444 west third street sex: dayton, ohio 45402-1460...
TRANSCRIPT

Patient Name: Date of Birth: Sex: Health Record Number: Account Number: Patient Type: Race:
Admit Date· 04/01/20xx
Admitting Diagnosis
Final (Principal) Diagnosis
Sarah Tonin 04/01/28 years ago F 144247
Inpatient Caucasian
Secondary Diagnoses and Complications
Operations/Procedures
Date Discharged: 04/03/20xx
Sinclair Memorial Hospital 444 West Third Street
Dayton, Ohio 45402-1460
.. ~ .. ..... . . . . . """'!:i
CODES
SIGNATURE OF ATTENDING PHYSICIAN DATE
[8] DISMISSED 0 EXPIRED 0 DISMISSED-ICF 0 DISMISSED TO SNF 0SIGNED SELF OUT 0 DISMISSED SPECIALITY UNIT 0 DISMISSED TO ANOTHER HOSPITAL 0 DISMISSED TO HOME UNDER 0 DISMISSED- OTHER
ADV DIRECTIVES: Y or N ADMITTING PHYS: Helen Loss, D.O. FAMILY PHYS: Henry Kostic, M.D.
INSURANCE INFORMATION: PATIENT EMPLOYER
HOME HEALTH CARE
ATTENDING PHYS: Helen Loss, D.O.
1::. 1 CARRIER : 0 MEDICARE 0 MEDICAID [8] : Medicaid HMO POLICY HOLDER: INSURED'S EMPLOYER: GROUP NAME: GROUP NUMBER: POLICY#: EFFECTIVE DATE:
2ND CARRIER: 0 MEDICARE 0MEDICAID D: POLICY HOLDER: INSURED'S EMPLOYER: GROUP NAME: GROUP NUMBER: POLICY#: EFFECTIVE DATE:
3RD CARRIER: 0 MEDICARE 0 MEDICAID 0 : POLICY HOLDER: INSURED'S EMPLOYER: GROUP NAME: GROUP NUMBER: POLICY#: EFFECTIVE DATE:
1

( , _
Sinc(air :Memoria( J-fosyita( 444 West 'lfiircf Street 'Dayton, Ofiio 45402
Obstetric Discharge Summary Maternal I Newborn Record System
Admitting Diagnosis 0 _____ _ Reasons Foi Admission on Date Time
0 Onset of Labor
0 Induction of Labor
0 Spontaneous Abortion
----------- -------0 Preterm Labor 0 __________________ _
Cesarean Section 0 Primary)1"Repeat
0 Tubal Ligation
0 Observation/Evaluation
0 Fetal Status
0 Medical Complications
0 Vaginal Bleeding
0 ROM 0 Premature 0 Prolonged 0 Obstetric Complications
Prenatal Procedures 0 Cerclage 0 Ultrasound # ______ _
0 NST O CST
0 Amniocentesis
O CVS 0 PUBS
0 None 0 Management of Medical Complications
0 Management of Obstetric Complications
Intrapartum Procedures Del --· :-,.,_.~...!-++ D vndelivered 0 Spontaneous Vaginal Delivery rean Delivery 0 Primaryp epeat
0 VBAC 0 Cesarean: Low Cervical, Transverse
0 Episioto.my: D Cesarean: Low Cervical ." Vertical
0 Vacuum Extraction D Cesarean: Classical
0 Forceps (Low) (Mid) 0 Cesarean: Hysterectomy
0 Rotation to 0 Uterine Exploration
0 Breech Extraction (Partial) (Total) 0 Tubal Ligation 0 Forceps to Extract Breech 0 Anesthesia ___________________ _
0 Curettage 0 ---------------
Postpartum/Operative Complications ~me 0 Transfusion 0 RHo (D)(ig 0 Tubal Ligation 0 Rubella lg __________ __
Ll Curettage 0 Antibiotics 0 [] ___________ _
Postpartum/Operative Complications )Gone r J __ Perineal Laceration ~ ] Psychological Maladaptation
1 (Vaginal) (Cervical) Laceration
r.J Pelvic Infection
~ Drug Transfus1on React1on
Eclamps1a
r' Unnary Infection
~~ Pulmonary Infection :·-, Wound Infection
0 Hematoma 0 Spinal Headache
Discharge Diagnosis 0 Amnionitis
0 Antepartum Bleeding
0 Failed Induction
0 False Labor
0 Hyperemesis Gravidarum 0 Placenta Previa
0 Postterm Pregnancy
0 Preeclampsia
1 Hemorrhage C Ulenne
~ Retained Placenta
:~· Phlebitis [] Morbidity (undetermined) 0 _____________ _
~rm Pregnancy-Delivered
/ D Premature Labor D Preterm Delivery
0 Postterm Delivery
0 PROM x Hours
D Spontaneous Abortion
0 Incompetent Cervix 0 __________________ ....,.., D __________________ __c_;
Comments
Circumcised 0 No ~ ~(DW-, q;rr
Discharge ~Mother 0 Other--------
Complications 0 No ~ Discharge Information Medication [] None
(or)
Pain
Diet
~(srte _ ______ -+------lntensity o \ i"
none h ig~1est :.. Routine
(or) --,..-------;..----------0 Unrestricted I ()
(or) -----+1 _;_I\+'-. ...,-'-1-'-' 4± ..._\4\,.._ . .J--=---D Routine / ' ~
(or) -------+------------
Activity
Instructions
Discharge to D Home (or) ------,----f----,-,-,------Follow up in --+----
2

Sinc{air Memoria{ Jfosyita{ 444 West 'lfiirc[ Street 'Dayton, Ofiio 45402
----~(:~----~----PATIENT IDENTIFICATION
Dayton, Ohio
Health History Summary
Pati€nt 's narm~ ...................... ....
Hon1e f.\ddress ............................................. ..
Date: •.· / . 1 • Race or Marital Years Age__ birth ______ ethnicity ______ Religion _ _______ status _____ _ married Education ___ _ Social Security Work Home number ______________ Occupation _______________ Tel. no. Tel. no. ______ _
Alternate Relation Work Home contact ----------------,---..,.,-----to patient ________ Tel. no. Tel. no. ______ _ Referring Attending
Medical History Check and detail positive findings including date and place of treatment. Precede findings by reference number.
1. Congenital anomalies .... .. .... .. .. .. ... . 8- .... D <..,i.l£ f ~ 2. Genetic diseases ............... ......... . -9 ..... ~ .(_
1 If r!.£
3. Multiple births .. ...... .. ....... .... ......... MB ..... ~ 7 . ,#..l . 4. Diabetes mellitus ............... .. ....... .-Q_ .. UY rj U-<.J<..J!.-( fl((J F 5. Malignancies ...... .. ..... .. .. ................. ~/.
6. Hypertension .. .. ........................... .. ...B~ ... :t£;1/~ F 7. Heart dis~ase ..... .... .... .. ... ,.zi ....... . ..Q ..... o f) &.! F 8. Rheumatrc fever ... .f}l..i/.r ........ -0 ~ fJ ~ 9. Pulmonary disease ......... ........ ...... '§:.r f.1 . ' ((_<._..
10. Gl problems .. .. .. ... .............. .. .... ...... \1..6 't.'L.l( l(p . 11 . Renal disease ..... .. ........... .. ............ .8 .... .0 12. Genitourinary tract problems .. .. ...... bOJ----13. Abnormal uterine bleeding ............ !:11-----· 14. Infertility .................... .. .. .... .. ........ .,.,a-r- . . ...;;_, 15. Venereal disease ........................... fd'. .. & ~ 16. Phlebitis, varicosities .. ......... .. ...... .. ..1-.f]-1---
17. Neurologic disorders .................. .. .. Q .. § .7 ...,1_
18. Metabol./endocrine disorders .. .. .. ...B:-:-... lif ft1. /T 19. Anemia/hemoglobinopathy .. .. ....... .ld ..... O 20. Blood disorders ......... ..... ............. ,LJ 0 21 Drug abuse .. ... .... .. .. . ............ ... o·":vtt.~·~d I Cf1 11-¥' 22.~alcohol use .................... ~ 1 f/Ljc/ tf.;f / / 23 ~us drseases ...... . . ..... ~ , 1 /t /.- 1 1
24. Operatrons/accrdents.... .. .... :,_..Q"" itA1/...t'-(. .tt:.JI A .. f..t.4ff. /{., C 25. Allergies/meds sensitivity .......... . ,...Q m Krt 26. Blood transfusions .. ..... ........ .. ... .... .,Q--. . . '-f- ;J . fi! 27. Other hospitalizations ....... .. ........ :./l-x...e./JtA tJ .££L:.j<..W.,_
Preexisting Risk Guide Indicates pregnancy/outcome at risk 31 . 0Age<15or>35 32. 0 <8th grade education 33. 0 Cardiac disease (class 1 or II) 34. 0 Tuberculosis, active 35. 0 Chronic pulmonary disease 36. 0 Thrombophlebitis 37. 0 Endocrinopathy
0 Epilepsy (on medication) 39. 0 Infertility {treated) 40. 0 2 abortions (spontaneous/induced) 41. 0 2::.,? deliveries
0 Previous preterm or SGA infants 0 Infants 2:,4,000 gms 0 Isoimmunization (ABO, etc.) 0 Hemorrhage during previous preg. 0 Previous preeclampsia 0 Surgically scarred uterus 0 Preg. without familial support 0 Second pregnancy in 12 months
Smoking (2:.1 pack per day)
51 . 0 --'------------52. 0 ----::----=------53. 0 -----------
Indicates pregnancy/outcome at high risk
54. 0 Age 2:,40 55. 0 Diabetes mellitus 56. 0 Hypertension 57. 0 Cardiac disease (class Ill or IV) 58. 0 Chronic renal disease ~: . :: ·: :: ::::::::::::::::::.: .. .. ........ o ..... o t'~uf'?t
0 Congenital/chromosomal anomalies 5-----"''r-------r------.....lo..------.,..------r--....W..I...O~::...-'"f"':~,...-~~:;n 0 Hemoglobinopathies
. l J lso.immunization (Rh) t-----J._...._._ __ .,..__~-+--..._,,......_...._..,.._..._.-,.;;.;;;~-~---'+',;,.;;;.+f...,---to.::. 0 Alcohol or drug abuse
6
7
8
63. LJ Habitual abortions Ll lncompetent cervix [] Prior fetal or neonatal death
3

(
Sinc[air .Memoria[ Jfosyita[ 444 'West Tfiin£ Street 'Dayton, Ofiio 45402 PATIENT IDENTIFICATION
Dayton, Ohio
Initial Pregnancy Profile Date: me I day I yr
• • 'Check and detail po$jtiV6 H1story Smce LMP (/) ~ . >oz -;;7 ,, , ~> ""·%~} ·' .. •.
1 Heartaches ... .............. ... .......... 8"" ~ '"'" omiting ...................... B' ' "
3 alpain ................ ..... ~ 4. Urinary complaints ...... ...... .... :-8·--rm 5. Vaginal discharge ................... ..a-----f " 6. Vaginal bleeding .................... ~ 7. Edema (specify area) ............. ~.
8. Febrile episode ....................... :B--i 9. Rubella exposure ..................... 9---
10. Other viral exposure .. .... .... ...... 9--- . 11 . Radiation exposure .... .. ............ g.--- ~ 12. 0 13. 0 14. Contraception prior
to conception
Last used: ___ r:_cr,_· 1_,_1$_-"_l_>_·r __
Pa1ient's nama
Initial Physical
SYSTEM Check and 'detail till abnormalfindi~~; ·t;~iow. Use ~renee numbers, 17. Skin .. ............................ .
18. EENT ..... .............. ......... .
19. Mouth .......................... ..
20. Neck ............................ ..
21. Chest.. ......................... .
22. Breast.. ........................ .
23. Heart ......................... ..
24 Lungs .... ..
25. Abdomen ..
26 Musculoskeletal . . .. . ..
27. Extremities ..
28. Neurologic ....
Pelvic Examination
29. Ext ge'litalia ..
30. Vagina .... ... ..
31. Cervix .. .. ..................... .
32. Uterus (describe) ...... ..
33. Adnexa .............. .. ........ .
34. Rectum .................. .. .... .
35. Other ........................... .
36 Diag. conj .
D
D
D
D
D
0
0
:::J
D
D
D
0
D
D
37 Shape sacrum -----
38 s.s. notch
39 Ischial spines
Bony 40 Pubic 41 Trans 42 Post 43 Coccyx arch -----.:--- outlet sag. diam ______ _
Pelvis 44 Classification 0 Android 0 Anthropoid 0 Platypelloid
45 Estimation 0 Borderline D Contracted
15. Nutritional Assessment
Adequate 0 Inadequate Nutritional counseling
16. Medications Since LMP
0 Exposure to Drugs
v
v
I I
I
4

Sinc{air :.Memoria{ J-iosyita{ 444 West 'lfiinf Street 1Jayton, Ofiio 45402
~ ....... · ............ ~~r, .....,....'-"~---:-----PA_T...,..IE~f IDENTIFICATION -----,
Prenatal Flow Record
Dayton, Ohio Patient's name _ _ =
Has no known risk Is "at risk" Is at high risk
Continuing Risk Assessment Guida {revise RISK STATUS) Date At risk factor Date High Risk factors
_ I_ Uterine/cervical malformation _ !_ Diabetes mellitus _I_ Suspect Pelvis _!_Hypertension _ I_ Rh Negative (nonsensitized) _ I_ Thrombophlebitis _ !_ Anemia (Hct<30%: Hgb< 1 0%) _I_ Herpes (type 2) _I_ Venereal disease _ I_ Rh sensitization _ 1 _ Acute pyelonephritis ~ I_ Uterine bleeding _ I_ Failure to gain weight _ I_ Hydramnios _I_ Abnormal presentation _I_ Severe preeciampsia _ 1 _ Postterm pregnancy _I_ Fetal growth retardation _I_ Alcohol use _I_ Premature rupt. membranes _ 1 _ _I_ Multiple pregnancy (preterm) _I_ _I_ Alcohol and drug abuse
_!_ _I_ ----------_ !_ _I_ ----------_/_ I
I
;--I
l I I +
I I 'l +
I I I +
I I I +
I I I +
I I ·' I +
I I / +
DS-2694 00/00 Physician's signature
Result
Return visit Sig .
5

Sinc{air :Memoria{ J-fosyita{ 444 West Tfiirr£ Street 'Dayton, Ofiio 45402
Osteopathic Musculoskeletal Examination of the Hospitalized Patient
1. AntJPost. Spinal Curves: I N D
Cervical Lordosis 0 1Lr 0 Thoracic Kyphosis 0 fJ 0 Lumbar Lordosis 0 0 0
!-Increased N-Normal D-Decreased
Scoliosis (Lateral Spinal Curves)
~ None 0 Sitting 0 Functional 0 Standing 0 Mild 0 Prone/Supine 0 Moderate 0 Lateral Recumbent 0 Severe 0 Unable to Examine
Reasons:
3. SOMATIC DYSFUNCTIONS CORRELATE WITH:
D Traumatic D Rheumatological 0 Orthopedic 0 EENT 0 Neurological 0 Cardiovascular D Viscera somatic 0 Pulmonary D Primary Ms-Skeletal 0 Gastrointestinal D Activities of Daily Living 0 Genitourinary D Other 0 Congenital
4. PEDS ONLY: a. Cranium:
Fontanelles: Anterior Posterior Patent/closed
@ Overnding Sutures Present/absent
b. Ambulat1on:
L1 Walks 0 Sits unassisted 0 Crawls [J F1olls over
CHIEF COMPLAINT: I .__A./}
Instructions: Complete Boxes #1 - 3 (#4 Pediatrics Only)
2. SEVERITY KEY:
0 = No SD or background (BG) levels
1 = Minor TART more than BG levels
2 =TART obvious (R&T esp) +1- symptoms
3 = Symptomatic, R and T very easily found, "key lesion"
Head (739.0) !21 D Neck (739.1) ~ D Thoracic T1-4 (739.2) D
TS-9 D T1 0-12 D
Lumbar (739.3) D Sacrum Coccy eal (739.4) D Pelvis/Innominate/ Pubis (739.5) I2J D
R Extremity (lower)
L (739.6) D R
Extremity (upper) L (739.7) tJ 0
Ribs (739.8) [3 r c--1
Other I Abdomen (739.9) 0 LJ
D D D D 0 D
D
D
0
0 0
0
ASSESSMENT TOOLS:
D 0 0 0 0 0
0
0
0
0 0
[]
T =Tenderness A = Asymmetry R = Restricted Motion
Active Passive
T =Tissue Texture Changes
Physician Signature· _,__ _ _____ -==-.., Date :_~....l...f-/--l./-+"/tl._~ ----
6

Name: DOB :
Adm. Date:
FIRST ASSISTANT :
Sine fair Memoria{ J{osyita{ 444 West Tfiirc[ Street 'Dayton, Ofiio 45402
MRN: Acct#: Fac: VS Rm: 1202 Date of Surgery : 04/01/20JI Disc Date:
ANESTHES I A : Spinal anesthetic.
PREOPERATIVE DIAGNOSES : Intrauterine pregnancy 40 weeks , previous Cesarean section x2.
POSTOPERATIVE DIAGNOSES : Intrauterine pregnancy 40 weeks, previous Cesarean section x2.
PROC: A repeat low- transverse cesarean section .
PROCEDURE TECHNIQUE : This 28-year-old female was taken to the operating room , placed in supine position after having a spinal anesthetic placed . She had a Foley catheter sterilely placed and she was sterilely prepped and draped . She was checked for adequate analgesia, when this was assured, a low Pfannenstiel skin was subsequently made through the previous skin scar. The incision was carried down through the anterior abdominal wall in the usual fashion and entrance into the abdominal cavity was then achieved. Bladder blade was then positioned. The lower uterine bladder flap was then developed off the lower uterine segment, bladder blade was repositioned. A low uterine transverse incision was subsequently made. Incisions of the intrauterine cavity was noted clear fluid. With the aid of a device, one pull was utilized to deliver the infant through the lower uterine segment vertex. The infant's nasopharynx was suctioned . No nuchal cord. Remaining infant delivered without difficulties . Cord was doubly clamped and fired , and the infant given t o the nursery personnel present at the time o f delivery. The co r d b l ood was obta i ned. Placenta was ma n uall y extracted fr om t he uterus. The uteru s was e xterna lize d to t h e abd omen. Old blood and fragments were removed from the lower uterine segment. The lower uter i ne segment was then reapproximated using a runn1ng lock stitch of 0 Vicryl at ~he f1rst layer approximating the myometrial layer and second layer was utilized to imbricate this first layer. Several figure-of-eight sutures were olaced along the suture line for hemostasis. The uterus was placed bac~ 1ntra-abdom1nally. Pelvic lavage was performed with hemostasis being assured. The bladder flap was then reapproximated using 3-r Vicryl. Pelvic .avage was once again performed. The abdominal wall was then closed in usual £ash1on w~th the f1rst layer approx1mating •he peritoneum. Tne same suture was u~ilized to reapproximate the rectus abdom1n1s muscle. Anterior rectus fascia was reapproximated by using 0 V1cryl starting laterally and t1ed midline . Subcu was closed with 3 - 0 Vicryl. Irrigation had been performed throughout all the closure layers and the skin was c l o s ed wi th a runn i ng st itch o f 4- 0 Monocryl . Dermabo nd was app l ied . All blood c l o t s remo ved fr om v agina, which was minimal . Urine draining yellow clear fluid at the completion of procedure. Estimated blood loss 300 cc. She was taken to the recovery room in satisfactory condition.
PROC RPT Page 1 7

Sinc{air Memoria{ J-fosyita{ 444 West Tfiirci Street
--,
1Jayton, Ofiio 45402
Name: ......... l'jj MRN: ~I?Qi:UeC?f Acct: • Job#:
GROSS PATHOLOGY: This is a 28-year-old gravida 5, para 2-0-2-2 with an EDC of 03/27, previous C-sections x2 was brought back for elective repeat Csection. She had the above procedure performed. Delivered a viable male infant through the lower uterine segment. The uterus, tubes, and ovaries were unremarkable. No tubal ligation was performed at this time. Estimated blood loss 300 cc. Urine draining yellow yellow clear fluid at ~~------ ~ completion of procedure.
0 : T: P:
04/01/2 04/01/2 04/01/20
Job #: ..gy;n a a•
08:05:11 15:05:59 15:40:00PM
PROC RPT Page 2 8

Sinc{air Jvtemoria{ J{osyita{ Treatment Consent-Information Release-Financial Statement
Facility:
CONSENT FOR TREATMENT : The patient or his agent, recognizing the need for hospital care, consents to hospital services
as ordered by the attending physician, including emergency, outpatient, observation, and inpatient care, anesthesia,
laboratory procedures, medical or surgical treatment, x-ray examination or other hospital services rendered under the
general and specific instructions of the physician.
CONSENT TO RELEASE INFORMATION: Authorization is given to K~ ~ fl!llil? 3 u•· !frko!tconsisting of'~· !1aiJIIJli1811IIJII!II .. and -~~ Center and affiliated
and hospital records to any~loyee, facility or
affiliate, to any insurer, government agency, health care provider or facility or a.11y ether entitjp for the purpose of
{a)obtaining payment for hospital, medical or other services or products provided to the patient, {b)discharge planning
and future hospital, medical or nursing care, {c)permitting independent health care providers or their designees who
have provided services to or for the patient, access to information needed for billing purposes and filing of claims
with insurers or other third-party payers, {d)disclosing identification data to affiliated foundations for charitable
purposes, {e)disclosing data for health care services monitoring, assessment and improvement or for state, federal, or
local regulatory compliance, or {f)for legal consultation, risk management and quality assurance purposes . This auth
orization includes records which may contain information concerning care of psychiatric conditions, drug or alcohol
abuse, HIV test results, AIDS and/or AIDS related conditions .
ASSIGNMENT OF INSURANCE BENEFITS: In consideration of the hospital , medical, and nursing care given to the patient, and
in the event the patient is entitled to hospital and/or medical benefits said benefits are hereby assigned to the
hospital . authorize payment to be made directly to the .acility providing care and treatment .
PHYSICIAN CARE: The pat ient will be under the professional care of a doctor called the attending or ordering physician,
who arranges the services for care and treatment of the patient . The attending/ordering physician is usually selected
by the patient, or the patient's agent, but may, under unusual or emergency circumstances be otherwise selected .
NOTICE: Physicians who render professional services to you in a are independent practitioners and are
not employees or agents of the~facil ity . ls not responsible for the acts or omissions of the physicians that
3re not directed or controlled by the~entity providing care and treatment.
fiNANCIAL AGREEMENT: The undersigned agree that the patient, and guarantor if any, in consideration of the services to
~e rendered to the patient, is/are individually obligated to pay the full account of th~ntity providing care and
treatment upon the patient's discharge, or sooner if requested. Because NO ..... entity extends credit , the undersigned
~derstands all accounts for the patient are due in full at the time of service to the patient. Individuals may be elig
ible to receive basic, medically necessary hospital-level services at reduced or no cost if family income is at or below
:he federal poverty guidelines.
<ALUABLES: We recommend that the patient send home, or leave at home any personal valuables on their person at the time
)f treatment , service or admission . However, for the convenience of the patients, a safe is available without charge if
1ecessary. Therefore the hospital shall not be liable for the loss or damage to any personal proper ty {including cloth
eng) <lf the patient's brought into the hospital unless it is deposited in the facility safe for safe keeping.
lTHERo l h'lve received a copy o• ··.h Not1ce o~ Privacy Practice dnd Patient Bill of Rights with gnevance process,
1i s:-.. ati•ln gu1de lines 1 contact numbers 1 ~' state a gene 1es, and 1nform<1t ion on smoking cessation.
~ have read the i terns above, or i · • s read to me, or expla~ned t.o >:he satisfaction of the undersigned patient or
L~-~· and agree to the terms hereof
litness
Rela t ionship to Patient
Reason unable to sign {if applicable)
MRII: ifll. •••· Name:
Acct II: ,... . • 11 DOB : 01/08/
9

Sinc{air Memoria{ J{osyita{ 444 VVest J(hirc(Street ~~~------~-----------r--~o~o~N~o~ri~M~PR~IN~r~A~s~ov~E~T~HI~s~LI~NE~------------------
1Jayton, Ohio 45402
PHYSICIAN'S ORDERS
The Pharmacy may dispense another identical drug, unless specifically ordered otherwise.
GS0002U (02/07)
2. _______________ _
3. ________________ _
4. _______________ _
ORDERS & TREATMENTS
PHYSICIAN'S ORDERS 10
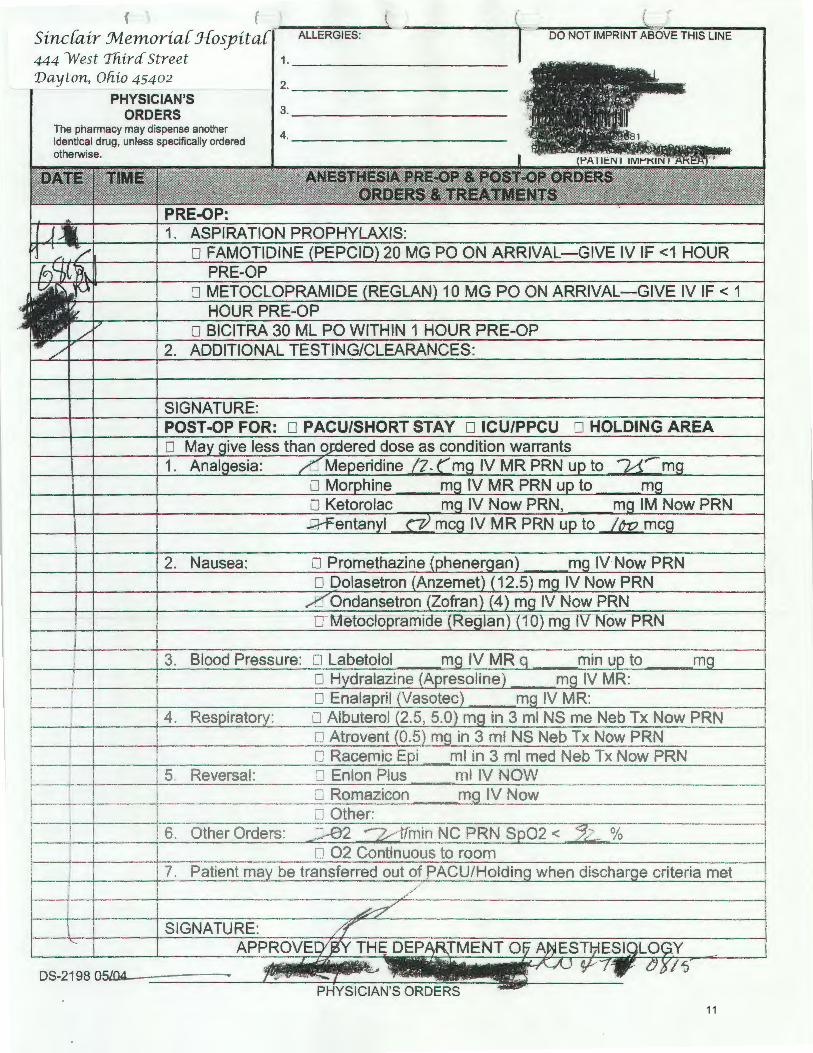
{ ( ~r-~~~~---------------~~-~~~~~~~~~~~ Sinc{air Jvlemoria{ Jfosyita ALLERGIES: LINE
444 West 'lliircf Street Dayton, Oliio 45402
PHYSICIAN'S ORDERS
The pharmacy may dispense another identical drug, unless specifically ordered otherwise.
2. Nausea:
5. Reversal:
1. __________ _
2. __________ _
3. __________ _
4. __________ _
11

'·
Sinc(air Jvlemoria( J{osyita( 444 West 'lfiira Street 1Jayton, Ofiio 4 5402
ELECTRONIC ORDER REPORT
ALLERGIES: DIPHENHYDRAMINE
CC: C/S REPEAT
Entry Location: _. •••
ORD NUM:9, PSAD-C-SECTION ADMISSION ONCE,MAX ACTIONS: 1
PRG- TRM;PREV C SECT
NW/New(Start date 04/01/2 0639 - No Stop Date found - )
Ordered By: ~l I uall&LC.t . DO (Electronic
ORD NUM:10 ,C-SECTION ADMIT LABS (DONE WITH ADMIT) cent,
NW/ New(Start date 04/01/2~ 0639 - No Stop Date found - )
Ordered By: DO (Elec troni c
ADMITTING: ,~~--~~~----~~
Session Start: 04/01/20 0639
Session Stop: 04/01/2
Run Date : 04/01/2
0639
0640
ORD NUM:ll ,PLACE AMNIO AND us REPORTS ON CHART ONCE,MAX ACTIONS: 1
NW/New (Start - No Stop Date found -)
Ordered By :~~~~im DO (Elec t r onic
ORD NUM:12, VITAL SIGNS AND FHT ' S ON ADMISSION cent,
0639 - No Stop Dat e f ound -) NW/ New (Start date 04 / 01/2 0
Ordered By:~~-~-~~~li~ DO (Ele c tronic
ORD NUM:13, ELECTRONIC FETAL MONITORING ONCE,MAX ACTIONS: 1
NW/New( Start date 04/ 0l/2 tiJ 0639 - No Stop Dat e f ound -)
Ordered By : 1.. ' ' DO (Electronic
ORD NUM:14,DIET-NPO- (NOTHING BY MOUTH) meals,
NW/New(Start date 04/01/2~ 0639 - No Stop Date found -)
Ordered By: . " ' , DO (E lectronic
ORD NUM: 15. c- SECTION ABDOMINAL P REP ONCE' MAX ACTIONS: 1
NW/New(Start date 04 /0 1/2 - . 0639 - No Stop Date found -)
Ordered By: , DO (Electronic
,~L NJM ;, ANTI EMBOLIC STOCKINGS PRE-OP con::.,
NW/New(Start date 04/01/2 0639 · No Stop Date found -)
Jrdcr•" ~-~ !'l,,. .. _.i!!!I'I!IEiiiiiii'iiiiiYtt'•••sll·_.l.il* DO
Adm1tted: 04/01/2
HT: 5 ft 7 in WT: 174 lbs
Age : 2 8 Sex: F
)QB: 01/08/~
(Electronic
3 ozs
DO
DO
Signed By: ····-~~ DO
Signed By: 41lla.~~,.~~~~~~ DO
Signed By: ·····~~~~~~~IJ!IJJ!j)J. DO
Signed By -~- ~- --~~~~--~~~~~~-~~" DO
MRN:
Account: NS Room/Bed : l LDY 1390A
ELECTRONIC ORDER REPORT
\
/
PAGE 01
12

ALLERGIES: DIPHENHYDRAMINE
( .,..........._.
Sinc{air :Memoria{ J{ospita{ 444 West Tfiircf Street 'Dayton, Ofzio 45402
ELECTRONIC ORDER REPORT
L
CC: C/S REPEAT ADMITTING: .... iM.$ 'Rif'l?.0'
Entry Location: r til I • .
ORD NUM:23, P/O C-SECTION VITAL SIGNS - SEE ORD REF cont.
NW/New(Start date 04/01/2~ 0806 7 No Stop Date found 7)
Ordered Byi<J· i!M!!tlifilllftllllif'.· DO (Electronic )
ORD NUM:24, CHECK FUNDUS C-SECTION cont,
NW/New(Start date 04/01/20 0806 - No Stop Date found 7)
Ordered By<:·?J!I!!I.!l'!IJIIi!!!l!l!lll• DO (Electronic
ORD NUM:25, NOTIFY PHYSICIAN OF EXCESS LOCHIA RUBRA cant,
NW/New(Start date 04/01/2 '
Ordered By !Iii' Wj-iltl!IIJII[M~ DO
0806 7 No Stop Date found -)
(Electronic
ORD NUM:26, REMOVE ABDOMINAL DRESSING IN AM cant,
NW/New(Start date 04/01 /2 0 0806 - No Stop Date found -)
Ordered By:~• DO (Electronic
ORD NUM:27, ABDOMINAL BINDER cant,
as needed
NW/New(Start date 04 /01/20
Ordered By~.llbbiZSSIIII .. a!&WBr.< DO
0806 7 No Stop Date found -)
(Electronic
ORD NUM:28, REMOVE STAPLES FROM INCISION cont.
a t time of discharge
NW/New(Start date 04/01/2
Ordered By f!IIJI!!I!J!l!!!!I!'I•~J> DO
0806 - No Stop Date found -)
(Electronic
ORD NUM:29,P LACE STERI STRIPS cont,
at time of discharge
N"I'I/New(St.art date 04/01/2 0806 - lio Stop Date found ·1
Clrdered By· lfl IB k DO (Electronic
Adm1tted: 04/01/2 HT: 5 ft
Ag e: 28
DOB: 01/0
7 i n WT: 174 lbs
Sex: F
3 ozs
Session Start: 04/01/20
Session Stop: 04/01/20
Run Date : 04/01/20
Signed By: :r tlJ££ •ww. DO
Signed By: •••••• DO
Signed By: -·~~~-~~- DO
Signed By: ......... DO
Signed By: ~--~~~~~~--~DO
Signed By: 'Ill!&, . DO
Signed By· ~llllllll .. • DC.
MRN:
Account: ~ NS Room/Bed:
~ , ELECTRONIC ORDER REPORT
0805
0811
0812
PAGE 01
13

ALLERGIES : DIPHENHYDRAMINE
Sinc{air Memoria{ J{osyita{ 444 West Third Street 'Dayton, Ofiio 45402
ELECTRONIC ORDER REPORT
CC: C/S REPEAT ADMITTING:AIIIIIIIIIII~~~o
Entry Location : Tllbi P
ORD NUM:3o, ACTIVITY AS TOLERATED cant,
NW/New(Start date 04/01/2~806 - No Stop Date found -)
Ordered By ='ll!lltililliU 1•1 H. DO (Electronic
ORD NUM: 14, DIET-NPO- (NOTHING BY MOUTH) meals,
ID/DC'D(Start date 04/01/2. 0806 -H)
Ordered By: ~*&*llaiii?.ZIIIILLSLLS • DO (Paper Chart)
NW/New(Start date 04/01/2011 0639 - Stop date 04/01/2 0806 -H)
Ordered By:~· ~~~~~~~~~la~~~~~ DO (Electronic )
ORD NUM:31, DIET-FULL LIQUID DIET meals,
ID / DC'D(Start date 04/01/ 20 0808 -H)
(Paper Chart)
NW/ New(Start date 04 / 01 / 20 0806 - Stop date 04/ 01 / 20 0808 -H )
Ordered By: tllllllliliJ DO (Electronic )
ORD NUM:32, ADVANCE DIET AS TOLERATED cont,
NW/ New(Start dat~' ~4 / 01/2~080 6 -No St op Date f ound-)
Ordered By , DO (Elec tronic
ORD NUM: 33, FOLEY CATHETER TO STRAIGHT DRAINAGE cont ,
NW/New (Start date 04/ 01/20. 0806 - No Stop Date found -)
Orde red By: ~I&MI~~~~ DO (Electronic )
ORD NUM:34,DC FOLEY IN 8 HRS- UA , C&S F IRST I F ORDER cont.
Obtain UA, C&S before de' i.ng if ordered
NW/ New(Start date 04/01/ 2
Adm1tted: 04/01/20
DO
0806 - No St.op Date foUDd -)
(Electronic
HT: 5 ft 7 in WT: 174 lbs 3 ozs
Age: 28 Sex: F
DOB : 01/08/~
04/01/2 1 04/01/2 ' 04/0!/2 ....
Session Start:
Session Stop :
Run Date :
, DO
Signed By: USER PAPER-CHART
Signed By: USER PAPER-CHART
Signed By : .,. ..... .,,,, DO
Signed By: ........ DO
Signed By: · ···-DO
Signed By: i.«JliJIJI!Ii. DO
ELECTRONIC ORDER REPORT
0805
0811
0812
PAGE 02
14

ALLERGIES : DIPHENHYDRAMINE
(
'~
Sinc[air Memor ia[ J{osyita[ 444 West Thircf Street Day ton, Ohio 45402
ELECTRONIC ORDER REPORT
L
CC: C/S REPEAT ADMITTING: ........ DO
Entry Location : :t:!M-••IIIIU .. IWr
ORD NUM:3s, STRAIGHT CATH X 1 UNABLE TO VOID x 12hrs cont,
NW/New(Start date 04/01/20 ; 0806 - No Stop Date found - )
Ordered By: DO (Elec t ronic
oRD NUM:36, COMPLETE CURRENT IV AT 200 ML/HR, THEN cont.
NW/ New(Start date 04/01/20~ 0806 - No Stop Date found - )
Ordered By: ~llllllllll· DO (El ectronic
ORD NUM:37, IV DEXTROSE 5% AND 1/2 NS AT 125 ML/HR cont,
NW/ New (Start date 04 / 01/2
Ordered By ·····~If, DO
0806 - No Stop Date found - )
(Electronic )
ORD NUM:38, DC IV IN AM IF STABLE cont.
NW/New (Star t date ·04/01/ 2 · 0806 - No Stop Date f ound - )
Ordered By llJ44#!1'*111!111\CY, DO (Electronic
Session Start:
Session Stop:
!tun Date :
04/01/210 0805 04/01/2 0811
04/01/2 0812
Signed By: .......... DO
Signed By: t!!l!lllilf!ililflll•iiiJI DO
Signed By: ,tfllllllfl·-· DO
Signed By: W#l!lii·£2·-···Jir,ti'\; DO
ORD NUM:39, 0RDER ANTIBODY TITRE- I F RhNEG & BABY POS ONCE,MAX ACTIONS: 1
Give RhoD Immune Globulin if indicated
NW/New (S t art date 0 4/ 0 1/2~080 6 · - No Stop Da t e found -)
Ordered By.zt~•••••1f'-· DO (Electronic Signed By~ .. -..-11111Mt
ORO NUM:40,PB-HOME HEALTH CARE VISIT IF ELIGIBLE ONCE,MAX ACTIONS: 1
OB patient
NW/New(Start date 04/01/2
Ordered By: DO
0806 - No Stop Date found -)
(Electronic
ORD NUM:4l,SEQUENTIAL COMPRESSION DEVICES cont.
NW/New(Start date 04/01 /2 0806 - No Stop Date found -)
Ordered By .... ., 'Rf DO (E l ectroni<-
Signed By:
DO
DO
DO
Admitted: 04/0l7/~2~~r--------------------------------------------------jiijiiiiiiiiiiiiiiij~--------------------------
HT: 5 ft 7 in WT: 174 lbs 3 ozs
MRN: ~!:!::: ... Account: Age: 28 Sex: F
DOB: 01/08/~ . , NS Room/Bed: PAGE 03
E LECTRONI C ORDER REPORT
15

(
ALLERGIES: DIPHENHYDRAMINE
CC: C/S REPEAT
Sinc{air :Memoria{ J{osyita{ 444 West Tftira Street 'Dayton, Ohio 45402
ELECTRONIC ORDER REPORT
ADMITTING: ...... ... DO
Session Start: 04/01/2 0805
Entry Loca tion: YP&&b&#z•a Session Stop: 04/01/20
Run Date : 04/0 1/20
ORD NUM:42,CALL:DVT PROPHYLAX INDICATED & NO ORDER cent,
Notify Physician
NW/New(Start date 04/0l/20~ 0806 - No Stop Date found -)
Ordered By,....... ~~ Signed By: IT .JI.J liP , DO (Electronic
ORD NUM :43, LAB-CBC W/DIFF - COMPLETE BLOOD COUNT Qty: 1' ONCE,MAX ACTIONS: 1
date ID/DC'D(Start 04/01/20 ''
0811 -H)
Ordered By: DO (Paper Chart)
NW/New(Start date 04/02 /20. 0500 - Stop date 04 / 02/2"' 0500 -H)
Ordered By . DO ( ectronic )
ORD NUM:44, P/O C-SECTION VITAL SIGNS - SEE ORD REF cent,
NW/New(Start date 04/01/20 , 0807 - No Stop Date found -)
Ordered By !Ill. ···--·l!j-, DO (Electronic
ORD NUM:45, CHECK FUNDUS C-SECTION cent,
NW/New(Start date 04/01/20 0807 - No Stop Date found -)
Ordered By:.iilfM!Iitlii'IM!i! ll' DO (Electronic
ORD NUM:46, NOTIFY PHYSICIAN OF EXCESS LOCHIA RUBRA cent,
NW/New(Start date 04 / 01/20
Ordered By:U!fRIJM~ft' · DO
0807 - No Stop Date found -)
(Electronic
ORD NUM:47 , REMOVE ABDOMINAL DRESSING IN AM cent,
NW/New(Start date 04/01/2
Or dered By Wlllllii•IJI••• DO
0807 - No Stop Date found - )
(Electronic
ORD NUM:48, ABDOMINAL BINDER cent,
as needed
NW/ New(Start date 04/01/20 0807 - No Stop Date found -)
Ordered By ti!il!!lllllli!l···· DO ( E l ectron~ c
Admitted: 01/01/
5 ft 7 1n WT: 174 lbs 3 ozs
Age : 28 Sex: F
DOB: 01 /0 8/ 1
Signed By: USER PAPER-CHART
Signed By: liJb . a: Y , DO
Signed By: ! .. $ ••• , .. , DO
Signed By: ······~ DO
Signed By:1!iii······ DO
Signed By: ~····· DO
S1gned By : ••••. DO
MRN:
Account: NS Room/Bed:
ELECTRONIC ORDER REPORT
0811
0812
PAGE 04
16

Sinc{air Memoria{ J{osyita{ 444 West Tfiirc{ Street Vayton, Ohio 45402
ELECTRONIC ORDER REPORT
ALLERGIES : DIPHENHYDRAMINE
CC: C/S REPEAT
Entry Location: .IIII!IIJIPl!l\
ORD NUM:49, REMOVE STAPLES FROM INCISION cant,
at time of discharge
NW/New (Start date ~4/0l/24 0807 - No Stop Date found -)
Ordered B · • DO (Electronic
ORD NUM: so, PLACE STERI STRIPS cant,
at time of discharge ~
NW/New(Start date 04/01/2~ 0807 - No Stop Date found -)
Ordered B DO (Electronic
ORD NUM:Sl, ACTIVITY AS 'I;OLERATED cant,
NW/New(Start date 04/0l/20 , ., 0807 - No Stop Date found -)
Ordered By~ DO (Electronic
ORD NUM:52, DIET-FULL LI~ID DIET meals,
ID/DC ' D(Start date 04/0l/2~ 0809 - H)
Ordered By ·fl!.~~~~· fflllll!l!ll!liJJt DO
NW/New(Start date 04/01/20' 080 7 - Stop date 04/01/2
Ordered BV,······· DO
(Paper Chart )
0809 -H)
(Electronic )
ORD NUM:53,ADVANCE DIET AS TOLERATED cant,
NW/New(Start date 04/0l/20[ ' 0807 - No Stop Date found -)
Ordered B"· .~ D ~~Fr.tiM'-~, (Electronic
ORD NUM:S4,FOLEY CATHETER TO STRAIGHT DRAINAGE cant , 4
NW/New(Start date 04/0l/20 0807 - No Stop Date found -) t•
Ordered B ·.-' DO (Electronic )
ORD NUM:ss,DC FOLEY IN 8 HRS -UA, C&S FIRST IF ORDER cant
Oltai,-, UA, C&S !:lef .•·e dc'ing _, 0ydered
NW/New(Start date 04/01/2~ 0807 - No
·")rdc·H-d Hy ..... I!S!ill!l§;·l· DO
; Admltted- 04/01/2
Stop Date found -)
{E lectronic
HT: 5 ft 7 in WT: 174 lbs 3 ozs
Age: 2 8 Sex: F
DOB: 01/08
ADMITTING: ·~~~~ .... ~. Session Start: 04/01/2
Session Stop: 04/01/2
Run Date : 04/01/2
Signed By: ....... ~~!!!!~- DO
Signed By: tlfiiJIIIIJ!'·, DO
Signed By: ' DO
Signed By: USER PAPER-CHART
Signed By: DO
DO
Signed By:
.)( ..
ELECTRONIC ORDER REPORT
DO
0805
0811
0812
PAGE 05
17

ALLERGIES : DIPHENHYDRAMINE
C-Sinc{air :Memoria{ J{osyita{ 444 West Thirc( Street 1Jayton, Ohio 45402
ELECTRONIC ORDER REPORT
CC: C/S REPEAT ADMITTING: ,. .......... ~ DO
Entry Location:
ORD NUM:56, STRAIGHT CATH x 1 UNABLE TO VOID x 12hrs cont,
NW/New(Start date 04/01/20~0807 -No Stop Date found -)
Ordered By:f)g ••• p DO (Electronic )
ORD NUM :57,COMPLETE CURRENT IV AT 200 ML/HR, THEN cont,
NW/New(Start date 04/01/2,~ 0807 - No Stop Date found -)
Ordered By:d IJ-IIm Q DO (Electronic )
ORD NUM:58,IV DEXTROSE 5% AND 1/2 NS AT 125 ML/HR cont,
NW/New(Start date 04/01/2
Ordered By: DO
0807 - No Stop Date found -)
(Electronic )
ORD NUM:59, DC IV IN AM IF STABLE cont,
NW/New(Start date 04/0l/241t 0807 - No Stop Date found -)
Ordered By , DO (Electronic
Session Start:
Session Stop:
Run Date : 04/01/20 -
Signed By:····~J.II!-I!tt, DO
Signed By: Ql!\l!JI!MIIIIIf1,.DO
Signed By""!llflllllllii!,III··=~DO
ORD NUM:6o, ORDER ANTIBODY TITRE-IF RhNEG & BABY POS ONCE,MAX ACTIONS: 1
Give RhoD Immune Globulin if indicated
NW/New(Start date 04 / 01 /2~ 0807 - No Stop Date found -)
Ordered By:~ R 11M• DO (Electronic Signed By : •ti IIU!..,t DO
ORD NUM:6l,PB-HOME HEALTH CARE VISIT IF ELIGIBLE ONCE ,MAX ACTIONS: 1
OB patient
NW/New(Start date 04/01/2
Orde red By: DO
0807 - No Stop Date found -)
(Electronic
ORD NUM: 62, CALL: DVT PROPHYLAX I NDI CATED & NO ORDER cent,
Notify Physician
lm/New(Start date 04/01/2
Ordered By :IJiiilliillrilf
Admitted 04/01/2~
DO
0807 - No Stop Date found -)
(Electronic )
HT: 5 ft 7 in WT: 174 lbs 3 ozs
Age: 28 Sex: F
DOB: 01/08/1-
Signed By:~ii{liljj(MIIJ •• jiW
DO
ELECTRONIC ORDER REPORT
0805
08 11
08 12
PAGE 06
18

Sinc[air Memoria[ J{osyita[ 444 West 'lfiira Street 'Dayton, Ohio 45402
ELECTRONIC ORDER REPORT
ALLERGIES : DIPHENHYDRAMINE
CC: C/S REPEAT
Entry Location : BPI&2~
ORD NUM :63, P/O C-SECTION VITAL SIGNS - SEE ORD REF cont,
NW/New(Start date 04/01/20~0809 - No Stop Date found -)
Ordered By (Electronic )
ORD NUM:64, CHECK FUNDUS C-SECTION c ont,
NW/New(Start date 04/01/20,., 0809 - No Stop Date found -)
Ordered B , DO (Electronic
ORD NUM:6s, NOTIFY PHYSICIAN OF EXCESS LOCHIA RUBRA cont,
NW/New(Start date 04/01/2~ 0809 - No Stop Date found -)
Ordered B) b [j'ip -~t, DO (Electronic
ORD NUM :66, REMOVE ABDOMINAL DRESSING IN AM cont,
NW/New(Start date 04/01/2~ 0809 - No Stop Date found - )
Ordered By--@?S'~ DO (Electronic
ORD NUM:67, ABDOMINAL BINDER c ont,
as needed
NW/ New(Start date 04/01/20 0809 - No Stop Date found -)
Ordered By : V''i!l · 1Ui•L• DO (Electronic
ORD NUM :6s ,REMOVE STAPLES FROM INCISION cont ,
a t time o f d i scharge
NW/New(Start date 04/ 01 / 20 0809 - No Stop Date found -)
Ordered By ~= llll .. li~~ DO (Electronic
ORD NUM :69, PLACE STERI STRIPS cont,
at t i me of discharge
NW/ New (Sta rt da.te 04/01/2 . 0809 - No Stop Date found ·I
Ordered By !tflilllliiiJIIIilfiiW DO (Electronic
ADM! TTING : ~>{!dlddliiiJ···~
Session Start: 04/01/2
Session Stop: 04/01 / 2
Run Date :
Signed By ::'Jlllf!lllli!JIII\i.M~r,. DO
S i gne d By :······rt, DO
Signe d By~~ DO
Signed By: ·~~~~-~- .~,I!J,~-.. ~'· DO
Signed By·- ~~~~~~· DO
s.gned By -~ifiti'M·jil~ DC
DO
0805
ORll
0812
cdmitted: 04/01/2~;---------------------------------------------------~~--.. --~~--~~~--~----------------------------IT: 5 ft 7 in
ge: 28 Sex: F
0 8 : 01/0 8 /1
WT: 174 lbs 3 ozs MRN : '•2 UD IR J Account : MMIJJJt• NS Room/Bed: ~~11 .. 1111~- ~
ELECTRONIC ORDER REPORT PAGE 07
19

IF DICTATING DISCHARGE SUMMARY ON UNIT, USE THIS FORM TO DICTATE MEDICATIONS FROM. IF DICTATING DISCHARGE SUMMARY lATER DICTATE FROM THE LOGICARE MEDICATION SUMMARY.
PATIENT HEIGHT 11 · PATIENT wEIGHT I'll/ IPs (KG)
Do have any Medication, X-Ray Dye, Food, Environmental, Latex Allergies?
0 NO KNOWN ADVERSE REACTIONS OR ALLERGIES S -- List below and include the type of reaction
ALLERGY AND TYPE OF REACTION ALLERGY AND TYPE OF REACTION
DATE I TIME RECONCILING NURSE SIGNATURE
ADDITIONAL DISCHARGE MEDICATION ORDERS
·-------------------------------------------· Patients with a diagnosis of Ml, Heart Failure, Open Heart Surgery, or Percutaneous Coronary lnteJVention (PCI) : Evidence Based Medicine and National Quality Measures recommend these patients be on Aspirin, Beta Blockers, Ace Inhibitors (ACEI) or Angiotension Receptor Blocker (ARBs).
Product name Dose Frequency
- -·--------···-·-·-·-------·-·--____j_ __________ j ________ ,, ____ . __ , ___ _ ! i I - ---- -.-1 -----r-·
Route or Topical Site
~ --- --- -
--~~ -----I - 1 - -
_----=---~~-=-+~~~----= I ----- .... __ ----- ·--· -- ·-----+-----r _:_:::- -:-:---= - -- -----
~~~~~-~~~~~~~~~~~------Sinc{air Memoria{ J{ospita{
PHYSICIAN ADMISSIONAND DIS'CFfARGE MEDICATION RECONCILIATION ORDERS K7510-010 ~FRONT ©K-IdU .... IllPI ' u"""
...... -------· /28
Page __ of __ 20

ALLERGIES: DIPHENHYDRAMINE
CC: C/S REPEAT
Sinc[air Jvlemoria[ J{osyita[ 444 West Thircf Street 'Dayton, Ohio 45402
ELECTRONIC ORDER REPORT
ADMITTING:
Session Start: 04/01/2 · 0805
oRD NUM:63, P/O C-SECTION VITAL SIGNS - SEE ORD REF cent,
NW/ New(Start date 04/01/20 0809 - No Stop Date found -)
Ordered By ,qQ]jl!U!IIIJI• DO (Electronic )
ORD NUM:64, CHECK FUNDUS C-SECTION cent,
NW/New(Start date 04/01/2 0' 0809 - No Stop Date found -)
Ordered BY'=••· .. ··~ DO (Electronic
ORD NU!-1:6s, NOTIFY PHYSICIAN OF EXCESS LOCHIA RUBRA c e nt,
NW/New(Start date 04 / 01/2~0809 - No Stop Date found -)
Ordered By :1 DO (Electronic
ORD NUM:66, REMOVE ABDOMINAL DRESSING IN AM cent,
NW/ New(Start date 04/01/2~ 0809 - No Stop Date found -)
Ordered By:•; S !IIIJU'f DO (Electronic
ORD NUM :67, ABDOMINAL BINDER c ent,
as needed
NW/ New(Start
Ordered By: _.. •• lilllllfijoo. 0809 - No Stop Date found -)
(Electronic
ORD NUM :68, REMOVE STAPLES FROM INCISION cent ,
at time of discharge
NW/New (Start date 04/01/20 . 0809 - No Stop Date found -)
Ordered By:·!''C'Iiiii •• !J DO (Electronic
ORD NUMo69, PLACE STERI STRIP S cent,
at time of discharge
NW/New(StarL date 04/01/20 0809 - No Stop Date found -)
Ordered RY 'tldllJI£1&811••1EIIIb -1118; EJ0
Admitted: 04/01/~
HT· 5 ft 7 in WT: 174 lbs
Age: 28 Sex: F
DOB: Ol/08/ .
(Electronic
3 ozs
Session Stop: 04/01/2
Run Date : 04/0 1/2 '
Signed By,'- H Ill. DO
Signed By: .-...... If.:. DO
Signed By: DO
Signed By DO
DO
Signed By: ~~~~llllll DO
MRN:
Account: NS Room/Bed :
ELECTRONIC ORDER REPORT
0811
0812
PAGE 07
21

(
t~" = '-=-
Sinc(air :Memoria( J{osyita( 444 West 'Third Street Vayton, Oliio 45402
ELECTRONIC ORDER REPORT
ALLERGIES : DIPHENHYDRAMINE
CC: C/S REPEAT
Entry Location:
ORD NUM:7o, ACTIVITY AS TOLERATED cont,
NW/New(Start date 04/01/20
Ordered By:•UJMiil!mlili .I .aaoo 0809 - No Stop Date found -)
(Electronic
ORD NUM:7l, DIET-FULL LIQUID DIET meals,
NW/New(Start date 04/01/2011 0809 - No Stop Date found -)
Ordered By: •lilll!illl.l£11 4!lifli!.lll DO (Electronic
ORD NUM:72, ADVANCE DIET AS TOLERATED cont,
NW/New(Start date 04/01/2011 0809 - No Stop Date found -)
Ordered By:S2t E ..... DO (Electronic
ORD NUM:73, FOLEY CATHETER TO STRAIGHT DRAINAGE cent,
NW/New(Start date 04/01/24 0809 - No Stop Date found -)
Ordered By :oi • .... MN!Iflllll;; DO (Electronic )
ORD NUM:74, DC FOLEY IN 8 HRS-UA, C&S FIRST IF ORDER cont,
Obtain UA, C&S before dc'ing if ordered
NW/New(Start date 04 / 0l /2 0tr 0809 - No Stop Date found -)
Ordered By :J!I!II&II•M•Ifi&, DO (Electronic
ORD NUM:7s,STRAIGHT CATH x l UNABLE TO VOID x l2hrs cont,
NW/New(Start date 04/0l/20 4l 0809 - No Stop Date found -)
Ordered By . DO (Electronic
ORD NUM :76,COMPLETE CURRENT I V AT 2 0 0 ML / HR , THEN cont,
No St op Date f ound -)
(Electronic
ORD NUM: 77, IV DEXTROSE 5% AND 1/2 NS AT 125 ML/ HR cont
NW/NewiStart date 04/0l/2
0rdered By~~~ .. ~~
Adm1tted. 04/01/2
DO
0809 No Stop Dat~ fo~~d
(Electronic
HT: 5 ft 7 in WT: 174 lbs 3 ozs
Age : 2 8 Sex : F
DOB : 0 1/0 8
ADMITTING:._~~~~~~~~ .. Session Start: 04/01/2
Session Stop: 04/01/2
Run Date 04/01/2
signed By: ~Mth•-..oo
Signed By:.,'lii . • !III!III!IIJa,.po
Signed By:·~ .•. MMiiil.l*' · ··a DO
Signed By: ·~~~~~~~~~~~·' DO
Signed By: ,.! $'JIM l DO
Signed By : DO
Signed By: ....... ,DO
Signed By
ELECTRONIC ORDER REPORT
c.
DO
0805
0811
0812
PAGE 0 8
22

,~
ALLERGIES: DI PHENHYDRAMINE
f f= ~·
Sinc{air Jvlemoria{ J{osyita{ 444 West Thira Street 'Dayton, Ohio 45402
ELECTRONIC ORDER REPORT
CC: C/S REPEAT
En t ry Locat ion: ~ .. ~~~
ADMITTI NG: . ••m• & •, DO
Ses s ion St art: 04/01/2 J
Session Stop: 04/01/2
Run Da te : 04/01/2rJ.
0805
0811
0812
ORD NUM:78, DC IV IN AM IF STABLE cont .
NW/New(Start date 04/01/2~ 0809 - No Stop Date found -)
Or dered By~-~-· DO (Electronic
ORD NUM:79, 0RDER ANTIBODY TITRE-IF RhNEG & BABY POS ONCE,MAX ACTIONS: 1
Give RhoD Immune Gl obul in i f ind icated
NW/New(Start date 04/01/20,0809 - No Stop Date found -)
Order ed By: ~l~d~JIIIIr DO (Electronic Signed By: MIIIJ~·, . DO
ORD NUM:80 , PB-HOME HEALTH CARE VISIT IF ELIGIBLE ONCE,MAX ACTIONS: 1
OB patient
NW/New(Start date 04/01/20~ 0809 - No Stop Date found -)
Or de r ed By: d f(I!.Mllf. ', DO (Electronic
ORD NUM:81, MEDICATION COMMENT Dose : 1 EACH, IV, q24hr,
USE DURAMORPH PROTOCOL X 24 HR
NW/New (Start date 04 / 01/2~ 0810 - Stop date 04 / 02/2011 0809 -S )
Ordered By: mqt 111111 . DO (Electronic )
Current Status: AU/Pending
Signed By: DO
ORD NUM:82, METHY LERGONOV INE 0.2MG /ML AMP I N J Dose: 0.2 MGS, IM, prnq8, PRN,MAX ACTION
EXCESSIVE VAG BLEEDING, IF NO HTN (MAY GIVE X 2 DOSES)
Current Status: AU/Pending
NW/New(Start date 04/0l/20~' 0810 - No Stop Date found -H)
Ordered By:~, DO (Electronic) Signed By: --~~lilll!llllf!~, DO
ORD NUM: 8 3, METHYLERGONOVINE 0 • 2MG 'l'AB Dose: 0. 2 MGS, PO, prnq8, PRN, MAX ACTIONS: 6
EXCESSIVE VAG BLEEDING, IF NO HTN 18 HOURS AFTER LAST IM DOSE)
NW/New(Start date 04/01/2 - 0810 - No Stop Date found -H)
Ordered r:vi."~ DO (Electronic}
Admitted: 04/01/2~ HT: 5 ft 7 in
Age: 2 8 Sex: F
DOB: 01/08/1~
WT: 174 lbs 3 ozs
Current Status· AU / Pending
·• ,_ .. ,, ... MRN: ra •1 zr Account .t4t••••-r N S Room/Bed: 1\ID1l,,ll!il.f
ELECTRONIC ORDER REPORT
PAGE 09
23
ALLERGIES: DIPHENHYDRAMI NE
Sinc{air Jvlemoria{ Jfosyita{ 444 West Tfiircf Street Dayton, Ofiio 45402
ELECTRONIC ORDER REPORT
CC: C/S REPEAT ADMITTING: "'')iiilllililiillliilllifMiii~t~DO
Entry Location: i' .... t\l Session Start: 04/01/20 0805
Session Stop: 04/01/20
Run Date : 04/01 / 20
0811
0812
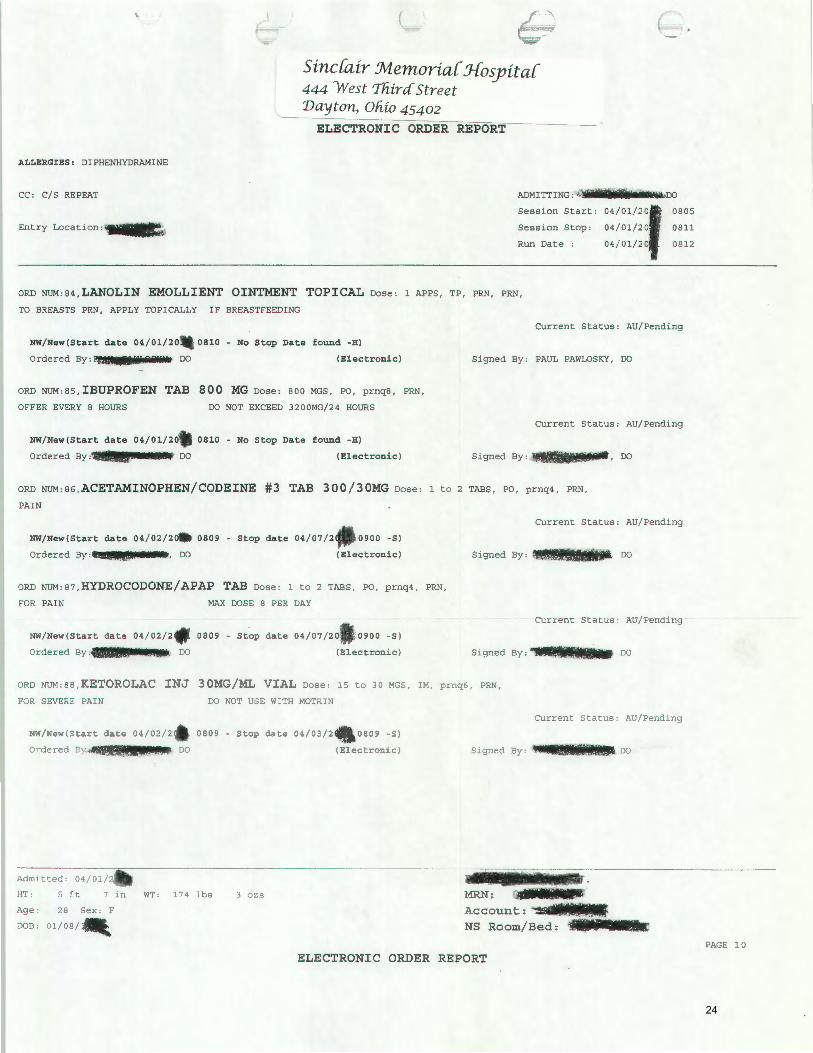
ORD NUM:84,LANOLIN EMOLLIENT OINTMENT TOPICAL Dose: 1 APPS, TP, PRN, PRN,
TO BREASTS PRN, APPLY TOPICALLY IF BREASTFEEDING
NW/New(Start date 04/01/20,..0810 - No Stop Date found -H)
Ordered By:J!lll-tH23JIJi' DO (Electronic)
ORD NUM:85, IBUPROFEN TAB 800 MG Dose: BOO MGS, PO, prnq8, PRN,
OFFER EVERY 8 HOURS
NW/New(Start date 04/01/20
Ordered By :11!111·~--· DO
DO NOT EXCEED 3200MG/24 HOURS
0810 - No Stop Date found -H)
(Electronic)
Current Status: AU/Pending
Signed By: PAUL PAWLOSKY, DO
Current Status: AU/ Pending
Signed By: !.J!I .. Lii!iiJfJ!IWi•· DO
ORD NUM : 86, ACETAMINOPHEN/CODEINE #3 TAB 300/30MG Dose: 1 to 2 TABS, PO, prnq4, PRN,
PAIN
NW/New(Start date 04/02/2~ 0809 - Stop date 04/07/2 0900 -S)
Ordered By :t'llii!!U£•tllii!lillllil. •u-•. DO (Electronic)
ORO NUM:87,HYDROCODONE/APAP TAB Dos e : 1 t o 2 TABS , PO, prnq4 , PRN ,
FOR PAIN MAX DOSE 8 PER DAY
NW/New(Start date 04/02/2 . 0809 - Stop date 04/07/20 , ' 0900 -S)
Or dered By:UQ$ tO. DO (Electronic)
Current Sta t us: AU/ Pending
DO
Curre n t Status : AU/ Pending
Si gned By : ,. .. ll .. lllll DO
ORO NUM:BB, KETOROLAC INJ 3 0MG/ ML V IAL Dose: 15 to 30 MGS, IM, prnq6, PRN,
FOR SEVERE PAIN
NW/New(Start date 04/02/2
Ordered By~~~~~~l'~~
Admitted. 04/01/
DO NOT USE WITH MOTRIN
0809 - Stop date 04i03/ 2
DO
Current Status: AU/Pending
0809 -S)
{Electronic ) S1gned By: ...... DO
HT: 5 ft 7 in WT: 174 lbs J ozs MRN: Age: 28 Sex: F
DOB: 01/08/
Account : ~~--.. ~~ NS Room/Bed:
ELECTRONIC ORDER REPORT
PAGE 1 0
24

Sinc{air :Memor ia{ Jfosyi ta{ 444 YVest 'lliira Street 'Dayton, Oliio 45402
ELECTRONIC ORDER REPORT
ALLERGIES : DIPHENHYDRAMINE
CC: C/S REPEAT
Entry Location: lffl.(;i .. ...,..
ORD NUM:89 ,0NDANSETRON INJ 2 MG/ML PF VIAL Dose: 4 MGS, IV, prnq8, PRN,
FOR NAUSEA/VOMITING
NW/New{Start date 04 / 02/20- 0809 - No Stop Date found - H)
Ordered By:>). ilfJ!IIrJIIIIIfll.lillw.., DO {Electronic)
ORD NUM:9o, ZOLPIDEM TAB 10 MG Dose: 10 MGS, PO, prnhs, PRN,
INSOMNIA
NW/ New {Start date 04 / 02 /2 0 • 0809 - No Stop Date found - H)
ADMITTING :
04/0l / 2, , ~Rns 04/01/20 0811
04/01/2 0812
Session Start:
Session Stop:
Run Date :
Current Status: AU/Pending
DO
Current Status: AU/ Pending
Ordered By;'IIJIIIIJ····- {El ectr oni c) Signed By: ·:i· ..... .. DO
ORD NUM:9l ,CETYLPYRIDINIUM/MENTHOL LOZENGE Dose: 1 EACH, PO, PRN, PRN,
NW/New {Start date 04 / 01/2
Ordered B DO
0 810 - No Stop Da te f ound -H)
{Elec t r onic) Signed By:
Current Status: AU/ Pending
ORD NUM: 92, SENNOSID ES/DOCUSATE 8 . 6 /SOMG T AB Dose: 1 to 2 TABS, PO, prnqd , PRN,
CONSTIPATION
Current Status : AU/Pending
NW/New{Start date 04/01/20. 0810 - No Stop Date found -H)
Ordered By11JII···· DO {Electronic) Signed By : llllitj1Ji!lfi8Ji~ DO
ORD NUM : 93, SIMETHICONE TAB CHEWABLE 80 MG Dose: 160 MGS, PO, prnq6, PRN,
INDIGESTION
NW/ New{Start date 04/01/2
Ordered By: , DO
0810 - No Stop Date found -H)
{Electronic}
Current Status: AU/Pending
Signed By: 11= ;zai!lfo DO
dmitted: 01/01/20, ~~~~~~~~~~~~~~~~~~jJS~~~~~~~~-J~P~~~-~~~·~~~~~~~~~~~~~~~~~-T: 5 ft 7 1n WT: 174 lbs 3 ozs MRN:
Account: ~~~===~lll!llll NS Room/Bed : "'! Je: 28 Sex: F
' lB: 01/08 /.
PAGE 11
ELECTRONI C ORDER REPORT
25

ALLERGIES : DIPHENHYDRAMINE
CC: C/S REPEAT
Entry Location: ~ii~
I c
Sinc[air :Memor ia[ Jfosyita[ 444 West Tfi ira Street 'Dayton, Ofii o 4 5402
ELECTRONIC ORDER REPORT
Session
Session
Run Date :
ORD NUM:94, MAG & AL HYDROX/SIMETH EXTRA-STR SUSP Dose: 30 MLS, PO, prnq6, PRN,
INDIGESTION USE FOR MYLANTA
OA05
0811
0812
Current Status: AU/Pending
NW/New(Start date 04/01/2
Ordered By:(!· m!!Mlii •• IJ. f(~ DO
0810 - No Stop Date found -H)
(El ectronic ) Signed By: '¥ !J ll na. DO
ORD NUM:9S, BISACODYL SUPPOSITORY lOMG Dose: 10 MGS, RECTAL, PRN, PRN,
IF REQUESTED
NW/ New (Start date 04 / 01 /~ 0810 - No Stop Date found - H)
Ordered By. " , DO (Electronic )
ORD NUM:96, 0XYTOCIN Dose: 20 UNITS, IV, 125.0 rnl/hr, TITRA, PRN,
OXYTOCIN 20 UNITS/LR lOOOML, MAX 200ML/HR POST PARTUM BLEEDING
OXYTOCIN 20 UNITS,
RINGERS SOLUTION, LACTATED 1000 MLS,
NW/ New(Start date 04 / 01/2 . 0810 - No Stop Date found -H)
Ordered B ,DO (Written)
ORD NUM:97, SEQUENTIAL COMPRESS I ON DEVI CE S cont,
NW/New( Start da t e 04/ 01/2 . 080 9 - No Stop Da te found -)
Ordered By: DO (Electronic
ORD NUM:9a,CALL :DVT PROPHYLAX INDICATED & NO ORDER cont,
Notify Physician
NW/New(Start date 04/01/2
Ordered By: DO
0809 - No Stop Date found -)
(Electronic
Current Status: AU/Pending
Signed By :,..£
Current Status: AU/Pending
Current Status:
Signed B)X1l.lfillliii!MI!!J~$DO
ORD NUM:9<?J,LAB-CBC W/DIFF - COMPLETE BLOOD COUNT Qty: 1, ONCE,i'IIAX ACTIONS: l
NW/New(Start date 04/02/2
Orden~d By
drnitted: 04/0lt~
0500 - No Stop Date found -)
(Electronic Signed B)~········lt!)C
T: 5 ft 7 in WT: 174 lbs 3 ozs MRN: •'!>
Ac c o unt: ~~~=~~;~··~·: -~ NS Room/Bed :
3e: 28 Sex: F
JB: 01/0S&IIf
EL ECTRONIC ORDER REPORT PAGE 12
26

Sinc[air Memoria[ Jfosyita[ 444 'West T'fz ira Street 'Dayton, Oliio 45402
ELECTRONIC ORDER REPORT
ALLERGIES: DIPHENHYDRAMINE
CC: C/S REPEAT
Entry Location: is tOll
ORD NUM:17, INSERT PERIPHERAL IV: #18- #20 ANGIOCATH cont,
NW/New(Start date 04/01/20 ' 0639 - No Stop Date found -)
ADMITTING:
Session Start:
Session Stop :
Run Date :
..
DO
04/01/2 , 0639 04/01/2 0639 04/01/20 0640
Ordered By·~ .. IJlliiiiiJIIIi.M,; DO (Electronic ) Signed By: iii!fiilllil.llliJilj··· DO
ORD NUM:18, LACTATED RINGERS AT 125 ML/HR cont,
NW/New(Start date 04/01/2 0639 - No Stop Date found -)
Ordered By:-<· •••••····~ DO (Electronic Signed By: jl······~~·- DO
' ORD NUM:19, FOLEY CATHETER-INSERT PRE-OP ONCE,MAX ACTIONS: 1
NW/New(Start 0639 - No Stop Date found -)
Ordered By~~~MI~~~~~~~~ .. ~ DO (Electronic Signed By: 4dlfillllill•······ DO
ORD NUM:20, IF AP RECORDS NOT AVAIL-CALL DR OFFICE ONCE, MAX ACTIONS: 1 NW/New(Start - No Stop Date found -)
Ordered B:~~IIIIIIII .... ~~~J DO
Admitted: 04/01/ HT : 5 ft 7 1n WT: 174 lbs
Age: 28 Sex: F
DOB : 0 1 /08~
3 ozs
(Electronic Signed By:~-lil~ifiiillllllfli •• DO
'•
MRN : ~~~~~~ Account:
NS Room/Bed:
ELECTRONIC ORDER REPORT PAGE 02
27

c Sinc(air Memoria( J-fosyita( 444 West 'lfiira Street 'Dayton, Ofiio 454 0 2
COMPREHENSIVE PLAN OF CARE INTEGRATED PROGRESS NOTE
AT -Art Therapist C - Case Manager
Ch - Chaplain D - Dietician/Diet Technician
ET - Enterostomal Therapist
FORM GS0380U (03/07)
LC - Lactation Consultant N - Nursing
OT - Occupational Therapist 0 - Other (specify in code)
PT- Physical Therapist
P - Physician RT - Recreational Therapist
R - Respiratory SP- Speech Therapist SS - Social Service
blue
28

./ /=
Sine fair :Memoria( J-{osyita( b 444 'West Tfiirc{ Street
Dayton, ofiio 45402 Physician's L & D Progress Entry
Entry Time: 4/1/2 05:25
Pt. Admit Date : 04/01 · 06:19 EDT
EDC: 03/27 Gestational Age: 40.8
Fetal Monitor Strip Reviewed:ves
FHTs
Fetal Monitor Strip Status: Active
Contractions:
Intrapartum Procedures:
Admit Plan : CSection
L & D Progress Notes:
Gravida Term Preterm AB Living 5 2 2
Membrane Rupture
Patient Seen: Yes Vitals Reviewed: VS_WNL
Labor Curve ReYiewed:1 1 d t• t<eason .or n uc ton:
pt to LQ. for repeat c/s without tubal. previous c/ s x2 . pt counseled on r/ b/c/a and pros/cons and accepts. will proceed with c/s.
Documentation by:
Sinc(air :Memoria( J-{osyita( ~ I'U'1
__ ... - -, .
444 'West Tfiircf Street MR# • ,,. 1 Acct#
'Dayton, Ofiio 45402 DOB ' Age 28
Date Printed 4/1/2.06:21 h UNIT LD-.r .
Bed 1390-A Printed By : DO Attending : ·- Adm Date:
I'J'c, "" :c;·::.~:- :~;' .,
' 1.!: ' ", !
sinc(air :Memoria( J-fosyita( Physician's L & D Progress Entry 444 'West Tfiircf Street 'Dayton, Ofiio 45402
04/0l;f'06:19 EDT
,, ·~ '
·'
Page 1 29
I also understand that m) surgeon or his agent may wke photographs and/or videotape the surgery. The usc\\ ill he only tor medical.
~cientitic. {lr cuucati\lnal purposes. !VIy identity i~ not to be revealed by the pictures or descripti1-e te:-as accompanying them .
I authorize release of my social security number if necessary. w enahlc..IS •• III!EP . ...., Sinc[air Jvlemoria[ J-fosy ita [ ' to meet regulatory requirements or the Safe Medical Devices or other federa l or state laws. •
I undcrst<Jnd that an) ONR (Do Not Resuscitate) {>rdcr is automatically rescinded Juring the operating and recovery period. I am
:1ware that the practice l'f medicine and surgery is nt>l an o :act scicnr:•:. <Jnrl I acknowledge that no guarantees have been made to me
as to the resu lts or trcatmenL~ or examination in the hospiwl.
I have read the above and have had the ·appropriate procedure(s) explained to me in detail. all questions have been ansvven;d to my
to the performance of the designated proccdurc(sl.
-----·---------f----·-·:_f ____ · --Date
'
Signature or RelativeiRepresentativeior Parent/Guardian's signature necessary if patient ts under 18 years of age and not an
emancipated minor. if patient is incompetent. or i r patient is unconsciou s l.i r required):
Relationship to patient Date
_____ i-:!:: Date
DS-2679 Page 2 of 2 05-07
30

L WOMEN'S CENTER at
Sinc{air :M.emoria{ J{ospita{ 444 West Tfiirc[ Stree t Dayton, Ofiio 45402
( .
Stamper
Labor and Delivery Consents INFANT CARE CONSENT
{
Infant's follow-up Physician is: _...~..U~f'I:...../I..__:....VI~O~·uJ:.:.._h...~...--___________ _
have designated __ O_n..:..-5_ {_-te __________ for the care of my infant. Physician's Name
I presently do not have a physician to care for my infant for the initial physical examination or discharge of my infant. I understand that a physician on staff of · · · ,\_o/ill care for my infant, for a fee, while in the hospital. I understand that findings at the time o · examination~and discharge are inclusive only of hospitalization. I understand that I am responsible for obtaining appropriate continuing medical care for my infant, including making an appointment for a check-up for my infant, based on the advice of my infant's examining physician.
BIRTH INFORMATION RELEASE
-tJPermfs"'si;n is hereby granted for Sinc{air .Jvtemoria{to release information to:
TELEPHONE INQUIRIES
V YES __ NO Concerning the Mother of Infant. This includes general condition, Room and telephone numbers.
ONLY THE INFORMATION MARKED YES MAY BE RELEASED.
CONSENT FOR PHOTOGRAPHS, AUDIO AND VIDEO TAPING
hereby give consent for family members and/or friends to photograph, audiotape, and videotape myself and my by during our hospital stays. I understand that the physicians and/or hospital employees included in such
· activities must give their verbal consent. ! also understand that the activities must be discontinued upon the request of the physician and/or the hospital employee. In connection therewith , I hereby release and agree to hold harmless Sinc[air :M.emoria[- and Family Health Center, its personnel. representatives, attending physicians and any other persons involved , from any liability concerning the taking or use of said photographs, audiotaping and/or videotaping.
RELATIONSHIP __ 'S;:_:1_ .. ~_/ _/-_~ --------
DATE lf// ~ TIME -------
DS-1379 1/11
31

Regional Anesthesia Orders Soinal I Eoidural I Extremity Sinc{air_ _.1vteJ?1oria{ J-fosyita[
The pat~ has received ~ .J t"L1 ..,EfDuramorph 0 DepoDur dntrathecal 0 Epidural :f'vmg a( "Jot'_
0 Continuous ~ngle-shot _______ regional anesthetic~_;:;;---J
Epidural 0 catheter D Level. _____ _
j This protocol will remain in effect until on·,..-,-,----,---,---..,..---,----j During this period no additional narcotics or sedatives are to be given to the patient unless ordered by or cleared with the Anesthesia on-call.
These orders ~ meet this requirement. j IV access must be maintained during this time period. j Elevate head of bed 30 degrees first 24 hours. Infusion solution: (prepared by 0 Pharmacy I 0 Anesthesia with preservative-free 0.9% NaCI)
Local Anesthetic (Methylparaben Free) D Bupivacaine 0 Ropivacaine 0 Lidocaine D Mepivicaine 0 Nesacaine Concentration %
Narcotic D Fentanyl 0 Morphine meg or mg /ml Amount or Concentration mg __ I __ %
j j j
0 Other .,--------,-,---c-:----:-,.,..--,---:--:-~-=----:--Run infusion @ __ ml.hr, then titrate in 1 ml/hr increments to comfort. Range to ml/hr. Inspect catheter site q 8 hrs - Notify anesthesia if catheter dislodged, excessive redness, discolored discharge. If lower extremity numbness or inability to move the lower extremities, stop the infusion and notify anesthesia on-call.
Patient Assessments Vital Signs: P, R, BP, 02 sats before procedure·,
BP q 3-5 min for 15 minutes following placement, t11en q 15 minutes x4, then q 30 minutes or more often if indicated
Aldrete Score: Obtain baseline prior to Epidural insertion, At beginning of recovery and prior to transfer or change of status (see key below for specifics)
Pain status: Every 4 hours Position change: Every hour as tolerated while awake Duramorph: After insertion, place on continuous oxygen monitoring,
Document 02 sats q 15 minutes x 8 until recovery complete Continue documenting 02 sats & Respirations q hour x 12.
if any additional narcotics given post-op, continue
Pain
documenting 02 sats and Resp . q hour for 24 hours. if 02 sat 92% or less, place 02 via nasal cannula @ 2-6 liters and call anesthesia.
~-= Tylenol 650 mg PO/PR q 4 hrs PRN r:-:: Toradol 30 mg IV q hrs. hold If Creatintne > 1.4 [' Celebrex 100 mg 1-2 tablets PO BID PRN Oj)arvocet N-1 00 1-2 tablets PO q 4 hrs PRN E1 jicodin 5/325 1-2 tablets PO q 4 hrs PRN efPercocet 5/325 1-2 tablets PO q 4 hrs PRN
Itching G?Benad~ mg IV/PO q 4 hrs PRN (Hold if pt 2 65 y/o) 0 Vistaril __ mg IM/PO q 4 hrs PRN (Hold if pregnancy or Asthma)
arcan 0.1 mg Sub-Q q 2 hours PRN Nubain 5mg IV/Sub-0 q 6 hrs PRN
~~ Zofran mg IV q 6 hrs PRN 0 Reglan 1 mg IV q 6 hrs PRN 0 Scopolamine Transdermal patch T q days 0 Other~------
Respiratorv I Sensory Peoressipn If Resp 8, give Narcan 0.1 mg IV. Repeat Q 5 min. PRN. Notify Anesthesia on-call Immediately.
Urinary Retention D Straight catheter 0 Other_
the Anesthesia on-call for any pain
k you .
Signed: __ _
Date: ___ -&
TOTAL MODIFIED ALDRETE SCORE= 10 IF .::;,5 NOTIFY PHYSICIAN 6-7 Remain in Acute Care Setting* 8-10 Transfer to Unit or Discharge *Must include at least a 2 in respirations or a return to baseline SCORE
Respirations Deep breath, cough freely Dyspnea or limited breathing Apnea
2 Blood Pressure BP=20mm Hg Pre-anesth. level 2 BP=20-50mm Hg Pre-anesth. 1 BP= 50mm Hg Pre-anesth. level o
Consciousness Fully Aware Arousable
2 1 0
Oximeter 02 Sat >92 on R/A 2 02 Sat >90 w/02 1
Activity Scores Able to move 4 Extremities = 2 Able to move 2 Extremities = 1 Able to move 0 Extremities = 0 0 Not Responding 02 Sat <90 w/02 o
DS-2783 8/09 32

{
reassessed immediately preop and frt to proceed with planned
J..=:..:..:::...:...:.:.:::...:...=...:.:..-.J---+--+---+---lf---1---.J-----+--+---t---f---lf----l ~=~:: :::~:~::"::nned
~=~:.:.:.._..t---+---=-~---+-----lf-----+-----lf------+----1f----+----lf------+---1 ~PIN At: o 7of/ j!YL L·07t3
~-----------4----~----~---+----4---~~--~----+----1----~----r----+----~ (/I : 07t f{
'011r ~~~~+-r-~'---1--+--+-1---+--+-+---+-----t--+------1 f""'" 017,()
• X
e Ci
0
HR
START 180 ANES 170 START 160 OP 150 END 140 OP 130
END 120
ANES 110 100
RESP. 90 80
0
0'
c.:
Position: Sitting 0 Lateral
Levji:.Jdi-S ~~~~~~~~~~~~~~=~=t=t=~=~=~=~=~~~~=~=t=t=~=~=~=~=~~~~=~=~=~=t=~=~=~=~=~~~~=~~ cfJterile Prep /), ci 1% Lidocaine to skin/SO _t/_ml
Needle:
Loss of resistance with (for epidural):
OAir O Saline
Djes D No
[ii(ves D No
~.j-~'"'-4--t-..f-..;.4-f.~_,.-f-I-I-I~~~I-+-+-+-+-+++++-+-+-+-+-+-I-I-1H Paresthesia: 0 Yes 0 No
l~+-+-+-++-f-+-+-+~-+-f-I-I-I~~I-I-+-+-+-+-+++++-+-+-+-+-+-I-I-1H 0 Catheter advanced __ em r & Secured I Dressed
Epidural Test dose: ___ ml
~+-+-+-++..f-~..:j.l*~~-f-1-1-1~~1-1-+-+-+-+-+++++-+-+-+-+-+-1-1-H LJ Lidocaine 1.5% with epi ~~d-+~d-+~~-t~~--f-l-l-lf--f--f--1-t-t-t-~~~~~+-+-+-t-t-t-i-l-,ri O rnher· __________ _
~~+--HH-++-If-*--+H-~~-1-I-If--f--+--1-i-1-i--t-+++++-+--+-+-t-t-t-i........JH Bolus: __ ml Rop1vaca1ne 0.2% & Fentanyl 2.5 mcg/ml
Other:------
N/G /
Insensible -.,,1!/;___ __ _ TOTAL __ / _ __ _
08 ANESTHESIA RECORD
Applicable Items: [/'Arms Tucked
~_Armboards ~ Pressure points j 'd I
D Vent O TV: __ O R _ _ _
E~ 3 D yLeads !6 NIBf'lD L [!)' R
~Arm 0 Forearm
D)lerve Stim
0 Radial 0 Axillary O AIIens. ___ _
0 Fowlers I protected
0 Lateral O Air Blanket
0 Fluid Vllarmer
0 Intubation-Size __ _
0 Oral 0 Nasal 0 Bilat Breath Sounds
0 Taped 0 Atraumatic 0 ETC02 +
O BIS
~Eyes: O CVP/PA
0 Lubed 0 Taped
Ds-2491 6104
D SCCOz Absorption
0 <;6z Analysis
&'Pulse Oximetry 33

Entry Time: 4/1/20
Allergies Drugs/Medications: Yes
Foods: No Latex:
Diagnosis/Procedures Pre-Op Ox:
Surgical Procedures : CSection Post-Op Diagnosis:
Anesthesia Type:
08:00
FHT's in OR: 128
OR Room #:
ASA: Two Time Antibiotic
(_
Anesthesia Type other: Given: 04/01/ 07:09 EDT Times Time C/S Called:
Patient in OR Start/ Arrive Time:
Stop/Depart Time:
Personnel Anesthesiologist: M.D.
AAMsthesiologist) Surgeon:~ II/
Assistant: Pediatrician:
Neonatologist: 0 1 l
Resident: others in OR:
Arrival/ Position/Settings Mode of Arrival:
Mental/Emotional State: Sensory Limits:
Aids/Pros Removed : Position :
Safety Equip used : Verification of Patient and Procedure:
Drains/ Dressings
Drains: Drain (A) Type /Size:
Drain (A) Location: Drain (B) Type/Size:
Drain (B) Location:
EBL (cc's):
Anesthesia Surgery
CRNA:
Circulator: ••lllililiiiiiiiMIIRN Cirulator Relief:
Scrub Tech: Nolen Scrub Relief: SCN Nurse:
Dressings Applied: Dressings Types:
Dressings Other types: Secured with:
Secured with Other: Foley: Yes Foley Size: N/A Inserted by: mcd
Bovie Pad Location: LAT
Surgical Procedure . . verification Checklist:1. __ Conft,2._Check,3 ._Commu,4._Conft
Sinc{air .Jvl.emoria{ :J-fosyita{-----, r-------------------, 444 'West Thirc£ Street Dayton, Ohio 45402
Date Printed
Printed By :
1/8/1
LD
Labor & Delivery Surgical Record
MR#
Age 28
Bed 1390-A
Adm Date 04/01/./1.
34

Lab ~ -==-:X DeliverYc:'urgical AS: ~~rd ,_.
Transfer Transfer Condition:
Transported by:
Operative Site: Intact
Surgical Wound Classification:
Prep PREP Solution
CLIPPER Complete
SCRUB Betadine
PAINT
Electrocautery I Equipment/Settings Electrocautery: Yes
Type Instrument#
ESU OR RM#l = KN013963 OR RM#2 = KN051760
Anes. Unit OR RM# 1 = KN032366 OR RM#2 = KN002184
Dinamap OR RM#l = KN054469 Monitor OR RM#2 = KN053682
Dinamap OR RM#l = KN054470
PulseOx OR RM#2 = KN053683
Fetal Monitor OR RM#l = KN054513 OR RM#2 = KN016403
Counts IX -ray flrrigants
Items/Counts First Second
Instruments
Sponges
Needles
Blades
Transfered To: Transfered to other:
Location COMPLETED BY:
Peri/Abd pt
Peri/Abd
OR Room#: 1
Coag # Cut# Pad Site Post-Op
50 50 WNL
Third Xrays taken for Incorrect count?
All counts correct: Yes,Circ/Scr
Specimens/Cultures Specimens Obtained:
Specimen (A) Type: Specimen (A) Site: Specimen (B)Type: Specimen (B) Site:
Sinc[air Memoria[ J-fosyita[ 444 W est 'Tfiira Stree t Dayton, Ofiio 45402
Date Printed 09: 30
Pr inted By :
Cultures Taken: Culture (A) Type: Culture (A) Site:
Culture (B) Type: Culture (B) Site:
DOB 1/8/11/111
Labor & Delivery Surgical Record
None
MR#
Acct# 0 ••••
Age 28
Bed 1390-A
Adm Date 04/01/tl
35

~ r ing Labor an~~elivery Re ... 'r-~ L
Maternal Labor/Delivery Informaton EDC:03/27.
Deliver Doctor:IJII···~, D.O.
Anesthesiologist:
Anesthetist:
Delivery Anesthesia: Spinal
Meds in Delivery:
nnC!'o• -* I ~a...-.-. -··--.. -· ........ _ ...... Complete Cerv Dilate: 04/01 . 07 :13 EDT
ROM Method: Artificial
ROM Date/Time: 04/01/.07:10 EDT
Oxytocin: N/A
Labor Anesthesia:
EBL (cc's): 300
NRT: :t• IS
Other Personnel: rl'll It i Pt. Trfd to: N/ A
Vaginal Delivery
Laceration Type/Ext.: None
Other Laceration:
EXT TOCO: Yes
EXT US: Yes
FSE:
IUPC:
C- Section Delivery
Pr i mary Indication: Repeat Elective
Other Primary Indicat:
Secondary Indication:
Other Second Indicat:
Labor: N/A
Maternal Complications Delivery_ Complications: None
Other Complications:
Delivery Comments:
/N/A
Sinc{air Jvtemoria{ J{osyita{ 444 West Third" Street 'Dayton, Ohio 45402
Date Printed
Printed By :
G/ 5 P/ 2
Delivery/Circulating RN:
Scrub N
Resident:
Nurse Midwife:
No. of Babies in Womb: 1
Amniotic Fluid Color: ; Fluid Clear
Amniotic Fluid Odor : Normal
Amniotic Fluid Amount: Moderate
Cervical Ripening Agent:
Other Cerv Ripening Agent:
Stage 1:
Stage 2:
Stage 3 :
Total Time in Labor:
Episiotomy: Sutures:
Hrs
0 Hrs
0 Hrs
Hrs
None Vicryl
3
0
min
min
min
min
Baseline Count: Final Count: Sharps 10
Sponge (4x4s)
Sponge (RayTec) 10
Sharps 10 Sponge (4x4s)
Sponge (RayTec) 10
Urgency: Scheduled
Elective: Elective
L/ 2
Incision: Lower Uterine Transverse
Other Incision:
. '
• Attending :
SAI-Jik'·
Incidence: Repeat
MR# ···-~~~ Acct# .. I.IJM
Age 28
Bed 1390-A
Adm Date 04/0dl:r T
Nursing Labor and Delivery Record Page 1 36

.. t • b L . I" rt~"mg La or a~)e 1very Re
Baby A Delivery Information
Delivery Date: 04/01
ROM Date Time: 04/ 01
07 : 16 EDT
07 : 10 EDT
Method of Delivery: Scheduled C/Section
Born en Route: No
VBAC: N/ A
Forceps: N/ A
Vacuum Extraction; Successfui
Vacuum Extract # pulls:
Vacuum min-sec p/pull:
Baby 'A' Information Sex: Male 40 (wks}/US
GA at Delivery/Status: 40 .5
IDBand#: ....
MR#JI8£ IIJI.II Suction: Mouth,Nose
Co;;ditlon: Stabie
Outcome: Liveborn
Term
Birth Weight: 3741 (grams)
8 (lbs) 4 (oz)
Wks/LMP
cc's
Vacuum Pressure appl:
Presentation: Cephalic
Cephalic Position: Vertex
Breech Positon: N/A
Length: 53 .3 (em) 21.00 ( in)
Head Circ. (in): 15.0
Vertex Position: Direct Occipital Anterior
Scalp pH:
Placenta Deliv Time: 04/01.,. 07 :16 EDT
Placenta Deliv Method: Manual Removal
Placenta Status:
Placenta Disposition:Routine_
Cord Blood Taken: Yes
Bank/Donate Info:
Neonatology Called: Yes
Apgars
Time 1 Min 5 Min 10 Min
Heart Rate >100 >100
GBS (+/Ukn} Tx'd X:
Delivery Comments:
Stnc air :Memoria 444 West T fiirci Street 'Dayton, Ofiio 45402
Date Printed 4/1/2. 09:41
Resp Effort Cry Cry
osyita{
Printed By: 1111 ....... !iJii RN
,.
Muscle Tone Active Active
DOB
~ UNIT
1/
LD
Chest Circ. (in):
Abd Circ. (in):
# Cord Vessels: 3
Nuchal Cord:N/A
Other Nuchal:
True Knot:
Cord pH:
Transfered to:
Reflex Cry Cry
MR#
Acct#
Age r~ Atte~
Bed ~
(art.)
Color BodyPink Body Pink
Wit,-Mi .••••.
28
1390-A
Adm Date 04/ 01/. n~> · t'l EDT . .
. . Nursmg Labor and Dehvery Record
(ven.)
Score 9 9
~ •.
Page 2
I
I I
37

N,..., ing Labor an .. .=-. .Jelivery Rec~
Baby A Information Continued
Complications
Infant Complications:None
Other Complications:
IU Death: Neonate Death:
Resuscitation: Tactile,Bulb
Medications:
Assessment Respiratory Rate Deliv: 40
Respirations Type: Normal
Physical Findings: WNL
Other Phys Findings:
Congenital Anomalie(s): None Apparent
Other Congen Anom:
Sinc{air Jvlemoria{ J-iosyita{ 444 W est ThircfStree t 'Dayton, Ohio 45402
Date Printed 4/1/2" 09:41
Printed By: .•• II lfl.djg;,}N
DOB 1/8/
Nursing Labor and Delivery Record
Age 28
Bed 1390-A
Adm Date
Page 3 (EOD) 38

Sinc[air :Memoria[ J-fosyita[ \ --. \.
Demographics
County: 012 Race: hite_
Religion: ••• ill. Other Religion: Father's Name: ••••
Father of Baby Involved: Yes Next of Kin Information
Next of Kin Name:Jiillli...,_ Next of Kin Relationship: grandmother
Labor & Delive-:y Admission Reco d F ~
Age: 28 Zip Code: •••
Home Telephone: (4Jii"'ll®ilruai6 Work Te hone:
Martial Education (yrs):
SSN: Occupation:
Other Occupation:
Next of Kin Telephone, ...... ,
Person acctbqrized to re'ease patient's pur 'Persona' Hea'Hz Tgfqcmatigg) Name:
Pregnancy Information G/ 5 P/ 2 T/2 Pt/ SAB/2 lAB/
EDC: 03/27
Allergies
Height: 67.0 (in) Weight (pre-pregnancy): 130
EGA per Dates: 40.8 EGA per Ultrasound:
Medication Allergies: Yes Benadryl - hyper reaction Food Allergies: No
Environmental Allergies: Yes metals - rash Latex Allergies: Latex rash, itching
Allergies Potential Latex Allergies: No
Medications Prenatal/Prescription Meds
Prenatal Medications: None
Herbal Supplements: None Prescription/OTC Meds: No
Medication 1: Medication 2: Medication 3: Medication 4 : Medication 5:
Alcohol /Smoking/Drug Use Alcohol Use: No
Advised to Stop Alcohol: Alcohol Comments:
Cigarette Use: YES Advised to Stop Smoking: Yes
Smoking Comments: 1 pack per day Marijuana Use: No
How Long Used (yrs)?: PreviousTreatment:
Marijuana Comments: Cocaine/Crack Use: No
How Long Used (yrs)?: PreviousTreatment:
Cocaine/Crack Comts: Other Illicit Drugs: No
Illicit Drug Comments: Communication
Primary Language: English
Communication Barriers: None
Sinc[air .'Jvlemoria{ J-fosyita{ 444 'West 'lhircf Street 1Jayton, Ohio 45402
Date Printed
Printed By:
Pharmacy
Smoking Cessation Literature Offered:
Avg Alcohol Consumption:
Avg Cigarettes Smoked: > 10 per day
How often Marijuana used: Date Last Used:
How often Cocaine used: Date Last Used:
English Abilities:
MR# ,.
Acct# UNIT LD
Age 28 Attending:
p Bed 1390-A
Page 1
W\1'
L/2
,_
"t,
39

Sinc[ai'!:_;!1en:!:oria[ .J{osyita[ Labor & Deliv~ Admission Ret ord,
Antepartum Procedures Procedures Done: Ultrasound AP Procedures Comments: US x 4, WNL
Vaccines
Labs
Influenza: No Pneumococcal: No
Tetanus: Uncertain
When: When: When:
Blood Type/Rh: A Pos Group B Strep: Negative
RPR/VDRL: Nonreactive Rubella/Titer: Immune
Chlamydia: No HIV+ Exposure/Results: Negative
Rhogam this pregnancy: N/A HbSAg: Negative
TB Exposure: Denies Chickenpox: Non Susceptible Gonorrhea: Negative
Herpes: Denies (No HX) Pt offered HIV test: PrevDone Lab Comments: Qf).l
I Date HbSAg drawn: 09/07 tClh-1- 1
Prenatal Care Histor Month of 1st PN Visit: 0
Support Person: Prenatal Classes Attend: No Pain Management Plans: None
Plans for L & D: None
Cultural/Spiritual Practices Practices to Incorp in Care: No Describe Cultural Practices:
Diet to Incorp in Care: No Describe Dietary Practice:
Living Situation/Discharge Planning
Pans E B: ·
Adequate PN Care: AdqPNC Relationship: Sigf_Oth
Anesthesia Plans:Spinal Pediatrician: Onsite
Circumcision Requested: Yes Feeding Preference: Breast
Tubal Ligation: No
Tubal Authorization Signed: N/A
Living Arrangements: House Person to_ Help_after D/C·~ Adequate Access to: Electric,Heat,Refrigeration,Piumbing/Running water,Pflone, 1 ranspol'tatiO"'''""""'
Person Taking Pt Home: Using Community Resource: es
If YES, please specify: medical card Outside Agency /Soc1al or Caseworker: No
If YES, please specify: Car Seat: Yes WIC: Yes
Adoption Requested: No Help Required to Obtain Car Seat: Agency Handling Adpt: Pt Contact w/Infant after Birth:N/A
Adolescent Screening Pt Grade in School:
A~e of Father Of Baby: Fam1ly Response to Preg:
Orientation and Safety:
Plans Regarding School: FOB Involvement:
Other Support:
Dry Marker Board (Nurse & Ph_'s),Call ligt1t,Bed operation/ Telephone/Teievislon, Mea is/ Vrsitmg hours,Ident1ty bands with Baby ,Employee verification ,Instucted on Mother and Baby safety in room and unit,Side Rails X2 ONLY1Given Admission Folder with all Hospital Information
Page 2
rnc arr ' [Jfc em orr a osyita [ _ ....... 444 West Thin£ Street
~.~ .. 'Dayton, Ohio 45402 MR# O§J~ll•'
DOB 1/~ - Acct# oeuu••-.r UNIT LD
4/ 1/ 2,06:22 Age 28
Date Printed Attending :
nvtAI!lfAk#·· Bed 1390-A Printed By:
04/01 .. _.. PP!!WP
Adm Date 06 : 19EDT
40

vosr:er:nca1 n1sr:ory S inc ~a i~,_,IQiBP.rtlfSIP.ei•very AdPI\J~§Nil' JJJ~'ilbruption: No
F ·me Anomaly: No F_. Bre. .eding Hx: Yes Gestational ~{''3tes: No Incompeten vix: No
In ertility: No Hx of Previous CSection:Yes
IUGR: No
Macrosomia: Yes DES:
Hx Stillborn: No Hx Neonatal Death: No
OB Hx Comments:
Systems Review HEENT Heart Lungs Breast Abdomen GI Extremities Teeth Skin Neurologic Comments:
Normal Normal Normal Normal
Normal Norma! Normal Normal Normal Normal has abdominal hernia
Infectious History Chlamydia: No
Genital Herpes: No
Hepatitis: No Gonorrhea: No
Infectious Hx Comments:
Previous Pt HX
Previous HX 1: Previous HX 2:
Bronchit Migraine
PIH:No
Previous Surgeries: hernia repair 2008, previous c/s x 2
Risk Assessments Morse Fall Risk Assessment
No No None Yes Normal
History of Falls Secondary Diagnosis Ambulatory Aid IV/Hgparin Lock Gaitt 1 ransferring Mental Status Morse Fall Risk Score
Oriented to own ability Low Risk
z.nc atr :Jvlemoria ( J-losyita( 444 West ThiraStreet Dayton, Ohio 45402
Date Printed 4/1/20.6: 22
Printed By: ~~
'_,._, .
-
,;.
~~
PTL/PROM: No PP Depression: No
PP Hemorrhage: No
Syphillis: No Tuberculosis: No
Human Papilloma Virus: No HIV/AIDS: No
DVT Risk Assessment Freely Ambulating
;;ii..'!£!.""~'" ~~
' ··-··· -'
DOB
Yes
MR# Uiff!IM
Page 3 (EOD)
1/~' Acct# a., •• Ill
UNIT LD Age 28
Attending:
~L Bed 1390-A
Adm Date 04/01 06:19EDT
' .. ~ •"'• '% «'
~ ~~ 1-'
1'1
t
41