2011 douglas t. miller symposium dennis wagner, acting director, office of clinical standards and...
TRANSCRIPT

2011 Douglas T. Miller Symposium
Dennis Wagner, Acting Director, Office of Clinical Standards and QualityCenters for Medicare & Medicaid Services
April 29, 2011
Plan for This Segment
• “Gestalt” Overview of CMS, Health Reform and Quality Improvement
• Quality Improvement Lessons from the Organ Donation Breakthrough Collaborative
• Partnership for Patients• Discussion

Questions to Run On
• What is happening at CMS?• What is going on with the implementation of
healthcare reform – especially on quality?• What can we learn from the success of the national
organ donation quality improvement work?• What is the Partnership for Patients?• What is my advice for CMS?
3

CMS is Changing
4

CMS Vision
CMS is a major force and a trustworthy partner for the continual
improvement of health and health care for all Americans.
5

Operating Values
How we shall work together and with others?• Boundarilessness• Speed and Agility• Unconditional Teamwork• Valuing Innovation• Customer Focus
6

Better Health forthe Population
Better Carefor Individuals
Lower CostThrough
Improvement
The “Three-Part Aim”
7

5 New Centers and Functions Added in 1 Year
1. Center for Strategic Planning, Tony Rodgers2. Center for Program Integrity, Peter Budetti3. Center for Medicare and Medicaid Innovation, Rick Gilfillan4. Center for Consumer Information and Insurance Oversight,
Steve Larsen5. Federal Coordinated Health Care Office, Melanie Bella
• Center for Medicare, Jon Blum• Center for Medicaid, CHIP, and S&C, Cindy Mann• Office of Clinical Standards and Quality, Dennis Wagner & Paul
McGann, MD
8

Office of Clinical Standards and QualityLevers for Safety, Quality & Value
• Contemporary Quality Improvement• Transparency, Public Reporting & Data
Sharing• Incentives• Regulation• National & Local Coverage Decisions• Demonstrations, Pilots, Research, Grants,
Innovation9

Office of Clinical Standards and QualityLevers for Safety, Quality & Value
• Contemporary Quality Improvement: Quality Improvement Organizations
• Transparency, Public Reporting & Data Sharing: Hospital Inpatient Quality Reporting Program
• Incentives: Hospital Value Based Purchasing• Regulation: Conditions of Participation (OPOs, Hospitals,
14 other provider types)• National & Local Coverage Decisions: Coverage for
Preventative Services• Demonstrations, Pilots, Research, Grants, Innovation:
Diabetes Self Management in Mississippi10

Affordable Care ActSome Key CMS Accountabilities
• Major, Ongoing Demonstration & Testing Authority & Resources (CMMI)
• Accountable Care Organizations• Value Based Purchasing Programs• Health Insurance Exchanges• Expanded Medicaid Programs• Care Transitions to Reduce Readmissions• Expanded Quality Reporting Programs• Expanded Preventative Services• ….and Much More

Affordable Care Act Provision with Quality Focus
Value based purchasing• 3001 - Hospital value-based purchasing• 3006 - Value-based purchasing for SNF• 3014 - Quality and efficiency measurement• 10301 - Develop a plan to implement VBP for ambulatory surgical
centers• 10326 - Pilot testing for pay-for-performanceHospital readmissions• 3025 - Hospital readmissions reduction program• 3026 - Community-based care transitions programHealthcare acquired conditions• 2702 - Payment adjustment for health care-acquired conditions• 3008 - Payment adjustment for conditions acquired in hospitalsAccountable care organizations• 2706 - Pediatric accountable care organization demonstration
project• 3022 - Medicare Shared Savings ProgramDual eligibles• 2602 - Providing federal coverage and payment coordination for dual
eligible beneficiariesPreventative services• 4103 - Annual wellness visit providing a personalized plan• 4104 - Removing barriers to preventive services• 4105 - Evidence-based coverage of preventive services
Coordination of care• 2703 - State option to provide health homes for enrollees with chronic
conditions• 2704 - Demonstration project to evaluate integrated care around a
hospitalizationLong term care• 2401 - Community first choice option• 2402 - Removal of barriers to providing home and community based services• 2403 - Money follows the person rebalancing demo• 2404 - Protection for recipients of home and community-based services
against spousal• impoverishment• 10202 - Incentives for states to offer home community based servicedPublic reporting• 10303 - Development of outcome measures• 10327 - Improvements to the physician quality reporting system -- also see
Provision 3002• 10331 - Public reporting of performance informationQuality reporting initiative• 2701 - Adult health quality measures• 3002 - Improvements to the physician quality reporting system.• 3004 - Quality Reporting for Long Term Care Hospitals (LTCH), inpatient
rehabilitation• hospitals, and hospice programs• 3005 - Quality reporting for PPS-exempt cancer hospitals• 10322 - Quality reporting for psychiatric hospitals
12

CMS Approach to Managing the Affordable Care Act
13
Quadrant 1High impact, high complexity
program areas tomanage
Quadrant 2High impact priorities to
monitor and maintain
Quadrant 4Tertiary priorities tominimize resources
and conserve focus
Quadrant 3Secondary priorities to monitor
and manage

OCSQ Quadrant 1: High Impact, High Complexity Program
Areas to Manage
14
1.Value Based Purchasing2.Public and Quality Reporting3.Reduced Readmissions4.Hospital Acquired Conditions5.ACOs6.Center for Medicare and Medicaid Innovation7- 8-9-10-11-12-13
Quadrant 2
Quadrant 3Quadrant 4

OCSQ Quadrant 2: High Impact Priorities to Monitor and Maintain
1.Preventative services
-- more in other CMS components --
Quadrant 2High impact priorities to monitor and maintain
15
Quadrant 2
Quadrant 3Quadrant 4
Quadrant 1
What Will the Affordable Care ActLook Like on the Front Lines?
• Increasing measurement of quality, efficiency & value• Public reporting and sharing of data• Reimbursement linked to quality improvement, efficient
service delivery and cost reduction thru improvement• Increasing integration of delivery systems and coordination
of care across settings• Greater role in addressing public health issues• Greater use of health information technology• Creation of a learning environment in healthcare
16

New Tools, New Incentives, New Penalties, New Organizations
What does it all mean?
17

Value-Based Purchasing and Linking Payment to Quality
18

New Tools, New Incentives, New Disincentives, New Organizations
What does it all mean?
Doing the right things for patients will become easier and doing the wrong things will become more difficult.
19
Questions for Quick Reaction and Discussion
• What do you like about what you see in this high level gestalt?
• What does CMS need to do more of, better, differently?
20

21
The Healthcare Quality/Value Challenge
• U.S. spends more per capita on healthcare than any other country in the world
• Quality is often inferior to that of other nations
• Significant variation in quality and cost by geographic location
• Serious disparities in the quality of health care by race, and socioeconomic status

How do we make quality better?
22

How do we make quality better?
• Improvement as a Strategy• Customer-Mindedness• Process-Mindedness• Employee-Mindedness• Statistical Thinking• Supplier-Mindedness• Continual Improvement (PDSA)• Leadership

How do we make quality better?-- Stages of Facing Reality --
• Stage 1. “The data are wrong”• Stage 2. “The data are right, but it’s not a
problem”• Stage 3. “The data are right; it is a problem;
but it is not my problem.”• Stage 4. “I accept the burden of
improvement”

How do we make quality better?
• Clear Intent – Will• Proven Practices – Ideas• Focused, Constant Action -- Execution
25

How do we make quality better?
• Clear Intent – Will• Proven Practices – Ideas• Focused, Constant Action – ExecutionOur work on organ donation is an
extraordinary national example of what is possible.
26
50% of eligible donors are found in 206 hospitals
75% of eligible donors are found in 483 hospitals
90% of eligible donors are found in 846 hospitals
Concentration of Potential DonorsConcentration of Potential DonorsIn Nation’s Largest HospitalsIn Nation’s Largest Hospitals

Tremendous Variation in Donation Rates in 300 Largest Hospitals
Conversion Rate Distribution among the Largest 300 Hospitals 9/02-8/03
0
10
20
30
40
50
60
70
80
[0%,10%] [10%,20%] [20%,30%] [30%,40%] [40%,50%] [50%,60%] [60%,70%] [70%,80%] [80%,90%] Over 90%
Conversion Rate
Nu
mb
er o
f H
osp
ital
s

Collaborative Model An intensive, full-court-press to facilitate
breakthrough transformations in the performance of organizations, based on what already works.
Designed To: Designed To: Define, Document, and Disseminate Best Define, Document, and Disseminate Best
PracticesPractices Accelerate ImprovementAccelerate Improvement Achieve Results at a Rapid PaceAchieve Results at a Rapid Pace Build Clinical Leaders of ChangeBuild Clinical Leaders of Change
“All Teach, All Learn”

Collaborative Engine
Select Topic
Planning Group
Identify Change
Concepts
Enroll Participants
Prework
LS 1 LS3LS 2
Support System
ListServe Site Visits & Filming
Conference Calls Rapid Sharing
Data Reporting Website
S
A D
P
S
A D
P
Measures of Success
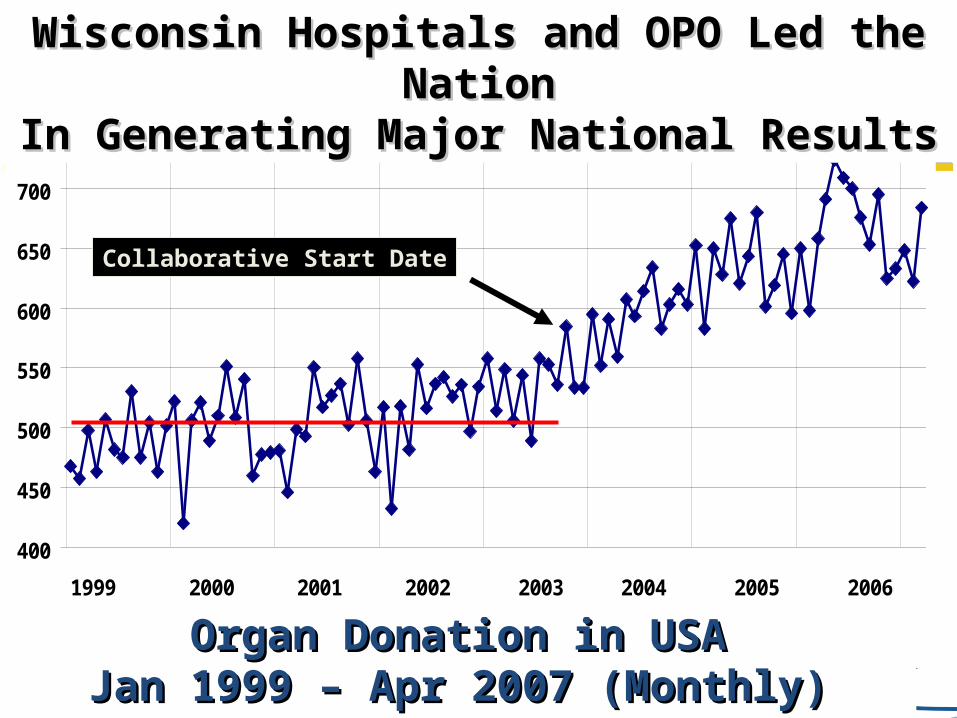
Organ Donation in USAOrgan Donation in USAJan 1999 – Apr 2007 (Monthly)Jan 1999 – Apr 2007 (Monthly)
400
450
500
550
600
650
700
750
1999 2000 2001 2002 2003 2004 2005 2006
Collaborative Start Date
Wisconsin Hospitals and OPO Led the NationWisconsin Hospitals and OPO Led the NationIn Generating Major National ResultsIn Generating Major National Results

Conversion Rate by Month: 2002-2010
40.0%
45.0%
50.0%
55.0%
60.0%
65.0%
70.0%
75.0%
80.0%
JAN02
AUG02
MAR03
OCT0
3
MAY04
DEC04
JUL0
5
FEB06
SEP06
APR07
NOV07
JUN08
JAN09
AUG09
MAR10
OCT1
0
Month/Year
Co
nv
ers
ion
Ra
te Collaborative starts here
data source: OPTN

UWHC OPO Performance Rates by Year
7369
66
7875
78 8184 84 84
8278
8386 88 88 88
52 5459 62
6771 72 75
70
0
10
20
30
40
50
60
70
80
90
100
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Conv
ersi
on R
ate
(%)
OPO Conversion Rate
OPO Adjusted Conversion Rate
National Conversion Rate (2010 Jan-Jun)
OPO Conversion Rate: (Eligible Donors/Eligible Deaths)OPO Adjusted Conversion Rate: (Eligible Donors + Other Donors/Eligible Deaths + Other Donors)

What made it work? Including the Customer: Donor Families and
Recipients Clear, Ambitious, Achievable Aims Transparent About Data and Practice Model for Improvement and Collaborative
Methodology Teaming Nationally to Work Smarter, Faster Creating Bolder, Thoughtful Agendas for Action Rapid Testing & Change Using Proven Practices Doing More Of What Works Relentless Pursuit of Improvement, Never Settling
for the Status Quo

Questions for Discussion and Action
• What are our key insights about the organ donation improvement work?
• How can we take this further?
• What can we learn and apply to our current challenges and opportunities with healthcare reform?
36

Partnership for Patients: An Overview
April 2011

The Affordable Care Act Improves Health Care Quality
• The Affordable Care Act (ACA) is best known for fixing broken health insurance laws and helping to cover millions of previously uninsured Americans.
• What many people don’t know is all of the ways the new law is also reducing costs while improving the experience of being a patient, being a caregiver, and being a health care provider.
• The Partnership for Patients: Better Care, Lower Costs is one example of how Secretary Sebelius is using provisions of the ACA to make health care in America safer, more efficient, and less costly.

Meet Josie King

Unfortunately, Josie King’s story is not rare.
• On any given day, 1 out of every 20 patients in American hospitals is affected by a hospital-acquired infection.
• Among chronically ill adults, 22 percent report a “serious error” in their care.
• 1 out of 7 Medicare beneficiaries is harmed in the course of their care, costing the federal government over $4.4 billion each year.
• Despite pockets of success -- we still see massive variation in the quality of care, and no major change in the rates of harm and preventable readmissions over the past decade.
We can do much better – and we must.

Partnership for Patients Better Care, Lower Costs
1. Reduce harm caused to patients in hospitals. By the end of 2013,
preventable hospital-acquired conditions would decrease by 40% compared to 2010.
– Achieving this goal would mean approximately 1.8 million fewer injuries to patients with more than 60,000 lives saved over the next three years.
2. Improve care transitions. By the end of 2013, preventable complications during a transition from one care setting to another would be decreased such that all hospital readmissions would be
reduced by 20% compared to 2010.
– Achieving this goal would mean more than 1.6 million patients would recover from illness without suffering a preventable complication requiring re-hospitalization within 30 days of discharge.
Potential to save up to $35 billion dollars over three years.

How Will Change Actually Happen?
• There is no “silver bullet”• We must apply many incentives• We must show successful
alternatives• We must offer intensive supports
– Help providers with the painstaking work of improvement

We Know Major Improvement Is Possible
• 150 New Jersey health care facilities reduced pressure ulcers by 70%
• Rhode Island reported a 42% decrease in Central Line-Associated Bloodstream Infections (CLABSI) (2006-2007)
• More than 65 Institute for Healthcare Improvement Campaign hospitals reported going more than a year without a ventilator-associated pneumonia in at least one unit.
• Ascension Health sites participating in a 2007 peri-natal safety initiative achieved birth trauma rates that were at or near zero.
• And much more…

44
Workin
g D
raft - La
st Mod
ified
04
/19
/23
05
:31
AM

Our Request to You• Join the Partnership for Patients
• Go to healthcare.gov/partnershipforpatients

Core Topics in Improvement
• Improvement as a Strategy• Customer-Mindedness• Process-Mindedness• Employee-Mindedness• Statistical Thinking• Supplier-Mindedness• Continual Improvement (PDSA)• Leadership

Defining “Quality”
“Meeting and Exceeding the Needs and Expectations of
Customers”

Learning about the Customer
• Observe• Survey• Use your own experience• Ask!

As a Customer…
• What is the #1 thing you would like CMS to improve?
• What is the #1 thing you want CMS to keep the same?
49

“Never doubt that a small group of thoughtful, committed citizens can change the world. Indeed, it is the only thing that ever has.” –Margaret Mead

Contact Information
Dennis WagnerActing Director, Office of Clinical Standards and Quality
Centers for Medicare and Medicaid ServicesOffice of Clinical Standards and Quality
7500 Security Blvd., MSC: S3-02-01Baltimore, MD 21244-1850
Phone Number: 410-786-6841E-mail Address: [email protected]
51

Question for Reflection and Action
What is it about this work that makes my heart sing?
52