a comparative review of essential health benefits pertinent€¦ · a comparative review of...
TRANSCRIPT


A Comparative Review of Essential Health Benefits Pertinentto Children in Large Federal, State, and Small Group Health Insurance
Plans: Implications for Selecting State Benchmark Plans
Prepared by Peggy McManus, MHSfor the American Academy of Pediatrics
July 2012
Executive Summary This report compares benefit and cost-sharing policies pertinent to children in the three
largest federal employee health plans and in one of the largest state employee and small groupplans in Alabama, Colorado, Maryland, Texas, and Washington. The purpose of this study is toexamine how well these plans meet the needs of children from birth through age 21, including thosewith special health care needs, and what policy issues the U.S. Department of Health and HumanServices (HHS) and states will likely face in selecting and monitoring states’ benchmark plans underthe Affordable Care Act (ACA).
Overall, federal employee plans offered the most comprehensive coverage for children,followed next by state employee plans. Small group plans, with some exceptions, have the mostlimited coverage and cost-sharing policies for children. Of course, none of these plans compared tothe expansive coverage available in Medicaid’s Early Periodic Screening, Diagnosis and Treatment(EPSDT) program or even in separate Children’s Health Insurance Program (CHIP) plans.
Two categories of essential health benefits (EHBs) – rehabilitative and habilitative servicesand pediatric services, including oral and vision (as well as hearing) services – will likely need to besupplemented, as required by HHS, because coverage was often missing. Specifically, planssurveyed in this study often failed to cover or specify habilitative therapy and private duty nursing,and they also excluded or failed to articulate coverage for specific preventive, diagnostic, andrestorative oral services as well as services such as hearing aids and hearing-related implants. Atissue will be the extent to which, even with added coverage, oral health and habilitative services willbe sufficient to meet the basic and specialized needs of children.
With respect to preventive and wellness services, plans sometimes failed to specify theirpolicies regarding routine hearing and vision as part of well-child care and also allergy testing andtreatment, nutritional counseling, diabetic education, and smoking cessation treatment. Consistentwith requirements under the ACA, HHS and states will need to ensure that qualified health plansclearly indicate coverage consistent with Bright Futures.
Oversight of new preventive care cost-sharing prohibitions will be needed, as this studydiscovered a few plans still charging copayments or applying deductibles to well-child care andprenatal care, services for which no cost-sharing is allowed under the ACA.i Importantly also, mentalhealth parity requirements will need to be continuously enforced, as this study found examples ofdifferences in coverage and cost-sharing for both outpatient and inpatient mental health andsubstance abuse treatment services versus general outpatient and inpatient hospital care.
1
Another area of concern pertains to the already high level of deductibles and cost-sharing inthe federal, state, and small group plans studied. Since so many benefits are currently subject todeductibles and also have significant cost-sharing requirements, it will be critical for HHS and statesto carefully consider potential access and medical debt issues as they select their benchmarkoptions and define their cost-sharing features under bronze, silver, gold, and platinum plans. Familieswill need to be fully informed that their choice of plans must take into account not only the premiumamount but also the deductibles, copayments, coinsurance, and maximum benefit amounts. It will becritical that families’ annual out-of-pocket maximum contributions be set at reasonable levels in orderto protect against excessive financial risk. A hospitalization or emergency room visit, for example, willresult in very high costs for families unless their out-of-pocket maximum contribution is set at anaffordable amount. Moreover, many families may not realize until they are at the point of using a givenservice that the deductible must first be met. To the extent feasible, it is important that plans areselected without deductibles applied to primary care services and prescription drugs. Of course, formany low to moderate income families, cost-sharing protections are built into the ACA.ii
The issue of state mandates is another critical area of concern. For many children withspecial health care needs, mandates have been adopted that allow for additional medicallynecessary therapeutic services. However, certain plans – including federal plans, some small groupplans, and Health Maintenance Organizations (HMOs) – are not likely to offer these expandedservices.iii That is, when certain children have therapeutic needs that extend beyond the coveredbenefits or that exceed the families’ financial means, their options will be limited. Take, for example, a16-year-old who is severely injured in a car accident and who requires extended therapies and homecare. Future deliberations regarding the use of Medicaid through spend-downiv or the use ofMedicaid or CHIP as a wrap-around/supplemental option will need to be considered by HHS.Alternatively, HHS may want to consider using a state’s CHIP plan as the benchmark plan forchildren. All of these are important options that would enable families to have more comprehensiveinsurance protection for their children.
Introduction and MethodologyHHS has directed states to select one of several existing health insurance plans to serve as
the “benchmark” plan that defines their EHB package. Under the ACA, the EHB must be covered byall qualified health plans in state health insurance exchanges and all non-grandfathered plans outsideof exchanges as well as by Basic Health Program and Medicaid benchmark andbenchmark-equivalent plans. These benchmark options include 1) one of the three largest smallgroup plans in the state by enrollment, 2) one of the three largest state employee health plans byenrollment, 3) one of the three largest federal employee health plan options by enrollment, and 4)the largest HMO plan offered in the state’s commercial market by enrollment. States are now in theprocess of deciding which of these options to select as their EHB benchmark plan.
2

This report examines how federal, state, and small group insurance plans will likely meet theneeds of children and adolescents, including those with special health care needs. The reportincludes a comparison of coverage and cost-sharing policies available in the three largest federalemployee plans and one of the largest state employee and small group insurance plans in each offive states, effective in 2012. The five states in our study are Alabama, Colorado, Maryland, Texas,and Washington. These states were selected to represent a geographic and population mix. Forcomparison purposes, Medicaid and CHIP plans in these same five states were also examined.
Information for federal employee plans was available online. Information for state employeeand small group plans was obtained from the state insurance commissioner’s office, the state healthinsurance exchange coordinator’s office, the state employee benefit office, or through directcommunication with the insurance carrier. Medicaid and CHIP information was obtained directlyfrom each state’s program office or website. For the most part, standard insurance contracts orcertificates of coverage were reviewed.
A total of 59 services pertinent to children’s health care were examined under the 10 EHBcategories required by HHS to implement the ACA: 1) ambulatory patient services, 2) emergencyservices, 3) hospitalization, 4) maternity and newborn care, 5) mental health and substance usedisorder services, including behavioral health treatment, 6) prescription drugs, 7) rehabilitative andhabilitative services and devices, 8) laboratory services, 9) preventive and wellness services andchronic disease management, and 10) pediatric services, including oral and vision care.v
Plan coverage and cost-sharing policies reported on were for preferred, or in-network,providers. For many services, coverage and cost-sharing policies were not specified, and it is likelythat coverage for these services is not available.
There are several limitations with this study. Most importantly, states will be selecting theirbenchmark health plan using 2013 plan options. Therefore, the plans reviewed in this report are onlyillustrative of the plan policies that states will be reviewing. In addition, several of the benefitexclusions or limitations described in this report will be remedied, at least in part, by states in orderto be consistent with new HHS requirements.vi Further, many of the cost-sharing policies describedin this report will be adjusted to reflect the actuarial value of bronze, silver, gold, and platinumproducts. Another limitation of the study is that the largest commercial HMO products were notanalyzed in the five states. In addition, the scope of each plan’s coverage policies does not take intoaccount prior authorization requirements nor does it take into account the specific types of healthcare organizations and professionals defined by the plan to be preferred. Finally, the pediatricservices described in this report are limited to the dental, vision, and hearing services specified inthe ACA statutory language. The AAP and other child health organizations have advocated for amuch more comprehensive definition of pediatric services — consistent with Medicaid’s EPSDTbenefit definition.
This report is intended for use by federal and state officials as well as by child healthprofessional and advocacy organizations. It is organized into four sections: 1) an executive summary,2) benefits and cost-sharing in federal and state benchmark plans, 3) strengths and weaknesses ofthe 10 EHB categories under federal and state employee and small group options, and 4)comparison of coverage in Medicaid and separate CHIP programs. A set of five tables providesdetailed benefit information on the federal and state employee and small group plans and theseparate CHIP and Medicaid/EPSDT programs.
3

Benefitsand Cost-Sharing inFederal andState BenchmarkPlans
A. Federal Employee Insurance Plans
The three largest federal employee health plan options in 2012 are all Preferred ProviderOrganizations (PPOs): two Blue Cross and Blue Shield Service (BCBS) Benefit Plans (standardand basic options) and the Government Employees Health Association (GEHA) Benefit Plan.Overall, these plans were not substantially different in terms of scope of coverage. Eight of the 10EHB categories were covered with few if any benefit restrictions, as shown in Table 1. Only therehabilitative/habilitative services and devices category and the pediatric oral, vision, and hearingservices category had excluded or limited services. The specific services most often excluded werehabilitative therapy, private duty nursing, residential treatment for mental health and substance abusedisorders, and primary tooth crowns. The services most often limited were physical, occupational,and speech therapies; fillings; tooth extractions; and hearing aids.
With respect to cost-sharing, also shown in Table 1, the differences across the three planswere more apparent. The BCBS Basic Option imposed no family deductible, unlike the other twoplans that each required a $700 annual family deductible. This deductible was typically applied toemergency services, inpatient and outpatient hospital care, rehabilitative therapies, laboratoryservices, and hearing services. The BCBS Standard Option applied the deductible to many moreservices than GEHA. The three federal employee plans used a combination of copayments andcoinsurance requirements. Copayment levels for primary care physicians were between $10 and$25, and for specialists, between $25 and $35. For hospital services, copayments ranged from$150/day up to $750/admission. Coinsurance rates were often set at 15% for several EHBs, withhigher rates for a few specific services, most often brand-name prescription drugs. Maximum dollaramounts were applied to several dental services in all three plans. On a positive note, all threefederal plans offered a similar set of services at no charge, including preventive care for children andimmunizations, prenatal care, nutritional counseling, and smoking cessation treatment.
B. State Employee Health Insurance Plans
Among the largest state employee health benefit plans reviewed in Alabama, Colorado,Maryland, Texas, and Washington, three were BlueCross BlueShield PPO products and two wereHMO products (Kaiser Foundation Health Plan and Group Health Cooperative Plan). Compared tofederal employee insurance options, coverage policies in these state employee plans were not quiteas generous and were also more variable. Seven of the 10 EHBs were covered with few if anyrestrictions. Most often benefit exclusions or limitations were imposed on rehabilitative/habilitativeservices; pediatric oral, vision, and hearing services; and also on mental health and substance abuseservices, as shown in Table 2. Exclusions were often applied to eyeglasses, contacts, andimplantable hearing devices. Services that had visit limits or dollar maximum amounts were physical,occupational, and speech therapies; hearing aids; and home nursing care. The mentalhealth/substance abuse visit limits were found in two of the five state employee plans. Specifically,one plan restricted outpatient treatment for mental disorders to 20 visits per year and for substanceabuse disorders to 40 visits. Another plan limited outpatient mental health treatment to 30 visits peryear, except for individuals with a serious mental disorder defined by state law to include bipolardisorders, depression in childhood and adolescence, obsessive compulsive disorders, paranoidand other psychotic disorders, pervasive developmental disorders, schizo-affective disorders,and schizophrenia.
4

Large state employee benefit plans in four of the five states used a more complicated mix ofdeductibles, copayments, and coinsurance than the federal employee benefit plans. While only twoof the five states imposed a family deductible ($300 and $750, respectively), four out of the fivestate employee plans imposed significant cost-sharing on two services in particular — hospital care(both inpatient and outpatient care) and brand-name drugs. Copayments for ambulatory services,including outpatient mental health and substance abuse services, were typically between $15 and$50 per visit. Copayments for emergency room and hospital services ranged from $150/day to$750/admission. Coinsurance rates were often set at 20% for several EHB categories, but as highas 50% for dental care. State employee plans were less likely to offer services at no charge thanfederal plans. In fact, one plan still charged for well-child exams in 2012. Also, one plan imposedcost-sharing for inpatient behavioral health care at $150/day up to a maximum of $750/day plus20% for the first 15 days and 40% for the next 15 days.
C. Small Group Insurance Plans
Among the largest small group plans reviewed in the five states, two were BCBS PPOplans, one was a UnitedHealth point-of-service plan, and two were HMO plans (BCBS and KaiserFoundation Plan). Coverage under these five plans was less expansive than in the state employeeplans. Still, coverage of ambulatory services, emergency services, inpatient services, maternity andnewborn care, drugs, labs, and preventive care was generous. Gaps in coverage were mostly foundfor rehabilitative/habilitative services and especially for pediatric oral, vision, and hearing services. Ofparticular concern was the large number of services that were not specified and presumably notcovered — far more than in either the state or federal employee health plans. For the most part, asshown in Table 3, services not specified were psychological testing, partial hospitalization for mentalhealth/substance abuse treatment, private duty nursing, genetic testing, preventive and restorativedental care, vision care, and hearing services.
With respect to cost-sharing, a big difference was found between small group plans andstate and federal employee plans with respect to the use of higher family deductibles ranging from$1,000 to $1,500. In three of the small group states, a separate, lower deductible was applied tocertain services — ambulatory services and prescription drugs. Deductibles were applied to arelatively large number of services (between 11 and 22, depending on the plan), including in acouple of instances services that are offered at “no charge,” such as prenatal care and delivery.Copayment rates for primary care physicians ranged from $20-$35, and for specialists, between$20 and $50. Not unlike state employee plans, hospital and emergency room copays were either$100 or $200. The difference in copayments among a Tier 1 generic drug versus a Tier 3non-preferred brand name was four-fold or higher. Coinsurance rates were most often set at 20%.One small group HMO plan covered numerous services at no charge in addition to well-childservices — specifically, ambulatory primary care provider services, outpatient mental health services,generic drugs, and diagnostic labs and imaging.
5

Strengths and Weaknesses of Federal and State Employee and Small GroupInsurance Plans by EHB Category1. Ambulatory Services
Strengths: Primary care provider (PCP) and specialist services were covered in all of the 13federal and state employee and small group plans reviewed.
Weaknesses: In one state employee plan and one small group plan, families must first meeta deductible (of $300 and $350, respectively) before the insurer reimbursed for PCP orspecialist services.
2. Emergency Services
Strengths: Emergency facility and physician services were covered in all of the 13 federal, state,and small group plans reviewed.
Weaknesses: Cost-sharing requirements were consistently used to discourage emergencycare. In two of the federal employee plans, two of the state employee plans, and all of thesmall group plans, first the deductible must be met. In addition to the deductible, all of theplans imposed a copay (ranging from $100 - $200) and/or coinsurance (15%, 20%) foremergency services. One of the plans failed to specify its coverage of ambulance services,and another plan imposed a maximum benefit of $500 for ambulance services.
3. Hospitalization (Inpatient and Outpatient) Services
Strengths: All of the federal and state employee and small group plans covered inpatient andoutpatient hospital services without exclusions or limitations.
Weaknesses: Two of the federal employee plans, one of the state employee plans, and fourof the small group plans required that the deductible be met before hospital services werereimbursed. In addition, plans always imposed an additional copay ($25-$200/day,$200-$250/admission) and/or coinsurance fee (10%-20%). Outpatient hospital serviceshad lower copayments. Several of the plans also charged separately for surgery.
6

4. Maternity and Newborn Care
Strengths: All of the three largest federal employee plans covered prenatal care withoutcharge, and two covered delivery services, as well, without charge. All of the state employeeand small plans also covered prenatal and delivery services.
Weaknesses: Three of the state employee plans and two of the small group plans imposedcost-sharing on prenatal care services. In addition, one of the state employee plans and threeof the small employee plans applied the deductible to prenatal care.
5. Mental Health and Substance Abuse Services, Including BehavioralHealth Treatment
A. Licensed Professional Services, Psychotherapy, and Pharmacotherapy
Strengths: All but two of the federal and state employee plans covered these mentalhealth/substance abuse ambulatory services without any limits, just as they are covered in otherambulatory services. Two small group plans covered each of these services without charge.
Weaknesses: Two state employee plans set visit limits on licensed professional services andpsychotherapy. The first of these plans limited mental health outpatient treatment to 20 visits/yearand substance abuse treatment to 40 visits/year. The second of these plans limited outpatientmental health treatment to 30 visits per year, except for individuals with a serious mental illnessdefined by the state’s law to include bipolar disorders, depression in childhood and adolescence,major depressive disorders, obsessive compulsive disorders, paranoid and other psychoticdisorders, pervasive developmental disorders, schizoaffective disorders, and schizophrenia.
B. Outpatient Hospital and Partial Hospitalization Services
Strengths: All of the federal employee plans offered both outpatient hospital and partialhospitalization services for treatment of mental health and substance abuse disorders. Two ofthe federal plans eliminated the deductible and charged either a copayment ($25) orcoinsurance rate (15%). One small group plan required no charge for these services.
Weaknesses: The same restrictions in the two state employee plans described above underlicensed professional services apply to this benefit as well. In addition, partial hospitalization wasalso limited in one of these two plans to $75/day up to a maximum of $375 plus 20% forthe first 15 days and 40% for the next 15 days. The other state employee plan had a 60-visitlimit on partial hospitalization. Three of the small group plans and one of the state employee plansdid not specify their coverage policy for partial hospitalization.
7
C. Inpatient Hospital and Residential Treatment Services
Strengths: Five of the 13 federal, state, and small group plans covered both inpatient andresidential services for treatment of mental health and substance abuse disorders, and one ofthe plans applied no cost-sharing for residential treatment services.
Weaknesses: Two of the three federal plans did not cover residential treatment services.In addition, two of the state employee plans and four of the small group plans did not specifytheir policy for residential services. In one of the state employee plans, cost-sharing for inpatientmental health and substance abuse treatment was different than for general inpatient hospitalcare. It was $150/day up to a maximum of $750 plan and 20% for the first 15 days and 40%for the next 15 days (same as for outpatient hospital and partial hospitalization). In one of thesmall group plans, inpatient mental health services was limited to 30 days/year, and inpatientphysician services for mental health and substance abuse treatment was subject to thedeductible, unlike physician services in the general inpatient hospital benefit.
D. Psychological Testing and Applied Behavioral Analysis
Strengths: Five of the 13 plans covered psychological testing, and two without charge.Only one plan expressly covered applied behavioral analysis, consistent with its state mandateof coverage up to a maximum of $34,000 for children ages 0-8, and $12,000 for childrenages 9-18.
Weaknesses: The majority of plans reviewed failed to specify their coverage policies forpsychological testing and applied behavioral analysis. Two federal plans expressly excludedcoverage for applied behavioral analysis.
6. Prescription Drugs
Strengths: All 13 plans covered generic (Tier 1), preferred (Tier 2), and non-preferred drugs(Tier 3), most often with no deductible requirement. Copays for generic drugs were between$15-$20, with only one federal plan charging a 20% coinsurance rate.
Weaknesses: Two small group plans applied a separate prescription drug deductible ($100and $500, respectively). The copayment difference between generic and non-preferred brandname drugs was large in all plans — four-fold or higher. The plan with the greatest difference – astate employee plan – charged a $20 copayment for a Tier 1 drug and a 50% coinsurance rateup to a maximum of $250 for a Tier 3 drug.
8
7. Rehabilitative and Habilitative Services and Devices
A. Physical Therapy (PT), Occupational Therapy (OT), and Speech Therapy (ST)
Strengths: Three state employee plans covered PT without defined limits, and one covered OTand ST without limits. In one state employee plan and one small group plan, visit limits did notapply to children ages 0-3 in the state’s early intervention program or to children with autism.Deductibles were not applied to rehabilitative therapies in two federal employee plans, threestate employee plans, and three small plans.
Weaknesses: In the three federal plans, coverage for PT, OT, and ST was limited to 50, 60, or75 visits per therapy or combined. In all but one state employee plan, coverage for PT, OT, andST was also restricted – either 20, 30, 50 or 60 combined visits. Similar restrictions wereimposed in all but one of the small group plans.
B. Habilitative Therapy
Strengths: Two states (in both the state employee and small group plans) covered habilitativetherapy – in one for youth with autism and in another for youth with congenital or genetic birthdefects.
Weaknesses: All three of the federal employee plans excluded habilitative therapy as a coveredbenefit, and one small group plan also excluded this benefit. More often state employee andsmall group plans failed to specify whether habilitative therapy was a covered benefit.
C. Durable Medical Equipment (DME) and Medical Supplies
Strengths: All of the federal employee benchmark plans covered DME and medical supplies.Three of the state employee plans and two of the small group plans covered these benefits.
Weaknesses: The limitation for DME and medical supplies came in the form of a maximumbenefit amount in one state employee plan and one small group plan ($2,000 and $5,000,respectively). Deductibles were required before reimbursement in five of the 13 plansreviewed two federal plans, two small group plans, and one state employee plan.
9

D. Home Nursing Care and Private Duty Nursing
Strengths: Two of the state employee plans and two of the small group plans covered homenursing care without defined limits, and one of each of these plans eliminated cost-sharing for thebenefit. (Home nursing care usually is provided by a physical, occupational, or speech therapistor home health aide.) Three of the state employee plans and one of the small group planscovered private duty nursing. (Private duty nursing is usually provided by a nurse who isdelivering specialized care.)
Weaknesses: All three federal plans excluded private duty nursing coverage, and one of thesmall group plans did as well. In addition, three of the small group plans and two of the stateemployee plans did not specify coverage of private duty nursing. Home nursing care was typicallyrestricted to limits – i.e., to 6 services/month, 25 visits/year, 28 hours/week, or 130 days/year.One of the small group plans limited its home nursing coverage only for enrollees who werehomebound.
8. Laboratory Services
A. Diagnostic Laboratory and X-rays and Imaging
Strengths: All 13 of the federal, state, and small group plans covered diagnostic lab and X-raysand imaging services. Two of the state employee plans and one of the small group plansimposed no charge on lab and X-rays.
Weaknesses: One small plan imposed a separate $350 deductible for imaging services. Inabout half of the 13 plans, the regular deductible applied. Generally, copayments ranged from$25-$100/test, and coinsurance rates were either 10% or 20%.
B. Genetic Testing
Strengths: Two of the 13 plans expressly covered genetic testing – both federal employeeplans. In one of these plans, there was no charge, but the deductible applied.
Weaknesses: Four of the small group plans and three of the state employee plans failed tospecify their coverage policies for genetic testing.
10

9. Preventive and Wellness Services and Chronic Disease Management
A. Routine Physical Exams, Routine Hearing and Screening, and Immunizations
Strengths: All of the 13 plans covered well-child exams and immunizations, and all but twoexpressly mentioned coverage for routine hearing and vision as part of the well-child exam.
Weaknesses: One of the state employee plans imposed a copayment for well-child care, andone small plan applied its deductible to preventive care.
B. Allergy Testing and Injections, Nutritional Counseling, Smoking CessationTreatment, and Diabetic Education
Strengths: All of the state employee plans and most of the other federal employee plans andsmall group plans covered allergy testing and injections.
Weaknesses: One small group plan imposed a $200 maximum benefit and one federal planimposed a $500 maximum benefit on allergy testing and injections. In addition, two small groupplans, one federal employee plan, and one state employee plan imposed the deductible beforereimbursement was provided.
C. Nutritional Counseling
Strengths: Five of the 13 plans expressly covered nutritional counseling services without limits(two federal plans, two state plans, and one small group plan), and three of these plans coveredthis service without any charge.
Weaknesses: Four of the 13 plans – all small group plans — did not specify coverage ofnutritional counseling services. Two of the plans covered nutritional counseling up to a maximumof $150 per lifetime in one plan and $250/year in the other.
11
D. Smoking Cessation Treatment
Strengths: Seven of the 13 plans covered smoking cessation treatment, and five of thesedid so without any charge.
Weaknesses: One state employee plan imposed a 20% coinsurance rate and a $150maximum lifetime benefit for smoking cessation treatment. Five state plans failed to specifytheir coverage policy for this service.
E. Diabetic Education
Strengths: Seven of the 13 plans specifically covered diabetic education, four without charge.
Weaknesses: Five state plans – four small group plans and one state employee plan — didnot specify whether diabetic education was a covered benefit, and two required that thedeductible be met.
10. Pediatric Services, including Oral and Vision Care and Hearing Services
A. Preventive and Diagnostic Oral Care
Strengths:With respect to periodic oral exams, prophylaxis, and fluoride treatment, two of the13 plans covered these services, and one state employee plan covered them at no charge. Withrespect to radiographs, one of the 13 plans – a state employee plan – covered this servicewithout cost-sharing. With respect to sealants, two plans covered them, and again, the samestate plan without cost-sharing.
Weaknesses: Two plans – one state employee and one small group plan – expressly excludedcoverage for all preventive and diagnostic oral health care. More often, small plans failed tospecify coverage for these services. Plans that covered this benefit often imposed limitations,usually in the form of a maximum per service benefit or a per total dental care benefit. Per servicemaximums ranged from $8 to $150 depending on the service and age of the child (younger than13, older than 13), and per year dental maximum benefits were set at $1,500 and included allcovered dental services (excluding in one case, orthodontic expenses).
12

B. Restorative Oral Care
Strengths: Only one plan – the same state employee plan that covered preventive oral healthcare — covered fillings, crowns, and tooth extractions.
Weaknesses: One state employee plan excluded all restorative dental services, and threesmall group plans and one state employee plan failed to specify coverage for these services.Orthodontic care was expressly excluded in six of the 13 plans (in three federal plans, two stateemployee plans, and one small group plan). The limitations that plans imposed – similar topreventive and diagnostic oral care — were maximum amounts per service or per all dentalservices. Another limitation was coverage only for accidental injury (in two plans).
C. Vision Care
Strengths: Ten of the 13 federal, state, and small group plans covered vision exams, onewith no charge, and one plan covered eyeglasses and contacts without charge.
Weaknesses: Six of the 13 plans excluded coverage of eyeglasses, and five excludedcoverage of contacts. In a few plans, a maximum benefit was imposed on eyeglasses andcontacts (i.e., $28.80 for single vision glasses; $150/year for eyeglasses and contacts).
D. Hearing Services
Strengths: Eight of the 13 plans covered hearing exams, four of which had no deductiblerequirements. Three of these plans also covered implanted hearing-related devices and one ofthese plans with no cost-sharing.
Weaknesses: Three plans excluded coverage of hearing exams – two state employee and onesmall group plan. Four of the plans that covered hearing aids applied the deductible first. Oneplan excluded coverage for hearing aids (a small group plan) and 10 imposed limits, usually amaximum benefit — $100, $250, $500, $800, or $1,250/ear. Five of the 13 plans expresslyexcluded coverage of implanted hearing-related devices (four state employee plans and onesmall group plan), and two small group plans failed to specify their coverage policy.
13

Comparison of EHB Coverage in Separate Chip and Medicaid/EPSDT CoverageA. Separate CHIP Programs
For comparison purposes, EHB coverage and cost-sharing policies were examined in theseparate CHIP programs in Alabama, Colorado, Texas, and Washington. Maryland provided itsCHIP enrollees Medicaid coverage. Washington’s separate CHIP program had the same benefitsas its state’s Medicaid program for children, and except for premium requirements, there was noadditional cost-sharing. Thus, for these two states, CHIP coverage and cost-sharing werecomprehensive and free.
In the other three states, with few exceptions, public insurance coverage of the EHBs underseparate CHIP programs was far more generous than in all of the private options, as shown in Table4. With few exceptions, the 10 EHB categories were generously covered. The only service exclusionfound was for private duty nursing (one state) and orthodontics (one state). While several serviceswere not specified, there is a reasonable likelihood that these services were covered if they met thestate’s medical necessity qualifications. Among the services most likely to fall into this category wereapplied behavioral analysis, psychological testing, partial hospitalization and residential treatment formental health or substance abuse treatment, habilitative therapy, genetic testing, nutritionalcounseling, smoking cessation treatment, diabetic education, and implanted hearing-related devices.
Cost-sharing policies in the four separate CHIP programs were either non-existent or verylow, with the exception of one state that applied copays for most ambulatory services at $25 andhospital services at $125. No state imposed a family deductible.
B. Medicaid/EPSDT Programs
Also for comparison purposes, Medicaid’s EPSDT policies were reviewed in the same fivestates. As shown on Table 5, all of the 10 EHB categories were comprehensively covered withoutcost-sharing. There are several services – similar to those listed above – that were not specified inthe state documents reviewed. However, given the EPSDT federal mandate, the presumption is thatmost, if not all, of these services would be covered if deemed by the state to be medicallynecessary.
Acknowledgements. This report has benefitted from the thoughtful review and commentof AAP staff, especially Robert Hall and Ielnaz Kashefipour. Also participating in providinguseful suggestions were Molly Droge, MD, FAAP; Tom Long, MD, FAAP; Renee Turchi, MD,FAAP; Mike McManus, MD, FAAP (no relation to Peggy McManus); Dan Walter, Ian Van Dinther,and Lou Terranova from the AAP; Janice Guerney from Family Voices; Joe Touschner fromGeorgetown University’s Center for Children and Families; Janice Kupiec with the AmericanDental Association; Melissa James with the Children’s Hospital Association; and Meg Comeauwith the Catalyst Center.
14
End Notes
i The ACA requirement to cover recommended preventive services without any cost-sharing requirementsdoes not apply to grandfathered health plans. However, grandfathered plans are required to abide by otherACA requirements, such as prohibiting lifetime limits on coverage for essential health benefits.
ii For individuals with incomes up to 400% of the Federal Povery Level (FPL), for 2014, the out-of-pocket limitwill be equal to the current limit on out of pocket expenses for high deductible plans, $5,950 for self-onlycoverage and $11,900 for family coverage. For 2015 and beyond, the limits will be adjusted based onpremium increases.
iii For further explanation of the state mandates issue, please see: the Centers for Medicare and MedicaidServices (CMS) Frequently Asked Questions on Essential Health Benefits Bulletin, available athttp://ccio.cms.gov/resources/files/Files2/02172012/ehb-faq-508.pdf.
iv Individuals with higher incomes who meet a “spend-down” obligation can qualify for Medicaid coverage.Spend-down is met when, after deducting medical expenses from income, a person’s remaining income isbelow the state’s medically needy income level. See http://www.kff.org/medicaid/8048.cfm.
v Essential Health Benefits: HHS Informational Bulletin. Posted on December 16, 2011 and updated onFebruary 24, 2012. Available atwww.healthcare.gov/news/factsheet/2011/12/essential-health-benefits12162011a.html. Accessed on June14, 2012.
vi The ACA requires all plans in the Exchanges and all non-grandfathered plans outside of the Exchanges tocover without any cost-sharing “recommended preventive services.” For children, these recommendedservices are listed in the Periodicity Schedule of the Bright Futures Recommendations for PediatricPreventive Health Care.(http://brightfutures.aap.org/pdfs/AAP%20Bright%20Futures%20Periodicity%20Sched%20101107.pdf)Even if a state chooses a grandfathered plan as its benchmark plan, this provision of the ACA as well asother Patient’s Bill of Rights provisions, still apply to plans in the Exchanges and non-grandfathered plansoutside of the Exchanges. In other words, these plans must abide by both the EHB requirements as well asthe Patient’s Bill of Rights and other requirements of the ACA. In addition, any scope and durationlimitations in a plan would be subject to review pursuant to ACA prohibitions on discrimination in benefitdesign. See: CMS Frequently Asked Questions on Essential Health Benefits Bulletin,http://ccio.cms.gov/resources/files/Files2/02172012/ehb-faq-508.pdf. Accessed on June 14, 2012.
15

TABLE 1. Coverage and Cost-Sharing for Essential Health Benefits Pertinent toChildren in the Largest Federal Employee Health Plans
16
Essential Health BenefitsBCBS Standard1 BCBS Basic2 GEHA3
Coverage Cost-Sharing Coverage Cost-Sharing Coverage Cost-Sharing
Annual Family Deductible $700 None $700
1. Ambulatory services- PCP
Y $20 Y $25 Y $10
- Specialist Y $30 Y $35 Y $25
2. Emergency services- Physician/facility
Y (D) 15% Y $125 Y (D) 15%
- Ambulance Y $100 Y $100 Y (D) NC
3. Hospitalization Inpatient Services
Y (D)$250/ADM +15%
Y$150/day up to$750/ ADM
Y (D) 15%
- Surgical services Y (D) 15% Y$150/surgeon
Y (D) 15%
Outpatient Services Y (D) 15% Y $75 Y (D) 15%
- Surgical services Y (D) 15% Y $75 Y (D) 15%
4. Maternity and newborn care- Prenatal and postpartum care.
Y NC Y NC Y NC
- Delivery Y NC Y $150 Y NC
- Routine nursery care Y NC Y NC Y NC
5. Mental health and substance abuse services,including behavioral health treatment
- Licensed professional services Y $20/$30 Y $25/$35 Y $10
- Psychotherapy Y $20 Y $25 Y $10
- Pharmacotherapy Y $20 Y $25/$35 Y $10/$25
- Psychological testing Y 15% NS NS Y 15%
- Applied behavioral analysis N N N N NC NC
Outpatient services Y (D) 15% Y $25 Y 15%
- Intensive outpatient services/partialhospitalization
Y (D) 15% Y $25 Y 15%
Inpatient services Y $250/ADM Y$150/day up to$750/ADM
Y 15%
- Residential services N N N N Y 15%
Code: Y = Yes, benefit is covered ADM = AdmissionN = No, benefit is not covered NC = No chargeL = Limited benefit MB = Maximum benefitD = Deductible applies TX = TreatmentNS = Not specified PCP = Primary care provider

17
Essential Health BenefitsBCBS Standard BCBS Basic GEHA
Coverage Cost-Sharing Coverage Cost-Sharing Coverage Cost-Sharing
6. Prescription drugs- Generic drugs (Tier 1)
Y (D) 20% Y $10 Y $5
- Preferred brand-name drugs (Tier 2) Y (D) 30% Y $40 L24 50%
- Non-preferred brand-name drugs (Tier 3) Y (D) 45% Y 50% L24 50%
7. Rehabilitative and habilitativeservices and devices- Physical therapy
L4 $20/$30 L15 $25/$35 L (D)25 15%
- Occupational therapy L4 $20/$30 L15 $25/$35 L (D)25 15%
- Speech therapy L4 $20/$30 L15 $25/$35 L (D)25 15%
- Habilitative therapy N N N N N N
- Durable medical equipment Y (D) 15% Y 30% Y (D) 15%
- Medical supplies Y (D) 15% Y 30% Y (D) 15%
- Home nursing care L5 15% L16 $25 L (D)26 15%
- Private duty nursing N N N N Y N
8. Laboratory services- Diagnostic lab and X-rays
Y (D) 15% Y $25 Y (D) 15%
- Imaging (CT scans/MRIs/PET scans) Y (D) 15% Y $75 Y (D) 15%
- Genetic testing Y (D) 15% Y $75 N N
9. Preventive and wellness services andchronic disease management- Routine physical exams/well-child visit
Y NC Y NC Y NC
- Routine hearing and vision screenings Y NC Y NC Y NC
- Immunizations Y NC Y NC Y NC
- Allergy testing and injections Y (D) 15% Y $25/$35 L27 MB27
- Nutritional counseling Y NC Y NC L28 MB28
- Smoking cessation treatment Y NC Y NC Y NC
- Diabetic education Y (D) 15% Y $25/$35 Y NC
Code: Y = Yes, benefit is covered ADM = AdmissionN = No, benefit is not covered NC = No chargeL = Limited benefit MB = Maximum benefitD = Deductible applies TX = TreatmentNS = Not specified PCP = Primary care provider

18
Code: Y = Yes, benefit is covered ADM = AdmissionN = No, benefit is not covered NC = No chargeL = Limited benefit MB = Maximum benefitD = Deductible applies TX = TreatmentNS = Not specified PCP = Primary care provider
Essential Health BenefitsBCBS Standard BCBS Basic GEHA
Coverage Cost-Sharing Coverage Cost-Sharing Coverage Cost-Sharing
10. Pediatric services, including oral andvision careOral CarePreventive and Diagnostic- Periodic oral examinations
L (D)6 MB6 L17 MB17 Y 50%
- Prophylaxis-child L (D)7 MB7 L18 MB18 Y 50%
- Fluoride treatment L (D)8 MB8 Y NC Y 50%
- Radiographs (two bitewing, panoramic) L (D)9 MB9 L19 MB19 L29 50%
- Sealants (permanent molar) Y (D) NC L20 MB20 NS NS
Restorative- Two surface primary tooth composite filling
L (D)10 MB10 L21 MB21 L30 MB30
- One surface permanent tooth composite filling L (D)10 MB10 L22 MB22 L31 MB31
- Anterior incisor fracture repair L (D)11 MB11 N N Y N
- Primary tooth stainless steel crown N N N N L32 NS32
- Primary tooth extraction L (D)12 MB12 N N L33 MB33
- Bilateral fixed space maintainer Y (D)13 MB13 Y N NS NS
- Orthodontics N N N N N N
Vision Care- Vision examination
Y $20 Y $25/$35 Y $5
- Eyeglasses L (D) 15% Y 30% Y $50
- Contact lenses L (D) 15% Y 30% Y 15%
Hearing services- Hearing examination
Y (D) 15% Y $25/$35 Y (D) 15%
- Hearing aids L (D)14 MB L23 MB23 Y (D)35 MB
- Implanted hearing related device NS NS NS NS Y (D) NS

Table 1 Endnotes
1 The BlueCross and BlueShield Service Standard Option PPO Benefit Plan for 2012 was reviewed.2 The BlueCross and BlueShield Service Basic Option PPO Benefit Plan for 2012 was reviewed.3 The Government Employees Health Associate Standard Option PPO Benefit Plan for 2012 was reviewed.4 In BCBS Standard, PT, OT, ST are limited to 50/year per therapy or combined.5 In BCBS Standard, home nursing care is limited to 2 hours/day up to 25 visits a year.6 In BCBS Standard, the periodic oral evaluation benefit maximum is $12/child < 13 and $8/child > 13.7 In BCBS Standard, the prophylaxis benefit maximum is $22/child < 13 and $14/child > 13.8 In BCBS Standard, the flouride benefit maximum is $22/child < 13 and $8/child > 13.9 In BCBS Standard, the radiograph bitewing maximum is $19/child < 13 and $12/child > 13; the panoramic benefitmaximum is $36/child < 13 and $25/child > 13.
10 In BCBS Standard, the one or two surface filling maximum benefit is $25/child < 13 and $16/child > 13.11 In BCBS Standard, palliative treatment is limited to $24/child < 13 and $15/child > 13.12 In BCBS Standard, the primary tooth extraction maximum benefit is $30/child < 13 and $19/child > 13.13 In BCBS Standard, the space maintainer maximum benefit is $139/child < 13 and $87/child > 13.14 In BCBS Standard, the hearing aid maximum benefit is $1,250 per hearing aid.15 In BCBS Basic, PT, OT, and ST are limited to 75/therapy or combined.16 In BCBS Basic, home nursing care is limited to 2 hours/day up to 25 visits/year.17 In BCBS Basic, the periodic oral evaluation maximum benefit is $25.18 In BCBS Basic, the prophylaxis maximum benefit is $25.19 In BCBS Basic, the bitewing radiograph maximum benefit is $25/year; the panoramic radiograph maximum benefit is$150/year.
20 In BCBS Basic, the sealant maximum benefit is $25.21 In BCBS Basic, the two surface primary tooth filling maximum benefit is $37/child < 13 and $23/child > 13.22 In BCBS Basic, one surface permanent tooth composite filling maximum benefit is $21.23 In BCBS Basic, the hearing aid maximum benefit is $1,250 per hearing aid.24 In GEHA, the brand name prescription drug maximum benefit is $200.25 In GEHA, PT, OT, and ST are limited to 60/year per therapy or combined.26 In GEHA, home health nursing is limited to 2 hours/day up to 25 visits/year.27 In GEHA, the allergy testing and injection maximum benefit is $500.28 In GEHA, the nutritional counseling maximum benefit is $250.29 In GEHA, the radiograph maximum benefit is $150/year.30 In GEHA, the two surface filling maximum benefit is $28.31 In GEHA, the one surface filling maximum benefit is $21.32 In GEHA, crowns are covered only if the result of accidental injury.33 In GEHA, the primary tooth extraction maximum benefit is $21.34 In GEHA, contact lenses are covered only if required to correct an impairment existing after intraocular surgery oraccidental injury.
35 In GEHA, the hearing aid maximum benefit is $250.
19

20
TABLE 2. Coverage and Cost-Sharing for Essential Health Benefits Pertinent toChildren in Large State Employee Health Plans in Five States
Essential Health BenefitsAlabama1 Colorado16 Maryland24
Coverage Cost-Sharing Coverage Cost-Sharing Coverage Cost-Sharing
Annual Family Deductible $300 None None
1. Ambulatory services- PCP
Y$35 MD(D)$20 NP/PA
Y $30 Y $15
- Specialist Y $30 (D) Y $50 Y $30
2. Emergency services- Physician/facility
Y$35 MD(D)$20 NP/PA +$50
Y $100 Y$75/MD$75/facility
- Ambulance Y 20% Y 20% + $500 Y 10%
3. Hospitalization Inpatient Services
Y
$200(D)$25/day fordays 2-5 +20%
Y $750/ADM Y 10%
- Surgical services Y NAC Y NAC Y 10%
Outpatient Services Y $100 Y $30/$50 Y 10%
- Surgical services Y 20% Y $150 Y 10%
4. Maternity and newborn care- Prenatal and postpartum care.
Y$35 MD$20 NP/PA
Y NC Y 10%
- Delivery Y $200(D) Y $750/ADM Y 10%
- Routine nursery care Y+ $25/day fordays 2-5
Y NAC Y 10%
5. Mental health and substance abuse services,including behavioral health treatment
- Licensed professional services L2 $14 Y $30 Y25 $1525
- Psychotherapy L2 $14 Y$30 indiv.$15 group
Y $15
- Pharmacotherapy Y $14 Y $30 Y $15
- Psychological testing NS NS Y NS NS NS
- Applied behavioral analysis NS NS L17 MB17 NS NS
Outpatient services L2 $14 Y $30 Y 10%
- Intensive outpatient services/partialhospitalization
L3 20% Y $30 Y 15%
Inpatient services Y 20% Y $750/ADM Y 10%
- Residential services NS NS Y $750/ADM Y 10%
Code: Y = Yes, benefit is covered NC = No charge SP = SpecialistN = No, benefit is not covered MB = Maximum benefitL = Limited benefit TX = TreatmentD = Deductible applies NP/PA = Nurse practitioner/Physician assistantNS = Not specified PCP = Primary care providerADM = Admission NAC = No added charge

21
Essential Health BenefitsAlabama Colorado Maryland
Coverage Cost-Sharing Coverage Cost-Sharing Coverage Cost-Sharing
6. Prescription drugs- Generic drugs (Tier 1)
Y $10 Y $10 Y $10
- Preferred brand-name drugs (Tier 2) Y 20%iv Y $30 Y $25
- Non-preferred brand-name drugs (Tier 3) Y 20%v Y20% withup to $75
Y $40
7. Rehabilitative and habilitativeservices and devices- Physical therapy
Y 20% (D) L18 $30 L26 $30
- Occupational therapy L6 20% (D) L18 $30 L26 $30
- Speech therapy L7 20% (D) L18, 19 $30 L26 $30
- Habilitative therapy NS NS L20 $30 L26 $30
- Durable medical equipment Y 20% (D) L21 MB21 Y 10%
- Medical supplies Y 20% (D) NS NS Y 10%
- Home nursing care L8 20% (D) L22 NS L27 10%
- Private duty nursing Y 20% (D) NS NS Y 10%
8. Laboratory services- Diagnostic lab and x-rays
YLab - $10Xray - $75
Y NC Y 10%
- Imaging (CT scans/MRIs/PET scans) Y $75 Y $100 Y 10%
- Genetic testing NS NS N N Y NS
9. Preventive and wellness services andchronic disease management- Routine physical exams/well-child visit
Y $35/$20 Y NC Y NC
- Routine hearing and vision screenings NS NS Y NC Y NC
- Immunizations Y NC Y NC Y NC
- Allergy testing and injections Y 20% (D) Y$50 – test$30–injection
Y$15/PCP$30/SP
- Nutritional counseling L9 20% + MB9 N N Y NC
- Smoking cessation treatment L10 20% + MB10 Y NS NS NS
- Diabetic education L11 NC Y NS NS NS
Code: Y = Yes, benefit is covered NC = No charge SP = SpecialistN = No, benefit is not covered MB = Maximum benefitL = Limited benefit TX = TreatmentD = Deductible applies NP/PA = Nurse practitioner/Physician assistantNS = Not specified PCP = Primary care providerADM = Admission NAC = No added charge

22
Essential Health BenefitsAlabama Colorado Maryland
Coverage Cost-Sharing Coverage Cost-Sharing Coverage Cost-Sharing
10. Pediatric services, including oral andvision careOral CarePreventive and Diagnostic- Periodic oral examinations
L12 MBxii NS NS N N
- Prophylaxis-child L12 MB12 NS NS N N
- Fluoride treatment NS NS NS NS N N
- Radiographs (two bitewing, panoramic) L13 MB12 NS NS N N
- Sealants (permanent molar) L12 MB12 NS NS N N
Restorative- Two surface primary tooth composite filling
L12$25 (D)50% MB12
NS NS N N
- One surface permanent tooth composite filling L12 50% MB12 NS NS N N
- Anterior incisor fracture repair L12 50% MB12 NS NS N N
- Primary tooth stainless steel crown L12 50% MB12 NS NS N N
- Primary tooth extraction L12 50% MB12 NS NS N N
- Bilateral fixed space maintainer L12 50% MB12 NS NS N N
- Orthodontics L14 50% MB12 N N N N
Vision Care- Vision examination
Y $40 Y$30-optome-trist $50 optha-mologist
L28$15 PCP$30 SPMB28
- Eyeglasses N N N N L29 MB29
- Contact lenses N N N N L30 MB30
Hearing services- Hearing examination
N N Y $30 Y $15
- Hearing aids L15 MB15 L23 MB23 L31 NC
- Implanted hearing related device N N N N NS NS
Code: Y = Yes, benefit is covered NC = No charge SP = SpecialistN = No, benefit is not covered MB = Maximum benefitL = Limited benefit TX = TreatmentD = Deductible applies NP/PA = Nurse practitioner/Physician assistantNS = Not specified PCP = Primary care providerADM = Admission NAC = No added charge
23
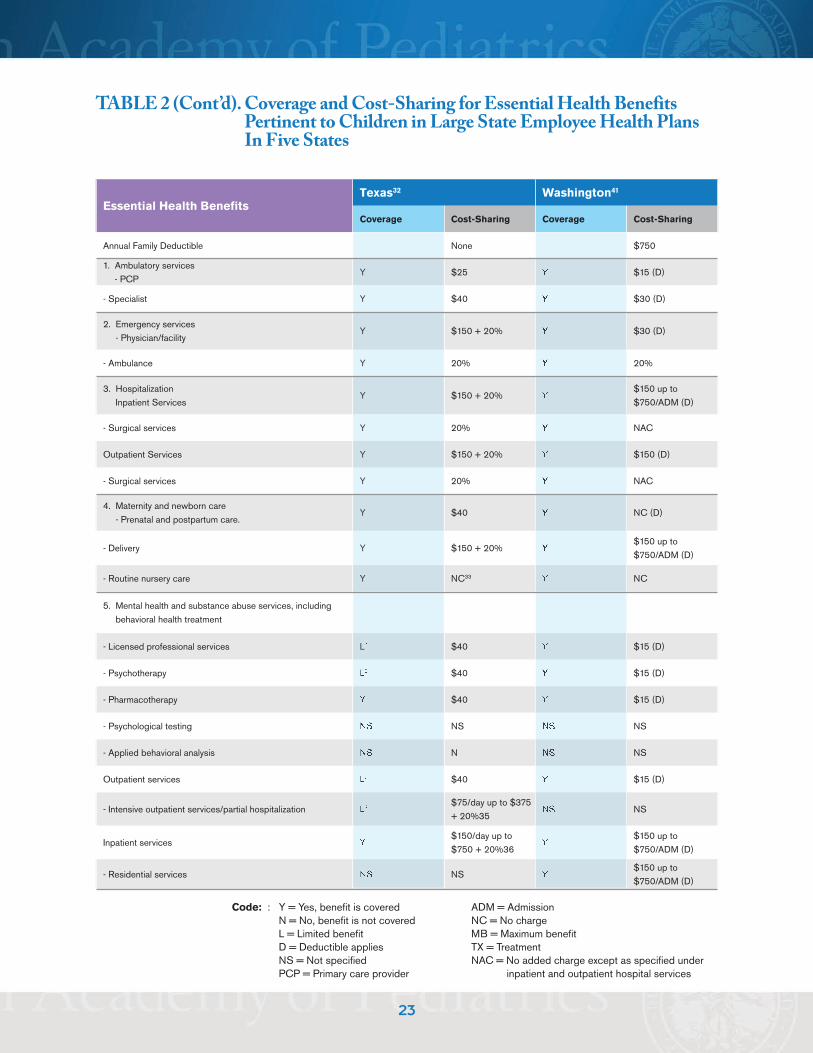
TABLE 2 (Cont’d). Coverage and Cost-Sharing for Essential Health BenefitsPertinent to Children in Large State Employee Health PlansIn Five States
Essential Health BenefitsTexas32 Washington41
Coverage Cost-Sharing Coverage Cost-Sharing
Annual Family Deductible None $750
1. Ambulatory services- PCP
Y $25 Y $15 (D)
- Specialist Y $40 Y $30 (D)
2. Emergency services- Physician/facility
Y $150 + 20% Y $30 (D)
- Ambulance Y 20% Y 20%
3. Hospitalization Inpatient Services
Y $150 + 20% Y$150 up to$750/ADM (D)
- Surgical services Y 20% Y NAC
Outpatient Services Y $150 + 20% Y $150 (D)
- Surgical services Y 20% Y NAC
4. Maternity and newborn care- Prenatal and postpartum care.
Y $40 Y NC (D)
- Delivery Y $150 + 20% Y$150 up to$750/ADM (D)
- Routine nursery care Y NC33 Y NC
5. Mental health and substance abuse services, includingbehavioral health treatment
- Licensed professional services L2 $40 Y $15 (D)
- Psychotherapy L2 $40 Y $15 (D)
- Pharmacotherapy Y $40 Y $15 (D)
- Psychological testing NS NS NS NS
- Applied behavioral analysis NS N NS NS
Outpatient services L2 $40 Y $15 (D)
- Intensive outpatient services/partial hospitalization L3$75/day up to $375+ 20%35
NS NS
Inpatient services Y$150/day up to$750 + 20%36
Y$150 up to$750/ADM (D)
- Residential services NS NS Y$150 up to$750/ADM (D)
Code: : Y = Yes, benefit is covered ADM = AdmissionN = No, benefit is not covered NC = No chargeL = Limited benefit MB = Maximum benefitD = Deductible applies TX = TreatmentNS = Not specified NAC = No added charge except as specified underPCP = Primary care provider inpatient and outpatient hospital services

24
Essential Health BenefitsTexas Washington
Coverage Cost-Sharing Coverage Cost-Sharing
6. Prescription drugs- Generic drugs (Tier 1)
Y$50(D)$15
Y $20
- Preferred brand-name drugs (Tier 2) Y $35 Y $40
- Non-preferred brand-name drugs (Tier 3) Y $60 Y 50% up to $250
7. Rehabilitative and habilitativeservices and devices- Physical therapy
Y 20% L42 $15 (D)
- Occupational therapy Y 20% L42 $15 (D)
- Speech therapy Y 20% L42 $15 (D)
- Habilitative therapy NS NS NS NS
- Durable medical equipment Y 20% L43 20%
- Medical supplies Y 20% L43 20%
- Home nursing care Y 20% Y NC
- Private duty nursing Y 20% NS NS
8. Laboratory services- Diagnostic lab and X-rays
Y 20% Y NC (D)
- Imaging (CT scans/MRIs/PET scans) Y $100 + 20% Y $30 (D)
- Genetic testing NS NS Y N (D)
9. Preventive and wellness services and chronic diseasemanagement- Routine physical exams/well-child visit
Y NC Y NC
- Routine hearing and vision screenings Y NC Y NC
- Immunizations Y NC Y NC
- Allergy testing and injections Y$50/test +$30/injection
Y 20%
- Nutritional counseling Y NC N N
- Smoking cessation treatment NS NS Y NC
- Diabetic education Y NC Y $15 (D)
Code: : Y = Yes, benefit is covered ADM = AdmissionN = No, benefit is not covered NC = No chargeL = Limited benefit MB = Maximum benefitD = Deductible applies TX = TreatmentNS = Not specified NAC = No added charge except as specified underPCP = Primary care provider inpatient and outpatient hospital services

25
Essential Health BenefitsTexas Washington
Coverage Cost-Sharing Coverage Cost-Sharing
10. Pediatric services, including oral andvision careOral CarePreventive and Diagnostic- Periodic oral examinations
L37 MB37 Y NC
- Prophylaxis-child L37 MB37 Y NC
- Fluoride treatment L37 MB37 Y NC
- Radiographs (two bitewing, panoramic) L37 MB37 Y NC
- Sealants (permanent molar) L37 MB37 Y NC
Restorative- Two surface primary tooth composite filling
L37$150 (D)38MB37
Y $10 - $50
- One surface permanent tooth composite filling L37 MB37 Y $10 - $50
- Anterior incisor fracture repair L37 MB37 NS NS
- Primary tooth stainless steel crown L37 MB37 Y $100 - $175
- Primary tooth extraction L37 MB37 Y $10 - $15
- Bilateral fixed space maintainer L37 MB37 NS NS
- Orthodontics L39 50% MB39 L44 MB44
Vision Care- Vision examination
Y $40 Y $15 (D)
- Eyeglasses N N L45 MB45
- Contact lenses N N L45 MB45
Hearing services- Hearing examination
N N Y $15 (D)
- Hearing aids L40 MB40 L45 MB46
- Implanted hearing related device N N N N
Code: : Y = Yes, benefit is covered ADM = AdmissionN = No, benefit is not covered NC = No chargeL = Limited benefit MB = Maximum benefitD = Deductible applies TX = TreatmentNS = Not specified NAC = No added charge except as specified underPCP = Primary care provider inpatient and outpatient hospital services

26
Table 2 Endnotes
1 The Alabama large state employee health insurance plan reviewed was BlueCross BlueShield of Alabama PPO, effectiveJanuary 2012.
2 In AL, outpatient treatment for mental disorders is limited to 20 visits/year; for substance abuse disorders outpatienttreatment is limited to 40 visits/year.
3 In AL, intensive outpatient or partial hospitalization is limited to 60 visits/year.4 In AL, Tier 2 prescription drugs coinsurance is 20% with a minimum copay of $25 and maximum of $40.5 In AL, Tier 3 prescription drug coinsurance is 20% with a minimum copay of $55 and a maximum of $105.6 In AL, occupational therapy is limited to hand therapy procedures and services related to lymphedema.7 In AL, speech therapy is limited to 30 visits/year and no coverage is available for delayed language development orarticulation disorders.
8 In AL, home health services are limited to 6 services (including PT, OT, and ST) each 30 consecutive days. Additionalservices must be authorized.
9 In AL, the nutritional counseling lifetime maximum benefit is $150.10 In AL, smoking cessation treatment lifetime maximum benefit is $150.11 In AL, diabetic education is limited to 6 visits each 30 consecutive days. Additional services must be authorized.12 In AL, covered dental services are provided up to a maximum of $1,500/member/year.13 In AL, panoramic bitewings are limited to one every three years.14 In AL, orthodontic coverage is limited to treatment of handicapping malocclusion that is abnormal and correctable.15 In AL, the hearing aid maximum is $100.16 The Colorado large state employee health plan reviewed was the Kaiser Foundation HMO Plan of Colorado (HMO),effective July 2011 – June 2012.
17 In CO, the applied behavioral analysis maximum benefit is $34,000 for children ages 0-8, and $12,000 for children ages9 – 18.
18 IN CO, OT, PT, and ST is limited to 20 visits/year for children with congenital defects or with abnormalities. For childrenunder three participating in early intervention programs and children with autism, visit limits do not apply.
19 In CO, speech therapy is not covered to improve articulation in the absence of injury, illness, or medication condition.20 In CO, habilitative therapy is only available for children with autism and those in the early intervention program.21 In CO, the durable medical equipment maximum benefit is $5,000/year.22 In CO, the home health services are limited to 28 hours/week. Additional time up to 35 hours/week with priorauthorization.
23 In CO, the hearing aid maximum benefit is $500/ear every three years.24 The Maryland large state employee plan that was reviewed was CareFirst BlueCross BlueShield PPO Plan, effectiveJuly 2012 – June 2013.
25 In MD, behavioral health benefits are provided by APS Healthcare.26 In MD, PT, OT, and ST are subject to 50 visits/year combined, except for children under age 19 with congenital orgenetic birth defects.
27 In MD, home health is limited to 120 days/year.28 In MD, eye exams have a maximum benefit of $45.29 In MD, eyeglasses have a maximum benefit of $28.80 for single vision, double bifocals is $88.20, and trifocals is$70.20. The plan pays up to $45 for frames.
30 In MD, contacts that are medically necessary have a maximum benefit of $201.60. If cosmetic, then $50.40.31 In MD, 1 hearing aid/ear every three years.

Table 2 (Cont’d) Endnotes
32In Texas, the large state employee plan reviewed was BlueCross BlueShield Health Select for plan year 2012.
33In TX, if the newborn hospital stay exceeds the mother’s stay, a separate inpatient copayment will be charged.
34In TX, outpatient mental health treatment is limited to 30 visits/year. Individuals with a serious mental illness, as definedby Texas state law, are not subject to this limit. Serious mental illness is defined as bipolar, depression in childhood,major depressive disorder, obsessive compulsive disorder, paranoid and other psychotic disorders, pervasivedevelopmental delay, schizo-affective disorder, schizophrenia.
35In TX, cost-sharing for intermediate behavioral health care is $75/day up to a maximum of $375 plus 20% for first 15days and 40% for next 15 days.
36In TX, cost-sharing for inpatient behavioral health care is $150/day up to a maximum of $750 plus 20% for first 15 daysand 40% for next 15 days.
37In TX, the dental care maximum benefit is $1,500/year, not including orthodontic care.
38In TX, the $150 deductible for restorative care does not include orthodontic care.
39In TX, the orthodontic maximum benefit is $1,500.
40In TX, the hearing aid maximum benefit is $500/ear every three years.
41The large Washington state employee play reviewed was Group Health Cooperative HMO Classic Plan, 2012. TheDental Care’s plan for 2012 was reviewed.
42In WA, PT, OT, and ST limited to 60 visits for all therapies combined.
43In WA, durable medical equipment and medical supplies are only covered in lieu of hospitalization.
44In WA, the orthodontic maximum benefit is $1,500.
45In WA, the eyeglasses and contact lens maximum benefit is $150.
46In WA, the hearing aid maximum benefit is $800/ear every three years.
27

28
TABLE 3. Coverage and Cost-Sharing for EssentialHealth Benefits Pertinent to Children in LargeSmall Group Plans in Five States
Essential Health BenefitsAlabama1 Colorado8 Maryland15
Coverage Cost-Sharing Coverage Cost-Sharing Coverage Cost-Sharing
Annual Family Deductible $1,050 $1,500 $1,000
1. Ambulatory services- PCP
Y$350 (D)$35
Y $25 Y NC
- Specialist Y $50 Y $45 Y $35
2. Emergency services- Physician/facility
Y$50 – MD$200-facility Y 20% (D) Y
$100
- Ambulance Y 20% (D) L920% (D) +MB9
Y $50 (D)
3. Hospitalization Inpatient Services
Y$200/day fordays 1-5
Y $750/ADM Y$200/ADM(D)
- Surgical services Y NAC Y 20% (D) Y NAC (D)
Outpatient Services Y $200 Y 20% (D) Y $35 (D)
- Surgical services Y NAC Y 20% (D) Y NAC (D)
4. Maternity and newborn care- Prenatal and postpartum care.
Y NC (D) Y NC (D) Y NC
- Delivery Y NC (D) Y 20% (D) Y NC (D)
- Routine nursery care Y NC (D) Y NC (D) Y NC
5. Mental health and substance abuse services,including behavioral health treatment
- Licensed professional services Y NC Y $25 Y NC
- Psychotherapy Y NC Y$25-indiv.$12-group
Y NC
- Pharmacotherapy Y NC Y $25 Y NC
- Psychological testing Y NC NS NS Y NC
- Applied behavioral analysis NS NS NS NS NS NS
Outpatient services L2 50% (D) Y 20% (D) Y NC
- Intensive outpatient services/partialhospitalization
NS NS Y 20% (D) Y NC
Inpatient services L3$200/day fordays 1-54
Y 20% (D) Y $200/ADM (D)
- Residential services NS NS NS NS Y NC
Code: Y = Yes, benefit is covered ADM = Admission SP = SpecialistN = No, benefit is not covered NC = No charge PCP = Primary care providerL = Limited benefit MB = Maximum benefitD = Deductible applies TX = TreatmentNS = Not specified NAC = No additional charge except as specified
under inpatient and outpatient services
29
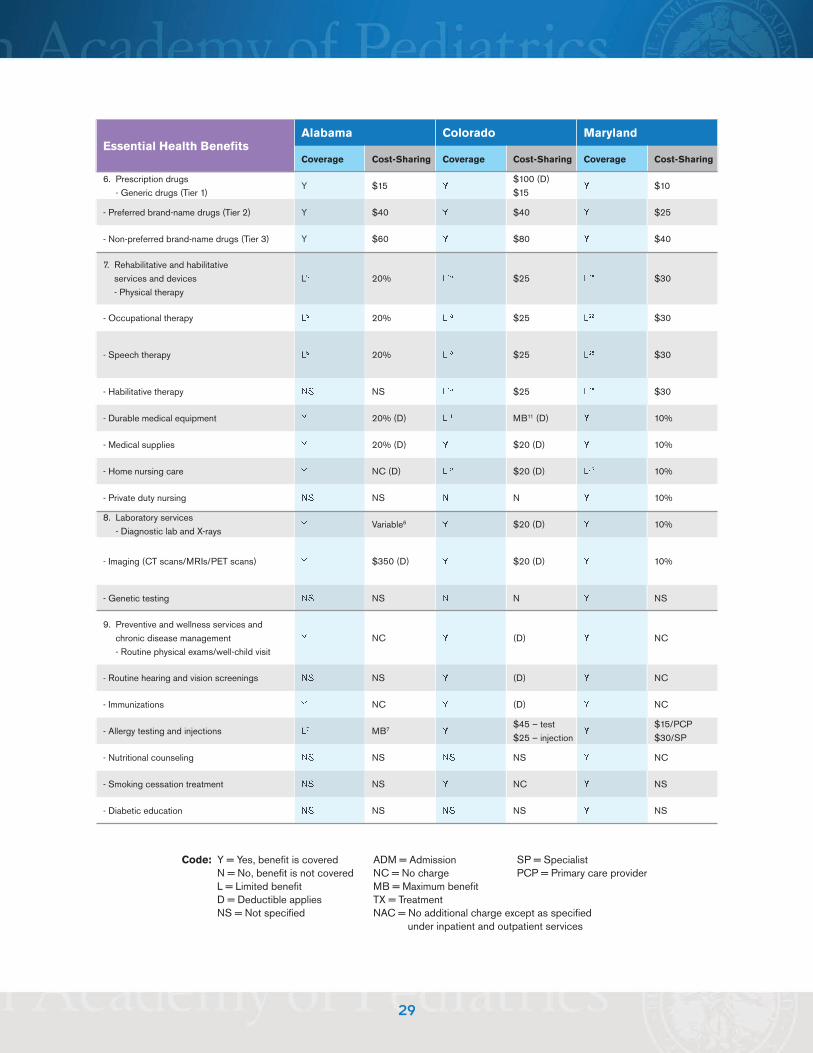
Essential Health BenefitsAlabama Colorado Maryland
Coverage Cost-Sharing Coverage Cost-Sharing Coverage Cost-Sharing
6. Prescription drugs- Generic drugs (Tier 1)
Y $15 Y$100 (D)$15
Y $10
- Preferred brand-name drugs (Tier 2) Y $40 Y $40 Y $25
- Non-preferred brand-name drugs (Tier 3) Y $60 Y $80 Y $40
7. Rehabilitative and habilitativeservices and devices- Physical therapy
L5 20% L10 $25 L26 $30
- Occupational therapy L5 20% L10 $25 L26 $30
- Speech therapy L5 20% L10 $25 L26 $30
- Habilitative therapy NS NS L10 $25 L26 $30
- Durable medical equipment Y 20% (D) L11 MB11 (D) Y 10%
- Medical supplies Y 20% (D) Y $20 (D) Y 10%
- Home nursing care Y NC (D) L12 $20 (D) L27 10%
- Private duty nursing NS NS N N Y 10%
8. Laboratory services- Diagnostic lab and X-rays
Y Variable6 Y $20 (D) Y 10%
- Imaging (CT scans/MRIs/PET scans) Y $350 (D) Y $20 (D) Y 10%
- Genetic testing NS NS N N Y NS
9. Preventive and wellness services andchronic disease management- Routine physical exams/well-child visit
Y NC Y (D) Y NC
- Routine hearing and vision screenings NS NS Y (D) Y NC
- Immunizations Y NC Y (D) Y NC
- Allergy testing and injections L7 MB7 Y$45 – test$25 – injection
Y$15/PCP$30/SP
- Nutritional counseling NS NS NS NS Y NC
- Smoking cessation treatment NS NS Y NC Y NS
- Diabetic education NS NS NS NS Y NS
Code: Y = Yes, benefit is covered ADM = Admission SP = SpecialistN = No, benefit is not covered NC = No charge PCP = Primary care providerL = Limited benefit MB = Maximum benefitD = Deductible applies TX = TreatmentNS = Not specified NAC = No additional charge except as specified
under inpatient and outpatient services

30
Essential Health BenefitsAlabama Colorado Maryland
Coverage Cost-Sharing Coverage Cost-Sharing Coverage Cost-Sharing
10. Pediatric services, including oral andvision careOral CarePreventive and Diagnostic- Periodic oral examinations
NS NS N N NS NS
- Prophylaxis-child NS NS N N NS NS
- Fluoride treatment NS NS N N NS NS
- Radiographs (two bitewing, panoramic) NS NS N N NS NS
- Sealants (permanent molar) NS NS N N NS NS
Restorative- Two surface primary tooth composite filling
NS NS L13 20% NS NS
- One surface permanent tooth composite filling NS NS NS 20% L18 $35
- Anterior incisor fracture repair NS NS NS 20% L18 $35
- Primary tooth stainless steel crown NS NS NS NS L18 $35
- Primary tooth extraction NS NS NS 20% (D) L18 $35
- Bilateral fixed space maintainer NS NS NS N NS NS
- Orthodontics NS NS N N NS NS
Vision Care- Vision examination
NS $NS Y $25/$45 Y $35
- Eyeglasses NS NS N N N N
- Contact lenses NS NS N N N N
Hearing services- Hearing examination
NS NS Y 20% (D) Y $35
- Hearing aids NS NS L23 20% (D) L19 (D)
- Implanted hearing related device NS NS N N Y (D)20
Code: Y = Yes, benefit is covered ADM = Admission SP = SpecialistN = No, benefit is not covered NC = No charge PCP = Primary care providerL = Limited benefit MB = Maximum benefitD = Deductible applies TX = TreatmentNS = Not specified NAC = No additional charge except as specified
under inpatient and outpatient services

31
TABLE 3 (Cont’d). Coverage and Cost-Sharing for EssentialHealth Benefits Pertinent to Children in LargeSmall Group Plans in Five States
Essential Health BenefitsTexas21 Washington23
Coverage Cost-Sharing Coverage Cost-Sharing
Annual Family Deductible $1,500 $1,500
1. Ambulatory services- PCP
Y $25 Y $20
- Specialist Y $25 Y $20
2. Emergency services- Physician/facility
Y $200 + 20% (D) Y$100 + 10% (D)
- Ambulance Y 20% (D) NS NS
3. Hospitalization Inpatient Services
Y 20% (D) Y 10% (D)
- Surgical services Y 20% (D) Y 10% (D)
Outpatient Services Y 20% (D) Y 10% (D)
- Surgical services Y 20% (D) Y 10% (D)
4. Maternity and newborn care- Prenatal and postpartum care.
Y $20 – first visit only Y 10% (D)
- Delivery Y 20% (D) Y 10% (D)
- Routine nursery care Y 20% (D) Y 10% (D)
5. Mental health and substance abuse services, includingbehavioral health treatment
- Licensed professional services Y $20 Y $20
- Psychotherapy Y $20 Y $20
- Pharmacotherapy Y $20 Y $20
- Psychological testing NS NS NS NS
- Applied behavioral analysis NS NS NS NS
Outpatient services Y $20 Y 10% (D)
- Intensive outpatient services/partial hospitalization NS NS NS NS
Inpatient services Y 20% (D) Y 10% (D)
- Residential services NS NS NS NS
Code: Y = Yes, benefit is covered ADM = Admission SP = SpecialistN = No, benefit is not covered NC = No charge PCP = Primary care providerL = Limited benefit MB = Maximum benefitD = Deductible applies TX = TreatmentNS = Not specified NAC = No additional charge except as specified
under inpatient and outpatient services

32
Essential Health BenefitsTexas Washington
Coverage Cost-Sharing Coverage Cost-Sharing
6. Prescription drugs- Generic drugs (Tier 1)
Y $500(D) Y $10
- Preferred brand-name drugs (Tier 2) Y $25 Y $35
- Non-preferred brand-name drugs (Tier 3) Y $50 Y $75
7. Rehabilitative and habilitativeservices and devices- Physical therapy
Y 20% (D) L24 10% (D)
- Occupational therapy NS22 NS22 L24 10% (D)
- Speech therapy NS22 NS22 L24 10% (D)
- Habilitative therapy NS22 NS22 N N
- Durable medical equipment NS NS NS NS
- Medical supplies NS NS NS NS
- Home nursing care NS NS L25 10% (D)
- Private duty nursing NS NS N N
8. Laboratory services- Diagnostic lab and X-rays
Y 20% (D) Y Variable26 (D)
- Imaging (CT scans/MRIs/PET scans) Y 20% (D) Y Variable26 (D)
- Genetic testing NS NS NS NS
9. Preventive and wellness services and chronic diseasemanagement- Routine physical exams/well-child visit
Y NC Y NC
- Routine hearing and vision screenings Y NC Y NC
- Immunizations Y NC Y NC
- Allergy testing and injections Y 20% (D) NS NS
- Nutritional counseling NS NS NS NS
- Smoking cessation treatment NS NS NS NS
- Diabetic education NS NS NS NS
Code: Y = Yes, benefit is covered ADM = Admission SP = SpecialistN = No, benefit is not covered NC = No charge PCP = Primary care providerL = Limited benefit MB = Maximum benefitD = Deductible applies TX = TreatmentNS = Not specified NAC = No additional charge except as specified
under inpatient and outpatient services

33
Essential Health BenefitsTexas Washington
Coverage Cost-Sharing Coverage Cost-Sharing
10. Pediatric services, including oral andvision careOral CarePreventive and Diagnostic- Periodic oral examinations
NS NS NS NS
- Prophylaxis-child NS NS NS NS
- Fluoride treatment NS NS NS NS
- Radiographs (two bitewing, panoramic) NS NS NS NS
- Sealants (permanent molar) NS NS NS NS
Restorative- Two surface primary tooth composite filling
NS NS NS NS
- One surface permanent tooth composite filling NS NS NS NS
- Anterior incisor fracture repair NS NS NS NS
- Primary tooth stainless steel crown NS NS NS NS
- Primary tooth extraction NS NS NS NS
- Bilateral fixed space maintainer NS NS NS NS
- Orthodontics NS NS NS NS
Vision Care- Vision examination
NS NS Y NC
- Eyeglasses NS NS L27 MB27
- Contact lenses NS NS NS NS
Hearing services- Hearing examination
NS NS N N
- Hearing aids NS NS N N
- Implanted hearing related device NS NS N N
Code: Y = Yes, benefit is covered ADM = Admission SP = SpecialistN = No, benefit is not covered NC = No charge PCP = Primary care providerL = Limited benefit MB = Maximum benefitD = Deductible applies TX = TreatmentNS = Not specified NAC = No additional charge except as specified
under inpatient and outpatient services
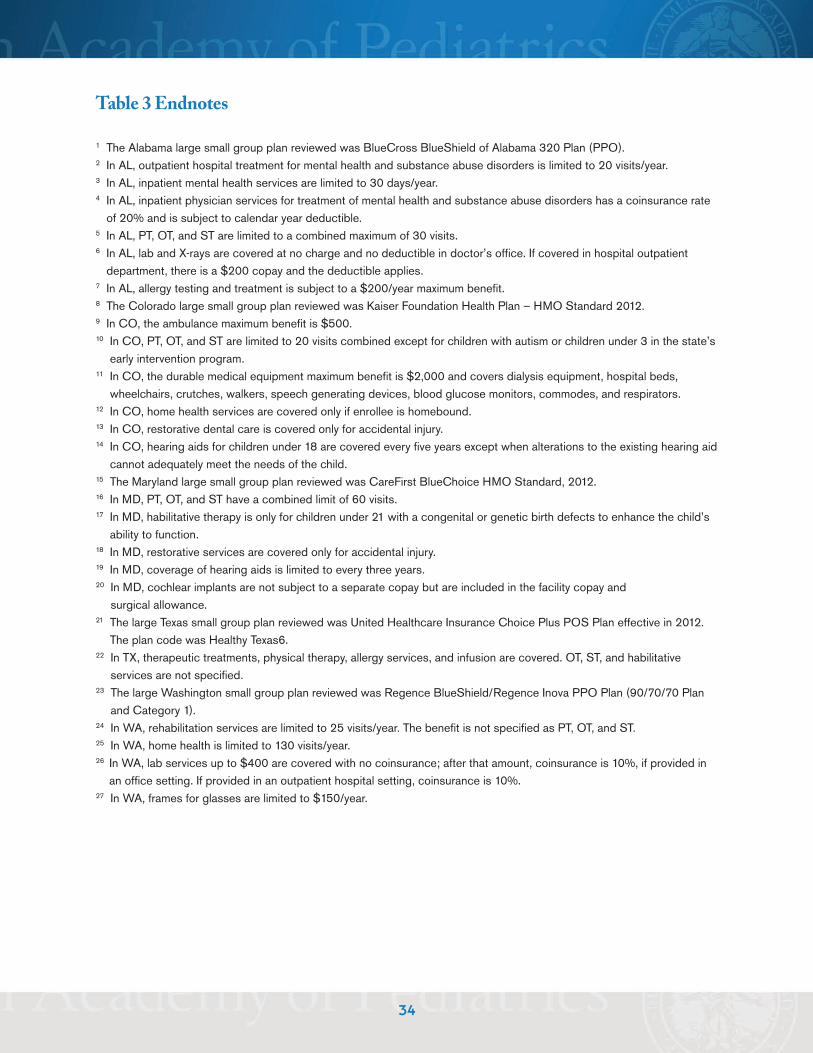
Table 3 Endnotes
1 The Alabama large small group plan reviewed was BlueCross BlueShield of Alabama 320 Plan (PPO).2 In AL, outpatient hospital treatment for mental health and substance abuse disorders is limited to 20 visits/year.3 In AL, inpatient mental health services are limited to 30 days/year.4 In AL, inpatient physician services for treatment of mental health and substance abuse disorders has a coinsurance rateof 20% and is subject to calendar year deductible.
5 In AL, PT, OT, and ST are limited to a combined maximum of 30 visits.6 In AL, lab and X-rays are covered at no charge and no deductible in doctor’s office. If covered in hospital outpatientdepartment, there is a $200 copay and the deductible applies.
7 In AL, allergy testing and treatment is subject to a $200/year maximum benefit.8 The Colorado large small group plan reviewed was Kaiser Foundation Health Plan – HMO Standard 2012.9 In CO, the ambulance maximum benefit is $500.10 In CO, PT, OT, and ST are limited to 20 visits combined except for children with autism or children under 3 in the state’searly intervention program.
11 In CO, the durable medical equipment maximum benefit is $2,000 and covers dialysis equipment, hospital beds,wheelchairs, crutches, walkers, speech generating devices, blood glucose monitors, commodes, and respirators.
12 In CO, home health services are covered only if enrollee is homebound.13 In CO, restorative dental care is covered only for accidental injury.14 In CO, hearing aids for children under 18 are covered every five years except when alterations to the existing hearing aidcannot adequately meet the needs of the child.
15 The Maryland large small group plan reviewed was CareFirst BlueChoice HMO Standard, 2012.16 In MD, PT, OT, and ST have a combined limit of 60 visits.17 In MD, habilitative therapy is only for children under 21 with a congenital or genetic birth defects to enhance the child’sability to function.
18 In MD, restorative services are covered only for accidental injury.19 In MD, coverage of hearing aids is limited to every three years. 20 In MD, cochlear implants are not subject to a separate copay but are included in the facility copay andsurgical allowance.
21 The large Texas small group plan reviewed was United Healthcare Insurance Choice Plus POS Plan effective in 2012.The plan code was Healthy Texas6.
22 In TX, therapeutic treatments, physical therapy, allergy services, and infusion are covered. OT, ST, and habilitativeservices are not specified.
23 The large Washington small group plan reviewed was Regence BlueShield/Regence Inova PPO Plan (90/70/70 Planand Category 1).
24 In WA, rehabilitation services are limited to 25 visits/year. The benefit is not specified as PT, OT, and ST.25 In WA, home health is limited to 130 visits/year.26 In WA, lab services up to $400 are covered with no coinsurance; after that amount, coinsurance is 10%, if provided inan office setting. If provided in an outpatient hospital setting, coinsurance is 10%.
27 In WA, frames for glasses are limited to $150/year.
34

35
TABLE 4. Coverage and Cost-Sharing for Essential Health Benefits in Separate Children’sHealth Insurance Plans in Four States
Essential Health BenefitsAlabama1 Colorado16 Texas10 Washington19
Coverage Cost-Sharing Coverage Cost-Sharing Coverage Cost-Sharing Coverage Cost-Sharing
Annual Family Deductible None None None None
1. Ambulatory services- PCP
Y $5 Y NC Y $25 Y NC
- Specialist Y $5 Y NC9 Y $22 Y NC
2. Emergency services- Physician/facility
Y $15 Y $15 Y NC Y NC
- Ambulance Y $15 NS NS Y NC Y NC
3. Hospitalization Inpatient Services
Y $10/ADM Y NC Y $125/ADM Y NC
- Surgical services Y NC Y NC Y NC Y NC
Outpatient Services Y $10 Y $5 Y $25 Y NC
- Surgical services Y $10 Y $5 Y $25 Y NC
4. Maternity and newborn care- Prenatal and postpartum care.
Y NC Y $5 Y$25/1st visitonly
Y NC
- Delivery Y NC Y $150 Y NC Y NC
- Routine nursery care Y NC Y NC Y NC Y NC
5. Mental health and substanceabuse services, includingbehavioral health treatment
- Licensed professional services Y NC Y $5 Y $25 Y NC
- Psychotherapy Y NC Y $5 Y $25 Y NC
- Pharmacotherapy Y NC Y $5 Y $25 Y NC
- Psychological testing NS NS NS NS Y $25 Y NC
- Applied behavioral analysis NS NS NS NS NS NS NS NS
Outpatient services Y NC Y $5 Y $25 Y NC
- Intensive outpatient services/partialhospitalization
NS NS NS NS Y $25 Y NC
Inpatient services Y $10 Y NC Y $125/ADM L20 NC
- Residential services NS NS Y NC L11 $25 NS NS
Code: Y = Yes, benefit is covered ADM = AdmissionN = No, benefit is not covered NC = No chargeL = Limited benefit MB = Maximum benefitD = Deductible applies TX = TreatmentNS = Not specified PCP = Primary care provider

36
Essential Health BenefitsAlabama Colorado Texas Washington
Coverage Cost-Sharing Coverage Cost-Sharing Coverage Cost-Sharing Coverage Cost-Sharing
6. Prescription drugs- Generic drugs (Tier 1)
Y $2 Y $3 L12 $10 Y NC
- Preferred brand-name drugs (Tier 2) Y $5 Y $5 L13 $35 Y NC
- Non-preferred brand-name drugs (Tier 3) Y $10 Y $5 L13 $35 Y NC
7. Rehabilitative and habilitative servicesand devices- Physical therapy
Y NC Y $5 Y $25 Y NC
- Occupational therapy Y NC NS $5 Y $25 Y NC
- Speech therapy Y NC Y $5 Y $25 Y NC
- Habilitative therapy NS NS Y NS Y $25 Y NC
- Durable medical equipment Y NC Y NC L14 MB14 Y NC
- Medical supplies Y NC Y NC L14 MB14 Y NC
- Home nursing care Lii NC Y $5 Y $25 Y NC
- Private duty nursing NS NS Y N L15 $25 NS NS
8. Laboratory services- Diagnostic lab and X-rays
Y $5 Y NC Y $25/test Y NC
- Imaging (CT scans/MRIs/PET scans) Y $5 Y NC Y $25 Y NC
- Genetic testing NS NS Y Y NS NS Y NC
9. Preventive and wellness services andchronic disease management- Routine physical exams/well-child visit
Y NC Y NC Y NC Y NC
- Routine hearing and vision screenings NS NS NS NC NS NS Y NC
- Immunizations Y NC NS NC Y NC Y NC
- Allergy testing and injections Y$10 Test$5 TX
Y NS Y $25 Y NC
- Nutritional counseling Liii NC NS NS NS NS Y NC
- Smoking cessation treatment NS NS Y NS L16 MB16 NS NS
- Diabetic education NS NS Y NS NS NS NS NS
Code: Y = Yes, benefit is covered ADM = AdmissionN = No, benefit is not covered NC = No chargeL = Limited benefit MB = Maximum benefitD = Deductible applies TX = TreatmentNS = Not specified PCP = Primary care provider

37
Essential Health BenefitsAlabama Colorado Texas Washington
Coverage Cost-Sharing Coverage Cost-Sharing Coverage Cost-Sharing Coverage Cost-Sharing
10. Pediatric services, including oral andvision careOral CarePreventive and Diagnostic- Periodic oral examinations
Y NC Y NC Y NC Y NC
- Prophylaxis-child Y NC Y NC Y NC Y NC
- Fluoride treatment Y NC Y NC Y NC Y NC
- Radiographs (two bitewing, panoramic) Y NC Y NC Y NC Y NC
- Sealants (permanent molar) Y NC Y NC Y NC Y NC
Restorative
- Two surface primary tooth composite filling Y $5 Y NC L17 $25/visit Y NC
- One surface permanent toothcomposite filling
Y $5 Y NC L17 $25 Y NC
- Anterior incisor fracture repair Y $5 Y NC L17 $25 Y NC
- Primary tooth stainless steel crown Y $5 Y NC NS NS Y NS
- Primary tooth extraction Y $5 Y NC L17 $25 Y NC
- Bilateral fixed space maintainer Y NC NS NS NS NS Y NC
- Orthodontics Liv NC N N L17 MB Y NC
Vision Care- Vision examination
Y MB5 Y $5 Y $25 Y NC
- Eyeglasses Lv MB6 Y NC L18 MB18 Y NC
- Contact lenses N N NS NS Y NS NS NS
Hearing services- Hearing examination
Y NC Y $5 Y $25 Y NC
- Hearing aids Lvi MB7 Y NC L14 MB14 Y NC
- Implanted hearing related device NS NS NS NS L14 MB14 NS NS
Code: Y = Yes, benefit is covered ADM = AdmissionN = No, benefit is not covered NC = No chargeL = Limited benefit MB = Maximum benefitD = Deductible applies TX = TreatmentNS = Not specified PCP = Primary care provider

Table 4 Endnotes
1 The Alabama All Kids CHIP Program, effective January 2012, was examined. Eligible children are 0 through 18 withfamily incomes at or below 300% FPL. Cost-sharing policies examined are for eligible children with incomes between151-300% FPL.
2 In AL, home health care is limited to 60 visits/year.3 In AL, medical nutrition therapy for obesity is limited to 2 visits/year.4 In AL, orthodontic coverage is limited to trauma, disease, or dysplasia resulting in significant facial growth impact or jawdeferment, short palate, cleft lip/cleft palate, craniofacial anomalies, and a few selected other conditions.
5 In AL, the routine eye exam maximum benefit is $48 for a new patient and $37 for an established patient. 6 In AL, the eyeglasses maximum benefit is $180 for single vision, $230 for bifocals, and $250 for trifocals.7 In AL, the hearing aid maximum benefit is $750/ear every two years.8 The Colorado Child Health Plan Plus (CHP+) Program template for 2012 was examined. Eligible children are childrenages 0 through 18 with family incomes at or below 250% FPL. Coverage form is benchmark – equivalent. Cost-sharingpolicies reported on are for eligible children between 151-300% FPL.
9 In CO, there is no cost-sharing for evaluation and management codes 99201-99205 and 99211-99215.10 The Texas Children’s Health Insurance Program template for 2012 was examined. Eligible children are children ages 0through 18 with family incomes at or below 200% FPL. Coverage form is secretary-approved coverage. Cost-sharingpolicies examined are for eligible children with incomes above 185% up to 200% FPL.
11 In TX, residential treatment for substance abuse disorders is not covered.12 In TX, contraceptive medications are not covered.13 In TX, brand-name prescription drugs may be limited to a four prescription limit and a 34-day supply limit if determinedto be cost effective.
14 In TX, the durable medical equipment and medical supplies’ maximum benefit is $20,000/year, not including diabeticsupplies and equipment and implantable devices. Hearing aids and surgical implants, glasses and contacts are includedin this DME limit.
15 In TX, the skilled nursing service benefit are only for intermittent use and not intended to provide 24-hour care.16 In TX, approved tobacco cessation programs are covered up to $100 maximum benefit per year.17 In TX, the dental benefit maximum is $564/year. Preventive and emergency dental services are not subject to the dentalbenefit limit. Dental services are covered for relief of significant pain, to eliminate acute infections, to treat traumaticclinical conditions, to attain basic function such as eating and speech, and to prevent a condition from seriouslyjeopardizing health/function or deteriorating in an imminent time frame to a more serious and costly dental problem.
18 In TX, the contracted health plan may reasonably limit the cost of frames/lenses.19 The Washington Apple Health for Kids CHIP Program template for 2012 was reviewed. Eligible children are ages 0through 18 with incomes up to 300% FPL. The coverage form is Secretary-approved coverage – the same asWashington’s Medicaid State Plan.
20 In WA, inpatient treatment for substance abuse detoxification is limited to three days.
38
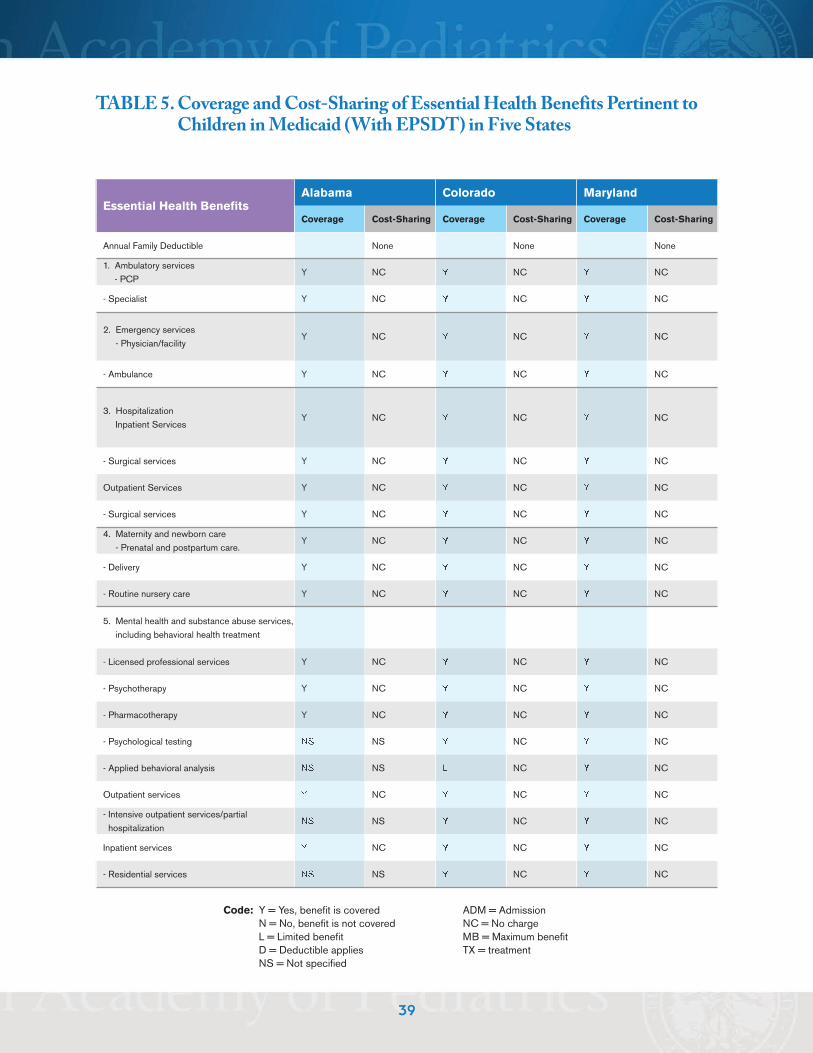
39
TABLE 5. Coverage and Cost-Sharing of Essential Health Benefits Pertinent toChildren in Medicaid (With EPSDT) in Five States
Essential Health BenefitsAlabama Colorado Maryland
Coverage Cost-Sharing Coverage Cost-Sharing Coverage Cost-Sharing
Annual Family Deductible None None None
1. Ambulatory services- PCP
Y NC Y NC Y NC
- Specialist Y NC Y NC Y NC
2. Emergency services- Physician/facility
Y NC Y NC Y NC
- Ambulance Y NC Y NC Y NC
3. Hospitalization Inpatient Services
Y NC Y NC Y NC
- Surgical services Y NC Y NC Y NC
Outpatient Services Y NC Y NC Y NC
- Surgical services Y NC Y NC Y NC
4. Maternity and newborn care- Prenatal and postpartum care.
Y NC Y NC Y NC
- Delivery Y NC Y NC Y NC
- Routine nursery care Y NC Y NC Y NC
5. Mental health and substance abuse services,including behavioral health treatment
- Licensed professional services Y NC Y NC Y NC
- Psychotherapy Y NC Y NC Y NC
- Pharmacotherapy Y NC Y NC Y NC
- Psychological testing NS NS Y NC Y NC
- Applied behavioral analysis NS NS L NC Y NC
Outpatient services Y NC Y NC Y NC
- Intensive outpatient services/partialhospitalization
NS NS Y NC Y NC
Inpatient services Y NC Y NC Y NC
- Residential services NS NS Y NC Y NC
Code: Y = Yes, benefit is covered ADM = AdmissionN = No, benefit is not covered NC = No chargeL = Limited benefit MB = Maximum benefitD = Deductible applies TX = treatmentNS = Not specified
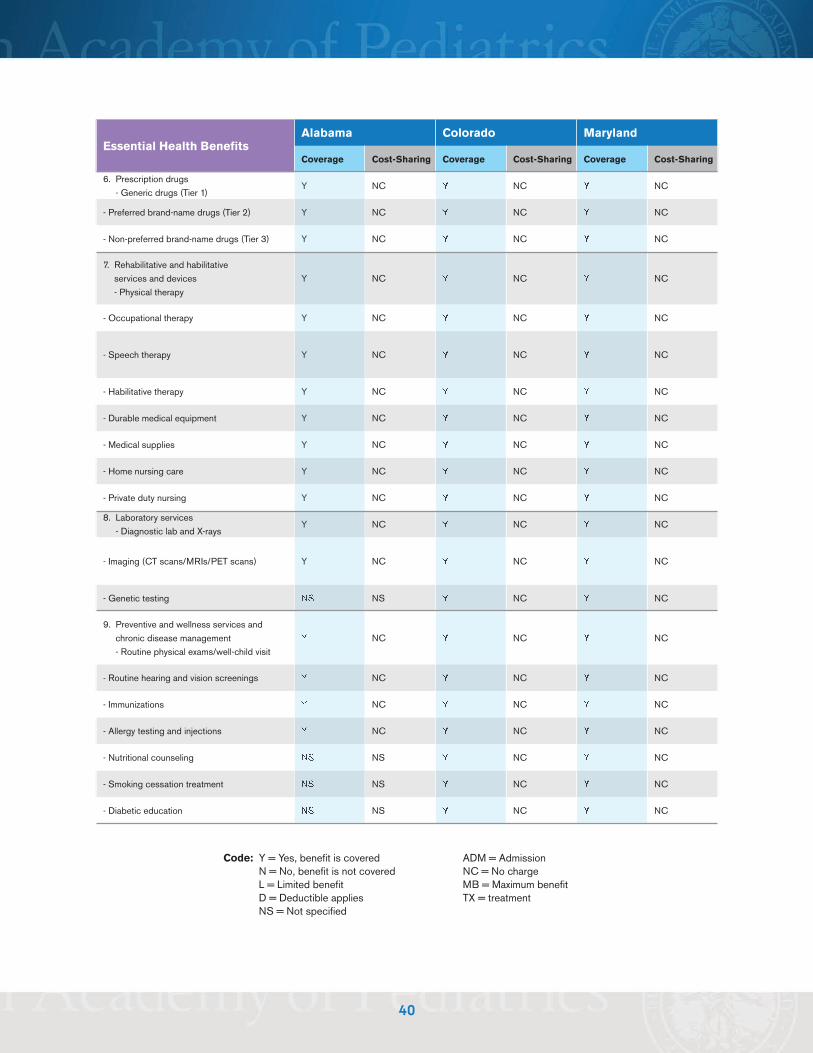
40
Essential Health BenefitsAlabama Colorado Maryland
Coverage Cost-Sharing Coverage Cost-Sharing Coverage Cost-Sharing
6. Prescription drugs- Generic drugs (Tier 1)
Y NC Y NC Y NC
- Preferred brand-name drugs (Tier 2) Y NC Y NC Y NC
- Non-preferred brand-name drugs (Tier 3) Y NC Y NC Y NC
7. Rehabilitative and habilitativeservices and devices- Physical therapy
Y NC Y NC Y NC
- Occupational therapy Y NC Y NC Y NC
- Speech therapy Y NC Y NC Y NC
- Habilitative therapy Y NC Y NC Y NC
- Durable medical equipment Y NC Y NC Y NC
- Medical supplies Y NC Y NC Y NC
- Home nursing care Y NC Y NC Y NC
- Private duty nursing Y NC Y NC Y NC
8. Laboratory services- Diagnostic lab and X-rays
Y NC Y NC Y NC
- Imaging (CT scans/MRIs/PET scans) Y NC Y NC Y NC
- Genetic testing NS NS Y NC Y NC
9. Preventive and wellness services andchronic disease management- Routine physical exams/well-child visit
Y NC Y NC Y NC
- Routine hearing and vision screenings Y NC Y NC Y NC
- Immunizations Y NC Y NC Y NC
- Allergy testing and injections Y NC Y NC Y NC
- Nutritional counseling NS NS Y NC Y NC
- Smoking cessation treatment NS NS Y NC Y NC
- Diabetic education NS NS Y NC Y NC
Code: Y = Yes, benefit is covered ADM = AdmissionN = No, benefit is not covered NC = No chargeL = Limited benefit MB = Maximum benefitD = Deductible applies TX = treatmentNS = Not specified

41
Essential Health BenefitsAlabama Colorado Maryland
Coverage Cost-Sharing Coverage Cost-Sharing Coverage Cost-Sharing
10. Pediatric services, including oral andvision careOral CarePreventive and Diagnostic- Periodic oral examinations
Y NC Y NC Y NC
- Prophylaxis-child Y NC Y NC Y NC
- Fluoride treatment Y NC Y NC Y NC
- Radiographs (two bitewing, panoramic) Y NC Y NC Y NC
- Sealants (permanent molar) Y NC Y NC Y NC
Restorative- Two surface primary tooth composite filling
Y NC Y NC Y NC
- One surface permanent tooth composite filling Y NC Y NC Y NC
- Anterior incisor fracture repair Y NC Y NC Y NC
- Primary tooth stainless steel crown Y NC Y NC Y NC
- Primary tooth extraction Y NC Y NC Y NC
- Bilateral fixed space maintainer NS NS Y NC Y NC
- Orthodontics Y NC Y NC Y NC
Vision Care- Vision examination
Y NC YNC
Y NC
- Eyeglasses Y NC Y NC Y NC
- Contact lenses Y NC Y NC Y NC
Hearing services- Hearing examination
Y NC Y NC Y NC
- Hearing aids Y NC Y NC Y NC
- Implanted hearing related device NS NS Y NC Y NC
Code: Y = Yes, benefit is covered ADM = AdmissionN = No, benefit is not covered NC = No chargeL = Limited benefit MB = Maximum benefitD = Deductible applies TX = treatmentNS = Not specified

42
TABLE 5 (Cont’d). Coverage and Cost-Sharing of EssentialHealth Benefits Pertinent to Children in Medicaid(With EPSDT) in Five States
Essential Health BenefitsTexas32 Washington41
Coverage Cost-Sharing Coverage Cost-Sharing
Annual Family Deductible None None
1. Ambulatory services- PCP
Y NC Y NC
- Specialist Y NC Y NC
2. Emergency services- Physician/facility
Y NC Y NC
- Ambulance Y NC Y NC
3. Hospitalization Inpatient Services
Y NC Y NC
- Surgical services Y NC Y NC
Outpatient Services Y NC Y NC
- Surgical services Y NC Y NC
4. Maternity and newborn care- Prenatal and postpartum care.
Y NC Y NC
- Delivery Y NC Y NC
- Routine nursery care Y NC Y NC
5. Mental health and substance abuse services, includingbehavioral health treatment
- Licensed professional services Y NC Y NC
- Psychotherapy Y NC Y NC
- Pharmacotherapy Y NC Y NC
- Psychological testing NS NC NS NC
- Applied behavioral analysis NS NS N NC
Outpatient services Y NC Y NC
- Intensive outpatient services/partial hospitalization NS NS Y NC
Inpatient services Y NC Y NC
- Residential services NS NC
Code: : Y = Yes, benefit is covered ADM = AdmissionN = No, benefit is not covered NC = No chargeL = Limited benefit MB = Maximum benefitD = Deductible applies TX = TreatmentNS = Not specified
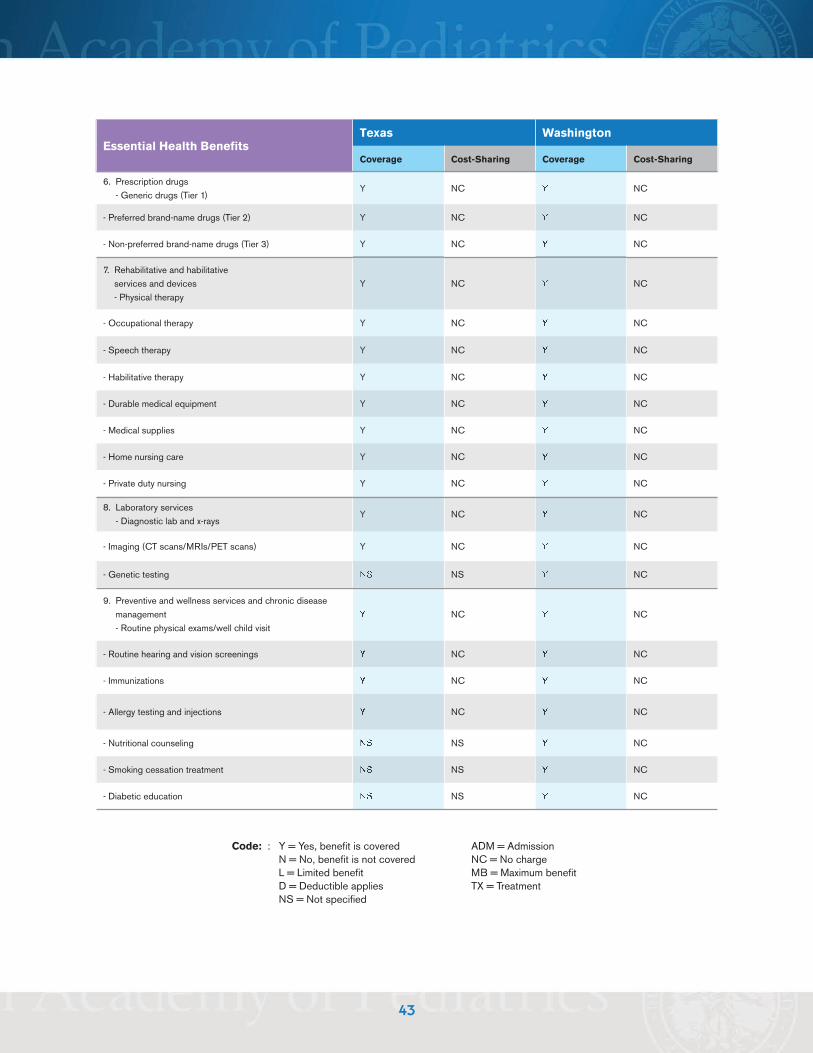
43
Essential Health BenefitsTexas Washington
Coverage Cost-Sharing Coverage Cost-Sharing
6. Prescription drugs- Generic drugs (Tier 1)
Y NC Y NC
- Preferred brand-name drugs (Tier 2) Y NC Y NC
- Non-preferred brand-name drugs (Tier 3) Y NC Y NC
7. Rehabilitative and habilitativeservices and devices- Physical therapy
Y NC Y NC
- Occupational therapy Y NC Y NC
- Speech therapy Y NC Y NC
- Habilitative therapy Y NC Y NC
- Durable medical equipment Y NC Y NC
- Medical supplies Y NC Y NC
- Home nursing care Y NC Y NC
- Private duty nursing Y NC Y NC
8. Laboratory services- Diagnostic lab and x-rays
Y NC Y NC
- Imaging (CT scans/MRIs/PET scans) Y NC Y NC
- Genetic testing NS NS Y NC
9. Preventive and wellness services and chronic diseasemanagement- Routine physical exams/well child visit
Y NC Y NC
- Routine hearing and vision screenings Y NC Y NC
- Immunizations Y NC Y NC
- Allergy testing and injections Y NC Y NC
- Nutritional counseling NS NS Y NC
- Smoking cessation treatment NS NS Y NC
- Diabetic education NS NS Y NC
Code: : Y = Yes, benefit is covered ADM = AdmissionN = No, benefit is not covered NC = No chargeL = Limited benefit MB = Maximum benefitD = Deductible applies TX = TreatmentNS = Not specified
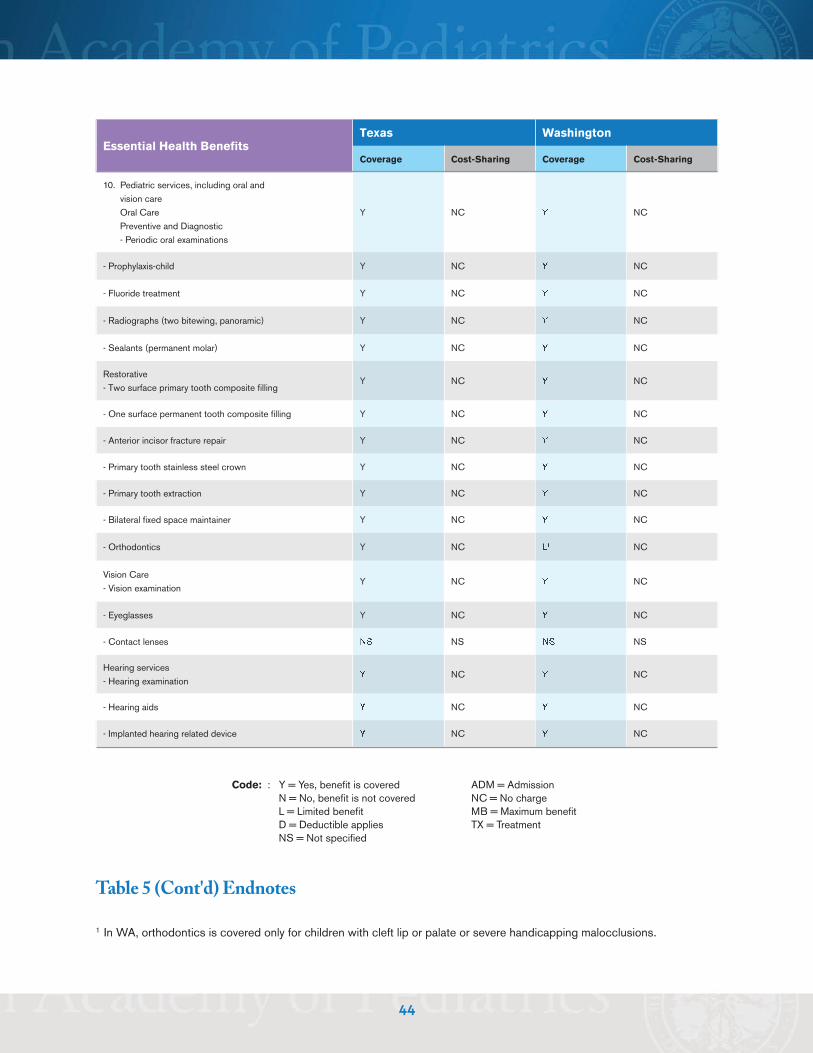
44
Essential Health BenefitsTexas Washington
Coverage Cost-Sharing Coverage Cost-Sharing
10. Pediatric services, including oral andvision careOral CarePreventive and Diagnostic- Periodic oral examinations
Y NC Y NC
- Prophylaxis-child Y NC Y NC
- Fluoride treatment Y NC Y NC
- Radiographs (two bitewing, panoramic) Y NC Y NC
- Sealants (permanent molar) Y NC Y NC
Restorative- Two surface primary tooth composite filling
Y NC Y NC
- One surface permanent tooth composite filling Y NC Y NC
- Anterior incisor fracture repair Y NC Y NC
- Primary tooth stainless steel crown Y NC Y NC
- Primary tooth extraction Y NC Y NC
- Bilateral fixed space maintainer Y NC Y NC
- Orthodontics Y NC L1 NC
Vision Care- Vision examination
Y NC Y NC
- Eyeglasses Y NC Y NC
- Contact lenses NS NS NS NS
Hearing services- Hearing examination
Y NC Y NC
- Hearing aids Y NC Y NC
- Implanted hearing related device Y NC Y NC
Code: : Y = Yes, benefit is covered ADM = AdmissionN = No, benefit is not covered NC = No chargeL = Limited benefit MB = Maximum benefitD = Deductible applies TX = TreatmentNS = Not specified
Table 5 (Cont'd) Endnotes
1 In WA, orthodontics is covered only for children with cleft lip or palate or severe handicapping malocclusions.