2015 spring iga news
TRANSCRIPT

Patron Dame Maggie Smith
IGA NEWSSpring 2015
Normal Vision
Mild Glaucoma
Advanced Glaucoma

CEO Report Page 1Open Patient Meeting Page 3Public Awareness Page 15Drug Update Page 16Michael Banes Page 17DVLA Page 18Words from Sightline Page 19Fond Farewell Page 20Research Recruitment Page 21Becky’s Blog Page 23Support Groups Page 24
INTERNATIONAL GLAUCOMA ASSOCIATIONWoodcote House,15 Highpoint Business VillageHenwood, Ashford, Kent TN24 8DH
Sightline: 01233 64 81 70Administration: 01233 64 81 64Fax: 01233 64 81 79Email: [email protected]: www.glaucoma-association.comEditor-in-chief: Russell YoungWriter and deputy editor: Karen BrewerSub-editor: Tracey FabreDesign/artwork: Yes DesignPrinted by: Fuller Davies Ltd
Charity registered in England & Wales No. 274681, in Scotland No. SC041550Cover image ‘Driving with Glaucoma’ © IGA 2015
C O N T E N T S

Once again this has been a very busystart to the year and I am delightedto report we now have our first twogroups of volunteers ‘on the road’.
One group is based in Scotland andthe other in the South East. I havebeen referring to them as our ‘TrailBlazers’ as the IGA has never usedvolunteers in its 40 year history. Sowe are on a very steep learningcurve. This will be a very interestingpilot study to ensure everything is inplace to support teams. We arelooking forward to learning fromeach other on what can and cannotbe achieved.
Their initial priorities will be to tryand expand the use of our freepatient information literature,principally in the primary care
setting such as GP practices,community pharmacies and highstreet opticians. However there are numerous other sites that couldbe approached including seniorcitizen luncheon clubs, care homesand libraries.
Whilst we have been having goodsuccess in setting up glaucomapatient support groups, there isnothing like a direct question to anophthalmologist from one of theirown patients asking why there is no support group in the local area, as recommended by the NICEQuality Standards, to gain that initial stimulus on which one of our Development Managers could follow up.
In addition, we are hoping thevolunteers may be able to placecollecting boxes in appropriate sitesto help raise funds for futureresearch and also assist theDevelopment Managers when theyhave a large meeting organised as an extra pair of hands would helpthe event run smoothly.
We continue to develop a verypositive relationship with the DVLAwho have recently supplied us withsome interesting statistics suggestingup to 60% of the identified glaucomapatients holding a driving licence inthe UK have not declared their
1News Spring 2015
CEO Report

News Spring 2015
condition to the DVLA. This is veryworrying as it is illegal to continuedriving under the Road Traffic Act of1979 unless the DVLA has beeninformed. In addition there is apotential fine of up to £1000 and apossible criminal conviction shouldthe non-reporting patient driver beidentified. Perhaps even moreworrying is the implication on thevalidity of the driver’s motorinsurance should they be involved in an accident.
A number of members have beengood enough to report theirexperience of having the DVLAEsterman test under the newSpecSavers DVLA contract where, intheir opinion, the quality standardshave not been achieved and we arefeeding this information back to thesenior management at the DVLA. Weanticipate, and hope to be able tofollow this up with a face to facemeeting mid-year, when we will alsowish to raise a number of otherissues you have highlighted over thelast few months. Any furtherfeedback, both good andquestionable, on this subject would be gratefully received.
I am delighted to report we havenow finished our negotiations andsigned the contract to expand our
office space which will improve theworking conditions for our valuableand committed staff and allow us todispose of our warehouse, where westore all the patient informationliterature and support materials,which should be a cost-effectivemove. Tracy Dorman, our GeneralManager, is now working hard toarrange the necessary infrastructureto be put in place ready for there-organisation, besides doing herday job!
Russell YoungChief Executive
2
CEO Report

Good afternoon everyone, it’s very nice to be here and thank you all forcoming to the Scottish meeting ofthe International GlaucomaAssociation. For those of you whodon’t know me, my name is AndrewTatham, and I am a consultantglaucoma surgeon here in Edinburgh,at the Princess Alexandra EyePavilion. The topic I wish to covertoday is what’s new in the treatment of glaucoma.
Although glaucoma affects about oneper cent of those aged over fortyand four per cent of those aged over80 years, about 50 per cent ofpeople who have glaucoma actuallyaren’t aware that they are affectedand have not been diagnosed. That’s ahuge problem, because althoughglaucoma is one of the mostcommon causes of irreversibleblindness, if we pick it up early thereare effective treatments that canprevent loss of vision. It is thereforevery important for us to raiseawareness of glaucoma among thegeneral population and encourage
people to attend their optometristregularly, so that it can be detectedat an earlier stage. So, what’s new inglaucoma?
Lamina CribrosaFirst, we are beginning to understandmore about what causes glaucoma.This structure, the Lamina Cribrosa,which looks like a little sponge, is
very important (slide 1). Glaucoma isdamage to the optic nerve, (slide 2)which is a cable, made of one millionindividual fibres, that sends visualmessages from the eye to the brain.
3News Spring 2015
Open Patient Meeting - Edinburgh -
What’s new in the treatment of glaucoma
Andrew Tatham MBChB FRCOphth FRCSEd FEBOConsultant Eye Surgeon, Princess Alexandra Eye Pavilion, Edinburgh
Slide 1

As the optic nerve leaves the eye onits journey to the brain, it passesthrough the sieve-like openings inthe Lamina Cribrosa. The optic nerveis vulnerable to damage as it passesthrough the Lamina Cribrosa, and itis here that the nerve fibres arethought to be damaged in glaucoma.When we look at a photograph ofthe optic nerve, we can sometimesactually see the small pores, theopenings in the Lamina Cribrosa.These are the openings throughwhich the nerve fibres pass as theyexit the eye and travel towards the brain.
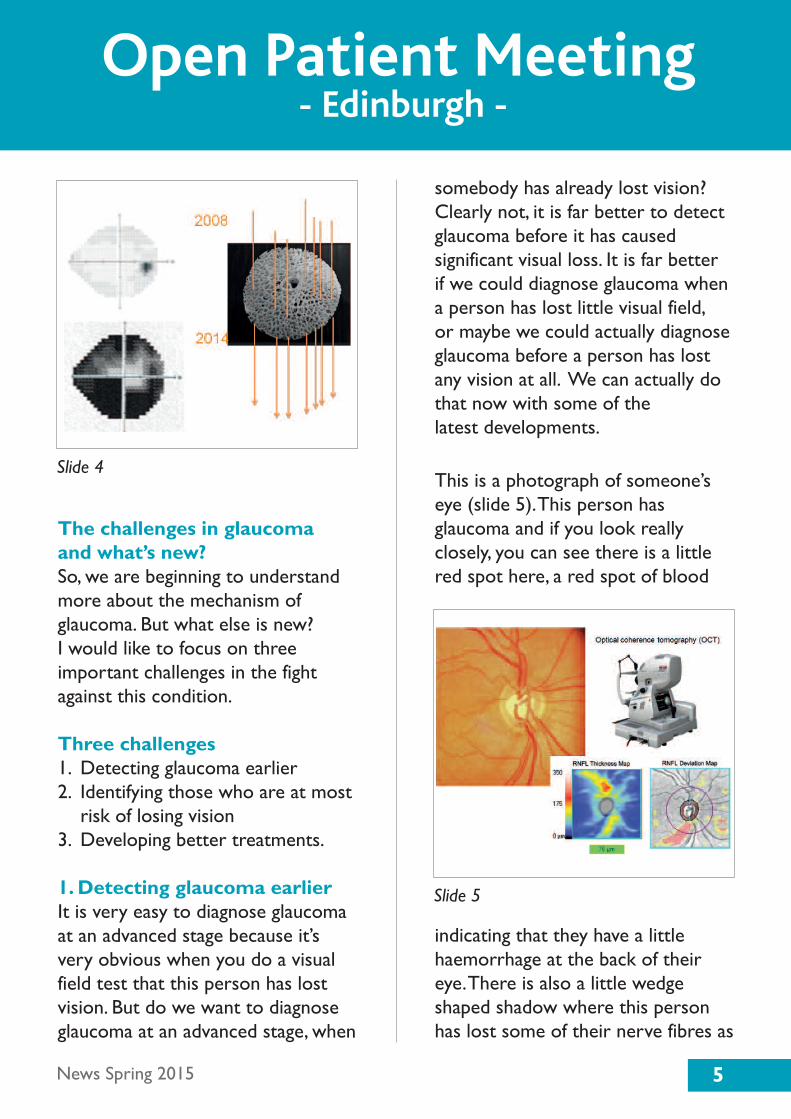
Glaucoma and nerve damageTo give an example of how glaucomamay affect a patient, here is a pictureof someone’s optic nerve in 2008(slide 3). Over time this person losestheir optic nerve fibres one by one.Everyone starts with about a millionnerve fibres and there is a natural
ageing of the nerve, but in glaucomathat process of nerve loss isaccelerated. With this particularpatient, the nerve changesappearance over the next six years,as the optic nerve fibres are lost. Wecan see the result of this for thisperson’s vision. In 2008, when she
was first seen, the visual field testwas normal (slide 4), but by 2014 shehas lost a large amount of vision, asoptic nerve fibres had been lost. Sothis person has progressed veryquickly. Using new imaging deviceswe can now see the Lamina Cribrosain greater detail, so for the first timewe can see the location where opticnerve damage occurs in glaucoma.This has the potential to help usbetter understand the mechanism ofnerve damage.
4 News Spring 2015
Open Patient Meeting - Edinburgh -
Slide 2
Slide 3
The challenges in glaucoma and what’s new?So, we are beginning to understandmore about the mechanism ofglaucoma. But what else is new? I would like to focus on threeimportant challenges in the fightagainst this condition.
Three challenges 1. Detecting glaucoma earlier2. Identifying those who are at most
risk of losing vision 3. Developing better treatments.
1. Detecting glaucoma earlierIt is very easy to diagnose glaucomaat an advanced stage because it’svery obvious when you do a visualfield test that this person has lostvision. But do we want to diagnoseglaucoma at an advanced stage, when
somebody has already lost vision?Clearly not, it is far better to detectglaucoma before it has causedsignificant visual loss. It is far better if we could diagnose glaucoma whena person has lost little visual field, or maybe we could actually diagnoseglaucoma before a person has lostany vision at all. We can actually dothat now with some of the latest developments.
This is a photograph of someone’seye (slide 5). This person hasglaucoma and if you look reallyclosely, you can see there is a littlered spot here, a red spot of blood
indicating that they have a littlehaemorrhage at the back of theireye. There is also a little wedgeshaped shadow where this personhas lost some of their nerve fibres as
5News Spring 2015
Open Patient Meeting - Edinburgh -
Slide 4
Slide 5
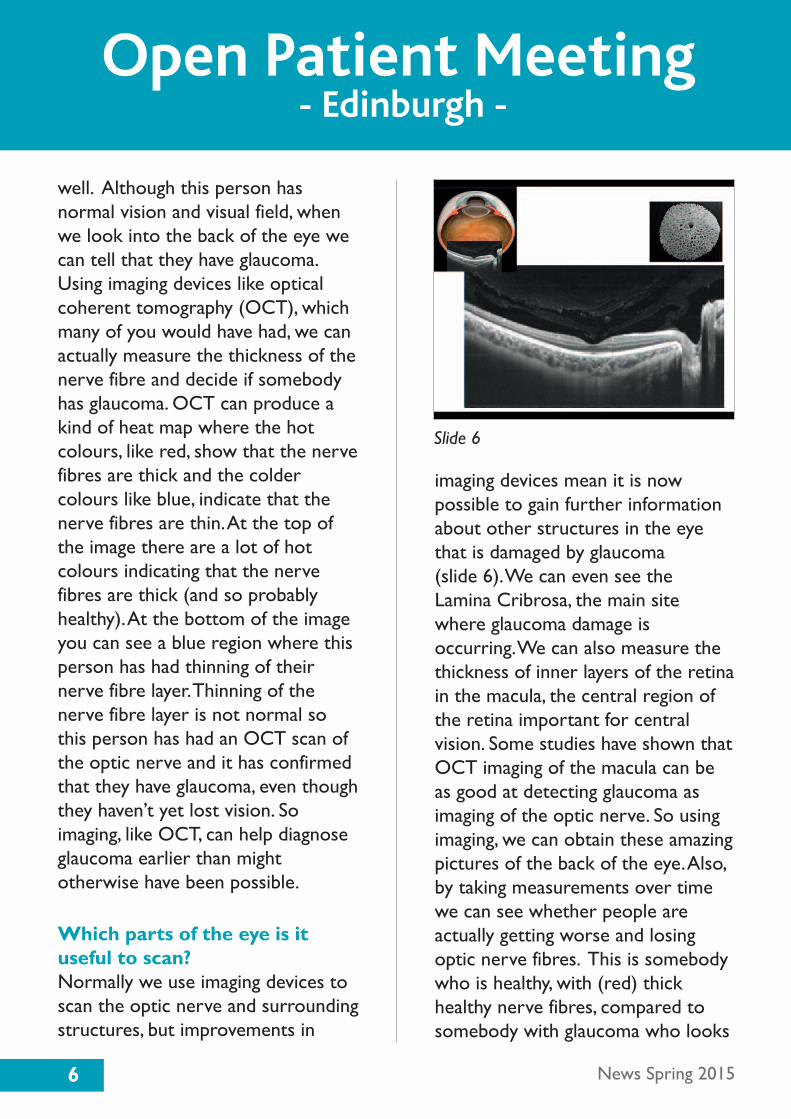
well. Although this person hasnormal vision and visual field, whenwe look into the back of the eye wecan tell that they have glaucoma.Using imaging devices like opticalcoherent tomography (OCT), whichmany of you would have had, we canactually measure the thickness of thenerve fibre and decide if somebodyhas glaucoma. OCT can produce akind of heat map where the hotcolours, like red, show that the nervefibres are thick and the coldercolours like blue, indicate that thenerve fibres are thin. At the top ofthe image there are a lot of hotcolours indicating that the nervefibres are thick (and so probablyhealthy). At the bottom of the imageyou can see a blue region where thisperson has had thinning of theirnerve fibre layer. Thinning of thenerve fibre layer is not normal sothis person has had an OCT scan ofthe optic nerve and it has confirmedthat they have glaucoma, even thoughthey haven’t yet lost vision. Soimaging, like OCT, can help diagnoseglaucoma earlier than mightotherwise have been possible.
Which parts of the eye is ituseful to scan? Normally we use imaging devices toscan the optic nerve and surroundingstructures, but improvements in
imaging devices mean it is nowpossible to gain further informationabout other structures in the eyethat is damaged by glaucoma (slide 6). We can even see the Lamina Cribrosa, the main site where glaucoma damage isoccurring. We can also measure thethickness of inner layers of the retinain the macula, the central region ofthe retina important for centralvision. Some studies have shown thatOCT imaging of the macula can beas good at detecting glaucoma asimaging of the optic nerve. So usingimaging, we can obtain these amazingpictures of the back of the eye. Also,by taking measurements over timewe can see whether people areactually getting worse and losingoptic nerve fibres. This is somebodywho is healthy, with (red) thickhealthy nerve fibres, compared tosomebody with glaucoma who looks
6 News Spring 2015
Open Patient Meeting - Edinburgh -
Slide 6
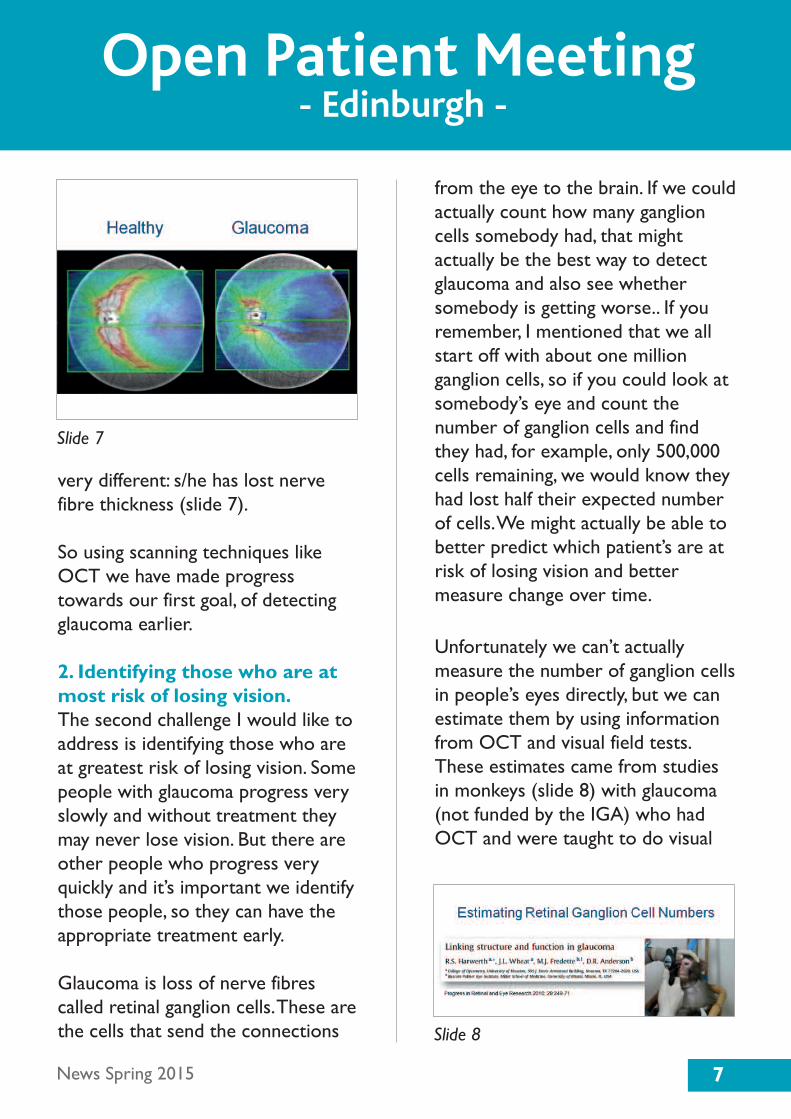
very different: s/he has lost nervefibre thickness (slide 7).
So using scanning techniques likeOCT we have made progresstowards our first goal, of detectingglaucoma earlier.
2. Identifying those who are atmost risk of losing vision. The second challenge I would like toaddress is identifying those who areat greatest risk of losing vision. Somepeople with glaucoma progress veryslowly and without treatment theymay never lose vision. But there areother people who progress veryquickly and it’s important we identifythose people, so they can have theappropriate treatment early.
Glaucoma is loss of nerve fibrescalled retinal ganglion cells. These arethe cells that send the connections
from the eye to the brain. If we couldactually count how many ganglioncells somebody had, that mightactually be the best way to detectglaucoma and also see whethersomebody is getting worse.. If youremember, I mentioned that we allstart off with about one millionganglion cells, so if you could look atsomebody’s eye and count thenumber of ganglion cells and findthey had, for example, only 500,000cells remaining, we would know theyhad lost half their expected numberof cells. We might actually be able tobetter predict which patient’s are atrisk of losing vision and bettermeasure change over time.
Unfortunately we can’t actuallymeasure the number of ganglion cellsin people’s eyes directly, but we canestimate them by using informationfrom OCT and visual field tests.These estimates came from studiesin monkeys (slide 8) with glaucoma(not funded by the IGA) who hadOCT and were taught to do visual
News Spring 2015
Open Patient Meeting - Edinburgh -
Slide 7
Slide 8
7
field tests. We all know visual fieldtests are difficult but the monkeysactually did the visual field testsbetter than some people can! I thinkthe researchers bribed the monkeyswith bananas! Anyway, the number ofretinal ganglion cells was countedindividually for each monkey andrelated to the OCT and visual fieldfindings. These formulae are notperfect but it is possible to estimatethe number of ganglion cells in aneye from OCT and how well they dothe field test.
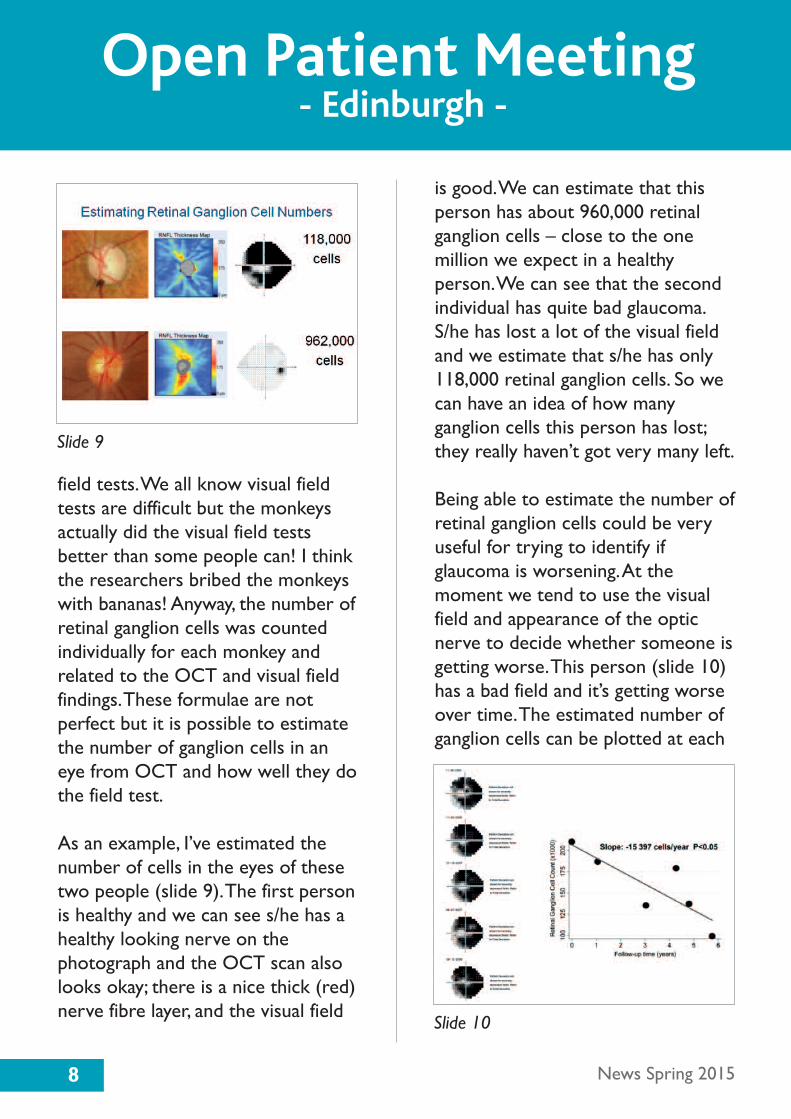
As an example, I’ve estimated thenumber of cells in the eyes of thesetwo people (slide 9). The first personis healthy and we can see s/he has ahealthy looking nerve on thephotograph and the OCT scan alsolooks okay; there is a nice thick (red)nerve fibre layer, and the visual field
is good. We can estimate that thisperson has about 960,000 retinalganglion cells – close to the onemillion we expect in a healthyperson. We can see that the secondindividual has quite bad glaucoma.S/he has lost a lot of the visual fieldand we estimate that s/he has only118,000 retinal ganglion cells. So wecan have an idea of how manyganglion cells this person has lost;they really haven’t got very many left.
Being able to estimate the number ofretinal ganglion cells could be veryuseful for trying to identify ifglaucoma is worsening. At themoment we tend to use the visualfield and appearance of the opticnerve to decide whether someone isgetting worse. This person (slide 10)has a bad field and it’s getting worseover time. The estimated number ofganglion cells can be plotted at each
8 News Spring 2015
Open Patient Meeting - Edinburgh -
Slide 9
Slide 10

visit, so we can gauge how quicklythe glaucoma is changing over time. Ifwe know this person’s age we couldextend the plot to predict how manyretinal ganglion cells might be leftshould they live to, for example, 100
years of age. Are they still going to beseeing okay at this age?
We can use visual field alone to lookfor progression, however, considerthis next person. Would we say thisperson is getting worse? (slide11)Probably not, because their visualfield has not really changed but aswe’ve said, some people can actuallyhave large changes to the optic nervewithout losing visual field. You canprobably appreciate the difference inthe appearance of this person’s opticnerve over time. The nerve haschanged and if we estimate howmany retinal ganglion cells this
person has lost it comes toapproximately 50,000 cells per year.So this person is losing a largenumber of optic nerve fibres, eventhough the tests of vision remainnormal. This might not be a problemin an elderly person, but in a youngperson this rate of ganglion cell losscould well result in loss of visionlater in life. This illustrates why it isimportant to use measurements ofoptic nerve structure, as well asvisual field tests, in monitoringglaucoma. We can then better decideif somebody needs extra treatmentor lower eye pressure.
Tasks of daily livingWhat matters most to you? It isprobably not how many retinalganglion cells you have, or even howwell you do on visual field tests.What matters most is likely to bethe ability to live life fully, the abilityto take part in activities importantfor day-to-day life, activities likeshopping or driving. Unfortunatelywe don’t know very much abouthow the results of tests like visualfield actually relate to ability toperform important daily tasks. This is an important area for research,and several groups have been tryingto investigate and answer thisimportant question.
9News Spring 2015
Open Patient Meeting - Edinburgh -
Slide 11

Recently I have been involved in astudy to examine the effect ofglaucoma on driving. Loss of a drivinglicence is something that worriesmany people, and although driverswith glaucoma have been shown tobe at increased risk of accidents,many people with glaucoma are likelyto be very safe drivers. It isimportant to better understand therelationship between conventionaltests of vision, like visual field, andthe ability to drive and detectpotential hazards when driving.Recently, in conjunction withUniversity of California in San Diego,USA, we have been looking at this,using a driving simulator. The drivingsimulator tests how well drivers candivide their vision between taskswhen driving. This is different tovisual field testing which tries tominimise distractions.
During the driving task, the driverwas asked to follow a car in the roadand at the same time, detect a smalltarget out in the periphery. Thedriver was asked to press a buttonon the steering wheel when thetarget appeared and we measuredthe reaction time to this target. Thiswas repeated several times as thedriver continued to follow the car.We found that by combininginformation from visual fields and
OCT we were better able to predictdrivers with problems on simulateddriving. In the future, we might beable to relate rates of change invisual field or OCT to changes in theability to perform daily tasks likedriving. If we are also able toestimate numbers of retinal ganglioncells, we might even be able to seethat somebody is losing a certainnumber of retinal ganglion cells peryear, and because of this, identify thatthis person is at risk of losing theirdriving licence. We might be able tothen recommend that this patientconsider extra treatment or anoperation to slow down the rate ofganglion cell loss and prevent theloss of their driving licence. Furtherstudies that investigate therelationship between commonmeasures of glaucoma severity andthe ability to perform importantdaily tasks, will mean we have muchbetter information to make theseimportant decisions abouttreatment.
Intraocular pressureWe know that intraocular pressureis important in glaucoma, but we alsoknow that many people have “normalpressure”, or a pressure not above21 mmHg. Population based studieshave shown that up to about 50 percent of people with glaucoma have
10 News Spring 2015
Open Patient Meeting - Edinburgh -

“normal pressures” but there aregeographic variations and in Japan 90per cent of people with glaucomahave normal pressures. The termnormal pressure glaucoma is a littlecontroversial, due partly to the factthat we are really bad at measuringpressure and many people may infact have higher pressure at othertimes. A single pressure-reading islike a snapshot, like taking one framefrom an entire movie. We’re justseeing what the pressure is like atone second in time. In contrast,glaucoma is a 24 hour condition andso really we need to be able tomeasure pressure over 24 hours.
One way this can be done is in sleeplabs. There are actually laboratorieswhere patients can spend acomfortable night, sleeping in thelaboratory, only to be woken upevery hour to have their intraocular
pressure checked. About two-thirdsof people have their peak pressureduring the night. Recently I saw apatient whose pressure was onlyabout 15mmHg during the day, and ifyou remember a normal pressure isabout 10 to 21 mmHg, but when thepressure was measured in the sleeplab, it actually went up to 30mmHgduring the night. So there may bepeople who appear to have normalpressure, who actually don’t havenormal pressure at all. Despite thissome people do have low pressureall the time and their optic nerve isjust very sensitive and vulnerable todamage. The pressure might benormal for other people, but forthem it is too high.
Another way to measure the effectsof eye pressure over 24 hours isusing this contact lens sensor (slide 12). This contact lens can befitted by the doctor and then wornat home for 24 hours. The lens has atiny pressure sensor that sendsinformation wirelessly to a deviceworn on the waist. After 24 hoursthe patient needs to come back tothe clinic to have the lens removedand the stored data can bedownloaded by the doctor. The lensdoes not measure intraocularpressure directly but insteadmeasures the changes in the shape of
11News Spring 2015
Open Patient Meeting - Edinburgh -
Slide 12
the cornea that are believed tooccur as a result of changes in eyepressure. Although more work needsto be done to see how thesechanges relate to eye pressure, andwhether fluctuations in pressureactually increase the risk ofglaucoma, these sorts ofdevelopments could help us betterunderstand glaucoma.
3. Developing bettertreatments.What is the ideal glaucomatreatment? Perhaps the ideal wouldbe something you need to use onlyonce, or at least less often than thecurrent treatments. Definitelysomething that has few side effects;something that doesn’t irritate theeyes or make them red or make theeyelashes grow longer. And probablysomething that doesn’t involveputting any drops in your eye at all;you could just throw the drops away.What about something that couldprotect the nerve and re-grow thenerve: something that might actuallyimprove vision? We are still a longway from being able to improvedamage from glaucoma, but there issome progress being made toimprove current treatments anddevelop new ones.
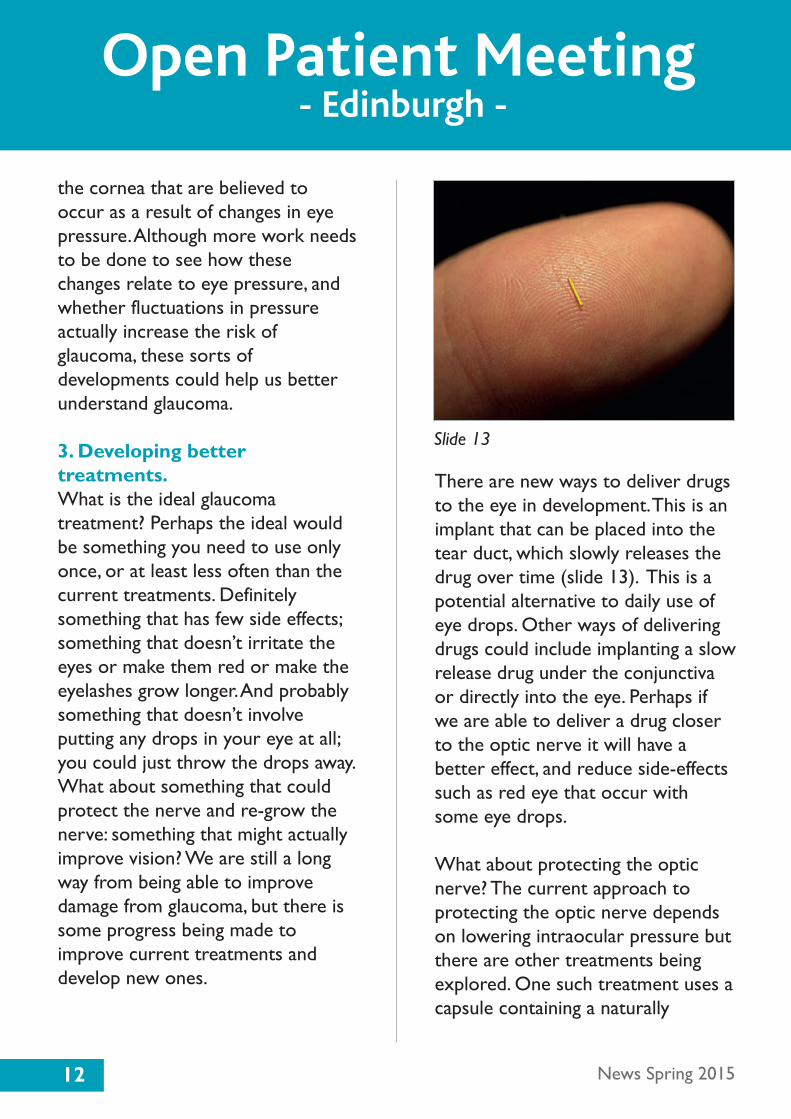
There are new ways to deliver drugsto the eye in development. This is animplant that can be placed into thetear duct, which slowly releases thedrug over time (slide 13). This is apotential alternative to daily use ofeye drops. Other ways of deliveringdrugs could include implanting a slowrelease drug under the conjunctivaor directly into the eye. Perhaps ifwe are able to deliver a drug closerto the optic nerve it will have abetter effect, and reduce side-effectssuch as red eye that occur withsome eye drops.
What about protecting the opticnerve? The current approach toprotecting the optic nerve dependson lowering intraocular pressure butthere are other treatments beingexplored. One such treatment uses acapsule containing a naturally
12 News Spring 2015
Open Patient Meeting - Edinburgh -
Slide 13
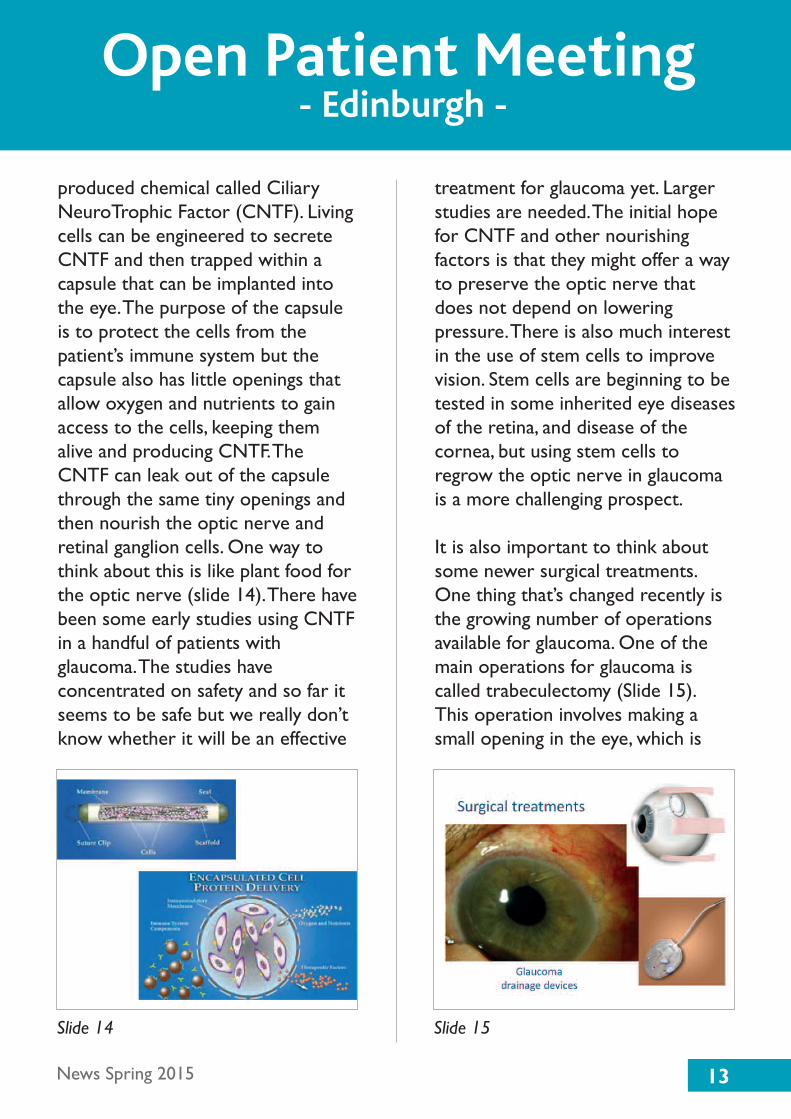
produced chemical called CiliaryNeuroTrophic Factor (CNTF). Livingcells can be engineered to secreteCNTF and then trapped within acapsule that can be implanted intothe eye. The purpose of the capsuleis to protect the cells from thepatient’s immune system but thecapsule also has little openings thatallow oxygen and nutrients to gainaccess to the cells, keeping themalive and producing CNTF. TheCNTF can leak out of the capsulethrough the same tiny openings andthen nourish the optic nerve andretinal ganglion cells. One way tothink about this is like plant food forthe optic nerve (slide 14). There havebeen some early studies using CNTFin a handful of patients withglaucoma. The studies haveconcentrated on safety and so far itseems to be safe but we really don’tknow whether it will be an effective
treatment for glaucoma yet. Largerstudies are needed. The initial hopefor CNTF and other nourishingfactors is that they might offer a wayto preserve the optic nerve thatdoes not depend on loweringpressure. There is also much interestin the use of stem cells to improvevision. Stem cells are beginning to betested in some inherited eye diseasesof the retina, and disease of thecornea, but using stem cells toregrow the optic nerve in glaucomais a more challenging prospect.
It is also important to think aboutsome newer surgical treatments.One thing that’s changed recently isthe growing number of operationsavailable for glaucoma. One of themain operations for glaucoma iscalled trabeculectomy (Slide 15). This operation involves making asmall opening in the eye, which is
13News Spring 2015
Open Patient Meeting - Edinburgh -
Slide 14 Slide 15
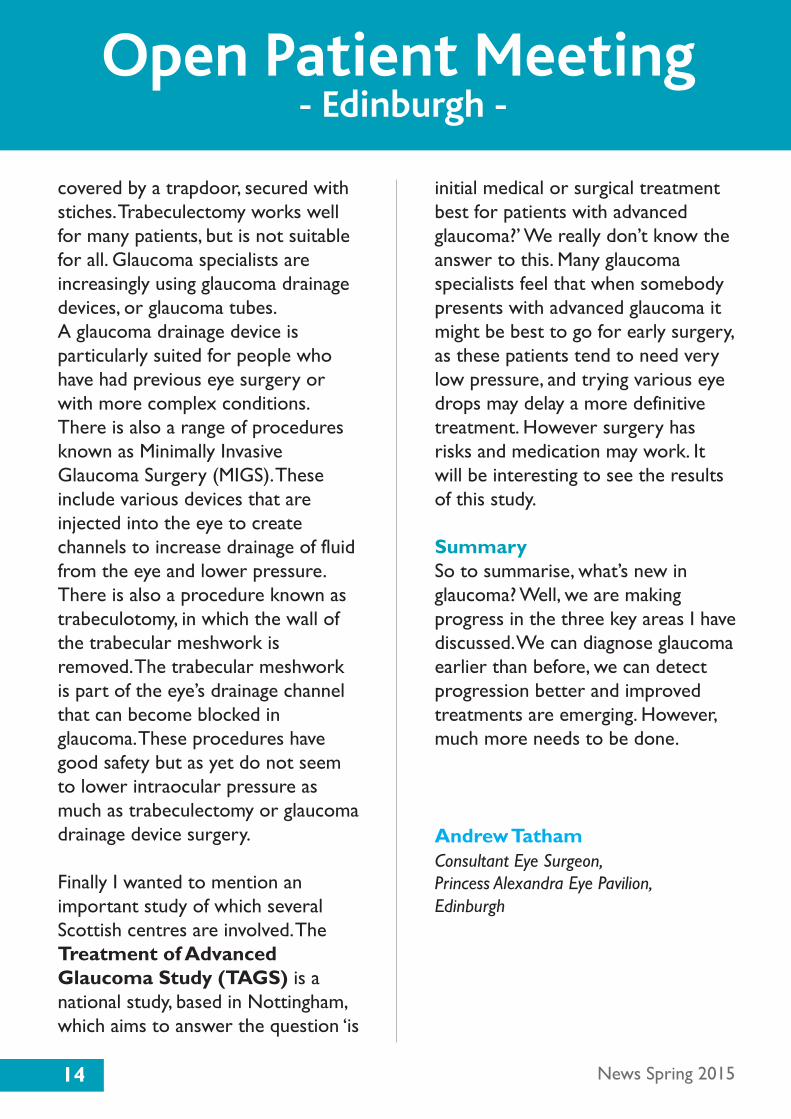
covered by a trapdoor, secured withstiches. Trabeculectomy works wellfor many patients, but is not suitablefor all. Glaucoma specialists areincreasingly using glaucoma drainagedevices, or glaucoma tubes. A glaucoma drainage device isparticularly suited for people whohave had previous eye surgery orwith more complex conditions.There is also a range of proceduresknown as Minimally InvasiveGlaucoma Surgery (MIGS). Theseinclude various devices that areinjected into the eye to createchannels to increase drainage of fluidfrom the eye and lower pressure.There is also a procedure known astrabeculotomy, in which the wall ofthe trabecular meshwork isremoved. The trabecular meshworkis part of the eye’s drainage channelthat can become blocked inglaucoma. These procedures havegood safety but as yet do not seemto lower intraocular pressure asmuch as trabeculectomy or glaucomadrainage device surgery.
Finally I wanted to mention animportant study of which severalScottish centres are involved. TheTreatment of AdvancedGlaucoma Study (TAGS) is anational study, based in Nottingham,which aims to answer the question ‘is
initial medical or surgical treatmentbest for patients with advancedglaucoma?’ We really don’t know theanswer to this. Many glaucomaspecialists feel that when somebodypresents with advanced glaucoma itmight be best to go for early surgery,as these patients tend to need verylow pressure, and trying various eyedrops may delay a more definitivetreatment. However surgery hasrisks and medication may work. Itwill be interesting to see the resultsof this study.
SummarySo to summarise, what’s new inglaucoma? Well, we are makingprogress in the three key areas I havediscussed. We can diagnose glaucomaearlier than before, we can detectprogression better and improvedtreatments are emerging. However,much more needs to be done.
Andrew TathamConsultant Eye Surgeon, Princess Alexandra Eye Pavilion, Edinburgh
14 News Spring 2015
Open Patient Meeting - Edinburgh -

15News Spring 2015
Public Awareness
National Glaucoma Awareness Week, 8-14 June 2015
This year's National Glaucoma Awareness Week will take place on the 8 - 14 June2015. The focus will be on driving and encouraging people to have regular eyehealth checks to ensure they are safe to drive.
As you all know, it is only with regular eye health checks, through an optometrist,that people will know if their driving vision is affected. Please ensure that your closeblood relatives (brother, sister, parent or child) are aware of the increased risk ofglaucoma, and encourage them to have regular eye health checks.
We will be reinforcing the message that glaucoma has no early symptoms but withearly detection and continued treatment people will often retain useful sight for life,and be safe to drive for many years.
The IGA will be supporting the campaign with information packs including posters,leaflets, banners and facts on glaucoma and driving. If you are interested in receiving a pack or would like to find out more about the week please email:[email protected]
Are you safe to drive?
GLAUCOMA could steal your driving licenceBook an eye test todayFor FREE help and advice call us on
Normal Vision
Mild Glaucoma
Advanced Glaucoma

16 News Spring 2015
Drug Update
We have been advised by Allergan that as of the 1st July 2015 they will ceaseproduction of Lumigan 0.3mg/ml (Bimatoprost 0.03%) Multidose bottle butwill continue in producing the 0.01% Multidose bottle.
Statement from Allergan:
Allergan has taken the decision to extend the date to cease supply of Lumigan(bimatoprost) 0.3mg/ml (0.03%) eye drops, solution to 1st July 2015.
The decision to cease supply and simplify our product range has been based on the needs of clinicians, pharmacists and patients to minimize confusion in prescribing. Thedecision was made after considerable deliberations and plans for managing the processwere created. This decision to extend the time to cease of supply has been made basedon the feedback from clinicians, RCOphtha, MHRA, DoH and patient organizations, inorder to minimize any impact on the patients and physicians. This additional time will help clinicians to manage their patients through transition and demonstrates our ongoing commitment to supporting the NHS.
The cease of supply is now being mirrored across Europe and as such any action has awider impact across the region. However, the mechanism by which patients are reviewedand followed up in the NHS has not moved as quickly as anticipated.
Below is a simplified explanation.
Lumigan (Bimatoprost 0.03%) Multidose Bottle – Discontinued 1st July 2015Lumigan (Bimatoprost 0.01%) Multidose Bottle – AvailableLumigan (Bimatoprost 0.03%) UD (Preservative Free) – AvailableGanfort (Bimatoprost/Timolol 0.03%) Multidose Bottle – AvailableGanfort (Bimatoprost/Timolol 0.05%) Multidose Bottle – AvailableGanfort (Bimatoprost/Timolol 0.03%) UD (Preservative Free) – AvailableGanfort (Bimatoprost/Timolol 0.05%) UD (Preservative Free) – Available
Allergan will ensure sufficient supply of the alternative formulations particularly Lumigan(Bimatoprost 0.01%) Multidose during this period to ensure a smooth transition.
If you have any additional questions you can call Allergan Medical Information on:01628 49 44 44 or if you prefer to email them you can do so to:[email protected]
17News Spring 2015
Michael Banes1947 - 2015
It was with great sadness that the IGA learnt of the death of Michael Banes, ahighly respected and valued trustee of the IGA and senior optometrist atMoorfields Eye Hospital.
Michael had been a trustee for four years. He was very active in board meetings andtackled issues from a positive perspective, and with good humour. He had the great skill of summarising a complex issue and offeringalternative solutions, frequently based on hisextensive scientific and clinical knowledge,always with the patient at the forefront of his mind. He was also a member of the IGA Medical and Scientific Advisory Committee and was quick with aresponse to allay a patients concerns.
Michael was passionate about his role as an optometrist and was instrumentalin helping the IGA to shape a response to The Government's views on howeye care services should be changed for the future. Many of theserecommendations are now being considered, so his legacy may be far reaching,and could benefit hundreds of thousands of patients resulting in an earlydiagnosis of glaucoma and the receipt of treatment of glaucoma in a locationthat is convenient and suits their needs.
Michael will be missed.

18 News Spring 2015
DVLA
Further information about visual field tests
The DVLA was recently in touch with IGA to clarify when a person may be askedto perform a second or third visual field test. The Driving and Glaucoma leaflet, asapproved by DVLA says: “Customers can take up to three visual field tests if thefirst or second charts do not comply with accuracy standards”.
The accuracy standard does not refer to numbers of points missed. Instead itrelates to “false positives” which is when a person has pressed the button tohighlight a point, when none is present. These are measured by the visual fieldmachine, not the operator. The visual field machine is designed to check for falsepositives a certain amount of times during a test (it is different for each machine).For example, if the machine does 10 checks and it identifies that the customer haspressed the button on five occasions when there is no point visible, then the falsepositives score for that test would be 50 per cent.
If the number of false positives is over 20 per cent, then the person will be asked tocarry out a second and even third visual field test. The operator is required toexplain in detail what the applicant has done wrong on the previous occasion.
If the false positives score remains over 20 per cent for all three visual field charts,then the DVLA will use this information and make the appropriate decision in linewith the investigation procedure.
We would like to remind everyone that both the visual field test and the visualacuity test must be carried out by an appropriately qualified and trained operator, ina quiet location, free from distraction with appropriate illumination for theequipment being used.
If you have further questions about this, please call our Sightline: 01233 64 81 70

19News Spring 2015
Words from Sightline
Medication contraindicated in acute angle closure glaucoma
An IGA member has highlighted the medications which are contraindicated with acuteangle closure glaucoma. Given that we have a number of new members, we are writingabout this again.
The medications are:
Motion sickness medicationAntihistaminesDecongestantsAsthma medicationSome antiparkinson drugsSome antidepressants (tricyclic antidepressants)Antispasmolytics eg. medication for irritable bowel syndrome etc
However you should always read the leaflet which comes with your medication.
Helen DoeSightline Advisor and Patient Support
Scottish Members SIGN DECIDE patient consultation.
Our grateful thanks to all of those Scottish members who respondedto our recent call for volunteers to participate in a consultation tohelp improve the quality of future Patient Guidelines throughout Europe. The organisers were delighted by the overwhelming responseand actually doubled the number of available slots before they wereforced to close the offer. Particular thanks goes to all those who wereunsuccessful on this occasion. We will keep you posted regardingprogress in further editions of IGA News.

20 News Spring 2015
Fond Farewell
Jini Gandolfi, Sightline Advisorretires after ten years with the IGA
I can just about remember the first day I started to workat the IGA in London. It was in the old offices in WarnerRoad, South East London, and what a journey it involved!First the train and then a bus ride and even then, wedidn’t get in for 09.30! I’m glad to say, I do now that we’ve moved to Ashford, Kent.
It has been ten years since that day, and I am finally taking retirement as from10th April, so it is a fond farewell to all the lovely members and friends of the IGA,and the independent callers who I have spoken to over the years, not forgetting theTrustees, and the helpful consultants along the way. It goes without saying, (and if Idon’t they’ll lynch me), I shall miss my colleagues, who are a wonderful group. We’ve all been together for a number of years now, so there will be a void,especially where all my colleagues are concerned.
Learning about glaucoma has been an interesting journey, and in the beginning, I never thought I would remember the names of the drops, let alone all theprocedures, but I did have some wonderful teachers. It has been amazing seeing the changes in treatments and the development in research and the ever hopefulnews of a cure for glaucoma one day.
So, altogether it has been an incredible learning process and whilst I know I havehelped some people, there will be some I couldn’t help and to those, I say -hopefully you got things sorted out eventually. This job has been rewarding, butsometimes heartbreaking as well, because there are just some things to which there is no answer.
I’m looking forward to a great summer and I hope you all have a great one as well!
Jini GandolfoSightline Advisor and Patient Support
21News Spring 2015
Research Recruitment
22 News Spring 2015
Research Recruitment
The feasibility of self-monitoring of eye pressure
Participants wanted for a Research Study
The measurement of the pressure within the eye (tonometry) is an essential test in thediagnosis and management of glaucoma. As with blood pressure, variability in eye pressureis a well-known phenomenon. However despite this variability, in many clinical situationsdecisions have to be taken based on a pressure reading at a single time point. A possiblemethod for obtaining more pressure readings is for patients to measure their eyepressure at home. A new instrument (the Icare Home tonometer) has been designedspecifically for self-tonometry.
The aim of this study is to determine how many people can be taught to record theirown eye pressure using the Icare tonometer and to compare the results to the readingstaken with the clinic standard (Goldmann) tonometer. We can then establish whether this additional information is helpful in clinical decision-making.
If you consent to taking part in the study, you will be asked to attend City University, Fight for Sight Clinic for a single 40-minute visit. You will not be paid for your time, butreasonable travel expenses will be covered.

23News Spring 2015
Becky’s Blog
Hello, time goes so fast these days it only feels like yesterday I was typing to all of you (even though I don’t really remember what I said… Thankfully I havethe last issue next to me).
Not much has happened these past three months concerning my eyes. I havebeen back to the hospital and my pressures in both eyes are 10. It’s the firsttime they’ve both been the same - which is pretty cool. I also had my fieldvision tested which is always fun; it’s like a little game where I get to pressbuttons. Thankfully my field vision is good so that gives me more confidence toapply for my driving licence. It’s strange that I might actually be learning todrive very soon.
It’s my birthday almost exactly a week from writing, which means it’s almost a year until I’m an actual adult. It’s a terrifying thought but I also can’t wait.Next time you hear from me I’ll be 17 and I’ll have lived with glaucoma for five years! The time since diagnosis has gone so quickly. I’m looking forward tocelebrating my birthday since I have a sheep cake; my favourite animal! I’m alsogoing to be having three of my good friends round for “scary films” (since mybirthday’s on Friday the 13th), although knowing all my friends, it’ll turn into a how-many-episodes-in-a-row-can-we-watch of Merlin, because that’s ourfavourite TV show!
I think that’s all I have to say this time, see you next season!
Becky is a 16 year old who loves anythingSherlock or Doctor Who, the music of Queen,reading, writing and playing the guitar. Shewas diagnosed with glaucoma at the age of 12.

Gloucestershire 0300 42 28 358Gloucestershire Royal Hospital, Redwood CentreGreat Western Road, Gloucester GL1 3NNHelen Jaggard • Date: 15/5/15 Time: 4.00pm
Derbyshire 01298 21 28 50Cavendish Hospital, Buxton Methodist Church, Chapel Street, Buxton SK17 6HX • Norma Ayres Date: 22/5/15 Time: 1.30pm
East Yorkshire 01482 34 22 97HERIB, Beech Holme, Beverley Rd, Hull HU5 3HSDate: 15/4/15 and 17/6/15 Time: 2.00pm
Scotland
01355 58 46 30or
01698 36 63 76
Hairmyres Hospital, Education Centre, East Kilbride Caroline Ferguson or Jackie McGowan Date: 20/5/15 Time: 2.30pm
07875 31 29 45
RNIB Offices, Meeting Room 1, 12-14 Hillside Crescent (off London Road), Edinburgh EH7 5EA • John HughesDate: 15/5/15 Time: 1.30pm
BedfordshireBedford Gurdwara, 84 Ford End Road, Bedford MK40 4JX • Roslyn HardingDate: 26/4/15 Time: 11.00am
Lancashire01204 39 03 90
extn 4806
Royal Bolton Hospital, Seminar Room, Eye Unit, H Block • Cathy Settle Dates: 7/5/15 and 2/7/15 Time: 1.30pm
24 News Spring 2015
Support Groups
Our patient support group model is based on recommendations from the NICE GlaucomaGuidelines published in 2009 and followed up with the NICE Glaucoma Management QualityStandards two years later which recommend that a support group should be initiated by eachhospital. The concept of these groups is to allow patients to meet their health careprofessionals in a relaxed atmosphere, away from the time restricted atmosphere on outpatients, so the condition and treatment can be discussed in more depth. It does require thepresence of at least one of your local health care professionals whether it be anophthalmologist, an optometrist or an ophthalmic nurse.

25News Spring 2015
Support Groups
0121 42 40 543or
0121 42 45 067
Solihull Patient Support Group, John Palmer Hall, Union Road, SolihullCarole Atkins or Denise Casey Date: 24/6/15 Time: 1.00pm
West Midlands
07884 31 09 92Neath Port Talbot Hospital, Room 300 ResourceCentre, Moor Road, Port Talbot SA12 7BJMaureen Griffiths • Date: 21/4/15 Time: 10.30am
029 20 74 77 47University Hospital of Wales, Sports and Leisure Facility, Cardiff CF14 4XW • Julia SwaffieldDate: 17/4/15 Time: TBC
Wales
01745 44 83 30extn 2439
Abergele Hospital, Stanley Eye Unit, Llanfair Road, Abergele, Conwy LL22 8DP • Hazel Lindop orMichelle Higgins • Dates: 20/4/15, 18/5/15,15/6/15 and 20/7/15 Time: 1.30pm
WestLancashire
01772 81 36 15
Southport and West Lancashire Support Group,Royal Clifton Hotel, The Promenade Southport Pam Ladlow Dates: 20/5/15 and 22/7/15 Time: 2.30pm
The above list contains details of support groups around the country which have beenorganised at the time the newsletter went to print. There are, however, other support
groups around the country which can be found listed below. Updated support group detailsfrom across the UK can be found on the IGA website (www.glaucoma-association.com)
or by calling Sightline on 01233 64 81 70.
Updated Support Group details from across the UK can be found on the IGA website www.glaucoma-association.com
07918 67 39 99or emma.mawson
@careuk.com
Care UK, Croft Shifa Health Centre, Belfield Road, Rochdale OL16 2UP • Emma MawsonDates: 20/4/15 and 27/7/15 Time: 1.30pm
Staffordshire
01785 23 02 40
Stafford Glaucoma Club, Postgrad Centre, CountyHospital, Weston Road, Stafford ST16 3SAShankar Chappiti or Kelli Cowlishaw Date: 1/5/15 Time: 2.00pm

26 News Spring 2015
Support Groups
Area Organised by Contact Name Contact Details
Buckinghamshire Milton Keynes Jill Kimber 01908 24 36 28 Hospital
Cambridgeshire Addenbrookes Hospital Deborah Jankowski 01223 24 51 51
Cheshire Leighton Hospital Debra Noden [email protected]
Cornwall Royal Cornwall Kate Claridge 01872 25 00 00 Hospital or Nichola Townend
Devon Royal Devon and Jane Kingett 01392 40 60 45 Exeter Hospital
Dorset Royal Bournemouth Peter Clark or Jackie Spence 01202 72 60 36
East Sussex Sussex Eye Hospital Gaynor Paul 01273 60 61 26
Conquest Hospital Huma Thomas 01424 75 52 55 extn 8442
Essex Broomfield Hospital 01245 44 36 73
Essex County Jocelyn Murphy or Lynn Barker 01206 74 46 72
Southend Hospital 01702 43 55 55
Greater Stepping Hill Angela Hilton 0161 48 31 010Manchester Hospital
Hampshire Southampton General Alex Macleod or Michelle Sayell 023 80 77 72 22
Hertfordshire Barnet Hospital Tracy Gavin 020 82 16 49 62
Kent Bromley Osteoporosis Stevie West 0208 31 39 835 Group
Maidstone General Margaret Gurney 01622 22 63 14

27News Spring 2015
Support Groups
Area Organised by Contact Name Contact Details
Kent Princess Royal Chris Wilsdon [email protected]
QEQM, Margate Nicola Anwar 01843 22 55 44 extn 63472
Queen Mary’s Maria Moutsou 020 83 02 26 78
Lancashire Rochdale Infirmary Julie Bremner 01706 90 17 57
Lincolnshire Pilgrim Hospital Darralynne Stell 01205 36 48 01
Liverpool Royal Liverpool and Vicki Travers 0151 70 63 968 Broadgreen University Hospital
London Central Middlesex Jenny Coelho 020 89 63 71 29 Croydon University Maria Kavanagh 020 84 01 30 00
Croydon Visual Regan Ruther 020 86 88 24 86
King’s College Viviane Brackenbury 020 32 99 16 68
St Ann’s Hospital Gissel Tapper 020 82 11 83 23
St Georges Hospital Edmore Mcube 020 82 66 61 15 or Christine Real 020 82 66 61 19
Western Eye Zena Rodrigues 020 96 66 66 66
Whipps Cross Katy Sommersgill 020 85 35 67 10
Manchester Henshaws Society Adrian Brooks 07925 96 21 84 for Blind People
Middlesex Ashford Hospital Maggie Lewis 01784 88 44 88
Hillingdon Hospital Amar Ghattaora 01895 23 82 82
28 News Spring 2015
Support Groups
Area Organised by Contact Name Contact Details
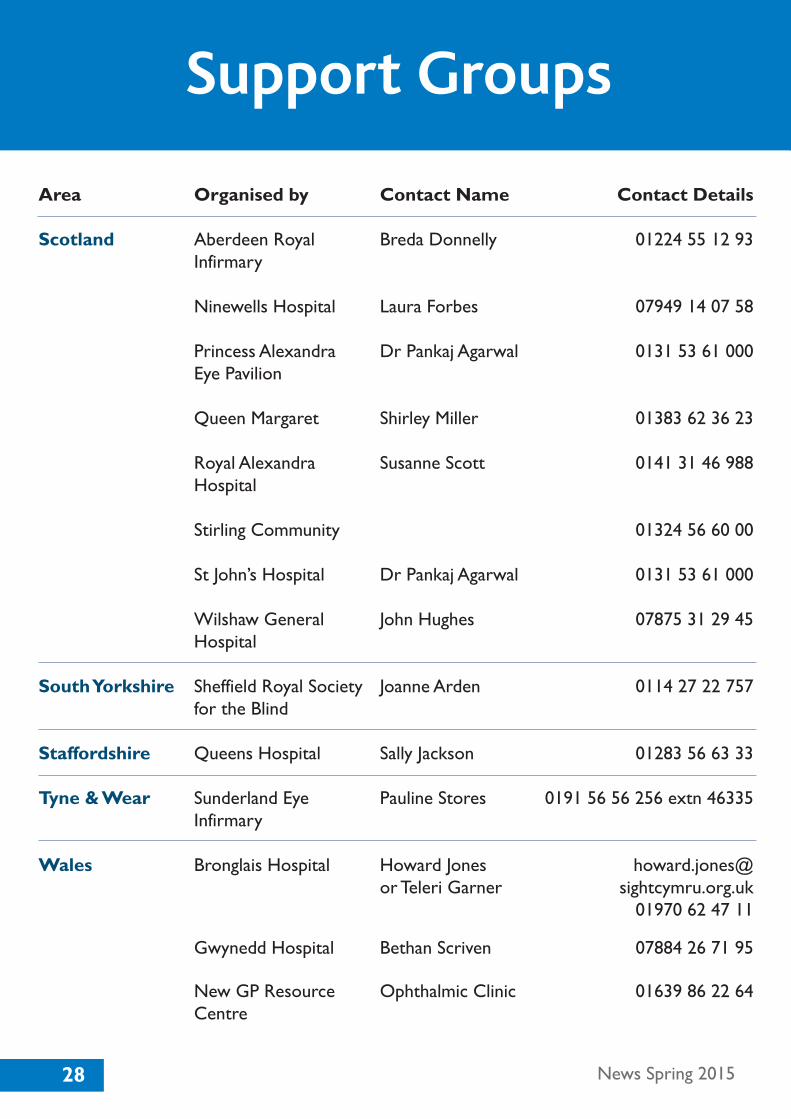
Scotland Aberdeen Royal Breda Donnelly 01224 55 12 93 Infirmary
Ninewells Hospital Laura Forbes 07949 14 07 58
Princess Alexandra Dr Pankaj Agarwal 0131 53 61 000 Eye Pavilion
Queen Margaret Shirley Miller 01383 62 36 23
Royal Alexandra Susanne Scott 0141 31 46 988 Hospital
Stirling Community 01324 56 60 00 St John’s Hospital Dr Pankaj Agarwal 0131 53 61 000
Wilshaw General John Hughes 07875 31 29 45 Hospital
South Yorkshire Sheffield Royal Society Joanne Arden 0114 27 22 757 for the Blind
Staffordshire Queens Hospital Sally Jackson 01283 56 63 33
Tyne & Wear Sunderland Eye Pauline Stores 0191 56 56 256 extn 46335 Infirmary
Wales Bronglais Hospital Howard Jones howard.jones@ or Teleri Garner sightcymru.org.uk 01970 62 47 11
Gwynedd Hospital Bethan Scriven 07884 26 71 95
New GP Resource Ophthalmic Clinic 01639 86 22 64 Centre

29News Spring 2015
Support Groups
Area Organised by Contact Name Contact Details
Princess of Wales Karen Phillips [email protected]
Singleton Hospital Sue Neale 01792 20 03 90
Ysbyty Cwm Sue Brooks 07884 36 22 64 Rhondda Llwynypia West Midlands Good Hope Hospital Sarah Morris 0121 42 42 000
Heartlands Hospital Carole Atkins or Clair Rea 0121 42 40 543
Kidderminster Helen Hipkiss 01562 51 23 82 extn 55369 Treatment Centre
New Cross Hospital Mary Stott 01902 30 79 99 extn 5807
Russells Hall Hospital Julia Phillips 01384 45 61 11 extn 3649 University Hospital Jay Pankania 024 76 96 64 91
West Sussex Worthing Hospital Annette Brampton 01903 20 51 11 extn 5658 or Julie State
Worcestershire Alexandra Hospital Julie Manning 01527 50 79 15
Worcester Sara Ruck 01905 76 33 33 extn 33379 Royal Hospital
Registered Office: Woodcote House15 Highpoint Business Village
Henwood, AshfordKent TN24 8DH
Administration: 01233 64 81 64Sightline: 01233 64 81 70
Fax: 01233 64 81 79Email: [email protected]
www.glaucoma-association.comCharity registered in England & Wales No. 274681 and Scotland No. SC041550 • Registered Company No. 1293286
Important Announcement
In the Spring edition of the IGA Newsletter, we published an article concerning the cease of supply of Lumigan (bimatoprost) 0.03% Multidose eye drops on 1st July 2015. Unfortunately an error was made in the information regarding the active ingredients. Please find below a corrected list:
Lumigan (bimatoprost 0.03%) Multidose Bottle – Cease of supply 1st July 2015Lumigan (bimatoprost 0.01%) Multidose Bottle – AvailableLumigan (bimatoprost 0.03%) UD (Preservative Free) – AvailableGanfort (bimatoprost/timolol 0.03%/0.5%) Multidose Bottle – AvailableGanfort (bimatoprost/timolol 0.03%/0.5%) UD (Preservative Free) – Available
If you have any additional questions you can call Allergan Medical Informationon: 01628 49 40 26 or if you prefer to email them you can do so to:[email protected]
We apologise for the error contained within the published article and for anyconfusion this may have caused.
Russell YoungChief Executive
Printing of this announcement has been paid for by a grant from Allergan
IGA Letterhead 2015.qxp_IGA 15/05/2015 12:51 Page 1


NationalGlaucomaAwareness
Week8th - 14th June 2015
INTERNATIONAL GLAUCOMA ASSOCIATIONWoodcote House
15 Highpoint Business VillageHenwood,AshfordKent TN24 8DH
Sightline: 01233 64 81 70
Administration: 01233 64 81 64
Fax: 01233 64 81 79
Email: [email protected]
Website: www.glaucoma-association.com
For Free Leaflets and PostersPlease Contact
Sightline +44 (0)1233 64 81 70
Information, support & advice
Sightline +44 (0)1233 64 81 70
Information, support & advice
IGA Newsletter Spring 2015.qxp_IGA 19/03/2015 15:34 Page 33

For F
REE h
elp a
nd ad
vice c
all u
s on
ww
w.g
lauco
ma-a
ssoci
ation.c
om
info
@ig
a.o
rg.u
k
· Glau
com
a Ste
als S
ight
· Eye C
heck
Vita
l
· Prot
ect y
our D
rivin
g L
icen
ce an
d Visi
on
· Be Sa
fe on
the R
oad
IGA Newsletter Spring 2015.qxp_IGA 19/03/2015 15:34 Page 35