a decade of innovation 2006 in chronic diseases...
TRANSCRIPT

A Decade of Innovation in Chronic Diseases
20062016
A Decade of Innovation in Chronic Diseases

A Decade of Innovation in Chronic Diseases

3PhRMA 2016 |
A Decade of Innovation in Chronic Diseases:2006-2016
4 Introduction
5 High Cholesterol: Meeting Unmet Needs for Patients
9 Diabetes: Better Management and Control
14 Mutiple Sclerosis: Expanded Treatment Options Improve Outcomes for a Disabling Chronic Condition
17 Rheumatoid Arthritis: An Improved Quality of Life, Never Before Seen
21 HIV/AIDS: Advances Continue to Improve Patients’ Lives
25 Hepatitis C: Breakthroughs Revolutionize Treatment for Patients
29 Continued Progress for Patients with Chronic Diseases
30 References

A Decade of Innovation in Chronic Diseases4
A Heavy Burden on Patients and Society
Chronic diseases are one of the most complex and important health care challenges of our time.
Generally regarded as health conditions lasting a year or more, chronic health conditions require ongoing medical attention and place considerable burden on both patients and caregivers. Chronic diseases encompass a broad range of illnesses that often limit the activities of daily life, have detrimental effects on quality of life, cause disability, disrupt families and often take the lives of loved ones.
Seven out of ten deaths in the United States are due to chronic health conditions and about half of all American adults—or 117 million people—have one or more of these conditions.1 The sizable prevalence of chronic illness is due in large part to the growing population of older adults in this country, as well as increases in life expectancy resulting from advances in public health and clinical medicine.2 In coming years, the prevalence of chronic diseases is expected to continue to grow with 157 million Americans projected to have more than one chronic condition by 2020.3
In addition to the profound clinical burden placed on patients and caregivers, chronic diseases also place a substantial strain on the health system and economy. Patients with chronic conditions are the most frequent users of medical care in the United States, accounting for 81% of hospital admissions and 76% of physician visits.4 The costs of treating patients with these conditions account for 86% of the nearly $3 trillion spent on health care in the U.S. each year.5 Not surprisingly, chronic diseases also result in productivity losses from missed work days, disability, and premature death.
With the burden of chronic disease on the rise in coming years, the crucial role that medicines play in treating illness, preventing unnecessary complications and allowing patients to enjoy healthier and more productive lives will prove increasingly important.
IntroductionA note on methodology: advances described over the past decade span the period beginning on January 1, 2006 and ending on December 31, 2015.
A Decade of Progress
In recent years we have seen the emergence of new treatment options which have had a profound impact on the lives of patients with chronic diseases. Comparing treatment options available ten years ago with those available today demonstrates the remarkable extent of this progress.
This report highlights several chronic health conditions where significant advances over the past decade have improved a variety of patient outcomes. The diverse group of conditions examined here—including high cholesterol, diabetes, multiple sclerosis, rheumatoid arthritis, HIV/AIDS, and hepatitis C—demonstrate a number of common themes:
• In many chronic diseases, individual patients respond to various medications differently and responses can vary over time. For these reasons, therapeutic advances that offer patients a broad range of options are critically important in helping patients find appropriate and effective treatments for chronic illness.
• Chronic diseases are often lifelong conditions requiring diligent management and careful adherence to prescribed treatment regimens. Treatment options which eliminate barriers to patient compliance are crucial to successful chronic disease management.
• Despite tremendous progress, there remains significant unmet medical need in many chronic disease areas—particularly given the many subcategories and varied patient populations that comprise these conditions.
The therapeutic advances examined in this report are helping patients avoid serious disease complications and hospitalizations, preventing disability, improving quality of life, and, most importantly, extending lives. As the prevalence of chronic illness grows in coming years, these treatment advances, and those to come, will continue to play a central role in alleviating substantial burden for patients and caregivers, as well as the health care system as a whole.

5PhRMA 2016 |
Cholesterol is a waxy, fat-like substance found in all cells of the body and is needed to perform many necessary functions. However, too much of low-density lipoprotein cholesterol (LDL-C) in the blood—otherwise known as “bad” cholesterol—can lead to a condition known as atherosclerosis in which plaque builds up in and narrows the walls of the arteries. This makes it increasingly difficult for blood to flow through the body, potentially leading to heart attack, stroke or other serious cardiac events.11 CVD is most often driven by this condition.12
QUICK FACTS: • Over 100 million Americans have high cholesterol.6
• High cholesterol is a major risk factor for cardiovascular disease (CVD), which remains the leading cause of death in the United States.7,8
• Nearly 800,000 Americans die each year from cardiovascular diseases, accounting for 1 in 3 deaths. Every 43 seconds, someone in the United States has a heart attack.9
• In some patients, high cholesterol is linked to a genetic condition known as familial hypercholesterolemia.10
Some patients have extremely high levels of cholesterol due to a condition known as familial hypercholesterolemia (FH). Those with FH face a significantly greater risk of developing CVD and related complications, even at an early age. FH is an inherited disease associated with mutations in the LDL receptor gene, which ultimately result in increases in the levels of LDL in the blood. The type of FH an individual has depends on whether they have inherited a mutated form of the receptor gene from one or both parents:
High Cholesterol: Meeting Unmet Needs for Patients
The introduction of statin therapy nearly 30 years ago transformed the treatment of high cholesterol for many patients, yet some continued to face challenges. Advances over the past decade have provided important treatment options for these patients.

A Decade of Innovation in Chronic Diseases6
• Heterozygous FH (HeFH): Those with HeFH have inherited a genetic mutation involved in FH from one parent. The condition affects approximately 1.5 million Americans. The mean age of onset of CVD for males with HeFH is 42 to 46 years and 51 to 52 years for women.13, 14, 15
• Homozygous FH (HoFH): Those with HoFH have inherited an FH-associated genetic mutation from both parents. The condition is less common but more severe than HeFH and affects approximately 2,000 Americans.16 The mean age of diagnosis of CVD in HoFH patients is just 20 years of age.17
Lowering cholesterol levels can reduce the risk of developing CVD and related adverse events—including heart attack, stroke and death.18 For many patients, lifestyle changes, such as eating healthy and exercising, are sufficient to lower cholesterol to targeted treatment goals. A number of therapeutic options are also available to help patients gain better control over cholesterol levels.
A Decade Ago: Widely Effective Treatment Options Available but Unmet Need Remained
In addition to diet and exercise, a number of effective therapeutic options were available to patients a decade ago which offered to help control high cholesterol. The introduction of statin therapy in the late 1980s revolutionized treatment and contributed greatly to reductions in prevalence of high cholesterol.19 By the early 2000s, several statin therapies were available that offered patients cholesterol reductions ranging from 30-50%*.20
Additionally, a number of other cholesterol lowering agents were available to patients—including cholesterol absorption
inhibitors, bile acid sequestrants and niacin—each of which may have been used individually or as adjunctive therapy along with statins to achieve greater reductions in cholesterol levels.21, 22, 23
For the vast majority of patients, available treatment options were effective in reducing cholesterol to targeted treatment goals. Still, others continued to struggle, particularly those with cholesterol levels ranging as high as 2-5 times greater than a healthy individual, as is often the case for those with FH.24, 25 For these patients, available medicines were often insufficient to achieve targeted cholesterol reductions, and they continued to face considerable risk of experiencing a cardiac event.26,27
Some patients sought to manage their condition with a procedure known as LDL apheresis, in which blood is pumped through a machine designed to remove unwanted cholesterol. Although effective for some patients, the procedure was not widely available. Further, LDL apheresis was performed in hospitals, requiring recurrent treatment every few weeks.28, 29 Even with the procedure, many still were unable to achieve targeted reductions.30
Today: Advances in Treatment Provide Critical Options for Patients
Patients with high cholesterol today continue to benefit from the mainstays of treatment but have new options available to them if standard options are insufficient to meet treatment goals. Statins remain the basis of most treatment regimens. But for those previously unable to achieve targeted cholesterol reductions with available treatment options, four additional medicines, representing three entirely new drug classes, have become available over the past decade to help patients achieve
* Depending on which statin and the intensity of treatment

7PhRMA 2016 |
additional LDL-C reductions. Each of these treatments has contributed to the arsenal of medicines available to patients struggling to manage cholesterol levels.
Two first-in-class medicines treating the rarest and most severe form of FH, HoFH, were approved by the U.S. Food and Drug Administration (FDA) in 2012 and 2013, marking significant advancements for patients with this life-threatening condition. Both of these medicines work by impairing the creation of the lipid particles that lead to the production of bad cholesterol.31 The first approved medicine, lomitapide, is a microsomal triglyceride transfer protein (MTP) inhibitor, which is a once daily capsule taken in combination with a low-fat diet and other lipid-lowering treatments, such as statins and, when possible, LDL apheresis. The medicine has been shown to reduce cholesterol levels in HoFH patients by an average of 50%.32 In 2013, FDA also approved mipomersen sodium—known as an oligonucleotide inhibitor of apo B-100 synthesis. Also taken in combination with other lipid-lowering agents and a cholesterol-lowering diet, mipomersen sodium is injected once daily and has been shown to reduce cholesterol by 25%.33 By allowing patients to better manage their cholesterol levels, lomitapide and mipomersen are providing important treatment options for this rare and extremely life-threatening condition which can lead to heart attack or death by age 30.34
Treatment options to combat high cholesterol expanded again in 2015 with the introduction of two medicines from a new class called PCSK9 inhibitors. The medicines are monoclonal antibodies designed to inhibit the proprotein convertase subtilisin/kesin 9 (PCSK9), a protein that reduces the liver’s ability to breakdown bad cholesterol. The protein was not discovered until 2003, after which research progressed quickly to develop new treatments to inhibit the protein.35 PCSK9 inhibitors work in combination with statins, with each medicine targeting a different mechanism in the liver, together producing pronounced effects.36
The first PCSK9—alirocumab—was approved by the FDA in July of 2015 for the treatment of patients with the more common form of FH, HeFH, and also for those with known atherosclerosis-driven heart disease who require additional lowering of cholesterol. Alirocumab is a self-administered injection with dosing required every 2 weeks and is taken in conjunction with maximally tolerated dosing of statin therapy. The medicine has been shown to reduce cholesterol by an average of 36-59% in patients.37, 38
Following shortly thereafter, the FDA approved evolocumab in August 2015. The medicine was also indicated for the treatment of patients with HeFH and those with known
atherosclerosis-driven heart disease who require additional reductions in cholesterol. Additionally, evolocumab was approved for the treatment of patients with the rarer form of FH, HoFH, who require additional cholesterol reductions. The medicine is a self-administered injection with dosing required either every 2 or 4 weeks. When used in combination with a healthy diet and maximally tolerated dosing of statin therapy, evolocumab was found to reduce cholesterol in HeFH patients by 54-77%. For patients with HoFH, evolocumab in addition to a healthy diet and other cholesterol lowering treatments—including statins, cholesterol absorption inhibitors and LDL apheresis—has been found to reduce cholesterol by approximately 30%.39, 40
In addition to these major advances, researchers have continued to develop additional statin treatment options for high cholesterol patients with unmet needs. Some statins cannot be taken at all, or must be limited in dose when taken with other common medications—including some cardiovascular medications or HIV antiviral medications—due to the potential for drug interactions. In 2009, the FDA approved pitavastatin to treat patients with abnormal cholesterol levels despite diet and exercise.41 Pitavastatin is less likely to interact with certain drugs because it is minimally dependent on a common metabolic pathway in the liver.42 For those unable to take other statins due to potentially dangerous drug interactions and who are unable to manage their cholesterol levels with diet and exercise alone, the availability of pitavastatin represents an important advance.43
Research Continues to Focus on Unmet Need
Today, patients—including those with dangerously high cholesterol levels resulting from FH—have treatment options available to help them adequately manage their cholesterol. But treatment continues to evolve as researchers seek to meet the needs of patients who struggle with this condition.
“With this new class of drugs [PCSK9 inhibitors], you’re effectively curing the disease.”
–John Kastelein, M.D., Ph.D., Chair of Genetics in Cardiovascular Disease, University of
Amsterdam44

A Decade of Innovation in Chronic Diseases8
Then
• In addition to diet and exercise, most patients were able to manage cholesterol with statin therapy which offered patient cholesterol reductions ranging from 30-50%.
• Other cholesterol lowering agents were also available to patients which may have been used individually or as adjunctive therapy along with statins to achieve greater reductions in cholesterol levels.
• Some patients continued to struggle, particularly those with cholesterol levels ranging as high as 2-5 times greater than a healthy individual, which is often the case for those with Familial Hypercholesterolemia (FH), a genetic condition.
Now
• Patients continue to benefit from the mainstays of treatment, including statins and other lipid lowering agents.
• Patients with extremely high cholesterol levels—including those with FH—have 4 additional treatment options stemming from 3 entirely new classes of medicines, offering reductions in cholesterol ranging as high as 77%.
• There are 40 medicines currently in development to treat patients with high cholesterol, offering to further reduce substantial heart disease-related burden and mortality.
HIGH CHOLESTEROL
As heart disease remains the leading cause of death in the United States, providing treatments which help patients gain better control over cholesterol levels and the associated risk of heart attack and stroke will go a long way to alleviating this substantial burden.45
Evidence suggests that if all forms of CVD were eliminated, average life expectancy across the U.S. population would increase by 7 years.46 Providing effective treatments to help patients
better control CVD-related risk factors presents a tremendous opportunity to extend and improve the lives of patients.
Currently, there are 40 medicines in development aiming to provide important new treatment options for patients with high cholesterol.47 Looking forward, continuing to expand the availability of treatments to meet the needs of the more than 100 million Americans with high cholesterol will be critical to reducing the burden of CVD and CVD-associated mortality.

9PhRMA 2016 |
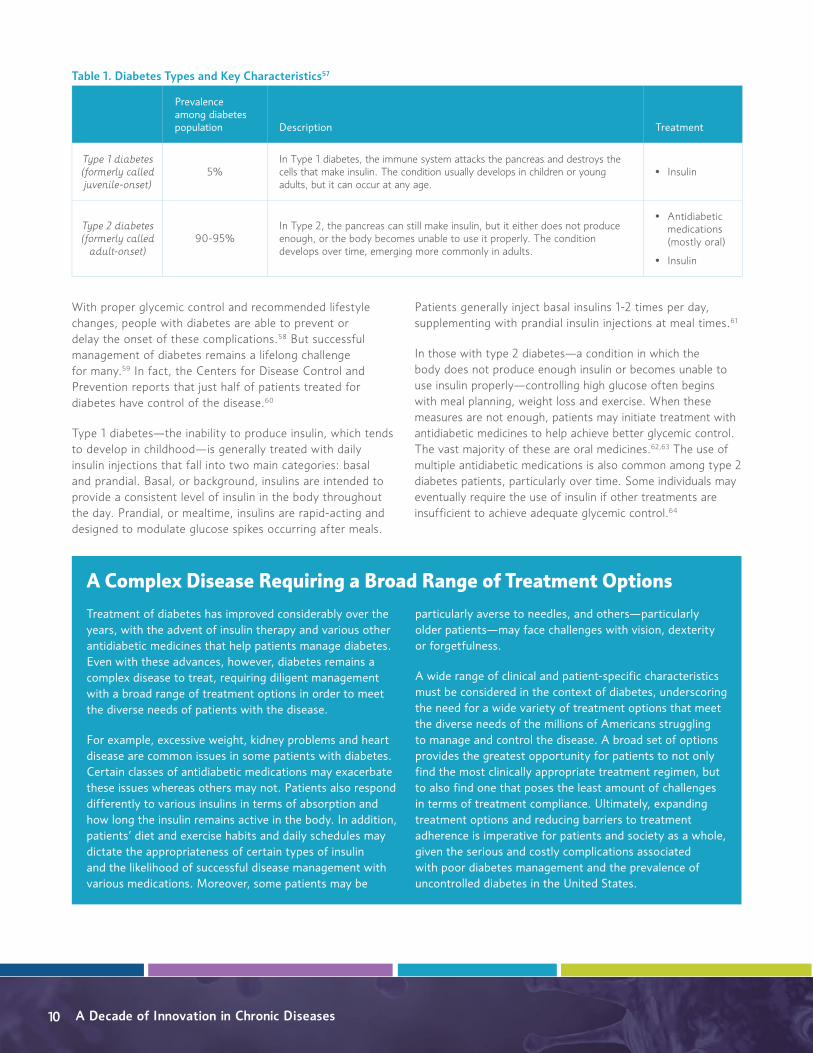
Diabetes is a chronic metabolic disorder caused by high glucose levels. Insulin is a hormone produced by the pancreas that signals the body’s cells to absorb glucose in the blood for energy. Without it, the body is unable to absorb glucose. There are two main types of diabetes, which are driven by different deficiencies in insulin production or use (See Table 1).53
The complications associated with diabetes are serious, disabling and often life-threatening. The risks of developing
these complications increase both over time and when blood glucose levels are poorly controlled. Extended periods of high glucose levels in the blood can damage the nerves and blood vessels leading to heart disease, general nerve damage (neuropathy), kidney disease (nephropathy), eye damage (retinopathy) and other disabling complications, such as foot or leg amputation. In fact, adults with diabetes are two to four times more likely to have a heart attack or stroke than adults without diabetes.54, 55, 56
Diabetes: Better Management and Control
Expanded treatment options over the past decade have reduced barriers to patient compliance and helped patients better manage diabetes and enjoy a better quality of life.
QUICK FACTS• More than 29 million Americans, or 9.3% of the population, have diabetes, and prevalence of the disease is
expected to double or triple over coming decades.48, 49
• People with diabetes may use insulin and/or other medicines to control the disease along with lifestyle changes.
• People with diabetes often face a number of complications that negatively impact their quality of life, including heart disease, kidney failure, vision or hearing loss, increased risk of infection and, in some situations, amputation.50, 51
• Diabetes remains the 7th leading cause of death in the United States.52
A Decade of Innovation in Chronic Diseases10
With proper glycemic control and recommended lifestyle changes, people with diabetes are able to prevent or delay the onset of these complications.58 But successful management of diabetes remains a lifelong challenge for many.59 In fact, the Centers for Disease Control and Prevention reports that just half of patients treated for diabetes have control of the disease.60
Type 1 diabetes—the inability to produce insulin, which tends to develop in childhood—is generally treated with daily insulin injections that fall into two main categories: basal and prandial. Basal, or background, insulins are intended to provide a consistent level of insulin in the body throughout the day. Prandial, or mealtime, insulins are rapid-acting and designed to modulate glucose spikes occurring after meals.
Patients generally inject basal insulins 1-2 times per day, supplementing with prandial insulin injections at meal times.61
In those with type 2 diabetes—a condition in which the body does not produce enough insulin or becomes unable to use insulin properly—controlling high glucose often begins with meal planning, weight loss and exercise. When these measures are not enough, patients may initiate treatment with antidiabetic medicines to help achieve better glycemic control. The vast majority of these are oral medicines.62,63 The use of multiple antidiabetic medications is also common among type 2 diabetes patients, particularly over time. Some individuals may eventually require the use of insulin if other treatments are insufficient to achieve adequate glycemic control.64
A Complex Disease Requiring a Broad Range of Treatment Options Treatment of diabetes has improved considerably over the years, with the advent of insulin therapy and various other antidiabetic medicines that help patients manage diabetes. Even with these advances, however, diabetes remains a complex disease to treat, requiring diligent management with a broad range of treatment options in order to meet the diverse needs of patients with the disease.
For example, excessive weight, kidney problems and heart disease are common issues in some patients with diabetes. Certain classes of antidiabetic medications may exacerbate these issues whereas others may not. Patients also respond differently to various insulins in terms of absorption and how long the insulin remains active in the body. In addition, patients’ diet and exercise habits and daily schedules may dictate the appropriateness of certain types of insulin and the likelihood of successful disease management with various medications. Moreover, some patients may be
particularly averse to needles, and others—particularly older patients—may face challenges with vision, dexterity or forgetfulness.
A wide range of clinical and patient-specific characteristics must be considered in the context of diabetes, underscoring the need for a wide variety of treatment options that meet the diverse needs of the millions of Americans struggling to manage and control the disease. A broad set of options provides the greatest opportunity for patients to not only find the most clinically appropriate treatment regimen, but to also find one that poses the least amount of challenges in terms of treatment compliance. Ultimately, expanding treatment options and reducing barriers to treatment adherence is imperative for patients and society as a whole, given the serious and costly complications associated with poor diabetes management and the prevalence of uncontrolled diabetes in the United States.
Table 1. Diabetes Types and Key Characteristics57
Prevalence among diabetes population Description Treatment
Type 1 diabetes(formerly called juvenile-onset)
5%In Type 1 diabetes, the immune system attacks the pancreas and destroys the cells that make insulin. The condition usually develops in children or young adults, but it can occur at any age.
• Insulin
Type 2 diabetes(formerly called
adult-onset)90-95%
In Type 2, the pancreas can still make insulin, but it either does not produce enough, or the body becomes unable to use it properly. The condition develops over time, emerging more commonly in adults.
• Antidiabetic medications (mostly oral)
• Insulin

11PhRMA 2016 |
A Decade Ago: Treatment Remained Complex and Challenging for Patients
A decade ago, patients with diabetes had a number of insulin options available, as well as oral and injected antidiabetic medications, to help manage both types of the disease. Many of these medicines continue to be widely used today. Yet an unmet need remained for those who struggled to achieve adequate glycemic control or faced challenges remaining adherent to available treatment regimens.
For patients with type 2 diabetes specifically, a number of options were available from a range of drug classes, each aiming to improve glycemic control through different disease mechanisms.† However, because type 2 diabetes is a progressive condition, most patients eventually require treatment with multiple medicines over time, often across multiple drug classes targeting different mechanisms of the disease. A decade ago, oral treatment options combining more than one medicine in one pill were limited, resulting in a high pill burden for patients. This burden contributed to treatment complexity and created challenges for patients in regards to adherence. For those requiring medications for other comorbid health conditions—common among patients with diabetes—the complexity of treatment regimens was additionally challenging.65, 66
For patients with types 1 and 2 diabetes who required the use of insulin, a number of both long-acting and mealtime
insulin options were available a decade ago. Long-acting insulins providing all-day coverage had just become available, and several premixed insulin options combining both long-term and mealtime coverage in the same formulation were options for some patients. In addition, insulin pens and insulin pumps were also being used, offering convenient delivery systems for some patients.67,
68, 69 Despite these advances, achieving adequate glycemic control remained a daily struggle for many, and the need remained for expanded, more convenient and improved treatment options to help meet the diverse needs of patients managing this challenging and complex disease.
Today: Continued Advances Facilitate Improved Disease Management
Over the past decade alone, more than 20 additional medicines have become available to meet the diverse needs of both type 1 and type 2 diabetes patients. Among these additions are two entirely new classes of oral therapies for type 2 diabetes and a broader range of oral combination therapies that reduce pill burden for patients. Importantly, four additional insulins for type 1 and type 2 have also become available—including two ultra-long-acting insulins as well as an inhaled insulin—each expanding treatment options for patients and providing greater convenience to help successfully manage the disease.70
† Common drug classes available included: sulfonylureas, biguanides, meglitinides, thiazolidinediones, GLP-1 receptor agonists, alpha-glucosidase inhibitors and bile acid sequestrants.

A Decade of Innovation in Chronic Diseases12
Advances in Type 2 Diabetes MedicinesThe first of a new class of oral medicines for type 2 diabetes called dipeptidyl peptidase 4 (DPP-4) inhibitors became available to patients in 2006 when the FDA approved sitagliptin phosphate, for use in combination with diet and exercise. DPP-4 inhibitors work by preventing the breakdown of glucagon-like peptide 1 (GLP-1), a naturally occurring compound that reduces glucose levels in the blood. DPP-4 inhibitors, and a previously approved class of medicines called GLP-1 receptor agonists, both target the same protein but they have different mechanisms of action. Because GLP-1 receptor agonists should not be used in patients with kidney problems, the addition of DPP-4 inhibitors provides an important new option for these patients.71 Moreover, whereas GLP-1 receptor agonists are injected, DPP-4 inhibitors are oral therapies, offering greater convenience for patients. Following the approval of sitagliptin phosphate, three additional DPP-4 inhibitors also joined this class: saxagliptin, linagliptin, and alogliptin.71, 72, 73, 74
Another class of oral medicines for type 2 diabetes emerged in 2013 with the FDA approval of a sodium-glucose cotransporter 2 (SGLT2) inhibitor, canagliflozin, for use in combination with diet and exercise.76 SGLT2 inhibitors work by impeding glucose reabsorption by the kidney, causing excess glucose to be eliminated in the urine. SGLT2 inhibitors improve glucose control and can be associated with reductions in body weight.‡ The addition of these medicines provides an important new option for patients in whom weight may be an issue. Two additional SGLT2 inhibitors have since joined this class, including dapaglifozin and empagliflozin.77, 78, 79
Importantly, the past decade has also seen the emergence of several combination medications. Ten oral combination therapies have been approved in the last decade, each
containing more than one class of type 2 diabetes medication.80 The combination of more than one medicine into one pill has reduced pill burden for many type 2 diabetes patients who typically require more than one oral medicine, particularly over time.81 The addition of fixed dose combinations has helped to simplify treatment regimens and reduce barriers in treatment compliance. In fact, diabetes patients on combination medications have been shown to be more adherent to treatment regimens, use fewer healthcare resources and have increased life expectancy than those on multiple single dose therapies.82, 83
Advances in Insulin Therapy for Types 1 and 2 DiabetesIn 2015, FDA approved two once-daily, ultra-long-lasting insulins for use in type 1 and type 2 patients. The first of these insulins is injected once daily and provides background insulin coverage for a full 24 hours and beyond for some.84, 85 Also in 2015, the FDA approved another long-acting option called insulin degludec. Insulin degludec can be administered at any point during the day and provides duration of action upwards of 42 hours.86, 87 The availability of these insulins provides patients with longer coverage than had previously been available. Ultra-long-acting insulins are remarkably important advances for patients with diabetes, as they may reduce the burden of daily injections.
In 2015, a premixed formulation of insulin degludec was approved, which combines the long-acting treatment option with another rapid-acting mealtime insulin in a single injection.88, 89 The premixed formulation offers another important treatment option for those who may require less complex treatment regimens or have trouble drawing insulin from multiple bottles—as is often the case for the elderly or those with physical impairments, which is common among many diabetes patients. The use of premixed insulin therapy has also been shown to improve adherence.90
In addition, improved insulin delivery mechanisms have become available to patients over the past decade. In 2014, the FDA approved an inhaled insulin for type 1 and type 2 diabetes patients. The mealtime insulin is rapid-acting and delivered through a small, portable inhaler at mealtimes to help patients achieve blood sugar control.91, 92 The ultra-rapid-acting formulation enables patients to administer the insulin right at the beginning of a meal rather than injecting the medicine in anticipation of a meal. Additionally, the formulation offers a new option for type 1 diabetes patients who may be looking to alleviate daily insulin injection burdens. In those with type 2 diabetes, the formulation may also be an important option if they require insulin therapy but may be averse to initiating daily injections.93
‡ These medicines are not specifically approved for weight loss in patients with diabetes.
13PhRMA 2016 |
Looking to the Future
For many, successful management of diabetes requires constant and diligent monitoring, multiple daily injections and/or the coordination of multiple oral medicines alongside a patient’s carefully planned daily routine to avoid serious disease complications. As a result, treatments offering better or more sustained glycemic control, reduced pill burden, more convenient delivery mechanisms, less frequent injections or simplified daily routines are remarkably valuable to patients with diabetes. The treatment advances occurring over the past decade have each sought to meet these important needs and improve and extend the lives of the millions of Americans struggling to manage this deadly and burdensome chronic condition.
However, as prevalence of the disease is expected to more than double over the coming decades, the importance of expanding treatment options that contribute to better management and control will continue to grow from both a patient and societal perspective.94 The continued development of medicines that meet the diverse needs of patients with diabetes, facilitate the ability for patients to remain adherent to treatment and achieve adequate glycemic control will prove critical to avoid the serious and expensive complications of the disease into the future.
Building on the progress made in the treatment of diabetes over the past decade, researchers continue to strive to bring important new treatment options to patients with both type 1 and type 2 diabetes—including insulins that may provide even longer duration of action for patients.95 Today, more than 200 medicines are in development to treat diabetes and diabetes-related conditions, such as chronic kidney failure and diabetic neuropathy.96 These potential medicines offer hope to the millions of patients who face challenges in successfully managing this complex chronic disease as well as its related complications.
Then• A number of insulin options were available to
patients, as well as oral and injected antidiabetic medications to help manage both type 1 and type 2 diabetes.
• Oral treatment options combining more than one medicine in one pill were limited, resulting in high pill burden for many patients.
• The need remained for expanded and improved treatments, including more convenient and less complex options for those struggling to achieve adequate control of their disease.
Now• Over the past decade alone, more than 20
additional medicines have become available to meet the diverse needs of both type 1 and type 2 diabetes patients.
• Ten oral combination medicines have been approved, each combining more than one class of diabetes medications, reducing pill burden for patients and barriers to treatment compliance.
• Two long-acting insulins offering duration of action lasting between 24-42 hours have been approved, reducing the burden of daily injections and the complexity of treatment. An inhaled insulin was also approved, offering a more convenient delivery mechanism for patients.
DIABETES

A Decade of Innovation in Chronic Diseases14
Multiple Sclerosis: Expanded Treatment Options Improve Outcomes for a Disabling Chronic Condition
Early and consistent treatment is crucial to successful management of multiple sclerosis. Therapeutic advances over the past decade have offered patients more convenient options with fewer side effects, leading to improved treatment outcomes.
Multiple Sclerosis (MS) is a chronic autoimmune disorder in which the immune system mistakenly attacks myelin, a substance that coats nerve fibers. This disrupts the flow of information between the brain and body and generally leads to disability. The vast majority of patients experience a form of the disease characterized by relapses and remissions. An MS attack or relapse, also known as a flare-up, can cause new symptoms or the worsening of existing symptoms, followed by
a partial or full remission with no apparent disease progression. About 10 percent of MS patients experience a steady, progressive form of the disease without distinct relapses or remissions. Patients with this progressive form of the disease currently do not have available treatment options.102, 103
Although there is no cure for MS, treatment has been transformed for those with the relapsing form of the disease
QUICK FACTS• MS affects more than 400,000 Americans and 2.3 million people worldwide.97
• The disease can emerge at any age, but people living with MS are often diagnosed between the ages of 20 and 50.98
• Common symptoms of MS include fatigue, walking difficulties, numbness, spasticity, muscle stiffness, weakness, vision problems, dizziness, bladder problems, sexual problems, bowel problems, pain, cognitive and emotional changes and depression.99
• Symptoms of MS vary widely among patients and can be unpredictable, with no two people experiencing the same symptoms and each person’s symptoms changing over time.100, 101

15PhRMA 2016 |
since the introduction of disease-modifying medicines in the 1990s. Early diagnosis and continuous treatment with these medicines is crucial for MS patients, and offers the best opportunity to prevent irreversible damage to the nervous system and progression of the disease. The introduction of disease-modifying treatments has improved overall quality of life for patients by reducing the number of relapses experienced, slowing disease progression and reducing future disease activity.104, 105
For MS patients, providing greater opportunity for successful management of the disease and its progression requires both treatment options that support patient adherence, as well as the availability of a broad range of therapeutic alternatives for when patients experience an unacceptable level of disease activity or cannot tolerate a particular treatment. This is especially true given that a treatment option that is effective and has few side effects in one patient may produce the opposite result in another patient due to the diverse nature of the disease.106 As a result of treatment advances over the past decade, a range of options are now available to meet the wide variety of needs of people with MS.
A Decade Ago: Limited Treatment Options
Patients diagnosed with MS a decade ago had several disease-modifying treatments available to them, including many that continue to be important treatment options today. These treatments included interferon beta-1a, interferon beta-1b, mitoxantrone, glatiramer acetate and natalizumab. Although these therapies were effective in slowing disease progression and were tolerable for many patients, each was administered via injection or infusion at a medical facility. Administration of these medicines often resulted in painful site reactions, and in some patients it produced flu-like side effects including fever, chills, malaise, muscle aches, and fatigue.107 If the patient failed these initial treatments they had few alternative options. Moreover, some patients found significant challenges adhering to available treatments, given the sometimes intrusive and logistically complex mechanisms for administering the medicines as well as the challenges related to managing the side effects.108
Today: Expanded Options for Patients Offer Greater Convenience
Patients with relapsing forms of MS today have a larger selection of treatment options available to them that can prevent relapse, slow disease progression and improve symptom management. This includes a number of oral medications, which are more convenient for many patients than medications requiring administration by injection or infusion. Each of these medicines works through different mechanisms of action to limit the damage caused by MS relapses, adding important new and convenient treatment options for patients.
The first daily oral disease modifying treatment for MS was approved in 2010. The FDA approved fingolimod to reduce relapses and delay disease progression in patients with the relapsing form of MS. The medicine was the first in a new class of drugs that blocks some blood cells in the lymph nodes. This activity reduces the migration of the blood cells to the brain and spinal cord, which may reduce the severity of MS.110 In addition to providing an easier mode of administration, research suggests that fingolimod may reduce the relapse rate and risk of relapse by approximately 50 percent, relative to previous standard therapies.111, 112, 113
Two additional oral disease modifying medicines followed fingolimod’s approval. Teriflunomide, a daily pill approved in 2012 for relapsing MS, inhibits the function of specific immune cells implicated in MS.114, 115 The medicine has demonstrated significant efficacy across a number of key measures of MS disease activity—including fewer relapses, slowed disease progression and reduced number of brain lesions.116 Results from a clinical trial demonstrated that teriflunomide reduced relapses among MS patients by approximately 30 percent relative to placebo.117
Dimethyl fumarate was approved in 2013 and is an oral disease-modifying medicine taken twice a day.118 Researchers believe the medicine exerts its effects by affecting the immune system through several different pathways. Results from clinical trials show that the risk of relapse was reduced by up to half, and the number of relapses by nearly half, in patients taking the dimethyl fumarate relative to placebo. Evidence also suggests the medicine may slow the development of brain lesions, reduce inflammatory disease activity, and slow progression to disability in some patients.119
Another disease-modifying treatment—alemtuzumab—was approved in 2014 as a second-line treatment for patients who have had an inadequate response to two or more MS disease-modifying therapies. The medicine is administered via infusion for five consecutive days initially and for three consecutive
“The best disease-modifying medication is the one that the person with MS will take, and that is best for the person’s situation.”
–Barbara Giesser, M.D., Director, The Marilyn Hilton MS Achievement Center at University of California Los Angeles
David Geffen School of Medicine109

A Decade of Innovation in Chronic Diseases16
days one year later. Alemtuzumab provides another important new treatment for patients who have tried and exhausted other therapeutic options.120, 121
In addition to disease-modifying treatments, advances over the past decade offer MS patients improved symptom management. Dalfampridine, approved in 2010, was the first treatment approved specifically for improving walking in MS patients.122 Difficulty walking is one of the most common mobility limitations among those with MS, and many find this to be among the most debilitating consequences of the disease. Dalfampridine represents a significant breakthrough for these patients. The medicine aids with the conduction of nerve impulses, improving the speed and consistency of signals to muscles, which, in turn, facilitates walking speed in MS patients.123
Research Continues to Focus on Unmet Need
Over the past decade, each of these therapies has contributed to the arsenal of medicines now available to help patients not only prevent relapses and slow disease progression, but to also more effectively manage disease symptoms and improve overall quality of life. Many of these medicines provide greater convenience and fewer side effects, while also providing alternatives to meet the diverse needs of people with MS, thereby supporting successful overall disease management.
Today there are 40 medicines in development to treat MS, offering even greater opportunity to transform the landscape of treatment.124 Researchers continue to focus on meeting the unmet needs of patients with the progressive form of MS, who presently lack available treatment options.125, 126 Experimental antibody medicines targeting a protein involved in MS which inhibits the production of myelin are among the innovative approaches demonstrating significant potential for MS patients—including those with the progressive form of the disease.127 Remarkable progress has been made over the past decade, but research and development continues to provide hope for patients struggling with this diverse and debilitating chronic disease.
“It’s so gratifying now that we have so many options…and to know that as the years go on, we’re seeing drugs that are not only easier to take—oral drugs rather than injectable drugs—but that have a higher degree of effectiveness.”
–Aaron Miller, M.D., Medical Director, Corinne Goldsmith Dickinson Center for Multiple Sclerosis,
Mount Sinai School of Medicine128
Then• Disease-modifying treatments were limited
to a handful of injected and infused medicines which were often intrusive and logistically complex.
• Available treatment regimens often meant painful site reactions and sometimes intolerable side effects for patients.
• Alternative treatments were needed for those who experience an unacceptable level of disease activity disease activity or could not tolerate available therapies.
Now• The number of treatment options for patients
has expanded dramatically. For the first time, three oral disease-modifying medicines are now available, offering more convenient administration options with fewer side effects.
• MS patients can better choose how and when to take their medication to fit their diverse needs, increasing overall compliance and leading to better treatment outcomes.
• Today, 40 medicines are in development to treat MS—including several offering to provide first-time treatments for those with the progressive form of progressive disease who currently lack treatment options.
MULTIPLE SCLEROSIS
17PhRMA 2016 |
Rheumatoid Arthritis: An Improved Quality of Life, Never Before Seen
New classes of targeted therapies over the last decade have expanded options, helping patients with rheumatoid arthritis achieve disease remission, avoid disability and experience an improved quality of life.
Rheumatoid Arthritis (RA) is a progressive and painful autoimmune disorder that causes inflammation of the joints. In RA, the body’s immune system attacks its own tissue—specifically a thin membrane that lines the joints called the synovium. Left unchecked, inflammation in the joints can
result in damage to cartilage and the bones themselves. Over time, joints can become unstable and deformed, ultimately causing patients to loose mobility and physical functioning. As joint damage cannot be reversed in RA, timely diagnosis and treatment is critical.134, 135, 136
QUICK FACTS• An estimated 1.5 million Americans suffer from RA129
• Women are nearly three times more likely to have the disease than men. RA generally begins between the ages of 30 and 60 for women but occurs later in life for men.130
• RA reduces the function of many joints, commonly affecting hands, feet, wrists, elbows, knees and ankles. Symptoms often involve joint pain, swelling, stiffness and limited range of motion.131, 132
• Periods of high disease activity, or “flares,” may come and go, with inflammation and other symptoms lasting anywhere from days to months.
• The joint damage caused by the disease is irreversible; therefore, early diagnosis and treatment is important in preventing and slowing disease progression.133

A Decade of Innovation in Chronic Diseases18
Early RA treatments, including analgesics, corticosteroids and non-steroidal anti-inflammatory drugs (NSAIDs), focused on reducing inflammation, but they only treated the symptoms not the root cause. More recent medicines called synthetic disease-modifying anti-rheumatic drugs (DMARDs) act on the immune system by slowing the progression of RA. Synthetic DMARDS, including hydroxychloroquine, leflunomide, methotrexate, and sulfasalazine, are important treatments for RA patients; however, they cannot prevent the structural joint damage caused by the disease.137, 138
Biologic DMARDs—otherwise known as biologic response modifiers—first emerged in the late 1990s and revolutionized the treatment of RA. These medicines are designed to reduce inflammation and structural damage in joints by interrupting cellular processes that cause inflammation. For the first time, biologic DMARDs offered patients the ability to target the underlying cause of the disease by suppressing key inflammatory pathways involved in joint inflammation and destruction, allowing for better disease control.139, 140
Although there is no cure for RA, with the right DMARD regimen, many patients can achieve a state in which they experience few or no signs of disease activity—otherwise known as “remission.”141 Remission and reduced disease activity are now the primary focus of RA treatment.142 However, no single medicine works for all patients, as response can vary among individual patients. Consequently, identifying a treatment regimen that is the most appropriate may require exploring several potential therapeutic options or treatment
combinations. Even after finding an appropriate treatment, patient response may change over time, making it necessary to find a suitable and effective alternative.143 It is for these reasons that the availability of a broad range of treatment options provides the greatest opportunity for patients to prevent irreversible joint damage, achieve disease remission, and experience better overall quality of life.
A Decade Ago: Critical Advances Begin to Transform Treatment
A decade ago patients were just beginning to benefit from the first wave of biologic DMARDs, allowing patients to target the underlying source of inflammation and joint damage involved in RA. Among this first wave of biologics were five medicines stemming from three different drug classes, each of which targeted different inflammatory pathways involved in RA, including three tumor necrosis factor (TNF) inhibitors, an interleukin-1 (IL-1) receptor antagonist, and a T-cell modulator.144
Although the treatment landscape was starting to transform dramatically with the addition of biologics to the arsenal of RA treatments ten years ago, there was still much to learn about the optimal use of available medicines, particularly biologic medicines, which were often recommended only for use in the most advanced cases of RA. Further, additional treatment options were still very much needed for those who did not respond or failed available treatment regimens.

19PhRMA 2016 |
Today: Expanded Treatment Options Improve Patient Outcomes
Over the last decade, clinical evidence has grown regarding the use of biologic DMARDs, providing a better understanding of optimal use and improved outcomes in patients. A patient diagnosed with RA today also has a broader range of treatment options available relative to the previous decade to help better manage their condition—including three entirely new classes of therapy. Expanded options allow patients to find the most appropriate treatment to meet their specific needs and provide a greater opportunity for patients to achieve remission, improve physical functioning and enjoy better quality of life.
Growth in Clinical EvidenceIn recent years, research has identified more effective ways for clinicians to use biologic DMARDs than before. A growing body of evidence suggests that when initiated early, biologics can achieve superior treatment responses and better control of disease progression. This information has led to a shift in treatment guidelines in recent years.145 Whereas previously, biologics were recommended for more advanced cases of RA, today they are now commonly initiated early in the course of the disease, when joint damage can be reduced or prevented.146, 147
In addition, ongoing research has demonstrated the synergistic effects of biologic DMARDs when used in combination with the synthetic DMARD methotrexate. These medicines used in combination provide more benefits to patients than when either treatment is used alone.148, 149, 150 As a result of this growth in clinical evidence, today these medicines are now commonly recommended for use in combination.151, 152
Growth in Treatment OptionsOver the past decade, expansions in treatment options have contributed greatly to the ability of patients to target the
underlying cause of their disease. TNF inhibitors, which were among the first class of biologic DMARDs to become available to RA patients in the previous decade, remain an important class of medicines today. In fact, two additional medicines have since been added to the arsenal of TNF inhibitors, including golimumab and certolizumab.153, 154 The medicines work by blocking the TNF-alpha protein, which contributes to the inflammation involved in RA. Because they work well for many patients, treatment initiation is commonly recommended with this class.155
Entirely new classes of medicines for the treatment of RA have also become available over the past decade, offering new ways to target the underlying cause of the disease. In 2006, the FDA approved rituximab, the first B-cell targeted biologic therapy for RA. Rituximab targets particular immune cells and affects multiple pathways by which B-cells are thought to contribute to the development of RA. The drug, which is also used for cancer and other autoimmune diseases, is an infused medicine approved for use in combination with methotrexate in adult patients who have had an inadequate response to one or more TNF inhibitors. Rituximab provides an important treatment option for those failing to respond or who were intolerant to TNF inhibitors.156, 157
In 2010, the FDA approved the first of another new class of biologic DMARDs called IL-6 receptor antibodies. Tocilizumab is designed to inhibit the biological activity of IL-6, a protein that is involved in inflammatory processes in the body. Levels of the
“Current therapy for RA is such that progression from symptom onset to significant disability is now no longer inevitable, and RA patients can anticipate comfortable and productive lives on medical therapy…Patients with RA can now expect to experience a quality of life that previously was unavailable to patients during the 20th century.”
–Katherine Upchurch, M.D., Division Chief, Rheumatology and Jonathan Kay, M.D., Professor, University of
Massachusetts Medical School145
A Decade of Innovation in Chronic Diseases20
IL-6 protein have been shown to be elevated in patients with RA. Tocilizumab was approved for use in moderate to severe RA in adult patients who have had an inadequate response to one or more TNF inhibitors. The medicine may be used alone or in combination with other synthetic DMARDs such as methotrexate.158, 159 Two years later, the medicine was also approved for use as a first-line option for patients, regardless of failure or inadequate response with a TNF inhibitor.160
In 2012, the FDA approved tofacitinib, the first of another new class of medicines called janus kinase (JAK) inhibitors. Tofacitinib is designed to inhibit the signaling of JAK pathways in cells, which play an important role in the inflammation involved in RA. Unlike biologic DMARDs, tofacitinib is an oral medication, and it was the first new oral DMARD to become available to patients in more than 10 years. Tofacitinib was approved for use in patients who have had an inadequate response to previous RA medicines or who were intolerant to methotrexate. Treatment failure on a biologic DMARD is not required before initiating treatment with tofacitinib.161, 162
Research Focuses on Continued Advances
Growing knowledge regarding the development of optimal treatment regimens for patients, as well as the expansion of treatment options, has contributed greatly to better disease management over the past decade. Today, not only is more known about how to most effectively treat RA patients, but more options are available for those who may have failed a particular treatment or ceased to benefit from a given treatment over time. This growing range of treatment options is providing patients with the greatest potential to date to prevent irreversible joint damage, achieve remission and avoid disability. Perhaps most importantly, advances in treatment are allowing patients to experience an improved quality of life.
Researchers continue to strive to improve patient outcomes for the 1.5 million Americans that struggle to manage this debilitating chronic disease. Currently, a total of 40 medicines are in clinical development offering hope to further transform the treatment of RA.163
Then• Biologic DMARDs were only prescribed for
patients with advanced cases of RA.
• Additional treatment options offering novel ways to target the underlying cause of the disease were needed.
• Treatment options were needed for patients who failed or ceased to benefit from available treatments over time.
Now• Based on ongoing research, biologic DMARDs are
now commonly used earlier in the progression of the disease, resulting in better clinical response, slowed disease progression and greater potential for remission.
• Four new biologic DMARD therapies have become available, several of which stem from entirely new classes of treatment for RA, and are offering patients new ways to target underlying inflammatory pathways involved in the disease.
• A new first-in-class oral DMARD is also now available offering a more convenient treatment option for patients.
RHEUMATOID ARTHRITIS

21PhRMA 2016 |
HIV/AIDS: Advances Continue to Improve Patients’ Lives
Expanded treatment options over the past decade have continued to bring down death rates, reduced barriers to patient adherence, improved patient quality of life, and paved the way for a future focused on prevention.
Unlike the early years of the AIDS crisis, HIV is no longer considered acutely fatal, but rather has become a chronic and manageable disease for those receiving appropriate treatment. This dramatic change followed the introduction of highly active antiretroviral therapy (HAART) in the mid-1990s, which transformed treatment, leading to a nearly 85% decline in death rates and preventing an estimated 862,000 premature deaths in the United States.168, 169
HAART, commonly referred to today as “ART,” generally involves a combination of three treatments from at least two drug classes and has become the cornerstone of HIV treatment. Each drug class works to suppress the replication of the virus through different mechanisms, reducing the amount of HIV in the body and preventing the disease from compromising the immune system.170 Treatment regimens are tailored to each patient and often evolve with the patient over time.171
QUICK FACTS• The human immunodeficiency virus (HIV) gradually destroys the body’s immune system by entering and
taking over infection-fighting T-cells.
• If left untreated, HIV will attack the immune system until it progresses to acquired immunodeficiency syndrome (AIDS).165
• 1.1 million people are currently living with HIV in the United States, and 35 million globally.166, 167
• Antiretroviral drugs for the treatment of HIV suppress the virus—sometimes to undetectable levels—by interfering with viral replication.

A Decade of Innovation in Chronic Diseases22
For HIV patients, consistent and sustained suppression of viral replication with combination antiretroviral therapy not only keeps viral load low—often to undetectable levels—but prevents the virus from mutating into forms that can be resistant to drug therapy. For this reason, it is critical for patients to begin and remain on a treatment regimen that supports patient adherence. It is equally important to have a broad range of treatment options available for those failing to respond adequately to their current treatment or who have developed viral resistance.172, 173
A Decade Ago: Patient Adherence to Treatment a Key Challenge
A patient diagnosed with HIV ten years ago was fortunate to benefit from multiple treatment options available across four major antiretroviral drug classes.§ Although twice-daily dosing was feasible for most patients, treatment was far from perfect.174 Few combination treatment regimens contained more than one class of antiretrovirals in a single dose, and pill burden and patient adherence remained a challenge.175
In addition, the side effects of available treatment options made it difficult for some to adhere to prescribed treatment regimens. Side effects commonly included diarrhea, nausea and headaches. Serious long-term complications included lipodystrophy, a redistribution of fat in the body, and lactic acidosis, which can lead to muscle aches and liver failure.176
Although much had been done to reduce mortality for HIV patients a decade ago, treatment regimens remained complex and the side effects of treatment were a challenge for many. Additional treatment options were needed to help patients better manage the disease and enjoy better overall quality of life.
Today: Continued Advances Improve Patient Outcomes through Greater Adherence
An HIV patient diagnosed today can live close to a normal life expectancy if they are appropriately treated with the broad range of medicines available.177 This decade has seen the approval of 15 antiretroviral medicines—five of which combine an entire HAART regimen into a once-daily pill. In addition, three entirely new classes of medicine and several therapies focused specifically on alleviating common side effects of treatment have been introduced.178 Relative to a decade ago, patients today have a reduced pill burden, decreased side effects, and improved ease of use, which in turn, has reduced barriers to treatment adherence, leading to better health outcomes and improved quality of life.179, 180
Once-Daily, Single-Tablet, Multi-Class Therapies Ease Treatment Burden Once-daily, single-tablet, multi-class treatment regimens have become an integral part of HIV management over the past decade. These fixed-dose combinations are better tolerated and have not only been associated with greater viral suppression, but by combining as many as four different therapies in a single tablet, they have also dramatically reduced pill burden for patients.181, 182 Relative to HIV patients taking two or more pills per day, those on once-daily, single-tablet regimens are more likely to achieve the adherence levels needed to avoid the development of drug resistance.183, 184 Moreover, adherent patients on single-tablet regimens have been found to experience fewer hospitalizations and lower health care costs.185, 186 Five such medicines have been approved since 2006 which have simplified dosing, reduced pill burden and maximized potential for successful disease management (see Table 2).187, 188
Table 2. Once-Daily, Single-Tablet, Multi-Class HIV Combination Products
Approval Year
Drugs Contained in Single Tablet Drug Classes
2006
• Efavirenz• Emtricitabine• Tenofovir disopxil
fumarate
• Non-Nucleoside Reverse Transcriptase Inhibitorsa
• Nucleoside Reverse Transcriptase Inhibitorsb
2011
• Rilpivirine • Emtricitabine• Tenofovir disopxil
fumarate
• Non-Nucleoside Reverse Transcriptase Inhibitors
• Nucleoside Reverse Transcriptase Inhibitors
2012
• Elvitegravir• Cobicistat• Emtricitabine• Tenofovir disopxil
fumarate
• Integrase Inhibitorsc
• Pharmacokinetic Enhancersd
• Nucleoside Reverse Transcriptase Inhibitors
2014• Dolutegravir• Abacavir• Lamivudine
• Integrase Inhibitors• Nucleoside Reverse
Transcriptase Inhibitors
2015
• Elvitegravir• Cobicistat• Emtricitabine• Tenofovir alafenamide
• Pharmacokinetic Enhancers
• Nucleoside Reverse Transcriptase Inhibitors
a. Nucleoside reverse transcriptase inhibitors block reverse transcriptase, an enzyme the virus needs to replicate itself.
b. Non-nucleoside reverse transcriptase inhibitors bind to and later alter reverse transcriptase, an enzyme the virus needs to make copies of itself.
c. Integrase inhibitors interfere with HIV integrase, an enzyme the virus needs to replicate itself.
d. Pharmacokinetic enhancers increase the effectiveness of other antiretroviral medicines in a treatment regimen.
§ Drug classes available to patients included include nucleoside reverse transcriptase inhibitors, non-nucleoside reverse transcriptase inhibitors, protease inhibitors and fusion inhibitors.

23PhRMA 2016 |
New Classes of HIV Treatments Increase Options for PatientsThree new classes of antiretrovirals have also offered tremendous advancements and expanded treatment options for patients. Because HIV can sometimes become resistant to drugs within the same class—a process known as “cross-resistance”—the availability of additional classes of medicines that target the virus through different mechanisms is important in providing treatment alternatives for patients.189
In 2007, raltegravir, the first medicine in a new class called integrase inhibitors, was approved. This class of medicines works by interfering with HIV integrase, an enzyme the virus needs to replicate itself.190 Because integrase inhibitors do not interfere with human cellular processes, they can also have fewer side effects than other drugs.191 Several integrase inhibitors have been also incorporated into once-daily, single-tablet treatment regimens contributing to reduced pill burden for patients (see Table 2).
Also approved in 2007 was maraviroc, the first of a class of medicines called CCR5 antagonists. The medicine was approved for use in patients infected with a specific type of HIV (the CCR5-tropic virus) and who have evidence of both viral replication and HIV strains resistant to multiple antiretroviral agents. Maraviroc works by blocking the CCR5 co-receptor, which is a primary route for the virus to enter immune cells. When the receptor is blocked, the virus cannot enter or infect the cell. Due to the medicine’s novel mechanism of action, maraviroc has provided an important option for patients who had developed resistance to available medicines.192, 193
In 2012, another class of medicines joined the arsenal of treatments available to patients with HIV. Known as pharmacokinetic enhancers, these medicines are termed “boosting agents” because they do not have antiviral activity on their own but instead inhibit enzymes in the body that normally metabolize or degrade antiretroviral medicines. Adding these boosting agents to HIV treatment combinations allows antiviral medicines to remain effective in the body for longer periods of time, thereby reducing pill burden and offering simplified dosing schedules.194 Cobicistat was the first of this class to be approved by the FDA in 2012. The boosting agent was approved for use combined with three other antiretroviral medicines in a once-daily, single-tablet combination in 2012 (See Table 2).195 The medicine has also since been approved in other fixed dosed combinations providing additional treatment options with reduced pill burden for patients.196, 197
New Therapeutic Options Manage Side EffectsOver the past decade, advances in HIV treatments have helped to decrease the side effects patients experience. In addition,
treatments have become available to help better manage common side effects of antiretroviral treatments. Advances such as these are particularly important for HIV patients as they continue to live longer lives.
Lipodystrophy is a condition associated with the use of antiretrovirals and can manifest in the form of excess fat in different areas of the body—commonly around the abdomen. In 2010, tesamorelin, a synthetic growth hormone-releasing factor (GRF) drug administered as a once-daily injection, was approved by the FDA for the management of lipodystrophy, having been shown to reduce abdominal fat in HIV patients.198
Another side effect commonly associated with antiretroviral treatment is diarrhea, with up to 60% of HIV patients reporting symptoms. Crofelemer was approved in 2012 to help relieve the condition specifically in HIV patients.199
The availability of medicines that manage the side effects of treatment not only improves quality of life for patients, but also reduces barriers to adhering to antiretroviral therapy and contributes to better overall disease management.

A Decade of Innovation in Chronic Diseases24
A New Era Focused on Prevention
The past decade has seen remarkable advances in treatment and disease management. Recent advances are also offering greater protection, when used along with safer sex practices and other awareness strategies, to prevent infection and transmission of the virus. Pre-exposure prophylaxis, or PrEP, is an HIV prevention strategy where individuals take certain HIV medications before coming into contact with HIV to prevent the spread of the virus to HIV-free individuals who may be at high risk for infection. In 2012, the FDA approved the first medicine for PrEP use. It contains two medicines, tenofovir disoproxil fumarate and emtricitabine. When taken consistently, PrEP has been shown to reduce the risk of HIV infection in high risk individuals by up to 92%.200 Looking forward, advances in prevention are offering substantial opportunity to prevent transmission of the disease.
Long-term prevention efforts today continue to focus on the development of a preventive vaccine, which many experts believe is the best strategy for controlling or even ending the HIV epidemic. Currently, 33 vaccine candidates are in clinical development, offering tremendous hope for a future without HIV/AIDS.201
Today, average life expectancy for patients has increased 10 years relative to that seen just a decade ago.202 Advances in patient medication adherence resulting from reduced side effects, improved ease of use, reduced pill burden and expanded treatment options have contributed significantly to improving and extending the lives of patients with HIV. With continued advances in prevention, a future is truly possible in which HIV can not only be better managed and controlled, but potentially eradicated.
“With collective and resolute action now and a steadfast commitment for years to come, an AIDS-free generation is indeed within reach.”
–Anthony S. Fauci, M.D., Director, National Institute of Allergy and Infectious Disease (NIAID)203
Then• Four antiretroviral drug classes were available to
patients suppressing the virus through different mechanisms of action.
• Patients required twice-daily dosing of multiple medicines and pill burden remained a challenge.
• Patients developing resistance to medicines from existing drug classes were limited in alternative treatment options.
• Patients were limited in treatment options for the management of side effects of antiretroviral therapy.
Now• Three new classes of antiretroviral medicines
are available to patients offering important new options for those failing or developing viral resistance to existing therapies.
• Five once-daily, single-tablet, multi-class combination products significantly reduce pill burden, provide greater efficacy and fewer side effects for patients, thus contributing to improved adherence and successful disease management.
• New treatments are available to help patients manage common and debilitating side effects of antiretroviral treatment.
• Average life expectancy for patients has increased 10 years relative to that seen just a decade ago.
• Prophylactic medications offer to reduce the risk of infection by 92% among high risk individuals and 33 vaccines are in development offering great hope for a future without HIV.
HIV/AIDS

25PhRMA 2016 |
Hepatitis C: Breakthroughs Revolutionize Treatment for Patients
More effective and convenient treatment options have more than doubled cure rates for patients with all forms of hepatitis C, providing the opportunity to avoid substantial disease-related burden.
QUICK FACTS• More than 3.2 million people have hepatitis C in the United States, and 170 million people have the disease
worldwide.204, 205
• Each year, approximately 30,000 Americans are newly infected with the virus, and nearly 20,000 die.206, 207
• Hepatitis C can lead to serious complications—including cirrhosis, advanced liver disease, liver cancer, and in some cases, may cause patients to need a liver transplant.208
• The hepatitis C virus has many different genetic variations; which are classified by “genotypes”. Genotype 1 is the most common in the United States, representing more than 70% of Americans with the disease (see Figure 1).209
Hepatitis C is a devastating, slowly progressing viral disease primarily affecting the liver. Patients often remain asymptomatic for some time and may not be diagnosed until serious complications emerge as a result of damage to the liver. Damage can progress over many years, starting with liver inflammation and liver scarring, called fibrosis. Without detection and treatment, this damage may lead to permanent, irreversible damage called cirrhosis, which prevents the liver from functioning normally. For those who have progressed to
end-stage liver disease, treatment options focus on preventing further damage in an effort to avoid the most serious complications, which include liver cancer, the need for a liver transplant, and premature death.211
As a disease primarily affecting baby boomers, the clinical consequences of the hepatitis C virus (HCV) have been on the rise over the past decade, and in the absence of effective treatments, this burden has been projected to continue to

A Decade of Innovation in Chronic Diseases26
grow. HCV is the leading cause of cirrhosis and liver cancer and is the most common reason for a liver transplant in the United States.212 National hospitalization rates for HCV patients have also been on the rise in recent years, increasing nearly 200% between 2004 and 2011.213 Cases of cirrhosis, liver cancer, and liver transplants resulting from HCV infection have all been anticipated to peak over the coming decade in the absence of effective treatments.214
A Decade Ago: Limited Treatment Options and Low Cure Rates
The only treatment option available to a patient with HCV a decade ago was pegylated interferon, an immunotherapy administered subcutaneously (under the skin) and given over a course of treatment lasting 24 to 48 weeks.** Interferon-based therapy was an important treatment option for patients at the time but could cause debilitating, flu-like side effects for patients, including fever, fatigue, and insomnia. These side effects made adherence challenging and led many to discontinue therapy before the full course was completed.215 Even for those patients able to complete treatment, only half were cured and many were left struggling with chronic infection.216
Today: A Decade of Progress has Transformed the Treatment of Hepatitis C
The past decade has completely transformed the treatment of HCV. The advent of new oral direct-acting antiviral (DAA)
agents—designed to attack HCV at every stage of the viral life cycle—has dramatically improved health outcomes for patients. Since the introduction of the first DAA in 2011, subsequently approved medicines have each brought successive improvements in cure rates, reductions in side effects and treatment duration, and provided effective treatment options for patients across genotypes. The medicines available today offer cure rates over 90% and the required duration of treatment has been reduced to as short as 8 weeks for many patients (see Table 3).
The first DAAs arrived in 2011 and included protease inhibitors, which work by preventing the virus from binding to the site that the virus’s protease enzymes use to replicate.232 Boceprevir and telaprevir were the first protease inhibitors approved to treat HCV and were used in patients with the most common form of HCV in the United States—genotype 1. Taken in combination with pegylated interferon over a course of 24 to 48 weeks, these medicines demonstrated improved cure rates in clinical studies ranging from 63-79% in patients who had not been previously treated.233, 234 Two years later, the first DAAs were joined by another protease inhibitor called simeprevir, also approved for genotype 1, providing yet another potent option for HCV patients. Taken in combination with pegylated interferon, in clinical studies simeprevir demonstrated cure rates of 80% in patients who had not been previously treated.235, 236
Figure 1. Hepatitis C Prevalence by Genotype, United States, 2011211
70%
15-20%
10-12%
<1% <1%
Genotype 1
Genotype 2
Genotype 3
Genotype 4
Genotype 5 and 6
** Interferon is taken in combination with ribavirin.

27PhRMA 2016 |
Table 3. Direct-Acting Antiviral Agents Approved Over the Past Decade‡‡
TypeYear
ApprovedApproved Treatment
or Treatment Regimen GenotypeTaken in combination with Peg-Interferon Treatment Duration Cure Ratea
Protease Inhibitors
2011 telaprevirb
1 X 24-48 weeks63%-80%c
217, 218, 2192011 boceprevirb
2013 simeprevir
Polymerase Inhibitors 2013 sofosbuvir
1 X 12 weeks 90%220
2 12 weeks 93%221
3 24 weeks 84%222
4 X 12 weeks 94%223
Combination Therapies
2014/2015
sofosbuvir/simeprevir 1 12-24 weeks 94-99%224
sofosbuvir/ledipasvir
1 8-12 weeks 94-100%225
4 12 weeks 93%227
5 12 weeks 93%227
6 12 weeks 96%228
ombitasvir/paritaprevir/ritonavir/
dasabuvir1 12 weeks 95-100%229
2015
ombitasvir/paritaprevir/ritonavir
4 12 weeks 100%230
daclatasvir/sofosbuvir 3 12 weeks 92-98%231
a. Cure rates denote measures of sustained virologic response (SVR), defined as a lack of detection of HCV RNA in the blood several months after completing a course of treatment. SVR is an outcome measure used to determine treatment success and is considered a virologic cure. Cure rates vary by treatment population. See FDA label for reported cure rates across treatment populations in clinical studies.
b. Telaprevir and boceprevir are no longer marketed in the United States.c. Reporting cure rates in clinical studies for treatment naïve patients.
‡‡ The FDA approved a new combination therapy outside the period examined in this report. Elbasivir/grazoprevir was approved for use on January 28, 2016 in patients with HCV genotypes 1 and 4. The agency also expanded the use of daclatasvir to genotype 1 patients on February 5, 2016 (in combination with sofosbuvir).
In 2013, another DAA, sofosbuvir, was approved as the first in a new class of medicines called polymerase inhibitors.237,
238 This class is designed to prevent the virus from replicating by blocking the RNA polymerase enzyme.239 Sofosbuvir marked a major advance for patients with HCV genotypes 1-4, delivering significant improvements in cure rates, fewer side effects and shorter duration of treatment. For patients with genotypes 1 and 4, these medicines were recommended for use in combination with interferon. In these patient populations, clinical studies demonstrated cure rates of 90% in genotype 1 patients and 96% in genotype 4 patients. For patients with genotypes 2 and 3, sofusbuvir was recommended without the use of interferon, marking it the first entirely oral and interferon-free HCV treatment. In these patients, clinical studies demonstrated cure rates of 93% in genotype 2 patients and 84% in genotype 3.240
Highly effective and entirely oral, interferon-free combination therapies for patients with the most common type of the disease were not far behind. In 2014, the FDA approved the first of these combination therapies which was comprised of sofosbuvir and a previously unapproved DAA called ledipasvir. The once-a-day pill was approved for
genotype 1 patients with clinical evidence demonstrating cure rates ranging from 94-100% across a variety of treatment populations.241 The introduction of interferon-free combination therapies marked an important advance for genotype 1 patients as it ushered in an entirely new era of effective and convenient HCV treatments with minimal side effects. Shortly thereafter, the FDA also approved the combination use of sofosbuvir with simeprevir, with cure rates ranging from 94-99%, providing yet another treatment option for genotype 1 patients.242 Rounding out this milestone year was the approval of a four-part combination therapy comprising ombitasvir, paritaprevir, ritonavir, and dasabuvir, which demonstrated cure rates ranging from 95-100%.243
Combination therapy approvals in 2015 have continued to meet the needs of patients with rarer forms of HCV—genotypes 3, 4, 5 and 6—providing oral treatment options across all HCV genotypes no longer requiring the use of interferon. Daclatasavir was approved for use in combination with sofosbuvir for the treatment of genotype 3 patients, one of the most difficult to treat genotypes. Although sofosbuvir was approved previously without the use of interferon for genotype 3, the addition of daclatasavir to the treatment

A Decade of Innovation in Chronic Diseases28
regimen cut treatment duration in half and boosted cure rates in non-cirrhotic patients to 86-96%.244 Also approved the same day was the combination of ombitasvir, paritaprevir and ritonavir for use without interferon in non-cirrhotic genotype 4 patients. The combination demonstrated cure rates in clinical studies of 100% and marked the first oral interferon-free treatment for patients with genotype 4.245 Closing out 2015, the FDA expanded the approved use of sofosbuvir/ledispavir to include genotypes 4, 5, and 6 based on clinical studies demonstrating cure rates ranging from 93-96%.246
A Future without Hepatitis C
The numerous breakthroughs that have occurred over the past decade, each filling an important unmet need for HCV patients, have transformed treatment of the disease. Not long ago, the only option available to patients was a challenging course of treatment with interferon over 24 to 48 weeks, which cured only half of patients. Today, available treatment options offer cure rates over 90% in as little as 8 weeks. Patients across genotypes can also choose from a range of oral treatments which do not require the use of interferon and therefore patients can avoid its accompanying side effects. While these revolutionary treatments have come a long way in providing important options for HCV patients, they are just
the beginning. There are currently nearly 60 HCV treatments in development, striving for improved cure rates, decreased treatment duration and more convenient and effective options from which patients can choose the treatment best suited to individual needs.247
Not only have these advances in treatment provided important and more effective options for patients, but they have provided the opportunity to avoid substantial disease-related burden. A decade ago, society faced a growing public health problem with limited treatment options. Today, effective treatments provide the ability to cure the vast and diverse HCV population and avoid the very serious clinical consequences of the disease. In fact, a recent study found that with current screening guidelines and the availability of today’s more effective treatments, HCV could become a rare disease by 2036 in the U.S. The same study estimated that 78,800 cases of liver cancer, 9,900 liver transplantations and 126,500 liver-related deaths could be avoided by 2050 with the availability of new and effective treatments for HCV.248 Due to the tremendous advances made over the past decade, the future is bright for both HCV patients and society, as the substantial burden associated with the disease can be avoided with new highly effective treatment options.
Then• The only treatment option available to a patient
with HCV was pegylated interferon, an injected immunotherapy administered subcutaneously over the course of 24 to 48 weeks.
• Treatment side effects were debilitating—including fever, fatigue, and insomnia—and led many patients with hepatitis C to discontinue treatment before the full course was completed.
• Among those patients completing treatment, only half were cured of the disease.
Now• A range of entirely oral, interferon-free treatments
provide new, effective options for hepatitis C patients with cure rates upwards of 90% in as little as 8 weeks.
• Patients across genotypes can also choose from a range of oral treatment options which do not require the use of interferon, therefore, allowing patients to avoid accompanying side effects.
• New medicines offer the opportunity to avoid the very serious clinical consequences associated with the disease.
HEPATITIS C

29PhRMA 2016 |
Continued Progress for Patients with Chronic DiseasesThe conditions examined in this report span a broad range of disease areas, but they all demonstrate the fast pace of advances in the fight against chronic disease over the past decade. As the burden of chronic illness is expected to grow in coming years, continued medical progress will prove critical to solving the complex problem of disease.
Medical progress against disease can take many forms. For instance, new medicines may offer patients a cure or transform an acutely fatal illness into a chronic and manageable condition. Progress may provide a treatment to fill an important unmet need or an effective alternative where there had previously been none. Advances can also sometimes make treating an illness easier or more manageable for patients, or facilitate adherence to treatment, halt disease progression and avoid serious complications. Progress may also mean an expanded understanding of how to best treat a given condition with existing medicines. Each of these types of advances mean progress for patients that can improve and extend lives.
Looking ahead, medicines will play an increasingly central role in helping us address our most costly and challenging diseases, including chronic diseases like Alzheimer’s. In fact,
a new medicine to treat this devastating illness could have a transformative effect not just on the lives of patients, but also on the health system. Research estimates that the United States health care system could save a total of $367 billion by 2050 if we could develop one new medicine to delay the onset of the disease by five years.250 There has never been greater urgency to develop medicines to treat this disease and many other illnesses where there continues to be substantial unmet need.
In the chronic disease space, and across the biopharmaceutical research and development ecosystem, the harnessing of new scientific and technological advances is ushering in a new era of treatment possibilities. Although the process is increasingly challenging and complex, researchers in the biopharmaceutical sector are dedicated to developing new medicines for patients with chronic diseases. Given the anticipated growth in chronic illness, it will be important that public policies are in place that support continued prevention, early detection, and treatment of patients, as well as support the R&D investment needed by biopharmaceutical companies to foster innovation. Ultimately, medicines will be an important part of the solution to making chronic disease more sustainable, both today and into the future.

A Decade of Innovation in Chronic Diseases30
References1. Centers for Disease Control and Prevention. “Chronic Disease Overview.” http://www.cdc.gov/chronicdisease/overview/index.htm
2. Centers for Disease Control and Prevention. “Multiple Chronic Conditions.” http://www.cdc.gov/chronicdisease/about/multiple-chronic.htm
3. The Lancet. “Tackling the burden of chronic diseases in the USA.” The Lancet. 2009. 373:185. http://www.thelancet.com/journals/lancet/article/PIIS0140-6736%2809%2960048-9/fulltext
4. FightChronicDisease.org. “The Growing Crisis of Chronic Disease in the United States.” http://www.fightchronicdisease.org/sites/default/files/docs/GrowingCrisisofChronicDiseaseintheUSfactsheet_81009.pdf
5. Centers for Disease Control and Prevention. “Chronic Disease Prevention and Health Promotion.” http://www.cdc.gov/chronicdisease/
6. Mozaffarian D, et al. “Heart disease and stroke statistics—2015 update: a report from the American Heart Association.” Circulation. 2015. 131:e29. http://circ.ahajournals.org/content/131/4/e29.extract
7. Centers for Disease Control and Prevention, “Cholesterol Fact Sheet,” http://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_cholesterol.htm
8. Centers for Disease Control and Prevention, “Leading Causes of Death,” http://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm
9. Mozaffarian D, et al. “Heart disease and stroke statistics—2015 update: a report from the American Heart Association.” Circulation. 2015. 131:e29. http://circ.ahajournals.org/content/131/4/e29.extract
10. The FH Foundation. “About HoFH.” https://thefhfoundation.org/about-fh/homozygous-familial-hypercholesterolemia/
11. American Heart Association, “What is Cardiovascular Disease?” http://www.heart.org/HEARTORG/Caregiver/Resources/WhatisCardiovascularDisease/What-is-Cardiovascular-Disease_UCM_301852_Article.jsp#
12. Mozaffarian D, et al. “Heart disease and stroke statistics—2015 update: a report from the American Heart Association.” Circulation. 2015. 131:e29. http://circ.ahajournals.org/content/131/4/e29.extract
13. The FH Foundation. “About HoFH.” https://thefhfoundation.org/about-fh/homozygous-familial-hypercholesterolemia/
14. Alonso R, et al. “Cardiovascular disease in familial hypercholesterolaemia: influence of low density lipoprotein receptor mutation type and classic risk factors.” Atherosclerosis. 2008;200(2):315. http://www.ncbi.nlm.nih.gov/pubmed/18243212
15. Jansen AC, et al. “The contribution of classical risk factors to cardiovascular disease in familial hypercholesterolaemia: data in 2400 patients.” J Intern Med. 2004. 256(6):482. http://www.ncbi.nlm.nih.gov/pubmed/15554949
16. The FH Foundation. “About HoFH.” https://thefhfoundation.org/about-fh/homozygous-familial-hypercholesterolemia/
17. Kolansky DM, et al. “Longitudinal evaluation and assessment of cardiovascular disease in patients with homozygous familial hypercholesterolemia.” Am J Cardiol. 2008.102(11):1438. http://www.ncbi.nlm.nih.gov/pubmed/19026292
18. Centers for Disease Control and Prevention. “Cholesterol Fact Sheet.” http://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_cholesterol.htm
19. Mozaffarian D, et al. “Heart disease and stroke statistics—2015 update: a report from the American Heart Association.” Circulation. 2015. 131:e29. http://circ.ahajournals.org/content/131/4/e29.extract
20. Stone NJ, et al. “2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines.” Circulation. 2014.129(suppl 2):S1–S45. http://circ.ahajournals.org/content/129/25_suppl_2/S1.full.pdf
21. Robinson JG. “Management of Familial Hypercholesterolemia: A Review of the Recommendations from the National Lipid Association Expert Panel of Familial Hypercholesterolemia.” J Manag Care Pharm. 19:139-49. 2013. http://www.amcp.org/WorkArea/DownloadAsset.aspx?id=16222
22. National Heart, Lung, and Blood Institute, “How is High Blood Cholesterol Treated?” http://www.nhlbi.nih.gov/health/health-topics/topics/hbc/treatment
23. “Zetia.” http://www.accessdata.fda.gov/drugsatfda_docs/label/2005/21445s007lbl.pdf
24. Robinson JG. “Management of Familial Hypercholesterolemia: A Review of the Recommendations from the National Lipid Association Expert Panel of Familial Hypercholesterolemia.” J Manag Care Pharm. 2013. 19:139. http://www.amcp.org/WorkArea/DownloadAsset.aspx?id=16222
25. The FH Foundation. “About HoFH.” https://thefhfoundation.org/about-fh/homozygous-familial-hypercholesterolemia/
26. The FH Foundation. “About HoFH.” https://thefhfoundation.org/about-fh/homozygous-familial-hypercholesterolemia/

31PhRMA 2016 |
27. Centers for Disease Control and Prevention. “Cholesterol Fact Sheet.” http://www.cdc.gov/dhdsp/data_statistics/fact_sheets/fs_cholesterol.htm
28. Walji S, et al. “Lipoprotein Apheresis for the Treatment of Familial Hypercholesterolemia.” Clin Lipidology. 2013.8(5):573.http://www.medscape.com/viewarticle/811660_2
29. Yokoyama S. “Brief history of low-density lipoprotein apheresis.” Ther Apher Dial. 2003. 7:378. http://www.ncbi.nlm.nih.gov/pubmed/12887718
30. Robinson JG. “Management of Familial Hypercholesterolemia: A Review of the Recommendations from the National Lipid Association Expert Panel of Familial Hypercholesterolemia.” J Manag Care Pharm. 2013. 19:139. http://www.amcp.org/WorkArea/DownloadAsset.aspx?id=16222
31. U.S. Food and Drug Administration. “FDA approves new orphan drug for rare cholesterol disorder.” December 26, 2012. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm333285.htm; U.S. Food and Drug Administration. “FDA approves new orphan drug Kynamro to treat inherited cholesterol disorder.” January 29, 2013. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm337195.htm
32. U.S. Food and Drug Administration. “FDA approves new orphan drug for rare cholesterol disorder.” December 26, 2012. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm333285.htm
33. U.S. Food and Drug Administration. “FDA approves new orphan drug Kynamro to treat inherited cholesterol disorder.” January 29, 2013. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm337195.htm
34. National Human Genome Research Institute. “Learning About Familial Hypercholesterolemia.” https://www.genome.gov/25520184
35. Sejdah NG & Prat A. “The biology and therapeutic targeting of the proprotein convertases.” Nature Reviews Drug Discovery. 2012. 11:367. doi:10.1038/nrd3699.http://www.nature.com/nrd/journal/v11/n5/full/nrd3699.html
36. Sheridan C. “New class PCSK9 blockers stride into cholesterol market.” Nature Biotechnology. 2015. 33:785. doi:10.1038/nbt0815-785. http://www.nature.com/nbt/journal/v33/n8/full/nbt0815-785.html
37. U.S. Food and Drug Administration. “FDA approves Praluent to treat certain patients with high cholesterol.” July 24, 2015. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm455883.htm
38. Sanofi. “Sanofi and Regneron Announce FDA Approval of PRALUENT®(alirocumab) injection, the first PCSK9 inhibitors in the U.S., for the treatment of high LDL cholesterol in adult patients.” July 24, 2015. http://en.sanofi.com/NasdaQ_OMX/local/press_releases/sanofi_and_regeneron_announce__1941221_24-07-2015!21_24_28.aspx
39. U.S. Food and Drug Administration. “FDA approves Repatha to treat certain patients with high cholesterol.” August 27, 2015. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm460082.htm
40. Amgen. “FDA Approves Amgen’s New Cholesterol-Lowering Medication Repatha™ (evolocumab).” August 27, 2015. http://investors.amgen.com/phoenix.zhtml?c=61656&p=irol-newsArticle&ID=2082837
41. U.S. Food and Drug Administration. “FDA Approves New Cholesterol-Lowering Drug.” August 3, 2009. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm175046.htm
42. Kowa Pharmaceuticals America, Inc.. “Livalo.” http://www.kowapharma.com/documents/livalofaq.pdf
43. Kowa Pharmaceuticals America, Inc. “Are you taking a statin other than LIVALO®?” https://www.livalorx.com/statin.php
44. Sheridan C. “New class PCSK9 blockers stride into cholesterol market.” Nature Biotechnology. 2015. 33:785. doi:10.1038/nbt0815-785. http://www.nature.com/nbt/journal/v33/n8/full/nbt0815-785.html
45. Centers for Disease Control and Prevention, “Leading Causes of Death,” http://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm
46. Mozaffarian D, et al. “Heart disease and stroke statistics—2015 update: a report from the American Heart Association.” Circulation. 2015. 131:e29. http://circ.ahajournals.org/content/131/4/e29.extract
47. Adis R&D Insight Database. Accessed December, 2015.
48. American Diabetes Association. “Statistics About Diabetes.” http://www.diabetes.org/diabetes-basics/statistics/
49. U.S. Centers for Disease Control and Prevention. “Number of Americans with Diabetes Projected to Double or Triple by 2050.” http://www.cdc.gov/media/pressrel/2010/r101022.html
50. Mayo Clinic. “Complications.” http://www.mayoclinic.org/diseases-conditions/diabetes/basics/complications/con-20033091
51. National Institute of Diabetes and Digestive and Kidney Diseases. “Diagnosis of Diabetes and Prediabetes.” http://www.niddk.nih.gov/health-information/health-topics/Diabetes/diagnosis-diabetes-prediabetes/Pages/index.aspx

A Decade of Innovation in Chronic Diseases32
52. U.S. Centers for Disease Control and Prevention. “Leading Causes of Death.” http://www.cdc.gov/nchs/fastats/leading-causes-of-death.htm
53. National Institute of Diabetes and Digestive and Kidney Diseases. “Causes of Diabetes.” http://www.niddk.nih.gov/health-information/health-topics/Diabetes/causes-diabetes/Pages/index.aspx
54. American Heart Association. “Cardiovascular Disease & Diabetes.” http://www.heart.org/HEARTORG/Conditions/Diabetes/WhyDiabetesMatters/Cardiovascular-Disease-Diabetes_UCM_313865_Article.jsp/#
55. Mayo Clinic. “Complications.” http://www.mayoclinic.org/diseases-conditions/diabetes/basics/complications/con-20033091
56. National Institute of Diabetes and Digestive and Kidney Diseases. “Diagnosis of Diabetes and Prediabetes.” http://www.niddk.nih.gov/health-information/health-topics/Diabetes/diagnosis-diabetes-prediabetes/Pages/index.aspx
57. National Institute of Diabetes and Digestive and Kidney Diseases. “Diagnosis of Diabetes and Prediabetes.” http://www.niddk.nih.gov/health-information/health-topics/Diabetes/diagnosis-diabetes-prediabetes/Pages/index.aspx
58. American Diabetes Association. “Complications.” http://www.diabetes.org/living-with-diabetes/complications/
59. National Institute of Diabetes and Digestive and Kidney Diseases. “Diagnosis of Diabetes and Prediabetes.” http://www.niddk.nih.gov/health-information/health-topics/Diabetes/diagnosis-diabetes-prediabetes/Pages/index.aspx
60. U.S. Centers for Disease Control and Prevention. “National Diabetes Fact Sheet, 2011.” http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2011.pdf.
61. American Diabetes Association. “Standards of medical care in diabetes – 2015.“ Diabetes Care. 2015. 38(suppl 1):S1. http://care.diabetesjournals.org/content/38/Supplement_1.toc
62. American Diabetes Association. “Standards of medical care in diabetes – 2015.“ Diabetes Care. 2015. 38(suppl 1):S1. http://care.diabetesjournals.org/content/38/Supplement_1.toc
63. American Diabetes Association. “Oral Medication.” http://www.diabetes.org/living-with-diabetes/treatment-and-care/medication/oral-medications/
64. American Diabetes Association. “Insulin Basics.” http://www.diabetes.org/living-with-diabetes/treatment-and-care/medication/insulin/insulin-basics.html
65. Lavernia F, et al. “Use of oral combination therapy for type 2 diabetes in primary care: Meeting individualized patient goals.” Postgraduate Medicine. 2015. 127(8): 808. http://www.tandfonline.com/doi/full/10.1080/00325481.2015.1085293
66. U.S. Food and Drug Administration. “Drugs@FDA.” https://www.accessdata.fda.gov/scripts/cder/drugsatfda/
67. Diabetes Forecast. “Insulins Available in the United States.” http://www.diabetesforecast.org/2015/jul-aug/images/insulin-chart2015rev.pdf
68. U.S. Food and Drug Administration. “Drugs@FDA.” https://www.accessdata.fda.gov/scripts/cder/drugsatfda/
69. http://www.diabetes.org/research-and-practice/student-resources/history-of-diabetes.html
70. U.S. Food and Drug Administration. “Drugs@FDA.” https://www.accessdata.fda.gov/scripts/cder/drugsatfda/
71. Filippatos TD & Elisaf MS. “Effects of glucagon-like peptide-1 receptor agonists on renal function.” World J Diabetes. 2013. 4(5):190. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3797884/
72. U.S. Food and Drug Administration. “FDA Approves New Treatment for Diabetes.” http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2006/ucm108770.htm
73. U.S. Food and Drug Administration. “FDA Approves New Drug Treatment for Type 2 Diabetes.” “http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm174780.htm
74. Boehringer Ingelheim. “FDA approves Tradjenta™ (linagliptin) tablets for the treatment of type 2 diabetes.” http://us.boehringer-ingelheim.com/news_events/press_releases/press_release_archive/2011/april_25_2011.html
75. Takeda. “Takeda Receives FDA Approval for Three New Type 2 Diabetes Therapies, NESINA (alogliptin) and Fixed-Dose Combinations OSENI (alogliptin and pioglitazone) and KAZANO (alogliptin and metformin HCl).” https://www.takeda.com/news/2013/20130126_5626.html
76. Johnson & Johnson. “U.S. FDA Approves INVOKANA™ (Canagliflozin) for the Treatment of Adults with Type 2 Diabetes.” http://www.jnj.com/news/all/us-fda-approves-invokana-canagliflozin-for-the-treatment-of-adults-with-type-2-diabetes
77. Johnson & Johnson. “U.S. FDA Approves INVOKANA™ (Canagliflozin) for the Treatment of Adults with Type 2 Diabetes.” http://www.jnj.com/news/all/us-fda-approves-invokana-canagliflozin-for-the-treatment-of-adults-with-type-2-diabetes
78. Boehringer Ingelheim. “FDA approves Jardiance® (empagliflozin) tablets for adults with type 2 diabetes.” http://us.boehringer-ingelheim.com/news_events/press_releases/press_release_archive/2014/08-01-14-fda-approves-jardiance-empagliflozin-tablets-reduce-blood-sugar-levels-adults-type-2-diabetes.html
33PhRMA 2016 |
79. U.S. Food and Drug Administration. “FDA approves Farxiga to treat type 2 diabetes.” http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm380829.htm
80. U.S. Food and Drug Administration. “Drugs@FDA.” https://www.accessdata.fda.gov/scripts/cder/drugsatfda/
81. García-Pérez L, et al. “Adherence to Therapies in Patients with Type 2 Diabetes.” Diabetes Therapy. 2013. 4(2):175. http://link.springer.com/article/10.1007/s13300-013-0034-y#/lCR72
82. García-Pérez L, et al. “Adherence to Therapies in Patients with Type 2 Diabetes.” Diabetes Therapy. 2013. 4(2):175. http://link.springer.com/article/10.1007/s13300-013-0034-y#/lCR72
83. Hutchins V, et al.“A systematic review of adherence, treatment satisfaction and costs, in fixed-dose combination regimens in type 2 diabetes.” Curr Med Res Opin. 2011. 27(6):1157. http://www.ncbi.nlm.nih.gov/pubmed/21466277
84. Sanofi. “Sanofi Receives FDA Approval of Once-Daily Basal Insulin Toujeo®.” http://www.news.sanofi.us/2015-02-25-Sanofi-Receives-FDA-Approval-of-Once-Daily-Basal-Insulin-Toujeo
85. Sanofi. “Toujeo®.” https://www.toujeo.com/
86. U.S. Food and Drug Administration. “FDA approves two new drug treatments for diabetes mellitus.” http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm464321.htm
87. Novo Nordisk. “Novo Nordisk receives US FDA approval for Tresiba® and Ryzodeg® 70/30.” http://www.novonordisk.com/content/Denmark/HQ/www-novonordisk-com/en_gb/home/media/news-details.1954709.html
88. U.S. Food and Drug Administration. “FDA approves two new drug treatments for diabetes mellitus.” www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm464321.htm
89. Novo Nordisk. “Novo Nordisk receives US FDA approval for Tresiba® and Ryzodeg® 70/30.” http://www.novonordisk.com/content/Denmark/HQ/www-novonordisk-com/en_gb/home/media/news-details.1954709.html l
90. García-Pérez L, et al. “Adherence to Therapies in Patients with Type 2 Diabetes.” Diabetes Therapy. 2013. 4(2):175. http://link.springer.com/article/10.1007/s13300-013-0034-y#/lCR72
91. U.S. Food and Drug Administration. “FDA approves Afrezza to treat diabetes.” http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm403122.htm
92. Sanofi. “Sanofi and MannKind Announce Afrezza®, the Only Inhaled Insulin, Now Available in the U.S.” http://en.sanofi.com/Images/38264_20150203_Afrezza_en.pdf
93. Diabetes Forecast. “Insulin Innovations.” http://www.diabetesforecast.org/2015/jul-aug/insulin-innovations.html
94. U.S. Centers for Disease Control and Prevention. “Number of Americans with Diabetes Projected to Double or Triple by 2050.” http://www.cdc.gov/media/pressrel/2010/r101022.html
95. Diabetes Forecast. “Insulin Innovations.” http://www.diabetesforecast.org/2015/jul-aug/insulin-innovations.html
96. Adis R&D Insight Database. Accessed January 2015.
97. National Multiple Sclerosis Society. “MS the Disease.” http://www.nationalmssociety.org/About-the-Society/Press-Room/MS-the-Disease
98. National Multiple Sclerosis Society. “MS the Disease.” http://www.nationalmssociety.org/About-the-Society/Press-Room/MS-the-Disease
99. National Multiple Sclerosis Society. “MS Symptoms.” http://www.nationalmssociety.org/Symptoms-Diagnosis/MS-Symptoms
100. National Multiple Sclerosis Society. “Types of MS.” http://www.nationalmssociety.org/What-is-MS/Types-of-MS
101. National Multiple Sclerosis Society. “MS Symptoms.” http://www.nationalmssociety.org/Symptoms-Diagnosis/MS-Symptoms
102. National Multiple Sclerosis Society. “Types of MS.” http://www.nationalmssociety.org/What-is-MS/Types-of-MS
103. National Multiple Sclerosis Society. “MS Symptoms.” http://www.nationalmssociety.org/Symptoms-Diagnosis/MS-Symptoms
104. National Institute of Neurological Disorders and Stroke. “Multiple Sclerosis: Hope Through Research.” http://www.ninds.nih.gov/disorders/multiple_sclerosis/detail_multiple_sclerosis.htm
105. National Multiple Sclerosis Society. “Adherence.” http://www.nationalmssociety.org/Treating-MS/Medications/Adherence
106. Coyle PK. “Switching therapies in multiple sclerosis.” CNS Drugs. 2013. 27:239. http://www.ncbi.nlm.nih.gov/pubmed/23508518
107. Castro-Borerro W., et al. “Current and emerging therapies in multiple sclerosis: a systematic review.” Ther Adv Neurol Disord. 2012. 5:205. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3388530/
108. Shryer D. “The medication map.” Momentum Magazine Online. Winter 2013-2014. http://www.momentummagazineonline.com/medication-map-choose-disease-modifying-treatment-ms/

A Decade of Innovation in Chronic Diseases34
109. Shryer D. “The medication map.” Momentum Magazine Online. Winter 2013-2014. http://www.momentummagazineonline.com/medication-map-choose-disease-modifying-treatment-ms/2/
110. U.S. Food and Drug Administration: News & Events. “FDA approves first oral drug to reduce MS relapses.” September 22, 2010. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm226755.htm
111. Spelman T., et al. “Real-world comparative effectiveness of Fingolimod and Interferon/Glatiramer therapies in a switch population using propensity-matched data from MSBase.” 29th Congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS) in Copenhagen, Denmark. October 4, 2013. http://registration.akm.ch/einsicht.php?XNABSTRACT_ID=178930&XNSPRACHE_ID=2&XNKONGRESS_ID=195&XNMASKEN_ID=900
112. Bergvall N., et al. “Relapse rates among patients with multiple sclerosis who switch from interferon therapy to fingolimod or glatiramer acetate: a retrospective US claims database analysis.” Neurology. 2014. 82(10): Supplement P7.211. http://www.neurology.org/content/82/10_Supplement/P7.211
113. Bergvall N., et al. “Relapse rates among patients with a history of relapses treated with fingolimod compared with interferons or glatiramer acetate for the treatment of multiple sclerosis: a retrospective US claims database analysis.” Neurology. 2014. 82(10): Supplement P7.222. http://www.neurology.org/content/82/10_Supplement/P7.222
114. U.S. Food and Drug Administration. “FDA approves new multiple sclerosis treatment Aubagio.” September 12, 2021. http://www.fda.gov/newsevents/newsroom/pressannouncements/ucm319277.htm
115. National Multiple Sclerosis Society. “Aubagio.” http://www.nationalmssociety.org/Treating-MS/Medications/Aubagio
116. Genzyme. “FDA Approves Genzyme’s AUBAGIO® (teriflunomide), a Once-Daily, Oral Treatment for Relapsing Multiple Sclerosis.” September 12, 2012, http://news.genzyme.com/press-release/fda-approves-genzymes-aubagio-teriflunomide-once-daily-oral-treatment-relapsing-multip
117. U.S. Food and Drug Administration. “FDA approves new multiple sclerosis treatment Aubagio.” September 12, 2012. http://www.fda.gov/newsevents/newsroom/pressannouncements/ucm319277.htm
118. U.S. Food and Drug Administration. “FDA approves new multiple sclerosis treatment: Tecfidera.” March 27, 2013. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm345528.htm
119. Biogen. “New Data Show Strong, Sustained Effects of TECFIDERA® (Dimethyl Fumarate) in Newly-Diagnosed and Early Disease Curse Multiple Sclerosis Patients.” October 7, 2015. http://media.biogen.com/press-release/neurology/new-data-show-strong-sustained-effects-tecfidera-dimethyl-fumarate-newly-dia
120. National Multiple Sclerosis Society: News. “FDA Approves Lemtrada™ (alemtuzumab) for Relapsing MS – UPDATE.” November 14, 2014. http://www.nationalmssociety.org/About-the-Society/News/FDA-Approves-Lemtrada%E2%84%A2-%28alemtuzumab%29-for-Relapsing
121. Genzyme. “Genzume’s Lemtrada Approved by the FDA.” November 14, 2014. http://news.genzyme.com/press-release/genzymes-lemtrada-approved-fda
122. U.S. Food and Drug Administration. “FDA Approves Ampyra to Improve Walking in Adults with Multiple Sclerosis.” January 22, 2010. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm198463.htm
123. National Multiple Sclerosis Society. “Walking (Gait) Difficulties.” http://www.nationalmssociety.org/Symptoms-Diagnosis/MS-Symptoms/Walking-%28Gait%29,-Balance-Coordination
124. Adis R&D Insight Database. Accessed January 2016.
125. Pharmaceutical Research and Manufacturers of America. “Medicines in Development for Neurological Disorders: 2015 Report.” http://phrma.org/sites/default/files/pdf/meddevelopment_neurologicaldisorders.pdf
126. Pharmaceutical Research and Manufacturers of America. “2015 Medicines in Development for Neurological Disorders: A Report on Disorders of the Brain, Spinal Cord and Nerves.” June 15, 2015. http://phrma.org/sites/default/files/pdf/2015-neurological-disorders_drug-list.pdf
127. Ledford H. “Drug that boosts nerve signals offers hope for multiple sclerosis.” Nature. April 23, 2015. doi:10.1038/520417a. http://www.nature.com/news/drug-that-boosts-nerve-signals-offers-hope-for-multiple-sclerosis-1.17367
128. United Press International. “’Explosion’ in MS treatments seen.” January 5, 2012. http://www.upi.com/Science_News/2012/01/05/Explosion-in-MS-treatments-seen/90571325786266/
129. National Institute of Arthritis and Musculoskeletal and Skin Diseases. “Handout on health: Rheumatoid Arthritis, What Causes Rheumatoid Arthritis?” http://www.niams.nih.gov/Health_Info/Rheumatic_Disease/#ra_5
130. Arthritis Foundation. “What is Rheumatoid Arthritis?” http://www.arthritis.org/about-arthritis/types/rheumatoid-arthritis/what-is-rheumatoid-arthritis.php
131. Arthritis Foundation. “Rheumatoid Arthritis Symptoms.” http://www.arthritis.org/about-arthritis/types/rheumatoid-arthritis/symptoms.php

35PhRMA 2016 |
132. Arthritis Foundation. “What is Rheumatoid Arthritis?” http://www.arthritis.org/about-arthritis/types/rheumatoid-arthritis/what-is-rheumatoid-arthritis.php
133. Arthritis Foundation. “What is Rheumatoid Arthritis?” http://www.arthritis.org/about-arthritis/types/rheumatoid-arthritis/what-is-rheumatoid-arthritis.php
134. Arthritis Foundation. “What is Rheumatoid Arthritis?” http://www.arthritis.org/about-arthritis/types/rheumatoid-arthritis/what-is-rheumatoid-arthritis.php
135. American College of Rheumatology. “Rheumatoid Arthritis.” http://www.rheumatology.org/I-Am-A/Patient-Caregiver/Diseases-Conditions/Rheumatoid-Arthritis
136. Raza A & Filer A. “The therapeutic window of opportunity in rheumatoid arthritis: does it ever close?” Ann Rheum Dis. 2016. 0:1. http://ard.bmj.com/content/early/2015/03/10/annrheumdis-2014-206993.full.pdf+html
137. Singh JA, et al. “2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis.” Arthritis Care & Research. 2016. 68(1):1. http://www.rheumatology.org/Portals/0/Files/ACR%202015%20RA%20Guideline.pdf
138. Upchurch KS, and Kay J. “Evolution of treatment of rheumatoid arthritis.” Rheumatology (Oxford). 2012. 6:vi28. http://rheumatology.oxfordjournals.org/content/51/suppl_6/vi28.short
139. Upchurch KS, and Kay J. “Evolution of treatment of rheumatoid arthritis.” Rheumatology (Oxford). 2012. 6:vi28. http://rheumatology.oxfordjournals.org/content/51/suppl_6/vi28.short
140. DeKeyser F. “Choice of Biologic Therapy for Patients with Rheumatoid Arthritis: The Infection Perspective.” Curr Rheumatoid Rev. 2011. 7(1):77. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3182090/
141. American College of Rheumatology. “Rheumatoid Arthritis.” http://www.rheumatology.org/I-Am-A/Patient-Caregiver/Diseases-Conditions/Rheumatoid-Arthritis#sthash.tImWusfZ.dpuf
142. Singh JA, et al. “2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis.” Arthritis Care & Research. 2016. 68(1):1. http://www.rheumatology.org/Portals/0/Files/ACR%202015%20RA%20Guideline.pdf
143. American College of Rheumatology. “Rheumatoid Arthritis.” http://www.rheumatology.org/I-Am-A/Patient-Caregiver/Diseases-Conditions/Rheumatoid-Arthritis#sthash.tImWusfZ.dpuf
144. Boston Healthcare. “Recognizing the Value of Innovation in the Treatment of Rheumatoid Arthritis.” March 2013. http://phrma.org/sites/default/files/pdf/BHARAWhitepaperMarch2013.pdf
145. Hyrich KL, et al., “Changes in disease characteristics and response rates among patients in the United Kingdom starting anti-tumour necrosis factor therapy for rheumatoid arthritis between 2001 and 2008,” Rheumatology (Oxford). 2011. 50: 117. http://www.ncbi.nlm.nih.gov/pubmed/20671021
146. Singh JA, et al. “2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis.” Arthritis Care & Research. 2016. 68(1):1. http://www.rheumatology.org/Portals/0/Files/ACR%202015%20RA%20Guideline.pdf
147. Boston Healthcare. “Recognizing the Value of Innovation in the Treatment of Rheumatoid Arthritis.” March 2013. http://phrma.org/sites/default/files/pdf/BHARAWhitepaperMarch2013.pdf
148. Rau R. “Efficacy of methotrexate in comparison to biologics in rheumatoid arthritis.” Clinical and Experimental Rheumatology. 2010. 28(5 Suppl. 61):S58. http://www.ncbi.nlm.nih.gov/pubmed/21044435
149. Singh JA, et al. “2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis.” Arthritis Care & Research. 2016. 68(1):1. http://www.rheumatology.org/Portals/0/Files/ACR%202015%20RA%20Guideline.pdf
150. U.S. Department of Health and Human Services, Agency for Healthcare Research and Quality (AHRQ), “Drug Therapy for Rheumatoid Arthritis in Adults: An Update, Executive Summary,” AHRQ Effective Health Care, Comparative Effectiveness Review, Number 55, 2012. http://www.effectivehealthcare.ahrq.gov/ehc/products/203/1042/CER55_DrugTherapies-rheumatoidarthritis_execsumm.pdf
151. Boston Healthcare. “Recognizing the Value of Innovation in the Treatment of Rheumatoid Arthritis.” March 2013. http://phrma.org/sites/default/files/pdf/BHARAWhitepaperMarch2013.pdf
152. Boston Healthcare. “Recognizing the Value of Innovation in the Treatment of Rheumatoid Arthritis.” March 2013. http://phrma.org/sites/default/files/pdf/BHARAWhitepaperMarch2013.pdf
153. U.S. Food and Drug Administration. “Highlights of Prescribing Information, SIMPONI (galimumab).” www.accessdata.fda.gov/drugsatfda_docs/label/2009/125289s000lbl.pdf
154. U.S. Food and Drug Administration. “Cimzia® (certolizumab pegol).” http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/125160s092lbl.pdf

A Decade of Innovation in Chronic Diseases36
155. Singh JA, et al. “2015 American College of Rheumatology Guideline for the Treatment of Rheumatoid Arthritis.” Arthritis Care & Research. 2016. 68(1):1. http://www.rheumatology.org/Portals/0/Files/ACR%202015%20RA%20Guideline.pdf
156. Genentech. “FDA Approval Rituxan – The First Targeted B-Cell therapy for Treatment of Moderate-to-Sever Rheumatoid Arthritis.” February 28, 2006. http://www.gene.com/media/press-releases/9407/2006-02-28/fda-approves-rituxan-the-first-targeted-
157. U.S. Food and Drug Administration. “Draft Labeling Text: Rituxan® (Rituximab).” http://www.accessdata.fda.gov/drugsatfda_docs/label/2006/103705s5230-s5231lbl.pdf
158. Genentech. “FDA Approves ACTEMRA® (tocilizumab) for the Treatment of Moderately to Severely Active Rheumatoid Arthritis.” January 8, 2010. http://www.gene.com/media/press-releases/12567/2010-01-08/fda-approves-actemra-tocilizumab-for-the
159. U.S. Food and Drug Administration. “Highlights of Prescribing Information: ACTEMRA® (tocilizumab).” http://www.accessdata.fda.gov/drugsatfda_docs/label/2010/125276lbl.pdf
160. U.S. Food and Drug Administration. “Highlights of Prescribing Information: ACTEMRA® (tocilizumab).” http://www.accessdata.fda.gov/drugsatfda_docs/label/2012/125276s0049lbl.pdf
161. Pfizer. “MULTIMEDIA: U.S. Food and Drug Administration Approves Pfizer’s XELJANZ® (tofacitinib citrate) for Adults with Moderately to Severely Active Rheumatoid Arthritis (RA) Who Have Had an Inadequate Response for Intolerance to Methotrexate.” November 7, 2012. http://press.pfizer.com/press-release/multimedia-us-food-and-drug-administration-approves-pfizers-xeljanz-tofacitinib-citrat
162. U.S. Food and Drug Administration. “Highlights of Prescribing Information: XELJANZ® (tofacitinib) tablets, for oral use.” http://www.accessdata.fda.gov/drugsatfda_docs/label/2015/203214s010lbl.pdf
163. Adis R&D Insight Database. Accessed January 2015.
164. Upchurch KS, and Kay J. “Evolution of treatment of rheumatoid arthritis.” Rheumatology (Oxford). 2012. 6:vi28. http://rheumatology.oxfordjournals.org/content/51/suppl_6/vi28.full
165. AIDS.gov. “ What is HIV/AIDS?” https://www.aids.gov/hiv-aids-basics/hiv-aids-101/what-is-hiv-aids/
166. Center for Disease Control and Prevention. “HIV in the United States: At A Glance.” September 29,2015. http://www.cdc.gov/hiv/statistics/basics/ataglance.html =
167. World Health Organization. “HIV/AIDS.” http://www.who.int/gho/hiv/en/
168. Centers for Disease Control and Prevention. “Health, United States, 2013, With Special Feature on Prescription Drugs,” http://www.cdc.gov/nchs/data/hus/hus13.pdf
169. Truven Health Analytics. “Impact of Pharmaceutical Innovation in HIV/AIDS Treatment During the Highly Active Antiretroviral Therapy (HAART) Era in the US, 1987-2010: An Epidemiologic and Cost-Impact Modeling Case Study.” December 2014. http://truvenhealth.com/wp/haart-era-pharma-innovation-hiv-aidstreatment
170. AIDS.gov. “Overview of HIV treatments” https://www.aids.gov/hiv-aids-basics/just-diagnosed-with-hiv-aids/treatment-options/overview-of-hiv-treatments/index.html
171. AIDSInfo. “HIV Treatment.” https://aidsinfo.nih.gov/education-materials/fact-sheets/21/58/fda-approved-hiv-medicines#
172. AIDS.gov. “Medication Adherence.” https://www.aids.gov/hiv-aids-basics/just-diagnosed-with-hiv-aids/treatment-options/medication-adherence/index.html
173. AIDS.gov. “Drug Resistance.” https://www.aids.gov/hiv-aids-basics/just-diagnosed-with-hiv-aids/treatment-options/drug-resistance/index.html
174. AIDSinfo. “HIV Treatment.” December 1, 2015. https://aidsinfo.nih.gov/education-materials/fact-sheets/21/58/fda-approved-hiv-medicines#
175. Astuti N & Maggiolo F. “Single-Tablet Regimens in HIV Therapy.” Infect Dis Ther. 2014. 3:1. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4108118/
176. United States Department of Health and Human Services, Panel on Clinical Practices for Treatment of HIV Infection. “Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents.” November 10, 2003. http://www.cimerman.com.br/artigos/Infectologia/consenso%20americano%20nov%202003.pdf
177. Samji H, et al. “Closing the Gap: increases in life expectancy among treated HIV-postive individuals in the United States and Canada.” PLoS One. 2013. 18:e81355. http://www.ncbi.nlm.nih.gov/pubmed/24367482
178. AIDSInfo. “HIV Treatment, FDA-Approved HIV Medicines.” http://aidsinfo.nih.gov/education-materials/fact-sheets/21/58/fda-approved-hiv-medicines
179. Astuti N & Maggiolo F. “Single-Tablet Regimens in HIV Therapy.” Infect Dis Ther. 2014. 3:1. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4108118/
180. Truong WR, et al. “Once-Daily, Single-Tablet Regimens For the Treatment of HIV-1 Infection.” P T. 2014. 40:44. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4296592/
37PhRMA 2016 |
181. Nachega JB, et al. “Lower pill burden and once-daily antiretroviral treatment regimens for HIV infection: a meta-analysis of randomized controlled trials.” Clin Infect Dis. 2014. 58(9):1297. http://www.ncbi.nlm.nih.gov/pubmed/24457345
182. Hodder SL, et al. “Patient-reported outcomes in virologically suppressed, HIV-1-infected subjects after switching to a simplified, single-tablet regimen of efavirenz, emtricitabine, and tenofovir DF.” AIDS Patient Care STDS. 2010. 24(2):87. http://www.ncbi.nlm.nih.gov/pubmed/20156091
183. Ickovics JR, et al. “Consequences and determinants of adherence to antiretroviral medication: results from Adult AIDS Clinical Trials Group protocol 370.” Antivir Ther. 2002. 7:185. http://www.ncbi.nlm.nih.gov/pubmed/12487386
184. Ickovics JR, et al. “Consequences and determinants of adherence to antiretroviral medication: results from Adult AIDS Clinical Trials Group protocol 370.” Antivir Ther. 2002. 7:185. http://www.ncbi.nlm.nih.gov/pubmed/12487386
185. Cohen CJ, et al. “Association between daily antiretroviral pill burden and treatment adherence, hospitalisation risk, and other healthcare utilisation and costs in a US Medicaid population with HIV.” BJM Open. 2013. 3(8). http://www.ncbi.nlm.nih.gov/pubmed/23906955
186. Truong WR, et al. Once-Daily, Single-Tablet Regimens For the Treatment of HIV-1 Infection.” P T. 2014. 40:44. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4296592/
187. AIDSInfo. “HIV Treatment, FDA-Approved HIV Medicines.” http://aidsinfo.nih.gov/education-materials/fact-sheets/21/58/fda-approved-hiv-medicines
188. Astuti N & Maggiolo F.” Single-Tablet Regimens in HIV Therapy.” Infect Dis Ther. 2014. 3:1. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4108118/
189. AIDSInfo. “HIV Treatment, Drug Resistance.” https://aidsinfo.nih.gov/education-materials/fact-sheets/21/56/drug-resistance
190. U.S. Food and Drug Administration. “FDA Approves New HIV Drug Raltegravir Tablets Used in Combination with Other Antiretroviral Agents.” October 16, 2007. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2007/ucm109008.htm
191. NAM AIDSMap. “New integrase inhibitor dolutegravir helps treatment-experienced people on failing therapy.” http://www.aidsmap.com/New-integrase-inhibitor-dolutegravir-helps-treatment-experienced-people-on-failing-therapy/page/2595521/
192. AIDSMeds.com. “Selzentry or Celsentri (maraviroc).” http://www.aidsmeds.com/archive/selzentry_1629.shtml
193. U.S. Food and Drug Administration. “FDA Approves Novel Antiretroviral Drug.” August 6, 2007. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/2007/ucm108960.htm
194. Bristol-Meyers Squibb. “U.S. Food and Drug Administration Approves Bristol-Meyers Squibb’s Evotaz™ (atazanavir and cobicistat) for the Treatment of HIV-1 Infection in Adults.” January 29, 2015. http://news.bms.com/press-release/financial-news/us-food-and-drug-administration-approves-bristol-myers-squibbs-evotaz-a
195. U.S. Food and Drug Administration. “FDA approves new combination pill for HIV treatment for some patients.” August 27, 2012. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm317004.htm
196. Bristol-Meyers Squibb. “U.S. Food and Drug Administration Approves Bristol-Meyers Squibb’s Evotaz™ (atazanavir and cobicistat) for the Treatment of HIV-1 Infection in Adults.” January 29, 2015. http://news.bms.com/press-release/financial-news/us-food-and-drug-administration-approves-bristol-myers-squibbs-evotaz-a
197. Janssen. “PREZOCOBIX™ (darunavir/cobicistat) Approved in the U.S. for the Treatment of Adults Living with HIV_1.” January 29, 2015. http://www.janssen.com/sites/www_janssen_com_usa/files/pdf/press_releases/PressRelease01292015.pdf
198. U.S. Food and Drug Administration. “FDA approves Egrifta to treat Lipodystrophy in HIV patients.” November 10, 2010. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm233516.htm
199. Patel TS, et al. “Crofelemer for the treatment of chronic diarrhea in patients living with HIV/AIDS.” HIV AIDS (Auckl). 2013. 5:153. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3722035/
200. Centers for Disease Control and Prevention. “Pre-Exposure Prophylaxis (PrEP): PrEP Clinical Trials.” October 28, 2015. http://www.cdc.gov/hiv/prevention/research/prep/
201. Pharmaceutical Research and Manufacturers of America. “Medicines in Development HIV/AIDS 2014.” http://www.phrma.org/sites/default/files/pdf/2014-meds-in-dev-hiv-aids.pdf
202. Samji H, et al. “Closing the Gap: Increases in Life Expectancy among Treated HIV-Positive Individuals in the United States and Canada.” PLoS One. 2013. 8:e81355. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3867319/
203. Faucy AS & Folkers GK. “Toward an AIDS-Free Generation.” JAMA. 2012. 308:343. http://jama.jamanetwork.com/article.aspx?articleID=1221711
204. Armstrong GL, et al. “The Prevalence of Hepatitis C Virus Infection in the United States 1999 through 2002.” Ann Int Med. 2008. 144:705. http://www.ncbi.nlm.nih.gov/pubmed/16702586 ; World Health Organziation. “Hepatitis C.” http://www.who.int/csr/disease/hepatitis/whocdscsrlyo2003/en/index4.html

A Decade of Innovation in Chronic Diseases38
205. World Health Organization. “Hepatitis C.” http://www.searo.who.int/entity/campaigns/world-hepatitis-day/2014/diarrhoea_ari_hepatitis_hepatitisc.pdf
206. Centers for Disease Control and Prevention. “Surveillance for Viral Hepatitis – United States 2013.” http://www.cdc.gov/hepatitis/statistics/2013surveillance/commentary.htm
207. Centers for Disease Control and Prevention. “Viral Hepatitis Surveillance, United States 2013.” http://www.cdc.gov/hepatitis/statistics/2013surveillance/pdfs/2013hepsurveillancerpt.pdf
208. Centers for Disease Control and Prevention. “Surveillance for Viral Hepatitis – United States 2013.” http://www.cdc.gov/hepatitis/statistics/2013surveillance/commentary.htm
209. Hepatitis C Online. “HCV Epidemiology in the United States.” http://www.hepatitisc.uw.edu/pdf/screening-diagnosis/epidemiology-us/core-concept/all
210. Centers for Disease Control and Prevention. “Hepatitis C FAQs for the Public.” http://www.cdc.gov/hepatitis/c/cfaq.htm
211. Hepatitis C Online. “HCV Epidemiology in the United States.” http://www.hepatitisc.uw.edu/pdf/screening-diagnosis/epidemiology-us/core-concept/all
212. Centers for Disease Control and Prevention. “Hepatitis C FAQs for the Public.” http://www.cdc.gov/hepatitis/c/cfaq.htm
213. Xu at al. “Hospitalizations And Costs Associated With Hepatitis C And Advanced Liver Disease Continue To Increase,” Health Affairs. 2014. 33(10):1728. http://content.healthaffairs.org/content/33/10/1728.abstract
214. Razavi H, et al. “Chronic Hepatitis C Virus Burden and Cost in the United States.” Hepatology. 2013. 57(6):2164. http://www.ncbi.nlm.nih.gov/pubmed/23280550
215. LaFleur J, et al. “High rates of early treatment discontinuation in hepatitis C-infected US veterans.” BMC Res Notes. 2014. 7:266. http://www.ncbi.nlm.nih.gov/pubmed/24758162
216. U.S. Food and Drug Administration. “Package Insert, PEG-Intron™ (Peginterferon alpha-2b). Powder for injection, Schering Corporation.” http://www.accessdata.fda.gov/drugsatfda_docs/label/2001/pegsche080701LB.htm
217. U.S. Food and Drug Administration. “VICTRELIS™ (boceprevir) Capsules.” http://www.accessdata.fda.gov/drugsatfda_docs/label/2011/202258lbl.pdf
218. U.S. Food and Drug Administration. “INCIVEK™ (telaprevir) Fil Coated Tablets.”http://www.accessdata.fda.gov/drugsatfda_docs/label/2011/201917lbl.pdf
219. U.S. Food and Drug Administration. “OLYSIO (simeprevir) capsules, for oral use.”http://www.accessdata.fda.gov/drugsatfda_docs/label/2013/205123s001lbl.pdf
220. Gilead. “SOVALDI combination therapy cure rates in clinical studies.” http://www.sovaldi.com/about-sovaldi/study-results
221. Gilead. “SOVALDI combination therapy cure rates in clinical studies.” http://www.sovaldi.com/about-sovaldi/study-results
222. Gilead. “SOVALDI combination therapy cure rates in clinical studies.” http://www.sovaldi.com/about-sovaldi/study-results
223. Gilead. “SOVALDI combination therapy cure rates in clinical studies.” http://www.sovaldi.com/about-sovaldi/study-results
224. U.S. Food and Drug Administration. “FDA approves first combination pill to treat hepatitis C.” October 10. 2014. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm418365.htm
225. Gilead. “A simple treatment regimen for Hep C.” http://www.harvoni.com/discover-harvoni/clinical-study-results
226. Gilead. “U.S. FDA Approves New Indications for Harvoni®, Gilead’s Once-Daily Single Tablet Regimen for Chronic Hepatitis C.” November 12, 2015. http://www.gilead.com/news/press-releases/2015/11/us-fda-approves-new-indications-for-harvoni-gileads-oncedaily-single-tablet-regimen-for-chronic-hepatitis-c
227. Gilead. “U.S. FDA Approves New Indications for Harvoni®, Gilead’s Once-Daily Single Tablet Regimen for Chronic Hepatitis C.” November 12, 2015. http://www.gilead.com/news/press-releases/2015/11/us-fda-approves-new-indications-for-harvoni-gileads-oncedaily-single-tablet-regimen-for-chronic-hepatitis-c
228. Gilead. “U.S. FDA Approves New Indications for Harvoni®, Gilead’s Once-Daily Single Tablet Regimen for Chronic Hepatitis C.” November 12, 2015. http://www.gilead.com/news/press-releases/2015/11/us-fda-approves-new-indications-for-harvoni-gileads-oncedaily-single-tablet-regimen-for-chronic-hepatitis-c
229. Abbvie. “Abbvie Receives U.S. FDA Approval of Viekira Pak™ (Ombitasvir/Paritaprevir/Ritonavir tablets; Dasabuvir tablets) for the Treatment of Chronic Genotype 1 Hepatitis C.” December 19, 2014. http://abbvie.mediaroom.com/2014-12-19-AbbVie-Receives-U-S-FDA-Approval-of-VIEKIRA-PAK-Ombitasvir-Paritaprevir-Ritonavir-Tablets-Dasabuvir-Tablets-for-the-Treatment-of-Chronic-Genotype-1-Hepatitis-C

39PhRMA 2016 |
230. Abbvie. “Technivie™ (Ombitasvir, paritaprevis, and ritonavir tablets) Receives FDA Approval as the First and Only All-Oral, Interferon-Free Treatment for Genotype 4 Chronic Hepatitis C in the U.S.” July 24, 2015. http://abbvie.mediaroom.com/index.php?s=20295&item=122629
231. Bristol-Myers Squibb. “FDA approves Daklinza (daclatasvir) for the Treatment of Patients with Chronic Hepatitis C Genotype 3.” July 24, 2015. http://news.bms.com/press-release/fda-approves-daklinza-daclatasvir-treatment-patients-chronic-hepatitis-c-genotype-3
232. Manns MP, et al. “The way forward in HCV treatment - finding the right path.” Nature Reviews. 2006. 6:991. http://www.nature.com/nrd/journal/v6/n12/full/nrd2411.html
233. U.S. Food and Drug Administration. “VICTRELIS™ (boceprevir) Capsules.” http://www.accessdata.fda.gov/drugsatfda_docs/label/2011/202258lbl.pdf
234. U.S. Food and Drug Administration. “INCIVEK™ (telaprevir) Fil Coated Tablets.”http://www.accessdata.fda.gov/drugsatfda_docs/label/2011/201917lbl.pdf
235. U.S. Food and Drug Administration. “FDA approves new treatment for hepatitis C virus.” November 22, 2013. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm376449.htm
236. U.S. Food and Drug Administration. “OLYSIO (simeprevir) capsules, for oral use.” http://www.accessdata.fda.gov/drugsatfda_docs/label/2013/205123s001lbl.pdf
237. Gilead. “U.S. Food and Drug Administration Approval Gilead’s SOVALDI™ (Sofosbuvir) for the Treatment of Chronic Hepatitis C.” December 6, 2013. http://www.gilead.com/news/press-releases/2013/12/us-food-and-drug-administration-approves-gileads-sovaldi-sofosbuvir-for-the-treatment-of-chronic-hepatitis-c
238. U.S. Food and Drug Administration. “FDA approval Sovaldi for chronic hepatitis C treatment.” December 6, 2013. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm377888.htm
239. Manns MP, et al. “The way forward in HCV treatment - finding the right path.” Nature Reviews. 2006. 6:991. http://www.nature.com/nrd/journal/v6/n12/full/nrd2411.html
240. Gilead. “SOVALDI combination therapy cure rates in clinical studies.” http://www.sovaldi.com/about-sovaldi/study-results
241. Gilead. “A simple treatment regimen for Hep C.” http://www.harvoni.com/discover-harvoni/clinical-study-results
242. U.S. Food and Drug Administration. “FDA approves first combination pill to treat hepatitis C.” October 10, 2014. http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm418365.htm
243. Abbvie. “Abbvie Receives U.S. FDA Approval of Viekira Pak™ (Ombitasvir/Paritaprevir/Ritonavir tablets; Dasabuvir tablets) for the Treatment of Chronic Genotype 1 Hepatitis C.” December 19, 2014. http://abbvie.mediaroom.com/2014-12-19-AbbVie-Receives-U-S-FDA-Approval-of-VIEKIRA-PAK-Ombitasvir-Paritaprevir-Ritonavir-Tablets-Dasabuvir-Tablets-for-the-Treatment-of-Chronic-Genotype-1-Hepatitis-C
244. Bristol-Myers Squibb. “FDA approves Daklinza (daclatasvir) for the Treatment of Patients with Chronic Hepatitis C Genotype 3.” July 24, 2015. http://news.bms.com/press-release/fda-approves-daklinza-daclatasvir-treatment-patients-chronic-hepatitis-c-genotype-3
245. Abbvie. “Technivie™ (Ombitasvir, paritaprevis, and ritonavir tablets) Receives FDA Approval as the First and Only All-Oral, Interferon-Free Treatment for Genotype 4 Chronic Hepatitis C in the U.S.” July 24, 2015. http://abbvie.mediaroom.com/index.php?s=20295&item=122629
246. Gilead. “U.S. FDA Approves New Indications for Harvoni®, Gilead’s Once-Daily Single Tablet Regimen for Chronic Hepatitis C.” November 12, 2015. http://www.gilead.com/news/press-releases/2015/11/us-fda-approves-new-indications-for-harvoni-gileads-oncedaily-single-tablet-regimen-for-chronic-hepatitis-c
247. Adis R&D Insight Database. Accessed January 2016.
248. M. Kabiri et al. “The Changing Burden of Hepatitis C Virus Infection in the United States: Model-Based Predictions,” Annals of Internal Medicine. 2014. 101(6):170. http://annals.org/article.aspx?articleid=1892615&resultClick=3
249. Alzheimer’s Association. “Changing the trajectory of Alzheimer’s Disease: how a treatment by 2025 saves lives and dollars.” Washington, DC: Alzheimer’s Association; 2015.
250. http://www.alz.org/documents_custom/trajectory.pdf.

for more information please visit: www.phrma.org
February 2016