54-year-old woman with two decades of...
TRANSCRIPT

54-year-old woman fwith two decades of
pancytopenia
Heather Cheng, MD, PhDH t l F ll C fHematology Fellows Conference
November 12, 2010

History of Present IllnessHistory of Present Illnessyy Age 33 (1989): incidentally found to have pancytopenia
WBC 3 5K ANC k “HCT l” PLT 30 50K WBC 3.5K, ANC unknown, “HCT normal”, PLT 30-50K. bone marrow biopsies in 1989, 1998 reportedly “inconclusive”
Age 46 (2002): hospitalized for FUO Age 46 (2002): hospitalized for FUO g ( ) pg ( ) p WBC 1.3K, ANC 900, HCT 38%, MCV 111, PLT 15KWBC 1.3K, ANC 900, HCT 38%, MCV 111, PLT 15K Hypocellular marrow with 0Hypocellular marrow with 0--20% cellularity20% cellularity Cytogenetics not performed Cytogenetics not performed Trial of prednisone 60mg daily x 3 months tTrial of prednisone 60mg daily x 3 months tolerated very poorlyolerated very poorly Trial of prednisone 60mg daily x 3 months, tTrial of prednisone 60mg daily x 3 months, tolerated very poorlyolerated very poorly WBC 3.9K WBC 3.9K 6.2K, HCT 33% 6.2K, HCT 33% 38%, PLT 15K 38%, PLT 15K 27K27K
Age 54 (2002 to 2010)Age 54 (2002 to 2010) WBC 2.1WBC 2.1--2.9K, ANC 5402.9K, ANC 540--710, HCT 36%, MCV 107 710, HCT 36%, MCV 107 PLT: 20PLT: 2011K (when we saw her)11K (when we saw her)14K14K No major bleeding eventsNo major bleeding events No PLT transfusions (except for surgeries)No PLT transfusions (except for surgeries) No PLT transfusions (except for surgeries)No PLT transfusions (except for surgeries)

Additional HistoryAdditional HistoryAdditional HistoryAdditional History PAST MEDICAL PAST MEDICAL
HISTORYHISTORYHISTORYHISTORY Congenital hip Congenital hip
dysplasia dysplasia Numerous hipNumerous hipNumerous hip Numerous hip
surgeries: 1962, surgeries: 1962, 1990, 1995, two in 1990, 1995, two in 20072007
Fractured ankleFractured ankle Fractured ankle Fractured ankle repair in 1973repair in 1973
HyperlipidemiaHyperlipidemia OsteopeniaOsteopenia History of left History of left
retinal tearretinal tear Chronic left sided Chronic left sided
sinus congestionsinus congestionsinus congestion sinus congestion
Additional HistoryAdditional HistoryAdditional HistoryAdditional History PAST MEDICAL PAST MEDICAL
HISTORYHISTORY FAMILY HISTORYFAMILY HISTORY
2323 ldld SOCIAL HISTORYSOCIAL HISTORY
15 PY ki15 PY kiHISTORYHISTORY Congenital hip Congenital hip
dysplasia dysplasia Numerous hipNumerous hip
2323--yearyear--old son old son childhood leukocytosis childhood leukocytosis
that nearly prompted that nearly prompted workup of leukemia workup of leukemia
now leukopenic WBCnow leukopenic WBC
15 PY smoking15 PY smoking Exposed to Exposed to
benzene and benzene and other chemicalsother chemicals, , including ferricincluding ferricNumerous hip Numerous hip
surgeries: 1962, surgeries: 1962, 1990, 1995, two in 1990, 1995, two in 20072007
Fractured ankleFractured ankle
now leukopenic WBC now leukopenic WBC 2.7K, PLT 110K.2.7K, PLT 110K.
h/o testicular cancerh/o testicular cancer Father: Father:
colon cancer colon cancer
including ferric including ferric ammonium citrate ammonium citrate and potassium and potassium ferrocyanide.ferrocyanide.
Fractured ankle Fractured ankle repair in 1973repair in 1973
HyperlipidemiaHyperlipidemia OsteopeniaOsteopenia
nonnon--melanoma skin melanoma skin cancercancer
Mother: Mother: breast cancer, breast cancer,
History of left History of left retinal tearretinal tear
Chronic left sided Chronic left sided sinus congestionsinus congestion
h/o stroke.h/o stroke. One brother with MI, two One brother with MI, two
other siblings healthy other siblings healthy
sinus congestion sinus congestion

Physical ExamPhysical ExamPhysical ExamPhysical Exam VITALS: T36.5, BP 120/78, P68, R12, 75.9kg, 169.5cmVITALS: T36.5, BP 120/78, P68, R12, 75.9kg, 169.5cm GEN: wellGEN: well--developed, welldeveloped, well--nourished woman nourished woman HEENT: PERRL, sclera anicteric, no palatal or subungual HEENT: PERRL, sclera anicteric, no palatal or subungual
petechiae, petechiae, no cleft lip or palate, no oral leukoplakiano cleft lip or palate, no oral leukoplakia NECK: supple, NECK: supple, not shortenednot shortened LUNGS: occasional wheeze in left lower lung field, otherwise LUNGS: occasional wheeze in left lower lung field, otherwise
clearclearCV RRR / /CV RRR / / CV: RRR, no m/r/gCV: RRR, no m/r/g
ABD: soft, nontender, ABD: soft, nontender, no hepatosplenomegalyno hepatosplenomegaly EXT: no clubbing/cyanosis, EXT: no clubbing/cyanosis, no nail, thumb or limb deformitiesno nail, thumb or limb deformities SKIN: SKIN: scattered petechiae, several spider angiomas in scattered petechiae, several spider angiomas in
suprasternal area, no other obvious rashsuprasternal area, no other obvious rash NEURO: CN2NEURO: CN2--12 intact, AOx4, asymmetric gait d/t R hip pain12 intact, AOx4, asymmetric gait d/t R hip pain

BONE MARROW FAILURE:BONE MARROW FAILURE:it l i d?it l i d?congenital or acquired?congenital or acquired?
5454 yearyear old woman > 20 years of pancytopeniaold woman > 20 years of pancytopenia 5454--yearyear--old woman > 20 years of pancytopeniaold woman > 20 years of pancytopenia VERY indolent courseVERY indolent course No documented normal counts No documented normal counts
CONGENITALCONGENITAL Fanconi anemiaFanconi anemia
Intriguing family historyIntriguing family history Chemical exposureChemical exposure
Fanconi anemiaFanconi anemia Dyskeratosis congenitaDyskeratosis congenita
ACQUIREDACQUIRED Idiopathic aplastic anemiaIdiopathic aplastic anemia Myelodysplastic syndromeMyelodysplastic syndrome Paroxysmal nocturnal Paroxysmal nocturnal
hemoglobinuriahemoglobinuria

Bone Marrow StudiesBone Marrow Studies
Hypocellular with Hypocellular with maturing trilineage maturing trilineage g gg ghematopoesis: 10hematopoesis: 10--20% 20% cellularitycellularity
No abnormal myeloid orNo abnormal myeloid or No abnormal myeloid or No abnormal myeloid or lymphoid populations lymphoid populations by flow cytometryby flow cytometry
No GPINo GPI--deficient deficient erythroid or myeloid erythroid or myeloid populations by flowpopulations by flow
Cytogenetics: 46, XX Cytogenetics: 46, XX [20], normal female [20], normal female karyotypekaryotype
Photos of bone marrow studies of 8/19/10 courtesy of Dr. Sandra BohlingPhotos of bone marrow studies of 8/19/10 courtesy of Dr. Sandra Bohling

BONE MARROW FAILURE:BONE MARROW FAILURE:it l i d?it l i d?congenital or acquired?congenital or acquired?
5454 yearyear old woman > 20 years of pancytopeniaold woman > 20 years of pancytopenia 5454--yearyear--old woman > 20 years of pancytopeniaold woman > 20 years of pancytopenia VERY indolent courseVERY indolent course No documented normal counts No documented normal counts
CONGENITALCONGENITAL Fanconi anemiaFanconi anemia
Intriguing family historyIntriguing family history Chemical exposureChemical exposure
Fanconi anemiaFanconi anemia Dyskeratosis congenitaDyskeratosis congenita
ACQUIREDACQUIRED Idiopathic aplastic anemiaIdiopathic aplastic anemia Myelodysplastic syndromeMyelodysplastic syndrome Paroxysmal nocturnal Paroxysmal nocturnal
hemoglobinuriahemoglobinuria

Congenital Marrow Failure Syndromes Congenital Marrow Failure Syndromes (that can present after age 15)(that can present after age 15)
SyndromeSyndrome Median Median age dx age dx (yrs)(yrs)
% dx % dx >15yo>15yo
NonNon--heme featuresheme features Heme/OncHeme/Onc Screening testScreening test geneticsgenetics
Fanconi Fanconi 6.66.6 99 Skin Skin Pancytopenia, Pancytopenia, Chromosomal Chromosomal Autosomal/Autosomal/anemiaanemia hyperpigmentation, hyperpigmentation,
café au lait spotscafé au lait spots
y p ,y p ,hypocellular hypocellular marrow, marrow, MDS, MDS, leukemia, solid leukemia, solid tumorstumors
breakage in breakage in cells cultured cells cultured with DNA with DNA crosslinkerscrosslinkers
XX--linked linked recessive ~13 recessive ~13 FANC genesFANC genes
D k t iD k t i 1515 4646 D k t ti ilD k t ti il P t iP t i T lT l DKC1 NHP2DKC1 NHP2Dyskeratosis Dyskeratosis congenitacongenita
1515 4646 Dyskeratotic nails, Dyskeratotic nails, lacy reticular rash, lacy reticular rash, oral leukoplakia, oral leukoplakia, pulm fibrosis, early pulm fibrosis, early gray hair, gray hair, osteoporosisosteoporosis
Pancytopenia, Pancytopenia, hypocellular hypocellular marrow, marrow, MDS, MDS, leukemia, solid leukemia, solid tumors tumors (head/neck)(head/neck)
Telomere Telomere length assaylength assay
DKC1, NHP2, DKC1, NHP2, NOP10, NOP10, TERC, TERT, TERC, TERT, TINF2TINF2(**in most pts (**in most pts mutation not yetmutation not yetosteoporosisosteoporosis (head/neck)(head/neck) mutation not yet mutation not yet identified)identified)
DiamondDiamond--Blackfan anemiaBlackfan anemia
0.250.25 11 Short stature, abn thumbs, Short stature, abn thumbs, hypertelorism, cleft lip/palatehypertelorism, cleft lip/palate
Macrocytic anemia, Macrocytic anemia, erythroid hypoplasia, erythroid hypoplasia, MDS, leukemiaMDS, leukemia
Elevated RBC Elevated RBC adenosine adenosine deaminasedeaminase
Autosomal Autosomal dominant dominant Mutations in >9 Mutations in >9 ribosomal prot in ribosomal prot in 50% of pts50% of pts50% of pts50% of pts
ShwachmanShwachman--Diamond Diamond syndromesyndrome
11 55 Short stature, exocrine Short stature, exocrine pancreas insufficiencypancreas insufficiency
Neutropenia, anemia, Neutropenia, anemia, MDS, leukemiaMDS, leukemia
Decreased serum Decreased serum trypsinogen and trypsinogen and pancreatic pancreatic isoamylaseisoamylase
Autosomal Autosomal recessive SBDSrecessive SBDS
Severe Severe congenital congenital neutropenianeutropenia
33 1313 nonenone NeutropeniaNeutropenia BM for BM for promyelocyte promyelocyte arrestarrest
Autosomal Autosomal recessive HAX1 recessive HAX1 or dominant ELA2or dominant ELA2
Modified from table 15Modified from table 15--1, ASH1, ASH--SAP: marrow failure syndromesSAP: marrow failure syndromes

Physical Exam features of Physical Exam features of F i A iF i A iFanconi AnemiaFanconi Anemia
short statureshort stature microcephaly microcephaly p yp y Café Au Lait Café Au Lait
spotsspots gonadal gonadal
abnormalitiesabnormalities malformationsmalformations malformations malformations
of thumb and of thumb and kidneykidneyyy
Fig.Fig. 2 from Shimamura and Alter 2010.2 from Shimamura and Alter 2010. Consent for publication obtainedConsent for publication obtained

Fanconi AnemiaFanconi AnemiaFanconi AnemiaFanconi Anemia Most common inherited bone marrow failure syndromeMost common inherited bone marrow failure syndrome
Hypersensitivity to DNA damaging and crossHypersensitivity to DNA damaging and cross--linking agentslinking agents Diepoxybutane (DEB)Diepoxybutane (DEB) mitomycin C (MMC)mitomycin C (MMC) mitomycin C (MMC) mitomycin C (MMC) ionizing radiationionizing radiation
Multigenic disorder with 13 genesMultigenic disorder with 13 genesg gg g
FA genes coordinate DNA repair, stress signaling, appropriate FA genes coordinate DNA repair, stress signaling, appropriate apoptosis, apoptosis,
FANCD1 BRCA2FANCD1 BRCA2 e.g. FANCD1=BRCA2e.g. FANCD1=BRCA2
Progressive aplastic anemia in Fanconi anemia results from loss of Progressive aplastic anemia in Fanconi anemia results from loss of hematopoietic stem cellshematopoietic stem cellshematopoietic stem cells hematopoietic stem cells
cumulative DNA damagecumulative DNA damage

Diagnostic Considerations:Diagnostic Considerations:Fanconi AnemiaFanconi Anemia
Fanconi Screen Fanconi Screen test lymphocytes for test lymphocytes for
chromosomal breakage with chromosomal breakage with DEB or MMC)DEB or MMC) SCCA Cytogenetics or OHSUSCCA Cytogenetics or OHSU
Diagnosis in females may be Diagnosis in females may be complicated by complicated by somatic mosaicism: genetic reversiongenetic reversionmosaicism: genetic reversion genetic reversion to wildtypeto wildtype skin punch biopsy to test skin punch biopsy to test
cultured skin fibroblasts (send cultured skin fibroblasts (send Fanconi screen, chromosome breakageFanconi screen, chromosome breakage((out test to Dana Farber) out test to Dana Farber)
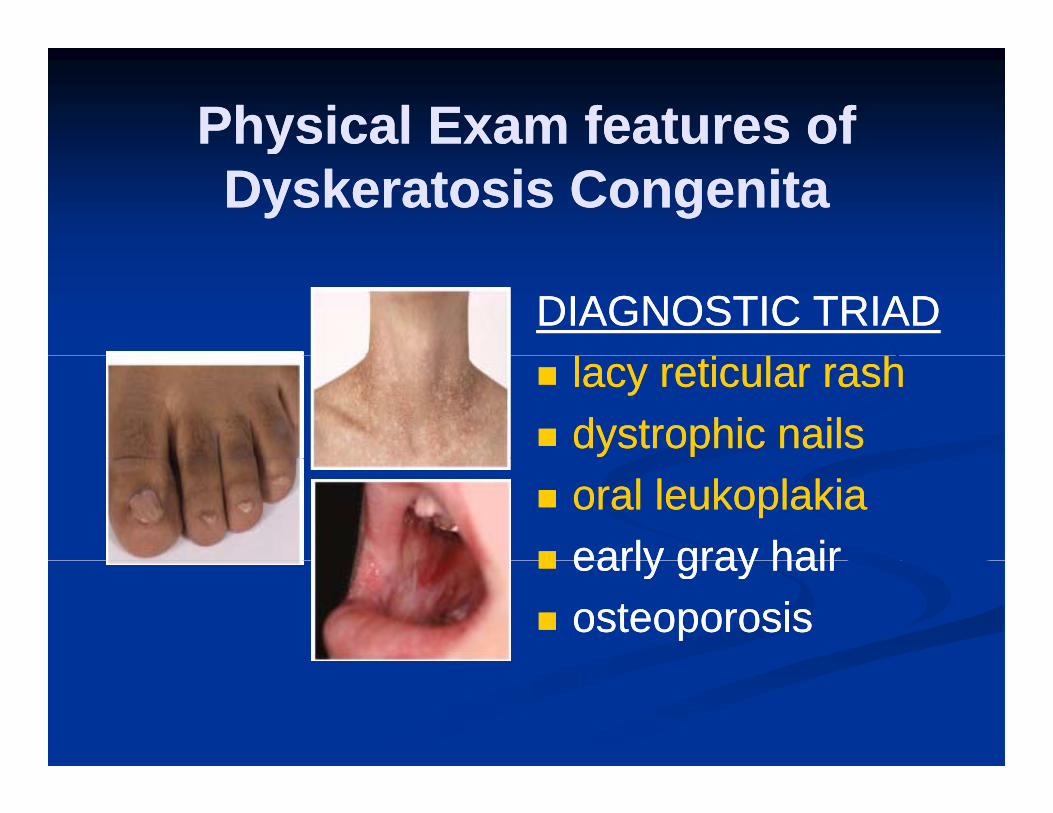
Physical Exam features of Physical Exam features of yyDyskeratosis CongenitaDyskeratosis Congenita
DIAGNOSTIC TRIADDIAGNOSTIC TRIAD lacy reticular rashlacy reticular rash dystrophic nailsdystrophic nails oral leukoplakiaoral leukoplakia early gray hairearly gray hair early gray hairearly gray hair osteoporosisosteoporosis

Telomeres, structure ,and the telomerase complex
Calado, R. T. Hematology 2009;2009:338-343

Diagnostic Considerations:Diagnostic Considerations:Dyskeratosis CongenitaDyskeratosis Congenita
FlowFlow--FISH: fluorescence probe FISH: fluorescence probe to telomere repeat sequence to telomere repeat sequence (CCCTAA) followed by flow(CCCTAA) followed by flow(CCCTAA), followed by flow (CCCTAA), followed by flow cytometry to quantify telomere cytometry to quantify telomere length length
S dS d t t R tt t R t SendSend--out to Repeat out to Repeat Diagnostics in Vancouver, BCDiagnostics in Vancouver, BCwww.repeatdiagnostics.comwww.repeatdiagnostics.com Basic procedureBasic procedureBasic procedureBasic procedure Detailed procedure Detailed procedure (includes (includes
BB--cells, Tcells, T--cells, NK cells)cells, NK cells)

Telomere length is shorter in dyskeratosis congenitag y g
Very short telomeresVery short telomeresare seen in DCare seen in DC
h in
kb Very short telomeresVery short telomeres
are seen in leukocyte are seen in leukocyte subsetssubsets
omer
e le
ngth
90th99th
subsetssubsets
Diagnostic sensitivity Diagnostic sensitivity and specificity of and specificity of very very short telomeresshort telomeres is >is >
Telo 90th
50th10th “short”1st “very short”
short telomeresshort telomeres is > is > 90% in leukocyte 90% in leukocyte subsets: lymphocytes, subsets: lymphocytes, naïve T cells, B cells.naïve T cells, B cells.
1st very short
(Percentiles of 400 nl controls)
Alter, B. P. et al. Blood 2007;110:1439-1447


Phenotype (including age of onset) Phenotype (including age of onset) varies with mutations in telomerase complex genesvaries with mutations in telomerase complex genesvaries with mutations in telomerase complex genes varies with mutations in telomerase complex genes
APLASTIC ANEMIA APLASTIC ANEMIA (a subset of “acquired AA”)(a subset of “acquired AA”)
DYSKERATOSIS DYSKERATOSIS CONGENITA CONGENITA (classically pediatric onset)(classically pediatric onset)
pulmonary fibrosispulmonary fibrosisl hil hi polymorphismspolymorphisms
Calado and Young, Calado and Young, Blood. 2008 May 1; 111(9): 4446Blood. 2008 May 1; 111(9): 4446––4455.4455.

Correctly identifying Correctly identifying inherited bone marrow failure syndromesinherited bone marrow failure syndromesinherited bone marrow failure syndromes inherited bone marrow failure syndromes
is imperativeis imperative
Impacts on medical management: Impacts on medical management: androgens vs immunosuppression vs transplantandrogens vs immunosuppression vs transplant
Impacts choice of stem cell donors and Impacts choice of stem cell donors and conditioning regimens for transplantconditioning regimens for transplantconditioning regimens for transplantconditioning regimens for transplant
Increased risk of other malignanciesIncreased risk of other malignancies need for increased surveillance need for increased surveillance
Genetic counselingGenetic counseling Genetic counselingGenetic counseling

Increased Risk of other MalignanciesIncreased Risk of other Malignancies(11(11--fold increase based on SEER data)fold increase based on SEER data)(11(11 fold increase based on SEER data)fold increase based on SEER data)
FANCONI ANEMIA Aplastic Anemia 50%L k i (AML) 25%
DYSKERATOSIS CONGENITALeukemia (AML) MDS (50% 7)Leukemia (AML) 25%
Solid tumors 10%Head and neckEsophagusLiver
MDS (50% monosomy 7)Head and neckEsophagusNasopharynxStomachLiver
VulvaCervixOsteosarcomaSoft tissue sarcoma
StomachAnorectalPancreas**pulmonary fibrosis**
Brain
-1. Annual bone marrow aspirates with cytogenetics2 Annual surveillance for solid tumors including oral exam and-2. Annual surveillance for solid tumors, including oral exam and nasolaryngoscopy -3. Annual gynecologic or anal exams-4. Consider HPV vaccination-4. Consider HPV vaccination-5. (for DC) Annual PFTs

Back to our patient…Back to our patient…Back to our patient…Back to our patient… Fanconi Anemia screenFanconi Anemia screen Fanconi Anemia screenFanconi Anemia screen
Peripheral blood testing: negativePeripheral blood testing: negative Skin fibroblast testing: negativeSkin fibroblast testing: negativeg gg g
Dyskeratosis congenita:Dyskeratosis congenita: Telomere testingTelomere testing “short” telomeres“short” telomeres
We did not definitively identify an IBMFS. We did not definitively identify an IBMFS. Therefore, we recommended treatment with ATG + cyclosporine, Therefore, we recommended treatment with ATG + cyclosporine, but patient prefers watchful waitingbut patient prefers watchful waitingp p gp p g

ConclusionsConclusions When considering a diagnosis of aplastic anemia, ALSO CONSIDER When considering a diagnosis of aplastic anemia, ALSO CONSIDER
the possibility of IBMFS, esp if family history, physical exam findings, the possibility of IBMFS, esp if family history, physical exam findings, t tit tietc are suggestive.etc are suggestive.
Fanconi anemia: compromised DNA repair/stress responseFanconi anemia: compromised DNA repair/stress response CaféCafé--auau--lait spots, short stature, thumb abnormalitieslait spots, short stature, thumb abnormalitiesp , ,p , , Lymphocyte chromosome fragility test with DEB/MMC (OHSU)Lymphocyte chromosome fragility test with DEB/MMC (OHSU) Consider somatic mosaicism and sending for skin fibroblast Consider somatic mosaicism and sending for skin fibroblast
testing (Dana Farber)testing (Dana Farber)
Dyskeratosis congenita: inappropriate telomere shorteningDyskeratosis congenita: inappropriate telomere shortening Abnormal nails, reticular skin rash, oral leukoplakiaAbnormal nails, reticular skin rash, oral leukoplakia FlowFlow--FISH to evaluate for very short telomeres (Vancouver, BC)FISH to evaluate for very short telomeres (Vancouver, BC)
Correct diagnosis has major implications for patient careCorrect diagnosis has major implications for patient care Treatment options, including transplant conditioningTreatment options, including transplant conditioning Surveillance for other malignanciesSurveillance for other malignanciesSurveillance for other malignanciesSurveillance for other malignancies Genetic counselingGenetic counseling

ReferencesReferencesReferencesReferences Alter, BP et al. (2007) Very short telomere length by Alter, BP et al. (2007) Very short telomere length by , ( ) y g y, ( ) y g y
flow fluorescence in situ hybridization identifies flow fluorescence in situ hybridization identifies patients with dyskeratosis congenita. Blood 110: patients with dyskeratosis congenita. Blood 110: 14391439--1447.1447.
Calado RT and NS Young (2008) TelomereCalado RT and NS Young (2008) Telomere Calado, RT and NS Young, (2008) Telomere Calado, RT and NS Young, (2008) Telomere maintenance and human bone marrow failure. Blood maintenance and human bone marrow failure. Blood 111: 4446111: 4446--44554455
Calado, RT and NS Young, (2009) Telomere Calado, RT and NS Young, (2009) Telomere , g, ( ), g, ( )Diseases. NEJM 361: 2353Diseases. NEJM 361: 2353--65. 65.
Maciejewski, JP and DP Steensma (2010) Marrow Maciejewski, JP and DP Steensma (2010) Marrow Failure Syndromes. ASHFailure Syndromes. ASH--SAP 2010.SAP 2010.
Shimamura, A and BP Alter (2010) Pathophysiology Shimamura, A and BP Alter (2010) Pathophysiology and management of inherited bone marrow failure and management of inherited bone marrow failure syndromes. Blood Reviews (24): 101syndromes. Blood Reviews (24): 101--122. 122.