
to improve functional recovery.
Due to limited evidence exercise programs appear to be based on clinical experience and
surgeon preference. However some evidence have shown that an eight week exercise
program focussing on strength and stability around the hip joint, resulted in a statistically
significant improvement in function and muscle strength in patients between 4 and 12
months post THR surgery. It has also been suggested in this study that patients should
�5
continue with functional strengthening exercise programs for at least one year after the
surgery and that the program should be progressed as function improved.
Pilates as an exercise approach could be useful in the management of THR’s. According
to a study by Levine et al 2009, the pilates method provides simple goal orientated
exercises resulting in a whole body approach to rehabilitation, and could be easily
modified to meet each clients individual needs with specific precautions taken into
consideration. These exercise could easily be progressed and made more difficult as the
clients function improves. Furthermore in this study, 38 patients were using Pilates as a
form of rehabilitation post joint arthroplasty, 21 of which were THR’s. At one year follow up,
it was revealed that 25 clients were extremely satisfied with the outcome of using pilates in
their rehabilitation. There were no dissatisfying or somewhat satisfying feedback from the
group.
Pilates also known as “contrology” puts emphasis on strengthening the core of the body.
This is also referred to as the powerhouse. By creating a strong powerhouse, Pilates
believed that ones ability to function during daily activities is optimised. The stability of the
core creates a stable base for movement of the extremities and could potentially prevent
injuries to the peripheral extremities. Quality of movement instead of quantity is important
in the Pilates method. The exercises are performed with control and therefore a strong
focus is drawn to the stabilizing role of muscles around the joints. Furthermore the 10
principles of pilates are Awareness, Balance, Control, Efficiency, Precision, Breath,
Concentration, Centre, Flow and Harmony. Pilates focuses on maintaining a neutral spine
during exercise and movement. This enforces balanced muscular development and
correct muscle recruitment in the whole body, focussing on the body as a whole
contributing to functional improvements.
�6
2. Anatomy of the hip joint and THR
The hip is the structural link between the lower body and the axial skeleton as it transmits
forces from the ground upwards and also carries forces from the trunk, head neck and
upper body. The hip is a ball and socket joint, enabling a wide range of mobility in different
planes as well as stability.
Stability around the hip joint is formed by a strong ligamentous capsule. It consists of the
iliofemoral ligament, the pubofemoral ligament, the ischiofemoral ligament, the ligamentum
teres and the angular ligament. These ligaments along with the labrum of the hip joint
contributes to the passive stability of the joint.
The active stability of the hip is determined by a large number of controlling muscles. The
22 muscles surrounding the hip joint also provides rotational motion in all directions. These
muscles can contribute to movement in several different planes, depending on the position
of the hip. This is called inversion of muscle action. For example gluteus medius and
minimus muscles act as hip abductors when the hip is extended and as internal rotators
when the hip is flexed.
For the purpose of this study, a trendellneburg gait could be described as the pelvis
sagging to the contra-lateral side due to weakness of the abductor muscle group on the
weightbaring side. This causes the individual to shift their centre of gravity (COG) towards
the affected joint by leaning over, therefore reducing the force required by the abductors to
counteract the movement. This is normally accompanied by a limp.
�7
Stability around the hip joint during the stance phase of gait is mainly contributed by the
hip abductors for hip control. This group of muscles include the upper fibres of the gluteus
maximus, tensor fascia lata, gluteus medius and minimus, piriformis and obturator internus
muscle. Hip control could be described as the stabilising muscles around the hip joint
working together to control the hip in the socket and therefore preventing a trendellenburg
gait.
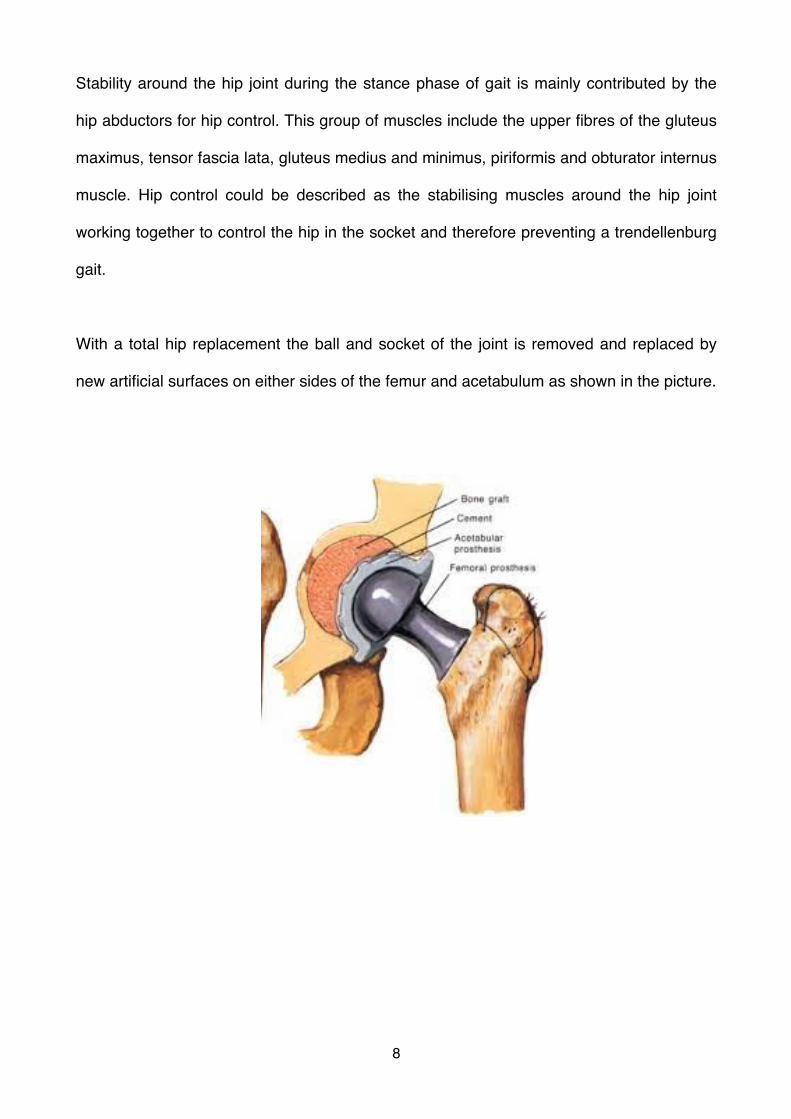
With a total hip replacement the ball and socket of the joint is removed and replaced by
new artificial surfaces on either sides of the femur and acetabulum as shown in the picture.
�8
3. Client History
Mrs. X is 6 weeks post operative left THR. She is a 48 year old female working as a high
school teacher. She has had multiple injuries to her left hip after falling on her hip as a
child at the age of 5 years old. After that incident numerous injuries followed, to such an
extent that she was diagnosed with Osteoarthritis a couple of years ago.
She had considerable groin pain with walking and climbing steps. She also noted that she
was developing a limp and struggled to put on shoes as the hip was becoming stiff. These
symptoms made it difficult for her to perform her daily activities as a teacher, as her job
required her to be on her feet constantly from morning to late afternoon. Considering all
possible options in the management of her condition, she decided along with an
orthopedic surgeon that the best solution was a total hip replacement.
Up to now, Mrs. X has had 6 sessions of intense physiotherapy, one session per week.
These sessions included soft tissue mobilization, light joint mobilization and stretching. A
general inpatient strengthening and ROM exercise program was continued and
progressed using a theraband and core activation exercises was commenced. The focus
was to decrease pain, increase ROM and to create body-awareness.
After 6 weeks Mrs. X still struggled with a limp, however she was ambulating pain free with
one crutch to eliminate the limp and the ROM in her left hip had improved significantly. At
this stage the orthopedic surgeon was happy with her progress and said she could now
leave the crutches if she feels comfortable. I advised her to keep one crutch on her right
side to help and improve the limp. As specified by the surgeon, Mrs. X was able to return
to normal day to day activities. However; further ongoing precaution for her hip
�9
replacement was pain free activity and exercise, no crossing of the legs and no twisting or
internally rotating of the hip. She was also not allowed to run for the next 6 months.
4. Physiotherapy assessment
On a 6 weeks post op THR evaluation Mrs. X had no more pain with walking, however she
still had to use one crutch in her right hand to eliminate the limp. It was also found that the
ROM in her hip was closely resembling her non-affected side. This included flexion, lateral
rotation and abduction of her left hip. Extension of her hip was limited due to tight hip
flexors and quadriceps muscle. All these movements were pain free and no overpressure
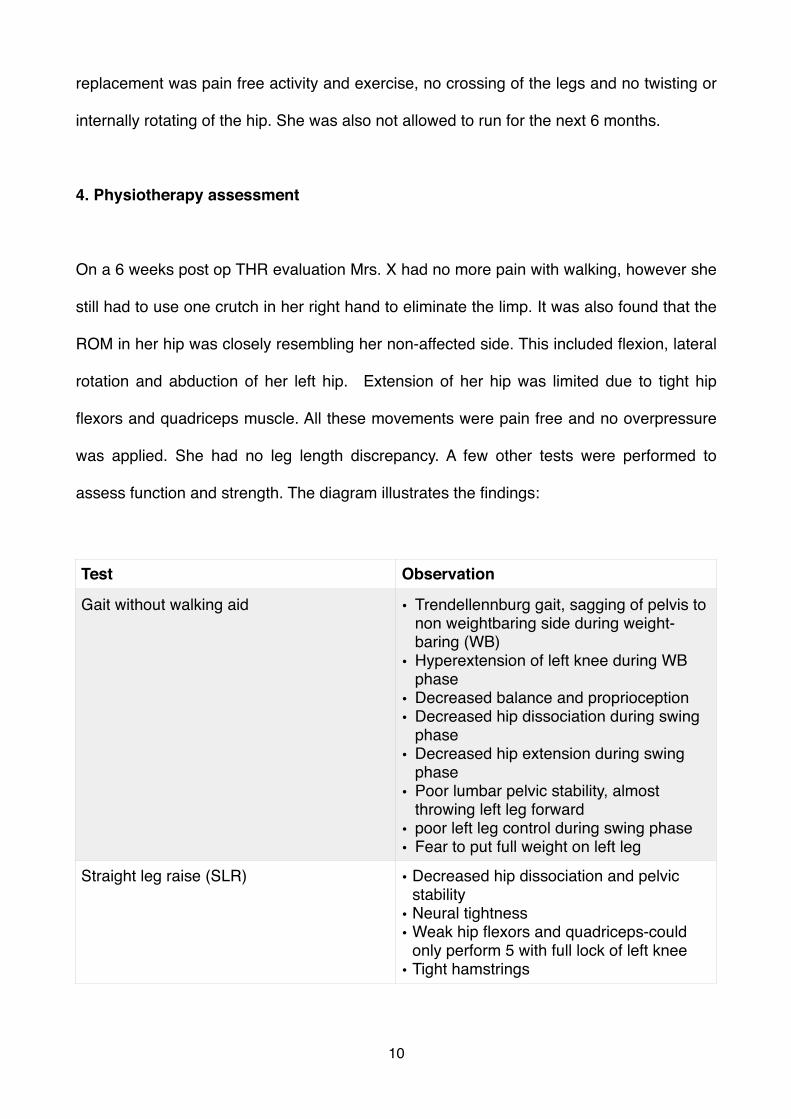
was applied. She had no leg length discrepancy. A few other tests were performed to
assess function and strength. The diagram illustrates the findings:
Test Observation
Gait without walking aid • Trendellennburg gait, sagging of pelvis to non weightbaring side during weight-baring (WB)
• Hyperextension of left knee during WB phase
• Decreased balance and proprioception• Decreased hip dissociation during swing
phase• Decreased hip extension during swing
phase• Poor lumbar pelvic stability, almost
throwing left leg forward• poor left leg control during swing phase• Fear to put full weight on left leg
Straight leg raise (SLR) • Decreased hip dissociation and pelvic stability
• Neural tightness• Weak hip flexors and quadriceps-could
only perform 5 with full lock of left knee• Tight hamstrings
�10
After observation and evaluation, I had a discussion with Mrs. X about her expectations
and wishes. She explained to me that her biggest wish was to to be able to walk without a
crutch and without a limp. I responded by explaining what the trendellenburg gait was and
that there were a few factors that could contribute to this walking pattern. I told Mrs. X that
this pattern of walking was adopted by her body long ago because of pain and weakness
that had developed around her hip joint. By walking with a limp, less strain was put on
weak muscles to control the hip joint and consequently helped to ease pain.
I also explained that now that she was pain free however, more emphasis could be placed
on rehabilitation and strengthening of the structures that are contributing to the limp. I
assured her that the limp would continue to improve with time with an appropriate
exercises program. I suggested an exercise routine that would be safe, enjoyable and
could become part of her lifestyle. I introduced her to Pilates.
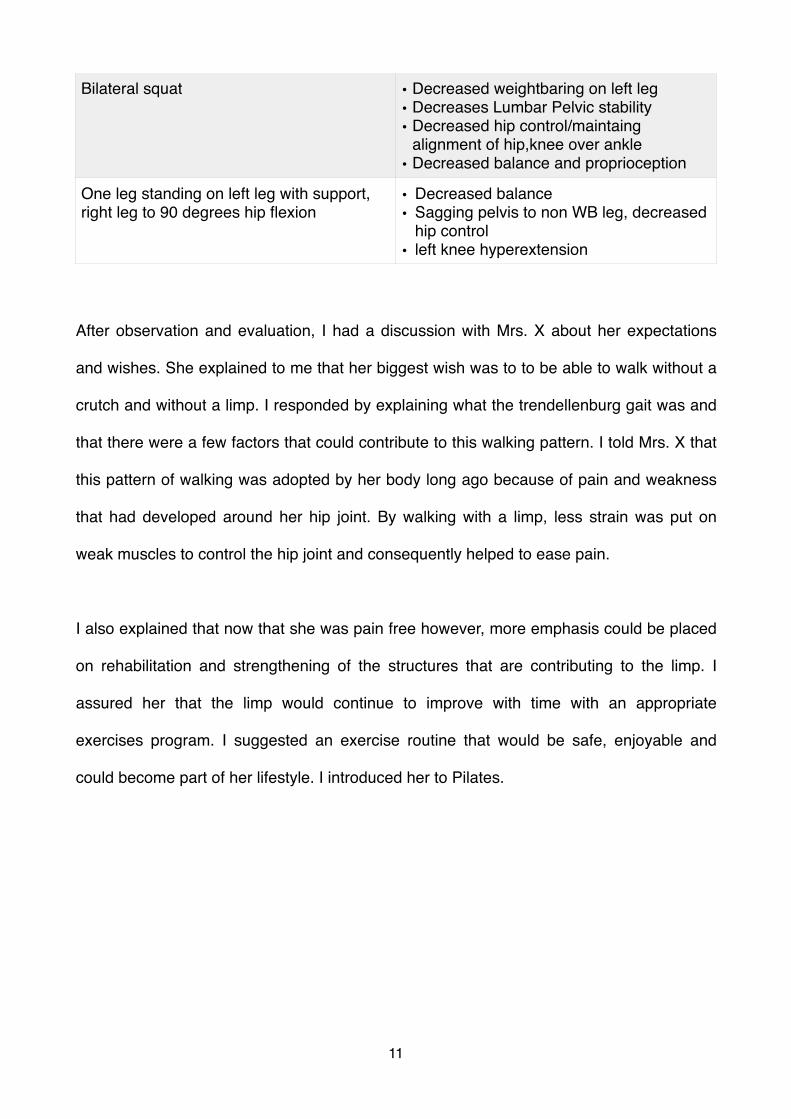
Bilateral squat • Decreased weightbaring on left leg• Decreases Lumbar Pelvic stability• Decreased hip control/maintaing
alignment of hip,knee over ankle • Decreased balance and proprioception
One leg standing on left leg with support, right leg to 90 degrees hip flexion
• Decreased balance• Sagging pelvis to non WB leg, decreased
hip control• left knee hyperextension
�11
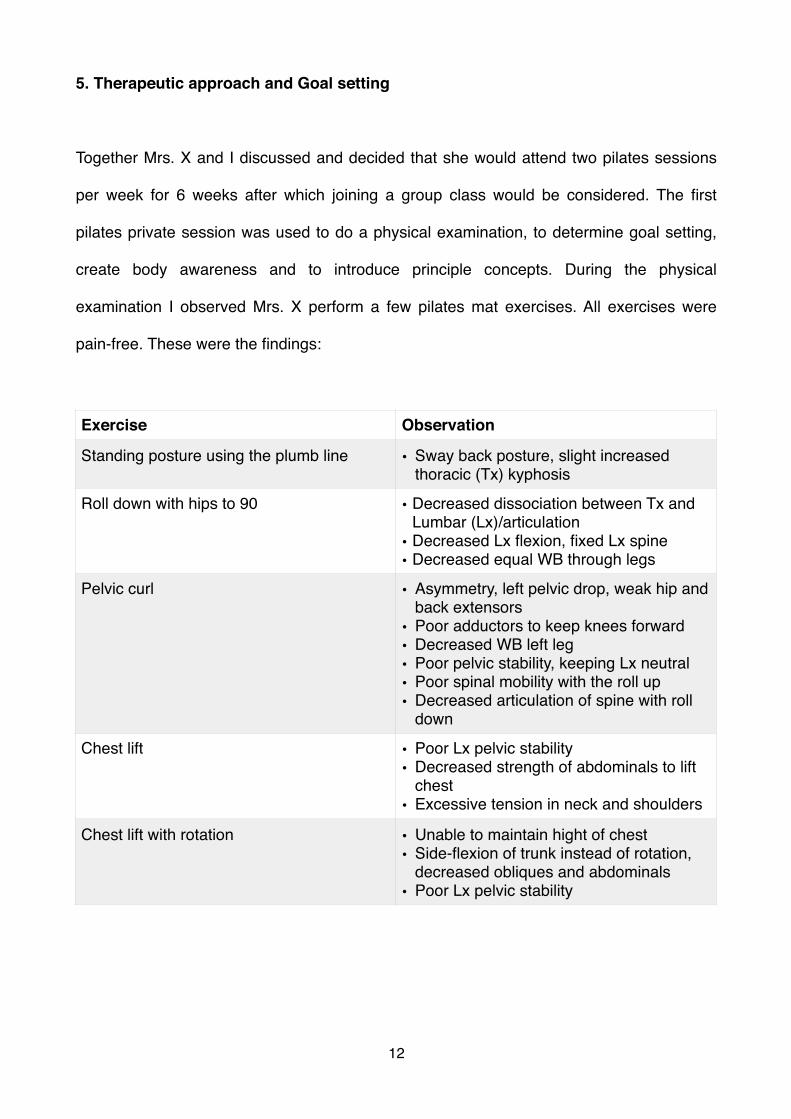
5. Therapeutic approach and Goal setting
Together Mrs. X and I discussed and decided that she would attend two pilates sessions
per week for 6 weeks after which joining a group class would be considered. The first
pilates private session was used to do a physical examination, to determine goal setting,
create body awareness and to introduce principle concepts. During the physical
examination I observed Mrs. X perform a few pilates mat exercises. All exercises were
pain-free. These were the findings:
Exercise Observation
Standing posture using the plumb line • Sway back posture, slight increased thoracic (Tx) kyphosis
Roll down with hips to 90 • Decreased dissociation between Tx and Lumbar (Lx)/articulation
• Decreased Lx flexion, fixed Lx spine• Decreased equal WB through legs
Pelvic curl • Asymmetry, left pelvic drop, weak hip and back extensors
• Poor adductors to keep knees forward• Decreased WB left leg• Poor pelvic stability, keeping Lx neutral• Poor spinal mobility with the roll up• Decreased articulation of spine with roll
down
Chest lift • Poor Lx pelvic stability• Decreased strength of abdominals to lift
chest• Excessive tension in neck and shoulders
Chest lift with rotation • Unable to maintain hight of chest• Side-flexion of trunk instead of rotation,
decreased obliques and abdominals• Poor Lx pelvic stability
�12
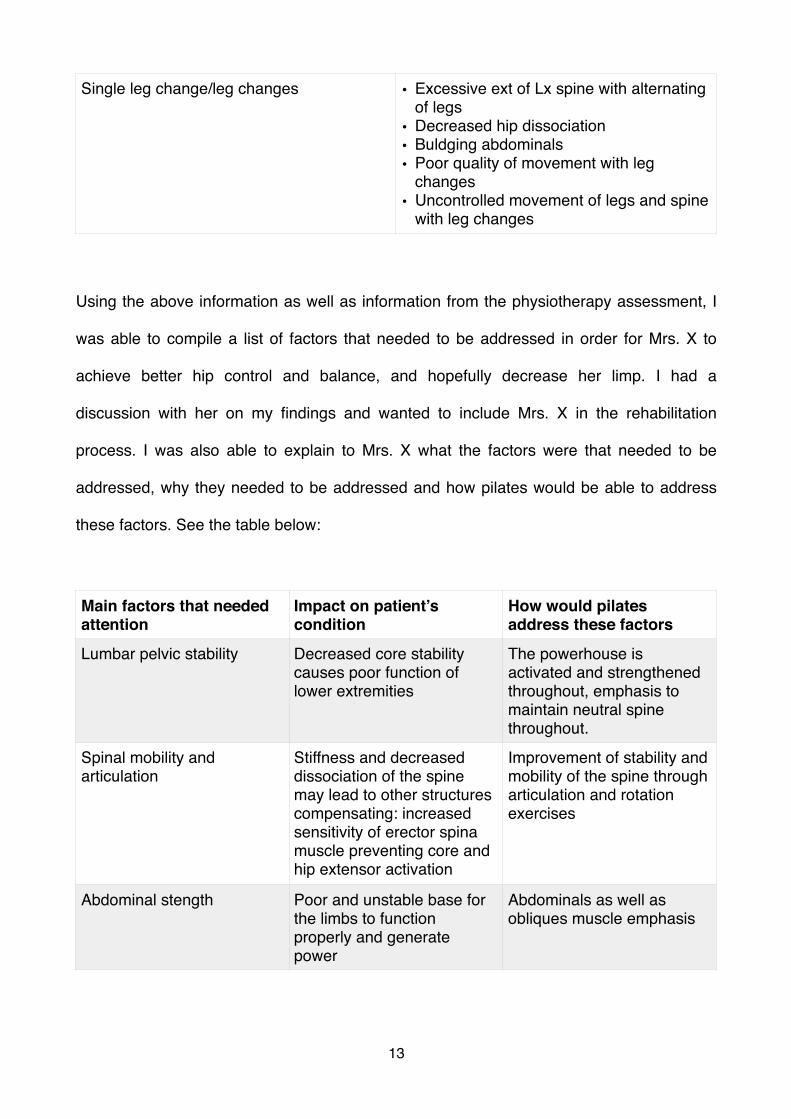
Using the above information as well as information from the physiotherapy assessment, I
was able to compile a list of factors that needed to be addressed in order for Mrs. X to
achieve better hip control and balance, and hopefully decrease her limp. I had a
discussion with her on my findings and wanted to include Mrs. X in the rehabilitation
process. I was also able to explain to Mrs. X what the factors were that needed to be
addressed, why they needed to be addressed and how pilates would be able to address
these factors. See the table below:
Single leg change/leg changes • Excessive ext of Lx spine with alternating of legs
• Decreased hip dissociation• Buldging abdominals• Poor quality of movement with leg
changes• Uncontrolled movement of legs and spine
with leg changes
Main factors that needed attention
Impact on patient’s condition
How would pilates address these factors
Lumbar pelvic stability Decreased core stability causes poor function of lower extremities
The powerhouse is activated and strengthened throughout, emphasis to maintain neutral spine throughout.
Spinal mobility and articulation
Stiffness and decreased dissociation of the spine may lead to other structures compensating: increased sensitivity of erector spina muscle preventing core and hip extensor activation
Improvement of stability and mobility of the spine through articulation and rotation exercises
Abdominal stength Poor and unstable base for the limbs to function properly and generate power
Abdominals as well as obliques muscle emphasis
�13
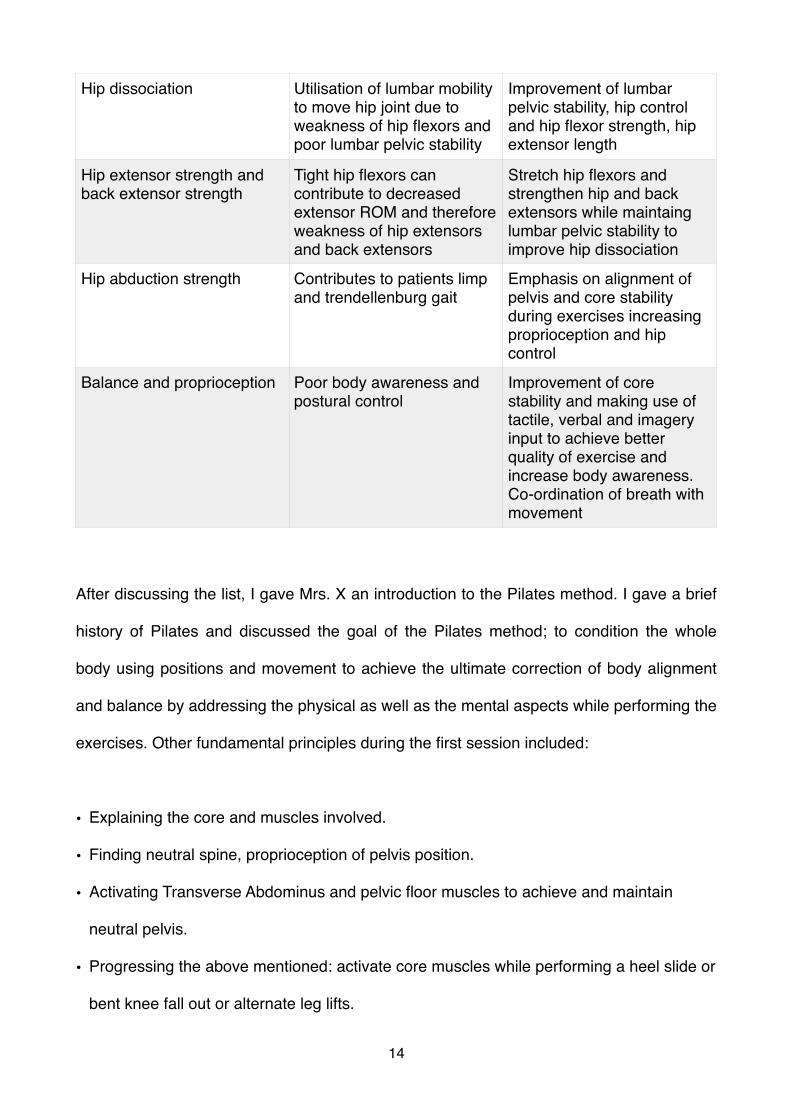
After discussing the list, I gave Mrs. X an introduction to the Pilates method. I gave a brief
history of Pilates and discussed the goal of the Pilates method; to condition the whole
body using positions and movement to achieve the ultimate correction of body alignment
and balance by addressing the physical as well as the mental aspects while performing the
exercises. Other fundamental principles during the first session included:
• Explaining the core and muscles involved.
• Finding neutral spine, proprioception of pelvis position.
• Activating Transverse Abdominus and pelvic floor muscles to achieve and maintain
neutral pelvis.
• Progressing the above mentioned: activate core muscles while performing a heel slide or
bent knee fall out or alternate leg lifts.
Hip dissociation Utilisation of lumbar mobility to move hip joint due to weakness of hip flexors and poor lumbar pelvic stability
Improvement of lumbar pelvic stability, hip control and hip flexor strength, hip extensor length
Hip extensor strength and back extensor strength
Tight hip flexors can contribute to decreased extensor ROM and therefore weakness of hip extensors and back extensors
Stretch hip flexors and strengthen hip and back extensors while maintaing lumbar pelvic stability to improve hip dissociation
Hip abduction strength Contributes to patients limp and trendellenburg gait
Emphasis on alignment of pelvis and core stability during exercises increasing proprioception and hip control
Balance and proprioception Poor body awareness and postural control
Improvement of core stability and making use of tactile, verbal and imagery input to achieve better quality of exercise and increase body awareness. Co-ordination of breath with movement
�14

• Addressed lateral breathing pattern while maintaining neutral pelvis and spine using a
theraband.
• What does “imprinting the spine” mean and how to achieve this, i.e. slight post tilt of the
pelvis.
• Improve standing posture, improve body awareness using a mirror.
6. Conditioning program
The Plates conditioning program was started at 6 weeks post operatively. The conditioning
program consisted of 6 weeks with private one on one sessions after which Mrs. X could
possibly join a pilates class if her progression was satisfactory. During the next 6 weeks
strong emphasis was placed on protecting the hip replacement joint on request of the
surgeon. This included:
• No exercise to be performed with pain or discomfort at groin site.
• No adduction of the left hip.
• No internal rotation or twisting on the left leg.
• No bending of left hip to more than 90 degrees.
It was important to maintain a slow pace, with the goal to introduce Mrs. X to pilates and in
order for her to master the fundamental principles of Pilates before introducing her to more
challenging exercises and concepts. The intensity, endurance and pace was increased as
Mrs. X became functionally stronger. Constant feedback was required from Mrs. X in terms
of pain and discomfort to modify exercises accordingly.
�15
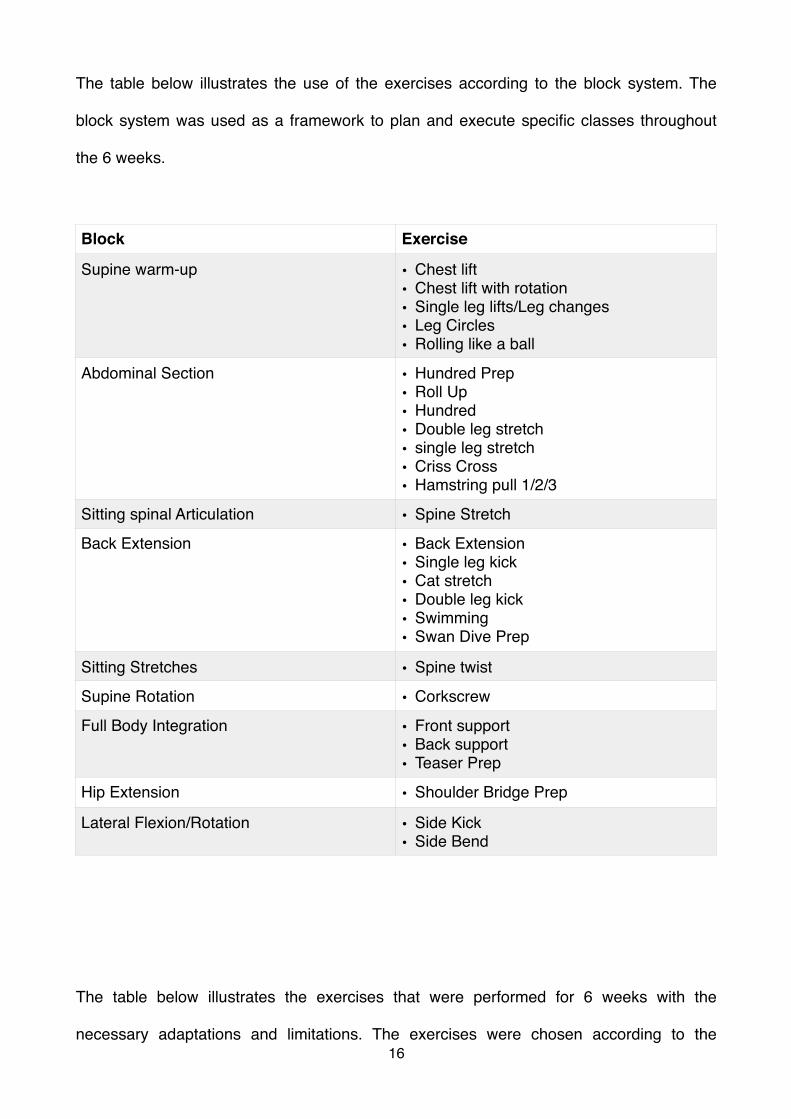
The table below illustrates the use of the exercises according to the block system. The
block system was used as a framework to plan and execute specific classes throughout
the 6 weeks.
The table below illustrates the exercises that were performed for 6 weeks with the
necessary adaptations and limitations. The exercises were chosen according to the
Block Exercise
Supine warm-up • Chest lift• Chest lift with rotation• Single leg lifts/Leg changes• Leg Circles• Rolling like a ball
Abdominal Section • Hundred Prep• Roll Up• Hundred• Double leg stretch• single leg stretch• Criss Cross• Hamstring pull 1/2/3
Sitting spinal Articulation • Spine Stretch
Back Extension • Back Extension• Single leg kick• Cat stretch• Double leg kick• Swimming• Swan Dive Prep
Sitting Stretches • Spine twist
Supine Rotation • Corkscrew
Full Body Integration • Front support• Back support• Teaser Prep
Hip Extension • Shoulder Bridge Prep
Lateral Flexion/Rotation • Side Kick• Side Bend
�16
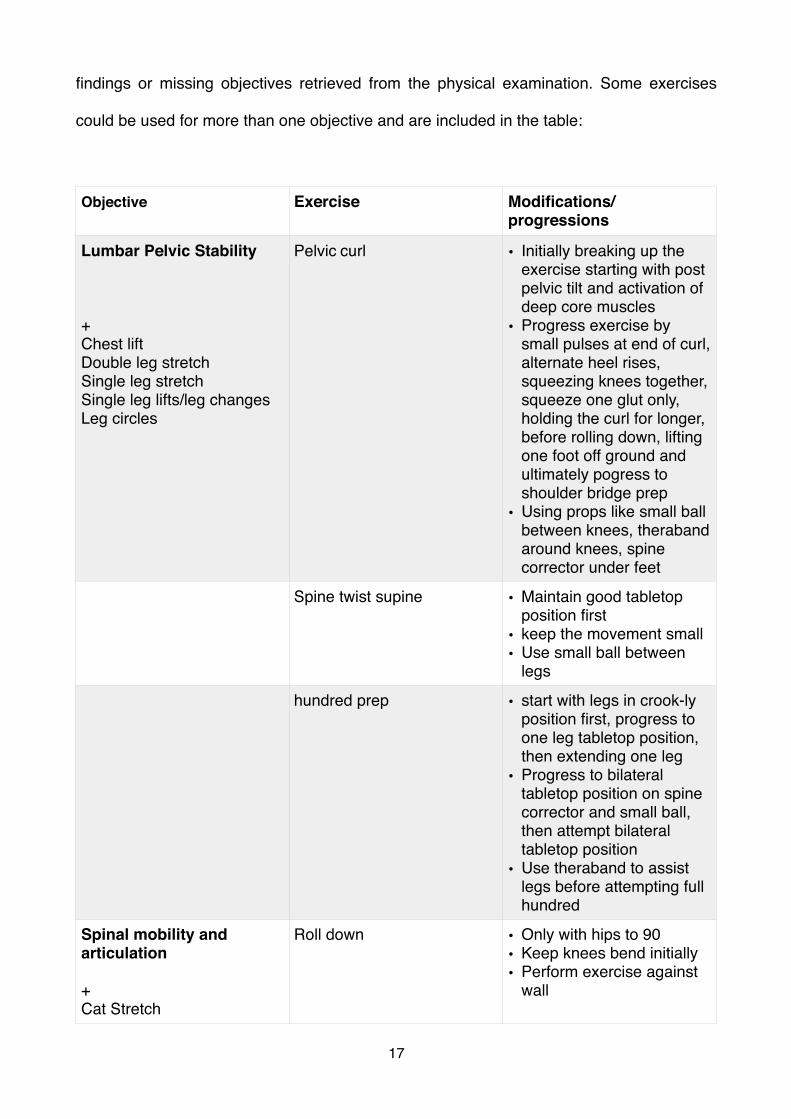
findings or missing objectives retrieved from the physical examination. Some exercises
could be used for more than one objective and are included in the table:
Objective Exercise Modifications/progressions
Lumbar Pelvic Stability
+Chest liftDouble leg stretchSingle leg stretchSingle leg lifts/leg changesLeg circles
Pelvic curl • Initially breaking up the exercise starting with post pelvic tilt and activation of deep core muscles
• Progress exercise by small pulses at end of curl, alternate heel rises, squeezing knees together, squeeze one glut only, holding the curl for longer, before rolling down, lifting one foot off ground and ultimately pogress to shoulder bridge prep
• Using props like small ball between knees, theraband around knees, spine corrector under feet
Spine twist supine • Maintain good tabletop position first
• keep the movement small• Use small ball between
legs
hundred prep • start with legs in crook-ly position first, progress to one leg tabletop position, then extending one leg
• Progress to bilateral tabletop position on spine corrector and small ball, then attempt bilateral tabletop position
• Use theraband to assist legs before attempting full hundred
Spinal mobility and articulation
+Cat Stretch
Roll down • Only with hips to 90• Keep knees bend initially• Perform exercise against
wall
�17
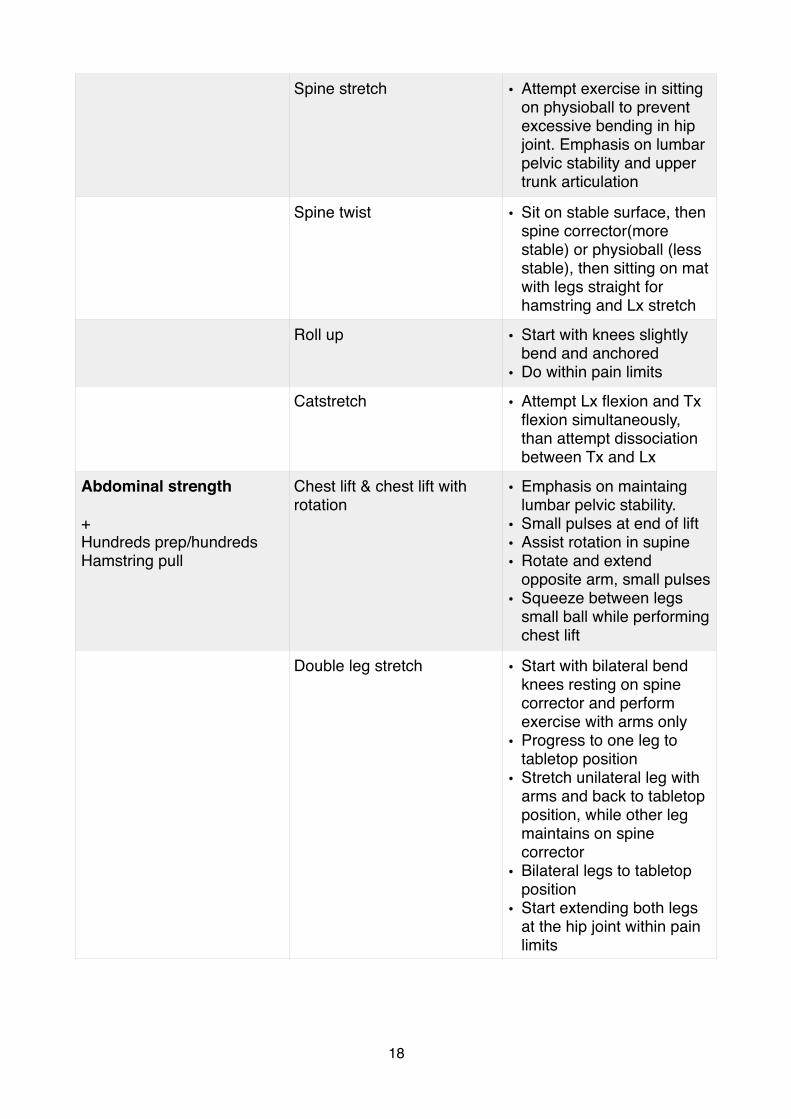
Spine stretch • Attempt exercise in sitting on physioball to prevent excessive bending in hip joint. Emphasis on lumbar pelvic stability and upper trunk articulation
Spine twist • Sit on stable surface, then spine corrector(more stable) or physioball (less stable), then sitting on mat with legs straight for hamstring and Lx stretch
Roll up • Start with knees slightly bend and anchored
• Do within pain limits
Catstretch • Attempt Lx flexion and Tx flexion simultaneously, than attempt dissociation between Tx and Lx
Abdominal strength
+Hundreds prep/hundredsHamstring pull
Chest lift & chest lift with rotation
• Emphasis on maintaing lumbar pelvic stability.
• Small pulses at end of lift• Assist rotation in supine• Rotate and extend
opposite arm, small pulses• Squeeze between legs
small ball while performing chest lift
Double leg stretch • Start with bilateral bend knees resting on spine corrector and perform exercise with arms only
• Progress to one leg to tabletop position
• Stretch unilateral leg with arms and back to tabletop position, while other leg maintains on spine corrector
• Bilateral legs to tabletop position
• Start extending both legs at the hip joint within pain limits
�18
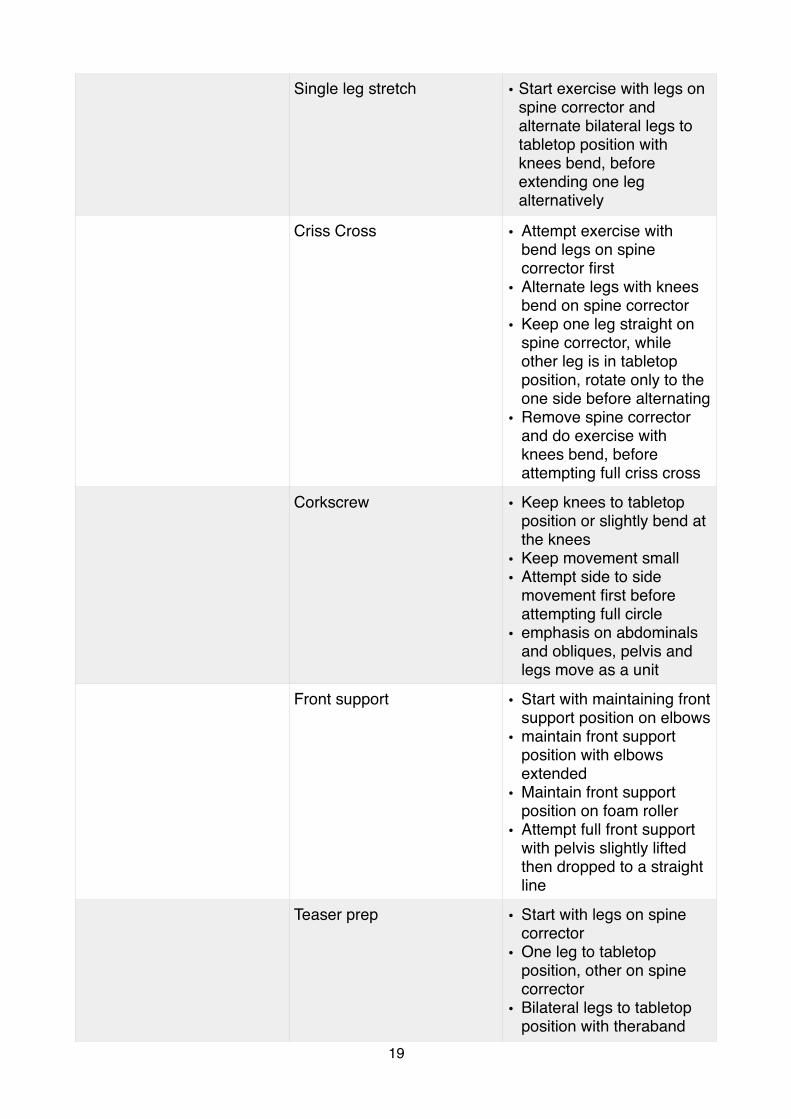
Single leg stretch • Start exercise with legs on spine corrector and alternate bilateral legs to tabletop position with knees bend, before extending one leg alternatively
Criss Cross • Attempt exercise with bend legs on spine corrector first
• Alternate legs with knees bend on spine corrector
• Keep one leg straight on spine corrector, while other leg is in tabletop position, rotate only to the one side before alternating
• Remove spine corrector and do exercise with knees bend, before attempting full criss cross
Corkscrew • Keep knees to tabletop position or slightly bend at the knees
• Keep movement small• Attempt side to side
movement first before attempting full circle
• emphasis on abdominals and obliques, pelvis and legs move as a unit
Front support • Start with maintaining front support position on elbows
• maintain front support position with elbows extended
• Maintain front support position on foam roller
• Attempt full front support with pelvis slightly lifted then dropped to a straight line
Teaser prep • Start with legs on spine corrector
• One leg to tabletop position, other on spine corrector
• Bilateral legs to tabletop position with theraband
�19
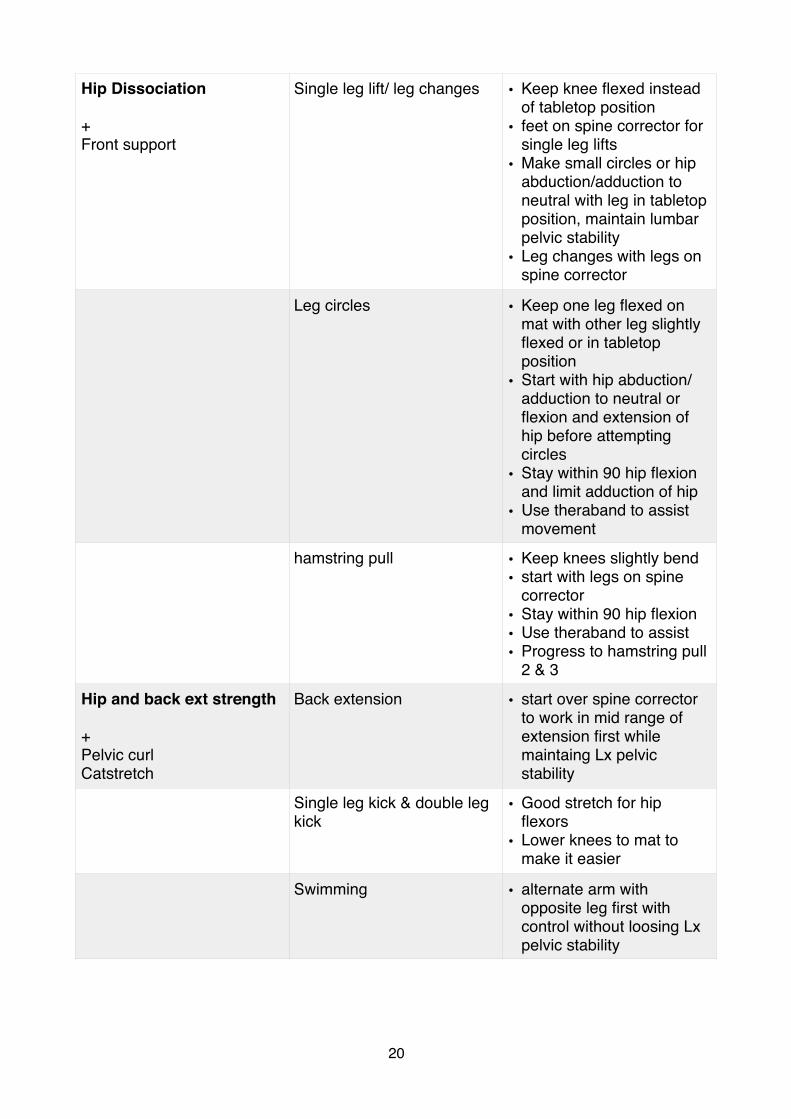
Hip Dissociation
+Front support
Single leg lift/ leg changes • Keep knee flexed instead of tabletop position
• feet on spine corrector for single leg lifts
• Make small circles or hip abduction/adduction to neutral with leg in tabletop position, maintain lumbar pelvic stability
• Leg changes with legs on spine corrector
Leg circles • Keep one leg flexed on mat with other leg slightly flexed or in tabletop position
• Start with hip abduction/adduction to neutral or flexion and extension of hip before attempting circles
• Stay within 90 hip flexion and limit adduction of hip
• Use theraband to assist movement
hamstring pull • Keep knees slightly bend• start with legs on spine
corrector• Stay within 90 hip flexion• Use theraband to assist• Progress to hamstring pull
2 & 3
Hip and back ext strength
+Pelvic curlCatstretch
Back extension • start over spine corrector to work in mid range of extension first while maintaing Lx pelvic stability
Single leg kick & double leg kick
• Good stretch for hip flexors
• Lower knees to mat to make it easier
Swimming • alternate arm with opposite leg first with control without loosing Lx pelvic stability
�20
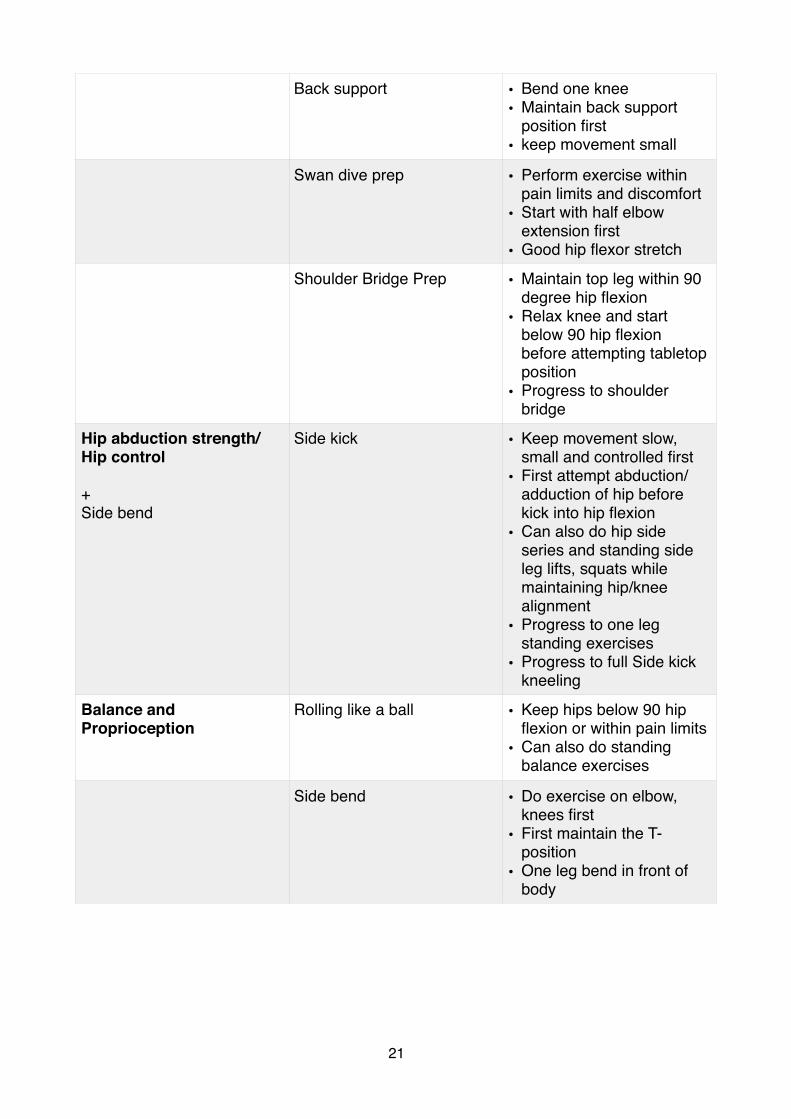
Back support • Bend one knee• Maintain back support
position first• keep movement small
Swan dive prep • Perform exercise within pain limits and discomfort
• Start with half elbow extension first
• Good hip flexor stretch
Shoulder Bridge Prep • Maintain top leg within 90 degree hip flexion
• Relax knee and start below 90 hip flexion before attempting tabletop position
• Progress to shoulder bridge
Hip abduction strength/Hip control
+Side bend
Side kick • Keep movement slow, small and controlled first
• First attempt abduction/adduction of hip before kick into hip flexion
• Can also do hip side series and standing side leg lifts, squats while maintaining hip/knee alignment
• Progress to one leg standing exercises
• Progress to full Side kick kneeling
Balance and Proprioception
Rolling like a ball • Keep hips below 90 hip flexion or within pain limits
• Can also do standing balance exercises
Side bend • Do exercise on elbow, knees first
• First maintain the T-position
• One leg bend in front of body
�21
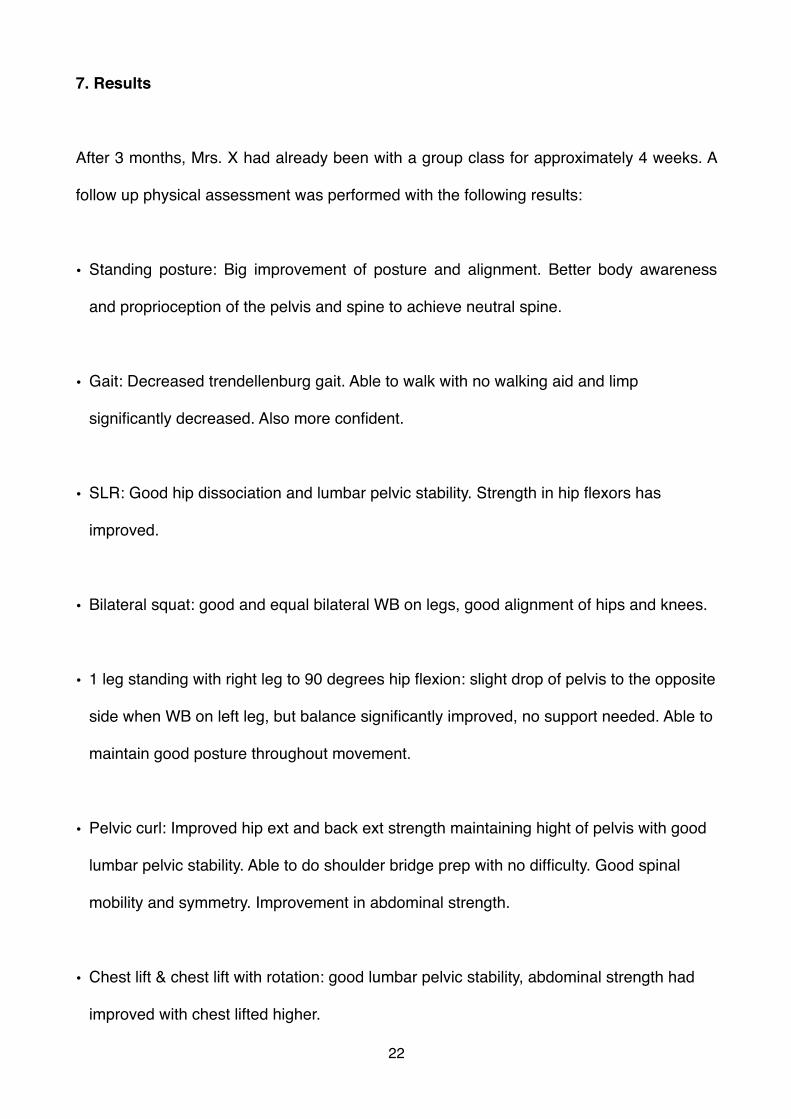
7. Results
After 3 months, Mrs. X had already been with a group class for approximately 4 weeks. A
follow up physical assessment was performed with the following results:
• Standing posture: Big improvement of posture and alignment. Better body awareness
and proprioception of the pelvis and spine to achieve neutral spine.
• Gait: Decreased trendellenburg gait. Able to walk with no walking aid and limp
significantly decreased. Also more confident.
• SLR: Good hip dissociation and lumbar pelvic stability. Strength in hip flexors has
improved.
• Bilateral squat: good and equal bilateral WB on legs, good alignment of hips and knees.
• 1 leg standing with right leg to 90 degrees hip flexion: slight drop of pelvis to the opposite
side when WB on left leg, but balance significantly improved, no support needed. Able to
maintain good posture throughout movement.
• Pelvic curl: Improved hip ext and back ext strength maintaining hight of pelvis with good
lumbar pelvic stability. Able to do shoulder bridge prep with no difficulty. Good spinal
mobility and symmetry. Improvement in abdominal strength.
• Chest lift & chest lift with rotation: good lumbar pelvic stability, abdominal strength had
improved with chest lifted higher.
�22

• Leg changes: Good hip dissociation and lumbar pelvic stability, better control of exercise
8. Conclusion
The trendellenburg gait and limp is a common side effect post THR surgery. One of the
factors that could be responsible for this dysfunctional walking pattern is weakness of the
muscles surrounding the hip complex providing control, balance and proprioception in the
hip joint. These muscles mainly include the hip abductors and extensors, but core
stabilizers also play a role. Weakness could be due recurrent pain and inflammation in the
joint after surgery or could be due to weakness even before the operation.
In this case report, Pilates as an exercise routine was used to improve functional ability as
a whole by addressing lumbar pelvic stability, spinal mobility and articulation, abdominal
strength, hip dissociation, hip and back extensor strength, hip abduction strength and
balance and proprioception. Pilates develops stabilization, refines posture, and re-
educates movement patterns that previously caused disability. Pilates also influences body
awareness and control of movement to ensure that the body is addressed as a whole.
To conclude, improved abdominal strength and lumbar pelvic stability could lead to a more
stable base from which the lower limbs including the hip joint can generate power from.
Furthermore, good proximal stability could increase hip control and decrease the
trendellenburg gait to improve overall functional performance after a THR .
�23
9. References
Articles:
• Levine B, Kaplanek B, Jaffe WL. Pilates training for use in rehabilitation after total hip
and knee arhroplasty. A preliminary report. Clinical Orthopaedic Related Research.
2009;467:1468-1475
• Gilbey HJ. Exercise improves early functional recovery after total hip arthroplasty
(Abstract). CORR No 2003;408:193-200
• Levine B, Kaplanek B, Scafura D, Jaffe WL. Rehabilitation after total hip and knee
arthroplasty. A new regime using Pilates training. Bulletin of the NYU Hospital for Joint
Disease. 2007;65(2):120-125
• Byrne DP, Mulhall KJ, Baker JF. Anatomy and Biomechanics of the Hip. The open Sport
Medicine Journal. 2010;4:51-57
• Lutwic A, Edwards M, Dennison E, Cooper C. Epidemiology and Burden of
Osteoarthritis. Br Med Bull. 2013;105:185-199
• Murphy LB, Helmick CG, Schwartz TA, Renner JB, Tudor G, Koch GG, Dragomir AD,
Kalsbeek WD, Luta G, Jordan JM. One in 4 people may develop symptomatic hip
osteoarthritis in his or her lifetime. (Abstract). Osteoarthritis Cartilage. 2010;18(11):
1372-1379
�24
• MacDonald Wood A, Brock TM, Heil K, Holmes R, Weusten A. A Review of the
Management of Hip and Knee Osteoarthritis. International Journal of Chronic Disease.
2013;Article ID:845015
• Trudelle Jackson E. Effects of a late phase exercise program after total hip arthroplasty.
A randomised controlled trial. Arc Phys Med Rehabill. 2004;85(7):1056-1062
Other:
• Basi Study Guide (Mat Work Course)
• Basi Mat (Movement Analysis Workbook)
�25