6.3 distal femoral physeal fractures
TRANSCRIPT

Distal femoral physealfractures
Prof. Dr. Thomas WirthDepartment of Orthopaedics
Olgahospital
Contents• frequency, mechanism of injury, fracture
pattern
• diagnostics
• treatment options
• complications
• management of complications
distal femoral physeal fractures
• account for 6 – 9% of physeal injuries• ~ 1% of children‘s fractures
• Causes– sports injuries ~49%– hit by a car ~25%– falls ~12%– car accident ~ 5%– other ~ 9%

Mechanism of injuryThe Growth plate generally is less resistant to bendingstresses in an immature skeleton. Ligamentous injuriesare less frequent than physeal fractures in children.
Varus or valgusdistraction forces
Hyperextensionforces
Compression forces
distal femoral physeal fractures

Fracturepattern,
classification
Salter III
Salter V(physealcompression)
Salter I
Salter IV
Salter II
distal femoral physeal fractures

distal femoral physeal fractures
classification according to direction of displacement
Displacement according to effective stresses:
anterior: anterolateral: anteromedial: poste-rior:
very rare
higher risk of associated vascular injury

• clinical signs:– inability to bear weight, axial deformity,
swelling, pain– skin damage, open fractures
• imaging:– conventional radiography– oblique radiographs in unclear cases– MRI-scans (Salter I and III)
• search for accompanying injuries
distal femoral physeal fracturesdiagnostics
• ligamentous damage– ACL– collateral ligaments– often diagnosed only after fracture healing
• vascular injury– popliteal artery
• nerve injury– peroneal nerve
distal femoral physeal fractures
associated injuries

treatment principles• risks:
– serious damage to the physis: 18 – 51% angular deformity; 36 – 68% shortening
– Loss of correction after reduction in 43 – 70% without internal fixation
– others (vascular or neural injury, compartment syndrome)
• treatment:– above knee plaster only for undisplaced and stable
fractures– closed or open reduction and internal fixation for any
displaced or unstable fracture
distal femoral physeal fractures

distal femoral physeal fractures
be aware of insufficient and incomplete closed reduction:
From: Rockwood & Wilkins: Fracturesin children 6th Ed. LWW, Philadelphia
The periosteum disrupts on theside of physeal fracture in Salter-Harris type II – fractures.
During reduction the periosteummay interpose within the fractureand prevent complete and anatomic reduction.
This may also favour loss of position with recurrence of deformity.

treatment principles
distal femoral physeal fractures
If possible, avoid implants which arecrossing the physis
From: Rockwood & Wilkins: Fracturesin children 6th Ed. LWW, Philadelphia
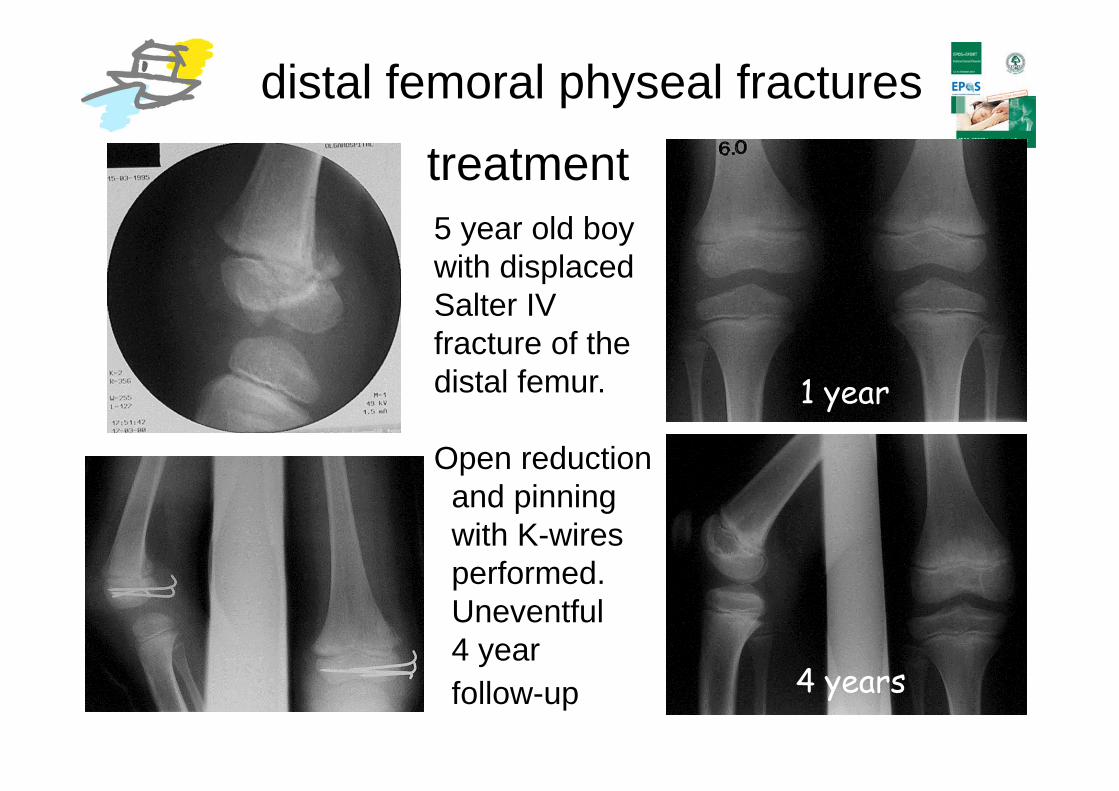
treatment5 year old boywith displacedSalter IVfracture of thedistal femur.
Open reductionand pinning with K-wires performed.Uneventful4 yearfollow-up
1 year
4 years
distal femoral physeal fractures

treatment
12 year old girl, Salter I fracture leftdistal femur (+ shaft fractures rightfemur and right tibia).Anatomic reduction achieved, K-wirestabilisation. Genu valgum, shortening
distal femoral physeal fractures

treatmentSalter II fracture of the distalfemur. Anatomic Reductionand K-wire fixation. In the following years a significant shortening of theleft femur developed, whichrequired leg lengthening.
distal femoral physeal fractures

treatment
Mildly displacedSalter II fractureof the right distal femur. Closed reduction and fixation of the metaphyseal fragment with a compression screw. The leg subsequently went into valgus with some shortening. Additionaltreatment was necessary.
distal femoral physeal fractures

• Physeal injury is very common.
• progressive angulation (and shortening)– 18 – 51 % (Czitrom et al [1981], Robert et al [1988], Thomson et al [1995],
Eid et al [2002])
• progressive leg-length discrepancy– 36 – 68% (Czitrom et al [1981], Robert et al [1988], Thomson et al [1995],
Eid et al [2002])
Physeal fractures aroundthe knee: growth disturbance

Physeal fractures aroundthe knee: growth disturbance
The degree of displacement of the fragments does most likelydefine the amount of growth disturbance to be expected.Lombardo et Harvey (1977), Thomson et al (1995)

Physeal fractures aroundthe knee: growth disturbance
treatment optionsShortening andgenu valgumafter physeal fracture of thedistal femur.Bone bridge resection and fatinterpositioning(Langenskjöldprocedure) as primary treatment to avoid further deformity.
Physeal fractures aroundthe knee: growth disturbance
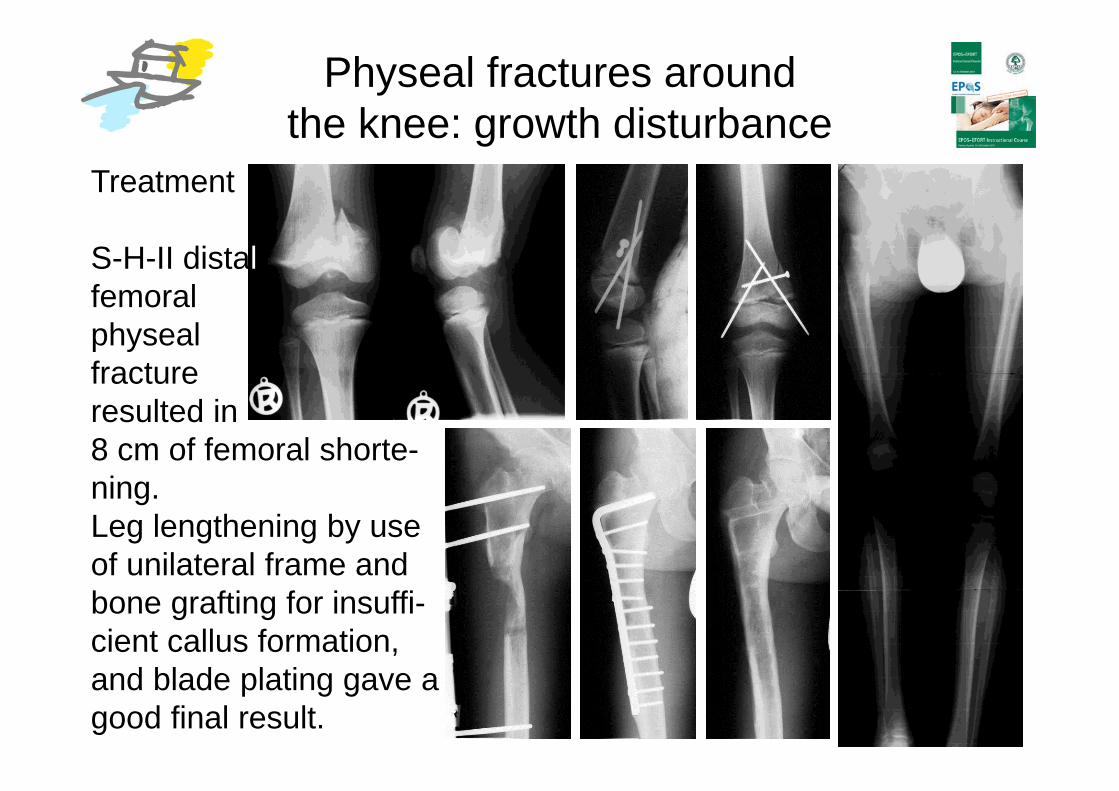
Treatment
S-H-II distalfemoralphyseal fractureresulted in8 cm of femoral shorte-ning. Leg lengthening by useof unilateral frame andbone grafting for insuffi-cient callus formation,and blade plating gave agood final result.

Physeal fractures aroundthe knee: growth disturbance
12 years old boy with adistal femoralphyseal fracturewith subsequentgenu valgum.Treated by bonebridge resectionand temporary epiphyseodesis

Summary
• Physeal fractures of the distal femur are uncommon but severe injuries.
• Closed reduction is rarely the best treatment option.
• Open and anatomical reduction with stable internal fixation is the method of choice.
• High rate of growth disturbances and the need for secondary intervention