78: reciprocal causation in relation between jnk and endoplasmic reticulum stress in diabetic...
TRANSCRIPT
STUDY DESIGN: Data were achieved from the Norwegian Mother andChild Cohort on the basis of answers to different questionnaires. Atotal of 83488 deliveries were included in this study. Pre-pregnancyBMI was categorized as underweight (�18.5), normal weight (18.5-24.9), pre-obese (25.0-29.9), mild obese (30.0-34.9), moderate obese(35.0-39.9) and advanced obese (�40). PTD was divided into earlypreterm (22�0 to 31�6 weeks) and late preterm (32�0 to 36�6weeks). Adjusted odds ratios (AORs) were calculated by logistic re-gression analysis adjusting for maternal age, marital status, parity,previous PTD, physical activity, education, smoking and fiber intake.RESULTS: In women who were underweight, normal weight, pre-obese, mild obese, moderate obese and advanced obese the incidenceof PTD was 7.1%, 4.7%, 5.3%, 7.1%, 7.3% and 9.3%, respectively. Byadjusting for the potential cofounders, increasing BMI from pre-obese to the advanced obese group was associated with an increasedrisk for PTD from AOR: 1.12 (95% confidence interval (CI) 1.02-1.22) to AOR: 1.90 (95% CI 1.33-2.74) in the group including allPTDs. This increased risk in the group with only late PTD was fromAOR: 1.13 (95% CI 1.03-1.24) in the pre-obese mothers to AOR: 1.67(95% CI 1.12-2.51) in the advanced obese mothers. Advanced obesemothers had an increased risk for both early and late PTD AOR: 3.39(95% CI 1.65-6.96) and AOR: 1.67 (95% CI 1.12-2.51), respectively.Advanced obese mothers were more likely to have early spontaneousPTD (AOR: 3.39 (95% CI 1.06-10.83)) but no increased risk for latespontaneous PTD could be shown (AOR: 1.45 (95% CI 0.76-2.77)) inthis group.CONCLUSION: Pre-pregnancy maternal overweight seems to increasethe risk for PTD even after adjusting for factors like physical activityand fiber intake as markers for healthy lifestyle. In the overweightmothers the increased risk for PTD is more prominent in late pretermdeliveries than early preterm deliveries.
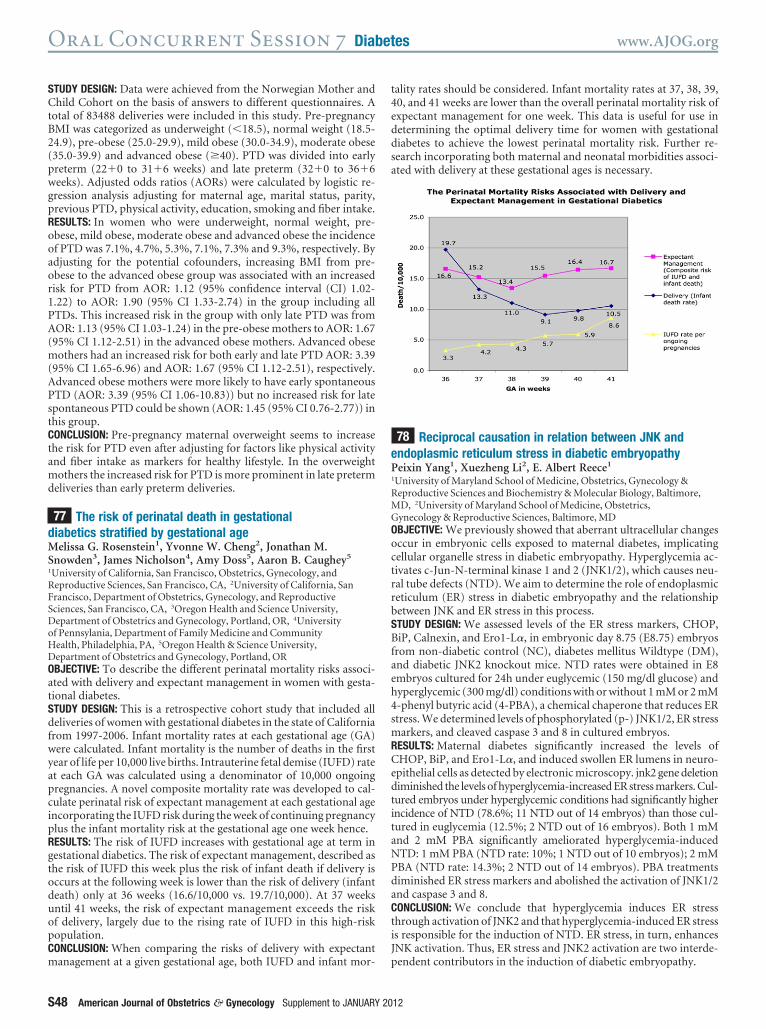
77 The risk of perinatal death in gestationaldiabetics stratified by gestational ageMelissa G. Rosenstein1, Yvonne W. Cheng2, Jonathan M.Snowden3, James Nicholson4, Amy Doss5, Aaron B. Caughey5
1University of California, San Francisco, Obstetrics, Gynecology, andReproductive Sciences, San Francisco, CA, 2University of California, SanFrancisco, Department of Obstetrics, Gynecology, and ReproductiveSciences, San Francisco, CA, 3Oregon Health and Science University,Department of Obstetrics and Gynecology, Portland, OR, 4Universityof Pennsylania, Department of Family Medicine and CommunityHealth, Philadelphia, PA, 5Oregon Health & Science University,Department of Obstetrics and Gynecology, Portland, OROBJECTIVE: To describe the different perinatal mortality risks associ-ated with delivery and expectant management in women with gesta-tional diabetes.STUDY DESIGN: This is a retrospective cohort study that included alldeliveries of women with gestational diabetes in the state of Californiafrom 1997-2006. Infant mortality rates at each gestational age (GA)were calculated. Infant mortality is the number of deaths in the firstyear of life per 10,000 live births. Intrauterine fetal demise (IUFD) rateat each GA was calculated using a denominator of 10,000 ongoingpregnancies. A novel composite mortality rate was developed to cal-culate perinatal risk of expectant management at each gestational ageincorporating the IUFD risk during the week of continuing pregnancyplus the infant mortality risk at the gestational age one week hence.RESULTS: The risk of IUFD increases with gestational age at term ingestational diabetics. The risk of expectant management, described asthe risk of IUFD this week plus the risk of infant death if delivery isoccurs at the following week is lower than the risk of delivery (infantdeath) only at 36 weeks (16.6/10,000 vs. 19.7/10,000). At 37 weeksuntil 41 weeks, the risk of expectant management exceeds the riskof delivery, largely due to the rising rate of IUFD in this high-riskpopulation.CONCLUSION: When comparing the risks of delivery with expectantmanagement at a given gestational age, both IUFD and infant mor-
tality rates should be considered. Infant mortality rates at 37, 38, 39,40, and 41 weeks are lower than the overall perinatal mortality risk ofexpectant management for one week. This data is useful for use indetermining the optimal delivery time for women with gestationaldiabetes to achieve the lowest perinatal mortality risk. Further re-search incorporating both maternal and neonatal morbidities associ-ated with delivery at these gestational ages is necessary.
78 Reciprocal causation in relation between JNK andendoplasmic reticulum stress in diabetic embryopathyPeixin Yang1, Xuezheng Li2, E. Albert Reece1
1University of Maryland School of Medicine, Obstetrics, Gynecology &Reproductive Sciences and Biochemistry & Molecular Biology, Baltimore,MD, 2University of Maryland School of Medicine, Obstetrics,Gynecology & Reproductive Sciences, Baltimore, MDOBJECTIVE: We previously showed that aberrant ultracellular changesoccur in embryonic cells exposed to maternal diabetes, implicatingcellular organelle stress in diabetic embryopathy. Hyperglycemia ac-tivates c-Jun-N-terminal kinase 1 and 2 (JNK1/2), which causes neu-ral tube defects (NTD). We aim to determine the role of endoplasmicreticulum (ER) stress in diabetic embryopathy and the relationshipbetween JNK and ER stress in this process.STUDY DESIGN: We assessed levels of the ER stress markers, CHOP,BiP, Calnexin, and Ero1-L�, in embryonic day 8.75 (E8.75) embryosfrom non-diabetic control (NC), diabetes mellitus Wildtype (DM),and diabetic JNK2 knockout mice. NTD rates were obtained in E8embryos cultured for 24h under euglycemic (150 mg/dl glucose) andhyperglycemic (300 mg/dl) conditions with or without 1 mM or 2 mM4-phenyl butyric acid (4-PBA), a chemical chaperone that reduces ERstress. We determined levels of phosphorylated (p-) JNK1/2, ER stressmarkers, and cleaved caspase 3 and 8 in cultured embryos.RESULTS: Maternal diabetes significantly increased the levels ofCHOP, BiP, and Ero1-L�, and induced swollen ER lumens in neuro-epithelial cells as detected by electronic microscopy. jnk2 gene deletiondiminished the levels of hyperglycemia-increased ER stress markers. Cul-tured embryos under hyperglycemic conditions had significantly higherincidence of NTD (78.6%; 11 NTD out of 14 embryos) than those cul-tured in euglycemia (12.5%; 2 NTD out of 16 embryos). Both 1 mMand 2 mM PBA significantly ameliorated hyperglycemia-inducedNTD: 1 mM PBA (NTD rate: 10%; 1 NTD out of 10 embryos); 2 mMPBA (NTD rate: 14.3%; 2 NTD out of 14 embryos). PBA treatmentsdiminished ER stress markers and abolished the activation of JNK1/2and caspase 3 and 8.CONCLUSION: We conclude that hyperglycemia induces ER stressthrough activation of JNK2 and that hyperglycemia-induced ER stressis responsible for the induction of NTD. ER stress, in turn, enhancesJNK activation. Thus, ER stress and JNK2 activation are two interde-pendent contributors in the induction of diabetic embryopathy.
Oral Concurrent Session 7 Diabetes www.AJOG.org
S48 American Journal of Obstetrics & Gynecology Supplement to JANUARY 2012