2015 the science of assessing risk of heart attack, stroke and diabetes
TRANSCRIPT
E
Diagnbody providprivatscieneventand poputo themedicidentibiomapapemethorationstratifindiviprovepractthe algorbiblio
PRE-
THEHEAR
EVIDENCE A
nosing risk is perform
ders. Alote compance to idents early in reversed alations of pe corporatecal data froify certain arkers in thr explainsodologies.
nale is expfying populdual risk le
en, the tesice under tcompany’sithms, is d
ography in in
-PUBLICAT
E SCIERT ATTA
BASE FORAND IMPLI
of heart dismed every dong with thny, Predictintify a pertheir develoand the e
people, suce setting of om an indiv
patterns he person’ss and d Each te
plained in lations of pevels, is ousting regimthe U.S. sts confidendocumentencluded.
TION DRAF
NCE OACK, STR PREDICTCATIONS
sease/attacday by a smhese physive Health son’s predopment, whevents avoch as emplo
an employidual is proand corre
s test resuldocuments esting proto
lay terms.people, sucutlined. Althmen that thtandard of ntial, propd and cite
FT, 2016
F ASSETROKETIVE HEALFOR SELF
K. Char
ck, stroke, amall but gricians, nurIntelligenc
dictive risk hile the conoided. pHi oyees, by byer and emocessed by espondencelts if risk o
the comocol in pH The comch as emphough widehe compancare. Tha
prietary pred in som
ESSINGE AND DLTH: AN INF-INSURED
rles Coope
and diabeterowing numrses, and ce (pHi),
of these nditions ca
applies tbringing cli
mployees’ wa series of
es betweeof disease impany’s Hi’s methodmpany’s mloyees, acc
ely publisheny applies at regimen, rotocols a
me detail. A
G RISK DIABETNTRODUCTD EMPLOY
er, CEO
es in the humber of mespecialists,applies cuconditions n be prevehis sciencinical stand
workplaces.f algorithmsen and amis present. protocols dology and
methodologycording to
ed and cliniis not cucombined
and diagnAn introdu
OF TES TION
YERS
uman edical , the
urrent and
ented ce to dards The
s that mong
This and
d its y for their ically
urrent with
nostic ctory
DRAFT, NOT FOR PUBLICATION 1
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
INTRODUCTION
Heart attack, stroke, and diabetes comprise the primary drivers of health care costs, disability, and death in America, and by extension, virtually all U.S. employers. (Heidenreich, Paul A. MD; et al, 2011) (U.S. Centers for Disease Control and Prevention, 2014) (Yoon, Paula W.; et al, 2014)
Each of these three diseases and their related events are preventable by applying the science upon which the company is founded. (Fries, James F.; Koop, C. Everett; et al, 1993) (U.S. Centers for Disease Control and Prevention, 2014) (Bradley Bale & Amy Doneen, 2014)
The applied science, the evidence base, was first outlined for lay audiences in 2014’s “How to Beat the Heart Attack Gene” by Dr. Bradley Bale and Amy Doneen. Much of what pHi does is based on the evidence documented in this book.
As Bale & Doneen and many, many others have argued, it makes supreme sense to prevent heart disease, stroke and diabetes simultaneously, as they are three preventable conditions that are inexorably linked in the human body. The scientific and medical literature proves that there exists an unmistakable, clinical, cause-effect relationship between the three; some of that empirical evidence is outlined herein.
However, preventing these three diseases is not currently the focus of the U.S. healthcare system; the entire U.S. healthcare ecosystem of providers, payers, patients, insurers, etc. still stubbornly functions almost exclusively as a self-feeding, perpetual, supply-and-demand cycle for disease management -- the treatment and care of disease once it arrives in a patient. (Fries, James F.; Koop, C. Everett; et al, 1993)
Rather than perpetuating the need and demand for medications and medical services, preventing the disease from ever arriving in the patient is the mission of pHi LLC: we exist to keep people healthy – off of medications and out of hospitals – by using the latest science and risk-diagnostic tools to help them get way out in front of disease that may be developing in their bodies.
Readers are strongly encouraged to diligently research the science behind what pHi LLC does, how we do it, why we do it, and the clinical outcomes that our approach produces.
A sampling of that science is introduced here…and the science we adopt and apply has been vetted very carefully over the years. (Marcus, Adam & Oransky, Ivan, 2015)
However, the scientific evidence base for pHi LLC is not built solely on the published results of clinical trials and research in the world’s leading scientific and medical journals; it is equally supported by the practical, first-hand, clinical results created by one of the authors as a practicing physician caring for hundreds of patients over many years. (Private-practice physician, 2015)
DRAFT, NOT FOR PUBLICATION 2
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Diabetes prevention was first reported to be possible in the landmark Diabetes Prevention Program (DPP) as reported in the New England Journal of Medicine in 2002. (Diabetes Prevention Program Research Group, 2002) The findings were subsequently verified in other clinical trials.
Among the key findings of the DPP: a fifty-eight percent (58%) reduction in new cases of diabetes occurred due to intensive lifestyle interventions—primarily due to an average weight loss of seven percent (7%) over six months. (Yoon, Paula W.; et al, 2014) (Moore LLVAJ; et al, 2000)
Moreover, the importance of extremely tailored, personalized health coaching, precisely the type of prevention planning and coaching pHi LLC applies to an individual’s health goals, was also essential to the results. (Whelton PK; et al, 1998)
The causes of heart attack and stroke, both closely linked to diabetes, go far beyond just a cholesterol problem. (Ross, 1999) (Jia Q.; et al, 2012) (Goldstein, Larry B. , et al, 2011) In fact, approximately fifty (50) percent of heart attacks and strokes occur in patients who present “normal” cholesterol levels. (Ridker P. , 2001)
Current science tells us that: “While routine lipid screening plays an important role in cardiovascular risk assessment it does not provide a complete picture of your health…[r]ecent evidence goes beyond lipids to suggest that inflammation within the artery wall is the primary contributor to this residual risk for heart attack and stroke.” (Cleveland HeartLab, Our Science, 2015)
As we shall see, diagnosing a person’s risk of heart attack and stroke often leads the provider or clinician to look elsewhere for that “complete picture” of a person’s health and risk of disease, e.g.: “One of the safest ways to check for plaque in your arteries is an ultrasound exam of the major blood vessels in your neck…abnormalities that can be detected by this painless 15-minute exam, known as carotid intima-media thickness (cIMT), are strongly linked to high risk for heart attacks and strokes.” (Bradley Bale & Amy Doneen, 2014) 1 (Stein, James H., et al, 2008)
In prevention science, detection of risk – and detection of evidence of the earliest “subclinical” stages of disease -- is an absolute prerequisite to prevention of disease and disease-caused events. Prevention of heart disease/attack, stroke and diabetes must detect all of the known contributory factors – based on current science and clinical evidence -- and apply established therapeutic principles essential to their prevention. (Shah, 2010)
1 p. 21
DRAFT, NOT FOR PUBLICATION 3
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
PHILOSOPHY AND APPROACH
The human body presents biomarkers of the presence of plaque, inflammation, and insulin resistance, which are the precursors of heart attacks, stroke, and diabetes.2 These biomarkers present themselves in identifiable patterns in certain test and lab results long before the disease ever arrives in a human body. (Penn, M. S., et al, 2015) (Bradley Bale & Amy Doneen, 2014)
It can take 20 years or more for diabetes, cardiovascular disease, coronary artery disease, and risk of heart attack and/or stroke to develop in the human body. The early warning signs for these conditions are there – in a person’s blood work, for example. The predictive patterns of certain relationships between a person’s biomarkers are there. They are road signs on the way to diseases and their consequences.
But, in spite of the overwhelming scientific evidence base, most employers – indeed, in our view, the vast majority of the healthcare ecosystem in the U.S. -- remain focused on looking for the presence of these conditions rather than the presence of their unmistakable early warning signs.
To repeat: pHi LLC endeavors to help a person at risk get way out in front of a disease developing in his or her body and prevent it…to leave the road to illness or do a 180 and turn around on that road and head the opposite way. This is disease prevention. (Fries, James F.; Koop, C. Everett; et al, 1993)
Obviously, disease prevention also prevents the need for “disease management” in corporate wellness terms.
The company applies a proven testing regimen and its own, proprietary methodology to discover the patterns of developing disease-risk quickly and with relative ease: test and lab results are processed by algorithms and analyzed clinically to diagnose risk and determine if additional testing is needed to determine root causes of certain conditions.
THE SCIENCE OF PREVENTION
The prevention science that pHi LLC applies presents a large body of clinical evidence documenting its efficacy over some two decades. The science and methods pHi LLC applies has been clinically proven and widely published in the scientific and medical literature for some time.3
Equally as important: the company constantly monitors clinical results from emerging scientific tools and updates its protocols and algorithms accordingly. Only proven science that has been clinically proven and peer-vetted is applied. (Marcus, Adam & Oransky, Ivan, 2015)
2 The presence of insulin resistance is in itself a predictor of diabetes mellitus. 3 The attached bibliography is representative only.

DRAFT, NOT FOR PUBLICATION 4
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
That literature is vast; it is far too prodigious to even be sufficiently outlined here. The clinical and research evidence base, demonstrating that heart attacks, stroke, and diabetes can and are being prevented using the techniques and methods applied by pHi LLC is broad, deep and solid.
Prevention of these diseases/events is not a recent discovery or practice; the efficacy and clinical results of disease prevention have been well-published for some two decades at least. (Fries, James F.; Koop, C. Everett; et al, 1993)
Again, however, current practice has not yet caught up with the science of prevention; pHi LLC applies prevention science – testing, analysis and diagnosis of risk, risk stratification of populations, interventions -- that is not yet the norm for current practice in the U.S. healthcare system. That system remains based, at its core, on discovering the presence of existing disease and then treating, caring for, or “managing” that disease. This is the current “standard of care” in the United States.
The prevention science that the company practices aims to prevent heart disease, risk of heart attack, stroke, and diabetes from ever developing in a person’s body -- through early detection of the risk of disease, detection of the presence of subclinical disease, intervention, and altering the behaviors that will produce the disease. (Bradley Bale & Amy Doneen, 2014)
pHi LLC’s preventative protocols and methodologies, as well as its testing regimen, are based on the three decades of clinical, real-world experience of its medical director and proven science and technology. It could be argued that our application of today’s preventive science is based on the results of a 30-year clinical trial, using the latest medical science and technology. (Private-practice physician, 2015)
The company’s prevention methodologies are, by definition, disruptive: they are a direct challenge to the current standard of care in the United States.
Again: “prevention” in a workplace setting means reducing an employee’s need and demand for medical services…specifically, reducing the need and demand for the treatment and care of diseases that can indeed be prevented. (Fries, James F.; Koop, C. Everett; et al, 1993)
This is prevention science at its most fundamental: again, preventing the disease, by definition, prevents the need to “manage” the disease.

DRAFT, NOT FOR PUBLICATION 5
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
MEASURING RISK OF DIABETES, HEART ATTACK AND STROKE
We believe our approach to measuring a person’s risk of diabetes, heart disease/attack, and stroke is unique – especially in the corporate wellness world.
For populations of people, such as employees, the company presents a risk-stratification model based on the empirical data each employee presents through pHi LLC’s testing regimen – quantitative data – and through the employee’s self-reported qualitative data from his/her health risk assessment.
pHi LLC’s testing regimen starts with basic labs – but we interpret the results of those labs quite differently than what is common practice under the current standard of care. We look for different things.
Providers operating within today’s standard of care analyze those lab results for the presence of disease; pHi LLC analyzes those lab results for the presence of risk of developing disease…the predictive biomarkers or precursors of diabetes, heart disease/attack, and stroke. (Bradley Bale & Amy Doneen, 2014)
Same basic labs…but different missions, different protocols, and entirely different methodologies to interpreting the results.
The company analyzes those lab results and searches for certain patterns – the precursors of risk, according to established science. If a person’s lab results present concerns, unmistakable evidence of likely risk, then the company suggests that she/he proceed to additional testing.
The precursors of heart disease/attack, stroke, and diabetes – three preventable conditions that are inexorably linked in the human body – are very much present in a person’s basic lab results, as the science referenced herein documents.
It bears repeating: risk of these diseases and related events are, without question, measurable and early detection provides an extraordinary opportunity to prevent the disease(s) – and their tragic consequences -- from ever developing.
More critical: early detection of these diseases and related events is dependent on the clinical ability to read or recognize clinically proven, science-based patterns and relationships between and among these existing biomarkers or precursors of disease in a person’s body. pHi LLC applies its own, proprietary methodologies and algorithms to recognize these patterns and relationships; it is how we diagnose risk. (Private-practice physician, 2015)
pHi LLC testing is, in essence, risk mitigation for these three diseases and related events. Understanding the causes of heart disease, stroke and diabetes is the first step towards preventing them.
© 2015 Pinformati
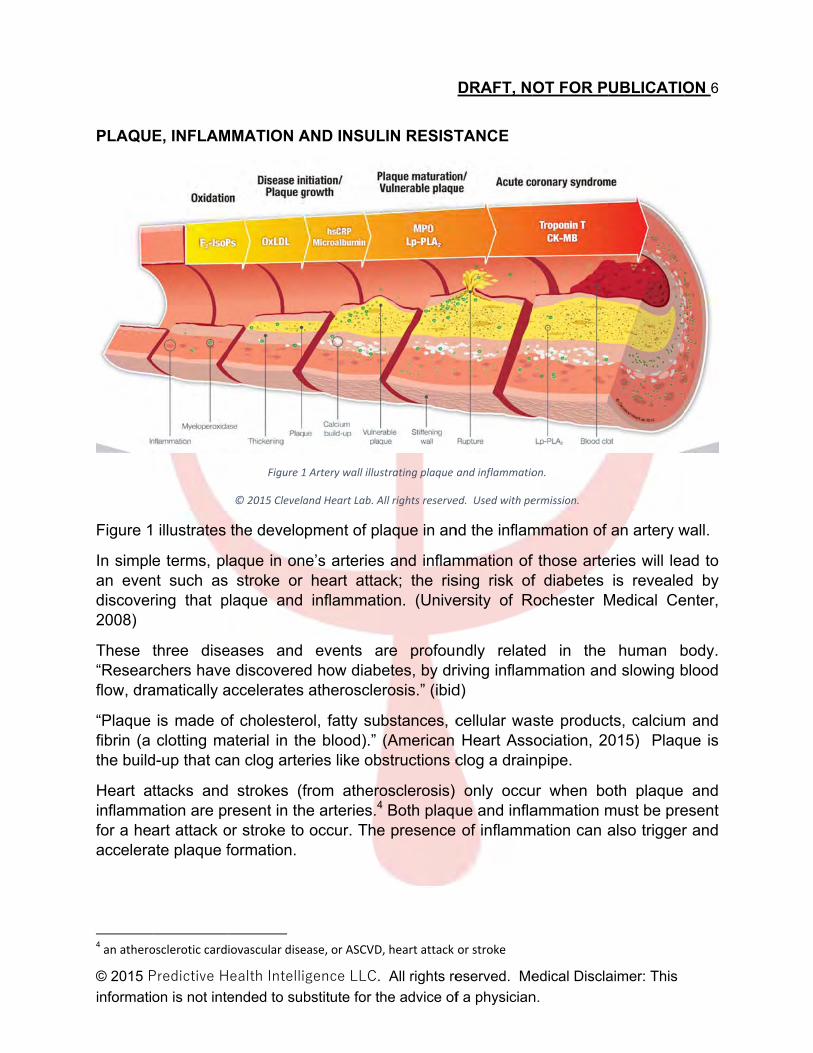
PLAQU
Figure 1
In simplan evendiscover2008)
These “Researflow, dra
“Plaque fibrin (a the build
Heart ainflammfor a heaccelera
4 an athero
Predictive Hon is not inte
E, INFLAM
illustrates
e terms, plnt such asring that p
three diserchers haveamatically a
is made oclotting ma
d-up that ca
ttacks andation are prart attack oate plaque f
osclerotic card
ealth Intelliended to sub
MMATION A
Figure 1
© 2015 Clevela
the develo
aque in onstroke or
plaque and
eases and e discovereaccelerates
of cholesteraterial in than clog arte
strokes (fresent in thor stroke to formation.
iovascular dise
gence LLC.
bstitute for t
AND INSUL
1 Artery wall illus
and Heart Lab. A
pment of p
ne’s arteriesheart attainflammat
events ad how diabatheroscle
rol, fatty suhe blood).” eries like ob
from atherohe arteries.4
occur. The
ease, or ASCVD
All rights re
he advice of
LIN RESIST
strating plaque
All rights reserve
laque in an
s and inflamack; the ristion. (Unive
are profoubetes, by drerosis.” (ibid
bstances, c(American
bstructions c
osclerosis) 4 Both plaque presence
D, heart attack
DRAFT, N
eserved. Me
f a physician
TANCE
and inflammatio
ed. Used with pe
nd the inflam
mmation of sing risk ofersity of R
ndly relateriving inflamd)
cellular waHeart Ass
clog a drain
only occuue and infla of inflamm
or stroke
OT FOR P
edical Discla
n.
on.
ermission.
mmation of
f those artef diabetes
Rochester M
ed in the mmation an
ste producsociation, 20npipe.
ur when boammation m
mation can a
UBLICATIO
aimer: This
an artery w
eries will leais reveale
Medical Ce
human bd slowing b
cts, calcium015) Plaq
oth plaque must be prealso trigger
ON 6
wall.
ad to d by
enter,
body. blood
m and ue is
and esent r and
DRAFT, NOT FOR PUBLICATION 7
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
However, a large percentage of heart attacks and strokes occur in people with apparently clear, unobstructed arteries, the reason being that a small amount of plaque -- so small it doesn't even begin to obstruct the flow of blood -- can rupture like a small volcano from the body's process of inflammation, which is intended to actually reduce plaque or stabilize it.
This rupture unleashes a clotting cascade that can completely obstruct an artery within just a few minutes. If this happens in the wrong spot (e.g., near the heart or brain), a heart attack or stroke is likely.
Thus, even “trivial” amounts of plaque may be, in fact, the most deadly kind because of plaque rupture. The science referenced herein tells us that the majority of heart attacks and strokes occur because of plaque rupture rather than plaque choking off the artery.
DETECTING INSULIN RESISTANCE
To further complicate things, our body's responses to blood sugar via insulin can also cause both plaque and inflammation. This disease is called insulin resistance, which is the underlying driver of diabetes; it is also the root cause of most cardiovascular disease. (Bradley Bale & Amy Doneen, 2014) 5
A critical late effect of diabetes: it drives inflammation and slows blood flow, dramatically accelerating atherosclerosis. This causes inflammation that makes plaque more likely to swell, rupture and cut off blood flow through the clotting cascade. This causes inflammation that makes plaque more likely to swell, rupture and cut off blood flow. (Woo, Chang-Hoon; et al, 2008). Inflammation can cause plaque, as well as rupture it.
Insulin resistance is the most common cause of plaque formation. Seventy percent of people who have plaque also have insulin resistance. People with insulin resistance grow more plaque, they grow it faster, and that plaque is more susceptible to becoming inflamed. Plaque in and of itself is not a precursor of metabolic syndrome but rather the likely result of undetected/untreated metabolic syndrome.
The connection: the insulin resistance that has been developing for years is the real cause for that plaque to grow and multiply and then become inflamed…ergo, the seventy percent of people with plaque for whom insulin resistance is the primary cause of such plaque formation.
5 p. 57
DRAFT, NOT FOR PUBLICATION 8
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Again, less than half of all people who experience a heart attack presented cholesterol problems prior to the attack. What this means: under the current standard of care in the United States, more than half of all heart attack victims present “normal” cholesterol levels prior to their heart attacks. (Cleveland HeartLab, Our Science, 2015) (Bradley Bale & Amy Doneen, 2014)
Yet seventy percent of these heart attack victims presented an insulin problem prior to their heart attacks…which is why detecting insulin resistance and metabolic syndrome is so critical and which is why this is a key component of the pHi LLC regimen.
METABOLIC SYNDROME AND INSULIN RESISTANCE
Why pay to treat or “manage” diabetes when it – and its often-fatal consequences -- can be prevented?
Diabetes treatment, including its complications, exceeds $245,000,000,000 annually6 (U.S. Centers for Disease Control and Prevention, 2014).
Many are using the word “epidemic” to describe the incidence and prevalence of diabetes in the U.S. and globally. The numbers are indeed fearsome and show no signs of abating:
Seventy-four percent (74%) of ischemic stroke (the largely preventable variety of stroke) victims are insulin resistant, a well-described precursor to diabetes (Jia Q.; et al, 2012)
Sixty-six percent (66%) of people with acute coronary syndrome (threatened heart attack) are insulin resistant. (Meschia, J., et al., 2014)
Sixty percent (60%) of diabetics will die of heart attack or stroke (Seshasai, S., et al, 2011) (Jia Q.; et al, 2012); this risk is 2-8 times higher than for nondiabetics (Howard, B. et al., 2002) and causes death six years sooner than predicted for a 50-year-old with diabetes (Martin, BC; et al, 1992)
Yet diabetes is eminently preventable. The progression to diabetes occurs over a period of at least 20 years (Martin, BC; et al, 1992), with a conversion rate of roughly 11 percent annually (Diabetes Prevention Program Research Group, 2001).
Diabetes is a direct cause of arterial plaque formation (Nigro, J., et al., 2006) and plaque rupture (the proximate cause of the majority of heart attacks and strokes.) (ibid)
Metabolic syndrome is easily detected through basic labs, biometrics, and a knowledge of currently prescribed drugs and supplements; its presence predicts a 90% risk for insulin resistance. (Howard, B. et al., 2002)
6 latest data available, 2012
DRAFT, NOT FOR PUBLICATION 9
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Ninety percent of people diagnosed with metabolic syndrome are also insulin resistant; and virtually 100 percent of those who are insulin resistant become diabetics...if they live long enough. Again, sixty percent of diabetics will die of a heart attack or stroke at some point in their lives. (Jia Q.; et al, 2012)
Metabolic syndrome therefore becomes the most important, the most easily identified, and the earliest identifiable trigger for heart attacks, strokes, and diabetes…but metabolic syndrome in itself is not a predictor for all cases of insulin resistance the human body. (Bradley Bale & Amy Doneen, 2014)
Complicating matters: half of people with IR do not have metabolic syndrome…so metabolic syndrome in and of itself is not the only way to diagnose insulin resistance. This is where other testing in the pHi LLC regimen helps us comprehensively test for risk of insulin resistance. (ibid)
For example, there are five factors that determine metabolic syndrome; under the current standard of care, at least three of those factors must be present for a diagnosis of metabolic syndrome. (ibid) 7
But in pHi LLC’s methodology and its algorithms, the presence of one or two of these factors is an accurate, predictive red flag that the person in question might be insulin resistant and in need of further testing.
pHi LLC analyzes other factors in diagnosing risk of insulin resistance.
7 pp. 56‐60
DRAFT, NOT FOR PUBLICATION 10
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
INSULIN RESISTANCE: OTHER FACTORS
For example, the ratio of tryglycerides to HDL (found in basic lab results and analyzed in the pHi LLC regimen) might be a very good indicator of someone having insulin resistance and yet not presenting metabolic syndrome. (Private-practice physician, 2015)
A fasting blood sugar result of more than 88 also may indicate insulin resistance. The presence of an inordinate amount of small dense LDL, or a very high ApoB score…these are also indicators of insulin resistance. (ibid)
pHi LLC tests for metabolic syndrome and other indicators of insulin resistance to provide a person with advance warning that he/she might be headed for diabetes, stroke, and/or a heart attack. Both metabolic syndrome and insulin resistance can be prevented and, in some cases, even reversed if detected early enough.
© 2015 Pinformati
RISK ST
That is aand meemployedisease/
This strpresentsself-repohistory, test resu
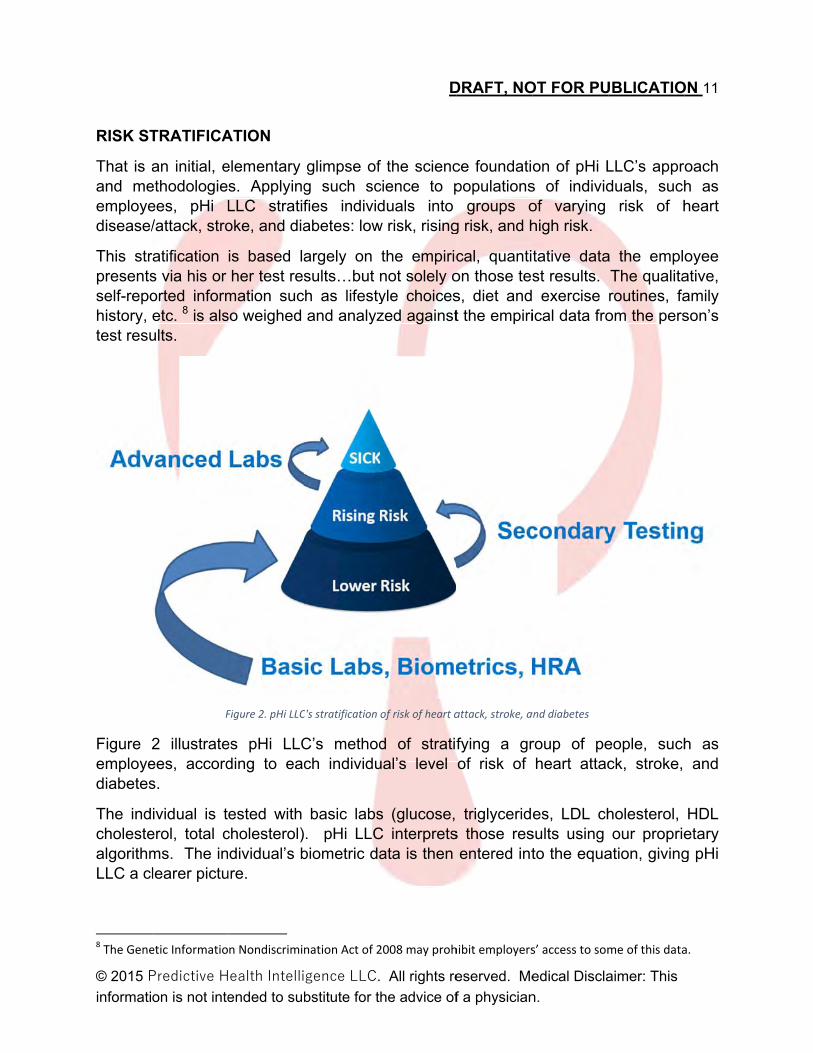
Figure 2employediabetes
The indcholestealgorithmLLC a cl
8 The Gene
Predictive Hon is not inte
TRATIFICA
an initial, eethodologieees, pHi L/attack, stro
ratification s via his or orted informetc. 8 is alsults.
F
2 illustrateees, accords.
ividual is terol, total cms. The inlearer pictu
etic Informatio
ealth Intelliended to sub
ATION
elementary s. ApplyingLLC stratifoke, and dia
is based laher test res
mation sucso weighed
Figure 2. pHi LLC
es pHi LLCding to eac
ested with cholesterol)dividual’s b
ure.
n Nondiscrimin
gence LLC.
bstitute for t
glimpse ofg such scfies individabetes: low
argely on sults…but nh as lifestyand analyz
C's stratification
C’s methodch individu
basic labs. pHi LLC
biometric da
nation Act of 2
D
All rights re
he advice of
f the scienccience to pduals into
w risk, rising
the empiricnot solely oyle choiceszed against
of risk of heart a
d of stratifual’s level
s (glucose, C interpretsata is then
2008 may proh
DRAFT, NO
eserved. Me
f a physician
ce foundatipopulations
groups og risk, and h
cal, quantion those tess, diet andt the empiri
attack, stroke, a
fying a grof risk of
triglycerids those res
entered int
hibit employers
OT FOR PU
edical Discla
n.
on of pHi Ls of individof varying high risk.
tative datast results. exercise ical data fro
and diabetes
roup of peheart attac
es, LDL chsults using to the equa
s’ access to som
UBLICATIO
aimer: This
LLC’s apprduals, such
risk of h
a the emplThe qualitaroutines, faom the pers
eople, suchck, stroke,
holesterol, our proprie
ation, giving
me of this data
ON 11
oach h as heart
oyee ative, amily son’s
h as and
HDL etary g pHi
a.
DRAFT, NOT FOR PUBLICATION 12
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Finally, the qualitative, self-reported information from the individual’s HRA is scored numerically.
The cumulative data from these three sources are processed by our algorithms and analyzed.
Depending on what the data present, the individual may present items that concern us. We recommend that the individual proceed to further testing…the carotid intima media thickness (CIMT) ultrasound. (Private-practice physician, 2015)
The data from the CIMT may present items that concern us further. We then recommend that individual for our advanced labs. (ibid)
When applied to a group of people, this protocol provides a dependable, accurate view of risk of heart disease, heart attack, diabetes and stroke. Each individual will know his or her risk of developing diabetes, risk of heart attack, and risk of stroke.
Some individuals will be classified in the low-risk group; others will fall into the rising-risk group; others will be classified as high-risk – all based on the empirical data they present, as interpreted through pHi LLC’s applied science and methodologies.
Each individual then receives a highly personalized prevention plan – according to their unique health profile in relation to these three diseases
What follows is a brief overview of pHi LLC’s testing and analytical protocols and regimen for a population of people, such as an employee group.
DRAFT, NOT FOR PUBLICATION 13
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
STEP ONE, FOR ALL: BASIC LABS AND INTERPRETATION
What is the science that enables pHi LLC to “see” or identify risk of disease in a person’s basic lab results?
As stated, metabolic syndrome is a primary and probably the most important cause of plaque growth and inflammation. Basic labs allow pHi LLC to identify the more specific indicators of metabolic syndrome. (Cleveland HeartLab, Our Science, 2015) (Bradley Bale & Amy Doneen, 2014) (pHi LLC, 2015)
What is different is in the way that pHi LLC interprets the results and information from those lab tests. pHi LLC synthesizes the results of multiple, clinical research findings9 to provide a more sophisticated and accurate analysis of those basic labs results.
Any one test in basic labs is only a suggestion of risk; the preponderance of the results taken together is what matters most. What we do is look at the totality of those individual indicators to help decide where an unacceptable level of probable risk exists; where such risk does exist, we recommend further diagnostic testing for that individual.
These diseases and conditions announce their intent to arrive in our bodies long before they do indeed arrive. Because of advances in prevention science and technology the past 25 years or so, we can recognize precursors of these diseases and conditions.
Those precursors are not a single “iffy” anomaly in a single test result but, rather, a pattern of relationships between biomarkers in our systems -- patterns in our blood and physiology that are predictors of diabetes, heart attack and stroke. (Private-practice physician, 2015)
As an example, when it comes to diagnosing the presence of risk of future or approaching diabetes, the science tells us that a normal fasting blood sugar score is 88 or below. Yet, the laboratory reports and the current standard of care in the U.S. are designed or “hardwired” to define a reading of below 100 as being “normal.” (ibid)
Also as an example, under the current standard of care, a lab test would report a fasting blood sugar score of 99 as being “normal” while the prevention science tells us that a normal blood sugar tells us that a score of 99 is “abnormal.” (ibid)
Why? Because current lab tests in the U.S. are configured to detect the presence of disease; if you have a score of 100, you have pre-diabetes. “You do not have a disease yet with a score of 99. You are normal.” (ibid)
9 See sample bibliography.

DRAFT, NOT FOR PUBLICATION 14
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
BLOOD SUGAR, TRIGLYCERIDES AND HDL
The science, however, is crystal clear that any fasting blood sugar score higher than an 88 indicates – with certainty – the presence of risk and the likelihood of progression towards disease. (Bradley Bale & Amy Doneen, 2014) “Your fasting blood sugar score is not normal. We need to find out why.” (Private-practice physician, 2015)
The route from 88 to 99 in a person’s fasting blood sugar is the road to diabetes, the development of disease. A score of 100 is pre-diabetes; a score of 126 is diabetes. pHi LLC, 2015)
However, according to current science and under pHi LLC’s regimen, a score of 89 or higher under pHi LLC’s regimen means risk of diabetes…”You are at risk of developing disease.” (ibid)
Under the current standard of care that often gets missed in basic lab results is that physicians are taught that the blood sugar itself is what is damaging the body via prediabetes or diabetes.
What they aren’t being taught, but upon which the science is clear, is that high insulin levels are very damaging to arteries…it acts as plaque fertilizer and a trigger for inflammation—precisely the conditions needed to have a heart attack or stroke. (Bradley Bale & Amy Doneen, 2014)
Insulin is not measured in standard blood tests…yet that is the smoking gun for arterial damage, as well as the direct cause of pre-diabetes and diabetes. pHi LLC uses other methods and testing to discover not only the presence of insulin resistance but the presence of risk of insulin resistance. (pHi LLC, 2015)
In addition to the factor of blood sugar levels in a person’s basic-labs results, another factor is the level of a person’s triglycerides. Under the current standard of care, diagnosing metabolic syndrome follows a similar “is it present?” approach using a person’s triglycerides score. (ibid)
If that score is above 150, that is a checkmark of “no disease present” under the current standard of care…but, just as we have seen with blood sugar levels, the science tells us that a truly “normal” triglyceride score is below 100. Therefore, under pHi LLC’s methodology, if a person presents a triglyceride score in the 100-150 range, that is a clear sign of the need for a closer look…a person who needs further scrutiny. (ibid)
Another factor is the HDL. For metabolic syndrome, the standard-of-care cutpoints are below 40 for men and below 50 for women. But the science tells us that you are at risk for plaque if you are below 50 for a man and below 60 for a woman. (ibid) Again, the search for the presence of disease under one protocol, the search for presence of predictive risk of disease under the pHi LLC preventative protocol.

DRAFT, NOT FOR PUBLICATION 15
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
So, let’s imagine that the individual presents enough cumulative data to warrant further testing. What type of further testing and why?
STEP TWO, FOR SOME: THE CAROTID ARTERY INTIMA MEDIA THICKNESS (CIMT) ULTRASOUND
Figure 3. Simple illustration of the utility of a carotid artery intima media thickness ultrasound.
Figure 3. The carotid intima media thickness (CIMT) ultrasound is one of the most effective diagnostic tools available for uncovering evidence of plaque or its precursor, arterial damage of the endothelium…factors that matter very, very much in diagnosing the risk of insulin resistance, diabetes, heart disease, heart attack, and stroke.
The CIMT ultrasound is inexpensive, noninvasive, and highly predictive of an event for heart attack or stroke; the tool has been researched and validated as a diagnostic tool for more than 25 years.
If the CIMT ultrasound discovers plaque, then we need to find out why. Is it a cholesterol issue, an inflammation issue or both or something else? Research in the past 15 years has shown that these two culprits are the main – but not the only – drivers in creating plaque:
DRAFT, NOT FOR PUBLICATION 16
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
“Experts once believed that atherosclerosis, or hardening of the arteries, developed when too much cholesterol clogged arteries with fatty deposits called plaques. When blood vessels became completely blocked, heart attacks and strokes occurred. Today most agree that the reaction of the body's immune system to fatty build-up, more than the build-up itself, creates heart attack risk. Immune cells traveling with the blood mistake fatty deposits for intruders, akin to bacteria, home in on them, and attack. This causes inflammation that makes plaques more likely to swell, rupture and cut off blood flow.” (Woo, Chang-Hoon; et al, 2008) (University of Rochester Medical Center, 2008)
Detection of arterial damage is central to the discovery of risk. Such detection and discovery using the inexpensive but sophisticated ultrasound technique mentioned above (CIMT) is critical to the success of prevention of arterial damage. (Belcaro, G. et al, 2001)
The panel of blood biomarkers used with the CIMT ultrasound has been validated in an economic modelling study to reduce national health care costs by 15 percent ($450 Billion annually). (Penn, M. S., et al, 2015) We believe these savings are soundly projectable for employee workforces…but we consider the average of 15 percent savings to be far too modest for employers.
If the CIMT ultrasound results present evidence of plaque and/or inflammation, pHi LLC recommends that the person proceed to our advanced labs, explained herein. Knowing the cause(s) of plaque and inflammation is the first step towards reversing and preventing both.
For corporations, we believe the CIMT ultrasound is the most effective and affordable method of identifying the presence, location, and amount of dangerous plaque and inflammation in an employee’s system.
There are no risks to taking the CIMT ultrasound. It is based on established technology, it is priced reasonably, and it’s quick. (Cedars-Sinai Heart Institute, 2015) In our view, the CIMT ultrasound is the most effective and efficient way of analyzing people who are already beginning to suffer from some of the risk factors.
The IMT taken by itself definitely can indicate risk of heart attack and stroke. If there is plaque present, it presents us with a 70 percent likelihood of an insulin problem. (Private-practice physician, 2015)
Even if you have only inflammation on your IMT and if you don’t do anything about it over ten years, you have a one-in-ten chance of having a heart attack or stroke -- without any plaque at all. (ibid)
If we find any plaque, even the tiniest amount, and you don’t do anything about it over ten years, then you have a forty percent (40%) chance of experiencing a heart attack or stroke. (ibid)
DRAFT, NOT FOR PUBLICATION 17
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
If you have significant amounts of plaque and you leave it untreated for ten years, then your odds of having a heart attack or stroke increase to 80 percent.
The CIMT is very predictive of an event over ten years. It is predictive of heart attack, stroke and, by extension, of the likelihood of insulin resistance, diabetes. (ibid)
The reason we use the CIMT ultrasound over a carotid duplex ultrasound is the difference in what each test shows us. (ibid)
A carotid duplex ultrasound, currently used under the standard of care, gives us a perspective only of blood flow through the artery to detect possible blockage -- a very advanced state of disease; it does not detect the cause of the restricted blood flow...the thickness, structure, etc. of the artery walls…where plaque and inflammation occur, where damage to the arterial wall occurs first, and where blood-flow blockages are born. (Cedars-Sinai Heart Institute, 2015) (Bradley Bale & Amy Doneen, 2014)10
Plaque and inflammation are the causes of the blockages or obstructions to arterial blood flow; a slowed or restricted blood flow is a consequence of those obstructions, plaque and/or inflammation.
We use the CIMT ultrasound to look at the structure of the artery itself to detect even the tiniest amount of plaque and/or inflammation…the earliest warning signs of trouble. (ibid)
Moreover: under the current standard of care, the carotid duplex ultrasound is normally ordered only for people who have had an event already…or on people for whom a physician expects existing blockage of an artery. (Private-practice physician, 2015)
What the science tells us about the CIMT ultrasound and its utility for early detection of plaque and inflammation:
“One of the safest ways to check for plaque in your arteries is an ultrasound exam of the major blood vessels in your neck…abnormalities that can be detected by this painless 15-minute exam, known as carotid intima-media thickness (cIMT), are strongly linked to high risk for heart attacks and strokes.” (Bradley Bale & Amy Doneen, 2014) 11 (Stein, James H., et al, 2008)
“Carotid intima-media thickness (CIMT) is associated with systemic atherosclerosis and cardioembolic conditions and predicts the risk of recurrent strokes.” (Ward, R. Parker, et al., 2008)
10 pp. 86‐89 11 p. 21
DRAFT, NOT FOR PUBLICATION 18
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
“A CIMT scan is a non-invasive technique using ultrasound (sound waves) to detect and quantify vascular disease and cardiovascular risk before any symptoms occur. The CIMT measures the thickness of the inner two layers of the carotid arteries (the intima and media) and the analysis tells your physician about your health and your risk for cardiovascular disease. Early detection of increased thickness may indicate the need for a more aggressive approach to managing the risk factors causally associated with heart disease and stroke. In addition, the scan is able to detect presence of plaques in the arteries – a manifestation of more significant vascular disease.” (Cedars-Sinai Heart Institute, 2015)
“Measurement of CIMT and determination of vascular age can identify individuals with advanced subclinical atherosclerosis, resulting in clinically meaningful alterations in CVD risk estimates.” (Adam D. Gepner, et al, 2006)
“Ultrasonographic measurement of intima media thickness has been reported as a procedure to detect the early stages of atherosclerosis. Carotid intima media thickness (CIMT) testing is a safe, noninvasive and cost effective method to detect early atherosclerotic vascular diseases.” (Kasliwal, Ravi R., et al, 2014)
“Over more than two decades, CIMT has been extensively researched and explored for its medical and clinical viability, and available in clinically since 2002. Several large, research-based cohort studies have clearly indicated a relationship between CIMT and CV events and emphasized its use.” (Kasliwal, Ravi R., et al, 2014)
“Presently, there are [sic] growing consensus for the use of CIMT in risk prediction in asymptomatic individuals or patients at risk of coronary diseases, especially type 2 diabetics. American Heart Association (AHA) prevention conference V in 2001 recognized that traditional risk factors alone were insufficient in categorizing risk of patients and had recommended the use of CIMT for risk stratification. (Smith SC Jr, et al, 2000) In 2004, Wackers et al. (Wackers FJ, et al, 2004) also suggested that two or more risk factors failed to identify large proportion of patients (41%) with silent ischemia as revealed from baseline analysis of the SPECT data. Two years later, the task force Screening for Heart Attack Prevention and Education (SHAPE) recommended all asymptomatic middle-aged and older men and women to be screened using noninvasive imaging to detect and treat patients with subclinical atherosclerosis. (Naghavi, M., et al, 2006) A large European prospective study called the Carotid and Femoral Ultrasound Morphology Screening and Cardiovascular Events (CAFES-CAVE) (Belcaro, G. et al, 2001)trial demonstrated significant predictive values in low-risk subjects. The recent consensus statement from the ASE in 2008 reiterated results of previous studies and recommended the use of carotid ultrasound for identifying subclinical atherosclerosis and in evaluating the CVD risk in asymptomatic individuals at intermediate risk.” (Kasliwal, Ravi R., et al, 2014)
DRAFT, NOT FOR PUBLICATION 19
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
“The scan takes 10 minutes and is performed by a sonographer. There is no preparation needed for the test and there is no radiation and no injections involved in the scan. Also, you do not need to disrobe for the test.” (Cedars-Sinai Heart Institute, 2015)
“More than a decade ago, this test’s extraordinary clinical value in predicting risk of heart attacks and disease were beginning to emerge in the scientific and medical literature: “Measurement of CIMT, a noninvasive estimate of current atherosclerotic burden, is feasible in a clinical setting and can be integrated into CHD risk assessment models. Determining VA [“vascular age”] using CIMT values may help individualize the age component of population-based CHD risk estimates.” (Stein, James H., et al, 2004) (Allan, Paul L., et al, 1997)
“Carotid intima media thickness testing provides a noninvasive, ultrasound-based technique to measure the burden of noninvasive atherosclerosis in the carotid artery. The principal evidence supporting the use of the test has been derived from large, research-based cohort studies, which clearly show a relationship between CIMT and incident coronary heart disease (CHD) events.” (The Society of Atherosclerosis Imaging and Prevention, 2010)
DRAFT, NOT FOR PUBLICATION 20
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
STEP THREE, FOR SOME: ADVANCED LABS
The CIMT ultrasound results tell us when damage to the arteries is occurring…but not the root causes for the damage, the reasons for the damage. Results from pHi LLC’s advanced-labs protocol tell us the causes of the damage, allowing us to develop a specific, personalized prevention strategy for the individual. (Bradley Bale & Amy Doneen, 2014) (Private-practice physician, 2015)
The CIMT ultrasound tells us the smoke…the advanced labs show us the fire, the root causes. CIMT shows us what is going on…advanced labs tell us why. (pHi LLC, 2015)
Some people have been misled to believe that heart attack, stroke, and diabetes is just a cholesterol problem. Not all cholesterol is bad, of course…our bodies need this vital chemical to exist and keep us alive. (ibid)
In our bodies, a system exists that takes cholesterol from where it is manufactured in the liver to where it is used in the body to keep us alive. The “bad” cholesterol is the LDL cholesterol – or the “least desirable” cholesterol. If you have too much LDL cholesterol, more than your body actually needs to keep you alive, it accumulates in and around the arteries as garbage. (ibid)
We now know that some types of that LDL cholesterol are more toxic than others. The large variety is actually so big that it can’t build up underneath the lining of the artery. The more toxic variety is called “small dense LDL” – it easily builds up underneath that artery lining and is indeed very toxic. So we now know now to look for and measure different varieties of LDL cholesterol and for different sizes. (ibid)
Another type of cholesterol is HDL – or “highly desired” cholesterol, the “good” cholesterol. Its function is to go through the body and find that excess cholesterol, the unused waste cholesterol. HDL too comes in sizes…the larger the HDL, the more excess cholesterol it is carrying back to the liver. (ibid)
One out of every three Americans is born with a type of cholesterol that doesn’t even show up on traditional cholesterol test…the “corkscrew” cholesterol known as Lipoprotein (a). (ibid)
Lipoprotein (a) looks like a corkscrew and functions like a corkscrew: it literally attaches itself to the lining of the artery and pulls cholesterol underneath the artery and makes it more toxic than it was. We can measure its presence. We can better tell who is at risk of heart attack and stroke. (ibid)
Some of these aspects of the behavior of cholesterol functions help us understand why more than half of all people who have a heart attack or stroke have been told that their cholesterol levels were “normal.” That is the result of looking only at total HDL and not at the entire picture. (ibid)
DRAFT, NOT FOR PUBLICATION 21
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
When an individual presents data from his or her basic labs, HRA, biometrics, and CIMT scan that points to larger root causes of problems, we recommend that individual for pHi LLC’s advanced labs protocol.
What follows is a brief explanation of those labs, why pHi LLC conducts them, why they are important detectors of risk of disease, what we look for, and why they matter.
A sampling of the science behind each dimension is presented.
DRAFT, NOT FOR PUBLICATION 22
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Small Dense Low Density Lipoprotein (sdLDL)
What it is: perhaps the most toxic type of LDL cholesterol yet discovered, a known cause of cardiovascular events. (Packard, Chris, et al, 2000) (Lamarche, B., et al, 1999) (Lamarche, Benoit; et al, 1997)
The large variety of LDL is actually too big build up underneath the lining of the artery. “Small dense LDL” easily builds up underneath that artery lining and is indeed very toxic. pHi LLC tests for the presence of sdLDL, determines its type, and measures that presence; the company’s protocols allow us to now to look for and measure different varieties of LDL cholesterol and for different sizes.
“LDL, which carries “bad” cholesterol, exists either as large, more buoyant particles or as smaller, denser particles (sdLDL). sdLDL is more easily oxidized, has a higher affinity for vessel walls, and remains in the circulation longer because it is less likely to be cleared by the liver, making it more atherogenic than larger LDL particles.” (Cleveland Heart Lab, sd-LDL, 2014)
According to the Cleveland Heart Lab and a large body of published scientific and medical literature: “The small dense form of LDL (sdLDL) cholesterol carries a three-fold increased risk of myocardial infarction compared to large LDL cholesterol.” (Cleveland Heart Lab, sd-LDL, 2014) (Lamarche, B., et al, 1999) (Lamarche, Benoit; et al, 1997) (Packard, Chris, et al, 2000)
“The small dense LDL test can be used to determine cardiovascular risk in individuals with metabolic syndrome or established/progressing coronary artery disease, individuals with triglyceride levels between 70 and 140 mg/dL, as well as individuals with a diet high in trans-fat or carbohydrates.” (Cleveland Heart Lab, sd-LDL, 2014)
pHi LLC tests for small dense low density lipoprotein (sdLDL) and measures it under our standard of care.
Gateway to evidence base:
1. Austin MA et al. Atherogenic lipoprotein phenotype. A proposed genetic marker for coronary heart disease risk. Circulation. 1990; 82: 495-506.
2. Chapman MJ et al. Atherogenic, dense low-density lipoproteins. Pathophysiology and new therapeutic approaches. Eur Heart J. 1998; 19 Suppl A: A24-30.
3. Grundy SM. Hypertriglyceridemia, atherogenic dyslipidemia, and the metabolic syndrome. Am J Cardiol. 1998; 81: 18B-25B.
4. Koba S et al. Significance of small dense low-density lipoproteins and other risk factors in patients with various types of coronary heart disease. Am Heart J. 2002; 144: 1026-1035.
5. Rosensen RS et al. Relations of lipoprotein subclass levels and low-density lipoprotein size to progression of coronary artery disease in the Pravastatin
DRAFT, NOT FOR PUBLICATION 23
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Limitation of Atherosclerosis in the Coronary Arteries (PLAC-I) trial. Am J Cardiol. 2002; 90: 89-94.
6. St-Pierre AC et al. Comparison of various electrophoretic characteristics of LDL particles and their relationship to the risk of ischemic heart disease. Circulation. 2001; 104: 2295-2299.
DRAFT, NOT FOR PUBLICATION 24
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
ApoB (apolipoprotein B)
What it is: a gene and a predictor or cardiovascular events and of type 2 diabetes. (Heart Health Special Report, 2008) (Martin, Seth S., et al, 2009) (Walldius, Göran MD, et al, 2001)
The Guidelines for the Primary Prevention of Stroke as enumerated by the American Heart Association and the American Stroke Association in 2014 (O’Donnell, M.,et al., 2010) and the INTERSTROKE study (Meschia, J., et al., 2014) specifically recommend measuring the ratio of ApoB:ApoA1 ratio in the blood.
Twenty-five percent (25%) of strokes are driven by an unbalanced ratio of ApoB:ApoA1 ratio in the blood. This is a modifiable risk factor – a factor that is overlooked if only basic labs are performed. (O’Donnell, M.,et al., 2010) (Meschia, J., et al., 2014).
Under its standard of care, pHi LLC measures the ApoB:ApoA1 ratio in the blood.
“Research published in The Lancet reviewed five studies of LDL cholesterol and apoB in nearly 200,000 people. The researchers concluded that high levels of apoB were more strongly linked with future heart attack risk than LDL cholesterol levels. (Heart Health Special Report, 2008)
“A second report published in Circulation studied more than 1,500 adults. The participants were categorized based on their LDL cholesterol and apoB levels. Those with normal LDL cholesterol and high apoB levels were more likely to have other heart attack risk factors—such as low high-density lipoprotein (HDL) cholesterol and high triglyceride levels, abdominal obesity, and high fasting insulin levels—than those with high LDL cholesterol and normal apoB levels. The researchers pointed out that if apoB levels were used to determine who needs cholesterol-lowering medication, 25% of the participants with normal LDL cholesterol levels would meet the criteria. (ibid), (Heart Health Special Report, 2008) (Walldius, Göran MD, et al, 2001) (Gene 388, National Center for Biotechnology Information, U.S. National Library of Medicine, National Institutes of Health. , 2015)
pHi LLC tests for apolipoprotein B and measures it under our standard of care.
Gateway to ApoB evidence base:
1. Genetic association of APOB polymorphisms with variation in serum lipid profile among the Kuwait population. Al-Bustan SA, Alnaqeeb MA, Annice BG, Ebrahim GA, Refai TM. Lipids Health Dis. 2014 Oct 8; 13:157.
2. Relationship between the Apolipoprotein AI, B gene polymorphism and the risk of nontraumatic osteonecrosis. Yin JM, Liu Z, Zhao SC, Guo YJ, Liu ZT. Lipids Health Dis. 2014 Sep 23;13:149

DRAFT, NOT FOR PUBLICATION 25
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
3. ApoB gene SpIns/Del, XbaI polymorphisms and myocardial infarction: a metaanalysis of 7169 participants. Li YY. J Cardiovasc Med (Hagerstown). 2014 Sep; 15(9):717-26.
4. Proprotein convertase subtilisin kexin type 9 promotes intestinal overproduction of triglyceride-rich apolipoprotein B lipoproteins through both low-density lipoprotein receptor-dependent and -independent mechanisms. Rashid S, Tavori H, Brown PE, Linton MF, He J, Giunzioni I, Fazio S. Circulation. 2014 Jul 29;130(5):431-41.
5. Apolipoprotein B-48: a unique marker of chylomicron metabolism. Nakajima K, Nagamine T, Fujita MQ, Ai M, Tanaka A, Schaefer E. Adv Clin Chem. 2014;64:11777. Review.
6. Bipolar disorder with comorbid binge eating history: a genome-wide association study implicates APOB. Winham SJ, Cuellar-Barboza AB, McElroy SL, Oliveros A, Crow S, Colby CL, Choi DS, Chauhan M, Frye MA, Biernacka JM. J Affect Disord. 2014 Aug;165:151-8
7. Ixeris dentata decreases ER stress and hepatic lipid accumulation through regulation of ApoB secretion. Lee MR, Lee HY, Lee GH, Kim HK, Kim NY, Kim SH, Kim HR, Chae HJ. Am J Chin Med. 2014;42(3):639-49.
8. Polymorphisms XbaI (rs693) and EcoRI (rs1042031) of the ApoB gene are associated with carotid plaques but not with carotid intima-media thickness in patients with diabetes mellitus type 2. Nikolajevic Starcevic J, Santl Letonja M, Praznikar ZJ, Makuc J, Vujkovac AC, Petrovic D. Vasa. 2014 May;43(3):171-80.
9. Relations of change in plasma levels of LDL-C, non-HDL-C and apoB with risk reduction from statin therapy: a meta-analysis of randomized trials. Thanassoulis G, Williams K, Ye K, Brook R, Couture P, Lawler PR, de Graaf J, Furberg CD, Sniderman A. J Am Heart Assoc. 2014 Apr 14;3(2):e000759
10. Skeletal muscle apolipoprotein B expression reduces muscular triglyceride accumulation. Bartels ED, Ploug T, Størling J, Mandrup-Poulsen T, Nielsen LB. Scand J Clin Lab Invest. 2014 Jun;74(4):351-7.
11. Combined use of apolipoprotein B/apolipoprotein A1 ratio and non-high-density lipoprotein cholesterol before routine clinical lipid measurement in predicting coronary heart disease. Pan L, Lu G, Chen Z. Coron Artery Dis. 2014 Aug;25(5):433-8.
12. Impact of myeloperoxidase-LDL interactions on enzyme activity and subsequent posttranslational oxidative modifications of apoB-100. Delporte C, Boudjeltia KZ, Noyon C, Furtmüller PG, Nuyens V, Slomianny MC, Madhoun P, Desmet JM, Raynal P, Dufour D, Koyani CN, Reyé F, Rousseau A, Vanhaeverbeek M, Ducobu J, Michalski JC, Nève J, Vanhamme L, Obinger C, Malle E, Van Antwerpen P. J Lipid Res. 2014 Apr;55(4):747-57.
13. Surface tensiometry of apolipoprotein B domains at lipid interfaces suggests a new model for the initial steps in triglyceride-rich lipoprotein assembly. Mitsche MA, Packer LE, Brown JW, Jiang ZG, Small DM, McKnight CJ. J Biol Chem. 2014 Mar 28;289(13):9000-
DRAFT, NOT FOR PUBLICATION 26
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
14. LDL receptor/lipoprotein recognition: endosomal weakening of ApoB and ApoE binding to the convex face of the LR5 repeat. Martínez-Oliván J, Arias-Moreno X, Velazquez-Campoy A, Millet O, Sancho J. FEBS J. 2014 Mar;281(6):1534-46.
DRAFT, NOT FOR PUBLICATION 27
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
ApoA1 (apolipoprotein A-I)
What it is: apolipoprotein A-I is an inherited gene (Gene ID: 335) that affects levels of a person’s HDL or “good” cholesterol. A deficiency of ApoA1 has been proven to decrease levels HDL and function as a primary driver of atherosclerosis. (Ordovas, J M; et al, 1989) (Funke, H., et al, 1991) (National Center for Biotechnology Information, U.S. National Library of Medicine, 2015)
As stated earlier, the Guidelines for the Primary Prevention of Stroke from the American Heart Association and the American Stroke Association in 2014 (O’Donnell, M.,et al., 2010) and the INTERSTROKE study (Meschia, J., et al., 2014) specifically recommend measuring the ratio of ApoB:ApoA1 ratio in the blood.
Twenty-five percent (25%) of strokes are driven by an unbalanced ApoB:ApoA1 ratio in the blood. This is a modifiable risk factor – a factor that is overlooked if only basic labs are performed. (O’Donnell, M.,et al., 2010) (Meschia, J., et al., 2014).
Under its standard of care, pHi LLC measures the ApoB:ApoA1 ratio in the blood.
“This gene encodes apolipoprotein A-I, which is the major protein component of high density lipoprotein (HDL) in plasma. The protein promotes cholesterol efflux from tissues to the liver for excretion, and it is a cofactor for lecithin cholesterolacyltransferase (LCAT) which is responsible for the formation of most plasma cholesteryl esters. This gene is closely linked with two other apolipoprotein genes on chromosome 11. Defects in this gene are associated with HDL deficiencies, including Tangier disease, and with systemic non-neuropathic amyloidosis.” (National Center for Biotechnology Information, U.S. National Library of Medicine, 2015)
pHi LLC tests for apolipoprotein A-I and measures it under our standard of care.
Gateway to ApoA1 evidence base:
1. A role for Apolipoprotein A-I in the pathogenesis of multiple sclerosis. Meyers L, et al. J Neuroimmunol, 2014 Dec 15. PMID 25468275
2. An experimentally robust model of monomeric apolipoprotein A-I created from a chimera of two X-ray structures and molecular dynamics simulations. Segrest JP, et al. Biochemistry, 2014 Dec 9. PMID 25423138,
3. Definition of human apolipoprotein A-I epitopes recognized by autoantibodies present in patients with cardiovascular diseases. Teixeira PC, et al. J Biol Chem, 2014 Oct 10. PMID 25170076
4. Investigation into the effect of hepatitis B virus on apoliprotein A1 expression and its mechanism. Jiang W, et al. Lipids Health Dis, 2014 Aug 13. PMID 25115832.
5. Elevated apolipoprotein A-I levels are associated with favorable prognosis in metastatic nasopharyngeal carcinoma. Jiang R, et al. Med Oncol, 2014 Aug. PMID 25023050

DRAFT, NOT FOR PUBLICATION 28
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
6. Anti-Apolipoprotein A-1 auto-antibodies are active mediators of atherosclerotic plaque vulnerability. Montecucco F., et al. Eur Heart J. 2011 Feb; 32(4):412-21.
7. Combined use of apolipoprotein B/apolipoprotein A1 ratio and non-high-density lipoprotein cholesterol before routine clinical lipid measurement in predicting coronary heart disease. Pan L, et al. Coron Artery Dis. 2014 Aug;25(5):433-8.
.
DRAFT, NOT FOR PUBLICATION 29
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Lipoprotein (a)
What it is: “the dangerous cholesterol most doctors don’t check.” (Bradley Bale & Amy Doneen, 2014)12
Misconceptions, myths, and misinformation about cholesterol abound in the United States. One of the most harmful myths is that doctors routinely check and treat patients for all forms of harmful cholesterol that raise heart attack and stroke risk. (ibid)
The reality is that “…most healthcare providers do not check patients for a common, inherited cholesterol problem that’s been shown, unequivocally, to actually cause heart attacks. (ibid).
Lipoprotein (a) is a “…subtype of LDL (bad) cholesterol that’s also known as Lp(a). Not only do elevated levels triple a person’s risk for heart attacks, three large studies recently found, but Lp(a) also boosts risk for blood clots that can trigger a stroke. Lifestyle doesn’t influence Lp(a) levels, which are mainly determined by genes. Nor are statin drugs an effective treatment for elevated Lp(a).” (ibid)13
The science behind the toxicity of Lipoprotein (a) is overwhelming and beyond question. “Yet in the United States, it’s still not the standard of care to treat – or even measure – this dangerous form of cholesterol, found in elevated levels in up to one-third of heart attack victims.” (ibid)
pHi LLC tests for lipoprotein (a) and measures it under our standard of care.
Gateway to lipoprotein (a) evidence base:
1. Greenland P, Alpert JS, Beller GA, et al. 2010 ACCF/AHA guideline for assessment of cardiovascular risk in asymptomatic adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol.
2. Genest J, Libby P. Lipoprotein disorders and cardiovascular disease. In: Bonow RO, Mann DL, Zipes DP, Libby P, eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine.
3. Semenkovich, CF. Disorders of lipid metabolism. In: Goldman L, Schafer AI, eds. Goldman's Cecil Medicine.
4. Lp-PLA2 Activity and Mass are Associated with Increased Incidence of Ischemic Stroke: A Population-Based Cohort Study from Malmo, Sweden. Persson M, Berglund G, Nelson JJ, Hedblad B. Lp-PLA2 Activity and Mass are Associated with Increased Incidence of Ischemic Stroke: A Population-Based Cohort Study from Malmo, Sweden. Atherosclerosis. 2008; 200(1): 191-8.
12 pp. 120‐121 13 p. 42

DRAFT, NOT FOR PUBLICATION 30
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
5. Lp-PLA2 Studies Collaboration, Lipoprotein-Associated Phospholipase A2 and Risk of Coronary Disease, Stroke, and Mortality: Collaborative Analysis of 32 Prospective Studies. Thompson A, Gao P, Orfei L, Watson S, Di Angelantonio E, Kaptoge S, Ballantyne C, Cannon CP, Criqui M, Cushman M, Hofman A, Packard C, Thompson SG, Collins R, Danesh J. Lp-PLA2 Studies Collaboration, Lipoprotein-Associated Phospholipase A2 and Risk of Coronary Disease, Stroke, and Mortality: Collaborative Analysis of 32 Prospective Studies. Lancet. 2010; 375(9725): 1536-44.
6. Oxidized Phospholipids, Lipoprotein(a), Lipoprotein-Associated Phospholipase A2 Activity, and 10-year Cardiovascular Outcomes: Prospective Results from the Bruneck Study. Kiechl S, Willeit J, Mayr M, Viehweider B, Oberhollenzer M, Kronenberg F, Widermann CJ, Oberthaler S, Xu Q, Witztum JL, Tsimikas S. Oxidized Phospholipids, Lipoprotein(a), Lipoprotein-Associated Phospholipase A2 Activity, and 10-year Cardiovascular Outcomes: Prospective Results from the Bruneck Study. Arterioscler Thromb Vasc Biol. 2007; 27(8): 1788-95.
7. Plasma Lipoprotein-Associated Phospholipase A2 in Patients with Metabolic Syndrome and Carotid Atherosclerosis. Lipids in Health and Disease. Gong HP, Yimeng Du, Li-na Zhong, Zhao-qiang Dong, Xin Wang, Yong-jun Mao, Qing-hua Lu. Plasma Lipoprotein-Associated Phospholipase A2 in Patients with Metabolic Syndrome and Carotid Atherosclerosis. Lipids in Health and Disease. 2011; 10(13):18.
8. Plasma Lipoprotein-Associated Phospholipase A2 Levels in Heart Failure: Association with Mortality in the Community. Gerber Y, Shannon D. Dunlay, Allan S. Jaffe, Joseph P. McConnell, Susan A. Weston, Jill M. Killian, Veronique L. Roger. Plasma Lipoprotein-Associated Phospholipase A2 Levels in Heart Failure: Association with Mortality in the Community. Atherosclerosis. 2008;.07.035. [Epub ahead of print]

DRAFT, NOT FOR PUBLICATION 31
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
hsCRP (High-Sensitivity C-Reactive Protein)
What it is: inflammatory biomarker testing to help practitioners evaluate cardiovascular risk in patients.
The scientific evidence base demonstrating the value of testing levels of hsCRP seems beyond question. Measuring serum levels of hsCRP has been shown to be essential in guiding appropriate therapy to reduce cardiovascular events. (JUPITER Study Group, 2008)
pHi LLC tests for hsCRP and measures it under our standard of care.
“A CRP test measures inflammation throughout the body. It is a quite reliable and affordable indicator of cardiovascular disease.” (Cleveland HeartLab, hsCRP, 2015)
As Ridker pointed out in 2001: “Several large-scale prospective studies demonstrate that HSCRP is a strong independent predictor of future myocardial infarction and stroke among apparently healthy men and women and that the addition of HSCRP to standard lipid screening may improve global risk prediction among those with high as well as low cholesterol levels.” (Ridker P. , 2001)
“This inexpensive blood test uses a technology called laser nephelometry to rapidly measure very small amounts of C-reactive protein (CRP) with high sensitivity (accuracy). CRP, a protein produced by the liver, rises in the bloodstream when there’s inflammation throughout the body, which may indicate fire [extreme risk] in the arteries that could ignite a heart attack or stroke.” (Bradley Bale & Amy Doneen, 2014)14
As the Physicians Health Study demonstrated, CRP is a reliable predictor of heart problems – much more reliable than cholesterol levels. (Sesso, H. et al, 2012)
In that study, elevated levels of CRP were linked to triple the risk of heart attack, compared to doctors with normal levels of CRP. (Bradley Bale & Amy Doneen, 2014)15
“This finding was confirmed by the Harvard Women’s Health Study, originally begun in 1993 to examine the supposed benefits of aspirin and vitamin E in the primary prevention of cardiovascular disease and cancer in U.S. women. Results of the CRP test were more accurate than cholesterol levels in predicting heart problems.” (ibid)
Further: approximately fifty (50) percent of heart attacks and strokes occur in patients who present “normal” cholesterol levels. (Ridker, Paul M, M.D., et al, 2008) But, in our experience, we know of no corporate wellness provider who tests employees for several other, clinically proven predictors of cardiorisk…tests that offer much more accurate assessments of risk than basic cholesterol levels. (Ridker, Paul M, M.D., et al, 2008)
14 p. 113 15 ibid
DRAFT, NOT FOR PUBLICATION 32
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Gateway to hsCRP evidence base:
1. Ridker PM et al. Inflammation, aspirin, and the risk of cardiovascular disease in apparently healthy men. N Engl J Med. 1997; 336: 973-979.
2. Ridker PM et al. Comparison of C-reactive protein and low-density lipoprotein cholesterol levels in the prediction of first cardiovascular events. N Engl J Med. 2002; 347: 1557-1565.
3. Rost NS et al. Plasma concentration of C-reactive protein and risk of ischemic stroke and transient ischemic attack: The Framingham study. Stroke. 2001; 32: 2575-2579.
4. Ndrepepa G et al. N-terminal probrain natriuretic peptide and C-reactive protein in stable coronary heart disease. Am J Med. 2006; 119: 355.e1-355.e8.
5. Nissen SE et al. Statin therapy, LDL cholesterol, C-reactive protein, and coronary artery disease. N Engl J Med. 2005; 352: 29-38.
6. Ridker PM et al. C-reactive protein levels and outcomes after statin therapy. N Engl J Med. 2005; 352: 20-28.
7. Ridker PM et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. 2008; 359: 2195-2207.
8. Buhlin K et al. Periodontitis is associated with angiographically verified coronary artery disease. J Clin Periodontol. 2011; 38: 1007-1014.
DRAFT, NOT FOR PUBLICATION 33
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
LpPLA2 (lipoprotein-associated phospholipase-A2)
What it is: inflammatory biomarker testing to help practitioners evaluate risk of type 2 diabetes and cardiovascular risk in patients.
LpPLA2 is “…a blood vessel-specific enzyme that’s mainly attached to LDL (bad) cholesterol. Levels of LpPLA2 rise when arterial walls become inflamed, which may indicate that plaque is more likely to rupture, which could lead to a heart attack or stroke.” (Bradley Bale & Amy Doneen, 2014)16
“This enzyme is now emerging not only as biomarker of arterial wall inflammation, but also a direct player in the atherosclerotic disease process, with a recently published study suggesting that Lp-PLA2 plays a key role in cholesterol plaque formation and vulnerability 9risk that the plaque may rupture explosively and trigger a heart attack or stroke.” (ibid)17
“Increased levels of Lp-PLA2 may lead to increased risk of coronary heart disease, stroke, myocardial infarction.” (Cleveland Heart Lab, Lp-PLA2, 2015)
“Lp-PLA2, or lipoprotein-associated phospholipase-A2, measures disease activity within the artery wall below the collagen or calcified cap due to the activation of macrophages. Lp-PLA2 is not an acute phase reactant. When disease is active in the artery, increased levels of Lp-PLA2 are produced by macrophages and foam cells within the intima of the artery. Lp-PLA2 also interacts with oxidized LDL, which increases inflammation and enhances a proatherogenic state, as well as plaque vulnerability. Research suggests that it plays a direct role in the atherosclerotic disease process.” (Serruys PW, et al, 2008) (Cleveland Heart Lab, Lp-PLA2, 2015)
“The Lp-PLA2 test may be performed on individuals at intermediate or high risk for developing coronary heart disease who are any age with at least two major risk factors, those ≥65 years of age with one major risk factor, smokers, those with a fasting blood glucose of ≥100 mg/dL, or who those have metabolic syndrome.” (ibid)
Lp-PLA2 has also been proven to be a predictive indicator of type 2 diabetes mellitus; “… it is consistently higher among type 2 diabetics than nondiabetics.” (Nelson, TL, et al, 2012). As Nelson, et al found in 2012: “Lp-PLA(2) activity is positively associated with insulin resistance and predicts incident type 2 diabetes among older adults independent of multiple factors associated with diabetes pathogenesis.” (ibid)
16 pp. 115‐116 17 p. 116
DRAFT, NOT FOR PUBLICATION 34
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Gateway to LpPLA2 evidence base:
1. Nelson, et al. Lipoprotein-associated phospholipase A2 (Lp-PLA2) and future risk of type 2 diabetes: results from the Cardiovascular Health Study. J Clin Endocrinol Metab. 2012 May;97(5):1695-701.
2. Ferguson JF et al. Translational studies of lipoprotein-associated phospholipase A(2) in inflammation and atherosclerosis. J Am Coll Cardio. 2012; 59: 764-772.
3. Gonçalves I et al. Evidence supporting a key role of Lp-PLA2-generated lysophosphatidylcholine in human atherosclerotic plaque inflammation. Arterioscler Thromb Vasc Biol. 2012; 32: 1505-1512.
4. Serruys PW et al. (2008). Effects of the direct lipoprotein-associated phospholipase A2 inhibitor darapladib on human coronary atherosclerotic plaque. Circulation. 2008; 118: 1172-1182.
5. Kolodgie FD et al. Lipoprotein-associated phospholipase A2 protein expression in the natural progression of human coronary atherosclerosis. Arterioscler Thromb Vasc Biol. 2006; 26: 2523-2529.
6. Ballantyne CM et al. Lipoprotein-associated phospholipase A2, high-sensitivity Creactive protein, and risk for incident coronary heart disease in middle-aged men and women in the Atherosclerosis Risk in Communities (ARIC) study. Circulation. 2004; 109: 837-842.
7. Daniels LB et al. Lipoprotein-associated phospholipase A2 is an independent predictor of incident coronary heart disease in an apparently healthy older population: The Rancho Bernardo Study. J Am Coll Cardiol. 2008; 51: 913-919.
8. Ballantyne CM et al. Lipoprotein-associated phospholipase A2, high sensitivity Creactive protein, and risk for incident ischemic stroke in middle-aged men and women in the Atherosclerosis Risk in Communities (ARIC) study. Arch Intern Med. 2005; 165: 24792484.
9. Gorelick PB. Lipoprotein-associated phospholipase A2 and risk of stroke. Am J Cardiol. 2008; 101 (suppl): 34F-40F.
10. Wassertheil-Smoller S et al. Lipoprotein-associated phospholipase A2, hormone use, and the risk of ischemic stroke in postmenopausal women. Hypertension. 2008; 51: 11151122.
11. Davidson MH et al. Efficacy and tolerability of adding prescription omega-3 fatty acids 4 g/d to simvastatin 40 mg/d in hypertriglyceridemic patients: An 8-week, randomized, double-blind, placebocontrolled study. Clin Ther. 2007; 39: 1354-1367.
DRAFT, NOT FOR PUBLICATION 35
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
12. Toyama K et al. Rosuvastatin combined with regular exercise preserves coenzyme Q10 levels associated with a significant increase in high-density lipoprotein cholesterol in patients with coronary artery disease. Atherosclerosis. 2011; 217: 158-164.
13. Lösche W et al. Lipoprotein-associated phospholipase A2 and plasma lipids in patients with destructive periodontal disease. J Clin Periodontol. 2005; 32: 640-644.
DRAFT, NOT FOR PUBLICATION 36
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Myeloperoxidase (MPO)
MPO is a white blood cell-derived inflammatory enzyme and measures disease activity from the luminal aspect of the arterial wall. pHi LLC analyzes and measures the presence of MPO to evaluate a person’s risk of developing cardiovascular risk. (Cleveland HeartLab, Myeloperoxidase (MPO), 2015)
Briefly, when the artery wall is damaged, or inflamed, MPO is released by invading macrophages where it accumulates. MPO mediates the vascular inflammation that propagates plaque formation and activates protease cascades that are linked to plaque vulnerability. White blood cell activation in the bloodstream, in response to luminal injury of the artery wall including fissures, erosions or a degrading collagen cap, leads to MPO release in the bloodstream. This combination of detrimental effects demonstrates that MPO is actively involved in the progression of atherosclerosis. The Cleveland HeartLab MPO test measures free MPO in the bloodstream. (ibid) (Penn, M. S., et al, 2015)
Clinical Use
The MPO test may be performed on individuals at intermediate or high risk for developing coronary heart disease who are any age with at least two major risk factors, those ≥65 years of age with one major risk factor, smokers, those with a fasting blood glucose of ≥100 mg/dL, or those who have metabolic syndrome. (ibid)
Gateway to myeloperoxidase evidence base:
1. Tavora F et al. Monocytes and neutrophils expressing myeloperoxidase occur in fibrous caps and thrombi in unstable coronary plaques. BMC Cardiovascular Disord. 2009; 9: 2733.
2. Hazen SL and Heinecke JW. 3-chlorotyrosine, a specific marker of myeloperoxidasecatalyzed oxidation, is markedly elevated in low density lipoprotein isolated from human atherosclerotic intima. J Clin Invest. 1997; 99: 2075-2081.
3. Fu X et al. Hypochlorous acid oxygenates the cysteine switch domain of pro-matrilysin (MMP-7). A mechanism for matrix metalloproteinase activation and atherosclerotic plaque rupture by myeloperoxidase. J Biol Chem. 2001; 276: 41279-41287.
4. Meuwese MC et al. Serum myeloperoxidase levels are associated with the future risk of coronary artery disease in apparently healthy individuals: The EPIC-Norfolk Prospective Population Study. J Am Coll Cardiol. 2007; 50: 159-165.
5. Karakas M et al. Myeloperoxidase is associated with incident coronary heart disease independently of traditional risk factors: Results from the MONICA/KORA Augsburg study. J Intern Med. 2012; 271: 43-50.

DRAFT, NOT FOR PUBLICATION 37
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
6. Baldus S et al. Myeloperoxidase serum levels predict risk in patients with acute coronary syndromes. Circulation. 2003; 108: 1440-1445.
7. Cavusoglu E et al. Usefulness of baseline plasma myeloperoxidase levels as an independent predictor of myocardial infarction at two years in patients presenting with acute coronary syndrome. Am J Cardiol. 2007; 99: 1364-1368.
8. Heslop CL et al. Myeloperoxidase and C-reactive protein have combined utility for longterm prediction of cardiovascular mortality after coronary angiography. J Am Coll Cardiol. 2010; 55: 1102-1109.
9. Buhlin K et al. Periodontitis is associated with angiographically verified coronary artery disease. J Clin Periodontol. 2011; 38: 1107-1014.
10. Toyama K et al. Rosuvastatin combined with regular exercise preserves coenzyme Q10 levels associated with a significant increase in high-density lipoprotein cholesterol in patients with coronary artery disease. Atherosclerosis. 2011; 217: 158-164.
11. Maradit-Kremers H et al. Increased unrecognized coronary heart disease and sudden deaths in rheumatoid arthritis: A population-based cohort study. Arthritis Rheum. 2005; 52: 402-211.
12. Melanson SE et al. Elevation of myeloperoxidase in conjunction with cardiac-specific markers after marathon running. Am J Clin Pathol. 2006; 126: 888-893.
DRAFT, NOT FOR PUBLICATION 38
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
DISCUSSION
Current science places employers in the awkward position of choosing to go beyond the current standard of care to help prevent costly and deadly disease in their workforces…of helping employees recognize the advent of coming health problems and of helping them to prevent it. (Mattke S, et al, 2013)
Arterial plaque and inflammation, metabolic syndrome, insulin resistance can be measured cost-effectively, however. More importantly: that they can be prevented is beyond dispute.
Why is prevention science not yet widely practiced under the current standard of care? (ibid) If the established science and clinical results are so compelling, why are providers not adopting the science, the methods?
Our answer to these questions: first, we are sensing an encouraging but minor, very minor, shift in the national conversation about prevention vs. treatment. There are positive signs of development but, without question, the entire U.S. healthcare system is still firmly rooted in treating disease when it presents itself in a patient, rather than trying to present the disease.
Second, the cause, in our view: prevention is not yet a curriculum cornerstone in medical schools, in nursing programs, etc. We continue to produce physicians, nurses, specialists, etc. who are obsessively focused on treatment rather than prevention. That treatment is generally considered by many to be the best on earth…but why keep perpetuating the need and demand for that treatment when the proven solution is easily available?
Corporate leadership is thus presented with several questions, starting with: “Is prevention more costly – in lives and money -- than the treatment and care of an employee’s diabetes, heart disease, heart attack or stroke? Is prevention more costly than “disease management?” (ibid)
Is not the purpose of corporate wellness programs to save lives and to save money? (Berry, Leonard L., et al, 2010) (PWC/PriceWaterhouseCoopers LLC, 2014)

DRAFT, NOT FOR PUBLICATION 39
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
QUESTIONS FOR CORPORATE WELLNESS COMMITTEES AND PROFESSIONALS:
Over the past 12-36 months, by what percentage have we reduced our employees’ claims for heart disease/attacks, strokes, and diabetes?
I am told that more than 500 specific ICD-9 and CPT codes are related to heart disease/attacks, stroke, and diabetes. Are employee claims against those codes moving downward?
Are we measuring our effectiveness in preventing those events and diseases?
Are we screening our employees for the presence of disease or the presence of risk of disease?
Are we applying advanced blood tests and inflammation testing to diagnose risk of heart attack and stroke -- tests recognized in the scientific and medical literature as offering the highest predictive ability available for those events?
Are we applying the following tests to diagnose risk of heart attack, stroke, and diabetes: Small Dense LDL, ApoB, ApoA1, Lp(a), hsCRP, LpPLA2, and Myeloperoxidase?
Do we fully understand the science-link between these diagnostic tests and the presence of CAD, CVD, insulin resistance, atherosclerosis, and metabolic syndrome – and the link to employee claims for treating these conditions?
How do we apply the latest science to uncover and diagnose risk of arterial disease? In our basic labs regimen, do we look for the presence of arterial plaque, inflammation? Metabolic syndrome? If so, how do we do that?
For example, what is our cutpoint for measuring our employees’ glucose levels?
How often and for which employees do we apply a carotid intima media thickness ultrasound to measure the presence of plaque in our employees’ arteries? Does our provider understand the link between the cIMT test and insulin resistance?”
DRAFT, NOT FOR PUBLICATION 40
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
CONCLUSIONS
The scientific foundation to pHi LLC’s protocol is well-documented. Diagnosing risk is the common-sense and logical first step to preventing diabetes, stroke, heart disease, and heart attacks. (Fries, James F.; Koop, C. Everett; et al, 1993)
Early detection of arterial plaque and inflammation, metabolic syndrome, and insulin resistance is essential to prevention. (Bradley Bale & Amy Doneen, 2014) The methodologies and diagnostic protocols applied by pHi LLC are efficacious.
In our view, employers need a reliable, science-based disease-prevention protocol to help their employees live longer, healthier lives. Such a protocol does not appear to currently exist among the portfolio of most corporate wellness providers’ services. (Mattke S, et al, 2013) (PWC (PriceWaterhouseCoopers LLP), 2011) (PWC/PriceWaterhouseCoopers LLC, 2014) (Berry, Leonard L., et al, 2010)
Employers intent on helping their employees prevent deadly disease should consider shifting the procurement model with wellness providers from “wellness” to “health” – that is, to evidence-based methods for actually preventing the need and demand for “disease management.” (Berry, Leonard L., et al, 2010) (Fries, James F.; Koop, C. Everett; et al, 1993)
Furthermore, self-insured employers18 should consider measuring wellness-campaigns outcomes and results using quantitative metrics, e.g. a reduction in employee claims against specific ICD-9 and CPT codes related to diabetes, stroke, heart disease, and heart attacks. The costs of disease treatment and care are a built-in metric and easy to track.
Indeed, “health” is one of the most easily measurable cost centers for any employer; the metric can be used to analyze corporate financial health, and it affects every balance sheet.
When quantitative metrics are applied, “health” becomes an objective, accurate, measureable insight into any workforce, as well as a reliable predictor of that workforce’s future availability and its “disease management” costs.
18 For smaller, non‐self‐insured employers, our experience is that obtaining data regarding spends against specific ICD‐9 and CPT codes from their insurers is difficult.

DRAFT, NOT FOR PUBLICATION 41
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Bibliography Adam D. Gepner, et al. (2006, September). Use of Carotid Intima‐Media Thickness and Vascular Age to
Modify Cardiovascular Risk Prediction. Journal of the American Society of Echocardiography,
19(9), 1170‐1174. Retrieved from http://www.onlinejase.com/article/S0894‐7317(06)00392‐
0/abstract
Allan, Paul L., et al. (1997). Relationship Between Carotid Intima‐Media Thickness and Symptomatic and
Asymptomatic Peripheral Arterial Disease: The Edinburgh Artery Study. Stroke, 28, 348‐353.
American Heart Association. (2015, Feb. 2). Atheroslecrosis. Retrieved from American Heart Association,
"Conditions":
http://www.heart.org/HEARTORG/Conditions/Cholesterol/WhyCholesterolMatters/Atheroscler
osis_UCM_305564_Article.jsp
Belcaro, G. et al. (2001, June). Carotid and femoral ultrasound morphology screening and cardiovascular
events in low risk subjects: a 10‐year follow‐up study (the CAFES‐CAVE study. Atherosclerosis,
156(2), 379‐87.
Berry, Leonard L., et al. (2010, December). What’s the Hard Return on Employee Wellness Programs?
Harvard Business Review. Retrieved from https://hbr.org/2010/12/whats‐the‐hard‐return‐on‐
employee‐wellness‐programs
Bradley Bale, M., & Amy Doneen, A. (2014). Beat the Heart Attack Gene. New York: Wiley General
Trade/Turner Publishing Company.
Cedars‐Sinai Heart Institute. (2015, May 12). Carotid Intima‐Media Thickness Test. Retrieved from
Carotid Intima‐Media Thickness Test (CIMT): http://www.cedars‐sinai.edu/Patients/Programs‐
and‐Services/Heart‐Institute/Centers‐and‐Programs/SHAPE‐Center/Carotid‐Intima‐Media‐
Thickness‐Test‐CIMT.aspx
Cleveland Heart Lab, Lp‐PLA2. (2015, Feb 3). Lp‐PLA2 (The PLAC® Test). Retrieved from Cleveland
HeartLab: http://www.clevelandheartlab.com/wp‐content/uploads/2013/10/Lp‐PLA2‐
Practitioner‐OnePager‐CHL‐D010b.pdf
Cleveland Heart Lab, sd‐LDL. (2014, September 4). sd‐LDL. Retrieved from Cleveland Heart Lab:
http://www.clevelandheartlab.com/tests/sd‐ldl/
Cleveland HeartLab, hsCRP. (2015, January 14). High Sensitivity C‐Reactive Protein (hsCRP). Retrieved
from Cleveland HeartLab: http://www.clevelandheartlab.com/wp‐
content/uploads/2013/10/hsCRP‐Practitioner‐OnePager‐CHL‐D009b.pdf
Cleveland HeartLab, Myeloperoxidase (MPO). (2015, January 14). Myeloperoxidase (MPO). Retrieved
from Myeloperoxidase (MPO): http://www.clevelandheartlab.com/wp‐
content/uploads/2014/11/MPO‐Practitioner‐One‐Pager‐CHL‐D006c.pdf
Cleveland HeartLab, Our Science. (2015, April 22). Cleveland HeartLab, Our Science. Retrieved from
Cleveland HeartLab: Cleveland HeartLab, Our Science
DRAFT, NOT FOR PUBLICATION 42
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
pHi LLC, M. (2015, February 4). Overview of pHi LLC's services...physician‐to‐patient view. (KC,
Interviewer)
Diabetes Prevention Program Research Group. (2001). Reduction in the Incidence of Type 2 Diabetes
with Lifestyle Intervention or Metformin. New England Journal of Medicine, 346, 393‐403.
Diabetes Prevention Program Research Group. (2002). Reduction in the Incidence of Type 2 Diabetes
with Lifestyle Intervention or Metformin. New England Journal of Medicine, 346, 393‐403.
Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1282458/
Farley, TA; et al. (2010). Deaths preventable in the U.S. by improvements in use of clinical preventive
services. American Journal of Preventive Medicine, 38, 600‐609.
Ford ES, et al. (2007). Explaining the decrease in U.S. deaths from coronary disease, 1980‐2000. New
England Journal of Medicine, 356, 2388‐2398.
Frieden, Thomas R., et al. (2011). The “Million Hearts” Initiative — Preventing Heart Attacks and Strokes.
New England Journal of Medicine, 365, e27.
Fries, James F.; Koop, C. Everett; et al. (1993, July 29). Reducing Health Care Costs by Reducing the Need
and Demand for Medical Services. New England Journal of Medicine, 329, 321‐325. Retrieved
from http://www.nejm.org/doi/full/10.1056/NEJM199307293290506
Funke, H., et al. (1991, January). A frameshift mutation in the human apolipoprotein A‐I gene causes
high density lipoprotein deficiency, partial lecithin: cholesterol‐acyltransferase deficiency, and
corneal opacities. Journal of Clinical Investigation, 87(1), 371–376. Retrieved from
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC295069/
Gene 388, National Center for Biotechnology Information, U.S. National Library of Medicine, National
Institutes of Health. . (2015, April 27). Apolipoprotein B, Gene 388. Retrieved from National
Center for Biotechnology Information, U.S. National Library of Medicine, National Institutes of
Health. : http://www.ncbi.nlm.nih.gov/gene/338
Goldstein, Larry B. , et al. (2011). Guidelines for the Primary Prevention of Stroke: A Guideline for
Healthcare Professionals From the American Heart Association/American Stroke Association.
Stroke, 42, 517‐584. Retrieved from http://stroke.ahajournals.org/content/42/2/517.full
Heart Health Special Report. (2008, October 1). Apo B ‐‐ A Better Marker for Heart Attack Risk Than LDL
Cholesterol? Scientific American. Retrieved from
http://www.healthafter50.com/reports/heart_health/135‐1.html
Heidenreich, Paul A. MD; et al. (2011). Forecasting the Future of Cardiovascular Disease in the United
States: A Policy Statement From the American Heart Association. Circulation, 123, 933‐944.
Howard, B. et al. (2002). Prevention Conference VI Diabetes and Cardiovascular Disease. Circulation,
105, e132‐e137.
DRAFT, NOT FOR PUBLICATION 43
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Jia Q.; et al. (2012, March). Abnormal glucose regulation in patients with acute stroke across China:
prevalence and baseline patient characteristics. Stroke, 43(3), 650‐7. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/22267822
JUPITER Study Group. (2008). Rosuvastatin to Prevent Vascular Events in Men and Women with Elevated
C‐Reactive Protein. New England Journal of Medicine, 359, 2195‐2207.
Kasliwal, Ravi R., et al. (2014, Jan‐Feb). Carotid intima–media thickness: Current evidence, practices, and
Indian experience. Indian Journal of Endocrinology and Metabolism, 18(1), 13–22. Retrieved
from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3968727/
Lamarche, B., et al. (1999, September). The small, dense LDL phenotype and the risk of coronary heart
disease; epidemilogy, patho‐physiology and therapeutic aspects. Diabetes Metabolism 1999
Sep;25(3):199‐211., 25(3), 199‐211. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/10499189
Lamarche, Benoit; et al. (1997). Small, Dense Low‐Density Lipoprotein Particles as a Predictor of the Risk
of Ischemic Heart Disease in Men. Circulation, 95, pp. 69‐75. Retrieved from
http://circ.ahajournals.org/content/95/1/69.long
Marcus, Adam & Oransky, Ivan. (2015, May 22). "What's Behind Big Science Frauds?". The New York
Times, p. A19. Retrieved from http://www.nytimes.com/2015/05/23/opinion/whats‐behind‐big‐
science‐frauds.html?ribbon‐ad‐
idx=4&rref=world&mwrsm=Email&_r=0&module=ArrowsNav&contentCollection=Opinion&acti
on=swipe®ion=FixedRight&pgtype=article
Martin, BC; et al. (1992). Role of glucose and insulin resistance in development of type 2 diabetes
mellitus: results of a 25 year follow‐up study. (1992, Ed.) Lancet, 340, 925‐929.
Martin, Seth S., et al. (2009). Apolipoprotein B but not LDL Cholesterol Is Associated With Coronary
Artery Calcification in Type 2 Diabetic Whites. Diabetes, 58(8), 1887‐1892. Retrieved from
http://diabetes.diabetesjournals.org/content/58/8/1887.full.pdf+html
Mattke S, et al. (2013). Workplace Wellness Programs Study. RAND Corporation. Retrieved from
http://www.rand.org/content/dam/rand/pubs/research_reports/RR200/RR254/RAND_RR254.p
df
Meschia, J., et al. (2014). Guidelines for the Primary Prevention of Stroke. Stroke 2014; 45:1‐79. Stroke,
45, 1‐79.
Moore LLVAJ; et al. (2000). Can sustained weight loss in overweight individuals reduce the risk of
diabetes mellitus? Epidemiology, 11, 269–273.
Naghavi, M., et al. (2006, July 17). From vulnerable plaque to vulnerable patient‐‐Part III: Executive
summary of the Screening for Heart Attack Prevention and Education (SHAPE) Task Force report.
American Journal of Cardiology, 98(2A), 2H‐15H.
DRAFT, NOT FOR PUBLICATION 44
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
National Center for Biotechnology Information, U.S. National Library of Medicine. (2015, January 14).
APOA1 apolipoprotein A‐I. Retrieved from National Center for Biotechnology Information, U.S.
National Library of Medicine: http://www.ncbi.nlm.nih.gov/gene/335
Nelson, TL, et al. (2012, May). Lipoprotein‐associated phospholipase A2 (Lp‐PLA2) and future risk of type
2 diabetes: results from the Cardiovascular Health Study. Journal of Clinical Endcrinology &
Metabolism, 97(5), 1695‐701.
Nigro, J., et al. (2006). Insulin Resistance and Atherosclerosis. Endocrine Reviews, 27, 242‐259.
O’Donnell, M.,et al. (2010). Risk Factors for Ischaemic and Intracerebral Haemorrhagic Stroke in 22
Countries (the INTERSTROKE study): a Case Control Study. Lancet, 376, 112‐123.
Ordovas, J M; et al. (1989, October 5). Familial apolipoprotein A‐I, C‐III, and A‐IV deficiency and
premature atherosclerosis due to deletion of a gene complex on chromosome 11. The Journal of
Biological Chemistry, 264, 16339‐16342. Retrieved from
http://www.jbc.org/content/264/28/16339.short
Packard, Chris, et al. (2000, June 30). The role of small, dense low density lipoprotein (LDL): a new look.
International Journal of Cardiology, 74(Supplement 1), S17‐S22. Retrieved from
http://www.internationaljournalofcardiology.com/article/S0167‐5273(99)00107‐2/abstract
Penn, M. S., et al. (2015, April 1). Journal of Medical Economics , 1, 109. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/25763924
PWC (PriceWaterhouseCoopers LLP). (2011). Health and Well‐Being Touchstone Survey Results May
2011. PriceWaterhouseCoopers LLP. Retrieved from http://www.pwc.com/en_US/us/hr‐
management/assets/PwC_2011_Health_and_Wellbeing_Touchstone_Survey_Results.pdf
PWC/PriceWaterhouseCoopers LLC. (2014). 2014 Health and Well‐being Touchstone Survey. Retrieved
from http://www.pwc.com/en_US/us/hr‐management/publications/assets/pwc‐touchstone‐
survey‐results‐june‐2014.pdf
Ridker, P. (2001). "High‐Sensitivity C‐Reactive Protein Potential Adjunct for Global Risk Assessment in
the Primary Prevention of Cardiovascular Disease". Circulation, 1813‐1818.
Ridker, P. (2001). Potential Adjunct for Global Risk Assessment in the Primary Prevention of
Cardiovascular Disease. Circulation, 103, 1813‐1818. Retrieved November 11, 2012
Ridker, Paul M, M.D., et al. (2008, November 20). Rosuvastatin to Prevent Vascular Events in Men and
Women with Elevated C‐Reactive Protein. New England Journal of Medicine, 359, 2195‐2207.
Ross, R. (1999). Atherosclerosis—An Inflammatory Disease. New England Journal of Medicine, 340, 115‐
126.
Serruys PW, et al. (2008). Effects of the direct lipoprotein‐associated phospholipase A2 inhibitor
darapladib on human coronary atherosclerotic plaque. Circulation., 118, 1172‐1182. Retrieved
from Serruys PW et al. (2008). Circulation. 2008; 118: 1172‐1182.
DRAFT, NOT FOR PUBLICATION 45
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Seshasai, S., et al. (2011). Diabetes Mellitus, Fasting Glucose, and Risk of Cause‐Specific Death. New
England Journal of Medicine, 364, 829‐841.
Sesso, H. et al. (2012). "Multivitamins in the Prevention of Cardiovascular Disease in MenThe Physicians'
Health Study II Randomized Controlled Trial". Journal of the American Medical Association.
Shah, P. (2010). The SHAPE Paradigm: A Commentary. Circulation: Cardiovascular Quality and Outcomes,
3, 106‐109.
Smith SC Jr, et al. (2000, January 4). Prevention Conference V: Beyond secondary prevention: identifying
the high‐risk patient for primary prevention: tests for silent and inducible ischemia: Writing
Group II. Circulation, 101(1), E12‐6.
Stein, James H., et al. (2004, July). Vascular age: Integrating carotid intima‐media thickness
measurements with global coronary risk assessment. Cardiology, 27(7), 388‐392. Retrieved April
19, 2015, from http://onlinelibrary.wiley.com/doi/10.1002/clc.4960270704/abstract
Stein, James H., et al. (2008, February). “Use of Carotid Ultrasound to Identify Subclinical Vascular
Disease and Evaluate Cardiovascular Disease Risk: A Consensus Statement from the American
Society of Echocardiography Carotid Intima‐Media Thickness Thickness Task Force. Journal of
the American Society of Echocardiography, 21(2), 93‐111.
The Society of Atherosclerosis Imaging and Prevention. (2010). Appropriate use criteria for carotid
intima media thickness testing. Atherosclerosis. Retrieved from https://www.vasolabs.com/wp‐
content/uploads/2013/10/SAIP‐Appropriate‐Use‐Criteria.CIMT_.Atherosclerosis‐2010.pdf
U.S. Centers for Disease Control and Prevention. (2014). National Diabetes Statistics Report. Centers for
Disease Control and Prevention.
U.S. Centers for Disease Control and Prevention. (2014). National Diabetes Statistics Report: Estimates of
Diabetes and Its Burden in the United States, 2014. Atlanta, GA:: U.S. Department of Health and
Human Services. Retrieved from http://www.cdc.gov/diabetes/pubs/statsreport14/national‐
diabetes‐report‐web.pdf
University of Rochester Medical Center. (2008, March 13). Study in Circulation Research Details How
Diabetes Drives Atherosclerosis; Mechanisms Suggest New Way to Treat Heart Disease Among
Diabetics. Retrieved from University of Rochester Medical Center:
http://www.urmc.rochester.edu/news/story/index.cfm?id=1922
Wackers FJ, et al. (2004, August). Detection of silent myocardial ischemia in asymptomatic diabetic
subjects: the DIAD study. Diabetes Care, 27(8), 1954‐61.
Walldius, Göran MD, et al. (2001, December 15). High apolipoprotein B, low apolipoprotein A‐I, and
improvement in the prediction of fatal myocardial infarction (AMORIS study): a prospective
study. The Lancet, pp. 2026–2033. Retrieved from
http://www.thelancet.com/pdfs/journals/lancet/PIIS0140‐6736(01)07098‐2.pdf
DRAFT, NOT FOR PUBLICATION 46
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Ward, R. Parker, et al. (2008). Use of Carotid Intima‐Media Thickness to Identify Patients With Ischemic
Stroke and Transient Ischemic Attack With Low Yield of Cardiovascular Sources of Embolus on
Transesophageal Echocardiography. Stroke, 39, 2969‐2974. Retrieved from
http://stroke.ahajournals.org/content/39/11/2969.full
Whelton PK; et al. (1998). Sodium reduction and weight loss in the treatment of hypertensionin older
persons: a randomized controlled trial of nonpharmacologic interventions in the elderly (TONE).
Journal of the American Medical Association, 279, 839–846.
Woo, Chang‐Hoon; et al. (2008). Extracellular Signal‐Regulated Kinase 5 SUMOylation Antagonizes Shear
Stress–Induced Antiinflammatory Response and Endothelial Nitric Oxide Synthase Expression in
Endothelial Cells. Circulation Research, 102, 538‐545.
Yoon, Paula W.; et al. (2014). Potentially Preventable Deaths from the Five Leading Causes of Death”.
U.S. Centers for Disease Control and Prevention, Morbidity and Mortality Weekly Report, CDC
2014;63(17);369‐374. Atlanta, GA: U.S. Department of Health and Human Services. Retrieved
from http://www.cdc.gov/mmwr/pdf/wk/mm6317.pdf
DRAFT, NOT FOR PUBLICATION 47
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
SUPPLEMENTAL BIBLIOGRAPHY

DRAFT, NOT FOR PUBLICATION 48
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Inflammation and Atherosclerosis
Ross R and Glomset JA. The pathogenesis of atherosclerosis (First of two parts). N Engl J Med. 1976; 295: 369-377.
Ross R and Glomset JA. The pathogenesis of atherosclerosis (Second of two parts).N Engl J Med. 1976; 295: 420-425.
Ross R. Atherosclerosis-An inflammatory disease. N Engl J Med. 1999; 340: 115-126.
Finn AV et al. Concept of vulnerable/unstable plaque. Arterioscler Thromb Vasc Biol. 2010; 30: 1282-1292.
Penn MS and Klemes AB. Multimarker approach for identifying and documenting mitigation of cardiovascular risk. Future Cardiol. 2013; 9: 497-506
Ikonomidis I et al. Multimarker approach in cardiovascular risk prediction. Dis Markers. 2009; 26: 273-285.
Libby P et al. Inflammation in atherosclerosis: From pathophysiology to practice. J Am Coll Cardiol. 2009; 54: 2129-2138.
Myeloperoxidase
Karakas M et al. Myeloperoxidase is associated with incident coronary heart disease independently of traditional risk factors: Results from the MONICA/KORA Augsburg study. J Intern Med. 2012; 271:43-50. Abstract
Ndrepepa G et al. Impact of therapy with statins, beta-blockers and angiotensinconverting enzyme inhibitors on plasma myeloperoxidase in patients with coronary artery disease. Clin Res Cardiol. 2011; 100: 327-333. Abstract
Tang WHW et al. Plasma myeloperoxidase predicts incident cardiovascular risks in stable patients undergoing medical management for coronary artery disease. Clin Chem. 2011; 57: 33-39. Abstract
Oemrawsingh RM et al. Multimarker risk model containing troponin-T, interleukin 10, myeloperoxidase and placental growth factor predicts long-term cardiovascular risk after non-ST-segment elevation acute coronary syndrome. Heart. 2011. Epub ahead of print. Abstract
Roman et al. Prognostic value of myeloperoxidase in coronary artery disease: Comparison of unstable and stable angina patients. Coron Artery Dis. 2010; 21: 129136. Abstract
Heslop et al. Myeloperoxidase and C-reactive protein have combined utility for long-term prediction of cardiovascular mortality after coronary angiography. J Am Coll Cardiol. 2010; 55: 1102-1109. Abstract

DRAFT, NOT FOR PUBLICATION 49
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Wong et al. Myeloperoxidase, subclinical atherosclerosis, and cardiovascular disease events. J Am Coll Cardiol Img. 2009; 2: 1093-1099. Abstract
Tang et al. Usefulness of myeloperoxidase levels in healthy elderly subjects to predict risk of developing heart failure. Am J Cardiol. 2009; 103: 1269-1274. Abstract
Ndrepepa et al. Myeloperoxidase level in patients with stable coronary artery disease and acute coronary syndromes. Eur J Clin Invest. 2008; 38: 90-96. Abstract
Morrow et al. Concurrent evaluation of novel cardiac biomarkers in acute coronary syndrome: Myeloperoxidase and soluble CD40 ligand and the risk of recurrent ischaemic events in TACTICS-TIMI 18. Eur Heart J. 2008; 29: 1096-1102. Abstract
Brevetti et al. Myeloperoxidase, but not C-reactive protein, predicts cardiovascular risk in peripheral arterial disease. Eur Hear J. 2008; 29: 224-230. Abstract
Mocatta et al. Plasma concentrations of myeloperoxidase predict mortality after myocardial infarction. J Am Coll Cardiol. 2007; 49: 1993-2000. Abstract
Tang WHW et al. Prognostic value and echocardiographic determinants of plasma myeloperoxidase levels in chronic heart failure. J Am Coll Cardiol. 2007; 49: 2364-2370.
Cavusoglu E et al. Usefulness of baseline plasma myeloperoxidase levels as an independent predictor of myocardial infarction at two years in patients presenting with acute coronary syndrome. Am J Cardiol. 2007; 99: 1364-1368.
Meuwese et al. Serum myeloperoxidase levels are associated with the future risk of coronary artery disease in apparently healthy individuals: the EPIC-Norfolk Prospective Population Study. J Am Coll Cardiol. 2007; 50: 159-165. Abstract
Exner M et al. Myeloperoxidase predicts progression of carotid stenosis in states of low high-density lipoprotein cholesterol. J Am Coll Cardiol. 2006; 47: 2212-2218.
Vita et al. Serum myeloperoxidase levels independently predict endothelial dysfunction in humans. Circulation. 2004; 110: 1134-1139. Abstract
Baldus S. et al. Myeloperoxidase serum levels predict risk in patients with acute coronary syndromes. Circulation. 2003; 108: 1440-1445.
Brennan M-L et al. Prognostic value of myeloperoxidase in patients with chest pain. N Engl J Med. 2003; 349:1595-1604.
Zhang R et al. Association between myeloperoxidase levels and risk of coronary artery disease. JAMA. 2001;286:2136-2142.
High-sensitivity C-reactive Protein
DRAFT, NOT FOR PUBLICATION 50
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Ridker PM et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. 2008; 359: 2195-2207.
Ndrepepa G et al. N-terminal pro-brain natriuretic peptide and C-reactive protein in stable coronary heart disease. Am J Med. 2006; 119: 355.e1-355.e8.
Nissen SE et al. Statin therapy, LDL cholesterol, C-reactive protein, and coronary artery disease. N Engl J Med. 2005; 352: 29-38.
Ridker PM et al. C-reactive protein levels and outcomes after statin therapy. N Engl J Med. 2005; 352: 20-28.
Ridker PM. et al. Comparison of C-reactive protein and low-density lipoprotein cholesterol levels in the prediction of first cardiovascular events. N Engl J Med.2002; 347: 1557-1565.
Rost NS et al. Plasma concentration of C-reactive protein and risk of ischemic stroke and transient ischemic attack: The Framingham study. Stroke. 2001; 32: 2575-2579.
Ridker PM et al. Inflammation, aspirin, and the risk of cardiovascular disease in apparently healthy men. N Engl J Med. 1997; 336: 973-979.
Review criteria for assessment of C-reactive protein (CRP), high sensitivity C-reactive protein (hsCRP), and cardiac C-reactive protein (cCRP) assays. Sept. 22, 2005. U.S. Department of Health and Human Services.
LDL
Bays HE et al. Chitin-glucan fiber effects on oxidized low-density lipoprotein: A randomized controlled trial. Eur J Clin Nutr. epub ahead of print 5 September 2012.
Rao VS et al. Association of inflammatory and oxidative stress markers with metabolic syndrome in Asian Indians in India. Cardiol Res Pract. 2010 Dec 28;2011:295976.
Holvoet P et al. Association between circulating oxidized low-density lipoprotein and incidence of the metabolic syndrome. JAMA. 2008; 299: 2287-2293.
Meisinger C et al. Plasma oxidized low-density lipoprotein, a strong predictor for acute coronary heart disease events in apparently healthy, middle-aged men from the general population. Circulation. 2005; 112: 651-657.
Tsimikas S et al. Oxidized phospholipids, Lp(a) lipoprotein, and coronary artery disease. N Engl J Med. 2005; 353: 46-57.
Nishi K et al. Oxidized LDL in carotid plaques and plasma associates with plaque instability. Aterioscler Thromb Vasc Biol. 2002; 22: 1649-1654.
DRAFT, NOT FOR PUBLICATION 51
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Holvoet P et al. Circulating oxidized LDL is a useful marker for identifying patients with coronary artery disease. Arterioscler Thromb Vasc Biol. 2001; 21: 844-848.
Ehara S et al. Elevated levels of oxidized low density lipoprotein show a positive relationship with the severity of acute coronary syndromes. Circulation. 2001; 103: 19551960.
Lp-PLA2
Reddy KJ et al. Lipoprotein-associated phospholipase A2 mass is significantly reduced in dyslipidemic patients treated with lifestyle modification and combination lipid-modifying drug therapy. Prev Cardiol. 2010; 13: 130-134.
Daniels LB et al. Lipoprotein-associated phospholipase A2 is an independent predictor of incident coronary heart disease in an apparently healthy older population: The Rancho Bernardo Study. J Am Coll Cardiol. 2008; 51: 913-919.
Gorelick PB. Lipoprotein-associated phospholipase A2 and risk of stroke. Am J Cardiol. 2008; 101 (suppl): 34F-40F.
Wassertheil-Smoller S et al. Lipoprotein-associated phospholipase A2, hormone use, and the risk of ischemic stroke in postmenopausal women. Hypertension. 2008; 51: 11151122.
Kolodgie FD et al. Lipoprotein-associated phospholipase A2 protein expression in the natural progression of human coronary atherosclerosis. Arterioscler Thromb Vasc Biol. 2006; 26: 2523- 2529.
Ballantyne CM et al. Lipoprotein-associated phospholipase A2, high sensitivity C-reactive protein, and risk for incident ischemic stroke in middle-aged men and women in the Atherosclerosis Risk in Communities (ARIC) study. Arch Intern Med.2005; 165: 24792484.
Ballantyne CM et al. Lipoprotein-associated phospholipase A2, high-sensitivity C-reactive protein, and risk for incident coronary heart disease in middle-aged men and women in the Atherosclerosis Risk in Communities (ARIC) study. Circulation.2004; 109: 837-842.
Ferguson JF et al. Translational studies of lipoprotein-associated phospholipase A(2) in inflammation and atherosclerosis. J Am Coll Cardio. 2012; 59: 764-772.
Gonçalves I et al. Evidence supporting a key role of Lp-PLA2-generated lysophosphatidylcholine in human atherosclerotic plaque inflammation. Arterioscler Thromb Vasc Biol. 2012; 32: 1505-1512.

DRAFT, NOT FOR PUBLICATION 52
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Serruys PW et al. Effects of the direct lipoprotein-associated phospholipase A2inhibitor darapladib on human coronary atherosclerotic plaque. Circulation. 2008; 118: 1172-1182.
Lösche W et al. Lipoprotein-associated phospholipase A2 and plasma lipids in patients with destructive periodontal disease. J Clin Periodontol. 2005; 32: 640-644.
Davidson MH et al. Efficacy and tolerability of adding prescription omega-3 fatty acids 4 g/d to simvastatin 40 mg/d in hypertriglyceridemic patients: An 8-week, randomized, double-blind, placebo-controlled study. Clin Ther. 2007; 39: 1354-1367.
Small Dense LDL (sdLDL)
Rosensen RS et al. Relations of lipoprotein subclass levels and low-density lipoprotein size to progression of coronary artery disease in the Pravastatin Limitation of Atherosclerosis in the Coronary Arteries (PLAC-I) trial. Am J Cardiol.2002; 90: 89-94.
Koba S et al. Significance of small dense low-density lipoproteins and other risk factors in patients with various types of coronary heart disease. Am Heart J. 2002; 144: 10261035.
St-Pierre AC et al. Comparison of various electrophoretic characteristics of LDL particles and their relationship to the risk of ischemic heart disease. Circulation.2001; 104: 22952299.
Chapman MJ et al. Atherogenic, dense low-density lipoproteins. Pathophysiology and new therapeutic approaches. Eur Heart J. 1998; 19 Suppl A: A24-30.
Grundy SM. Hypertriglyceridemia, atherogenic dyslipidemia, and the metabolic syndrome. Am J Cardiol. 1998; 81: 18B-25B.
Austin MA et al. Atherogenic lipoprotein phenotype. A proposed genetic marker for coronary heart disease risk. Circulation. 1990; 82: 495-506.
Lipoprotein(a)
Kamstrup PR et al. Genetically elevated lipoprotein(a) and increased risk of myocardial infarction. JAMA. 2009; 301: 2331-2339.
Kolodgie FD et al. Lipoprotein-associated phospholipase A2 protein expression in the natural progression of human coronary atherosclerosis. Arterioscler Thromb Vase Biol. 2006; 26: 2523-2529.
Anuurad E et al. Lipoprotein(a): A unique risk factor for cardiovascular disease. Clin Lab Med. 2006; 26: 751-772.
Berglund L et al. Lipoprotein(a): An elusive cardiovascular risk factor. Arterioscler Thromb Vasc Biol. 2004; 24: 2219-2226.
DRAFT, NOT FOR PUBLICATION 53
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Boffa MB et al. Lipoprotein(a) as a risk factor for atherosclerosis and thrombosis: Mechanistic insights from animal models. Clin Biochem. 2004; 37: 333-343.
Mackinnon LT et al. Effects of physical activity and diet on lipoprotein(a). Med Sci Sports Exerc. 1997; 29: 1429-1436.
Bostom AG et al. Elevated plasma lipoprotein(a) and coronary heart disease in men age 55 years and younger. A prospective study. JAMA. 1996; 276: 544-548.
Routi T et al. Correlation of toddlers’ serum lipoprotein(a) concentrations with parental values and grandparents’ coronary heart disease: The STRIP baby study. Acta Paediatr. 1996; 85: 407-412.
Jurgens G et al. Lipoprotein(a) serum concentration and apolipoprotein(a) phenotype correlate with severity and presence of ischemic cerebrovascular disease. Stroke. 1995; 26: 1841-1848.
Apolipoprotein A-I (ApoA1)
Bishop ML, Fody EP, Schoeff LE. Clinical chemistry, techniques, principles, correlations (7th edition). Philadelphia, PA, Lippincott Williams & Wilkins, 2013.
Mudd JO, Borlaug BA, Johnston PV, et al. Beyond low-density lipoprotein cholesterol: defining the role of low-density lipoprotein heterogeneity in coronary artery disease. J Am Coll Cardiol. 2007 30;50(18):1735-1741.
van Deventer HE, Miller WG, Myers GL, et al. Non-HDL cholesterol shows improved accuracy for cardiovascular risk score classification compared to direct or calculated LDL cholesterol in a dyslipidemic population. Clin Chem. 2011;57(3):490-501.
Nauck M, Warnick GR, Rifai N. Methods for measurement of LDL-cholesterol: a critical assessment of direct measurement by homogeneous assays versus calculation. Clin Chem. 2002;48(2):236-254.
Brunzell JD, Davidson M, Furberg CD, Goldberg RB, Howard BV, Stein JH, Witztum JL. American Diabetes Association; American College of Cardiology Foundation. Lipoprotein management in patients with cardiometabolic risk: consensus statement from the American Diabetes Association and the American College of Cardiology Foundation. Diabetes Care. 2008;31(4):811-822.
Blaha MJ, Blumenthal RS, Brinton EA, Jacobson TA. National Lipid Association Taskforce on Non-HDL Cholesterol. The importance of non-HDL cholesterol reporting in lipid management. J Clin Lipidol. 2008;2(4):267-273.
Walldius G, Jungner I, Holme I, Aastveit AH, Kolar W, Steiner E. High apolipoprotein B, low apolipoprotein A-I, and improvement in the prediction of fatal myocardial infarction (AMORIS study): a prospective study. Lancet. 2001;358 (9298):2026-2033.
DRAFT, NOT FOR PUBLICATION 54
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Saenger A. Cardiovascular Risk Assessment Beyond LDL Cholesterol: Non-HDL Cholesterol, LDL, Particle Number, and Apolipoprotein B. http://www.mayomedicallaboratories.com/articles/communique/2011/11.html.Accessed November 26, 2013.
Sniderman AD, Scantlebury T, Cianflone K. Hypertriglyceridemic hyperapob: the unappreciated atherogenic dyslipoproteinemia in type 2 diabetes mellitus. Ann Intern Med. 2001;18;135(6):447-459.
Craig WY, Neveux LM, Palomaki GE, Cleveland MM, Haddow JE. Lipoprotein(a) as a risk factor for ischemic heart disease: metaanalysis of prospective studies. Clin Chem. 1998;44(11):2301-2306.
Carmena R, Duriez P, Fruchart JC. Atherogenic lipoprotein particles in atherosclerosis. Circulation. 2004;109(23 Suppl 1):III2-1117.
Bachorik PS, Ross JW. National Cholesterol Education Program recommendations for measurement of low-density lipoprotein cholesterol: executive summary. The National Cholesterol Education Program Working Group on Lipoprotein Measurement. Clin Chem. 1995;41(10):1414-1420.
Viles-Gonzalez JF, Fuster V, Corti R, Badimon JJ. Emerging importance of HDL cholesterol in developing high-risk coronary plaques in acute coronary syndromes. Curr Opin Cardiol. 2003;18(4):286-294.
Morgan J, Carey C, Lincoff A, Capuzzi D. High-density lipoprotein subfractions and risk of coronary artery disease. Curr Atheroscler Rep. 2004;6(5):359-365.
Hodis HN. Triglyceride-rich lipoprotein remnant particles and risk of atherosclerosis. Circulation. 1999; 99(22):2852-2854.
Olofsson SO, Borèn J. Apolipoprotein B: A clinically important apolipoprotein which assembles atherogenic lipoproteins and promotes the development of atherosclerosis. J Intern Med. 2005;258(5):395-410.
Chapman MJ, Ginsberg HN, Amarenco P, et al. European Atherosclerosis Society Consensus Panel. Triglyceride-rich lipoproteins and high-density lipoprotein cholesterol in patients at high risk of cardiovascular disease: evidence and guidance for management. Eur Heart J. 2011;32(11):1345-1361.
Cullen P. Evidence that triglycerides are an independent coronary heart disease risk factor. Am J Cardiol. 2000;86(9):943-949.
Fujioka Y, Ishikawa Y. Remnant lipoproteins as strong key particles to atherogenesis. J Atheroscler Thromb. 2009;16 (3):145-154.
DRAFT, NOT FOR PUBLICATION 55
© 2015 Predictive Health Intelligence LLC. All rights reserved. Medical Disclaimer: This
information is not intended to substitute for the advice of a physician.
Jellinger PS, Dickey RA, Ganda OP, et al. AACE Lipid Guidelines Committee. AACE medical guidelines for clinical practice for the diagnosis and treatment of dyslipidemia and prevention of atherogenesis. Endocr Pract. 2000;6(2):162-213.
Grundy SM, Cleeman JI, Merz CN, et al. National Heart, Lung, and Blood Institute; American College of Cardiology Foundation; American Heart Association. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. Circulation. 2004;110(2):227-239.
Atherotech Diagnostics Lab. The VAP Lipid Panel. http://www.atherotech.com/VapCholTest/default.asp. Accessed November 26, 2013.
Kulkarni KR. Cholesterol profile measurement by vertical auto profile method. Clin Lab Med. 2006; 26(4):787-802.
ATP III At-A-Glance: Quick Desk Reference. National Heart, Lung, and Blood Institute. http://www.nhlbi.nih.gov/guidelines/cholesterol/atglance.html. Accessed November 11, 2013.
Analytical performance of the cholesterol profile measurement by Vertical Auto Profile [VAP]: analysis of NCEP III guidelines lipid analytes. http://www.atherotech.com/images/vapliterature/pdfs/vapaccuracywhitepaper_2011083 1.pdf. Accessed November 26, 2013.
Ton VK, Martin SS, Blumenthal RS, Blaha MJ. Comparing the new European cardiovascular disease prevention guideline with prior American Heart Association guidelines: an editorial review. Clin Cardiol. 2013;36(5):E1-6.