37 pleural effusion associated with other radiographic evidence
TRANSCRIPT

37 Pleural Effusion Associated with Other Radiographic Evidence of Chest
Disease

CLINICAL IMAGAGINGAN ATLAS OF DIFFERENTIAL DAIGNOSIS
EISENBERG
DR. Muhammad Bin Zulfiqar PGR-FCPS III SIMS/SHL
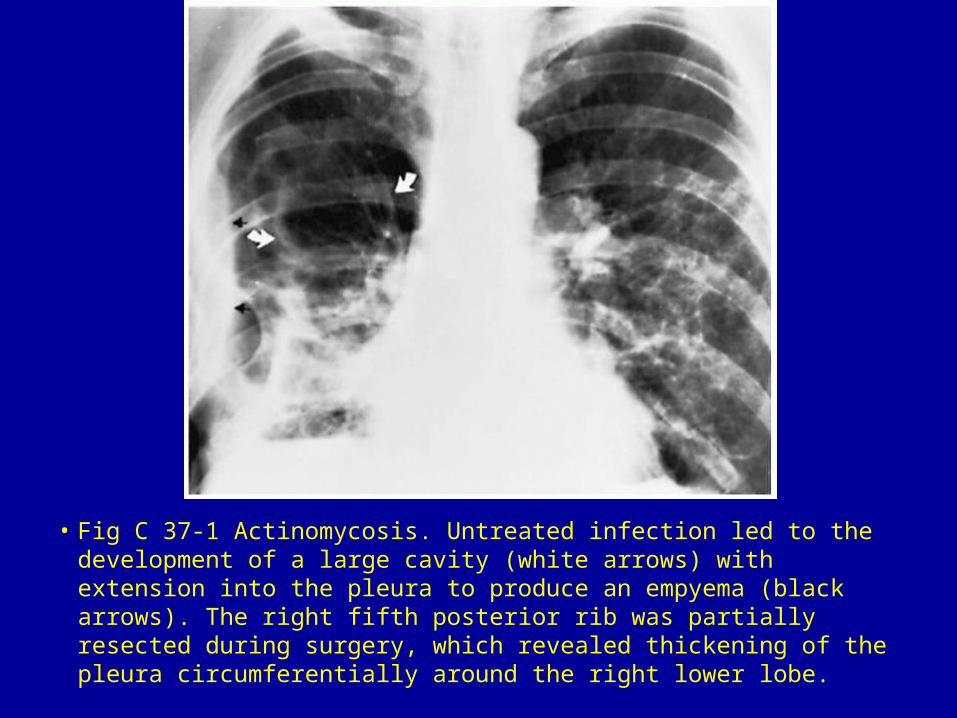
• Fig C 37-1 Actinomycosis. Untreated infection led to the development of a large cavity (white arrows) with extension into the pleura to produce an empyema (black arrows). The right fifth posterior rib was partially resected during surgery, which revealed thickening of the pleura circumferentially around the right lower lobe.
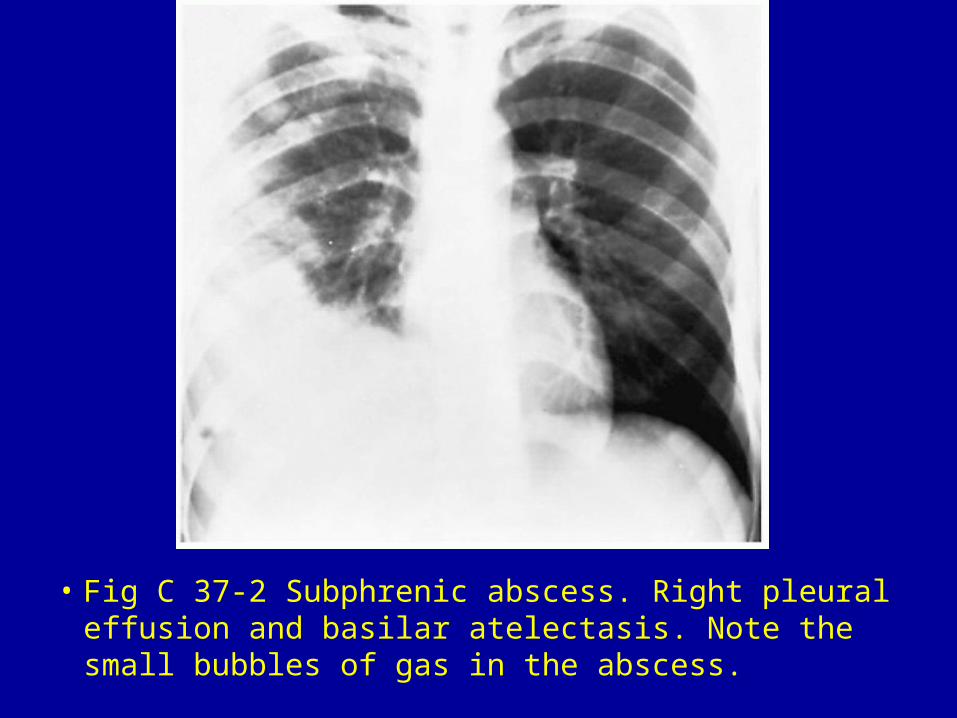
• Fig C 37-2 Subphrenic abscess. Right pleural effusion and basilar atelectasis. Note the small bubbles of gas in the abscess.

• Fig C 37-3 Diffuse pleural mesothelioma. After thoracentesis, the top of a large mass is evident (arrow).

• Fig C 37-4 Pulmonary embolism. (A) Plain chest radiograph demonstrates right basilar atelectasis associated with elevation of the right hemidiaphragm, representing a large subpulmonic pleural effusion. (B) Pulmonary arteriogram shows virtually complete obstruction of the right pulmonary artery (arrows).
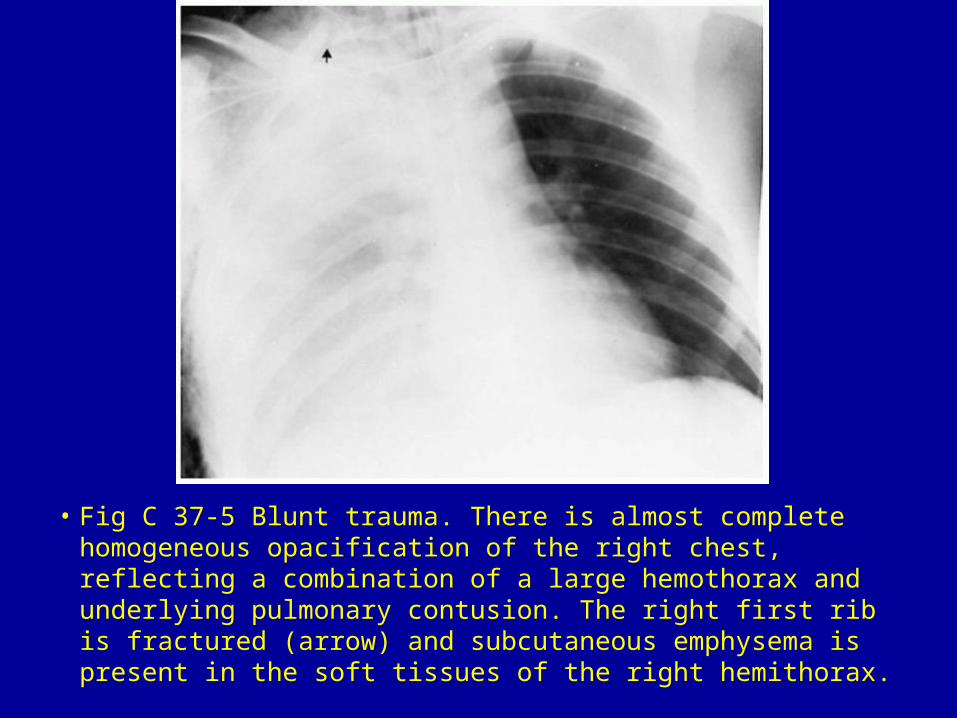
• Fig C 37-5 Blunt trauma. There is almost complete homogeneous opacification of the right chest, reflecting a combination of a large hemothorax and underlying pulmonary contusion. The right first rib is fractured (arrow) and subcutaneous emphysema is present in the soft tissues of the right hemithorax.

• Fig C 37-6 Phantom tumors. (A) Frontal chest radiograph taken during an episode of congestive heart failure demonstrates marked cardiomegaly with bilateral pleural effusions. Note the fluid collections along the lateral chest wall (closed arrow), in the minor fissure (open arrow), and in the left major fissure (arrowhead). (B) With improvement in the patient's cardiac status, the phantom tumors have disappeared. Bilateral small pleural effusions persist.

• Fig C 37-7 Constrictive pericarditis. Lateral decubitus view of the chest demonstrates moderate enlargement of the cardiac silhouette and a large right pleural effusion (arrowheads). Note the calcified plaque (arrows) in the pericardium.

• Fig C 37-8 Sarcoidosis. Small left pleural effusion in a patient with diffuse interstitial lung disease.

• Fig C 37-9 Systemic lupus erythematosus. Bilateral pleural effusions, more marked on the right, with some streaks of basilar atelectasis. The massive cardiomegaly results from a combination of pericarditis and pericardial effusion.



