5.3a highland alcohol and drugs partnership
TRANSCRIPT

Highland NHS Board4 February 2014
Item 5.3(a)
HIGHLAND ALCOHOL & DRUGS PARTNERSHIP
Report by Debbie Stewart, Coordinator on behalf of Margaret Somerville, Director ofPublic Health and HADP Chair
The Board is asked to:
Note and approve the update on the HADP Strategy 2012 – 2015. Note and approve the update on the HADP Actions 2012 – 2015. Continue to support implementation of the HADP Strategy and Action Plan across
NHS Highland and partner agencies.
1 Background and Summary
The purpose of HADP is to work in partnership to reduce drug and alcohol related harm.Since 2012 HADP has been delivering the current three year strategy in line with nationalpriorities in order to achieve the following strategic objectives:
RecoveryAn effective integrated care pathway offering a flexible range of services from assessment torecovery is in place
Maximising HealthHealth is maximised and communities feel engaged and empowered to make healthierchoices regarding alcohol and drugs
Protecting CommunitiesIndividuals and communities are protected against substance misuse harm
Children & FamiliesChildren affected by parental substance misuse are protected and build resilience throughthe joint working of adult and children’s services
Key ActionsThe table below summarises key actions related to each strategic priority:
Recovery – Key Actions Maximising Health – Key ActionsRecovery PathwayDrunk & Incapable ProvisionPreventing OverdoseWorkforce DevelopmentPerformance Management FrameworkPeer Support InitiativesThird Sector EngagementService User, Carer, Family Support
Communication InitiativesDiversionary ActivitiesHealth improvement InitiativesWhole Population ApproachesSchools Substance Misuse Prevention
Protecting Communities – Key Actions Children & Families – Key ActionsInput Enforcement ActivityScottish Police Alcohol StrategyLinks to Licensing ForumCommunity Safety- Prison Work- Persistent Offenders
Joint Framework- Hidden Harm/GOPR- Joint Training- Women Pregnancy & SM Guidance
Family Support Interventions

2
Performance ManagementHADP performance is measured against a set of national indicators (Appendix 1) with anannual report submitted to Scottish Government requiring self assessment of progress usinga commissioning cycle format. http://www.highland-adp.org.uk/library.asp
Strategic DirectionIn 2013 HADP was advised that the next stage of delivery of the national drugs strategy, theRoad to Recovery would require development of an Alcohol and Drug Quality ImprovementFramework in line with the four pillars of the Scottish Government’s approach to publicservice reform. This will ensure quality in the provision of care, treatment and recoveryservices and quality in the data that will evidence the medium and long term outcomes ofpeople in recovery.
It is envisaged that the alcohol and drug quality improvement framework will lead to HADPcommissioning services based on evidence of meeting principles of care. These will bemeasured by a range of tools including some quality indicators of recovery on the proposedsingle integrated drug and alcohol information system i.e. DAISy). It will contain a set of‘principles’ or expectations to benefit service users and their families and will be supportedwith guidance for HADP as a commissioner of services. The 2013/14 annual report sets outimprovement goals for HADP and measures for delivering these that reflect Ministerialpriorities (Appendix 2).
2 Progress Update on Current Strategy
RecoveryServices have worked extremely hard to deliver improvements in waiting times. However atSept 2013, 77.4% of people accessed treatment within 3 weeks against a national standardof 90%, although 93.9% of people did achieve access within 5 weeks. Provisional data forOct – Dec 2013 suggests the likelihood of significant progress toward achieving thestandard. Services are under going a DCAQ process that will address capacity issues andare devising an Improvement Plan that will be shared with government. A single point ofreferral has been piloted, reviewed and is now established in Inverness, resulting in greaterconsistency and faster access to treatment.
NHS Highland distributes more naloxone kits than other boards and is the first area inScotland to pilot administration of intranasal naloxone as an additional option to theintramuscular route. Training and procedures have been adapted to accommodate peoplewishing to choose the intra-nasal option and early indications suggest that thoseapprehensive about injecting may be encouraged to administer naloxone intra-nasally. Theinitiative is being evaluated with the support of public health.
Over the festive period, an overdose prevention campaign was mounted. HADP ran a seriesof awareness raising adverts via Moray Firth Radio and distributed a range of materials andleaflets via Harm Reduction and other services and worked in partnership with ScottishPolice and street pastor’s to improve the safety of party goers.
HADP are working in partnership with SMART Recovery to develop a network of mutual aidsupport groups with groups currently being established with support from; Osprey House,APEX, Beechwood House, Cale House, Criminal Justice Services and Porterfield Prison.
Workforce development has been supported through delivery of a diverse range of training inpartnership with STRADA, SDF and Crew 2000. A public protection training needs analysiswill shortly be piloted before being rolled out across services to inform development of atraining strategy.

3
Maximising HealthProgress on embedding alcohol brief interventions, has involved meeting and supersedinggovernment targets. To support roll out in wider settings materials on delivering briefinterventions to underage drinkers have been developed with partners in Action for Childrenroutinely applying the approach in street-work settings. Their experience has contributed toa national evaluation that will help strengthen the evidence base for delivery in widersettings.
HADP has provided funding to establish a prevention toolbox aimed at ensuring a moreconsistent approach to multi-agency substance misuse inputs to high school pupils. A socialmarketing initiative is underway to develop effective ways of communicating with youngpeople and their families in order to tackle underage drinking. Partners in Scottish Policeand the Youth Action service are involved in providing a range of diversionary activities withan increased number of schools participating in Rock Challenge and the majority of primaryseven pupils attending the annual Safer Highland event. Joint work was also undertakenover the festive period with the Youth Action Service and Action for Children to target schoolsfor substance misuse prevention.
A report on alcohol overprovision in Highland was produced and successfully influenced thelicensing board’s revision of their policy statement to place restrictions on the development oflarger scale off licenses.
Legal Highs or New Psychoactive Substances (NPS) have presented a number ofchallenges. In response, HADP have produced a briefing for schools with advice to parents,worked in partnership with Crew 2000 to provide training, organised a master-class forworkers, and facilitated Facebook chats that reached extensive audiences. The SafeNessgroup raised awareness with festival goers via the media and will continue to lobby festivalorganisers to discourage the sale of NPS’s. A scoping exercise is being initiated and willinvolve surveying the public and service providers to establish baseline data on prevalenceand trends to inform an Improvement Plan and develop more responsive support options.
Protecting CommunitiesHADP works closely with Scottish Police on an ongoing basis to support enforcementactivity. A number of local drug and alcohol forums have been involved in delivering jointinitiatives aimed at tackling underage drinking and anti-social behaviour including local testpurchasing and operation round up initiatives. Police Scotland and partners are involved indelivery of a range of diversionary and street-work interventions The Scottish Governmentannual report on drug seizures credited the Northern Constabulary area of Scottish Police fora significant increase in national ecstasy seizures.
HADP along with other Safer Highland partners contributed to a joint community safetyneeds assessment in order to inform future priorities and indicators for measuring progress.In addition, community safety partners have collaborated to roll out a programme of publicprotection training on cross cutting issues to multi-agency groups and the armed forces.
There has been a redesign of the Criminal Justice substance misuse service. The serviceoffers groups and 1-1 work for those subject to statutory requirements that have addictionissues. Progress on prison drug and alcohol work has also involved support to criminaljustice services to develop alcohol related work with offenders. The model of treatment inHMP Inverness has been reviewed with assessment procedures streamlined and moreproactive referral to community based services for those on short remand.
Children and FamiliesHADP works closely with the CPC on an ongoing basis with representation on each othersdelivery structures. HADP produced a profile collating a broad range of data relating tochildren and young people affected by drugs and alcohol to provide a platform forstrengthening the collection and sharing of information on this particularly vulnerable group.

4
The profile included findings from an audit of the child protection register that showedparental drug and alcohol misuse was a concern in the majority of cases.
The Women, Substance Misuse and Pregnancy Good Practice guidelines have beenupdated and ratified and FASD Awareness Days have been delivered. Bespoke trainingcommissioned by Scottish Government on the diagnosis and management of FASD hasbeen taken up in Highland and will contribute to addressing the need for a consistentdiagnostic and management process.
A CAPSM Improvement Group has been formed and an Improvement Plan is underdevelopment. A revised two day Getting Our Priorities Right training programme is beingrolled out to adult and children’s services and the participant resource and information packhas been updated. Electronic evaluations evidence the training is being well received. Morein-depth evaluation is planned to analyse the influence of the training on practice.
Youth Action Team and Action for Children staff have been trained to deliver “Dealing withTeenage Behaviour” programmes to parents. These will be rolled out as a universalprovision accessible to any parent of teenagers. A delivery model is under developmentusing feedback from parents and schools following some earlier pilot programmes.
Strategy DevelopmentWork will begin in 2014 to conduct an up to date needs assessment and consult withstakeholders, service users and their families in order to inform development of the HADPstrategy post 2015. In line with government priorities the direction of travel is likely toemphasise; a shift in emphasis towards prevention, greater integration of services at a locallevel, improved collaboration to develop recovery orientated systems of care, enhancedworkforce development and improved performance management through greatertransparency and accountability.
3 Contribution to Board Objectives
The strategy and action plan contributes to; 1, 2, 3, 4, 5, 6, 7, 8, 9, 10.
4 Governance Implications
Staff Governance – Workforce Development is a key delivery outcome of thestrategy. Informed by a competency based training needs analysis, targetedprovision of blended learning opportunities will aim to strengthen the drug and alcoholknowledge and skills of generic through to specialist staff.
Patient and Public Involvement – Strategic priorities and key actions reflectoutcomes from strategy consultation events and stakeholder engagement activities.More formal mechanisms for involvement in service design and policy developmentare a local delivery outcome of the strategy and are currently being developed.
Clinical Governance – Review of current services and development of an outcomesbased integrated recovery pathway is a key delivery outcome of the strategy.Establishing a clear pathway will enhance the quality and safety of treatment andensure services are delivered to a high standard. Development of a PerformanceOutcome Management Framework will provide mechanisms for measuring patientprogress toward recovery that will be utilised to continually improve the quality ofservice delivery.

5
Financial Impact – The main financial impact would be from not implementing the strategyand action plan. Research suggests a financial cost of £61,000 per individual misusingdrugs in Scotland in 2009. This figure includes the cost to the NHS, local authority, criminaljustice, courts, and victims of crime. The estimated cost to Highland is estimated annually at£51 - £62 million.
In 2010 the Scottish government produced ‘The Societal Cost of Alcohol Misuse in Scotlandfor 2007’ which estimated a central cost of £3.6bn. This national methodology has beenapplied to local data to provide estimates of the cost of alcohol-related harm at a HADP arealevel. The overall annual cost is estimated to be £84.85m (Health Service = £10.40m, SocialCare = £8.51m, Crime = £33.11m, Productive Capacity = £32.83m). The total cost does notinclude wider social costs that estimate the value of non-paid work and intangible socialcosts associated with people who experience premature mortality from alcohol-relateddiseases. As these costs are hard to estimate accurately they have been excluded from theoverall total, but are believed to be somewhere in the range of £48.20m-£88.16m for theHADP area. The overall cost per head is estimated to be £383 per head of population and isnot inclusive of wider social costs as described above. Including these costs increases theHADP area cost per head to £691 in 2010/11.
5 Risk Assessment
No formal risk assessment has yet been conducted. Again, the main risk would be from notprogressing the strategy and action plan. The overall strategy aims to minimise health andrelated risks to society from drug and alcohol use and misuse.
6 Planning for Fairness
Discussions have been initiated in order to undertake an impact assessment as it has beenhighlighted as a key action for 2014/15.
7 Engagement and Communication
HADP facilitates a number of regular communication initiatives aimed at increasingcommunity awareness of alcohol and drug use. These range from informing the public aboutunits of alcohol and encouraging responsible drinking, to highlighting harm reduction adviceto chronic drug users to reduce the risk of overdose. These can be local campaigns ornational campaigns contextualised for HADP e.g. Drop a Drink Size, Pregnant Pause, SafeNess Festival Advice, Overdose Prevention, NPS Briefings. On-line media is increasinglybeing utilised to communicate with a wider audience e.g. NPS Facebook chats in partnershipwith Scottish Police. Key messages include the promotion of sensible drinking, encouraginghealthier choices, drug abstinence and harm reduction, challenging discriminatory attitudesand promoting recovery. Annual Stakeholder events are organised to update partners onstrategy progress and consult on future priorities. The past three events have been wellattended by partner agencies, services users and families.
Debbie StewartCoordinator, Highland Alcohol & Drugs Partnership
24 January 2014

APPENDIX 1
HADP – Outcome Indicators - May 2013
HEALTH
1. Drug related hospital admissions
Both the Highland ADP area and Scottish rates per 100, 000 population have increasedsimilarly. The Highland ADP area rate however is significantly below the national rate.Caution is necessary when interpreting these figures. The recording of drug misuse mayvary from hospital to hospital.
Drug Related Hospital Admissions - ADP area
0
20
40
60
80
100
120
140
2005/06 –
2007/08
2006/07 –
2008/09
2007/08 –
2009/10
2008/09 –
2010/11
2009/10 –
2011/12
Year
pe
r1
00
,00
0p
op
ula
tio
n
Highland Scotland
Source: ISD, SMR01 (Mar 2013) Admissions from non-obstetric and non-psychiatric hospitals
General acute inpatient & day case discharges with a diagnosis of drug misuse in anyposition, 3 year rolling average rates per 100,000 populationADP 2005/06 –
2007/082006/07 –2008/09
2007/08 –2009/10
2008/09 –2010/11
2009/10 –2011/12
Highland 53 66 75 76 78Scotland 101 110 115 120 122
http://www.isdscotland.org/Health-Topics/Drugs-and-Alcohol-Misuse/Publications/2013-05-28/2013-05-28-DRHS2012-Report.pdf?4211062193
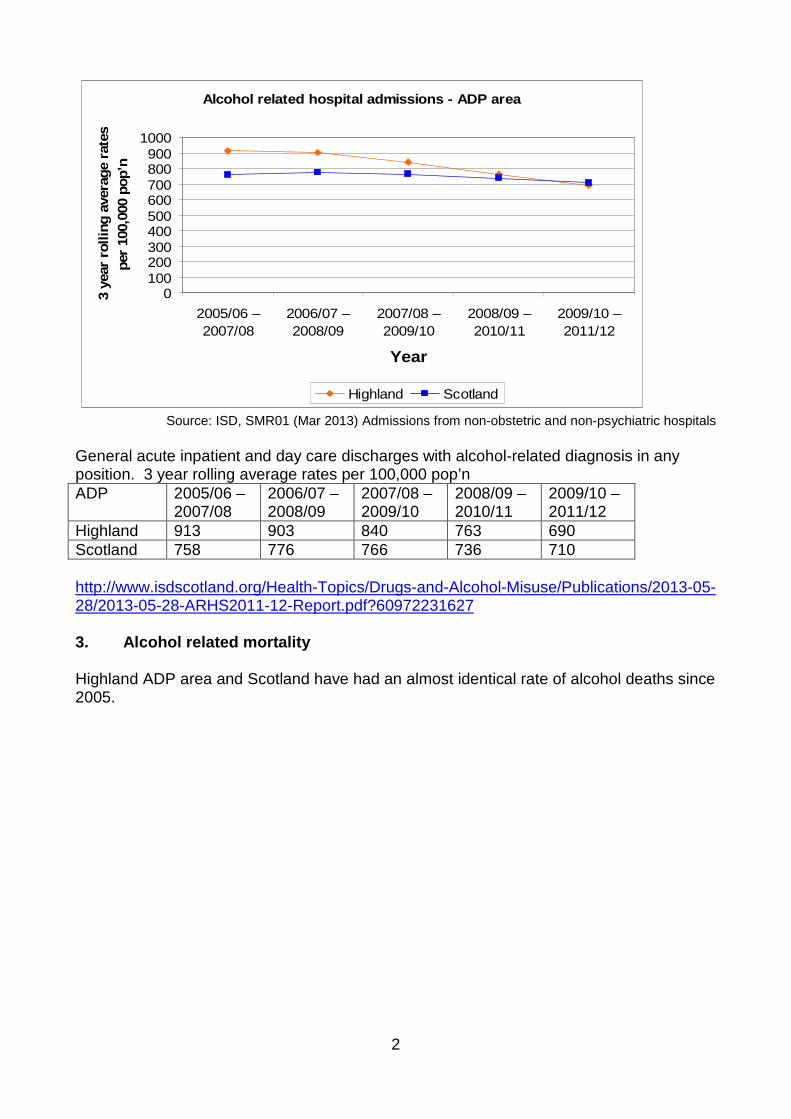
2. Alcohol related hospital admissions
Highland ADP area and Scotland both have a decreasing rate per 100,000 population.Highland ADP area remained above the national rate until 2011/12 where it fell just below.Caution is necessary when interpreting these figures. The recording of alcohol misusemay vary from hospital to hospital.
2
Alcohol related hospital admissions - ADP area
0100200300400500600700800900
1000
2005/06 –
2007/08
2006/07 –
2008/09
2007/08 –
2009/10
2008/09 –
2010/11
2009/10 –
2011/12
Year
3year
rollin
gavera
ge
rate
s
per
100,0
00
pop’n
Highland Scotland
Source: ISD, SMR01 (Mar 2013) Admissions from non-obstetric and non-psychiatric hospitals
General acute inpatient and day care discharges with alcohol-related diagnosis in anyposition. 3 year rolling average rates per 100,000 pop’nADP 2005/06 –
2007/082006/07 –2008/09
2007/08 –2009/10
2008/09 –2010/11
2009/10 –2011/12
Highland 913 903 840 763 690Scotland 758 776 766 736 710
http://www.isdscotland.org/Health-Topics/Drugs-and-Alcohol-Misuse/Publications/2013-05-28/2013-05-28-ARHS2011-12-Report.pdf?60972231627
3. Alcohol related mortality
Highland ADP area and Scotland have had an almost identical rate of alcohol deaths since2005.

3
Alcohol related mortality - ADP Area
0
5
10
15
20
25
30
2005 - 2007 2006 - 2008 2007 - 2009 2008 - 2010 2009 - 2011
Year
3year
rollin
gavera
ge
rate
s
per
100,0
00
popula
tion
Highland Scotland
Source: ISD (NRS), Mar 2013
Alcohol related deaths (underlying cause); Calendar years 2005 - 2011, 3 year rollingaverage rates per 100,000 populationADP 2005 -
20072006 -
20082007 -
20092008 -
20102009 -
2011Highland 26 27 24 24 22Scotland 27 26 24 23 22
4. Prevalence of hepatitis C among people who inject drugs
The Highland ADP area percentage is significantly below that of Scotland and hasremained consistent since 2008/09. The National figure shows a slight increase from2008/09 to 2010.
Prevalence of hepatitis C among people who inject drugs -
ADP Area
0
10
20
30
40
50
60
2008/09 2010
Year
Perc
en
tag
e
Highland
Scotland
Source: HPS, HCV antibody prevalence: data from the Needle Exchange Surveillance Initiative (NESI),2008-09 and 2010
4
Percentage of injecting drug users testing positive for HVC antibody (% is based on allinjecting drug users tested)Alcohol & DrugsPartnership area 2008/09 2010Highland 21.6% 21.6%Scotland 53.5% 56.1%
PREVALENCE
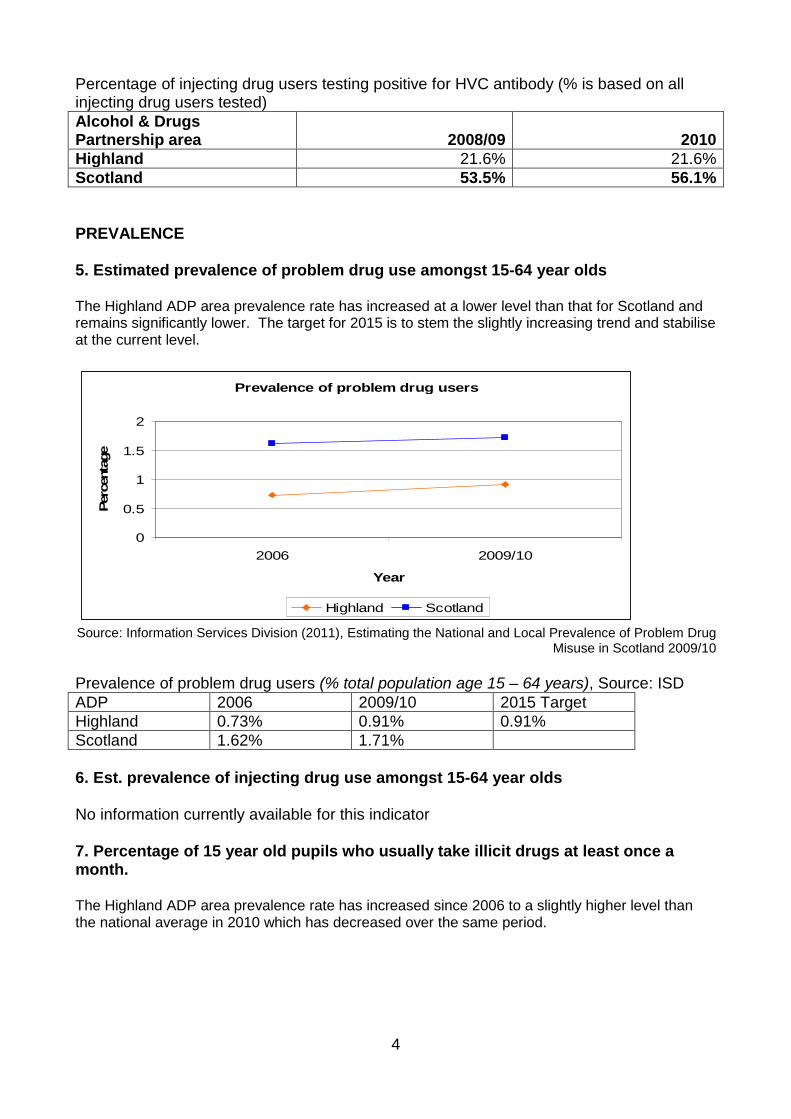
5. Estimated prevalence of problem drug use amongst 15-64 year olds
The Highland ADP area prevalence rate has increased at a lower level than that for Scotland andremains significantly lower. The target for 2015 is to stem the slightly increasing trend and stabiliseat the current level.
Prevalence of problem drug users
0
0.5
1
1.5
2
2006 2009/10
Year
Perc
enta
ge
Highland Scotland
Source: Information Services Division (2011), Estimating the National and Local Prevalence of Problem DrugMisuse in Scotland 2009/10
Prevalence of problem drug users (% total population age 15 – 64 years), Source: ISDADP 2006 2009/10 2015 TargetHighland 0.73% 0.91% 0.91%Scotland 1.62% 1.71%
6. Est. prevalence of injecting drug use amongst 15-64 year olds
No information currently available for this indicator
7. Percentage of 15 year old pupils who usually take illicit drugs at least once amonth.
The Highland ADP area prevalence rate has increased since 2006 to a slightly higher level thanthe national average in 2010 which has decreased over the same period.

5
Percentage of 15 year old pupils who usually take illicit
drugs at least once a month.
0
5
10
15
2006 2010
Year
Perc
enta
ge
Highland Scotland
Source: SALSUS, 2006, 2010(http://www.drugmisuse.isdscotland.org/publications/abstracts/salsus_local.htm)
Percentage of 15 year old pupils who used illicit drugs in the last month (2006, 2010)Alcohol & DrugsPartnership area 2006 2010Highland 9% 13%Scotland 14% 11%
8. Percentage of 15 year old pupils who used illicit drugs in the last year
The Highland ADP area prevalence rate has increased since 2006 to a slightly higher level thanthe national average in 2010 which has decreased over the same period. The target for 2015 is tostem the trend and reduce Highland ADP area levels to be at least comparative with the Scottishaverage for 2010.
Percentage of 15 year old pupils who used illicit drugs in the
last year (2006, 2010)
0
5
10
15
20
25
2006 2010
Year
Perc
enta
ge
Highland Scotland
Source: SALSUS, 2006, 2010(http://www.drugmisuse.isdscotland.org/publications/abstracts/salsus_local.htm)

6
Percentage of 15 year old pupils who used illicit drugs in the last year (2006, 2010)15 year olds 2006 2010 2015 TargetHighland 18% 20% 19%Scotland 23% 19%
9. Population exceeding weekly and/or daily limits
The indicator for exceeding weekly and/or daily limits was if an individual drank more than4 units (men) or 3 units (women) on heaviest drinking day, and/or drank more than 21units (men) or 14 units (women) in usual week. Figures show that locally and nationallymen exceeded daily/weekly limits more than women. In total the NHS Highland rate islower than the Scottish rate.
The proportion of individuals drinking above daily and/or
weekly recommended limits, 2008, 2009, 2010, 2011
0
10
20
30
40
50
60
Men Women Total
Pro
port
ion
Highland Scotland
Source: Scottish Health Survey (http://www.scotland.gov.uk/Topics/Statistics/Browse/Health/scottish-health-survey/Publications)
The proportion of individuals drinking above daily and/or weekly recommended limits,2008, 2009, 2010, 2011: Aged 16 and over (Figures based on all survey respondents) NHSBoardNHS Board Men Women TotalHighland 44.5 36.8 40.5Scotland 48.7 38.6 43.4
10. Proportion of individuals drinking above twice daily recommendations
The indicator for drinking above twice the daily recommendations was drinking >6 units onone occasion for women and >8 units for men. Locally and nationally men drink twiceabove recommended limits than women. NHS Highland has a lower rate than Scotland intotal.

7
The proportion of individuals drinking above twice daily
(“binge” drinking) recommended limits, 2008, 2009, 2010,
2011
0
5
10
15
20
25
30
Men Women Total
Pro
po
rtio
n
Highland Scotland
Source: Scottish Health Survey (http://www.scotland.gov.uk/Topics/Statistics/Browse/Health/scottish-health-survey/Publications)
The proportion of individuals drinking above twice daily (“binge” drinking) recommendedlimits, 2008, 2009, 2010, 2011; Aged 16 and over and current drinkerNHS Board Men Women TotalHighland 19.1 15.2 17.1Scotland 26.0 16.7 21.1
11. Proportion of individuals who are alcohol dependant
Please note that the original indicator agreed by the Short Life Working Group referred to'alcohol dependent drinkers'. This information is currently not available from the ScottishHealth Survey (though AUDIT board level data on alcohol dependent drinkers will beavailable in approximately four years). As a proxy measure of alcohol dependence wehave presented data on the proportion of problem drinkers, derived from responses to theCAGE questionnaire which highlights up to six indicators of problem drinking, includingthree indicators of physical dependency on alcohol. Prevalence of problem drinking ismeasure by agreement with two or more problem drinking indicators.
Men are more likely than women, locally and nationally to have 2 or more problem drinkingindicators. NHS Highland has a lower rate of problem drinking than Scotland.

8
Proportion of people with two or more problem drinking
indicators, 2008, 2009, 2010, 2011
0
2
4
6
8
10
12
14
16
Men Women Total
Pro
port
ion
Highland Scotland
Source: Scottish Health Survey (http://www.scotland.gov.uk/Topics/Statistics/Browse/Health/scottish-health-survey/Publications)
Proportion of people with potential problem drinking, 2008, 2009, 2010, 2011Aged 16 and over and current drinker
Two or more Problem Drinking IndicatorsNHS Board Men Women TotalHighland 9.4 7.2 8.4Scotland 13.9 9.5 11.7
12. Proportion of 15 year olds drinking on weekly basis (and their mean weekly levelof consumption.
The Highland ADP area prevalence rate has decreased since 2006, but at a lower levelthan the national average which has reduced significantly. The target for 2015 is tocontinue the trend of reducing prevalence in Highland ADP area to a level comparativewith the national average for 2010.
Percentage of 15 year old pupils drinking on a weekly basis
(2006, 2010)
0
10
20
30
40
2006 2010
Year
Perc
enta
ge
Highland Scotland
Source: SALSUS, 2006, 2010(http://www.drugmisuse.isdscotland.org/publications/abstracts/salsus_local.htm)
Percentage of 15 year old pupils drinking on a weekly basis (2006, 2010)

9
ADP 2006 2010 2015 TargetHighland 25% 22% 20%Scotland 30% 20%
RECOVERY
13. Percentage reduction in daily drugs spend during treatment
No information currently available for this indicator
14. Reduction in the percentage of clients in the last month during treatment
No information currently available for this indicator
15. Proportion of clients who abstain from illicit drugs between initial assessmentand 12 week follow-up
No information currently available for this indicator
16. Proportion of clients receiving drugs treatment experiencing improvements inemployment/education profile during treatment
No information currently available for this indicator
CAPSM/FAMILIES
17. Rate of maternities recording drug use
The Highland ADP area rate has been variable since 2004/05 however has shown adecrease between 2007/08 to 2010/11. Nationally the rate has steadily increased since2005/06.
Rate of maternities (per 1,000 maternities) recording drug misuse.
Financial years 2004/05 - 2010/11, three year rolling average - ADP
Area
02468
1012141618
2004/05-
2006/07
2005/06-
2007/08
2006/07-
2008/09
2007/08-
2009/10
2008/09-
2010/11
Year
per
1000
mate
rnit
ies
Highland Scotland
Source: ISD, Scottish Morbidity Record (SMR02), Mar 2013

10
Rate of maternities (per 1,000 maternities) recording drug misuse.Financial years 2004/05 - 2010/11, three year rolling averageAlcohol &DrugsPartnershiparea
2004/05-2006/07
2005/06-2007/08
2006/07-2008/09
2007/08-2009/10
2008/09-2010/11
Highland 6.6 7.2 7.0 8.9 7.9Scotland 9.6 9.5 9.9 11.9 15.8
18. Rate of maternities recording alcohol use
Maternities recording alcohol use in Highland ADP area has decreased between 2011/12and 2012/13. Over the same time period the national rate has increased.
Rate of maternities (per 1,000 maternities) recording alcohol
misuse - ADP Area
0
10
20
30
40
2011/12 2012/13
Year
Nu
mb
er
per
100
mate
rnit
ies
Highland Scotland
Source: ISD, SMR02
Rate of maternities (per 1,000 maternities) recording alcohol misuseAlcohol & DrugsPartnership area 2011/12 2012/13Highland 19.7 15.6Scotland 30.2 33.0
19. Number of Child Protection Case Conference where parental drug identified as aconcern/risk
Concerns identified at the case conferences of children who were on the child protectionregister at 31 July 2012, by local authorityAlcohol & Drugs Partnership area August 2011 - July 2012Highland 43Scotland 918
Source: Children’s Social Work Statistics 2011-12
20. Proportion of positive ABI screenings in ante-natal setting.

11
The number and proportion of ABI’s delivered in antenatal setting in NHS Highland was120 (2% of all ABI’s) in the year ending 31st March 2013.
http://www.isdscotland.org/Health-Topics/Drugs-and-Alcohol-Misuse/Publications/2013-06-25/2013-06-25-ABI-Report.pdf

12
COMMUNITY SAFETY
21. Percentage of new clients at specialist drug treatment services who reportfunding their drug use through crime
After an increase between 2009/10 and 2010/11 the Highland ADP area percentage ofnew patients/clients at specialist drug treatment services who report funding their drugsthrough crime has reached it lowest level in 2011/12 falling below the national figure.
Percentage of new patients/clients at specialist drug
treatment services who report funding their drugs through
crime
0
5
10
15
20
25
30
35
2009/10 2010/11 2011/12
Year
Perc
enta
ge
Highland Scotland
Source: ISD, SDMD (SMR25a), Mar 2013
Percentage of new patients/clients at specialist drug treatment services who report fundingtheir drugs through crimeAlcohol & DrugsPartnership area 2009/10 2010/11 2011/12Highland 22.6% 32.1% 18.7%Scotland 17.7% 22.4% 21.2%
http://www.isdscotland.org/Health-Topics/Drugs-and-Alcohol-Misuse/Publications/2013-03-26/2013-03-26-SDMDS-Report.pdf?22561281920
22. Percentage of offenders given a DTTO who are reconvicted within one year
The Highland rate per 100 offenders has decreased from 2007 to 2009/10. This is asignificant improvement. The target for 2015 is to continue the downward trend. Thenational figure has also decreased but at lower rate than Highland.

13
One year reconviction frequency rates for offenders given a
Drug Treatment and Testing Order - Community Justice
Area
0
50
100
150
200
250
2007/08 2008/09 2009/10
Year
Rate
per
100
off
en
ders
Highland Scotland
Source: SG, Criminal Justice Social Work Statistics
One year reconviction frequency rates for every 100 offenders given a Drug Treatmentand Testing Order. Financial years 2007/08, 2008/09 and 2009/10.CommunityJustice Area
2007/08 2008/09 2009/10 2015 Target
Highland 220 150 66.7 130Scotland 192.3 162.3 149.6
23. Antisocial behaviour offences recorded by police per 1000 population
For most indicators the Highland prevalence rate is below the national average and has reduced ata similar level. The target for 2015 is to continue the downward trend.
Alcohol 'related' offences recorded by the police. Financial years 2009/10, 2010/11,2011/12. Rates per 1,000 population
24. Number of community payback orders issued where alcohol and drug treatmentis required, and proportion that are completed successfully
ISD reported that there were 60 CPO’s issued in Highland and 772 in Scotland.
Number of Community Payback Order requirements issued with drug or alcohol treatment;Financial year 2011/12Alcohol & Drugs Partnership area 2011/12Highland 60Scotland 772
LocalAuthorityArea
Serious Assault Common AssaultVandalism Breach of the Peace
2009/10 2010/11 2011/12 2009/10 2010/11 2011/12 2009/10 2010/11 2011/12 2009/10 2010/11 2011/12
Highland 0.8 0.8 0.9 12.5 11.4 11.9 15.8 13.1 12.3 - - 7.4
Scotland 1.0 0.9 0.8 12.9 12.3 11.8 15.1 13.6 12.8 - - 6.3

14
Source: SG, Criminal Justice Social Work Statistics
The Highland Criminal Justice Service figures showed slightly less however it should benoted that there may have been data entry problems. Number of completed CPO’s alsomay not be robust. In 2011/12 12 of the 50 alcohol requirements were completed, and 2out of 38 in 2012/13. None of the 2013/14 requirements have been completed as yet.
Number of Community Payback Order requirements issued with drug or alcohol treatmentHighlandCommunityJustice Area
2011/12 2012/13 2013/14 to date
Alcohol treatmentrequirement
50 38 12
Drug treatmentrequirement
2 2 4
Source: Highland Community Justice Service
25. Proportion of victims of a crime who reported that the offender was under theinfluence of alcohol or drugs
The Police Scotland – Highland Division has made significant reductions from 2009/10 to 2010/11,but is still above the national average. The HADP target for 2015 is to be at least comparative tothe Scottish average.
Percentage of crimes where offender was under influence of
alcohol - Police Force Work Area
0
5
10
15
20
25
30
35
2009/10 2010/11
Year
Perc
enta
ge
Police Scotland - Highland Division Scotland
Source: SG, Scottish Crime and Justice Survey
Percentage of crimes where offender was under influence of alcoholPolice Force work area 2009/10 2010/11Police Scotland – HighlandDivision 32% 28%Scotland 23% 22%

15
The Police Scotland– Highland Division has made significant reductions from 2009/10 to 2010/11,but is still above the national average. The HADP target for 2015 is to be at least comparative tothe Scottish average.
Percentage of crimes where offender was under influence of
drugs - Police Work Force Area
0
2
4
6
8
10
12
14
16
2009/10 2010/11
Year
Perc
enta
ge
Police Scotland - Highland Division Scotland
Source: SG, Scottish Crime and Justice Survey
Percentage of crimes where offender was under influence of drugsPolice Force work area 2009/10 2010/11Police Scotland – HighlandDivision 8% 15%Scotland 12% 13%
LOCAL ENVIRONMENT
26. Percentage of young people who have been offered drugs in the last year
The Highland ADP area prevalence rate continues to be lower than the national average, but hasnot reduced at a similar rate since 2006. The target for 2015 is to sustain the decreasing trend bythe same percentage rate of reduction.

16
Percentage of 15 year olds who have ever been offered
drugs
0
10
20
30
40
50
60
2006 2010
Year
Pe
rce
nta
ge
Highland Scotland
Source: SALSUS, 2006, 2010
Percentage of 15 year olds who have ever been offered drugs Source: SALSUS 2006,2010ADP 2006 2010 2015 TargetHighland 45% 41% 37%Scotland 53% 42%
(http://www.drugmisuse.isdscotland.org/publications/abstracts/salsus_local.htm)
http://www.drugmisuse.isdscotland.org/publications/abstracts/salsus/Highland_2010.pdf
27. Percentage of people perceiving drug misuse or dealing to be common or verycommon in their neighbourhood.
The percentage of people who perceive drug use and dealing as common in their area hasreduced both locally and nationally. It is also perceived as less common in Highland ADParea than in Scotland as a whole.

17
Percentage of people perceiving drug misuse or dealing to
be very or fairly common in their neighbourhood. Financial
years 2007/08, 2009/10.
0
2
4
6
8
10
12
14
2007/08 2009/10
Year
Perc
en
tag
e
Highland Scotland
Source: Scottish Household Survey
Percentage of people perceiving drug misuse or dealing to be very or fairly common intheir neighbourhood. Financial years 2007/08, 2009/10.Alcohol & DrugsPartnership area 2007/08 2009/10Highland 10.3% 8.4%Scotland 12.5% 11.6%
28. Percentage of people noting ‘alcohol abuse’ as a negative aspect of theirneighbourhood
There has been an increase in Highland ADP area in the percentage of people notingalcohol abuse as a negative aspect in their neighbourhood between 2007/08 and 2009/10but it still remains below the Scottish figure. Over the same period the national rate hasremained consistent.

18
Percentage of people reporting 'alcohol abuse' as a negative
aspect of their neighbourhood. Financial years 2007/08,
2009/10.
0
0.5
11.5
2
2.5
33.5
4
4.5
2007/08 2009/10
Year
Perc
enta
ge
Highland Scotland
Source: Scottish Household Survey
Percentage of people spontaneously reporting 'alcohol abuse' as a negative aspect of theirneighbourhood. Financial years 2007/08, 2009/10.Alcohol & DrugsPartnership area 2007/08 2009/10Highland 2% 3%Scotland 4% 4%
29. Number of premise and occasional licenses in force per annum and theoverall capacity of premise licenses
Number of Premises licences in force on 31 March 2012 by type
of licence
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
On sale licence Off sale licence Total
Type of License
Nu
mb
er
Highland Scotland
Source: Liquor licensing statistics (Scotland): 2011-12, Scottish Government
19
Number of Premises licences in force on 31 March 2012 by type of licence
Local Authority On sale licence Off sale licence TotalHighland 896 316 1212Scotland 11553 4838 16391
30. Number of new applications for premise or occasional licenses, andproportion refused on the grounds of OP
Number of new applications for premise licences received during 2012-11 and numberrefused under Section 23 of the 2005 Licensing Act 1*
New applicationsApplicationsrefused
Local Authority on sale 2 off sale onlyHighland 17 15 1Scotland 239 206 21
Source: Liquor licensing statistics (Scotland): 2011-12, Scottish Government
* Section 23 of the 2005 Licensing Act lists five grounds on which a licence may berefused including overprovision of licensed premises in a locality
SERVICES
31. Number of screenings (using a validated screening tool) for alcohol usedisorders delivered and the percentage screening positive with thebreakdown of i) percentage eligible for ABI and ii) percentage eligible forreferral to treatment service
No information currently available for this indicator
32. Number of ABIs delivered in accordance with the HEAT Standard guidance
Both the NHS Highland and Scottish figures have increased, but nationally at a muchhigher rate. Both also exceeded the target number of interventions from 2008/09 to2011/12.

20
Number of alcohol brief interventions delivered in accordance with
the HEAT Standard guidance - NHS Board
0
20,000
40,000
60,000
80,000
100,000
120,000
2008/09 2009/10 2010/11 2011/12
Year
Num
ber
Highland Scotland
Source: Alcohol Brief Interventions 2011/2012, Information Services Division 2012
Number of alcohol brief interventions delivered In Highland
in accordance with the HEAT Standard guidance. Financial
years 2008/09 - 2011/12
11,500
12,000
12,500
13,000
13,500
14,000
14,500
15,000
Target Actual
Num
ber
Target Actual
Source: Alcohol Brief Interventions 2011/2012, Information Services Division 2012
Number of alcohol brief interventions delivered in accordance with the HEAT Standardguidance; Financial years 2008/09 - 2011/12
NHSBoard 2008/09 2009/10 2010/11 2011/12
Total No. ofInterventions2008/09 -2011/12
Target No. ofInterventions2008/09 -2011/12
Highland 2,267 2,217 4,497 5,658 14,639 12,766
Scotland 30,310 55,757 88,143 97,830 272,040 210,530
http://www.isdscotland.org/Health-Topics/Drugs-and-Alcohol-Misuse/Publications/2012-06-26/2012-06-26-ABI-Report.pdf?87046450377
21
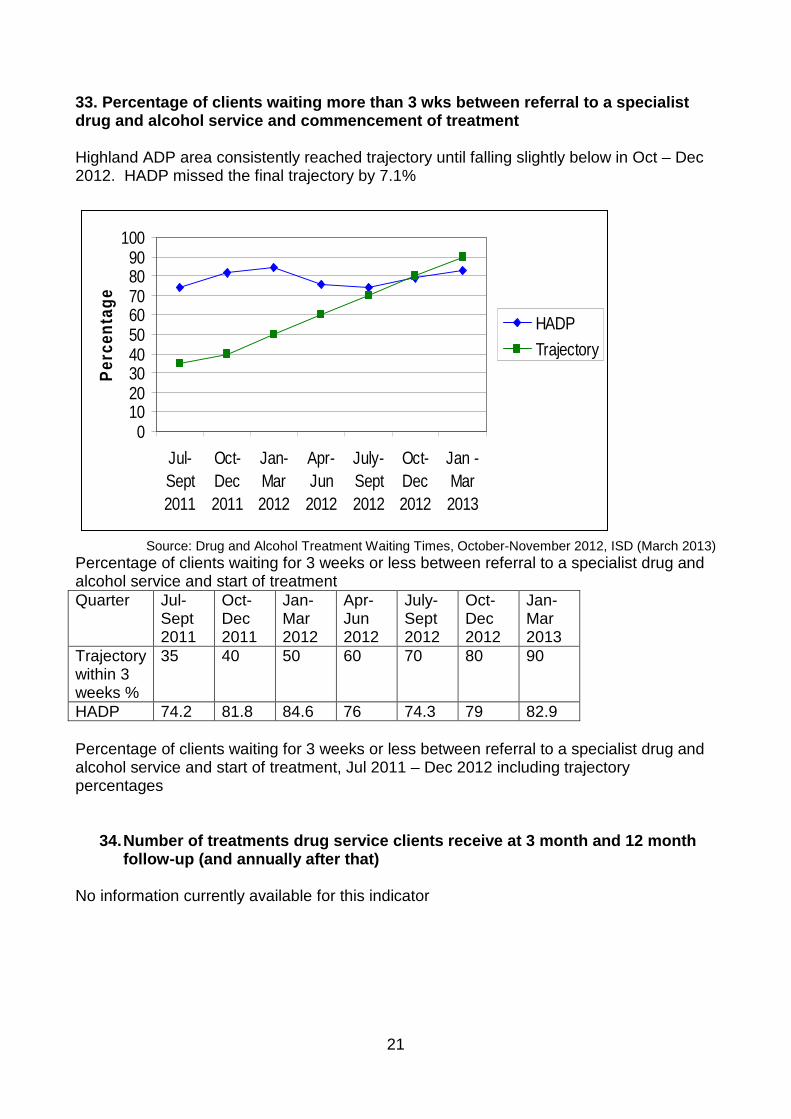
33. Percentage of clients waiting more than 3 wks between referral to a specialistdrug and alcohol service and commencement of treatment
Highland ADP area consistently reached trajectory until falling slightly below in Oct – Dec2012. HADP missed the final trajectory by 7.1%
0102030405060708090
100
Jul-
Sept
2011
Oct-
Dec
2011
Jan-
Mar
2012
Apr-
Jun
2012
July-
Sept
2012
Oct-
Dec
2012
Jan -
Mar
2013
Pe
rce
nta
ge
HADP
Trajectory
Source: Drug and Alcohol Treatment Waiting Times, October-November 2012, ISD (March 2013)
Percentage of clients waiting for 3 weeks or less between referral to a specialist drug andalcohol service and start of treatmentQuarter Jul-
Sept2011
Oct-Dec2011
Jan-Mar2012
Apr-Jun2012
July-Sept2012
Oct-Dec2012
Jan-Mar2013
Trajectorywithin 3weeks %
35 40 50 60 70 80 90
HADP 74.2 81.8 84.6 76 74.3 79 82.9
Percentage of clients waiting for 3 weeks or less between referral to a specialist drug andalcohol service and start of treatment, Jul 2011 – Dec 2012 including trajectorypercentages
34.Number of treatments drug service clients receive at 3 month and 12 monthfollow-up (and annually after that)
No information currently available for this indicator

APPENDIX 2
HADP IMPROVEMENT GOALS AND DELIVERY MEASURES 2013/14
Priority Improvement Goal Delivery Measures
HEAT standard for drug andalcohol treatment waitingtimes
Achieve and sustain 90% ofdrug/ alcohol clients startingtreatment within 3 weeks ofreferral
Conduct a DCAQ reviewto identify areas forfurther improvement tosupport the long termsustainability of ensuringfaster access totreatment.
Develop training andmentoring programmes toenhance the knowledgeand skills of Bank Nurses tosupport teams where thereare capacity issues.
Secure additionalcapacity throughstrengthening partnershipagreements with ThirdSector partners
HEAT standard for AlcoholBrief Interventions
Achieve and sustain deliveryof 160% of the standard target
Increase training uptakeand delivery of ABI’s inwider settings
Explore suitable systemsfor reporting and recordingdelivery across widersettings
Integrate ABI training withhealth behaviour changetraining
Consult with GPs to explorefuture options forembedding ABI delivery
Data compliance (SDMD &DATWTD)
Ensure compliance with theSDMD database and reduceanonymised records in theDATWTD
Take forward a localprogramme of workinformed by ISD guidanceand advice on consentissues
National naloxoneprogramme
Sustain high levels of kitdistribution and evaluate theimpact of the intranasal pilotand disseminate results
Conduct a formal reviewand evaluation of the prisonbased peer trainer initiative
Conduct a formal reviewand evaluation of theintranasal pilot
Seek to roll out theintranasal administrationoption across Highland

2
Priority Improvement Goal Delivery Measures
Outputs from the ORT expertgroup
Produce accurate data anddevise systems to monitor andstrengthen ORT practices andoutcomes
Raise awareness ofrecommendations fromORT group with localpartners
Consult and collaboratewith local partners to devisean ORT improvement plan
Work with pharmacycontractors to formaliseagreement to implementsuboxone as a substituteprescribing option
Prevalence and impact ofnew psychoactive substances
Conduct a scoping exerciseand produce a NPS actionplan
Conduct a consultation withNPS users, services andthe public to establish localprevalence and trends
Utilise the findings from thescoping exercise to inform alocal action plan
Explore suitable systemsfor reporting and recordingNPS prevalence and trends