2.1. col. jeffrey yarvis - reintegrating returning warriors
TRANSCRIPT
COL Jeffrey S. Yarvis, Ph.D., MSW, M.Ed.
Reintegrating Returning Warriors and the Subtleties of PTSD: Practice, Research and Policy.
Presented to the INTERNATIONAL MEDICAL REHABILITATION, MENTAL HEALTH SUPPORT, INSTITUTIONAL AND POLICY CONSIDERATIONS AND TACTICAL BATTLEFIELD MEDICINE
CONFERENCE IN UKRAINE 28-30 APRIL 2015, KYIV, UKRAINE
This briefing is unclassified and reflects the opinion of the presenter

Purpose: A personal mandate • Good Governance=Good
(Mental) Health • Introduction to Trauma and the
Intimacy of Trauma • Subthreshold PTSD • International Scholarship • Trauma Transmission • Informs US policy and Clinical
Practice
What you do matters!
Tactical To
Practical
Recognize the important change inherent in the shift to a new model that places the emphasis on building and
sustaining social connections

Keys to success: Community-Based Agencies
Leaders People
4 Relationships

Keys to Success: It Takes a Community
“Psychological health is a community responsibility. Leaders, front-line supervisors, peers, friends, family members, health care providers, and other helping agency members must all collaborate in building resilience, recognizing signs of distress and illness, serving as links to helping resources, and following up with those who have accepted or rejected assistance”. (p. 18)
Defense Health Board
5
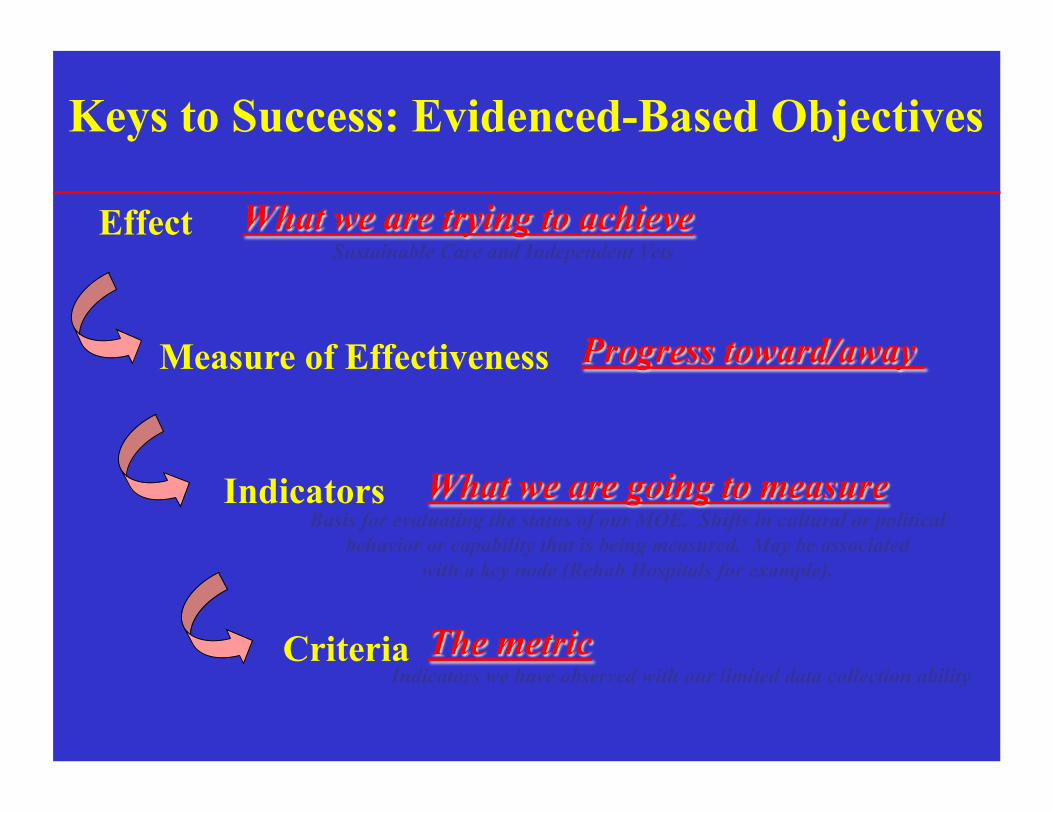
Effect Sustainable Care and Independent Vets
Measure of Effectiveness
Indicators Basis for evaluating the status of our MOE. Shifts in cultural or political
behavior or capability that is being measured. May be associated with a key node (Rehab Hospitals for example).
Criteria Indicators we have observed with our limited data collection ability
Keys to Success: Evidenced-Based Objectives

COMBAT STABILITY OPS
MED CIV-MIL OPERATIONS
INTER-AGENCY COOPERATION
KEYS TO SUCCESS: FOCUSED PARTNERSHIPS=
Ulkraine
Doctrine – Policy – Processes Funding Streams – Working Together
US Military Coalition
Forces
DoS, MN Agencies, IGOs, IOs, NGOs, Private sector, academia
DoD Security Cooperation
DoS, MN Agencies
IGOs IOs
NGOs
Development
SHAPING LEAD AGENCY TRANSITIONS
Key: Military Instrument Diplomatic, Political & Economic Instruments Synergy

BH Care and the Warrior
“We all serve!”
Veteran = ?
BH care starts with medical care

HBO Alive Day Memories: A Tribute
John Jones Marine Staff Sgt. Hometown: San Antonio, TX Age: 30 Date of Injury: 1/3/2005 List of Injuries: Double amputee below the knees, shrapnel in parts of thighs and wrists, some memory and hearing loss, post traumatic stress disorder.
http://www.hbo.com/aliveday/index.html
04.08.10 (adapted by: J. Martin)
Women and Warriors
A reality…

OIF/OEF Veterans
– Almost 1M OEF/OIF veterans have left active duty and are eligible for VA services (since FY2002) (currently 1.7M OIF/OEF veterans)
– 51% from AC; 49% from RC – 43% have already obtained VA care
(44% AC & 42% RC) (Male 88%; Female 12%) (59% age 29 or younger) (76% Army or Marine)
The three most common health issues: – Musculoskeletal (50%) – Mental Health (46%) – Symptoms, Signs and Ill-Defined Conditions (43%)
02.25.10 (adapted by: J. Martin)

Mental Health Issues among OIF/OEF Veterans: Are women
Diagnosed Properly? • Mental health problems reported among 46% of
eligible OEF/OIF veterans who have presented to VA (those Veterans actively seeking health care)
• Provisional MH diagnoses include: – PTSD 101,882 – Nondependent Abuse of Drugs: 30,406 – Depressive Disorder: 69,474 – Affective Psychoses 39,825 – Neurotic Disorders: 55,842 – Alcohol Dependence: 18,054
– A total of 193,879 unique patients have received a DX of a possible mental disorder
02.25.10 (adapted by: J. Martin)

PTSD : A need to understand…
“ A mental disturbance provoking pain, excessive joy, hope or anxiety, where it affects its temper, and rate, impairing general nutrition and vigor”
• William Harvey, 1628

Vietnam
Same or Different Today? Ex. Videos

Is there a stigma today?

Leadership Mitigates Stigmatizing Effects

Most Observed Reactions to Trauma
Fear and anxiety Intrusive thoughts about the trauma Nightmares of the trauma Sleep disturbance Feeling jumpy and on guard Concentration difficulties

Common Reactions to Trauma
Avoiding trauma reminders Feeling numb or detached Grandiosity Feeling angry, guilty, or ashamed Grief and depression Negative image of self and world Sexual Dysfunction
– The world is dangerous – I am incompetent – People can not be trusted

PTSD: Diagnostic Criteria
• Stressor • Intrusion Symptoms (aka re-experiencing) • Avoidance • Negative Alterations in Cognitions and Mood • Alterations in Arousal and Reactivity (aka
Numbing to Hyperarousal)
• Duration • Functional Significance • Exclusions
Diagnosing Subthreshold PTSD
“Pending further guidance, subthreshold PTSD should continue to be coded as an Unspecified Anxiety Disorder” (ICD-9 300.00; ICD-10 F41.9
OTSG/MEDCOM PTSD Policy Memo Para 7b(3)

Is PTSD clear to you?
• A common anxiety disorder that develops after exposure to a terrifying event or ordeal in which grave physical harm occurred or was threatened.
• Confounds two distinct constructs-stress and mental traumatization.
• Is a retrospective construct. • How cohesive is PTSD across different
groups? • Comorbidity

Taxonomic Issues
• Kraeplin’s classification system based on medical model –affecting predictive validity.
• Appears to be diagnostic yardstick with a sliding scale.
• No one size fits all category has persisted over time.
• Debate over what constitutes normal and pathological responses
• PTSD has been a “labile polymorphic disorder”- Solomon.
Overarching Research Question
Is Subthreshold PTSD
Clinically Relevant?

Subthreshold PTSD
• Symptom presentation that does not meet criteria necessary for diagnosis of PTSD BUT is sufficient for clinical attention.
• Defined as: -Meeting criteria for Re-experiencing, & -Meeting criteria for one Avoidance/
Numbing or Hyperarousal • Fairly common in at risk populations.
Recent studies: Subthreshold PTSD Prevalence
• Community sample. Marshall et al.'s (2001)
study noted 9 percent had full PTSD and another 18.9 percent had subthreshold PTSD.
• Out-patient psychiatric patients. The most recent study on subthreshold PTSD noted that in 1,000 patients, 156 (12 percent) met criteria for full PTSD, 84 (7 percent) for subthreshold PTSD, and 460 (35.4 percent) for trauma histories (Zlotnick et al., 2002).
Subthreshold PTSD and Veterans
• Asmundson (2002) found that subthreshold PTSD paralleled full PTSD in terms of symptomatology.
• Two Croatian veteran’s studies of 3,217 personnel showed 16.22 percent with current PTSD and 25 percent with partial PTSD one year after the war (Komar and Vukusic, 1999), and the rate of current PTSD increased to 24 percent just one year later (Kozaric-Kovacic, 1999), suggesting that some of the subthreshold group had developed full PTSD.

Implications of Time
• 1.7 million Vietnam vets 49 percent had PTSD (830,000)
• The contribution of sub-threshold PTSD would add another 350,000 veterans potentially in need of treatment (Weiss et al.,1992).
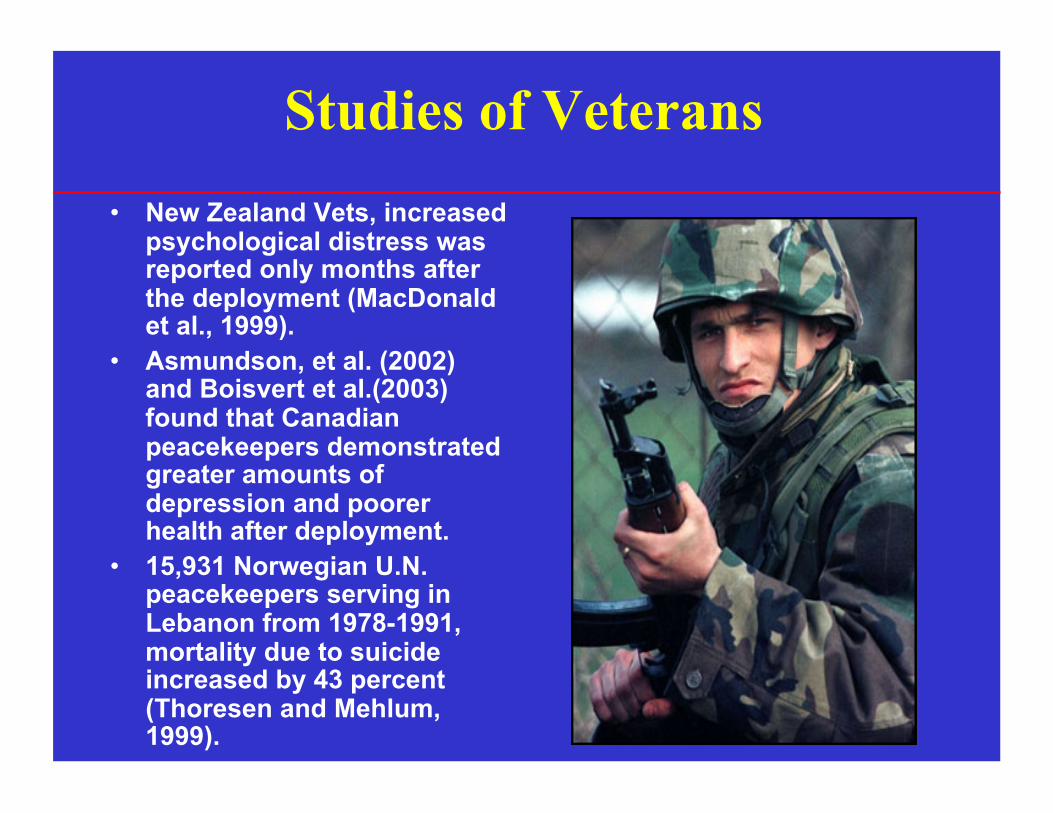
Studies of Veterans • New Zealand Vets, increased
psychological distress was reported only months after the deployment (MacDonald et al., 1999).
• Asmundson, et al. (2002) and Boisvert et al.(2003) found that Canadian peacekeepers demonstrated greater amounts of depression and poorer health after deployment.
• 15,931 Norwegian U.N. peacekeepers serving in Lebanon from 1978-1991, mortality due to suicide increased by 43 percent (Thoresen and Mehlum, 1999).

Deployment
• Veterans deployed more than once are 3.676 times more likely to be diagnosed with some level of PTSD than veterans never deployed. A spectrum disorder?
(Yarvis et al., 2005; Yarvis and Schiess, 2008, Yarvis, 2008)
• Risk Factors: • Trauma History • Gender • Number of Deployments • Age
Highest risk: Unmarried females deployed more than once.
What can comorbidity tell us?
• Veterans who present with depression or alcohol problems should raise suspicion for PTSD or subthreshold PTSD.
• Veterans who present with symptoms of PTSD should be screened for co-existing depression and alcohol problems.
• Veterans at subthreshold levels may seek treatment for other medical conditions and left untreated for their trauma symptoms may develop full PTSD.
The Sounds of Combat …
The Sounds of Combat …Stress
Weather

Poverty

Passive Posture & Locus of Control

First Exposure and Anticipatory Stress

Cultural Differences

Home-front, the Media & Unit Casualties
Events shaping attitudes toward returning vets.

Death of Children
• Critical incidents

Military-Induced Family Separation: Reintegration and Leaving Again

Spouse Satisfaction with Army Life Associated with Length of Separation

How do I explain what I’ve seen?
A Witness to Evil &
The Loudness of Silence…
The Subtleties of Coming home.

Adapted or Maladapted?
• Cohesion • Accountability • Targeted Aggression • Tactical Awareness • Armed • Emotional Control • Mission Security/OPSEC • Individual Responsibility • Combat Driving
• Withdrawal • Controlling • Inappropriate Aggression • Hypervigilance • “Locked and loaded” • Anger and Detachment • Secretiveness • Guilt • Aggressive Driving • Conflict • Discipline/Ordering
• WRAIR, LTC Carl Castro-Adapted from Battlemind
At War At Home

Problems with this model
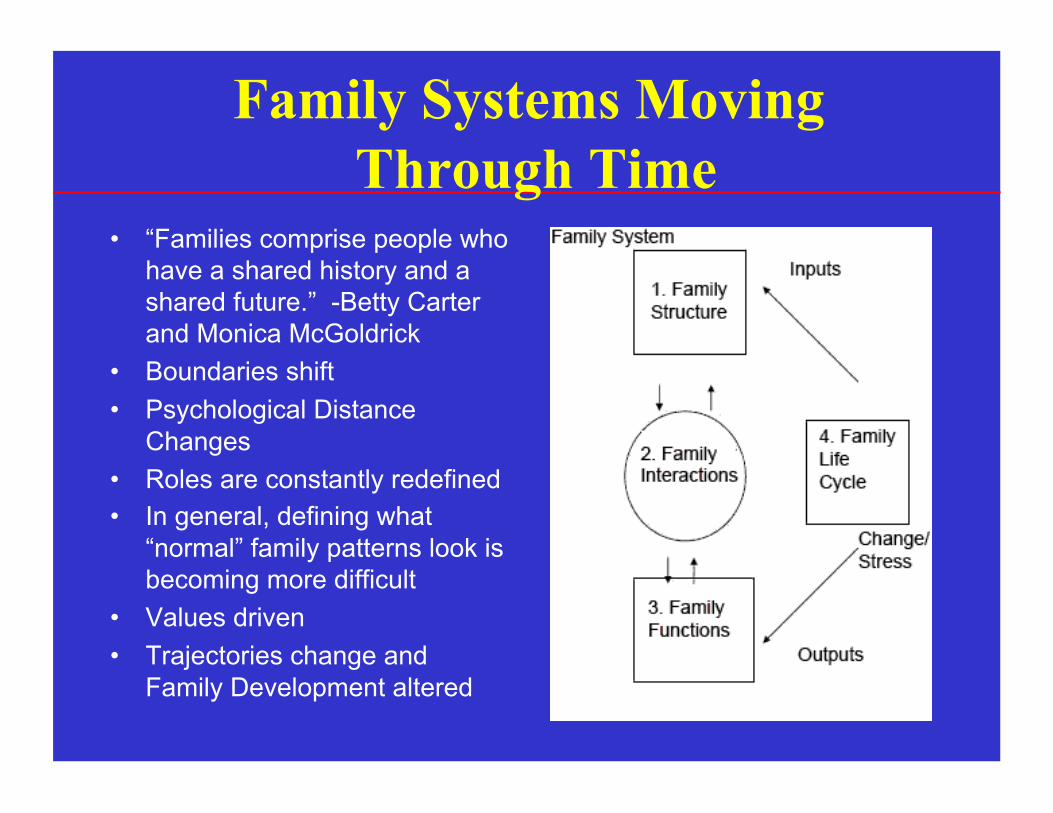
Family Systems Moving Through Time
• “Families comprise people who have a shared history and a shared future.” -Betty Carter and Monica McGoldrick
• Boundaries shift • Psychological Distance
Changes • Roles are constantly redefined • In general, defining what
“normal” family patterns look is becoming more difficult
• Values driven • Trajectories change and
Family Development altered
Relationship Between PTSD and Social Support
• One of the strongest predictors of recovery following trauma is social support – Perceived social support (PSS) – Received social support (RSS)
• Interaction is complicated – PSS is often negatively related to trauma severity – RSS is often positively related to trauma severity
• Deterioration of perceived social support over time may contribute to increased symptoms

Intergenerational Trauma-Holocaust
• Shoah • Slavery • Disaster • Forced Migration • Genocide • War
Parental PTSD and Children’s Distress
• Children of Vietnam veterans with PTSD, compared to children of veterans without PTSD, are more likely to experience symptoms
– 36% vs. 14% indicated symptoms severe enough to cause distress on GHQ (Westerink & Giarratano, 1999)
– more and more severe behavior problems reported (Kulka et al., 1988)
– 23% vs. 0% had received psychiatric treatment (Davidson et al., 1989)
PTSD and Parenting Skills Object Relations
• Clinical descriptions have characterized parenting by veterans with PTSD as: – Overprotective (or potentially avoidant) (Haley, 1984) – Controlling, overprotective, demanding (Harkness, 1993) – Enmeshed (Jurich, 1983; Rosenheck, 1986) – Highly emotional (Rosenheck, 1986)
• Children of PTSD veterans describe families as: – More conflicted (Westerink & Giarratano, 1999)
– Less Cohesive (Westerink & Giarratano, 1999)
• Veterans with PTSD are more likely than those without PTSD to endorse severe parenting problems – 54.7% vs. 17.3% (Jordan et al., 1992)
Understanding Children’s Reactions to War Deployment
• Children are affected by their parents’ traumatic experiences as well as their own
• Little scientific information about impact of parental combat exposure on children
• Equally dangerous to assume uniform resilience or uniform problems as a result of war exposure
• A real accounting of the trauma and its effects is an opportunity to honor the service and sacrifice
• War trauma is a primary source of difficulty for all military family members
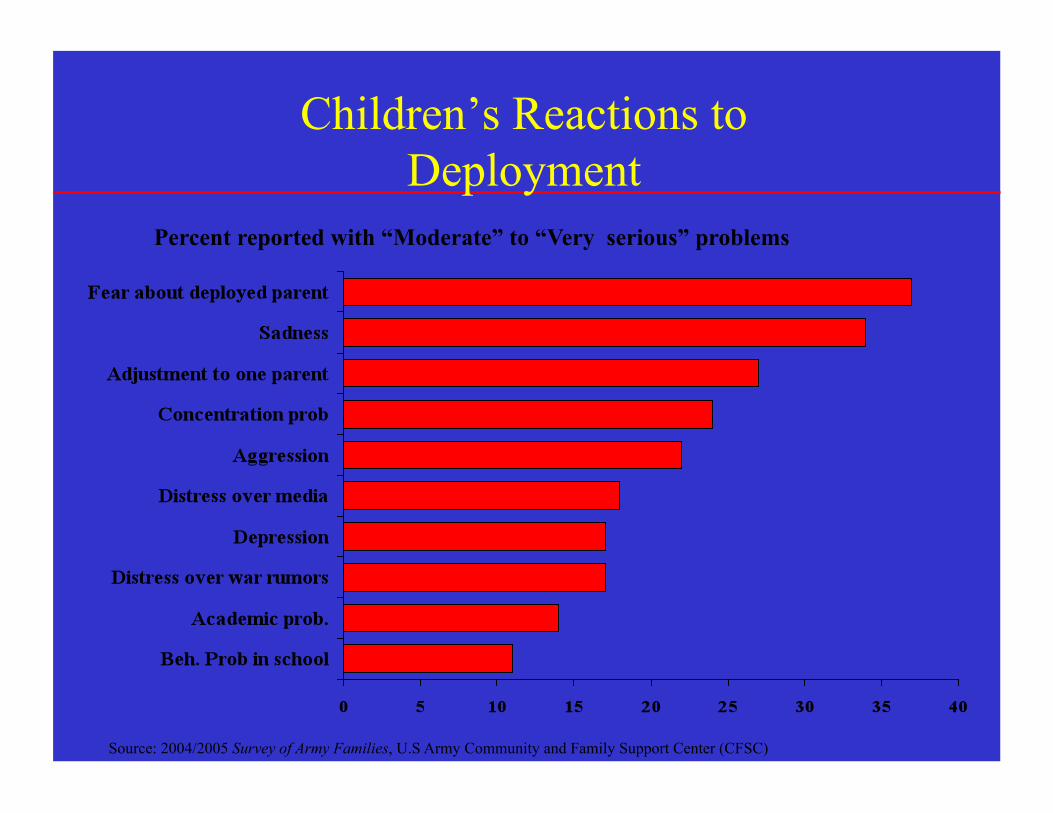
Children’s Reactions to Deployment
Percent reported with “Moderate” to “Very serious” problems
Source: 2004/2005 Survey of Army Families, U.S Army Community and Family Support Center (CFSC)
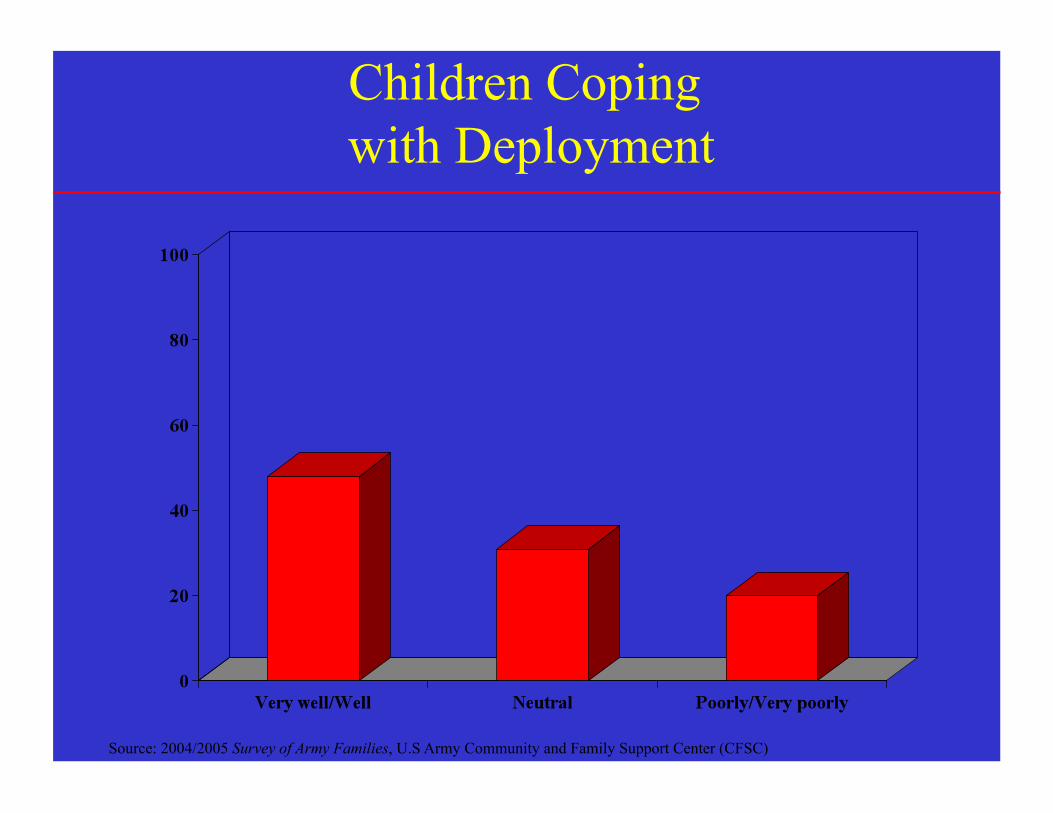
Children Coping with Deployment
Source: 2004/2005 Survey of Army Families, U.S Army Community and Family Support Center (CFSC)

Child Maltreatment and Deployment
• Rentz ED, Marshall SW, Loomis D, et al. Am J Epidem 2007
• McCarroll JE, Fan Z, Newby JH, et al., Child Abuse Rev, in press
• Rate of military family maltreatment twice as high in period after October 2002 compared to prior period versus no change in nonmilitary family population during similar period
• Greatest rise in maltreatment appears to be attributed to child neglect in younger children
• Rates of child neglect appear highest in junior enlisted population
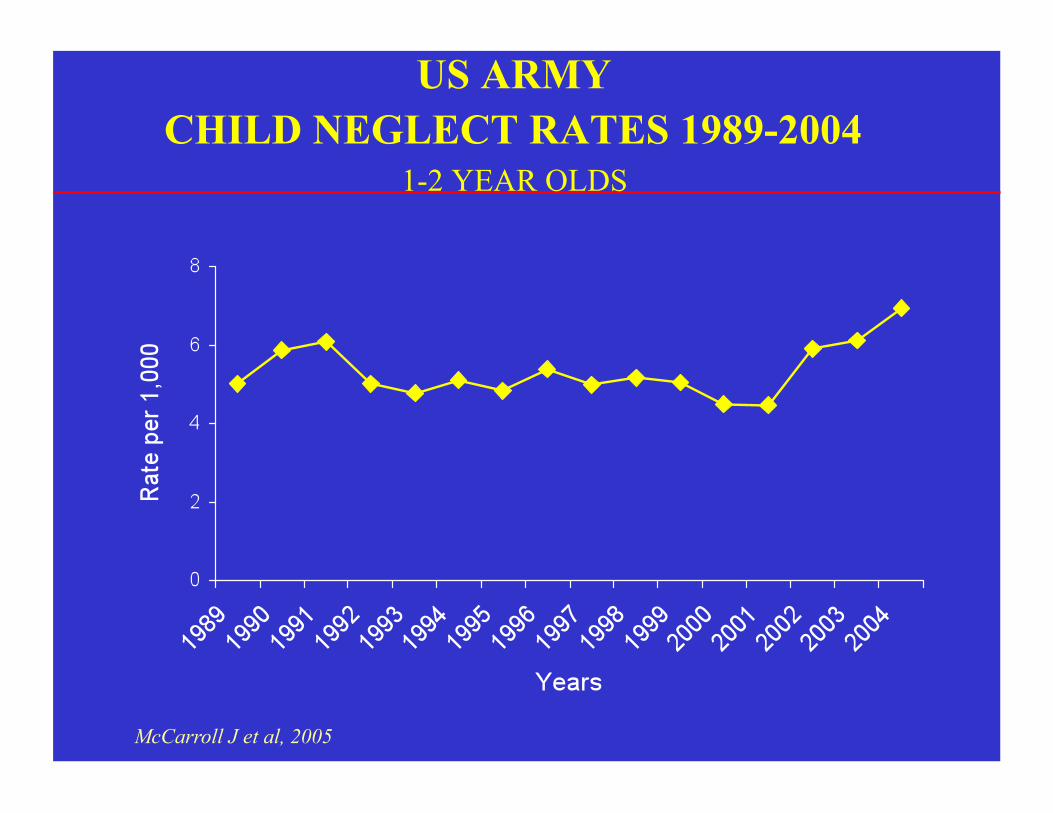
US ARMY CHILD NEGLECT RATES 1989-2004
1-2 YEAR OLDS
McCarroll J et al, 2005

Factors Affecting Family Adjustment During Deployment
• Families at increased vulnerability – Families in transition
– Young families
– Families with problems prior to deployment
– Pregnant spouses
– Families with multiple needs

Typical Course of Reintegration
• Family resilience is the rule, not the exception
• Usual for families to return to the normal routine
• Common to incorporate changes without disability in family functioning
• HOWEVER…We don’t always “want” to reintegrate. What does that mean?

Summary of Research on Families During Deployment
• In general, military families appear robust and healthy
• Deployment can have negative impact some families – Rarely reaches clinical levels – Usually resolves post-deployment – Pre-deployment functioning related to functioning during and
post deployment
• Unique aspects of OIF/OEF have not been studied with respect to families

• Consistent evidence-based practice is a high priority.
• Current policy is firmly rooted in the VA/DoD PTS Clinical Practice Guideline (CPG), with updated information on DSM-5.
Purpose of Policy: Provide Guidance on Assessment and Treatment of PTSD

Evidence-Based PTSD Psychotherapies From VA-DoD PTS CPG, 2010
SR Significant Benefit Some Benefit Unknown
Trauma-focused psychotherapy that includes components of exposure and/or cognitive restructuring; or Stress inoculation training
• Patient Education • Imagery Rehearsal Therapy • Psychodynamic Therapy • Hypnosis • Relaxation techniques • Group Therapy • Family Therapy • Web-based CBT
• Acceptance and Commitment Therapy • Dialectical Behavioral Therapy

CBT & VR Exposure Therapy
• VR exposure therapy has been used for the treatment of PTSD.

Healing SOUL Wounds: A paradigm shift
02.25.10 (adapted by: J. Martin)

65
Selected References Martin, J.A., & Kerse, E. (1997). Quality of Life for Future Naval and Marine Corps Forces. In Technology for the Future Naval Forces: Becoming a 21st Century Force. Volume 4: Human Resources. Washington, DC: National Research Council. Bowen, G. L. (1998). Effects of leader support in the work unit on the relationship between work spillover and family adaptation. Journal of Family and Economic Issues, 19, 25-52. Bowen, G. L., & Martin, J. A. (1998). Community capacity: A core component of the 21st century military community. Military Family Issues: The Research Digest, 2(3), 1-4. Bowen, G. L., Martin, J. A., & Mancini, J. A., & Nelson, J. P. (2000). Community capacity: Antecedents and consequences. Journal of Community Practice, 8(2), 1-21. Martin, J.A., Rosen, L.N., & Sparacino, L.R., Editors (2000). The Military Family: Meeting the Challenges of Service Life. Westport, CT.: Praeger Publishers, Inc. Bowen, G. L., Martin, J. A., Mancini, J. A., & Nelson, J. P. (2001). Civic engagement and sense of community in the military. Journal of Community Practice, 9(2), 71-93. Martin, J.A., Mancini, J.A., & Bowen, G.L. (2002). The Changing Nature of Our Armed Forces and Military Service Life. Family Focus, March, pp. F3-5. Bowen, G. L., Mancini, J. A., Martin, J. A., Ware, W. B., & Nelson, J. P. (2003). An empirical test of a community practice model for promoting family adaptation. Family Relations, 52, 33-52. Mancini, J.A., Martin, J.A., & Bowen, G. (2003). Community capacity. In T. Gullotta and M. Bloom (Eds.), Encyclopedia of Primary Prevention and Health Promotion. (Pp. 319-331). New York: Plenum. Mancini, J.A., Bowen, G.L., & Martin, J.A. (2005). Families in community contexts. In Bengtson, V., Acock, A., Allen, K., Dillworth-Anderson, P., & Klein, D. (Eds.), Sourcebook of Family Theory and Research. (Pp. 293-294). Beverly Hills, CA: Sage. Mancini, J. A., Bowen, G. L., & Martin, J. A. (2005). Community social organization: A conceptual linchpin in examining families in the context of communities. Family Relations, 54, 570-582. Mancini, J. A., Nelson, J. P., Bowen, G. L., & Martin, J. A. (2006). Preventing intimate partner violence: A community capacity approach. Journal of Aggression, Maltreatment, and Trauma, 13(3/4), 203-227. Bowen, G. L., Martin, J. A., Liston, B. J., & Nelson, J. P. (2008). Community practice in the United States Air Force: Connecting theory and practice. In A. R. Roberts (Eds.), Social Workers' Desk Reference (2nd Ed.). (Pp: 525-533). New York: Oxford University Press. Huebner, A. J., Mancini, J. A., Bowen, G. L., & Orthner, D. K. (2009). Shadowed by war: Building community capacity to support military families. Family Relations, 58, 216-228. Martin, J.A., & Sherman, M.D. (2009). The impact of military life on individuals and families: Resources and intervention. In S. Price & C. Price, (Eds.), Families and change: Coping with stressful events and transitions (4th ed., pp. 381-397). New York: SAGE.
Yarvis, J. (2008) Subthreshold PTSD in Veterans with Different Levels of Traumatic Stress: Implications for Prevention and Treatment with Populations with PTSD. Saarbrucken, Germany: VDM Verlag Dr. Muller Publishers, ISBN- 978-3-639-08332-3.
Yarvis, J.S., (2011) A Civilian Social Worker’s Guide to the Treatment of War-Induced PTSD. Social Work in Health Care (50) 1. Coulter, I., Nester, P. & Yarvis, J., (2010) Social Fitness and the Military. Military Medicine (175) Suppl 1.
Yarvis, J.S. and Schiess, L. (2008) Subthreshold PTSD as a predictor of depression, alcohol use, and health problems in soldiers. Journal of Workplace Behavioral Health 23(4).