2012 har education and information session amy camp, mdh jonathan peters, mha lucas hovila, mha
TRANSCRIPT
2012 HAR Education and Information Session
Amy Camp, MDHJonathan Peters, MHALucas Hovila, MHA

2012 Education and Information Topics
• Changes to the 2012 Formset & Extension Requests
• Data Requests & Usage• Capital Expenditure Hospital and
System Level Reporting• Diagnostic Imaging Reporting• Clinic Reporting on the HAR• Self-Pay and Charity Care• Reminders, Resources, and Tips
• Medical Care Surcharge Estimator

2012 Formset Changes
•NO CHANGES!
Extension Requests
• Increasingly, the legislature and the public are looking for more up-to-date information from government. MDH wants to work with MHA and hospitals on reducing the need for data filing extensions beyond the initial 21 days. We hope MDH will need to grant longer extension requests only in the most extreme cases, where sticking to the timeline would pose and undue hardship on hospitals or compromise the quality of the report.

New Changes to Extension Policy
• For the 2012 HAR, MHA is now only able to grant an initial extension of 21 days.
• If a hospital is 30 days late submitting their HAR (compared to 60 days in the past), the hospital will be turned over to MDH.

Extension Requests
• In FY 2011, 65% of hospitals asked for an extension.
• Of the 65% of hospitals that asked for an extension, 22% of hospitals asked for an extension of 30 days or greater.

Who Requests HAR Data?
• Other Areas of MDH• MN Legislature• MN Department of Human Services• Media• MN Nurses Association• Researchers in Public Policy
What HAR Data is Requested?
• Uncompensated Care• Community Benefit• Capital Expenditures• Staffing• Payer Mix• Financial Performance of the Industry• Trends in Utilization• Bed Type Information

How is HAR Data Used?
• Community Benefit Report to the Legislature http://www.health.state.mn.us/divs/hpsc/hep/publications/legislative/communitybenefits2009.pdf
• Capital Expenditure Reporting• Minnesota Health Care Markets
Chartbook (section 8) http://www.health.state.mn.us/divs/hpsc/hep/chartbook/index.html
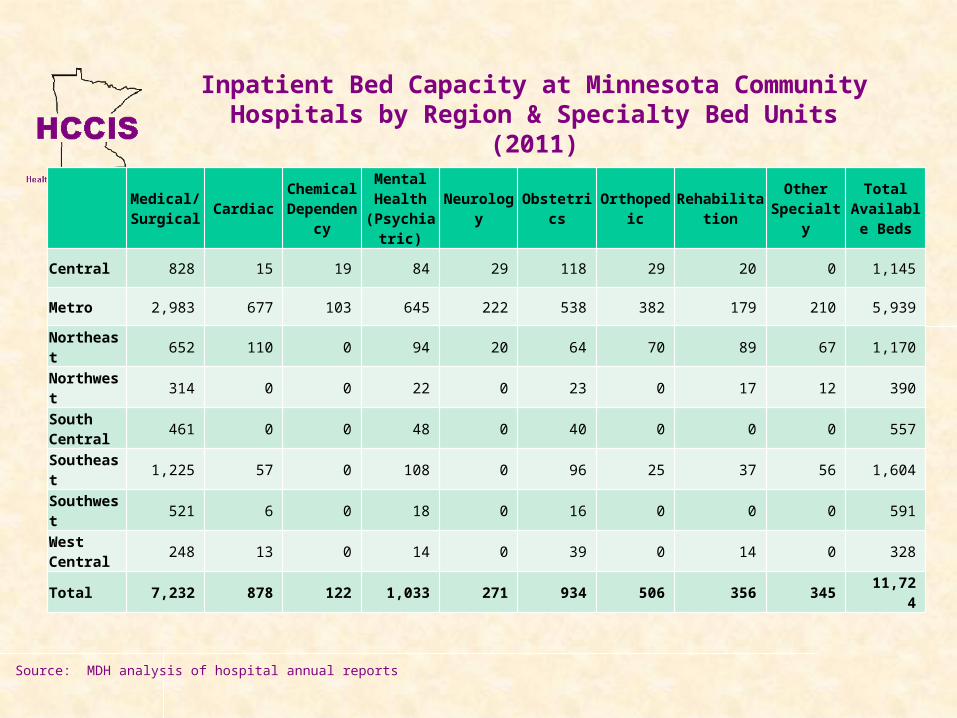
Inpatient Bed Capacity at Minnesota Community Hospitals by Region & Specialty Bed Units (2011)
Medical/Surgical Cardiac Chemical
DependencyMental Health
(Psychiatric)Neurology Obstetrics Orthopedic Rehabilitation Other
SpecialtyTotal
Available Beds
Central 828 15 19 84 29 118 29 20 0 1,145
Metro 2,983 677 103 645 222 538 382 179 210 5,939
Northeast 652 110 0 94 20 64 70 89 67 1,170
Northwest 314 0 0 22 0 23 0 17 12 390
South Central 461 0 0 48 0 40 0 0 0 557
Southeast 1,225 57 0 108 0 96 25 37 56 1,604
Southwest 521 6 0 18 0 16 0 0 0 591
West Central 248 13 0 14 0 39 0 14 0 328
Total 7,232 878 122 1,033 271 934 506 356 345 11,724
Source: MDH analysis of hospital annual reports
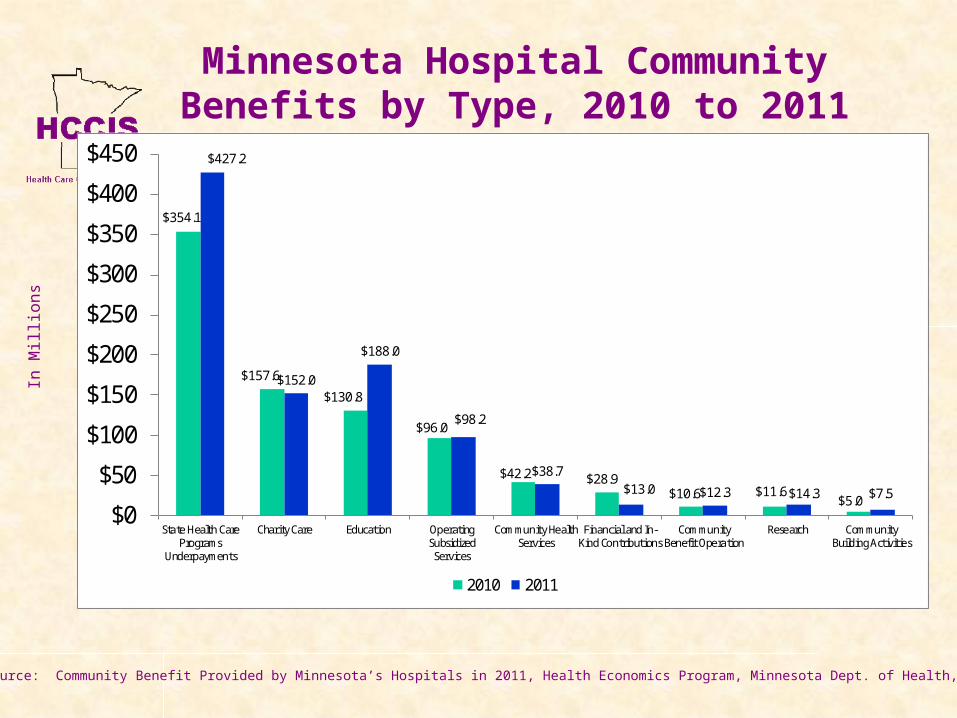
$354.1
$157.6
$130.8
$96.0
$42.2 $28.9$10.6 $11.6
$5.0
$427.2
$152.0
$188.0
$98.2
$38.7$13.0 $12.3 $14.3 $7.5
$0
$50
$100
$150
$200
$250
$300
$350
$400
$450
State Health CarePrograms
Underpayments
Charity Care Education OperatingSubsidized
Services
Community HealthServices
Financial and In-Kind Contributions
CommunityBenefit Operation
Research CommunityBuilding Activities
2010 2011
Minnesota Hospital Community Benefits by Type, 2010 to 2011
Source: Source: Community Benefit Provided by Minnesota’s Hospitals in 2011, Health Economics Program, Minnesota Dept. of Health, forthcoming
In M
illi
ons

Use of Capital Expenditure Information
• Capital expenditure information is used by MDH to fulfill statutory requirements to review major spending commitments by hospitals and other providers.
• MDH also uses capital expenditure data to produce informational documents to inform the public on spending trends.
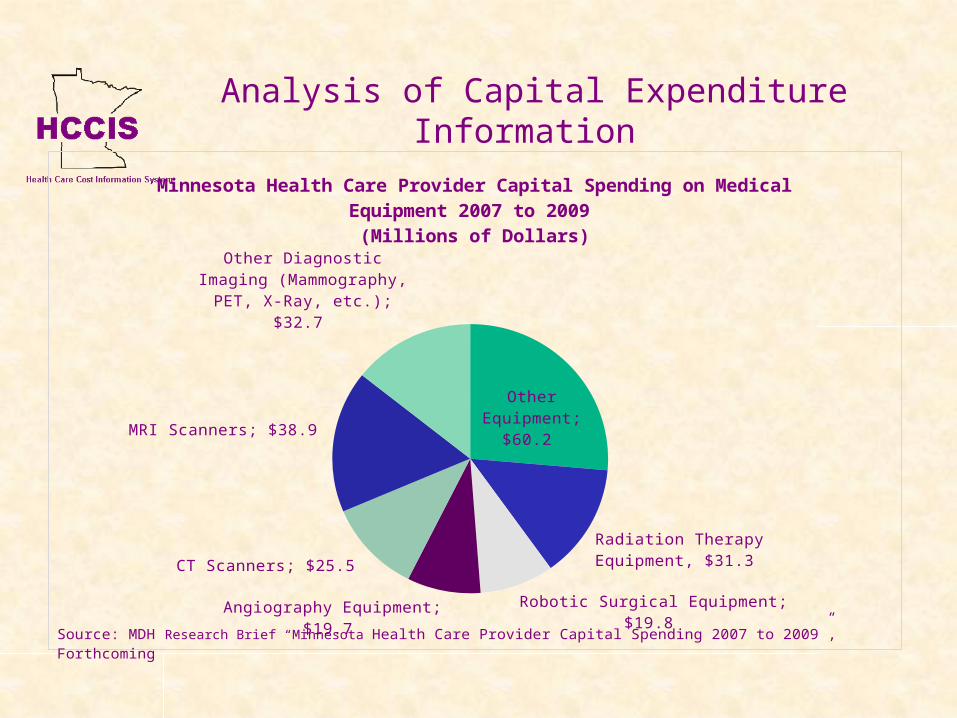
Analysis of Capital Expenditure Information
Other Equipment; $60.2
Radiation Therapy Equipment, $31.3
Robotic Surgical Equipment; $19.8 Angiography Equipment; $19.7
CT Scanners; $25.5
MRI Scanners; $38.9
Other Diagnostic Imaging (Mammography, PET, X-
Ray, etc.); $32.7
Minnesota Health Care Provider Capital Spending on Medical Equipment 2007 to 2009
(Millions of Dollars)
Source: MDH Research Brief “Minnesota Health Care Provider Capital Spending 2007 to 2009”, Forthcoming

-8.0%
-6.0%
-4.0%
-2.0%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
2008 to 20092009 to 20102010 to 2011
Trends at Minnesota Community Hospitals, 2008 to 2011
Percent Change from Previous Year
*Actual ValueSource: MDH analysis of hospital annual reports

Capital Expenditures
A Guide to Minnesota
Capital Expenditure Reporting

Contact Information
A Capital Expenditure Contact is required by all hospitals. This should list the individual responsible for any questions relating to Capital Expenditures.
The Capital Expenditure Contact is required, and is not optional.

Reporting Requirements
There are two separate reporting requirements for Capital Expenditures Reporting of major capital expenditure
commitments greater than one million dollars (see HAR sections 56 & 57).
Providing sufficient project specific information about capital expenditure commitments for MDH to complete a retrospective review of each project greater than one million dollars (see capital expenditure project specific tab of the formset).

Reporting Forms
Providers submit capital expenditures on existing annual financial reports Hospitals - Hospital Annual Report (HAR) Surgical Centers – Freestanding Outpatient
Surgical Center (FOSC) Report Imaging Centers - Diagnostic Imaging Facility
Report Physician Clinics or Clinic Systems – System
Capital Expenditure Report Health Care Systems - Capital Expenditure Report

Health Care Systems Decision Chart
Contact Information:
http://www.health.state.mn.us/healtheconomics
Amy CampHCCIS AdministratorMinnesota Department of [email protected]

Clinic Reporting
Reporting Guidelines for Clinic Information on the Hospital
Annual Report

Clinic Decision Flowchart

Offsite Locations Tab
• All outpatient departments, clinics, and components not located on the hospital's premise
• Offsite locations where services provided are billed under the hospital's Medicare and Medicaid provider numbers
• Verified against hospital license application

Offsite Locations Tab
• Reminder:– This tab is matched against Gross Clinic
Charges (account 0207) and Other Institution Charges (account 0208).
– If there is an offsite entity being listed in account 0207 and/or 0208, please list these entities on the Offsite Locations Tab.
– For each entity that is listed on the Offsite Locations Tab, please fill out all data fields.

Diagnostic Imaging
Reporting Guidelines for Diagnostic Imaging

Diagnostic Imaging Provider
• For Diagnostic Imaging Services, if your hospital has the service available on site (either by the hospital or contracted services), you will be asked to provide the name of the provider.
• This is being asked to help tie diagnostic imaging provider information (which is collected on separate report) to the HAR data.
• Contact your Radiation Safety Officer to confirm the DI equipment available at your facility.

Diagnostic Imaging
• If the hospital has a fee per scan/exam plan, the service should be listed as available and must list the owner of the equipment.
• If the hospital has a Capital Lease for a scanner then for purposes of HCCIS, the scanner should be listed as being hospital owned.

Diagnostic Imaging
• There will be an audit check to match the availability of service, the machine type, and the owner of the machine to what was reported the previous year.
• If anything has changed, please provide a note describing the change.
• This information is also verified against a report that DI providers supply MDH.
Self-Pay and Charity Care
Reporting Self-Pay and Charity Care on the HAR

Self Pay and Charity CareThe percentage discount offered to Self Pay patients will be collected. Please note that this will be non public data.
Charity Care Adjustments will be broken out into Insured vs. Uninsured.
Within Uninsured, three further pieces of data will be collected:• Amount that was 100%
discounted• Amount that was only a
partial discount of full bill
• The average partial discount given to uninsured patients

Self Pay and Charity CareRemember that only Uninsured Patients Charity Care needs to be broken out into Full and Partial Charity Care (accounts 7573 and 7574, respectively), not the total charity care adjustment amount.
Partial Charity Care (account 7574) is now an auto-calculated cell to aid preparers in filling this section out correctly.

Reminders, Tips, and Resources for Preparers
General Guidelines and Places for Further Information

Medical Care Surcharge Estimator
A Medical Care Surcharge Estimation Tool has been included on a separate tab in the HAR 2012.
After completing the HAR, please review this tab to verify that the information reported on the HAR for these key accounts is accurate.
DHS remains the sole determiner of your surcharge, and this tool is to be used only to give guidance and help in the correct completion of the HAR.
MCR and Audited Financial Statement Submission
• MHA has the ability to receive the Medicare Cost Report in the ECR file format.
• ECR format is the preferred format for the MCR.
• Your hospital’s AFS and MCR should be submitted as soon as they become available.

Data Transmission Method Available
• HTTPS data transmission available– Transmission encrypted and secure– As easy as web e-mail or online banking– Hospitals can download their prior year’s Commentary or
Hospital Profile report from same site as well.– More safe and secure than postal mail or e-mail– No file size restrictions, unlike e-mail
• This method is highly recommended by MDH and MHA for data transmission
• Please contact MHA to receive your login and password
• Web address: https://har.mnhospitals.org
Places for Further Information
• Both MDH and MHA’s website have further information on HAR related issues.– MDH Website: http://www.health.state.mn.us/divs/hpsc/dap/hccis/index.html – MHA Website:
http://www.mnhospitals.org/data-reporting/mandatory-reporting/health-care-costs-information-systems-hccis
• All Deadlines and Events are posted on websites.
• Power Point presentation of 2011, 2010 and 2009 HAR Education and Information Sessions available at sites above.
• Electronic Newsletters covering the following topics:– Getting Started– Microsoft Excel Tips and Useful Tools– Expense Allocation Methodology– Primary Payer Charges and Adjustments– Outpatient Charges
• If a question or problem arises while completing the Hospital Annual Report, please contact Jonathan Peters or Lucas Hovila at MHA or Amy Camp at MDH (see last slide for contact information).

Contact Information
• MHA staff at (800) 462-5393 or (651) 641-1121
• Jonathan Peters, MHA (651) 659-1422
• Lucas Hovila, MHA (651) 603-3536
• Amy Camp, MDH (651) 201-3575