a 7-year-old girl with periodic flank discomfort · a 7-year-old girl with periodic flank...
TRANSCRIPT
100 Copyright © SLACK Incorporated
Editor’s note: Each month, this department features a discussion of an unusual diag-nosis. A description and images are presented, followed by the diagnosis and an expla-nation of how the diagnosis was determined. As always, your comments are welcome via email at [email protected].
For diagnosis, see page 101
Case Challenge
A7-year-old girl with a 12-month history of inter-mittent left flank pain was
transferred to our institution from an outside hospital. Severe pain occurred about once per month and was asso-ciated with multiple episodes of non-bloody, nonbilious emesis. The pain did not radiate and was not allevi-ated or exacerbated by anything else. Symptoms lasted 2 to 3 days and then gradually resolved. The patient denied associated dysuria, hematuria, fever, or diarrhea. The patient had visited her pediatrician’s office several times, but diagnostic work-ups for urinary tract infection and constipation were negative. A recent renal ultrasound
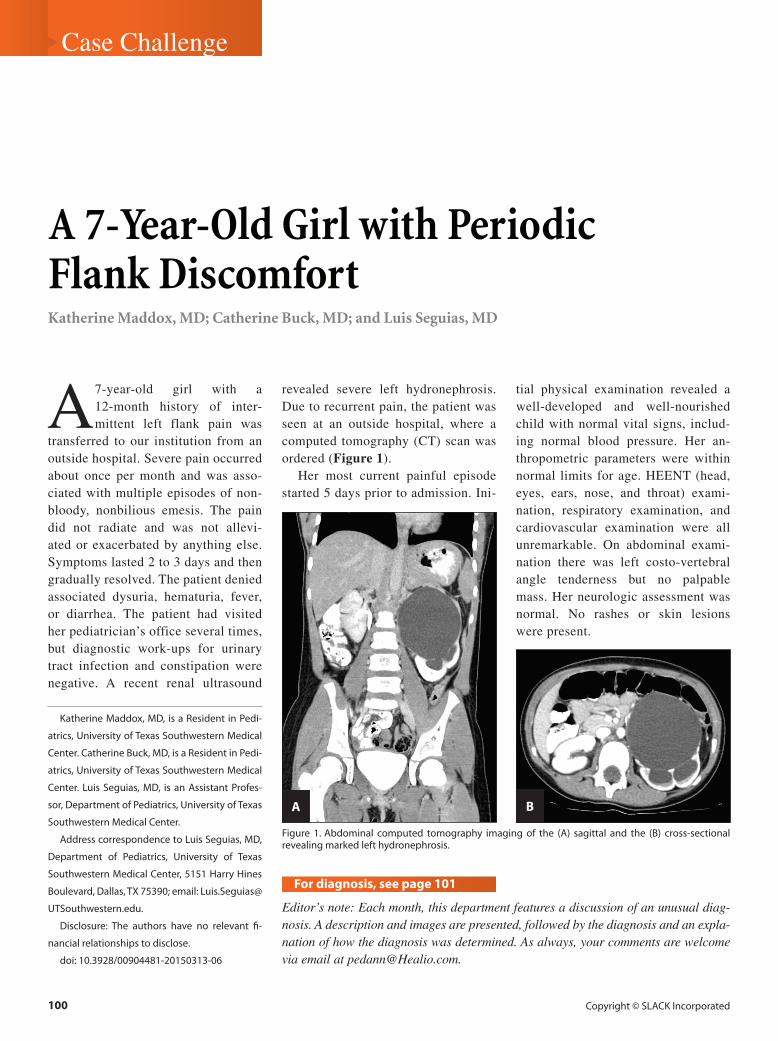
revealed severe left hydronephrosis. Due to recurrent pain, the patient was seen at an outside hospital, where a computed tomography (CT) scan was ordered (Figure 1).
Her most current painful episode started 5 days prior to admission. Ini-
tial physical examination revealed a well-developed and well-nourished child with normal vital signs, includ-ing normal blood pressure. Her an-thropometric parameters were within normal limits for age. HEENT (head, eyes, ears, nose, and throat) exami-nation, respiratory examination, and cardiovascular examination were all unremarkable. On abdominal exami-nation there was left costo-vertebral angle tenderness but no palpable mass. Her neurologic assessment was normal. No rashes or skin lesions were present.
A 7-Year-Old Girl with Periodic Flank DiscomfortKatherine Maddox, MD; Catherine Buck, MD; and Luis Seguias, MD
Katherine Maddox, MD, is a Resident in Pedi-
atrics, University of Texas Southwestern Medical
Center. Catherine Buck, MD, is a Resident in Pedi-
atrics, University of Texas Southwestern Medical
Center. Luis Seguias, MD, is an Assistant Profes-
sor, Department of Pediatrics, University of Texas
Southwestern Medical Center.
Address correspondence to Luis Seguias, MD,
Department of Pediatrics, University of Texas
Southwestern Medical Center, 5151 Harry Hines
Boulevard, Dallas, TX 75390; email: Luis.Seguias@
UTSouthwestern.edu.
Disclosure: The authors have no relevant fi-
nancial relationships to disclose.
doi: 10.3928/00904481-20150313-06
Figure 1. Abdominal computed tomography imaging of the (A) sagittal and the (B) cross-sectional revealing marked left hydronephrosis.
A B

PEDIATRIC ANNALS • Vol. 44, No. 3, 2015 101
Case Challenge
Diagnosis:Uretero-Pelvic Junction Obstruction
Her CT scan showed a marked left hy-dronephrosis, suggesting an uretero-pelvic junction obstruction (UPJO). At that time, referral to a pediatric urologist was made, but the patient’s current episode of pain and subse-quent emergency department visit led to transfer to our institution for a prompt evaluation. In our center, a di-uretic nuclear renography showed evi-dence of delayed excretion (Figure 2), confirming the diagnosis of left UPJO. The patient later had a robotic-assisted
laparoscopic dismembered left pyelo-plasty.
DISCUSSIONUPJO is a partial or total blockage
of urine flow at the level where the re-nal pelvis converges with the ureter. Congenital unilateral UPJO is the most common prenatally acquired urological obstructive disease. Incidence of UPJO is about 1 in 400 live births screened by antenatal ultrasound.1 It occurs more often in boys than in girls, and the left kidney is affected more frequently than the right.2
Classically, urological obstructions are classified as either intrinsic or ex-trinsic in cause. Congenital UPJO typi-cally results from an intrinsic aperistal-
tic segment of the ureter. Currently, no well-defined pathogenesis of this em-bryologic anatomical malformation has been recognized. Although controver-sial, an abnormal distribution of Cajal’s uroepithelial interstitial cells3,4 has been proposed as an underlying mechanism. Altered uroepithelial expression of type 2 helper (Th2) cytokines (interleukin-5 and eotaxin)5 and growth factors (epi-dermal growth factor and transforming growth factor-beta 1) have also been associated with UPJO. Crossing “aber-rant” vessels have been reported as an extrinsic cause of UPJO, but they rep-resent only a minority of documented cases of UPJO.6
Since the routine introduction of prenatal imaging, UPJO is usually
Figure 2. A diuretic radionuclide renograph showing left kidney delay excretion, which suggests uretero-pelvic junction obstruction (red curve). Split renal function showing “fair” left renal uptake (left: 39.2% versus right: 60.8%).

102 Copyright © SLACK Incorporated
Case Challenge
identified before any clinical mani-festation appears. Older children may experience back or flank pain, which may be associated with nausea and vomiting.
This intermittent clinical picture of UPJO, first described by Josef Dietl in 1864,7 is usually self-limited.8 Symp-tom-free periods are variable in dura-tion. Other symptoms might include hematuria and/or hypertension. It can also present in association with a urinary tract infection (eg, fever, dysuria, or in-continence).
Children with UPJO sometimes are misdiagnosed with cyclic vomiting syn-drome.9 It is important to include UPJO in the differential diagnosis of this un-usual entity to decrease renal morbidity.
Presently, the diagnosis of UPJO is generally suspected either by hydrone-phrosis on antenatal ultrasonography or by a flank mass on physical exami-nation during infancy. Diuretic nuclear renography testing is ordinarily used for diagnosis of UPJO because it provides quantitative data concerning differential renal function and urinary flow (Figure 2). Radionuclide delayed excretion mea-surement correlates with the degree of obstruction and is particularly helpful in differentiating UPJO from severe hydro-nephrosis secondary to vesicoureteral reflux. In some cases, CT imaging can further help to characterize the anatomi-cal lesion.
The overall goal in treating UPJO is to preserve renal function. Most experts recommend a restrained interventional approach. There are no randomized tri-als that provide evidence for the optimal management of congenital UPJO. The current management regimen is based on a small number of observational case reports. Common indications for surgical intervention include recurrent flank pain, progressive impairment of ipsilateral renal function, hypertension, history of pyelonephritis, or develop-ment of kidney stones. Bilateral UPJO is a rare cause of neonatal renal insuffi-ciency and it represents a neonatal emer-gency. When urological intervention is indicated, the procedure of choice has historically been dismembered pyelo-plasty. Nevertheless, minimally inva-sive surgery (eg, laparoscopic, balloon dilation, or robotic),10 even in younger children, has recently gained acceptance as an alternative approach. Prognosis is usually quite good. Some investigators have made attempts to identify urinary biomarkers in infants with UPJO to pre-dict the need for surgical intervention in early stages.11
REFERENCES 1. Masson P, De Luca G, Tapia N, et al. Post-
natal investigation and outcome of isolated fetal renal pelvis dilatation. Arch Pediatr. 2009;8:1103-1110.
2. Duong HP, Piepsz A, Collier F, et al. Pre-dicting the clinical outcome of antenatally
detected unilateral pelviureteric junction stenosis. Urology. 2013;82(3):691-696.
3. Solari V, Piotrowska AP, Puri P. Altered ex-pression of interstitial cells of Cajal in con-genital ureteropelvic junction obstruction. J Urol. 2003;170(6 Pt 1):2420-2422.
4. Apoznanski W, Koleda P, Wozniak Z, et al. The distribution of interstitial cells of Cajal in congenital ureteropelvic junction obstruction. Int Urol Nephrol. 2013;45(3):607-612.
5. Chiou YY, Shieh CC, Cheng HL, Tang MJ. Intrinsic expression of Th2 cyto-kines in urothelium of congenital uretero-pelvic junction obstruction. Kidney Int. 2005;67(2):638-646.
6. Lenz K, Thorup JM, Rabol A, Nielsen OH. Prenatal hydronephrosis caused by aberrant renal vessels: a follow-up challenge. Re-ports of two cases. Scand J Urol Nephrol. 1996;30(5):419-421.
7. Flotte T. Dietl syndrome: intermittent ure-teropelvic junction obstruction as a cause of episodic abdominal pain. Pediatrics. 1988;82(5):792-794.
8. Tsai JD, Huang FY, Lin CC, et al. In-termittent hydronephrosis secondary to ureteropelvic junction obstruction: clini-cal and imaging features. Pediatrics. 2006;117(1):139-146.
9. Schulte-Bockholt A, Kugathasan S, Mes-robian HG, Werlin SL. Ureteropelvic junction obstruction: an overlooked cause of cyclic vomiting. Am J Gastroenterol. 2002;97(4):1043-1045.
10. Parente A, Angulo JM, Romero RM, Rivas S, Burgos L, Tardáguila A. Management of ureteropelvic junction obstruction with high-pressure balloon dilatation: long-term outcome in 50 children under 18 months of age. Urology. 2013;82(5):1138-1143.
11. Decramer S, Wittke S, Mischak H, et al. Pre-dicting the clinical outcome of congenital unilateral ureteropelvic junction obstruc-tion in newborn by urinary proteome analy-sis. Nat Med. 2006;12:398-400.
The new and improved INFECTIOUS DISEASES IN CHILDREN Education Lab
at Healio.com has everything you need to
succeed in your fi eld.
Taking CME to the
The all new Healio Education Lab features:
A cleaner, faster user experience
Personal activity recommendations
Slides, video and audio
Trending topics
Expert faculty
Self-assessment opportunities
Mobile-friendly design
The next level of education is waiting for you at Healio.com/Education-Lab
NEW