21th wcc, shenzhen, china, aug 19, 2010 guo-liang jiang, md, facr min fan, md, jiayan chen, md fudan...
TRANSCRIPT

21th WCC, Shenzhen, China,
Aug 19, 2010
Guo-Liang Jiang, MD, FACRGuo-Liang Jiang, MD, FACR
Min Fan, MD, Jiayan Chen, MD Min Fan, MD, Jiayan Chen, MD
Fudan University Shanghai Cancer CenterFudan University Shanghai Cancer Center
Combination of radiation therapy and Combination of radiation therapy and
Gefitinib for non-small cell lung carcinomaGefitinib for non-small cell lung carcinoma
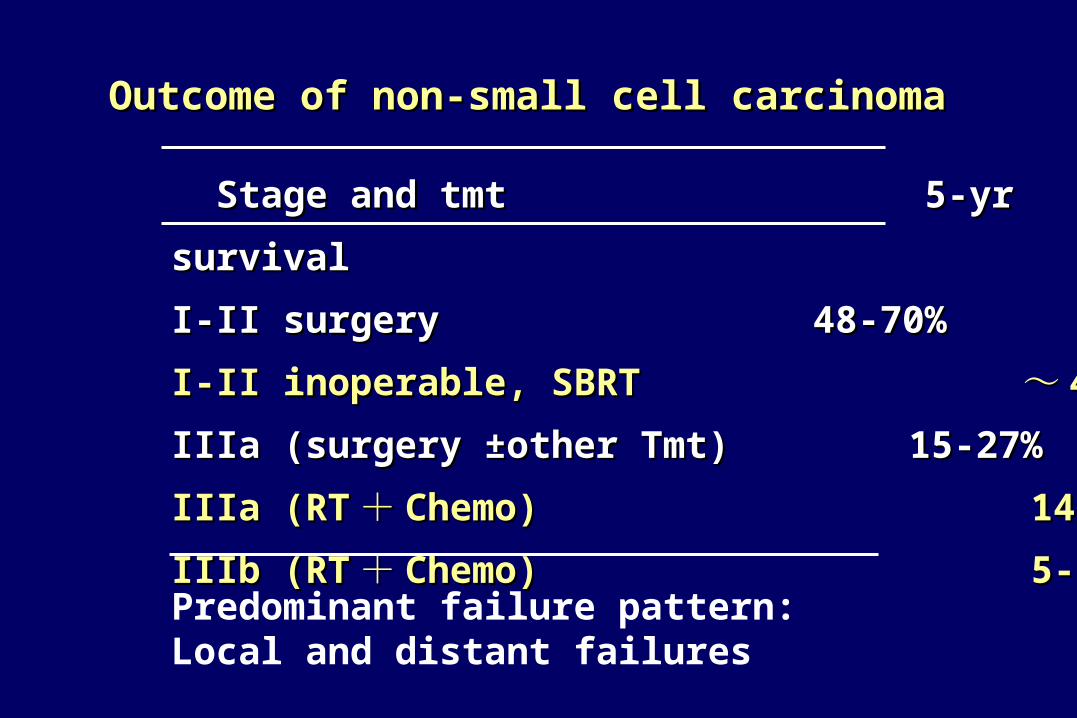
Outcome of non-small cell carcinomaOutcome of non-small cell carcinoma
Stage and tmt Stage and tmt 55-yr survival -yr survival
I-II surgeryI-II surgery 48-70% 48-70%
I-II inoperable, SBRT I-II inoperable, SBRT ~~ 40%40%
IIIa (surgery ±other Tmt) 15-27%IIIa (surgery ±other Tmt) 15-27%
IIIa (RTIIIa (RT ++ Chemo) 14-20%Chemo) 14-20%
IIIb (RTIIIb (RT ++ Chemo) 5-7%Chemo) 5-7%
Predominant failure pattern: Local and distant failures

Combination of radiation therapy and Gefitinib for
stage IIIb/IV non-small cell lung carcinoma
Clinical phase I trial
Irradiation dose escalation (NCT00497250)

Gefitinib enhanced radiosensitivity of tumor cells
Survival curve of Oral SCC (in vitro)
Shintani S. Int J Cancer 2003; 107:1030–37
• Shoulder of survival curve disappear (inhibition for SLD repair)
• Slop of survival curve reduced (intrinsic radiosensitivity increased)
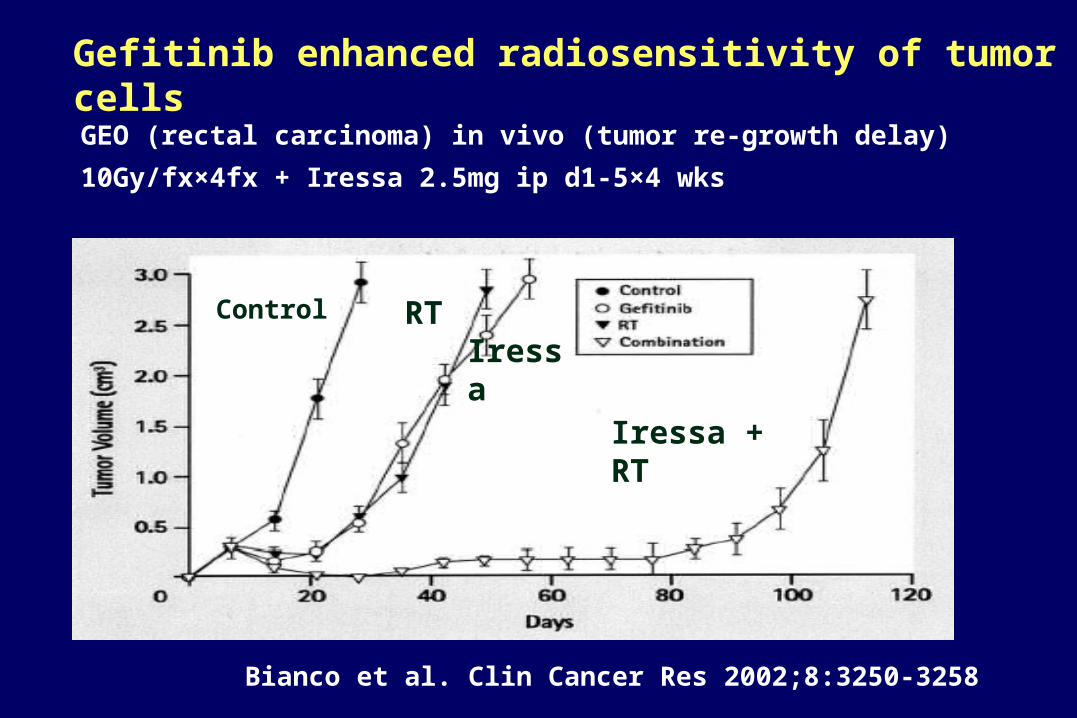
Gefitinib enhanced radiosensitivity of tumor cells
GEO (rectal carcinoma) in vivo (tumor re-growth delay)
10Gy/fx×4fx + Iressa 2.5mg ip d1-5×4 wks
Bianco et al. Clin Cancer Res 2002;8:3250-3258
Iressa + RT
Control RTIressa

The percentage of S phase decreased after Iressa
Iressa+RT (GEO in vivo)
Bianco C. Clin Cancer Res 2002;8:3250-3258
Mechanism of Gefitinib radiosensitization

Gefitinib speeds up apoptosis of tumor cells after RT
GEO in vivo
Bianco C. Clin Cancer Res 2002;8:3250-3258
RT+Iressa
RT
Iressa

Gefitinib inhibits RT induced damage repair
Oral SCC (Western blot)
Shintani S. et al. Int J Cancer 2003; 107:1030–1037
RT damage DNA
Need DNA repair enzyme
RT enzyme DNA repair Gefitinib enzyme DNA repair

Iressa+RT in Oral SCC (Western blot)
RT could activate EGFR-TK signaling pathway (Ras-Raf-MAPK). And And initiates a multistep phosphorylation cascade that leads to activation the pathway, and stimulates cell-cycle progression
Shintani S. Int J Cancer 2003; 107:1030–1037
Gefitinib could inhibit multistep phosphorylation of EGFR signaling pathway, so slow down the tumor cell proliferation and enhance the radiation sterilization.

Possible mechanisms for radiosensitization of Gefitinib
1. Decrease percentage of S phase and increase
G2/M phases of tumor cells
2. Enhance tumor cell apoptosis after RT
3. Inhibit radiation induced DNA repair
4. Inhibit multistep phosphorylation of EGFR
signaling pathway, so reduce the tumor cell
proliferation after RT

Rationales:
• Gefitinib as radiosensitizer to enhance local tumor sterilization.
• Inhibit or delay the growth of micrometastases
• What is concerned most for concurrent RT and Gefitinib for NSCLC?
• Pulmonary toxicity: Interstitial pneumonitis by Gefitinib Radiation pneumonitis

Goal of the trial
Main endpoint
Side-effect and toxicity, safety and MTD of
concurrent therapy of Gefitinib and RT for
advanced non-small cell lung carcinoma.
Second endpoint
Acute response (RECIST) and survival

Patient eligibility
NSCLC histologically or cytologically
confirmed
IIIb
IV: brain mets
ECOG 1-2
No contraindication for RT
Tolerable for RT and Gefitinib

Treatment
Concurrent Gefitinib (250mg, qd) and RT and continuously Gefitinib for 2 months after RT.
RT target: Gross tumor volume in thorax on CT2Gy/fx, 5 fx/wk,Total dose escalation54Gy, 56Gy, 58Gy, 60Gy
Dose limit toxicity (DLT) in 2 months after completion of RTCTCAE V3 >=3 for lungCTCAE V3 >=4 for othersWhen >=2/8 patients occurred DLT, dose escalation terminated and MTD was one dose level before.

Result
Status of dose escalation
Dose level No. pts
54Gy 8
56Gy 8
58Gy 8
60Gy 8+8
One patient in 60Gy occurred interstitial pneumonitis in both lung one week after RT and died of pulmonary failure in 30 days

Male/Female 28/12
Medium age (yr)
Medium cycle of chemo
55 (32–79)
3.5 (1-5)
ECOG 01
1030
Stage IIIB IV
1822
Histology Adeno-
Sq
Poor differentiated
35 (86%)4
1
Smoker/non-smoker 20/20
Clinical characteristics of patients (n=40)

Safety (MFT: 9.7 mos)
CTCAE 3.0 Incidence
Rash 1-2 24 (60%)
≥3 0
Pulmonary 1-2 29 (73%)
3G5
01 (3%)
Espophageal 1-2 23 (58%)
≥3 0
Hematological
1-2 16 (40%)
≥3 0

Outcome
At last follow-up visit
SD 8 (20%); PD 32 (80%)
Median progression-free time: 7 mos
Median survival time:
13.9 mos (11.4-16.4)
1-yr OS 62%

Conclusion
1. IIIB/IV NSCLC patients could tolerate concurrent RT (MTD
60Gy) and Gefitinib.
2. There was no excessive toxicity in NSCLC patients treated
with concurrent RT and daily Gefitinib, except for pulmonary
toxicity, which seemed like increased, especially the low
grades (1-2) of CTCAE.
3. MST of 13.9 mos and 62% of 1-yr OS were encouraging.
4. Clinical phase II trial was warranted, especially for non-
smoker and adnocarcinoma (EGFR mutated).

Thanks for your attention !
Shanghai 2010Shanghai 2010
EXPOEXPO