6 exposure to shs among workers in the restaurants in vientiane capital and luang prabang provinc
DESCRIPTION
liteTRANSCRIPT

Dr. Keonakhone Houamboun, NIOPH, MOH
Dr. Sengchanh Kounnavong, NIOPH, MOH
The Collaborative Funding Program for Southeast Asia Tobacco Control Research
Exposure to SHS among Workers in the Restaurants
in Vientiane Capital and Luang Prabang Province
Financial support from
The Rockefeller Foundation and Thai Health Promotion Foundation

Exposure to SHS among Workers in the Restaurants in Vientiane Capital
and Luang Prabang Province
by Dr. Keonakhone Houamboun, NIOPH, MOH
Dr. Sengchanh Kounnavong, NIOPH, MOH
Editors Foong Kin, PhD
Menchi G. Velasco
Supported by
Southeast Asia Tobacco Control Alliance (SEATCA) Under The Collaborative Funding Program for Tobacco Control Research
Financial support from
The Rockefeller Foundation and Thai Health Foundation (ThaiHealth)
June 2009

2
TABLE OF CONTENTS
ACKNOWLEDGEMENTS...........................................................................................4 INTRODUCTION .........................................................................................................7 LITERATURE REVIEW ..............................................................................................9 STUDY OBJECTIVES................................................................................................17
3.1 Overall Objective ...............................................................................................17
3.2 Specific Objectives ............................................................................................17
METHODS & DATA SOURCES...............................................................................18
4.1 Research Design.................................................................................................18
4.2 Sampling Frame .................................................................................................18
4.4 Sample Size........................................................................................................19
4.5 Respiratory symptoms in the last two months ...................................................20
4.6 Data Collection Methods ...................................................................................20
4.7 Pre-testing of the Questionnaire.........................................................................21
4.8 Data Collection and its Quality Control.............................................................21
4.9 Data Processing and Analysis............................................................................22
4.10 Ethical Consideration.......................................................................................22
RESULTS ....................................................................................................................23
5.1 General Characteristics of Respondents in Both Groups...................................23
5.2 The Association between Work Site and the Risk of Developing Respiratory
Symptoms ................................................................................................................27
5.3 Estimation of the Direct and Indirect Costs of Smoking-related Diseases Among
the Workers Who Are Exposed to SHS in the Restaurants .....................................29
DISCUSSION..............................................................................................................33 CONCLUSION AND RECOMMENDATIONS ........................................................35 REFERENCES ............................................................................................................36 ANNEXES...................................................................................................................40
A. Screening Form..................................................................................................40
B. Data Collection Tool ..........................................................................................41

3
LIST OF TABLES Table 1: Background characteristics of respondents, restaurant workers and
officers by province 23
Table 2: Percent distribution of respondents on policy knowledge by province
24
Table 3: Frequency distribution of respondents by occupation with past working experience
25
Table 4: Frequency distribution of respondents exposed to secondhand smoke by places and province
26
Table 5: Mean and Standard deviation of hours that respondents are exposed to smoking pollution
26
Table 6: Frequency distribution of people who are smokers that the respondents had contact with
27
Table 7: Frequency distribution of respondents in the worksites and respiratory symptoms
28
Table 8: Frequency distribution of respondents in worksites and respiratory symptoms by province
28
Table 9: Frequency distribution of respondents who are exposed to passive smoking by living with smokers at home and respiratory symptoms
29
Table 10: Frequency distribution of respondents who reported having respiratory symptoms by places of smoking exposure
29
Table 11: Frequency distribution of respondents who reported seeking care by services
30
Table 12: Health care cost by province 31
Table 13: Respiratory symptoms and health care cost by exposed and non-exposed restaurants workers and officers
31
Table 14: Respiratory symptoms and health care cost by exposed and non-exposed restaurants workers and officers in two provinces
32

4
ACKNOWLEDGEMENTS
This study received technical support from the Southeast Asia Tobacco Control Alliance (SEATCA) under The Collaborative Funding Program for Tobacco Control Research and financial support from The Rockefeller Foundation and the Thai Health Promotion Foundation (ThaiHealth).
The research team would like to thank Adventist Development and Relief Agency (ADRA Lao) for their coordination and support. This research could not be completed without the support and encouragement of Prof. Dr. Sithath Insisiengmay, all data collectors and respondents from Vientiane and Luang Prabang provinces.

5
EXECUTIVE SUMMARY The study on exposure to secondhand smoke (SHS) among non-smoking workers in the restaurants in comparison to non-smoking officers in the smoke-free offices in Vientiane capital city (VTE) and Luang Prabang Province (LPB), Lao PDR aimed to provide research-based evidences to policy-makers that would support the drive to enforce tobacco control policy under the Lao PDR Act of 2001, particularly Article 4 which is the implementation of smoke-free policy in places including restaurants. This cross-sectional study was carried out from September to October 2007 using the structured interview questionnaires to collect data on SHS exposure, health symptoms, and cost of treatment related to health symptoms from 300 cases of workers who are exposed to SHS in the restaurants and 300 staff in smoke-free offices. The collected data was entered into Epi-info 6.04 dataset and analyzed using cross-tabulation and logistic regression by SPSS statistical packages version 11.5. The respondents were mostly females in the young age group (15-35 years old), had completed secondary and higher education, and most of them were single. The study found that most of the workers at the restaurants had been exposed to secondhand smoke on average 11.6 hours per week in comparison to those who worked in the office where smoking is prohibited [1.63 hours (p<0.001)]. Higher rates of exposure to smoke at the work place were observed among the restaurant workers (99.3% in VTE and 60.7% in LPB) compared to the office workers (7.3% in VTE and 38.0% in LPB) (p<0.001). The mean number of hours that restaurant workers in Vientiane capital city were exposed to smoking pollution was higher than those in Luang Prabang province which has smoke-free areas (20 versus 2.48 hours). The study showed the strong association between exposure to secondhand smoke and respiratory symptoms including chest pain and coughing with phlegm in the morning (10.7%); 15.0% in the restaurant group and 6.3% in office group (OR=2.6, p=0.001) experienced such symptoms. In addition, among those respondents who were living with smokers, 11.7% reported having respiratory symptoms compared to 4.5% among those who were not living with smokers (p=0.041). The mean of total health expenditure spent on treating their illness was 319,612 Kips1 (US$37.3), in which 284,620 Kips (US$33.2) were direct cost and 66,160 Kips (US$7.7) were indirect cost. The exposed restaurant workers spent more (513,250 Kips or US$59.9) than the exposed office workers (197,315 Kips or US$23).
1 1 US Dollar is equivalent to 8,568 LAO KIPS as of August 2008

6
The data derived from this study confirmed that public places such as restaurants are among the worksites that have high level of secondhand smoke, but these workplaces are least likely to be covered by laws or policies on smoking ban; therefore, this study provides strong evidence to support a complete ban on smoking in restaurants, pubs, bars, and other public places as mentioned in Article 4 of the tobacco control policy.

7
INTRODUCTION Secondhand smoke (SHS) is a mixture of the smoke given off by the burning of a cigarette, pipe, or cigar, and the smoke exhaled from the lungs of smokers. There are more than 4,800 chemicals in secondhand smoke including 69 carcinogens as well as other chemicals that are irritants, toxicants and mutagens (Framework Convention Alliance on Tobacco Control, 2005). To control the risk of SHS, the World Health Organization (WHO) has promoted smoke-free legislations around the world by organizing the convention on tobacco control in 2003. Article 8 of the UN Framework Convention on Tobacco Control (FCTC) called for the expansion of smoke-free places at the national and other jurisdictional levels in signatory countries. Lao PDR, as a member country of the WHO, has adopted initiatives to implement smoke-free regulations in the country in accordance with Article 8 of the Framework Convention on Tobacco Control (FCTC). In 2000, the Ministry of Health (MOH) approved to develop the tobacco control policy following the national conference in Vientiane capital on 24 July 2000 which was attended by 46 participants from 12 ministries, mass organizations, and related organizations. The regulation on the establishment of smoke-free places is one of 9 articles of the policy which include the banning of smoking in schools, hospitals, government offices, restaurants, and other public places. Many places have begun to implement the policy; for example, 6 of 17 provinces of Laos have a pilot project in about 60 schools. The projects trained the teachers as educators who then train their school children about the dangers of smoking and secondhand smoke. The smoke-free policy was also adopted in government offices in the province of Luang Prabang (4 Provincial Department: Provincial Administration Office, Culture, Education and Health) and in the Ministry of Foreign Affairs, including most of the government hospitals. However, the enforcement of the policy is very limited, thus smoking is observed in many of the above-mentioned places. In Lao PDR, a number of researches have been conducted recently focusing mainly on the prevalence of smoking and smoking behaviors of different target groups in different places. Their findings showed that the prevalence of smoking in Laos continues to increase. Most recently, the National Institute of Public Health conducted a health survey as part of the World Health Survey (WHS) 2003 in Lao PDR, as a community based survey with national representatives and the results showed that the prevalence of smoking is about 40%, with males exceeding females, as well as a higher prevalence found in rural areas.

8
A tobacco control policy has been developed by MOH in 2001. The regulation on smoke-free places is one of 9 articles of the policy stating that smoking should be banned in schools, hospitals, governmental offices, restaurants and other public places. However, the effort in implementing the tobacco control policy is not so strong as smoking is still permitted in many places such as restaurants and other public places and on public buses. Currently, there is no data available concerning SHS or passive smoking and tobacco-related diseases in Laos. The study on the exposure to SHS among workers in restaurants in Vientiane Capital and Luang Prabang Province will generate strong evidences that can be used to push for the total ban on smoking in restaurants and other smoke-free places. Data derived from this study will also be very useful for policymakers in implementing the policy concerning tobacco control in Lao PDR.

9
LITERATURE REVIEW
Global Trend of Tobacco Consumption and Smokers The practice of cigarette smoking is the most widespread type of tobacco consumption worldwide. In the last few decades, the number of cigarettes consumed increased by about 76% from 1970 to 2000, with dramatic increases seen in the developing countries (those with low and middle incomes). In the South East Asia region alone, total cigarette consumption increased 2.5 times (from 141,345 million sticks in 1970 to 363,786 million sticks in 2000; Mackay & Eriksen, 2002 and Guindon & Boisclair, 2003), while the developed countries experienced a decline.
Based on the World Health Organization (WHO) estimates for 2000, one in three cigarettes is consumed in the Western Pacific Region. On the average, around 60% of the total consumption in the Region is by men and 6% by women. The largest number of smokers in the Region is Chinese men. Among the five largest countries by population in the Region, only Japan and the Republic of Korea are experiencing decline in tobacco use prevalence. The rates of tobacco use remained high in the rest of the developing nations in the Region. (Shafey, Dolwick & Guindon, 2003). Mackay and Eriksen estimated that the trend of active smoking in developed countries declined during last three decades. For example, in the United States, the percentage of cigarette smokers decreased from 38% to 24% (male smoking declined from 44% to 26% and female smoking declined from 32% to 22%) and similarly in the United Kingdom, the percentage of smokers dropped from 50% to 27% (55% to 28% for male smokers and 44% to 26% for female smokers) (Mackay & Eriksen, 2002).
The WHO estimated that there were approximately 1.3 billion people who smoke cigarettes or other products in the world in year 2003, of which almost one billion were males. Among the male smokers in the world, about 35% were in the developed countries and 50% in the developing countries, while female daily smokers in the world was about 22% of women in developed countries and around 9% of women in developing countries (Mackay & Eriksen, 2002 and Shafey, Dolwick & Guindon, 2003). The International Agency for Research on Cancer also presented the prevalence of cigarette use among smokers in the world, with male smokers accounting for five times more than females.

10
Prevalence of Smoking in Lao PDR Lao PDR is classified under the Western Pacific Region by the WHO. It is a nation that has a high prevalence rate of smoking compared to its neighboring countries and some other countries in the Region (2000). Also, Laos has a very high proportion of adult smoking among the other nations. Compared to other neighboring countries, Lao PDR has the second highest rate of adult smoking after Mongolia (46.7%) followed by Cambodia (37.0%), Myanmar (32.9%), Vietnam (27.1%), Malaysia (26.4%), and Thailand (23.4%) (Mackay & Eriksen, 2002, The Tobacco Atlas). Moreover, the percentage of smokers has increased among both men and women in the last few years, according to the Lao Health Survey, which is part of the World Health Survey conducted in 2003. The survey found that 40.3% of respondents reported that they were currently smoking, of which 78.9% was men and 20.0% was female. The average number of cigarettes smoked was up to 20 sticks and more among male respondents (NIOPH, 2006).
Definition of Secondhand Smoke Tobacco is consumed mainly by burning tobacco products and inhaling the smoke, and cigarette is the most prevalence form of tobacco consumption. The smoke from burning cigarettes and other type of tobacco products (sidestream smoke), and smoke that is exhaled from the lung of smokers (mainstream smoke) contain a complex mixture of gases and particles. The smoke that contaminates indoor spaces and outdoor environments by active smokers has often been referred to as Secondhand Smoke (SHS) or Environmental Tobacco Smoke (ETS), and the inhalation of the smoke by people who are not active smokers is commonly referred to as involuntary smoking or passive smoking (U.S. Dept. of Health and Human Services, 2006). Effects of Secondhand Smoke on Health There is a range of chemical constitutions in both sidestream and mainstream smoke, which comprises around 4000 different chemicals. Many of these substances are known to be toxic, such as carbon monoxide, ammonia, arsenic, mercury and formaldehyde, and they are harmful to the health of those who breathe in the tobacco smoke, especially referred to as human carcinogens. A number of studies illustrated that personal direct contact with tobacco smoking could lead to a wide range of diseases, of which the most common fatal illnesses include lung cancer, chronic lung disease such as chronic obstructive pulmonary disease (COPD) or asthma and cardiovascular disease and others (Royal College of Physicians, 2005). Therefore, since non-smokers who are exposed to secondhand smoke also breathe in the same poisons as the active smokers, they are also likely to face similar health hazards as the active smokers. The SHS

11
exposure not only could lead to ill health, at worst it could result to disability or mortality for the persons affected. Respiratory System Effects Chronic Obstructive Pulmonary Disease (COPD) Chronic obstructive pulmonary disease (COPD) is a chronic inflammation of the airways, referring to chronic bronchitis and emphysema. In both diseases, there is chronic obstruction of the flow of air through the airways and out of the lungs. Shortness of breath, coughing, producing sputum (mucus), and wheezing are symptoms of COPD. In the case of shortness of breath, it usually gets worse during exercise. Cigarette smoking is known as the most important risk factor for COPD. Likewise, secondhand smoke is another factor that researchers identified that can be a risk factor of this disease, especially among non-smokers (University of Pittsburgh Medicine Center, 2006). There have been a number of researches about an increased risk of COPD as shown by evidence of the damaging effects on lung function among adult non-smokers exposed to SHS, indicating that a causal relation exists for COPD (Royal College of Physicians, 2005). Recently, a longitudinal cohort study of adults in the US was conducted to explain the impact of SHS exposure on COPD health outcomes. The finding of this study illustrated that exposure to SHS was an important factor that influenced the severity of COPD. It was found that higher level of passive smoking exposure was associated with worse COPD severity (Eisner et al., 2006). Asthma Children can be exposed to secondhand smoke both during fetal and early postnatal life from maternal or parental smoking and exposure to SHS is a factor for asthma development. The exposure to maternal smoking during in utero and after birth is a risk factor for reduced lung function development that remains a serious childhood and public health issue (Moshammer et al., 2006). The result of over two years of study by Lannerö et al. (2006) indicated that mother’s smoking during pregnancy and during the first year of a child’s life was associated with an increased risk of wheezing in the child and the development of asthma at two years of age (Lannerö et al., 2006). Also, children who are exposed to in utero tobacco smoke from their mothers are 1.8 times more likely to develop asthma and wheezing than those without in utero SHS exposure (Dhala, Pinsker & Prezant, 2005). Although, there have been far fewer studies of passive smoking and respiratory system effects on adults compared to the number of research study on children, nonetheless,

12
passive smoking has been identified as a risk factor for asthma among adults. In a study by Dhala et al. which evaluated the respiratory health effects of secondhand smoke, it was shown that exposure to passive smoking during childhood could lead to an increased prevalence of asthma in adult never-smokers, especially among the never-smokers who have no family history of asthma (Dhala, Pinsker & Prezant, 2005). Adults who are exposed to SHS at home or in the workplace have an increased risk of around 40–60% of suffering from asthma compared to those without exposure to the smoke. Exposure to SHS also exacerbates respiratory symptoms and lung function among adults’ asthmatics (Coultas, 1998). Furthermore, results of a cross-sectional study that examined the association between SHS exposure and pulmonary function among non-smoking adults in US, focusing particularly on adults with asthma, indicated that high level of recent SHS exposure was related to greater asthma severity and a larger prospective risk of hospital admission for asthma (Eisner et al., 2005). Cardiovascular Effects Cardiovascular disease is the leading cause of mortality in the developed nations, which include coronary heart disease (CHD) and stroke. For example, in 2003, there were approximately 480,000 and 158,000 deaths due to CHD and stroke, respectively in United States, and it has been estimated that millions of Americans face the risk of new or recurrent heart attack and around 700,000 persons is likely to suffer from a new or recurrent stroke each year. The most important risk factor of the disease is active smoking; however, smoke from tobacco is a carcinogen that also has been considered as a major risk factor for heart disease (US Dept. of Health and Human Services, 2006). Recently, a number of studies which investigated secondhand smoke and its relationship to cardiovascular disease, has shown that exposure to cigarette smoke can significantly increase the risk of coronary heart disease mortality in non-smokers (especially, female non-smokers whose husbands smoke) by around 30% (Royal College of Physicians, 2005). Moreover, if people were to exposed to secondhand smoke for a long time period, there is clear evidence that they will risk facing long-term health effects, including reproductive system effect, carcinogenic effects (US Dept. of Health and Human Services, 2006) , and lung cancer (Dhala, Pinsker & Prezant, 2005; Nishino et al., 2001; Jee et al., 1999; Kreuzer et al., 2000). In addition, exposure to SHS is also linked to several other cancers, including breast nasopharyngeal and cervix cancers (US Dept. of Health and Human Services, 2006).

13
Economic Effects of SHS Exposure to SHS is significantly associated with increased morbidity and mortality from a wide range of diseases. This is a public health problem and a considerable economic burden on both the individual and household, and national levels. It results in excess cost of morbidity and mortality, including direct medical costs, costs associated with disability or mortality and the opportunity costs of unpaid caregivers. For example, in the United States in 2004, an estimated US$3.85 billion was spent on medical care for non-smokers who were suffering from lung cancer, COPD and CHD as a result of exposure to secondhand smoke. Diseases caused by SHS exposure not only incur increased direct medical costs, they also result in lost of economic value due to lost wages and fringe benefits, as well as the value of lost household services estimated at about US$4.10 billion due to disability and premature deaths from 3 categories of diseases caused by exposure to secondhand smoke. They are: lung cancer (US$469 million), COPD (US$886 million), and CHD (US$2,752 million) (Behan, Eriksen & Lin, 2005). The study on tobacco-related socio-economic cost of stroke, lung cancer, and chronic obstructive pulmonary diseases in Lao PDR revealed that the rate of tobacco smoking is significantly higher in patients suffering from the 3 diseases (62%). The mean total health care cost during hospitalization was 4,081,862 Kips (US$464) for lung cancer; 6,150,720 Kips (US$790) for stoke range; 2,413,310 Kips (US$310) for COPD (Chu Vang et al, 2007).
Trend in the Exposure to SHS of Non-smokers Exposure to SHS by non-smokers will depend upon the smoking prevalence (percentage of smokers) and the number of cigarettes smoked by each smoker per unit time that non-smokers are in contact with. Thus, with the decline in smoking prevalence in the last few decades in the developed countries, the number of people exposed to SHS in these countries would have decreased as well. In the United States, the trend showed that the number of non-smokers who are exposed to SHS has significantly decreased to approximately 70% overall, over a period of 14 years (1988 to 2002) based on examination of the blood fluid cotinine levels over four periods of time. In the first phase, nearly all non-smokers were exposed to tobacco smoke, or 88% of the survey population from 1988-1991 and the proportion continuously declined to 80% (1991-1994). The number of people exposed to SHS decreased to 51% during 1999-2000 and further decreased to 43% in 2001-2002. Additionally, approximately 126 million Americans were estimated to have been

14
exposed to SHS in 2000, including around 22 million children aged 3 to 11 years, 18 million non-smoking youth aged 12 to 19 years, and 86 million non-smoking adults aged 20 years or more (US Dept. of Health and Human Services, 2006). Although the number of non-smoking persons who experienced inhalation of tobacco smoke appreciably dropped over a period of one decade, however, there are still a huge number of non-smokers exposed to SHS. It makes one wonder about the trend of exposure to SHS by people in the developing countries. As 80% of the world’s population reside in the developing countries, where the prevalence of tobacco consumption and the percentage of smokers are the highest, the number of non-smokers who suffers from the SHS would be enormous. For example, a cross-sectional study of Gu et. al. in China during 2000-2001 estimated that 147,358,000 Chinese men and 15,895,000 Chinese women aged between 35-74 years of age were current cigarette smokers. About 8,658,000 men and 108,402,000 women were exposed to SHS at home, and 19,072,000 men and 55,372,000 women were exposed to Environmental Tobacco Smoke (ETS) in their workplaces. In total, there were 191,504,000 non-smoking Chinese who experienced SHS exposure during that period (Gu, D. et al., 2004). Smoke-free Law SHS exposure affects, at varying degrees, human health and the economies of a huge number of populations worldwide, especially those of non-smokers. A number of countries have responded by trying to reduce the health risks and burden of the population by restricting or prohibiting smoking in worksites and public places by imposing “smoke-free laws”. This can reduce the health risks to non-smokers, particular the group of people who are not smokers but are subjected to SHS because of their occupation. Positive results can been seen in California where one to two months after the establishment of a ban on smoking in bars and taverns in the state, the majority of bartenders who initially were suffering from respiratory and sensory irritation symptoms have reported that these symptoms have appreciably declined. Also, the function of pulmonary has improved following a decreased in SHS exposure in their workplace (Eisner, BS Smith & Blanc, 1998). Similar results were reported by the recent study by Menzies et al. in Scotland. After three months following a ban on smoking in public place, there was a rapid improvement in the health of the bar staff. Their respiratory and sensory symptoms were reduced and their respiratory function has also improved (Menzies et al., 2006).

15
Moreover, the advantage of having smoke-free workplaces is that not only would it reduce health risks or hazards among people who do not smoke, but it could also reduce cigarette consumption among smokers (Eisner, BS Smith & Blanc, 1998), and this could lead to a decrease in morbidity and mortality of smokers as well as reduce the economic costs related to smoking.
Tobacco Smoking Sites and Exposure to SHS The Report of the Surgeon General in 2006 confirmed that the three main places where exposures to secondhand smoke often occur were homes, worksites, and public places including restaurants, malls, and bars. These places contribute to personal exposures in varying degrees across different groups. Because the home is where many people, especially children, spend most of their time in, it is therefore potentially the most important place for SHS exposure especially for those who live with regular tobacco smokers. The workplace is the second most important site for SHS exposure because it is a place where adults spend most of their time. Although the home and workplaces are important sites where non-smokers are exposed to SHS, public places such as restaurants, pubs, bars etc. are also important contributors to SHS exposure for clients and staff who do not smoke. This is particularly true of pubs and bars which are places of refuge for smokers. While public places such as bars and restaurants have been identified as worksites where SHS exposure is high (Edwards et al., 2006), nonetheless, these workplaces are least likely to be covered by laws or policies that ban smoking. Hence, workers in these worksites, particularly the non-smokers, tend to suffer from the effects of high level of exposure to SHS, but they are least likely to be afforded protection from the health risk. Furthermore, an occupational mortality study found that being a waitress was the most hazardous occupation for women, and being a bartender ranks among the seven most hazardous occupations (Siegel, M., Barbeau, EM. & Osinubi, OY. (2005). According to two studies conducted by researchers at the Johns Hopkins Bloomberg School of Public Health, the results of the first study showed that the average level of particulate matter pollution in the bars surveyed was at least 10 times higher than the Environmental Protection Agency’s (EPA) outdoor air safety levels. The result of the second study showed that air nicotine was detected in all the bars where smoking was allowed, indicating that involuntary exposure to tobacco smoke occurs in Baltimore bars. No nicotine was detected in the hair of non-smoking employees working in a smoke-free bar, while high levels of nicotine were detected in the hair from non-smoking employees working in bars where smoking is allowed. The harmful effects of exposure to SHS on non-smokers are clearly established. Risk of SHS has not only been shown to be the main cause of human lung carcinogen, but it

16
also increases the risk of respiratory system illness in both children of all ages and adults (American College of Chest Physicians, 1995). SHS also results in acute and chronic respiratory ill health in non-smokers. The short-term respiratory effect that often occurs is respiratory symptoms, which is an acute pulmonary effect of SHS, including coughing, wheezing, chest tightness, and difficulty in breathing. These symptoms are linked to exposure to SHS. A number of studies have attempted to evaluate the relationship between SHS exposure and respiratory symptoms, but they have not consistently included asthma and some other environmental factors (US Dept. of Health and Human Services, 2006). However, recent studies have demonstrated that reduced SHS exposure of waitress or bartenders in their workplaces has decreased respiratory symptoms that they had previously suffered (Eisner, BS Smith & Blanc, 1998 and Menzies et al., 2006).

17
STUDY OBJECTIVES
3.1 Overall Objective
To provide the evidence based information on health-related issues caused by secondhand smoke to policy-makers in order to push for the adoption of the tobacco control policy of Lao PDR Act of 2001, particularly Article 4 on the establishment of smoke-free places including restaurants
3.2 Specific Objectives
• To investigate the association between passive smoking at restaurants with environmental tobacco smoke exposure and the risk of developing respiratory syndromes.
• To investigate the association between non-smoking workers in restaurants and the smoke-free offices on the risk of developing respiratory syndromes.
• To compare health status (respiratory syndromes) between the workers who are exposed to SHS in the restaurants and unexposed workers to SHS in smoke-free offices.
• To estimate the direct and indirect costs of smoking-related diseases among the workers who are exposed to SHS in the restaurants/offices
18
METHODS & DATA SOURCES
4.1 Research Design
This is a cross-sectional study that was carried out using structured interview questionnaires (Face to face interview) as data collection tool among non-smoking restaurant workers and non-smoking workers in smoke-free offices.
4.2 Sampling Frame
Vientiane capital city (VTE) and Luang Prabang (LPB) municipality were selected because they are popular tourist sites with many existing restaurants. The sampling frame was based on the following criteria:
• Restaurants with more than 5 workers and that allow smoking in both VTE and LPB municipality.
• Smoke-free offices in both VTE and LPB municipality. • Workers of both sexes who have at least one year of working experience in
either of the two places. • Workers at restaurants e.g. the waiters or waitress should have environmental
tobacco smoke (ETS) exposure 4.3 Sampling Method Due to the lack of information about the restaurants or offices where smoking is allowed or prohibited, the research team therefore conducted a pilot survey first in Vientiane capital city by collecting a list of all available restaurants that are registered at the district travel authorities of 5 districts namely Sikhottabong, Chanthabury, Sisattanack, Saysetha, and Saythany, followed by Luang Prabang municipality. After obtaining such a list, the researchers visited the restaurants. A screening form (Annex 1) based on the above mentioned criteria was used to list all target population for further sampling in addition to obtaining information about personal smoking habits. A total of 70 restaurants in VTE and 65 restaurants registered with Luang Prabang provincial travel authorities were in the frame for the first sampling unit. The restaurants were classified into 3 types as (1) Air-conditioned enclosed Restaurants; (2) Mixed enclosed/open air Restaurants; and (3) Open-air Restaurants.

19
All offices which were included in this study were smoke-free offices. They were also classified into 3 types as mentioned above. All these offices prohibit smoking in the workplaces.
4.4 Sample Size
The selection of the restaurants and office workers were made randomly from the list of restaurants and smoke-free offices provided by provincial/district travel authorities. The sample size was determined with 95% confident interval, 90% power, detecting an OR of 2, SHS was associated significantly with frequent colds, cough and phlegm, throat problems, and the presence of any respiratory symptoms with adjusted odds ratios of 1.89 (95% confidence interval) (Ho S. Y. et al, 2007), and about 27% of presence of any respiratory symptoms. Based on the 95% confident interval, α = 0.05, Z α =1.96, 90% power or 1- β, β = 0.1, Zβ =1.28, OR = 2, and P of exposure = 27 %, the calculation was made using software EPI 6.04 of unmatched case-control. The estimated sample for each province was 150 restaurant workers and 150 office workers with a sub-total of 300 in each site and with a total of 600 in the two provinces. In VTE, a total of 70 restaurants were registered with the travel district authorities. All restaurants which had 5 or more staff were included in the sampling frame. In order to get 150 cases for the restaurant group, 30 restaurants from 70 restaurants were randomly selected for the first selection. In a second step, visits were made to the selected restaurants and a list of staff members working in each restaurant was obtained. The respondents who smoke or ever smoked were excluded from the sampling frame to avoid bias. Five workers from each restaurant was then selected proportional to size (PPS) using simple random sampling. The same procedure was done in Luang Prabang province. For the Office group, all offices which had 5 staff or more were included in the sampling frame and to get 150 respondents, a total of 30 offices were randomly selected from all 90 offices in VTE and 62 offices in Luang Prabang province.

20
4.5 Measurement of Outcomes Exposure to Secondhand Smoke
• By living with smokers • Time exposure in the last seven days (number of hours) • Contact with smokers (household member, co-worker, customer, others)
Respiratory symptoms in the last two months
• Wheeze and tightness in the chest • Shortness of breath • Cough and phlegm from the chest • Breathing difficulty • Asthma
4.6 Data Collection Methods Structured Interview Questionnaires (Face to face interview) The 3 structured interview questionnaires were provided during the regional workshop in December 21-22, 2006, in Bangkok, Thailand. The first was respiratory health of bar workers abbreviated IUALD reproduced with permission of Mark D. Eisner, University of California and the second was the questionnaire prepared for the Respiratory Disease Committee of the International Union Against Tuberculosis and Lung Disease (UNION) by Burney P et al. and the last was a standard respiratory symptom questionnaire developed by Hedley et al. (2006). These questionnaires were revised accordingly to suit the objectives and situation of Lao PDR by the national research team with the technical assistance of the experts from SEATCA. To assess tobacco exposure, we based self-reported exposure to passive smoking. Non-smoking workers from both the restaurant and office groups were asked in a standard interview on matters relating demographic and their past exposure to secondhand smoke, including workplace and home exposures as well as their past smoking history. The questionnaire was also designed to capture information about the characteristics of the respondent’s workplace with respect to passive smoking and secondhand smoking related to health care cost (Annex).

21
4.7 Pre-testing of the Questionnaire
The questionnaire was developed in English and after it was finalized, the questionnaire was translated into Lao language and pre-testing was conducted in Vientiane capital city. The research team was divided into two groups of 4 persons each. The first group was responsible for interviewing 15 non-sampled restaurant workers and the other group was responsible for the same number of office workers. The total number of pre-testing questionnaire respondents was 30. After the completion of the pre-testing, the questionnaire was revised accordingly. 4.8 Data Collection and its Quality Control Training of interviewers and supervisors was performed before the collection of the data. The five-day training of 8 data collectors and 2 supervisors was conducted in mid-August 2007 with the aim to make the data collectors understand the objectives of the survey and the methodology on how to select targets for case and control groups. Question by Question review was done in order to familiarize members of the research team with and to ensure that they understand all the questions in the questionnaire. All the data collectors have had experience in many national surveys in the past. The training sessions included theory (2 days), role play in the class (1 day) and field practice (1 day), and one day of revision of all the contents of the survey tool plus feedback from the field practice. Research team members then provided comments and suggestions on how to improve the quality of data collection. One supervisor was assigned to take care of data collection in each site. Soon after the training, two teams with 4 enumerators were formed and each team was assigned the responsibility to collect the data in each study site. Data collection started in VTE capital city soon after the pilot from 20 August to 5 September 2007. The pilot survey in Luang Prabang started on 25 August with the same procedure as that conducted in VTE capital city and data collection started on 10 September 2007 and was completed on the 25 September 2007.
Limitation
The study could not draw on a non-exposed group of respondents from restaurants to compare with exposed non-smoking workers in the restaurants, as during the pilot survey it was not possible to find non-exposed restaurant workers as there were no
22
restaurants which prohibited clients from smoking. Therefore, the team decided to include offices that have similar environments to restaurants, such as banks, travel agencies, telecommunication offices where smoking is not allowed, to obtain a non-exposed group as an initial plan of this study. The matching selection of both groups was non-smokers and never-smoked and worked at the current place for more than 1 year. 4.9 Data Processing and Analysis All 600 questionnaire forms were checked for completeness and consistency by those 8 data collectors by exchanging them between the teams. Data entry set was developed by one of the team members using Epi-info 10.0 program. All questionnaire forms were completely entered one week after receiving all forms from each study site. All entered data was then transferred to SPSS statistical package version 11.5 for further analysis. The frequencies, mean, standard deviations, and proportions were calculated. The 95% confidence interval and the chi-square test were used to compare differences between groups and provinces. Logistic regression was performed.
4.10 Ethical Consideration
In order to ensure that ethical aspects of the subjects were protected, an Ethical clearance was issued and approved by the National Ethical Committee for Health Research, Ministry of Health Lao PDR. The objectives of the study were explained to all subjects recruited for the study who gave their verbal informed consents on a voluntary basis.

23
RESULTS
5.1 General Characteristics of Respondents in Both Groups
A total of 600 respondents were recruited for the study, 300 respondents from Luang Prabang province and 300 participants from Vientiane capital city. In each province, a total of 150 non-smoking restaurant workers and 150 non-smoking officers from smoke-free offices were recruited. Most of the respondents were female (55.8%), in the mean age of 27.09 years old (±6.8SD, range 15 to 55) with a high concentration in the age group 25 to 34 years old (44.8%). Most of the female respondents have secondary school and higher education. More than half of the restaurant workers sampled were in the age group 15-24 years old (59% and 69% for Vientiane (VTE) and Luang Prabang (LPB), respectively), single (78% and 74%) and had secondary education (67% and 53%), while most of the office workers sampled were in the age group of 25-34 years old (58% and 67%), married (52% and 67%) and had college/university education (89% and 89%) (Table 1).
Table 1: Background characteristics of respondents - restaurant workers, and officers - by province
Restaurant workers Officers
VTE capital
LPB VTE capital LPB
Total number
Sex N (%) N (%) N (%) N (%) N (%)Male 74 (49.3) 60 (40.0) 61(40.7) 70(46.7) 265 (44.2)
Female 76 (50.7) 90 (60.0) 89 (59.3) 80 (53.3) 335 (55.8)Age groups
15-24 88 (58.7) 104 (69.3) 33(22.0) 20 (13.3) 245 (40.8)25-34 47 (31.3) 35 (23.3) 87 (58.0) 100 (66.7) 269 (44.8)35-44 13 (8.7) 7 (4.7) 27 (18.0) 25 (16.7) 72 (12.0)
45+ 2 (1.3) 4 (2.7) 3 (2.0) 5(3.3) 14 (2.3)Marital status
Single 117 (78.0) 111 (74.0) 72 (48.0) 49 (32.7) 349 (58.2) Married 33 (22.0)
39 (26.0) 78 (52.0) 101 (67.3) 251 (41.8)
Educational level
Primary school 7 (4.7) 14 (9.3) 0 2 (1.3) 23 (3.8)Secondary
school 100 (66.7) 79 (52.7) 17 (11.3) 15 (10.0) 211 (35.2)
College/ University
43 (28.7) 57 (38.0) 133 (88.7) 133 (88.7) 366 (61.0)

24
5.1.1 Types of Workplaces
The number of seats in the restaurants surveyed differed from one restaurant to another. There were 3 types of restaurants surveyed; (1) with air condition only, (2) with and without air condition, and (3) without air condition. The restaurants with air conditioning had on average 157 ± 126.6 SD (range from 37 up to 800). The number of seats in the restaurant which had room with air condition and open room without air condition was around 60, and the restaurants without air conditioning on, an average had 76 seats ± 60 SD (range from 28 to 150).
The offices selected for the office workers group included bank offices (BCEL, Public bank, Lao-Viet Bank, Agricultural Promotion Bank), Library (NUOL), Telecommunication office (ETL), Social Security Organization, and City Development Organization, with an average of 15 seats (range from 3 to 140).
On the question asked of all respondents with regards to policy knowledge, the result showed that for the restaurant group in Luang Prabang, 92% of respondents stated that smoking was not allowed inside the building while 40.7% in VTE stated that smoking was allowed inside the building. Meanwhile 84.0% of the respondents in the office group in LPB and 82.7% in VTE stated that smoking was not allowed inside the building (Table 2).
Table 2: Percent distribution of respondents on policy knowledge by province
Type Province Policy knowledge Smoking not
allowed inside the building
No (%)
Special place for smoking No (%)
Smoking allowed No (%)
LPB 138 (92.0) 10 (6.7) 2 (1.3) Restaurant group
VTE 2 (1.3) 87 (58.0) 61 (40.7)
LPB 126 (84.0) 22 (14.7) 2 (1.3) Office group
VTE 124 (82.7) 20 (13.3) 6 (4.0)
5.1.2 Working Hours The workers in the restaurants in both provinces worked on average 54 to 56 hours per week and the officers work on average 40-42 hours per week. Most of the restaurant workers and officers have been working in their current workplaces for more than one year. Approximately 37.7% of the workers in the restaurants and 25.0% of the officers had previously worked elsewhere. Of those 113 restaurant workers who had previous
25
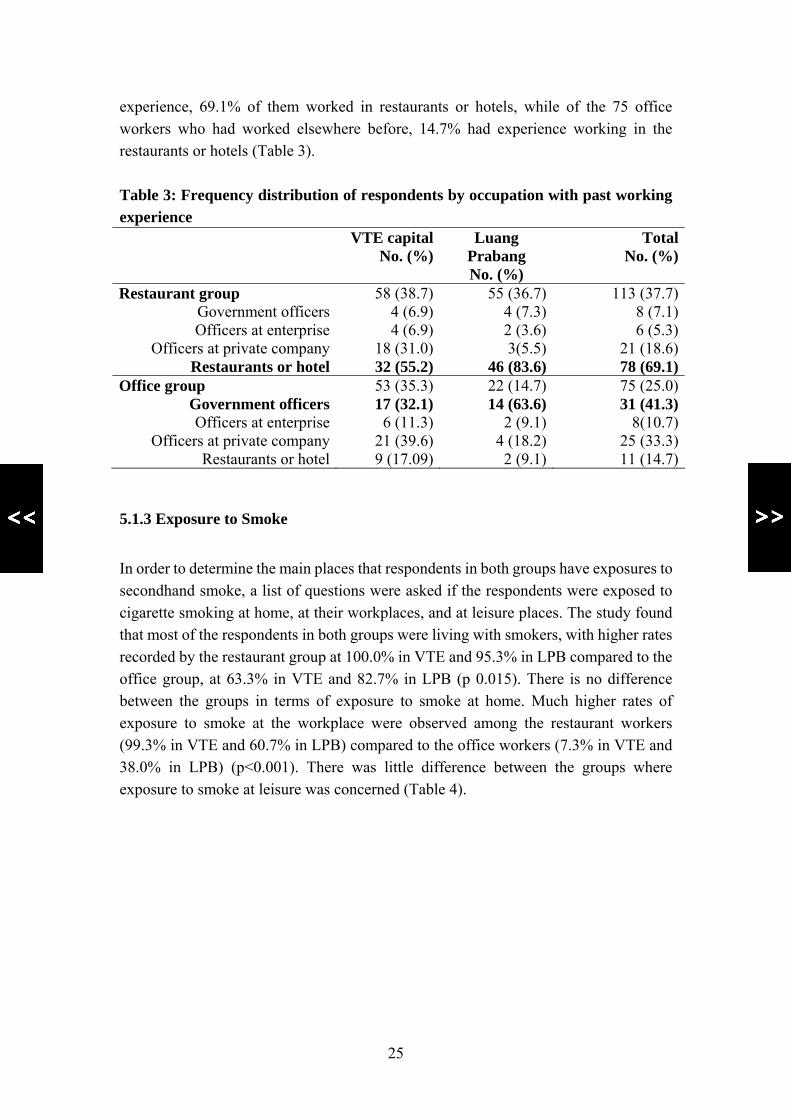
experience, 69.1% of them worked in restaurants or hotels, while of the 75 office workers who had worked elsewhere before, 14.7% had experience working in the restaurants or hotels (Table 3). Table 3: Frequency distribution of respondents by occupation with past working experience VTE capital
No. (%)Luang
Prabang No. (%)
Total No. (%)
Restaurant group 58 (38.7) 55 (36.7) 113 (37.7)Government officers 4 (6.9) 4 (7.3) 8 (7.1)Officers at enterprise 4 (6.9) 2 (3.6) 6 (5.3)
Officers at private company 18 (31.0) 3(5.5) 21 (18.6)Restaurants or hotel 32 (55.2) 46 (83.6) 78 (69.1)
Office group 53 (35.3) 22 (14.7) 75 (25.0)Government officers 17 (32.1) 14 (63.6) 31 (41.3)Officers at enterprise 6 (11.3) 2 (9.1) 8(10.7)
Officers at private company 21 (39.6) 4 (18.2) 25 (33.3)Restaurants or hotel 9 (17.09) 2 (9.1) 11 (14.7)
5.1.3 Exposure to Smoke
In order to determine the main places that respondents in both groups have exposures to secondhand smoke, a list of questions were asked if the respondents were exposed to cigarette smoking at home, at their workplaces, and at leisure places. The study found that most of the respondents in both groups were living with smokers, with higher rates recorded by the restaurant group at 100.0% in VTE and 95.3% in LPB compared to the office group, at 63.3% in VTE and 82.7% in LPB (p 0.015). There is no difference between the groups in terms of exposure to smoke at home. Much higher rates of exposure to smoke at the workplace were observed among the restaurant workers (99.3% in VTE and 60.7% in LPB) compared to the office workers (7.3% in VTE and 38.0% in LPB) (p<0.001). There was little difference between the groups where exposure to smoke at leisure was concerned (Table 4).

26
Table 4: Frequency distribution of respondents exposed to secondhand smoke by places and province Living with
smoker No. (%)
Exposure at home
No. (%)
Exposure at
workplace No. (%)*
Exposure at leisure No. (%)*
Exposure at other public places
VTE 150 (100.0) 52 (34.7) 149 (99.3) 72 (48.0) 9 (6.0)Restaurant group LPB 143 (95.3) 65 (43.3) 99 (60.7) 49 (27.3) 3 (2.0)
VTE 95 (63.3) 35 (22.0) 11 (7.3) 73 (48.7) 21 (14.0)Office group
LPB 124 (82.7) 63 (42.0) 57 (38.0) 92 (61.3) 2 (1.3)
VTE 245 (81.7) 85 (28.3) 160 (53.3) 145 (49.3) 30 (10.0)
LPB 267 (89.0) 128 (42.7) 148 (49.3) 133 (47.8) 5 (1.7)
Total
Total 512 (85.3) 213 (35.5) 308 (51.3) 278 (46.3) 35 (5.8)
5.1.4 Number of Hours that Respondents Spend with Smoking Pollution and Person Who Smokes The study found that restaurant workers were exposed to secondhand smoke for much longer periods than the office group with an average of 11.6 hours per week for the restaurant group (range from 0 to 70) and 1.63 hours for the office group (range from 0 to 15 hours (p<0.000) (Table 5).
Table 5: Mean and Standard deviation of hours that respondents are exposed to smoking pollution Province Mean Std. Deviation Minimum Maximum VTE capital city
Restaurant group (n=150) 20.05 18.156 0 70
Office group (n=95) 2.48 2.588 0 15
Total (n=245) 13.24 16.657 0 70Luang Prabang
Restaurant group (n=143) 2.78 4.422 0 28
Office group (n=124) .98 1.367 0 10
Total (n=267) 1.94 3.479 0 28Total
Restaurant group (n=293) 11.62* 15.892 0 70
Office group (n=219) 1.63 2.121 0 15
Total (n=512) 7.35 13.065 0 70* p<0.001

27
There were 5 cases which reported having been exposed to SHS for up to 70 hours per week (approximately 10 hours per day). It was found that customers were the main source of SHS for restaurant’s workers, while for the office group it was their colleagues and others ((friends, relatives, people at parties, in the bars, night clubs, etc.) (Table 6).
Table 6: Frequency distribution of people who are smokers that the respondents had contact with VTE capital city
Number (%)Luang Prabang
Number (%)Total
Number (%)Restaurant group
* P<0.001
HH members 52 (34.7) 65 (45.5) 117 (39.9)Colleagues 65 (43.3) 60 (42.0) 125 (42.7)Customers 147 (98.0) 84 (58.7) 231 (78.8)*
Others 29 (19.3) 6 (4.2) 35 (11.9)*Office group
HH members 35 (36.8) 49 (39.5) 84 (38.4)Colleagues 22(23.2) 96 (77.4) 118 (53.9)Customers 5 (5.3) 19 (15.3) 24 (11.0)
Others 69 (72.6) 24 (11.9) 93 (42.5)
5.2 The Association between Work Site and the Risk of Developing Respiratory Symptoms Respondents in both groups were asked about respiratory symptoms including wheezing in the chest, chest pain in the morning, short breath without workload, coughing in the early morning or at night, and with phlegm in the morning; wake up at night with short breath, and asthma. The time frame was in the last two months. The respiratory symptoms reported by the respondents in this study included chest pain in the morning and coughing in the morning with phlegm. Among the restaurant group 15.0% reported having such symptoms while 6.3% in the office group experienced these symptoms. The study showed a strong association between worksites, probably due to exposure to passive smoking at work, and the risk of developing respiratory symptoms (OR=2.6, p=0.001, Table 7).

28
Table 7: Frequency distribution of respondents in work sites and respiratory symptoms Restaurant Office Total OR 95% CI P
value No (%) No (%) No (%) Lower Upper Having Respiratory symptoms
45 (15.0) 19 (6.3) 64 (10.7) 2.610 1.487 4.580 0.001
No symptoms 255 (85.0) 281 (93.7)
536 (89.3)
The percentage of respondents having respiratory symptoms was higher among those residing in LPB compared to those in Vientiane at 13.0% and 8.3%, respectively. In both provinces, a higher percentage of those in the restaurant group reported respiratory symptoms compared to the office group at 10.7% and 6.0% in VTE and 19.3% and 6.7% in LPB, respectively (Table 8). Table 8: Frequency distribution of respondents in work sites and respiratory symptoms by province Restaurant Office Total OR 95% CI P
valueVTE No (%) No (%) No (%) Lower Upper Having respiratory symptoms
16 (10.7) 9 (6.0) 25 (8.3)1.871 0.799 4.378 0.149
No symptoms
134 (89.3) 141 (94.0) 274 (91.7)
LPB No (%) No (%) No (%) Lower Upper Having respiratory symptoms
29 (19.3) 10 (6.7) 39 (13.0) 3.355 1.571 7.166 0.002
No symptoms
121 (80.7) 140 (93.3) 261 (87.0)
The results showed that 10.7% of respondents in both groups reported having respiratory symptoms, with a higher rate recorded among those living with smokers (11.7%) than those who were not living with smokers (4.5%) (p=0.041) (Table 9).

29
Table 9: Frequency distribution of respondents exposed to passive smoking by living with smokers at home and respiratory symptoms Having respiratory symptoms Total Yes No
Yes 60 (11.7) 452 (88.3) 512
Living with smoker
No 4 (4.5) 84 (95.5) 88
Total 64 (10.7) 536 (89.3) 600P=0.041
The study found that in VTE, exposure to smoke at home, at the work place and at leisure was associated with having respiratory symptoms (14.1%, 11.3%, 10.3%, respectively), while in LPB exposure to smoke at home was associated with respiratory symptoms (Table 10). Table 10: Frequency distribution of respondents who reported having respiratory symptoms by places of smoking exposure VTE (n=300) LPB (n=300) Having
Respiratory symptoms
No symptoms
Having Respiratory symptoms
No symptoms
Exposure at home
Yes
No
12 (14.1)
13 (6.0)
73 (85.9)
202 (94.0)
17 (13.3)
22 (12.8)
111 (86.7)
150 (87.2) P-value 0.035 0.901
Exposure to smoking at work
place
Yes
No
18 (11.3)
7 (5.0)
142 (88.8)
133 (95.0
13 (8.8)
26 (17.1)
135 (91.2)
126 (82.9) P-value 0.057 0.035
Exposure to smoking at leisure
Yes
No
15 (10.3)
10 (6.5)
130 (89.7)
145 (93.5)
17 (12.8)
22 (13.2)
116 (87.2)
145 (86.8)
P-value 0.227 0.920
Total 25 (8.3) 275 (91.7) 39 (13.0) 261 (87.0)
5.3 Estimation of the Direct and Indirect Costs of Smoking-related Diseases Among the Workers Who Are Exposed to SHS in the Restaurants A total of 221 respondents who had reported having the above respiratory symptoms were asked if they had sought care and if yes, from where and how much they spent on health care cost related to smoking exposure.

30
A total of 185 respondents (84 respondents in VTE and 101 respondents in LPB) responded to this part of the survey. Most participants in both restaurant and office groups had sought care at government hospitals and private pharmacies (Table 11). Table 11: Frequency distribution of respondents who reported seeking care by services Place of seeking care
Restaurant group (n=94)
Office group (n=91)
VTE (n=45) LPB (n=49) VTE (n=39) LPB (n=52) Government hospital
4 ((8.9) 3 (6.1) 3 (7.7) 12 (23.1)
Private clinic 3 (6.7) 1 (2.0) 2 (5.1) 0 Private pharmacy 5 (11.1) 1 (2.0) 2 (5.1) 12 (23.1) Self medication 4 (8.9) 0 3 (7.7) 1 (1.9) Total 16 (35.5) 5 (10.2) 10 (25.6) 25 (48.0)
Those who sought care at a health facility reported both their direct and indirect costs. The mean of the total health expenditure spend per person for care of their illness related to respiratory symptoms was 319,612 Kips (US$37.3), in which 284,620 Kips (US$33.2) are direct cost such as doctor fees, drug, and 66,160 Kips (US$7.7) are indirect cost. Mean direct, indirect, and total cost spending for respiratory symptoms in Luang Prabang is higher than in Vientiane capital city, as well as higher in restaurant workers than in office workers, but they are not statistical significant (Table 12). The number of respondents who were exposed to smoke at any place was higher among restaurant workers (96%) compared to office workers (75%), and as such the former had more respiratory symptoms (14.0%) compared to those who were not exposed to smoke (0.7%), Similarly, those office workers who were exposed to smoke were more likely to have respiratory symptoms (6.0% ) compared to those in the non-exposed group (0.7%). The mean health care cost related to reported respiratory symptoms was higher for restaurant workers in the exposed group at 513, 250 Kips (US$59.9) compared to that of the office workers (197,315 Kips) (US$23.0) (Table 13). The respondents who were restaurant workers and were exposed to smoke in both VTE and LPB had more respiratory symptoms than those office workers and only those in the exposed group either restaurant workers or officers reported having to spend on health care related to respiratory symptoms (Table 14).

31
Table 12: Health care cost by province
Province DIRECT
COST INDIRECT
COST Total Health Expenditures
VTE capital city Mean 108,090 34,571 142,661 N 11 7 13 Std.
Deviation 136,492.09 38789.41 134497.49
Luang Prabang Mean 392,500 78,444 470,944 N 18 18 18 Std.
Deviation 955,064 205,440 999,916
P-value 0.338 0.585 0.208 Total Mean 284,620 66,160 319,612 N 29 25 31 Std.
Deviation 761,696 175,146 778,828
Table 13: Respiratory symptoms and health care cost by exposed and non-exposed restaurant workers and officers
Restaurant workers Officers Exposed to
smoke at any place
Not-exposed to smoke at all
Exposed to smoke at any place
Not-exposed to smoke at all
(n=288) (n=12) (n=225) (n=75) Respiratory symptoms
42 (14.0) 2 (0.7) 18 (6.0) 2 (0.7)
(n=12) (n=18) Mean health care cost (Kips)
513,250 - 197,315 -

32
Table 14: Respiratory symptoms and health care cost by exposed and non-exposed restaurant workers and officers in two provinces
Restaurant workers Officers Vientiane
capital LPB Vientiane
capital LPB
Exposed Non- exposed
Exposed Non- exposed
Exposed Non- exposed
Exposed Non- exposed
(n= 145) (n=5) (n=143) (n=7) (n=101) (n=49) (n=124) (n=26) Respiratory symptoms
15 (10.0) - 27 (18.0) 2 (1.3) 8 (5.3) 2 (1.3) 10 (6.7) -
(n=8) (n=4) (n=5) (n=10) Mean health care cost (Kips)
127,750 - 284,250 81,800 - 238,571 -

33
DISCUSSION
Most of the respondents in both restaurant and office groups were females, in particular those who worked in the restaurants, thus from the perspective of an occupational mortality study, being a waitress was the most hazardous occupation for women (Siegel, M., Barbeau, EM. & Osinubi, OY. (2005). High rates of exposure to smoke at workplaces such as restaurants were observed in the restaurant group. Those who work in restaurants are likely to be exposed to secondhand smoke for long periods of time, and thus restaurant jobs are among the seven most hazardous occupations (Siegel, M., Barbeau, EM. & Osinubi, OY. (2005). After the implementation of a smoke-free policy in the city in Luang Prabang, the study found that non-smoking restaurant workers were exposed to smoking pollution at an average of 2.78 hours per week compared to 20.05 hours per weeks for non-smoking workers in the restaurants in Vientiane capital city. The percentage of respondents who reported of exposure to customers' smoke was 58.7% in Luang Prabang compared with 98.0% in Vientiane capital city. In LPB, a world heritage city, even though the smoke-free policy has been declared and smoking indoor was not allowed since 2007, however, some respondents still reported having been exposed to smoke at the workplace. This may be because the policy is still at its infancy and, therefore, compliance among smokers is poor. In accordance with the report by the Surgeon General in 2006, this study confirms that the workplace is the main place for respondents who are workers in restaurants to be exposed to SHS. It has been a major SHS exposure site because it is a place where adults spend most of their time (Edwards et al., 2006), but these workplaces are least likely to be covered by smoking laws or policies banning smoking. Hence, the workers in these worksites tend to suffer adverse effects from the high level of SHS exposure, particular the non-smokers, but they are least likely to be afforded protection from the health risk. The study confirmed that those who live with smokers are 2.3 times more likely to have respiratory symptoms then those who live in a smoke-free environment and also confirmed that the rate of respiratory symptoms in non-smokers who worked in the SHS environment is higher than those who work in smoke-free places. The respiratory symptoms reported by the respondents include cough and phlegm, chest pain and difficulty breathing as reported by Ho SY et al. The cross-sectional and

34
prospective studies showed that SHS was associated significantly with frequent colds, cough and phlegm, throat problems, and the presence of any respiratory symptoms. According to the study at Baltimore by researchers at the Johns Hopkins Bloomberg School of Public Health, air nicotine was detected in all the bars where smoking was allowed, indicating that involuntary exposure to tobacco smoke occurs in Baltimore bars. No nicotine was detected in the hair of non-smoking employees working in a smoke-free bar, while high levels of nicotine were detected in the hair of non-smoking employees working in bars where smoking is allowed. Workers at the restaurants spend more time at their workplace than the office group , so they are at a greater risk of getting respiratory symptoms than those office workers working in a smoke-free environment as reported by Wakefield M et al. This cross-sectional study confirmed that exposure to SHS at work for part of the day was significantly associated with an increased risk of wheeze, frequent cough, sore eyes, and sore throat and this study had provided evidence that non-smoking workers are affected by exposure to SHS at work and underlined the importance of imposing a 100% smoking ban in the restaurants, pubs, and bars to protect the health of restaurant workers as well as other office workers as stated in the Article 4 of the policy on tobacco control. Exposure to SHS is a public health problem, which is significantly associated with increased morbidity and mortality from a wide range of diseases, especially in people who do not smoke as well as imposes considerable economic burden at both individual or household and national levels. The study found that eventhough few workers were ill and seeked care at health facilities, the mean health care expenditure for the treatment is relatively high compared to the overall health care expenditure at national level (NHS, 2000) at 319.612 Kips (US$37.3) versus 175,000 Kips (US$20.4). The mean health care cost reported by respondents in LPB was higher than in VTE, as there was one case who had repeated respiratory symptoms, who took self-treatment the first time and had to spend more for health check up (X-ray and blood test). In the United States, approximately US$7.96 billion in economic value was lost each year due to morbidity as a result of only 3 diseases as well as disability or premature death caused by exposure to passive smoking (Behan, Eriksen & Lin, 2005).

35
CONCLUSION AND RECOMMENDATIONS The respondents were mostly females in the young age group (15-35 years old), had completed secondary and higher education, and the majority were single. The study found that most of the workers at the restaurants were exposed to secondhand smoke on average 11.6 hours per week compared to 1.63 hours (p<0.001) by those who worked in offices where smoking was prohibited. Ninety two percent of respondents in restaurants in Luang Prabang recognized that smoking s not allowed inside the building, while only 1.3% of respondents in restaurants in VTE were aware of this ruling. The percentage of respondents in both restaurant and office groups who were living with smokers was higher among the restaurant group (100.0% in VTE and 95.3% in LPB) compared to the office group, (63.3% in VTE and 82.7% in LPB). Higher rates of exposure to smoke at the workplace were observed among the restaurant workers (99.3% in VTE and 60.7% in LPB) compared to the office workers (7.3% in VTE and 38.0% in LPB). The study showed that there is an association between respiratory symptoms including chest pain, coughing with phlegm in the morning and exposure to secondhand smoke, more so in restaurant workers than in officer workers who were also exposed to SHS. In both provinces, more cases of respiratory symptoms were reported by restaurant workers than by the office workers, at 10.7% versus 6.0% in VTE and 19.3% versus 6.7% in LPB, respectively. The results showed that 10.7% of respondents in both restaurant and office groups reported respiratory symptoms with a higher rate in those living with smokers (11.7%) than those who are not living with smokers (4.5%) (p=0.041). Most participants in both restaurant and office groups had sought care at government hospitals and private pharmacies. The mean total health expenditure spent to treat their illness is 319,612 Kips (US$37.3), in which 284,620 Kips (US$33.2) are direct cost and 66,160 Kips (US$7.7) are indirect cost, with higher cost spent by exposed restaurant workers (513,250 Kips or US$59.9) than exposed office workers (197,315 Kips or US$23.0). This study provides strong evidence that non-smoking workers are affected by exposure to SHS at work and underlines the importance of having a total ban on smoking in restaurant, pubs, and bars to protect the health of non-smoking restaurant workers and office workers as stated in Article 4 of the policy on tobacco control.

36
REFERENCES Anthony J Hedley et al, The Health Risks and Community Costs of Secondhand Smoke
Exposures, Department of Community Medicine, School of Public Health, University of Hong Kong
American College of Chest Physicians, American Thoracic Society, Asia Pacific
Society of Respiratory, Canadian Thoracic Society, European Respiratory Society, International Union Against Tuberculosis and Lung Disease. (1995). Smoking and health: a physician’s responsibility. A statement of the joint committee on smoking and health. European Respiratory Journal , 1808-1811.
Burney P et al, 1989, the questionnaire prepared for the Respiratory Disease Committee
of the International Union Against Tuberculosis and Lung Disease (UNION). Behan, DF., Eriksen, MP. & Lin, Y. (2005). Economic Effects of Environmental
Tobacco Smoke. Society of Actuaries. Coultas, DB. (1998). Passive Smoking and Risk of Adult Asthma and COPD: An
Update. Thorax, 53, 381-387. Dhala, A., Pinsker, K. & Prezant, DJ. (2005). Respiratory Health Consequences of
Environmental Tobacco Smoke. Clin Occup Environ Med; 5 (1), 139-156. Edwards, R. et al. (2006). Levels of Secondhand Smoke in Pubs and Bars by
Deprivation and Food-serving Status: A Cross-sectional Study from North West England. BMC Public Health, 6 (42).
Eisner, MD., Hammond, SK., Lactao, G. & Iribarren, C. (2005). Directly Measured
Secondhand Smoke Exposure and Asthma Health Outcomes. Thorax, 60, 814-821
Eisner, MD. Et al. (2006). Directly Measured Secondhand Smoke Exposure and COPD
Health Outcomes. BMC Pulmonary Medicine, 6 (12) Eisner, MD., BS Smith, KA. & Blanc, DP. (1998). Bartenders’ Respiratory Health after
Establishment of Smoke-free Bars and Taverns. JAMA, 280 (22), 1909-1914.
37
Framework Convention Alliance on Tobacco Control, 2005, Adapted and updated with permission from the 2000 World Conference on Tobacco OR Health fact sheets. Geneva, Switzerland.
Gu, D., et al. (2004). Cigarette Smoking and Exposure to Environmental Tobacco
Smoke in China: The International Collaborative Study of Cardiovascular Disease in Asia. American Journal of Public Health, 94 (11), 1972-1976.
Guindon, G.E. & Boisclair, D. (March, 2003). Past, Current and Future Trends in
Tobacco Use. World Bank. Available at URL: http://www1.worldbank.org/tobacco/publications.asp
Hecht, SS. (2006). Cigarette Smoking: Cancer Risks, Carcinogens, and Mechanisms.
Langenbecks Arch Surg. Ho Sai Yin et al, 2007, Cross-Sectional and Prospective Associations Between
Passive Smoking and Respiratory Symptoms at the Workplace, Ann Epidemiology 2007;17:126-131.
Jee, SH., Ohrr, H. & Kim, IS. (1999). Effects of Husbands’ Smoking on the Incidence
of Lung Cancer in Korean Women. In U.S. Department of Health and Human Services. (2006). The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
Kreuzer M, Krauss M, Kreienbrock L, Jöckel K-H, Wichmann H-E. Environmental
Tobacco Smoke and Lung Cancer: A Case-control Study in Germany. American Journal of Epidemiology 2000;151 (3):241–50.
Lannero, E., Pershagen, G., Wickman, M. & Nordvall, L. (2006). Maternal Smoking
During Pregnancy Increases the Risk of Recurrent Wheezing During the First Years of Life (BAMSE). Respiratory Research, BioMed Central, 7 (3).
Mark D. Eisner et al , Respiratory health of bar workers abbreviated, Medicine
University of California, San Francisco Ministry of Health, Lao PDR. , 2001, the tobacco control, Vientiane capital

38
Mackay, J. & Eriksen, M. (June, 2002). The Tobacco Atlas, Geneva: World Health organization. Available at URL: http://whqlibdoc.who.int/publications/2002/9241562099.pdf
Menzies et al. (2006). Respiratory Symptoms, Pulmonary Function, and Marker of
Inflammation Among Bar Workers Before and After a Legislation Ban on Smoking in Public Places. JAMA, 296 (14), 1742-1748.
Moshammer, H. et al. (2006). Parental Smoking and Lung Function in Children. Am J
Respir Crit Care Med, 173, 1255-1263. National Institute of Public Health. (2006). Health Status of the People in Lao PDR (as
part of the world health survey, supported by WHO). Vientiane: National Institute of Public Health, Ministry of Health of Lao PDR.
Nishino, Y., Tsubono, Y., Tsuji, I., Komatsu, S., Kanemura, S., Nakatsuka & al. (2001).
Passive Smoking at Home and Cancer Risk: A Population-based Prospective Study in Japanese Non-smoking Women. In U.S. Department of Health and Human Services. (2006). The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
National Institute of Public Health, Ministry of Health, Lao PDR. , 2003, Lao health
survey as part of the World Health Survey (WHS) in Lao PDR, Vientiane capital
Royal College of Physicians, (2005). Going Smoke-free: The Medical Case for Clean
Air in the Home, at Work and in Public Places. A report on passive smoking by the Tobacco Advisory Group of the Royal College of Physicians, July, 2005
Shafey, O., Dolwick, S. & Guindon, G.E. (2003). Tobacco control country profiles.
Second Edition, World Health Organization. Siegel, M., Barbeau, EM. & Osinubi, OY. (2005). The Impact of Tobacco Use and
Secondhand Smoke on Hospitality Workers. Clin Occup Environ Med, 5 (1), 31- 42.

39
Shafey, Dolwick & Guindon, 2003 University of Pittsburgh Medicine Center. (2006). COPD: Chronic Obstructive
Pulmonary Disease. Available at URL: http://patienteducation.upmc.com/Pdf/COPD.pdf
U.S. Department of Health and Human Services. (2006). The Health Consequences of
Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health.
World Health Organization. Tobacco Free Initiative. International Consultation on
Environmental Tobacco Smoke (ETS) and Child Health: Consultation Report. WHO. Technical Document Number WHO/TFI/99.10.1999
World Health Organization 2003, updated reprint 2004, 2005, WHO Framework
Convention on Tobacco Control, Geneva, Switzerland.

40
ANNEXES
A. Screening Form
ID: __ __ __ Q1. Have you ever smoked? 1. Yes
2. No Stop to Q2
Q2. Do you currently smoke any tobacco product such as cigarettes, cigars, or pipes?
1. Yes, daily 2. Yes, occasionally 3. No, not at all
Stop Stop to Q3
Q3. How long have you been working in this restaurant /office?
1. Less than one year 2. More than one year
Stop next
Asking for consent to participate in the study

41
B. Data Collection Tool
Questionnaire on Exposure to Second Hand Smoke (SHS) among Workers in the Restaurants
in Vientiane Capital and Luang Prabang Province, Lao PDR
WE ARE FROM THE MINISTRY OF HEALTH AND PROVINCIAL HEALTH DEPARTMENT. WE ARE WORKING ON A PROJECT CONCERN WITH SMOKING AND HEALTH. I WOULD LIKE TO TALK TO YOU ABOUT THIS. THE INTERVIEW WILL TAKE ABOUT 30 MINUTES. ALL THE INFORMATION WE OBTAINED WILL REMAIN STRICTLY CONFIDENTIAL AND YOUR ANSWERS WILL NEVER BE IDENTIFIED. DURING THIS TIME I WOULD LIKE TO SPEAK WITH YOU.
May I start now? IF PERMISSION IS GIVEN, BEGIN THE INTERVIEW. Note for enumerators: Fill in the answers in the blank or circle the suitable answers A. General Information Province:
Vientiane capital city…………………………01 Luangprabang …………………………………06
District: A. Vientiane capital city B. Luangprabang
A1. Sikhottabong................................. 01 A2. Chanthabury ................................-02 A3. Sisattanack.................................... 03 A4. Saisetha......................................... 04 B1. Luang Prabang.............................. 01
Q1. Interviewer name and number:
Name.................................. ___ ___
Q2. Supervisor name and number: Name_________________________ ___ ___ Q3. Day/Month/Year of interview: ___ ___ / ___ ___ / ___ ___ ___ ___ Q4. Result of interview:
Completed 1 Refused 2 Other (specify) 8
Q5. Data editor Name _______________________ ___ ___
Q6. Data entry clerk name and number: Name _______________________ ___ ___
B. Restaurant/Office information Q7. Name of Restaurant/Office :_________________________ Code ___ ___
Q8. Type of ventialtion:
1. Air conditioned enclosed Restaurants 2. Mixed enclosed/open air Restaurants 3. Open air Restaurants
Q9. Seating capacity ___ ___ ___ seats C. Respondent's Socio Demographic Characteristics I would like to start by asking you some background questions before asking you questions on
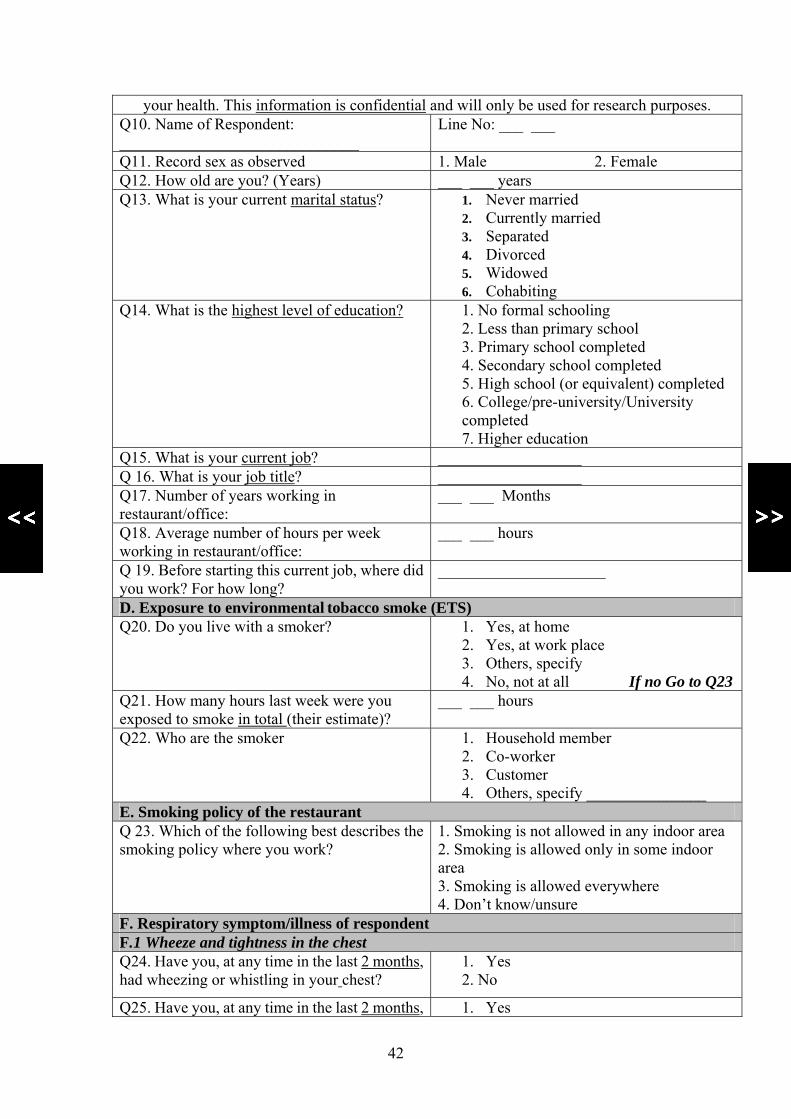
42
your health. This information is confidential and will only be used for research purposes. Q10. Name of Respondent: ______________________________
Line No: ___ ___
Q11. Record sex as observed 1. Male 2. Female Q12. How old are you? (Years) ___ ___ years Q13. What is your current marital status? 1. Never married
2. Currently married 3. Separated 4. Divorced 5. Widowed 6. Cohabiting
Q14. What is the highest level of education? 1. No formal schooling 2. Less than primary school 3. Primary school completed 4. Secondary school completed 5. High school (or equivalent) completed 6. College/pre-university/University completed 7. Higher education
Q15. What is your current job? __________________ Q 16. What is your job title? __________________ Q17. Number of years working in restaurant/office:
___ ___ Months
Q18. Average number of hours per week working in restaurant/office:
___ ___ hours
Q 19. Before starting this current job, where did you work? For how long?
_____________________
D. Exposure to environmental tobacco smoke (ETS) Q20. Do you live with a smoker? 1. Yes, at home
2. Yes, at work place 3. Others, specify 4. No, not at all If no Go to Q23
Q21. How many hours last week were you exposed to smoke in total (their estimate)?
___ ___ hours
Q22. Who are the smoker 1. Household member 2. Co-worker 3. Customer 4. Others, specify _______________
E. Smoking policy of the restaurant Q 23. Which of the following best describes the smoking policy where you work?
1. Smoking is not allowed in any indoor area 2. Smoking is allowed only in some indoor area 3. Smoking is allowed everywhere 4. Don’t know/unsure
F. Respiratory symptom/illness of respondent F.1 Wheeze and tightness in the chest Q24. Have you, at any time in the last 2 months, had wheezing or whistling in your chest?
1. Yes 2. No
Q25. Have you, at any time in the last 2 months, 1. Yes

43
woken up with a feeling of tightness in your chest first thing in the morning?
2. No
Q 26. Have these kinds of symptoms appeared before or is this the first time?
1. First time 2. Before
F.2 Shortness of breath Q27. Have you, at any time in the last 2 months, had an attack of shortness of breath that came on during the day when you were not doing anything strenuous?
1. Yes 2. No
Q28. Have you, at any time in the last 2 months, had an attack of shortness of breath that came on after you stopped exercising?
1. Yes 2. No
Q29. Have you, at any time in the last 2 months, been woken at night by an attack of shortness of breath?
1. Yes 2. No
Q 30. Have these kinds of symptoms appeared before or is this the first time?
1. First time 2. Before
F.3 Cough and phlegm from the chest Q31. Have you, at any time in the last 2 months, been woken at night by an attack of coughing?
1. Yes 2. No
Q32. Do you usually cough first thing in the morning? 1. Yes 2. No If no go to Q 35
Q32a. Do you have a cough like this most mornings for as much as 3 months per year?
1. Yes 2. No
Q32b. How many years have you had this cough? 1. Yes 2. No
Q33. Do you usually cough up phlegm from your chest first thing in the morning?
1. Yes 2. No If no go to Q 35
Q33a. Do you have phlegm like this most mornings for as much as 3 months per year?
1. Yes 2. No
Q33b. How many years have you had this phlegm? ___ ___ years Q 34. Have these kinds of symptoms appeared before or is this the first time?
1. First time 2. Before
F.4 Breathing Q 35. Which of the following statements best describes your breathing?
check only one: 1. I never or only rarely have trouble with
my breathing 2. I get repeated trouble with my
breathing but it always gets completely better
3. My breathing is never quite right F.5 Animals, dust, feathers
Q 36. When you are in a dusty part of the house or with animals (for example, dogs, cats or horses) or near feathers (including pillows and quilts) do you ever:
Q 36a. Get a feeling of tightness in your chest?
1. Yes 2. No
Q 36b. Start to feel short of breath? 1. Yes 2. No

44
F.6 Asthma Q37. Have you ever had asthma? 1. Yes
2. No
Q 37 a. How long has your asthma symptoms started?
_____ ____ months
Q38. Have you had an attack of asthma at any time in the last 2 months?
1. Yes 2. No
Q39. Are you currently taking any medicines (including inhalers, aerosols or tablets) for asthma?
1. Yes 2. No
40. 1. if having one of the above mentioned symptoms, ask the following questions 2. if do not have any of the above mentioned symptoms, end the interview by thanking the respondent for his/her cooperation and go back to Q4 at the first page to record the results of interview G. Tobacco related diseases management costs Q 41. For your last illness mentioned above,
where did you seek care 0. No care 1. Public hospital 2. Private clinic 3. Health center 4. Private pharmacy 5. Drug store 6. Traditional healer 7. Self medication 8. Others, specify_______________
Q 42. Thinking about your last visit to the health facilities for your last illness mentioned above, how much did you or your household pay? [Write 0 if the service was free. If respondent did not have tests or drugs, circle “not applicable, not have”]
A. Direct cost Q 42.1 Health care provider’s fees 8. DK
Q 42.2 Medicines 8. DK
Q 42. 3 Tests 8. DK B. Indirect cost Q 42.4 Transport 8. DK Q 42.5 Others (Food, lodging, etc.) 8. DK Q. 42.6 Income lost a) Salary b) others income per day
Q 43. Thinking about your last hospital stay for your last illness mentioned above, how much did you or your household pay? [Write 0 if the service was free. If respondent did not have tests or drugs, circle “not applicable, not have”]
A. Direct cost Q 43.1 Health care provider’s fees 8. DK

45
Q 43.2 Medicines Q 43. 3 Tests B. Indirect cost Q 44.4 Total costs for traveling to hospital and
back home ______________________
Q 44.5 Food costs ______________________ Q 44.6 Income loss for care provider a) Salary b) Other income
a) Salary _______________ b) Other income_________
Q 44.7 Income loss for patient a) Salary b) Other income
a) Salary _______________ b) Other income_________
Q 45. Health care cost paid by: a) Government/hospital _______________________
b) Insurance company _______________________ c) Pocket money _______________________
d) Others, please specify _______________________ Note for enumerator: End the interview by thanking the respondent for his/her cooperation and go back to Q4 at the first page to record the results of interview

46
C. The Research Study Team
Principal Investigator: Dr. Keonakhone Houamboun, NIOPH, MOH
Co-investigator: Dr. Sengchanh Kounnavong, NIOPH, MOH
Co-ordination: Dr. Maniphanh Vongphosy, ADRA Lao
Team members:
Data collectors in Vientiane capital city:
Dr. Manithong Vonglokham, NIOPH, MOH
Dr. Dalaphone Sithideth, NIOPH, MOH
Dr. Khouanchai Soundavong, NIOPH, MOH
Dr. Vilavanh Xayaseng, NIOPH, MOH
Data collectors in Luangprabang province:
Ms. Seng-aly Mr. Bounyai Mr. Somchit Ms. Phonevilay
Supervisor for Luangprabang team: Dr. Dalaphone Sithideht, NIOPH, MOH
Data entry clerk
Dr. Manithong Vonglokham, NIOPH, MOH
Dr. Dalaphone Sithideth, NIOPH, MOH
Dr. Khouanchai Soundavong, NIOPH, MOH
Dr. Vilavanh Xayaseng, NIOPH, MOH
Data management: Cleaning, processing and analysis
Dr. Sengchanh Kounnavong, NIOPH, MOH
Dr. Keonakhone Houamboun, NIOPH, MOH
Dr. Manithong Vonglokham, NIOPH, MOH
Report writing: Dr. Sengchanh Kounnavong, NIOPH, MOH

………………………………………………………………………………………………….. About SEATCA The Southeast Asia Tobacco Control Alliance (SEATCA) works closely with key partners in ASEAN member countries to generate local evidence through research programs, to enhance local capacity through advocacy fellowship program, and to be catalyst in policy development through regional forums and in-country networking. By adopting a regional policy advocacy mission, it has supported member countries to ratify and implement the WHO Framework Convention on Tobacco Control (FCTC) Contact persons: Ms. Bungon Ritthiphakdee: SEATCA Director Email: [email protected] Ms. Menchi G. Velasco: SEATCA Research Program Manager Email: [email protected]; [email protected] Southeast Asia Tobacco Control Alliance (SEATCA) Address: Thakolsuk Apartment Room 2B, 115 Thoddamri Rd., Nakornchaisri
Dusit, Bangkok 10300, THAILAND Tel./Fax: +662 241 0082
Website: http://www.seatca.org …………………………………………………………………………………………………..