document
TRANSCRIPT
THE HUMAN CHROMOSOME 22q11 region isprone to rearrangements that are as-
sociated with a wide spectrum of clinicalmanifestations1. One of the most com-mon syndromes associated with 22q11rearrangements is DiGeorge syndrome(DGS). DGS is characterized by malfor-mation of facial features, absence or hy-poplasia of the thymus and parathyroidglands, and a distinct set of heart defects.Most of these defects involve thecardiac outflow tract, with abnormalpatterning of the aortic arch arteries,improper alignment and septationof the two outflow vessels, and de-fects in septation of the ventricularchambers. Although many genesthat are included in the 22q11 re-gion have been identified, little isknown about their role in the devel-opment of the affected organs. Apaper by Lindsay et al. published inthe 23 September issue of Nature de-scribed the creation of a mousemodel possessing a homologouschromosomal deletion and cardio-vascular abnormalities similar tothose seen in DGS patients2.
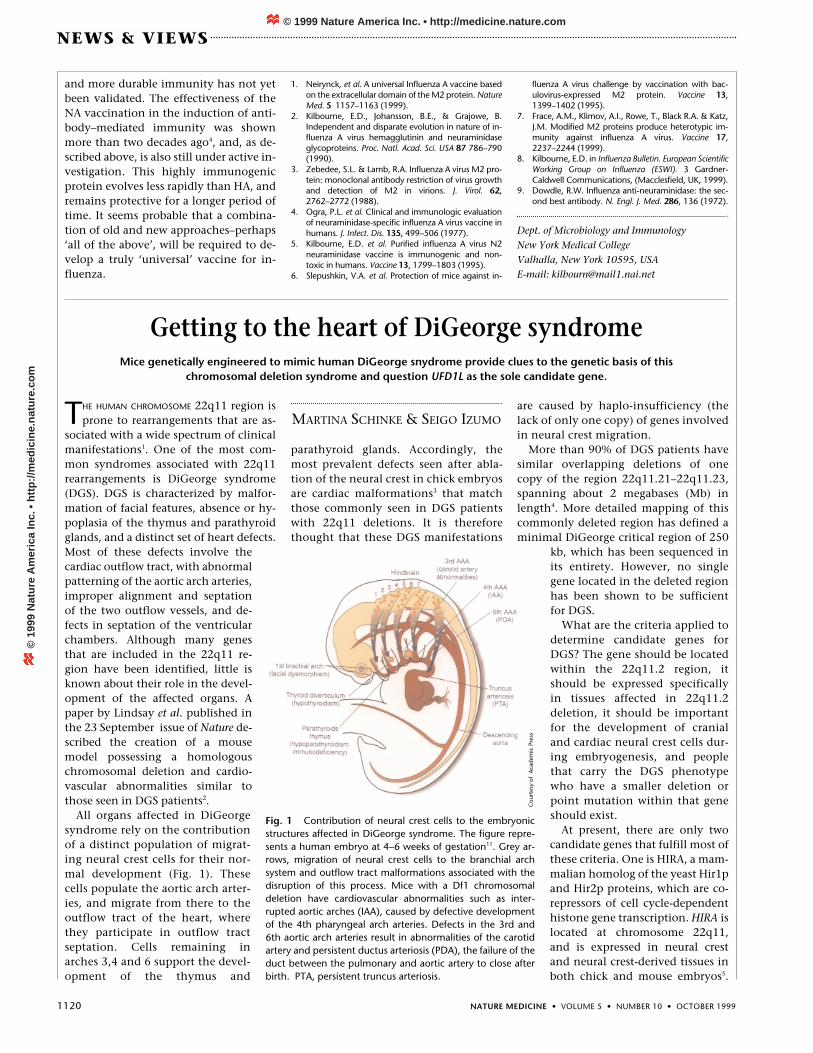
All organs affected in DiGeorgesyndrome rely on the contributionof a distinct population of migrat-ing neural crest cells for their nor-mal development (Fig. 1). Thesecells populate the aortic arch arter-ies, and migrate from there to theoutflow tract of the heart, wherethey participate in outflow tractseptation. Cells remaining inarches 3,4 and 6 support the devel-opment of the thymus and
parathyroid glands. Accordingly, themost prevalent defects seen after abla-tion of the neural crest in chick embryosare cardiac malformations3 that matchthose commonly seen in DGS patientswith 22q11 deletions. It is thereforethought that these DGS manifestations
are caused by haplo-insufficiency (thelack of only one copy) of genes involvedin neural crest migration.
More than 90% of DGS patients havesimilar overlapping deletions of onecopy of the region 22q11.21–22q11.23,spanning about 2 megabases (Mb) inlength4. More detailed mapping of thiscommonly deleted region has defined aminimal DiGeorge critical region of 250
kb, which has been sequenced inits entirety. However, no singlegene located in the deleted regionhas been shown to be sufficientfor DGS.
What are the criteria applied todetermine candidate genes forDGS? The gene should be locatedwithin the 22q11.2 region, itshould be expressed specificallyin tissues affected in 22q11.2deletion, it should be importantfor the development of cranialand cardiac neural crest cells dur-ing embryogenesis, and peoplethat carry the DGS phenotypewho have a smaller deletion orpoint mutation within that geneshould exist.
At present, there are only twocandidate genes that fulfill most ofthese criteria. One is HIRA, a mam-malian homolog of the yeast Hir1pand Hir2p proteins, which are co-repressors of cell cycle-dependenthistone gene transcription. HIRA islocated at chromosome 22q11,and is expressed in neural crestand neural crest-derived tissues inboth chick and mouse embryos5.
Getting to the heart of DiGeorge syndromeMice genetically engineered to mimic human DiGeorge snydrome provide clues to the genetic basis of this
chromosomal deletion syndrome and question UFD1L as the sole candidate gene.
MARTINA SCHINKE & SEIGO IZUMO
Fig. 1 Contribution of neural crest cells to the embryonicstructures affected in DiGeorge syndrome. The figure repre-sents a human embryo at 4–6 weeks of gestation11. Grey ar-rows, migration of neural crest cells to the branchial archsystem and outflow tract malformations associated with thedisruption of this process. Mice with a Df1 chromosomaldeletion have cardiovascular abnormalities such as inter-rupted aortic arches (IAA), caused by defective developmentof the 4th pharyngeal arch arteries. Defects in the 3rd and6th aortic arch arteries result in abnormalities of the carotidartery and persistent ductus arteriosis (PDA), the failure of theduct between the pulmonary and aortic artery to close afterbirth. PTA, persistent truncus arteriosis.
Cou
rtes
y of
Aca
dem
ic P
ress
1120 NATURE MEDICINE • VOLUME 5 • NUMBER 10 • OCTOBER 1999
NEWS & VIEWS
and more durable immunity has not yetbeen validated. The effectiveness of theNA vaccination in the induction of anti-body–mediated immunity was shownmore than two decades ago4, and, as de-scribed above, is also still under active in-vestigation. This highly immunogenicprotein evolves less rapidly than HA, andremains protective for a longer period oftime. It seems probable that a combina-tion of old and new approaches–perhaps‘all of the above’, will be required to de-velop a truly ‘universal’ vaccine for in-fluenza.
1. Neirynck, et al. A universal Influenza A vaccine basedon the extracellular domain of the M2 protein. NatureMed. 5 1157–1163 (1999).
2. Kilbourne, E.D., Johansson, B.E., & Grajowe, B.Independent and disparate evolution in nature of in-fluenza A virus hemagglutinin and neuraminidaseglycoproteins. Proc. Natl. Acad. Sci. USA 87 786–790(1990).
3. Zebedee, S.L. & Lamb, R.A. Influenza A virus M2 pro-tein: monoclonal antibody restriction of virus growthand detection of M2 in virions. J. Virol. 62,2762–2772 (1988).
4. Ogra, P.L. et al. Clinical and immunologic evaluationof neuraminidase-specific influenza A virus vaccine inhumans. J. Infect. Dis. 135, 499–506 (1977).
5. Kilbourne, E.D. et al. Purified influenza A virus N2neuraminidase vaccine is immunogenic and non-toxic in humans. Vaccine 13, 1799–1803 (1995).
6. Slepushkin, V.A. et al. Protection of mice against in-
fluenza A virus challenge by vaccination with bac-ulovirus-expressed M2 protein. Vaccine 13,1399–1402 (1995).
7. Frace, A.M., Klimov, A.I., Rowe, T., Black R.A. & Katz,J.M. Modified M2 proteins produce heterotypic im-munity against influenza A virus. Vaccine 17,2237–2244 (1999).
8. Kilbourne, E.D. in Influenza Bulletin. European ScientificWorking Group on Influenza (ESWI). 3 Gardner-Caldwell Communications, (Macclesfield, UK, 1999).
9. Dowdle, R.W. Influenza anti-neuraminidase: the sec-ond best antibody. N. Engl. J. Med. 286, 136 (1972).
Dept. of Microbiology and ImmunologyNew York Medical CollegeValhalla, New York 10595, USAE-mail: [email protected]
© 1999 Nature America Inc. • http://medicine.nature.com©
199
9 N
atu
re A
mer
ica
Inc.
• h
ttp
://m
edic
ine.
nat
ure
.co
m

NATURE MEDICINE • VOLUME 5 • NUMBER 10 • OCTOBER 1999 1121
NEWS & VIEWS
Its embryonic attenuation by antisenseoligonucleotides in chick cardiac neuralcrest cells results in an increased inci-dence of persistent truncus arteriosus(PTA), the failure of the truncus arterio-sus to divide into the aorta and pul-monary artery. However, disruption ofHIRA does not completely phenocopyneural crest ablation. In particular, itdoes not affect aortic arch patterning oroutflow tract alignment, both of whichare common features of DGS. Also, micehaplo-insufficient for Hira are apparentlynormal6, and no DGS patients with HIRAmutations have been discovered yet.
UFD1L, the homolog of a highly con-served yeast gene involved in the degra-dation of ubiquinated proteins, seems tobe an even more promising DGS candi-date gene. It was recently reported byYamagishi et al. that UFD1L haplo-insuf-ficiency causes the same congenital heartand craniofacial defects seen in 22q11deletion patients7, a finding that wasconsidered to be a major breakthroughin the hunt for the DGS gene. Indeed,UFD1L is expressed in all of the tissues af-fected in DGS patients, including thebranchial arches, palatal precursors, the
frontonasal region, telencephalon, andthe cardiac outflow tract. Yamagishi et al.also identified a DGS patient carrying amono-allelic deletion of exons 1 to 3 ofUFD1L and its neighboring geneCDC457, whose function is not yetknown. However, screens of DGS pa-tients without detectable deletion of22q11 reported no rearrangements ormutations of UFD1L, although some se-quence variants were observed8.
Lindsay et al.2 deleted a 1.2-Mb frag-ment (Df1) of mouse chromosome 16that is similar to the region deleted inhuman DGS patients in content and size,although it has a different genomic orga-nization9 (Fig. 2). The deleted Df1 regioncovers many of the genes commonlydeleted in DGS patients, includingUFD1L, but does not include others suchas HIRA (Fig. 2). Df1+/– mice have ahigher-than-normal incidence of neona-tal mortality, and Df1l homozygous nullmice were never recovered, indicative ofembryonic lethality. The heterozygousmice have cardiovascular defects, includ-ing aortic arch abnormalities caused bydefective development of the fourth pha-ryngeal arch arteries (Fig. 1)(ref. 2). Thesedo not cover the entire phenotypic spec-trum of DGS, as the third and sixth aorticarch arteries develop normally (Fig. 1),suggesting that at least two heart devel-opment-related loci lie within the 22q11region. However, it is also possible thatheterozygous mutations in the mouseare not sufficient to produce a pheno-type equivalent to humans. Also, thedeletion was created in a mixed geneticbackground, which might explain the30% penetrance of the phenotype.
Heart defects could be rescued bycrossbreeding heterozygous Df1 mutantmice with mice harboring a duplicatedDf1 segment on the complementarychromosome2. This finding proves thatgenes within the deleted segment, andnot neighboring genes, are responsiblefor the phenotype. Lindsay et al. alsoshowed that Ufd1 alone is not responsi-ble for the heart defects observed in het-erozygous Df1 deleted mice, since micespecifically haplo-insufficient for Ufd1are phenotypically normal. Homozygousdeletion of Ufd1 results in embryoniclethality before embryonic day 9.5, sothe Ufd1-dependent protein degradationpathway is important at very early stagesof development2. However, the pheno-type of Ufd1 mutant embryos has notbeen described yet, and the precise func-tion of Ufd1 remains to be discovered.
Lindsay’s findings indicate that addi-tional genes outside the region deleted inDf1+/– mice are necessary to produce thefull phenotype of DGS. These mice, how-ever, provide an interesting model foraortic arch artery malformation in DGS.
The incidence of 22q11 deletions hasbeen approximated to be 1 in 4,000 livebirths. The extreme phenotypic variabil-ity associated with 22q11 deletions andthe presence of non-overlapping deletionscausing DGS-related phenotypes10 suggestthat multiple genes and modifying factorsare associated with this disease. The chal-lenge remains to extract those genes thatcause DGS from the immense pool ofgenes contained within the various dele-tion regions. The potential for improveddiagnosis and perhaps even preventivetreatment of afflicted infants, many ofwhom must now undergo open heartsurgery or suffer from immunologic andendocrine disorders, makes the effort tosolve this puzzle worthwhile.
1. L. Edelmann, R.K. et al. A common molecularbasis for rearrangement disorders on chromo-some 22q11. Hum. Mol. Genet. 8: 1157–1167(1999).
2. Lindsay, E. A. et al. Congenital heart disease inmice deficient for the DiGeorge syndrome region.Nature 401 379-383.
3. M. L. Kirby & K. L. Waldo. Neural crest and car-diovascular patterning. Circ. Res. 77 211–215(1995).
4. Goldmuntz, E. et al. Frequency of 22q11 dele-tions in patients with conotruncal defects. J. Am.Coll. Cardiol. 32 492–498 (1998).
5. Farrell, M.J. et al. HIRA, a DiGeorge syndromecandidate gene, is required for cardiac outflowtract septation. Circ. Res. 84 127–135 (1999).
6. Scambler, P. et al. Hira, a gene from theDGS/VCFS region, is required for normal embryo-genesis. Am. J. Hum. Genet. 63 A7 (1998)
7. Yamagishi, H., Garg, V., Matsuoka, R., Thomas,T., & Srivastava, D. A molecular pathway reveal-ing a genetic basis for human cardiac and cranio-facial defects. Science 283 1158–1161 (1999).
8. Wadey, R. et al. Mutations of UFD1L Are not re-sponsible for the majority of cases of DiGeorgesyndrome/velocardiofacial syndrome withoutdeletions within chromosome 22q11. Am. J. Hum.Genet. 65 247–249 (1999).
9. Puech, A. et al. Comparative mapping of thehuman 22q11 chromosomal region and the or-thologous region in mice reveals complexchanges in gene organization. Proc. Natl. Acad.Sci. USA 94 14608–14613 (1997).
10. McQuade, L. et al. Patient with a 22q11.2 dele-tion with no overlap of the minimal DiGeorgesyndrome critical region (MDGCR). Am. J. Med.Genet. 86 27–33 (1999).
11. Emanuel, B.S., Budarf, M.L. and Scambler, P.J.The genetic basis of conotruncal defects: Thechromosome 22q11.2 deletion, in heartDevelopment 179–193 eds. R.P. Harvey and N.Rosenthal, Academic Press, 1999).
Cardiovascular DivisionBeth Israel Deaconess Medical CenterHarvard Medical School330 Brookline Ave.Boston, Massachusetts 02215, USAE-mail: [email protected]
Fig. 2 The human region on chromosome22q11 commonly deleted in DGS patients andthe orthologous region in mice on chromo-some 16 are very similar in gene content butshow a different genomic organization9.Recombination events that have possibly takenplace during evolution are indicated by lines.Some genes (boxed) are not present in the ho-mologous region of the other species. Verticalbracket, the Df1 region deleted in mice defi-cient for the DGS region.
Cou
rtes
y of
the
Nat
iona
l Aca
dem
y of
Sci
ence
s, U
SA.
© 1999 Nature America Inc. • http://medicine.nature.com©
199
9 N
atu
re A
mer
ica
Inc.
• h
ttp
://m
edic
ine.
nat
ure
.co
m