32nd infection prevention and control nurses college...
TRANSCRIPT

Kupu Taurangi Hauora o Aotearoa
32nd Infection Prevention and Control Nurses College Conference
‘Building Beyond’
The Commission’s Role in IPC

NZ Health Quality & Safety Commission
• Formally established under the NZ Public Health & Disability Act 2010
• Triple Aim:
– Improved quality, safety and experience of care
– Improved health and equity for all populations
– Better value for public health resources

Why establish a new national QI agency?

HQSC role and purpose
To lead and coordinate work across the health and disability sector to:
• monitor and improve the quality and safety of health and disability services
• help providers across the health and disability sector to improve the quality and safety of health and disability services

Measurable improvement
• For every patient, at the individual, population and systems level
• Open for better care campaign wrapped around the improvement programmes
• Publicly reported quality & safety markers: visibility and priority at senior levels in DHBs
• Clinical leadership
• Multidisciplinary teamwork
• Consumer engagement

How the Commission adds value
Shining the light on variation and key areas for improvement
Being an intelligent commentator and advocate for change
Lending a hand by making expert advice, guidance and tools available

Approach
• Mix of programmes
– Strategic
– Long Term
– Improvement
• Annual review of portfolio of programmes
• Continuous refreshing of improvement projects to keep pace with emerging trends, new knowledge and stakeholder expectations
7
HQSC Infection Prevention and Control• Overarching IPC programme focus:
– Raising the strategic profile and importance of IPC
– Supporting clinical leadership
– Measuring and monitoring progress
– Capability building in quality improvement
• Current improvement projects:
– Surgical Site infection Improvement Programme (SSIIP)
– Hand Hygiene New Zealand (HHNZ)
• Previous improvement projects:
– Target CLAB Zero

What is an ‘Improvement Project’? • Focus on a specific area or topic for improvement
– Known actions that if implemented will reduce harm– Call to action for people to make change– Builds leadership, re-usable networks and capability for
improvement– Uses a recognised improvement methodology– Improvement can be measured
• National scale, accelerated pace• Time limited, building sustainability• Significant resource investment• Quality and Safety Markers (QSMs) – process and outcome
measures
9

2011-12 2012-13 2013-14 2014-15 2015-16 2016-17
IPC:
• Hand Hygiene delivery delivery delivery evaluation/transition
transition/BAU
BAU
• CLAB start-up delivery transition / evaluation
BAU BAU BAU
• SSI (Ortho) scoping start-up delivery delivery delivery/ transition
evaluation/ BAU
Med. Safety:
• Hospital eMedicines
delivery delivery delivery / transition
evaluation BAU
• OpioidCollaborative
scoping start-up delivery delivery transition / evaluation
Perioperative Harm
scoping start-up delivery delivery transition / evaluation
Falls scoping start-up delivery delivery transition / evaluation
New Programme 1 scoping start-up delivery delivery
New Programme 2 scoping start-up delivery

Pipeline of new improvement programmes
• Emerging priorities
• Refining of current prioritisation criteria
• Shorter list of 2-3 probable new programmes
• Further scoping of value proposition
Implementation
Long-list of feasible
proposals for prioritisation
2-3 projects prioritised for
implementation
Project evaluation
Pipeline of proposals
collected during the year
Transfer to
the sector

Working list of proposed initiativesPotential Improvement Projects
High Risk Meds Delay cases
Pressure injuries Patient identification
Deteriorating patient Sepsis
VTE Transition points of care
Polypharmacy Blood products
Catheter associated urinary tract infections
Caesarean Section SSIs
Ventilator associated complications (VAC)
PIV Infections

Informed by the Commission’s Strategic IPC Governance Group, membership of which includes:
• Adrienne Morgan, IPC consultant, IPCNC private sector representative
• Arthur Morris, Clinical Microbiologist, Clinical Lead SSII Programme
• Don Mackie, Chief Medical Officer ,Ministry of Health (ex officio)
• Geoff Cardwell, Consumer representative
• Jane Pryer, Senior Advisor - Healthcare Associated Infections & Communicable Diseases
• Jenny Parr, Assistant Director of Nursing & Director of IPC WDHB
• Jo Stodart, Charge Nurse Manager IPC Service SDHB, IPCNC DHB representative
• Joshua Freeman, Clinical Microbiologist ADHB, Clinical Lead HHNZ
• Lorraine Rees, Charge Nurse Manager IPC Service MCDHB, IPCNC DHB representative
• Mo Neville, Assistant Group Manager Quality and Patient Safety Waikato DHB
• Nick Kendall, Manager, Treatment Injury, ACC
• Richard Everts, Infectious Diseases Physician, ASID representative
• Sally Roberts, Infectious Diseases Physician and Clinical Microbiologist, Clinical Head of Microbiology ADHB, National Clinical Lead IPC Programme
• Trevor English, consultant (prev. GM Hospital Support and Laboratories at Canterbury DHB)
• HQSC : Gabrielle Nicholson; Karen Orsborn; Gillian Bohm; Deborah Jowitt; Rachel Hill


Target CLAB Zero
• All 20 DHBs
• IHI methodology:
‘CLAB Collaborative’
• ICU focus
• Spread to other clinical areas
• Standard of care


Reducing CLAB to <1/1000 central line days

“Better for patients …”“It’s much better for patients …
if they are transferred from another ICU, we can see the insertion
checklist and feel confident about leaving the line in place.”
Merilyn Beken, ICU Nurse Specialist, Auckland DHB

Hand Hygiene New Zealand• WHO ‘5 moments for hand
hygiene’ programme:
– Senior sponsorship
– POC hand gel
– Education/audit & feedback
– Champions/Clinical Leadership
– Patient participation

Progress over time
Figure 1. Trends in national aggregate and average hand hygiene performance: October 2012 to June 2015
Trends in national aggregate and average hand hygiene
performance: October 2012 to June 2015

‘Frontline ownership – Waitemata DHB’
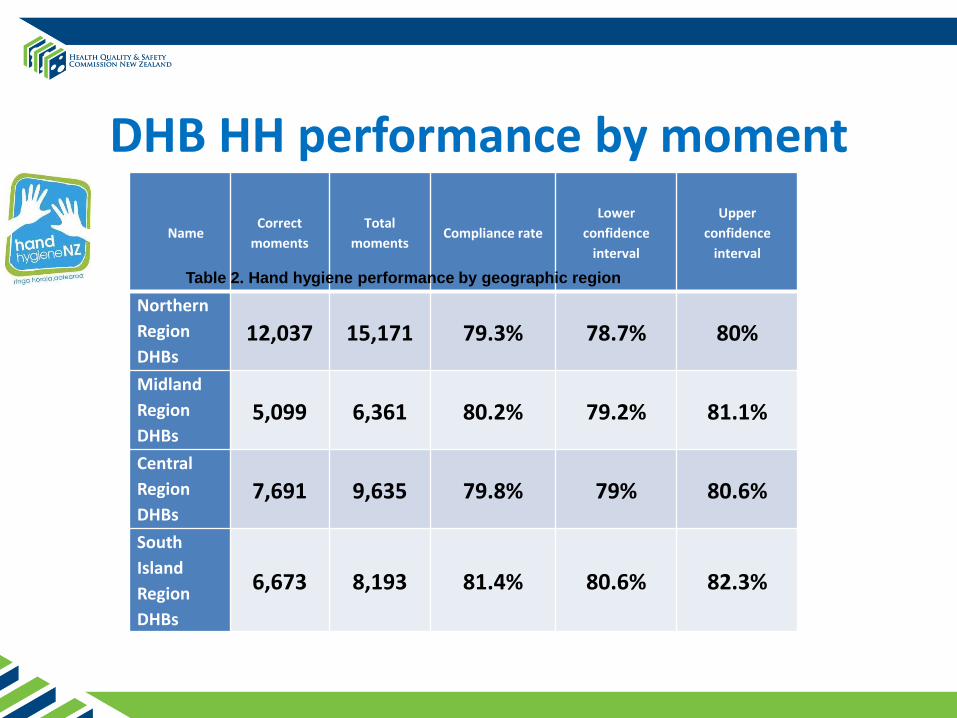
DHB HH performance by moment
NameCorrect
moments
Total
momentsCompliance rate
Lower
confidence
interval
Upper
confidence
interval
Northern
Region
DHBs12,037 15,171 79.3% 78.7% 80%
Midland
Region
DHBs 5,099 6,361 80.2% 79.2% 81.1%
Central
Region
DHBs 7,691 9,635 79.8% 79% 80.6%
South
Island
Region
DHBs
6,673 8,193 81.4% 80.6% 82.3%
Table 2. Hand hygiene performance by geographic region
Reaching 80 percent!

Hand Hygiene 2015/16
• HHNZ website being maintained
• Database being upgraded by Hand Hygiene Australia (HHA)
• Reporting maintained and enhanced
• National coordinator role
• Communications on-going

Working regionally
• The Commission working with the sector to support the development of regional IPC networks
• First round of meetings Dec 2014/Feb 2015 in Northern, Midland, Central and Southern regions
• Focused on what would be needed to sustain practice improvement as the hand hygiene programme is transitioned from being centrally led by the Commission, to being regionally supported

Approaches to improvementand results to date
SSIIP progress to date
• All 20 DHBs engaged in the orthopaedic workstream of the programme– Canterbury and Auckland DHBs delivering the
SSIIP in partnership with HQSC
– ICNet-based national data warehouse supports data collection, analysis and reporting (local and national reports – quality and safety markers)
• Three of five DHBs (Auckland; Canterbury; Southern) engaged in cardiac workstream of the programme

SSII Programme SG members:• Dr Sally Roberts, Clinical Head of Microbiology, ADHB
• Dr Arthur Morris, Clinical Microbiologist, ADHB
• Mr Imran Ramanathan, Cardiothoracic Surgeon, ADHB and NZ Representative on the Australian and New Zealand Society of Cardiac and Thoracic Surgeons (ANZSCTS)
• Mr Richard Lander, Orthopaedic Surgeon, MidCentral DHB, Executive Director for Surgical Affairs, Royal Australasian College of Surgery (RACS), representing the Surgical College (replaced Dr Allan Panting NMDHB March 2015)
• Mr Kelly Vince, Orthopaedic Surgeon, Northland DHB
• Claire Underwood, IPC Clinical Nurse Specialist, Hutt Valley DHB
• Marie Russell, Perioperative Nurse, Grace Hospital, representing from the NZNO Perioperative Nurses College
• Dr Andrew McWilliams, Anaesthetist, Canterbury DHB, representing the Australia and New Zealand College of Anaesthetists (ANZCA)
*Lisa Maxwell, IPC Clinical Nurse Specialist, Waikato DHB, on SSIIP Expert Faculty
Improvement approach
• A range of improvement methodologies:
‘the right tool for the right job’
• Continuous quality improvement – shift from initial Lean Six Sigma approach to a more inclusive approach that uses a mixture of methodologies including the IHI Model for Improvement (PDSA cycles)and Frontline Ownership

Local Barriers to EngagementSome similar to other IPC initiatives:
– ensuring senior executives actively involved
– overcoming resistance to working together in a multidisciplinary way
– creating local ‘ownership’ of improvement
Issues particular to SSIIP:
– time involved in manual inputting of data
– translating IT needs into action

QSMs: Process Markers
• QSMs for SSIIP confirmed in consultation with the sector as:
–Antibiotic prophylaxis given on time (0-60 minutes before knife to skin)
–Correct dose of recommended antibiotic
–Alcohol-based skin preparation – either chlorhexidine or povidone iodine

QSM Compliance over time
QSM March-June
2013
October-
December
2013
January-
March
2014
October-
December
2014
On time 91% 90% 92% 95%
Dose
>=2g cefazolin
51% 68% 78% 90%
Alcohol based
skin
preparation
94% 96% 98% 98%
Post-op
duration
<24hrs
61% 84% 76% 83%

‘On time’ antibiotic prophylaxis

Correct dose of antibiotic
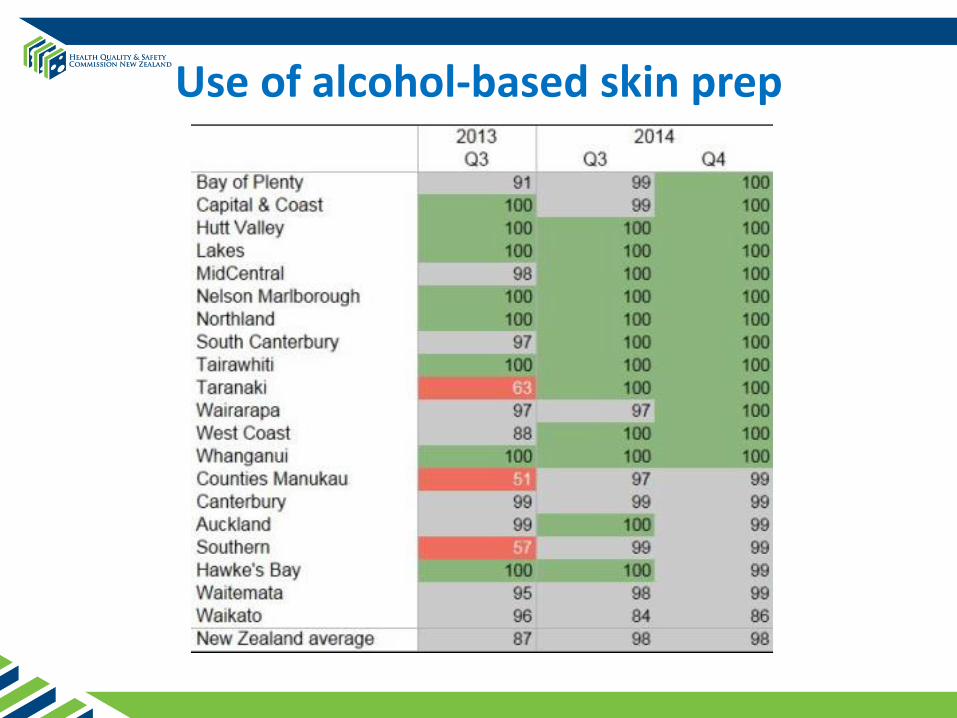
Use of alcohol-based skin prep

Outcome measure:Hip and knee SSI rates Mar 2013-Dec 2014
SSIIP 2015/16 …• Maintaining engagement in all 20 DHBs
• More in the consumer space
• Appointment of a new QI Advisor to
support local and regional work
• Automated data collection and reporting a
a priority for sustainability
• Improved reporting both local and
regional
• Frontline ownership?

Looking forward• Continue to raise the profile of IPC
• Focus on ‘connectedness’ - facilitate the sharing of good practice – from ‘islands of excellence’ to a more integrated network
• Put resources towards QI capability building with an IPC focus
• Consult, share, work in partnership across the sector to improve patient outcomes

Acknowledgments
• All the work being done by IPC nurses, hand hygiene champions, surgical teams and SSI champions, & others that support their efforts to improve patient safety & reduce HAIs
• Clinical Lead for IPC programme – Dr Sally Roberts
• Clinical Lead for SSII programme – Dr Arthur Morris
• Clinical Lead for tHand Hygiene Programme – Dr Josh Freeman