©2007 rush university medical center hyperuricemia in adolescents with primary hypertension: how...
TRANSCRIPT
©2007 RUSH University Medical Center
Hyperuricemia in adolescents with primary hypertension: how and when to intervene?
Farahnak Assadi, M.D.Professor Emeritus

Facts about uric acid and HTN
• Hyperuricemia is frequently associated with primary hypertension (HTN) in both adult and pediatric patients.
• Up to 60% of children with primary HTN may have elevated serum uric acid (UA) levels above 5.5 mg/dL.
• UA-induced HTN is mediated through the activation of the RAS and vascular endothelial dysfunction.
• Elevated UA level is a predictor of incident HTN and cardiovascular (VD) disease.
• Feig DI Adv Chronic Kidney Dis. 2012;19:377-385• Soletsky B et al. Hypertension. 2012; 60:1148-1156• Assadi F. J Nephrol. 2014;27:51-56
Hypothesis
• Treating primary HTN with usual antihypertensive agents may not completely reduce CV risk related to elevated serum UA levels.
• Lowering serum elevated serum UA levels may provide greater benefit than simply treating HTN with the conventional therapy.

Aim of the study
• Allopurinol in combination with ACE inhibition may reduce BP more effectively than ACE inhibitors alone in hyperuricemic adolescents with primary HTN.

Patients
• A total of 118 children and adolescents referred for evaluation of HTN in accordance with the recommendations of the Fourth Report of the Task Force on the Diagnosis, Evaluation and Treatment of HTN in Children and Adolescents.
• The 4th Task Report on High BP in Children and Adolescents, Pediatrics 2004, 114:555-574
©2007 RUSH University Medical Center
Exclusion criteria
• Patients excluded if they had pre-HTN, stage- 2 HTN, white-coat HTN, CVD, or known renal endocrine, cardiovascular or hepatic dysfunction.
• Also excluded were patients with a fasting blood sugar greater than 110 mg/dL, hemoglobin A1C greater that 6%
• Patients on medications known to cause high BP or increase serum uric acid level were also excluded.
Eligible patients
• Adolescent patients (12-19 years old) with newly diagnosed and never treated stage-1HTN, in whom secondary hypertension was excluded.
• All participant had baseline serum uric acid level >5.5 mg/dL.
©2007 RUSH University Medical Center

Methods
• The average of the three systolic BP (SBP) and diastolic BP (DBP) measurements, made at least 10 minutes apart, was used in the analysis.
• The first and the last Korotkoff sounds were used to determine SBP and DBP, respectively.
• The 4th Task Report on High BP in Children and Adolescents Pediatrics . 2004;114;555-574
©2007 RUSH University Medical Center
Methods (cont’d)
• Body mass index (BMI) was calculated as the ratio between weight in kilograms and height in square meter and then converted to a sex and age-specific BMI percentile value derived from the Centers for Disease Control and Prevention growth charts.
• Daniels SR., et al. Circulation 2011; 124:1673-1686
©2007 RUSH University Medical Center

Study design
• Eligible patients were randomly alternated between two groups to receive either enalapril alone (Group 1) or combination of enalapril and allopurinol (Group 2) for 8 weeks.
©2007 RUSH University Medical Center

Study design (cont’d)
• The enalapril dose was 0.15 mg/kg/day given once daily (maximum daily dose 20 mg).
• Allopurinol was administered as 5 mg/kg/day in 2 divided doses (maximum daily dose 300 mg) according to pediatric dosing guidelines.
©2007 RUSH University Medical Center

Study design (cont’d)
• Blood and urine samples were obtained for CBC, electrolytes, BUN, creatinine, uric acid, and alanine transaminase levels at the baseline and again at 4 and 8 weeks of treatment follow-up.
• Random urine samples were also collected for routine urinalysis.
©2007 RUSH University Medical Center

Study design (cont’d)
• Follow-up clinic visits for BP and safety assessments occurred at weekly intervals.
• Patients were excluded from the study if their rate of adherence to medications was less than 80% as measured by tablet count during weekly clinic visits.
©2007 RUSH University Medical Center

Patients referred for the evaluation hypertension (n=118)
Excluded (n=47) • Prehypertension (n=23) • Abnormal urinalysis (n=11) • Stage 2 hypertension (n=5) • Hydronephrosis (n=4) • Cystic kidney disease (n=2) • White coat hypertension (n=1) • Pheochromocytoma (n=1)
Patients with stage 1 hypertension (n=71)
Excluded (n=19)Serum uric acid <5.5 mg/dL
Patients randomized (n=52)
Enalapril plus allopurinol (n=28)
Excluded (n=4) • poor compliance (n=4)
Excluded (n=4) • Poor compliance (n=3) • stage 2 hypertension
Completed 8 weeks study and included in analysis (n=20)
Completed 8 weeks study and included in analysis (n=24)
Enalapril (n=24)
Methods (cont’d)
• All study subjects received recommended lifestyle education program consisting regular aerobic exercise, and a diet that was low in sodium enriched in potassium, calcium (vegetables and fruits) the so-called Dash diet which is known to have antihypertensive effect even in patients receiving antihypertensive medication.
• Daniels SR et al. Circulation 2011;124:1673-1686• Hardnes KE, et al. J hum NUTR Diet 201;23:3-10
©2007 RUSH University Medical Center
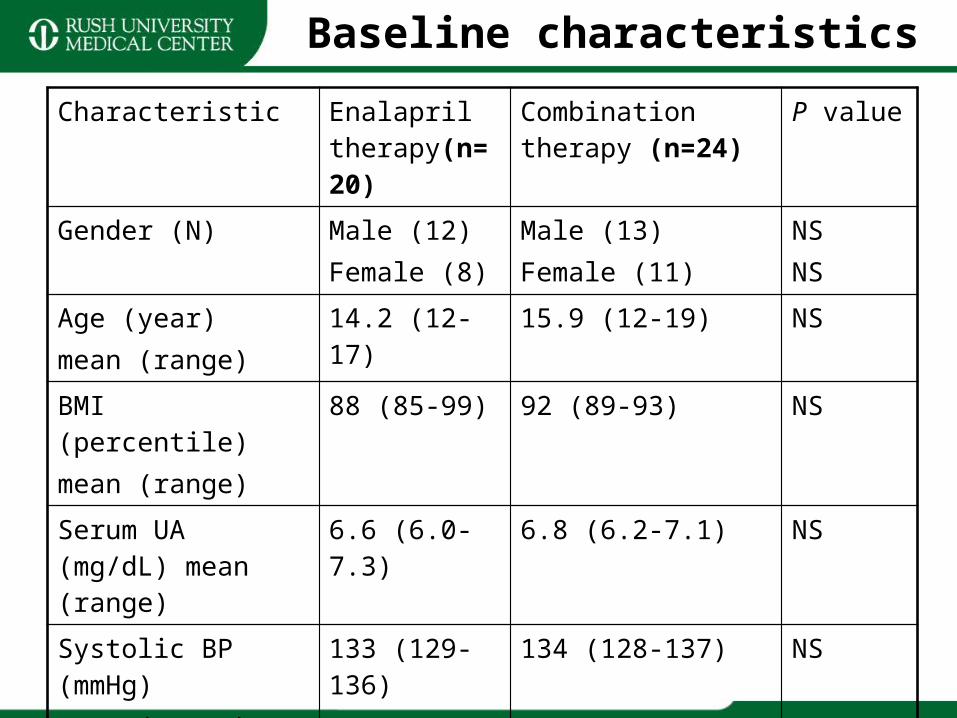
Characteristic Enalapril therapy(n=20)
Combination therapy (n=24)
P value
Gender (N) Male (12)Female (8)
Male (13)Female (11)
NSNS
Age (year) mean (range)
14.2 (12-17) 15.9 (12-19) NS
BMI (percentile)mean (range)
88 (85-99) 92 (89-93) NS
Serum UA (mg/dL) mean (range)
6.6 (6.0-7.3) 6.8 (6.2-7.1) NS
Systolic BP (mmHg)mean (range)
133 (129-136) 134 (128-137) NS
Diastolic BP (mmHg)Mean (range)
85 (82-86) 86 (80-87) NS
Baseline characteristics

Parameter Enalapril therapy (n=20)
Combination therapy (n=24)
P value
Change in systolic BP (mmHg)
-4.3 (-2.1 to -6.7) -8.2 (-7.2 to -9.8) 0.001
Change in diastolic BP
-2.4 (-1.1 to -2.2) -6.3 (-1.9 to -7.8) 0.006
Serum uric acid (mg/dL)
-5.1 (-5.8 to-6.7) -3.3 (-2.9 to-5.2) 0.002
Results


©2007 RUSH University Medical Center

Resaults (cont’d)
• After 8 weeks treatments, BP reduction was greater, percent of treatment group achieving target BP level was greater, and serum uric acid level was lower in the combination treatment group.
• There were no drugs adverse effects during the course of therapy.
©2007 RUSH University Medical Center
Conclusions
• Allopurinol enhances the BP lowering effect of enalapril in hyperuricemic adolescents with stage-1 primary HTN by reducing serum UA level.
• Treatment regimen that lowers serum uric level may be indicated to decrease the incidence of CVD by reducing serum UA level.
• Assadi F. J Nephrol, 2014, 27:51-56
©2007 RUSH University Medical Center