a comparison of somatosensory evoked and motor evoked potentials in stroke
TRANSCRIPT

A Comparison of Somatosensory Evoked and Motor Evoked Potentials in Stroke R. A. L. Macdonell, MBBS, FRACP, G. A. Donnan, MD, FRACP, and P. F. Bladin, MD, FRACP
~
Nineteen patients with radiologically confirmed stroke, and varying degrees of hemiparesis, were studied using somatosensory evoked potentials and the recently developed technique of transcutaneous motor cortex stimulation. The functional deficit caused by stroke was assessed at the time of evoked potential testing and again on follow-up 2 months after stroke. Stroke location and degree of recovery were compared with the evoked potentials elicited an average of 8 days after the acute event. The motor response was better ( p < 0.01) than somatosensory response at predicting an outcome in terms of functional recovery, both overall and when comparing patients with similar degrees of weakness. Normal somatosensory evoked potentials also predicted recovery but were not as sensitive as the motor evoked potentials (0.01 < p < 0.05). Motor evoked potentials in conjunction with clinical assessment may offer a means of more accurately predicting functional outcome following stroke than can be achieved with clinical assessment, with or without somatosensory evoked potentials. The additional finding that cortically evoked motor evoked potentials were delayed only by subcortical lesions is of interest and may extend the understanding of the pathophysiological mechanism of this response in humans.
Macdonell RAL, Donnan GA, Bladin PF. A comparison of somatosensory evoked and motor evoked potentials in stroke. Ann Neurol 1989;25:68-73
The ability of somatosensory evoked potentials (SEPs) to predict functional outcome following stroke has previously been investigated [l, 2). Although there appears to be a correlation between an intact SEP and functional improvement, the SEP is an indirect means of assessment, since it measures the electrophysiolog- ical integrity of sensory rather than motor pathways in the spinal cord and brain [ 3 , 4). Disability following stroke is mainly due to loss of motor function, which until recently could not be assessed directly using elec- trophysiological techniques.
The recent development of percutaneous electrical stimulation of the motor cortex has permitted for the first time investigation of corticospinal pathways in the awake human subject [S-9}. Several disease processes known to affect corticospinal pathways, including stroke, have been shown to be associated with abnor- malities of motor conduction using this technique, while disorders of extrapyramidal pathways, such as Parkinson’s disease, have been shown to be associated with normal motor conduction L9-181.
In this study, we compared motor and sensory evoked potentials and functional recovery after stroke and also examined the relationship between stroke lo- cation as defined radiologically and the motor evoked potential (MEP).
Patients and Methods Nineteen patients were studied, all inpatients of the Austin Hospital Stroke Unit. The 13 men and 6 women ranged in age from 60 to 81 years (mean 70 years). The diagnosis of stroke was made clinically, and location of infarction or hemorrhage was confirmed by computed tomographic scan- ning and in some cases also by magnetic resonance imaging. All patients gave informed consent to the study, which was approved by the hospital ethics committee.
Percutaneous stimulation of the cervical spine and motor cortex on each side was performed using a Digitimer D180 stimulator. This device produces stimuli of up to 750 V and peak current of up to 1.2 A. A time constant of 50 psec was used for each stimulus. The stimuli were delivered through two saline-soaked felt pads (2 cm diameter) mounted 6 cm apart. Cortical stimulation was performed with the cathode at the vertex and anode 6 cm lateral on a line between the vertex and the external auditory meatus. Stimulus intensity for cortical stimulation was between 90 and 100% of max- imum output. Spinal stimulation was performed with the cathode placed over the C-6 interspinous space and the anode placed 6 cm laterally. Stimulus intensity at this site was 50 to 60% of maximum output. The electromyographic sig- nals were recorded by saline-soaked pads 2 cm apart over the appropriate thenar muscles, then amplified using a Nihon Kohden Neuropack 8. The responses were recorded on a floppy disk by the Neuropack 8 built-in computer.
A series of single trials, each of equal stimulus intensity, 3
From the Department of Neurology, Austin Hospital, Victoria, Australia.
Received Mar 14, 1988, and in revised form Jun 10. Accepted for publication Jul 2, 1988.
Address correspondence to Dr Donnan, Department of Neurology, Austin Hospital, Studley Rd, Heidelberg, Victoria 3084, Australia
68 Copyright 0 1989 by the American Neurological Association

Table I. Normal Somatosensory Evoked Potential Valuesa
Latency (msec)
N13 13.8 t 1.1 N20 20.0 -t 1.4 Central conduction time 6.2 t 0.8 Interside difference of 1.8 (95% confidence limit)
central conduction time ~ ~-
"Values expressed as mean f standard deviation.
at each site, was recorded while the patient was instructed to relax. The response was not facilitated by contraction of the target muscle because it is difficult to compare percentage of maximal contraction exerted by normal compared with pa- retic or paralyzed muscles 111).
In most cases, a satisfactory response was recorded after each stimulus. The response of shortest latency recorded from each stimulation site was used for later analysis. Al- though this technique produced some discomfort, it was tol- erated without complaint by all patients and control subjects.
SEPs were elicited by stimulation of the median nerve at the wrist, and the responses were recorded from Erb's point, over the cervical spine at C-6, and from the scalp. Unilateral stimulation was performed on each side, and scalp recordings were made using Ag/AgC 1 electroencephalographic elec- trodes placed 7 cm lateral and 3 cm posterior to the vertex. A midfrontal (Fpz) electrode was used as reference. Five hundred and twelve responses were averaged, using a fre- quency band-pass of 20 to 3,000 H t . The averaged response was repeated to ensure reproducibility and recorded on a floppy disk as described above. During testing, the patients either lay on a couch or sat in a reclining chair.
Normal values for SEPs and motor conduction latencies, listed in Tables 1 and 2, were established using the protocols described above. The normal SEP group consisted of 40 volunteers without a history of neurological disease and rang- ing in age from 40 to 81 years. There were 10 subjects in each age decade over this range, and in each decade there were 5 men and 5 women. The normal motor conduction latency group consisted of 12 volunteers from our neurology department who ranged in age from 25 to 48 years (mean 35 years). Control subjects were stimulated at both scalp and cervical spine levels, and each response was recorded from the appropriate thenar muscles in a relaxed state. In all ex- cept 1 subject stimulation was performed bilaterally.
Absent thenar MEPs following either spinal or cortical stimulation or absence of the SEP response at the neck (N13) or the contralateral scalp (N20) after median nerve stimulation was considered abnormal. In assessing other ab- normalities, interpeak latency measurements were used; for SEPs these were the N13-N20 interpeak interval (central conduction time {CCT]) and the difference in CCT between right and left median nerve stimulation (interside difference) u97.
Central motor conduction time (CMCT), the difference between the latencies of spinally and cortically evoked thenar CMAPs, was used in the assessment of MEPs. CMCT ap- proximated the time taken for the stimulus to pass between the motor cortex and the cervical spinal cord 1203. The inter-
Table 2. Latencies of Thenar Compound Muscle Action Potentials"
Latency (msec)
Cortex 20.4 t 1.9 Spinal cord (C-6) 13.7 c 1.4 Central motor conduction 6.7 t 1.1
time
tral motor conduction limit) time
Interside difference of cen- 0.8 (95% confidence
"Values expressed as mean 2 standard deviation.
1
i n
: L stimulation I t h e m i
If--- 10.25mV
\( 60 . 8 0 , 1oopsec " 4.0 ,
Fig I . Electromyographic responses recorded from the right thenar muscles of a normal subject after stimuhtion wer the cervical spinal cord (upper trace) and the opposite motor cortex (lower trace).
side difference for CMCT comparing right with left sides was also measured. Interpeak measurements were preferred be- cause they do not vary with arm length and they are not affected by disorders of peripheral nerve [3]. CCT and CMCT were considered abnormal if the latency fell more than three standard deviations outside the mean of the con- trol population. Interside differences for CMCT and CCT were nongaussian in distribution; a 95% tolerance limit was therefore defined for each. Normal spinally and cortically evoked MEPs are illustrated in Figure 1.
The use of evoked potentials to assess the likelihood of functional recovery after stroke was assessed prospectively. The functional disability caused by stroke was assessed at the time of evoked potential testing and at outpatient follow-up several weeks after stroke (mean 2.2 months; range 1-6 months). Outcomes were classified into three groups based upon the relative degree of eventual recovery: complete, partial, or no recovery or death. Complete recovery was defined as an absence of functional disability. Completely recovered patients returned home from the hospital and were fully independent in their daily living. Partial recovery
Macdonell et al: MEPs and SEPs in Stroke G9

Table 3. Clinical Features, Radiographic Findings, Response to Motor Cortex Stimulation, and SEPs on the Side of Stroke and Recovery at Follow-up
Stroke-Testing Interside FO~~OW-UP Patient Age Arm Intervalb Difference SEP Interval' No. (yr) Strength" Sensation (days) CTIMRI Localization CMCT in CMCT (N20) Recoveryd (mo)
1 2 3 4 5 6 7 8 9
10 11 12 13 14 15 16' 17 18' 19
77 73 76 66 81 67 75 63 74 71 68 60 70 67 69 75 60 71 76
315 415 315 315 315 315 015 015 015 415 415 415 415 315 415 015 015 015 015
N D D N D+ D+ D+ D+ D+ D N N N N N D + D + D+ D+
8 8 1 2 4
20 1 8 5 3 2 3
30 4 4 1
20 6
28
L cortical infarct R cortical infarct L cortical infarct R cortical infarct L cortical infarct R cortical infarct R cortical infarct R cortical infarct L cortical infarct R subcortical hemorrhage R lacunar infarct L lacunar infarct L thalamic lacuna L pontine infarct L pontine infarct L thalamic hemorrhage R subcortical watershed L Sdcapsular infarct L Sdcapsular infarct
N N N N A A A A A N N N Del Del A Del A A A
N N N N N N N N . . . N . . . N . . . A . . . A . . . A N A N N AbN A AbN N AbN N . . . N AbN A . . . A . . . A . . . A
I 2 I1 1 I1 1 I1 2
111 2 111 3 111 2 111 1 111 3 I1 1 I 2 I 6 I 4 I 2 I 5
111 . . . 111 2 111 . . . 111 4
'0 = no strength, 5 = full strength. %me between stroke and evoked potential testing. 'Right versus left cortical stimulation. dI = full recovery; I1 = moderate, but not full, recovery; 111 = no recovery or death. T ime from evoked potential testing to outpatient follow-up. 'Died due to stroke within 3 weeks of onset.
SEP = somatosensory evoked potential; CT = computed tomography; MRI = magnetic resonance imaging; CMCT = central motor conduction time; R = nght; L = left; N = normal; D = decreased; D+ = much decreased; A = absent; Del = delayed; AbN = abnormal; St = striatocapsular.
meant an improvement in the level of disability compared with the initial assessment, although not complete improve- ment. At the time of reassessment, the patients in this cate- gory either already had or were expected to return home after a period of rehabilitation. No recovery represented no improvement in any functional disability compared with the initial assessment. These patients required full-time nursing care and were unable to return home.
Statistical analysis was performed using the chi-square test with Yates' correction.
Results The 19 patients were tested a mean of 8 days after the onset of stroke (range 1-30 days). They were divided into two groups depending on stroke location as im- aged by computed tomography. Nine patients had sus- tained recent cortical infarction, and 10 a recent sub- cortical stroke (8 infarcts, 2 hemorrhages). All were hemiparetic to varying degrees at the time of testing, and many also had sensory loss. Clinical, computed tomographic, and evoked potential findings are listed in Table 3.
Cortical Infarction According to appearance on computed tomographic or magnetic resonance scans, the infarcts were classified
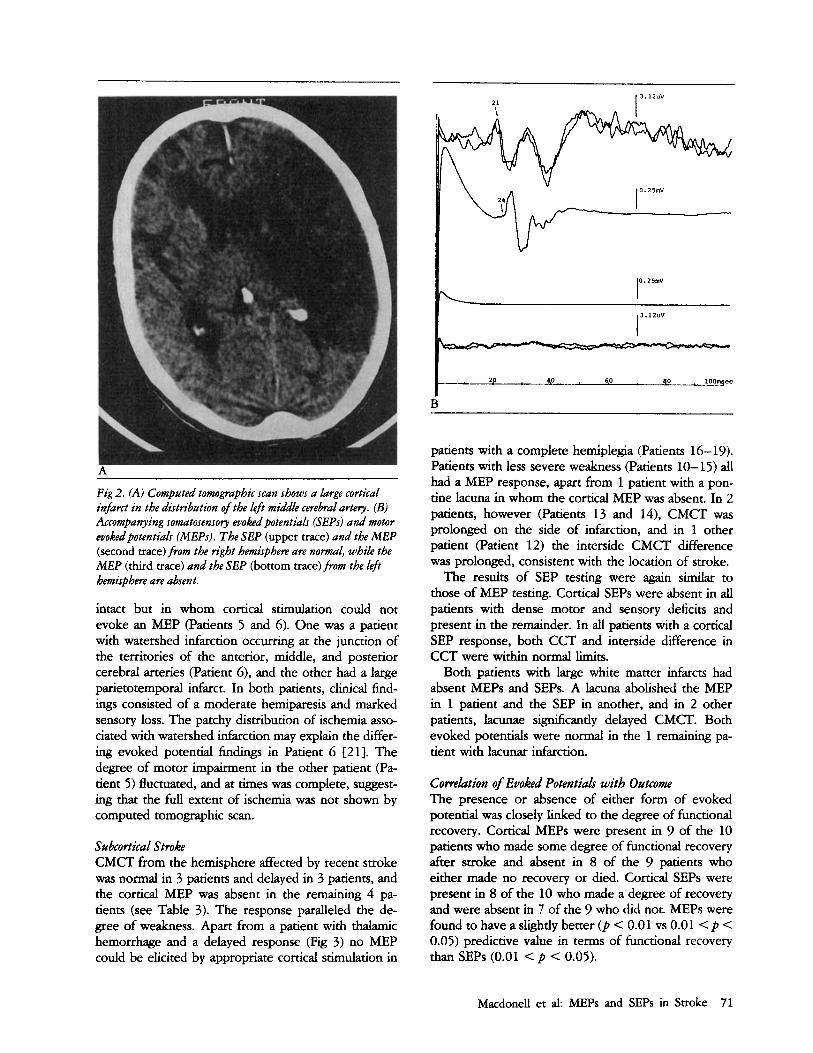
as being within the distribution of (1) a small distal branch of the middle cerebral artery (Patient l), (2) a major division of the middle cerebral artery (Patients 2-5), (3) the cortical watershed zone (Patient 6), or (4) the full middle cerebral artery territory (Patients 7-9). It was not possible to evoke a motor response from the affected side in 5 patients with cortical infarction (Pa- tients 5-9; see Table 3), although the responses to spinal stimulation and stimulation of the opposite hemisphere remained intact (Fig 2). CMCT in the re- maining 4 patients (Patients 1-4) was normal.
In general, SEP findings were similar to MEP findings. The cortical SEP response was absent in 3 of the 5 patients with no MEP response, and it was pres- ent in all patients from whom a cortical MEP could be elicited. Both CCT and the interside difference in CCT were within normal limits in all patients in whom it could be measured. Patients with preserved evoked potentials had smaller infarcts on computed tomo- graphic scans and as detected clinically and were less severely disabled than patients in whom both re- sponses were abolished. This latter group had infarcts in the full distribution of the middle cerebral artery or one of its major branches.
There were 2 patients in whom the cortical SEP was
70 Annals of Neurology Vol 25 No 1 January 1989
2 1 I 3.12uv
Fig 2. (A) Computed tomographic scan shows a large cortical infarct in the distribution ofthe left middle cerebral artery. (B) Accompanying somatosensory evoked potentials (SEPs) and motor evokedpotentials (MEPs). The SEP (upper trace) and the MEP (second trace) from the right hemisphere are normal, while the MEP (third trace) and the SEP (bottom trace) from the ldt hemisphere are absent.
intact but in whom cortical stimulation could not evoke an MEP (Patients 5 and 6). One was a patient with watershed infarction occurring at the junction of the territories of the anterior, middle, and posterior cerebral arteries (Patient 6), and the other had a large parietotemporal infarct. In both patients, clinical find- ings consisted of a moderate hemiparesis and marked sensory loss. The patchy distribution of ischemia asso- ciated with watershed infarction may explain the differ- ing evoked potential findings in Patient 6 f21). The degree of motor impairment in the other patient (Pa- tient 5) fluctuated, and at times was complete, suggest- ing that the full extent of ischemia was not shown by computed tomographic scan.
Sabcortical Stroke CMCT from the hemisphere affected by recent stroke was normal in 3 patients and delayed in 3 patients, and the cortical MEP was absent in the remaining 4 pa- tients (see Table 3). The response paralleled the de- gree of weakness. Apart from a patient with thalamic hemorrhage and a delayed response (Fig 3) no MEP could be elicited by appropriate cortical stimulation in
B
patients with a complete hemiplegia (Patients 16-19). Patients with less severe weakness (Patients 10-15) all had a MEP response, apart from 1 patient with a pon- tine lacuna in whom the cortical MEP was absent. In 2 patients, however (Patients 13 and 14), CMCT was prolonged on the side of infarction, and in 1 other patient (Patient 12) the interside CMCT difference was prolonged, consistent with the location of stroke.
The results of SEP testing were again similar to those of MEP testing. Cortical SEPs were absent in all patients with dense motor and sensory deficits and present in the remainder. In all patients with a cortical SEP response, both CCT and interside difference in CCT were within normal limits.
Both patients with large white matter infarcts had absent MEPs and SEPs. A lacuna abolished the MEP in 1 patient and the SEP in another, and in 2 other patients, lacunae significantly delayed CMCT. Both evoked potentials were normal in the 1 remaining pa- tient with lacunar infarction.
Cowelation of Euoked Potentials with Outcome The presence or absence of either form of evoked potential was closely linked to the degree of functional recovery. Cortical MEPs were present in 9 of the 10 patients who made some degree of functional recovery after stroke and absent in 8 of the 9 patients who either made no recovery or died. Cortical SEPs were present in 8 of the 10 who made a degree of recovery and were absent in 7 of the 9 who did not. MEPs were found to have a slightly better ( p < 0.01 vs 0.01 < p < 0.05) predictive value in terms of functional recovery than SEPs (0.01 < p < 0.05).
MacdoneU et al: MEPs and SEPs in Stroke 71

B
Fig 3. (A) Computed tomographic scan shows a ldt thabmic hemowhage. (B) Evoked potentials show a normal somatosensory evokedpotential (SEP) (upper trace) and motor evoked potential (MEP) (second trace) from the right hemisphere and a delayed MEP (third trace) and absent SEP (bottom trace) from the lt$t hemisphere.
Discussion The findings in this series of patients indicate that the MEP is able to detect abnormal conduction in de- scending corticospinal pathways following stroke and provides prognostic information regarding the likeli- hood of functional recovery.
A further finding of interest is that delayed CMCT following stroke may be indicative of a subcortical le- sion. While absent MEPs and normal MEPs were seen after both cortical and subcortical stroke, only subcor- tical involvement increased the latency of the cortical MEP. The reason for this is suggested by the likely physiological mechanism of the motor response, which is thought to be analogous to that operating in experi- mental direct motor cortex stimulation of animals 18, 11, 22-27]. Motor cortex stimulation in primates pro- duces a series of waves in the ipsilateral medullary pyramid or contralateral corticospinal tract. The initial wave, called the D-wave, is thought to be due to direct stimulation of pyramidal tract neurons. The D-wave is followed at approximately 1 to 2 msec intervals by a succession of later deflections known as I-waves. D- waves can be evoked by subcortical stimulation after
cortical ablation, whereas I-waves cannot, suggesting that I-waves are dependent on intact gray matter and are transsynaptically generated by “relayed excitation of pyramidal neurons through cortical interneurons” 122). The D-wave alone is insufficient to produce elec- tromyographic activity in relaxed limb muscles, but temporal summation of D-waves and I-waves on ante- rior horn cells can cause depolarization sufficient to exceed the firing threshold 111, 26, 281. Thus, for motor cortex stimulation to evoke electromyographic activity, the cerebral cortex must be capable of generating both the initial D-wave and a train of I- waves.
The observation that only subcortical lesions de- layed conduction and prolonged CMCT can be ex- plained if it is accepted that the response is cortically generated. Subcortical lesions would therefore have little effect on the generation of the response but might alter its transmission via corticospinal pathways to the spinal cord. Conditions such as multiple sclero- sis spare the cortex but affect the subcortex delay CMCT [7,9}. Subcortical strokes may produce similar effects by destroying andor distorting descending motor pathways through infarction, hemorrhage, or edema. If corticospinal pathways are sufficiently inter- rupted, the MEP is lost; if the interruption is less se- vere, the descending volley may be reduced and/or tem- porally dispersed, giving rise to a delayed response [ 111.
The results of motor cortex stimulation following cortical infarction suggest that after cortical infarction the response is an all-or-none phenomenon dependent on whether there are sufficient surviving corticospinal tract and cortical interneurons to propagate the stim-
72 Annals of Neurology Vol 25 No 1 January 1989
ulus to a degree capable of triggering the appropriate anterior horn cell pool. This contention is supported by the finding that the response to cortical stimulation is often absent in conditions affecting the cortex, such as motor neuron disease and stroke f12-15).
Comparison of MEPs and SEPs revealed that each may be affected independently by stroke, confirming that they rely on anatomically discrete pathways. This fact may be useful in assessing the extent of neurolog- ical dysfunction, particularly in patients whose mental state does not permit an accurate neurological exami- nation.
SEPs have previously been shown to be useful in the assessment of likely outcome following stroke f l , 2). We found that the MEP was slightly more reliable in predicting the likelihood of functional recovery, which is hardly surprising, considering that functional recov- ery relies more on the return of motor function than on the return of sensory function. Similar findings re- garding the comparative prognostic value of SEPs and MEPs following experimental spinal cord trauma have also recently been reported {29}. The recent advent of a painless magnetic technique for motor cortex stimu- lation overcdmes the major objection to motor cortex stimulation in routine use f27, 30-32). Motor cortex stimulation may prove useful in the future in assessing prognosis after stroke and in planning rehabilitation.
Dr Macdonell is supported by a Medical Postgraduate Research Scholarship from the National Health and Medical Research Council of Australia.
References 1. Pavot AP, Ignacio DR, Kuntavanish A, Lightfoote WE. The
prognostic value of somatosensory evoked potentials in cere- brovascular accidents. Electromyogr Clin Neurophysiol 1986;
2. LaJoie WJ, Reddy NM, Melvin JL. Somatosensory evoked po- tentials: their predictive value in right hemiplegia. Arch Phys Med Rehabil 1982;63:223-226
3. Chiappa KH. Evoked potentials in clinical medicine. New York Raven Pr., 1983
4. Halliday AM, Wakefield GS. Cerebral evoked potentials in pa- tients with dissociated sensory loss. J Neurol Neurosurg Psychi- atry 1963;26:211-219
5. Merton PA, Morton HB. Stimulation of the cerebral cortex in the intact human subject. Nature 1980;285:227
6. Merton PA, Morton HB, Hill DK, Marsden CD. Scope of a technique for electrical stimulation of human brain, spinal cord and muscle. Lancet 1982;2:597-600
7. Mills KR, Murray NMF. Corticospinal tract conduction time in multiple sclerosis. Ann Neurol 1985;18:601-605
8. Rothwell JC, Day BL, Thompson PD, et al. Some experiences of techniques for stimulation of the human cerebral motor cor- tex through the scalp. Neurosurgery 1987;20:156-163
9. Cowan JMA, Dick JPR, Day BL, et al. Abnormalities in central motor pathway conduction in multiple sclerosis. Lancet
10. Snooks SJ, Swash M. Motor conduction velocity in the human spinal cord: slowed conduction in multiple sclerosis and radia-
26:333-340
1984;2:304-307
tion myelopathy. J Neurol Neurosurg Psychiatry 1985;48: 135- 139
11. Thompson PD, Day BL, Rothwell JC, et al. The interpretation of electromyographic responses to electrical stimulation of the motor cortex in diseases of the upper motor neurone. J Neurol Sci 1987;80:91-110
12. Berardelli A, Inghilleri M, Manfredi M, et al. Cortical and cervi- cal stimulation after hemispheric infarction. J Neurol Neurosurg Psychiatry 1987;50:861-865
13. Ingram DA, Swash M. Central motor conduction is abnormal in motor neuron disease. J Neurol Neurosurg Psychiatry 1987;
14. Berardelli A, Inghilleri M, Formisano R, et al. Stimulation of motor tracts in motor neuron disease. J Neurol Neurosurg Psy- chiatry 1987;50:732-737
15. Hugon J, Lubeau M, Tabaraud F, et al. Central motor conduc- tion in motor neuron disease. Ann Neurol 1987;22:544-546
16. Thompson PD, Dick JPR, Asselman P, et al. Examination of motor function in lesions of the spinal cord by stimulation of the motor cortex. Ann Neurol 1987;2 1:389-396
17. Dick JPR, Cowan JMA, Day BL, et al. The corticomotoneurone connection is normal in Parkinson’s disease. Nature 1984;
18. Thompson PD, Dick JPR, Day BL, et al. Electrophysiology of the corticomotoneurone pathways in patients with movement disorders. Movement Dis 1986;1:113-117
19. Hume AL, Cant BR. Conduction time in central somatosensory pathways in man. Electroencephalogr Clin Neurophysiol
20. Mills KR, Murray NMF. Electrical stimulation over the human vertebral column: which neural elements are excited? Electroen- cephalogr Clin Neurophysiol 1986;63:582-589
21. Chu NS. Median and tibial somatosensory evoked potentials: changes in short- and long-latency components in patients with lesions of the thalamus and thalamo-cortical radiations. J Neurol Sci 1986;76: 199-2 19
22. Patton HD, Amassian VA. Single- and multiple-unit analysis of cortical stage of pyramidal tract activation. J Neurophysiol
23. Landau WM, Bishop GH, Clare MH. Site of excitation in sum- ulation of the motor cortex. J Neurophysiol1966;29:1206-1222
24. Kernell D, Wu CP. Responses of the pyramidal tract to stimula- tion of the baboon’s motor cortex. J Physiol 1967;191:653-672
25. Amassian VA, Stewart M, Quirk GJ, Rosenthal JL. Physiologi- cal basis of motor effects of a transient stimulus to cerebral cortex. Neurosurgery 1987;20:74-93
26. Phillips CG, Porter R. Corticospinal neurones, their role in movement. Monographs of the physiological society. No. 34. London: Academic Pr, 1977
27. Day BL, Thompson PD, Dick JP, et al. Different sites of action of electrical and magnetic stimulation of the human brain. Neurosci Lett 1987;75:101-106
28. Cracco RQ. Evaluation of conduction in central motor path- ways: techniques, pathophysiology, and clinical interpretation. Neurosurgery 1987;20:199-203
29. Levy WJ, McCaffrey M, Hagichi S. Motor evoked potential as a predictor of recovery in chronic spinal cord injury. Neurosurgery 1987;20 138-141
30. Barker AT, Jalinous R, Freeston IL. Non-invasive magnetic stimulation of human motor cortex. Lancet 1985;1:1106-1107
31. Hess CW, Mills KR, Murray NMF. Measurement of central motor conduction in multiple sclerosis by magnetic brain stimu- lation. Lancet 1986;2: 3 5 5-3 58
32. Barker AT, Freeston IL, Jalinous R, Jarratt JA. Clinical evalua- tion of conduction time measurements in central motor path- ways using magnetic stimulation of human brain. Lancet
50: 159- 166
3101407-409
1978;45:361-375
1954;17:345-363
1986;1:1325-1326
Macdonell et al: MEPs and SEPs in Stroke 73